

Abstract
Diffuse large B-cell lymphoma patients have a 5% overall risk of central nervous system events (relapse or progression), which account for high morbidity and frequently fatal outcomes,1 and shortened overall survival of <6 months.2 Early diagnosis of central nervous system events is critical for successful treatment and improved prognosis. Identification of patients at risk of central nervous system disease is critical to accurately identify candidates for central nervous system prophylaxis vs. therapy.3–5 This report by the Spanish Lymphoma Group (GELTAMO) aims to provide useful guidelines and recommendations for the prevention, diagnosis, and treatment of central nervous system diffuse large B-cell lymphoma patients with, or at risk of, leptomeningeal and/or brain parenchyma lymphoma relapse. A panel of lymphoma experts working on behalf of GELTAMO reviewed all data published on these topics available in PubMed up to May 2016. Recommendations were classified according to the Grading of Recommendations Assessment Development and Evaluation (GRADE) approach.6 A practical algorithm based on the proposed recommendations was then developed (Figure 1). Initial discussions among experts were held in May 2014, and final consensus was reached in June 2016. The final manuscript was reviewed by all authors and the Scientific Committee of GELTAMO.
Risk factors for central nervous system involvement in diffuse large B-cell lymphoma
Several factors hinder the identification of risk factors for central nervous system (CNS) involvement in diffuse large B-cell lymphoma (DLBCL), including the retrospective nature of most studies, the relatively low frequency of CNS relapse in DLBCL, and the heterogeneity of CNS prophylaxis methods used in these studies. Moreover, the impact of newly developed diagnostic tools (such as multiparameter flow cytometry [FCM]) and new treatments introduced in the last decade, in particular rituximab, has still not been fully clarified.
Several studies4,5,7–10 and a recent meta-analysis1 have described a decrease in rates of CNS relapse in the post-rituximab era (probably due to improved control of systemic lymphoma), in addition to a change in the pattern of CNS relapse, with predominance of parenchymal over leptomeningeal relapse, isolated over combined (systemic plus CNS) relapses, and delayed CNS relapses. Similarly, recently published British guidelines11 have concluded that the incidence of CNS relapse decreased after the introduction of rituximab (Table 1).
Table 1.
Influence of systemic rituximab treatment on the incidence of CNS relapse in DLBCL and risk factors for CNS disease.
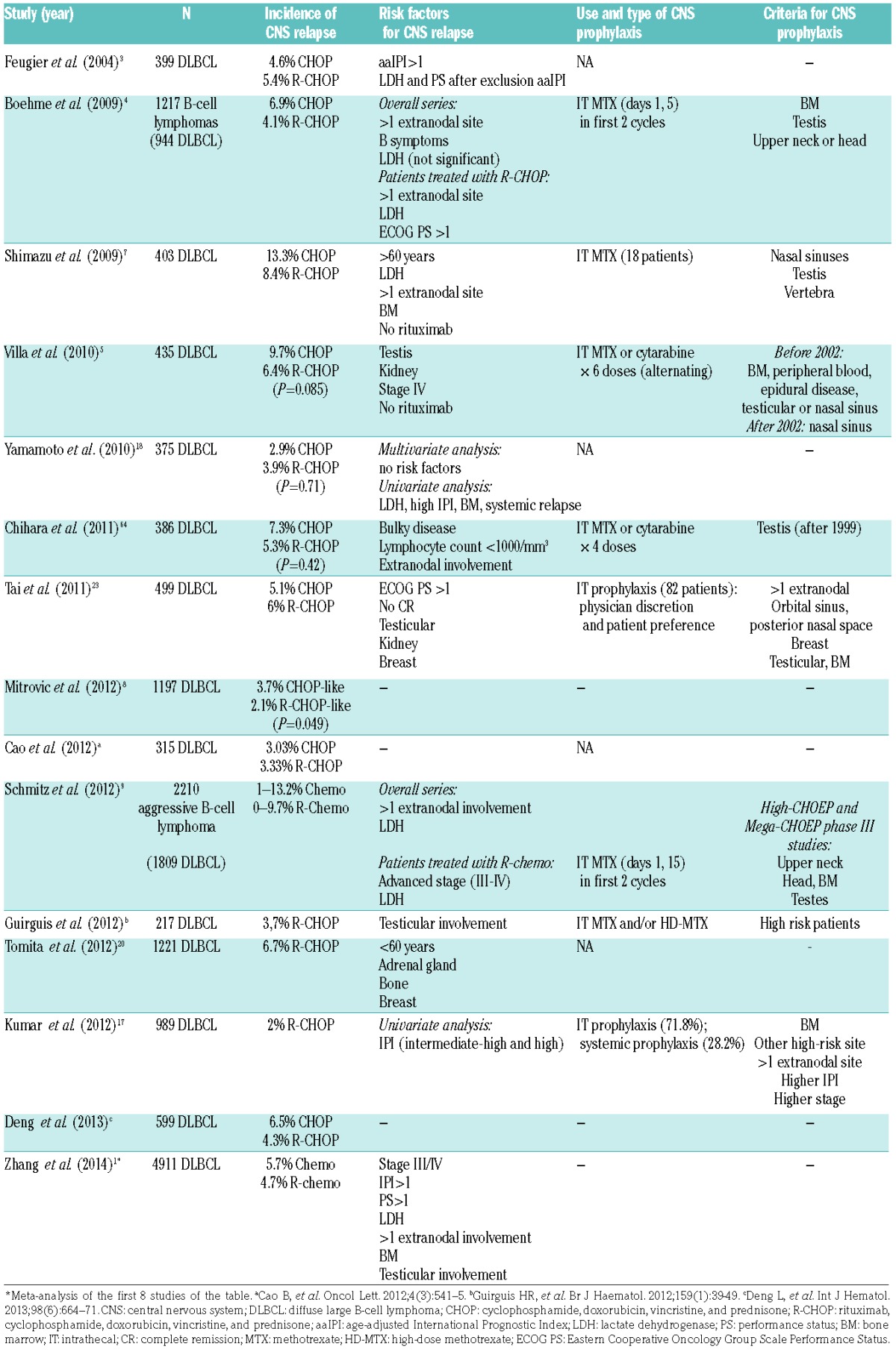
The identification of risk factors has been the major goal of many studies of CNS involvement. Several large retrospective studies conducted in the pre-rituximab era12–15 reported higher rates of CNS relapse in patients with increased serum lactate dehydrogenase (LDH) levels and/or involvement of >1 extranodal site, although these factors failed to predict CNS relapse in more than half of all cases.12 In addition to the involvement of >1 extranodal site and increased LDH, International Prognostic Index (IPI) score was also identified as an independent predictor for CNS relapse in other studies.13,16 A post-rituximab era study of 399 DLBCL patients, randomized to R-CHOP or CHOP chemotherapy,3 identified an age-adjusted IPI (aaIPI) >1 as the only risk factor for CNS involvement, although a high aaIPI score was recorded for more than 60% of the patients. When aaIPI was excluded from the analysis, elevated LDH and a poor performance status (PS >1) were identified as independent predictive factors for CNS relapse. Similarly, in the randomized RICOVER-60 trial,4 the combination of increased LDH levels, the involvement of >1 extranodal site, and PS >1 (recorded for 4.8% of patients) was associated with a probability of CNS relapse of 33.5% as compared with 2.8% in the remaining patients. Elevated LDH levels, the involvement of >1 extranodal site, and an intermediate-high or high IPI score have also been cited as risk factors in other retrospective studies, reviews, and meta-analyses of the post-rituximab era (Table 1).1,2,7,9,17,18
Accumulated evidence from studies of extranodal involvement have shown that testicular or breast involvement (particularly as primary lymphoma, but also as secondary involvement) is clearly associated with a higher rate of CNS relapse.5,19–21 A growing body of evidence indicates a higher CNS relapse rate among patients with renal involvement by lymphoma. Villa and colleagues22 reported CNS involvement in 36% of patients with DLBCL with renal involvement. Similarly, Tai and colleagues23 found that renal involvement was the primary risk factor for CNS relapse, ahead of even breast or testis involvement.
The association of other extranodal sites with CNS relapse is less clear. Epidural space involvement has been proposed as a risk factor in very old studies,24 but CNS prophylaxis is recommended for these patients in recently published British guidelines,11 potentially because of the anatomical proximity. Regarding extranodal craniofacial involvement, a recent review of 4,155 patients from 11 consecutive trials by the German High-Grade Non-Hodgkin Lymphoma Study Group25 reported no differences in the 2-year cumulative rate of CNS disease between rituximab-treated patients with and without craniofacial involvement (1.6% vs. 3.4%, P=0.682), in line with the findings of another more recent study.26
Based on all the above evidence, a new prognostic model to assess the risk of CNS disease in DLBCL (CNS-IPI) has been proposed.27 This model has been validated in other series from the British Columbia Cancer Agency,28 and includes the 5 IPI factors in addition to kidney/adrenal gland involvement, and it stratifies patients into 3 risk groups for CNS relapse: low risk (0–1 factors; 2-year risk of 0.6%), intermediate risk (2–3 factors; 2-year risk of 3.4%), and high risk (4–6 factors; 2-year risk of 10.2%).
The influence of the biology of DLBCL on CNS relapse remains a matter of debate. There is still insufficient evidence to demonstrate an influence of B-cell origin (germinal center vs. non-germinal center DLBCL) on CNS disease. However, many retrospective and recent studies have described a high percentage of CNS involvement in DLBCL cases with MYC rearrangement, particularly when associated with either additional BCL-2 or BCL-6 gene rearrangements: in these patients, the frequency of CNS disease ranges from 9% to 45%. Based on these results Fletcher and Kahl2 recommended that patients with DLBCL and MYC rearrangements be considered at high risk of CNS relapse. In another recent study, Savage et al.29 reported that DLBCL patients and dual expression of MYC (≥40% positivity) and BCL2 (≥50% positivity) determined by immunohistochemistry, had higher risk of CNS relapse (2-year risk of 9.7% vs. 2.2%, P=0.001). This study also showed increased risk for those patients with activated B-cell or non-germinal center B-cell origin, but significance was not retained in the multivariate analysis.
Summary and recommendations for CNS prophylaxis in DLBCL based on the presence of risk factors
The authors recommend screening patients for CNS involvement by lumbar puncture and cerebrospinal fluid (CSF) analysis by conventional cytology (CC) and FCM in order to provide prophylaxis in the following situations:
Increased serum LDH and involvement of >1 extranodal site (recommendation 1, level of evidence B)
Extranodal involvement of testis (recommendation 1, level of evidence B) or breast (recommendation 2, level of evidence B)
Extranodal involvement of kidney, adrenal gland (recommendation 2, level of evidence C) or epidural space (recommendation 2, level of evidence D).
High risk CNS-IPI (recommendation 2, level of evidence B)
MYC rearrangements associated to BCL2 or BCL6 rearrangements (recommendation 2, level of evidence C).
Diagnostic screening for CNS disease in DLBCL
Definitive diagnosis of central nervous system lymphoma (CNSL) relies on a positive CSF CC.30 However, CSF samples are only obtained in a selected subgroup of DLBCL patients14 due to the low frequency of CNSL, as discussed above in detail.14 Diagnosis based on histopathology of stereotactic biopsy specimens, including ocular biopsy in cases with positive ophthalmological evaluation, is usually limited to a small number of CSF-negative patients, mostly in cases of suspected primary CNS lymphoma (PCNSL).
Clinical presentation: Clinical symptoms associated with CNSL are the first indication of CNS disease in many patients. However, DLBCL patients who have CNSL frequently display subtle symptoms, which are either unrecognized or difficult to distinguish from those related to the primary disease or the treatment thereof. Thus, whenever present, neurological symptoms should prompt further CNS imaging and/or CSF analysis, depending on the clinical context of the patient and the results of complementary diagnostic procedures/tests.
Imaging techniques: Of the imaging techniques currently available, the most informative is magnetic resonance imaging (MRI), including contrast-enhanced MRI, with a sensitivity of 71% vs. 36% for computerized tomography (CT).31 Thus, evaluation of CNSL in symptomatic patients typically includes cranial MRI,32 except in the few cases in which the procedure is contraindicated and CT is recommended. Most CNSL lesions analyzed by MRI and/or CT are associated with either diffuse or, more frequently, local (contrast) enhancement, which often includes the leptomeninges, cranial nerves, or the periventricular region.33 However, these patterns have relatively low specificity and cannot be usually considered truly diagnostic, even in previously diagnosed DLBCL cases,34 particularly after corticosteroid therapy.35,36 Diagnosis of CNSL based exclusively on imaging techniques (e.g., MRI) thus continues to pose a clinical challenge, underscoring the need for more definitive diagnostic approaches to demonstrate the tumoral nature of the lesions.
More recently developed imaging techniques including positron-emission tomography have been proposed to potentially contribute to diagnosis in specific cases. However, due to their limited specificity, additional studies are still necessary to define their precise value in the diagnosis of CNSL.37,38
Histopathology: Histopathological and immunohistochemical analysis of stereotactic biopsy samples is considered a standard procedure for the diagnosis of PCNSL,32,39 but is not a routine procedure in patients who already have been diagnosed with DLBCL. Stereotactic biopsy is an invasive procedure, which is of relatively limited sensitivity (20%–65% in immunocompetent patients), particularly in patients treated with corticosteroids. Moreover, this approach cannot be used in a subset of patients due to the location of the lesions.
CSF cytology: While CSF cytology is a highly specific diagnostic approach for CNSL in DLBCL, it is of limited sensitivity, and produces a significant percentage (20%–60%) of false-negative results,40–42 particularly when used to analyze small volumes from single samples, processed with delay, from patients treated with corticosteroids.40,43 Furthermore, the morphological features of inflammatory lymphocytes in CSF can overlap with those of lymphoid tumor cells, leading to false-positive results in some cases.44
Multiparameter flow cytometry analysis of CSF samples
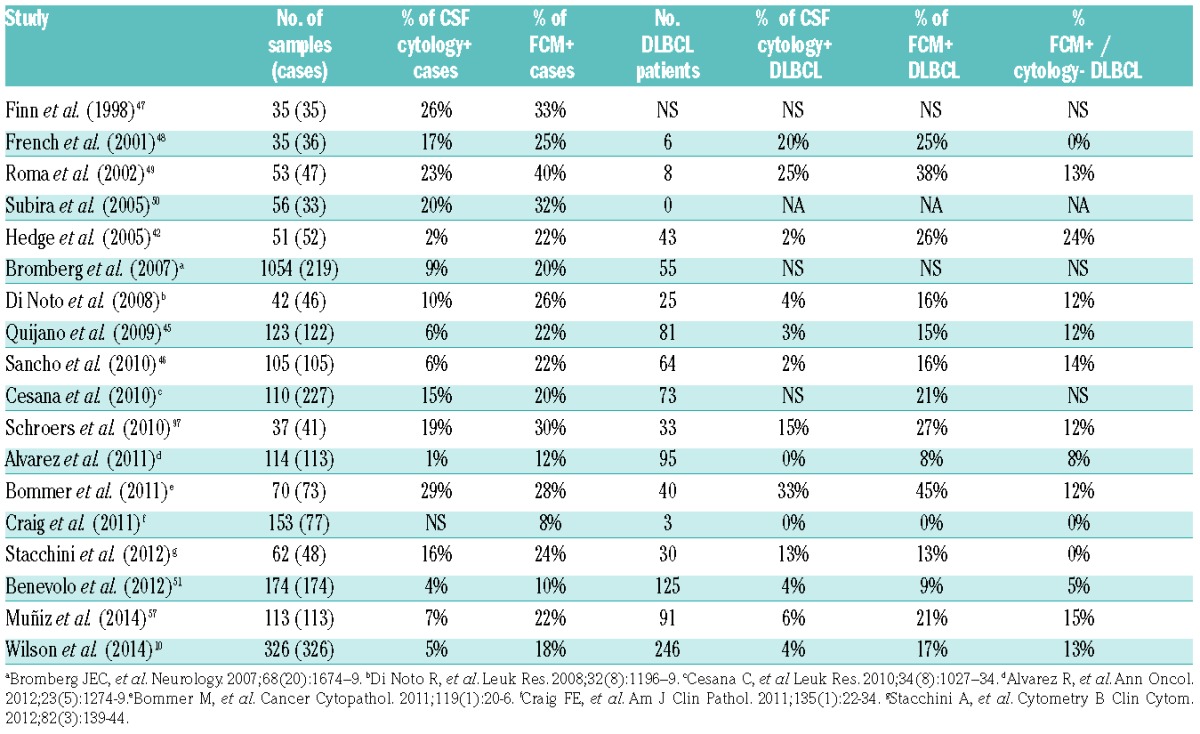
Many studies have demonstrated the utility of FCM for detecting CNS disease in DLBCL.10,42,45,46 Early studies analyzing non-stabilized CSF samples by ≤4-color FCM already demonstrated increased sensitivity in between 3% and 20% of cases as compared with cytology (Table 2).42,47–50 More recent analyses of larger series of CSF-stabilized samples using 4–8 color FCM have confirmed the greater sensitivity of FCM vs. CC with a median proportion of occult CNSL (FCM+/CC− CSF) of 12% (range: 5%–13%) (Table 1).10,45,51 Patients with occult CNSL (i.e., CC− and FCM+ CSF) typically showed lower levels of CSF infiltration (<20% or <1 tumor B cell/μL) than FCM+/CC+ cases,45 further supporting the greater sensitivity of FCM vs. CC. These studies10,45,51 also showed very few false-negative FCM results (range: 0%–<1%), further supporting its greater diagnostic efficiency with respect to CC.
Table 2.
Frequency of cases including diffuse large B-cell lymphoma (DLBCL) patients showing cerebrospinal fluid (CSF) involvement by cytology vs. flow cytometry (FCM).
Early studies showed that patients with occult CNSL more frequently present neurological symptoms than FCM−/CC− cases (57% and 10%, respectively),45 suggesting a clinical impact of occult CNS disease. More recently, Wilson and colleagues10 confirmed that among DLBCL cases with negative CSF cytology, the presence of occult CNSL as detected by FCM is associated with a significant reduction in CNS-recurrence-free survival (73% vs. 94%) and overall survival (OS at 3 years: 38% vs. 69%) compared with patients without CSF involvement. These results are in agreement with those of an analysis of 174 lymphoma patients, including 125 DLBCL cases.51 However, it should be noted that the prognostic impact of occult CNSL reported by Wilson and colleagues failed to reach significance among DLBCL cases treated with immunochemotherapy regimens.10
Taken together, these results provide sufficient evidence to support the mandatory use of FCM in the diagnostic work-up of CNS involvement in DLBCL. However, particular attention should be paid to the specific FCM approach used. Immediate sample preservation (preferably in TransFix®)52 and the use of standardized sample preparation procedures and validated ≥8-color antibody combinations for simultaneous identification of all cell subsets present in normal/reactive CSF samples, as well as tumor B-cells, is strongly recommended.53 Evaluation for blood contamination should also be considered in cases with peripheral blood involvement by systemic lymphoma, in which CSF infiltration by blood cells (e.g., red cells and neutrophils) is observed.10
Other biochemical and CSF biomarkers
Increases in overall protein and LDH levels, the presence of pleocytosis, and decreased glucose levels in CSF have long been associated with CNSL.14,54 However, these parameters are nonspecific and therefore unreliable for routine diagnosis of CNS disease.55,56 Similarly, CSF levels of soluble (s)CD21, sCD22, sCD24, sCD38, sCD44, sCD72, and immunoglobulin (IG) heavy and light chain isotypes are of limited diagnostic utility.57 Similar rates of CSF-positive cases (8%–13% vs. 11%–16%) have been obtained by polymerase chain reaction (PCR) analysis of IG gene sequences and cytomorphology, respectively, with a high frequency of unexplained discrepant cases,58 suggesting that the utility of PCR analysis of IG genes may be limited to selected cases in which CSF cytology and FCM are not informative.56 Furthermore, increased CSF levels of sCD19, sAnti-thrombin III (sATIII), sCD27, β2 microglobulin, IL-6, IL-10, CXCL13, neopterin, osteopontin, and several microRNAs (miRNA19b, miRNA21, and miRNA92a) have emerged as potentially useful biomarkers for CNS lymphoma, particularly in cases of PCNSL.57,59–63 However, the potential value of these markers has only been investigated in a few studies, which used varying endpoints (usually one per study), and included few DLBCL cases with secondary CNSL.
Summary and recommendations for diagnosis of CNS disease in DLBCL
Include CNS imaging in the diagnostic work-up of DLBCL patients who present with symptoms of suspected CNSL; in such cases, MRI (including contrast enhanced MRI) is preferable (recommendation 1, level of evidence A).
Use standardized and validated >8-color FCM evalua tion of stabilized CSF in the diagnostic work-up of DLBCL patients at risk of CNS disease for the identification of occult CNSL (CC−/FCM+) (recommendation 1, level of evidence A).
The presence of occult CNSL in high-risk DLBCL may be considered an adverse prognostic factor, although its independent prognostic value has not been definitively established (recommendation 2, level of evidence B).
Despite their potential value, several other CSF biomarkers (e.g., sCD19, sIL-10 and/or sCXCL13, neopterin, and several miRNAs) cannot be currently used for the diagnosis of CNSL in DLBCL (recommendation 2, level of evidence C).
In case of suspected CNSL in DLBCL patients with negative CSF, stereotactic brain biopsy is still not regarded as a useful routine diagnostic test. However, ophthalmological evaluation with ocular and/or brain biopsy may be required in specific cases (recommendation 2, level of evidence C).
Efficacy of chemoprophylaxis in preventing CNS relapse in DLBCL
CNS relapse in DLBCL mainly occurs within less than one year after diagnosis (median: 6 months).12,64,65 This pattern of early relapse suggests that affected patients probably harbor occult malignant cells in the CNS at diagnosis.16,42,65 Although FCM improves the identification of CNS involvement by 4- to 10-fold as compared with cytology, it identifies only a fraction of patients that are destined to experience CNS relapse.65 These findings support the consensus that any planned prophylactic measures should be adopted early in the treatment course.11
CNS-directed prophylaxis
Historically, CNS prophylaxis is most commonly delivered via the intrathecal (IT) route,11,66,67 targeting in particular the leptomeningeal compartment,11 although some authors suggest that IT prophylaxis may be ineffective.2,4
IT methotrexate prophylaxis: The administration of IT methotrexate (MTX) prophylaxis is recommended during each cycle of chemotherapy, with a total of 4 to 8 doses.68 The most common dose used is 12 mg, which achieves therapeutic levels in the CSF (>1 μmol/L) for 24 to 48 hours.68,69 IT MTX doses of 12.5 mg and 15 mg have also been reported.4,13,67,68,70 Of note, studies supporting this approach11,13,70–73 have several limitations, including small sample sizes, absence of a control arm, and co-administration of systemic MTX.
In contrast, two large trials4,16 reported no protective benefit of IT MTX prophylaxis. However, these studies were not originally designed to test the efficacy of CNS prophylaxis.11 Moreover, analysis was only possible in the RICOVER-60 trial4 due to a high number of protocol violations (49%). A recent study using the National Comprehensive Cancer Network (NCCN) database for non-Hodgkin lymphoma (NHL) reported no prophylaxis-associated survival benefit,17 although this study was clearly at risk of potential physician bias in selecting patients for IT therapy.
Despite all the above, published guidelines11 and clinical trials exploring new treatment options for DLBCL include IT MTX as prophylaxis for high-risk patients.
Data reported suggest that several regimens could be active against CNS relapses. Thus, improved outcomes have been suggested for R-DA-EPOCH in low and intermediate IPI patients, and in an ongoing phase 3 study comparing R-DA-EPOCH with R-CHOP that might clarify the potential impact of continuous infusion on CNS relapse rates in the IT MTX settings (IT MTX given for high risk patients as CNS prophylaxis in both protocol arms).74
Improved outcomes and lower CNS relapse rates have been reported in young patients for R-ACVBP vs. R-CHOP associated with IT MTX in both arms, but high dose systemic MTX being administered only in the R-ACVBP arm.75
Other IT drugs: A number of other drugs including liposomal cytarabine (LC) and rituximab can be administered intrathecally.
IT LC maintains cytotoxic concentrations in CSF for up to 14 days after a single IT injection,76,77 but is not licensed for prophylactic use.11 The efficacy and toxicity of LC in the prophylaxis of CNS involvement specifically in DLBCL has only been analyzed in two recently published studies.78,79
There are sufficient data to suggest that IT rituximab is efficacious in the treatment of CNS relapse,80,81 but no data support its use in a prophylactic setting.
Triple IT: In Spain, triple intrathecal therapy (TIT, methotrexate, cytarabine and hydrocortisone) is the most commonly used schedule for CNS prophylaxis in hematological malignances for the nationwide use of the PETHE-MA risk-adapted protocol for lymphoblastic lymphoma and Burkitt lymphoma, which includes TIT for CNS prophylaxis and limits the use of CNS irradiation.66 TIT is also commonly used in DLBCL for CNS prophylaxis, although no studies have compared TIT with IT MTX treatment, and there is no definitive evidence that CNS direct prophylaxis with IT administration improves CNS progression-free survival in patients with parenchymal CNS involvement. Importantly also, IT chemotherapy is not without clinical risk and toxicity, particularly for older and frail patients.
Systemic prophylaxis
Data on the potential effectiveness of systemic chemotherapy for CNS prophylaxis in patients with NHL at high risk of CNS relapse are mainly based on information extrapolated from studies of childhood acute lymphoblastic leukemia.11,82
The appropriate intravenous (IV) MTX dose to achieve therapeutic levels in the CNS is controversial. IV MTX doses ≥3 g/m2 appear to produce therapeutic levels in CSF and parenchyma. Three studies conducted in the post-rituximab era examined this method of prophylaxis using high-dose MTX (HD-MTX) doses of 3 g/m2 to 3.5 g/m2, although co-administered drugs, timing, and the number of doses administered varied by protocol.2,75,83,84 Abramson and colleagues reported good outcomes in a retrospective analysis of 65 high-risk patients with DLBCL who received a median of 3 cycles of HD-MTX (3.5 g/m2, range 1–8 cycles) administered on day 15 of alternating cycles of R-CHOP.83 Patients receiving this treatment regimen should have a good baseline condition, and should be closely and carefully monitored for potential toxicity. Adverse effects of MTX include mucositis, myelosuppression, neurotoxicity, and nephrotoxicity. Pre-treatment alkalization of urine and post-treatment leucovorin rescue are considered standard approaches to minimize these toxic effects.68
Systemic prophylaxis with HD-cytarabine in a small sample of DLBCL patients was found to have no clear beneficial role in preventing CNS disease.2,85
New agents like ibrutinib and lenalidomide, which cross the brain barrier, are being explored, and the impact on CNS relapse risk in DLBCL remains to be established.86,87
Systemic prophylaxis with HD-cytarabine in a small sample of DLBCL patients was found to have no clear beneficial role in preventing CNS disease.2,85
New agents like ibrutinib and lenalidomide, which cross the brain barrier, are being explored and the impact on CNS relapse risk in DLBCL remains to be established.86,87
Which prophylactic strategy should be chosen?
The question as to the most effective and least toxic route of CNS prophylaxis delivery (IT, parenteral, or a combination thereof) remains largely unanswered, and should be addressed in large scale randomized clinical trials comparing systemic and IT chemoprophylaxis.68
Aviles and colleagues88 analyzed a homogenous group of 3,258 DLBCL patients treated with CHOP or R-CHOP, 1,005 of whom received different CNS prophylaxis schedules (radiotherapy, IT MTX, HD-MTX, or rituximab). No clear differences were observed between the different prophylaxis schedules. Furthermore, rates of CNS relapse were similar in patients who received prophylaxis (6%) and those who did not (5.9%).
Cheah and colleagues89 recently performed a retrospective analysis of patients with high-risk DLBCL, comparing three different strategies of CNS-directed therapy: IT MTX with R-CHOP (group 1); R-CHOP with IT MTX and two cycles of HD-MTX (group 2); and dose-intensive systemic chemotherapy (Hyper-CVAD or CODOXM/IVAC) with IT/IV MTX (group 3). A total of 23 CNS relapses occurred (24%, 8%, and 2.3% in groups 1, 2, and 3, respectively). Although these data are limited by the retrospective nature of the study, the addition of HD-MTX and/or HD-cytarabine appears to be associated with lower incidence of CNS relapse as compared with IT chemotherapy alone.
Figure 1.
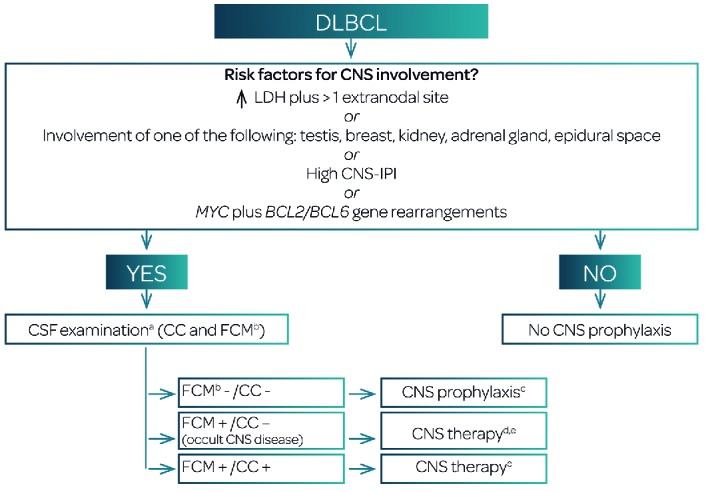
Practical algorithm based on the recommendations of the Guidelines. aCSF examination should be also performed in presence of neurological symptoms, in addition to imaging techniques (MRI, CT). bThe use of standardized and validated ≥8-color FCM evaluation of stabilized CSF samples is recommended (with immediate addition of RPMI1640 or Transfix® to CSF samples). cThe group recommends CNS prophylaxis in FMC−/CC− patients with high-risk factors for CNS relapse until future studies are available. IV HD-MTX (≥3 g/m2) alternating with immunochemotherapy or IT MTX administered during primary therapy (12 mg once per cycle, 4– 6 doses), depending on age, performance status, comorbidities and patient and/or physician’s preferences. IV MTX should be given in line with published schedules, and in the context of performance status and renal function. Delay of subsequent cycles of systemic immunochemotherapy should be avoided. Patients with primary testicular lymphoma should receive IT MTX during primary chemotherapy. Triple IT therapy (MTX 15 mg, cytarabine 40 mg, and hydrocortisone 20 mg) is a reasonable option for CNS prophylaxis. dThere is no direct evidence to support the adoption of different treatment decisions in patients with occult leptomeningeal disease (CC−/FCM+): HD-MTX and/or IT chemotherapy should be considered for these patients. eIn cases of CNS involvement at the time of DLBCL diagnosis: HD-MTX (associated IT therapy if leptomeningeal disease is demonstrated). In patients for whom HD-MTX is inadequate due to age or comorbidities, IT liposomal cytarabine should be considered. In the case of CNS relapse: salvage therapy (HD-MTX-based induction) followed by ASCT (depending of performance status and age of the patient). Thiotepa and BCNU should be included in the conditioning regimen before ASCT. In the case of refractoriness or early relapse after HD-MTX, consider clinical trial or radiotherapy. DLBCL, diffuse large B-cell lymphoma; CNS, central nervous system; LDH, lactate dehydrogenase; CNS-IPI, central nervous system-International Prognostic Index;28 CC, conventional cytology; FCM, multiparameter flow cytometry; MRI, magnetic resonance imaging; CT, computerized tomography; IV, intravenous; HD-MTX, high dose-MTX; MTX, methotrexate; IT, intrathecal; ASCT, autologous stem cell transplant.
Primary testicular lymphoma
Patients with primary testicular involvement have a particularly high risk of CNS involvement (>15%) when achieving a complete response (CR). Treatment recommendations for these patients differ from those for other forms of extranodal DLBCL. Vitolo and colleagues reported a 6% CNS relapse rate after 5 years in patients treated with a combination of R-CHOP plus four doses of IT MTX and contralateral testis irradiation.72 No data are available on treatment with IV MTX alone in this scenario.
Summary and recommendations for CNS prophylaxis
CNS-directed prophylaxis should be offered to patients at high-risk of CNS relapse (recommendation 1, level of evidence B).
IV MTX is recommended as CNS prophylaxis in high-risk patients (recommendation 2, level of evidence B).
IV MTX as CNS prophylaxis should be administered during primary therapy at a dose of ≥3 g/m2, alternating with immunochemotherapy (recommendation 1, level of evidence B), and should be given according to published treatment schemes and in the context of performance status and renal function. Delay of subsequent cycles of systemic immunochemotherapy should be avoided (recommendation 1, level of evidence B).
IT MTX (recommendation 2, level of evidence C) or triple IT (recommendation 2, level of evidence C) may be reasonable options for prophylaxis, depending on age, performance status, and comorbidities
IT MTX (12–15 mg once per cycle, 4–6 doses) or triple IT (MTX 15 mg, cytarabine 40 mg, hydrocortisone 20 mg) as CNS prophylaxis should be administered during primary therapy (recommendation 1, level of evidence B).
Patients with primary testicular lymphoma should receive IT MTX during primary chemotherapy (recommendation 1, level of evidence B).
Treatment of central nervous system involvement of lymphoma
Secondary involvement of CNS in aggressive NHL can occur at presentation or early in the first year, usually associated with or anticipating systemic relapse. Accordingly, both CNS and systemic lymphoma should be considered for the treatment of CNS dissemination.
Whole-brain radiotherapy
The usefulness of radiotherapy for the management of CNS lymphoma is limited by its toxicity, especially in older patients. Whole-brain radiotherapy has been used in combination with chemotherapy in PCNSL, but its true impact on outcome remains controversial.90 While reduced-dose radiotherapy may cause less neurotoxicity, there is a paucity of relevant randomized studies. At present, whole-brain radiation is generally reserved for salvage therapy in patients with MTX resistance.91
In secondary CNS lymphoma (SCNSL), radiotherapy could be considered as an adjuvant treatment in patients with large masses or with blockade of CSF flow.92
Systemic chemotherapy
Systemic chemotherapy agents that cross the blood-brain barrier (BBB) become distributed throughout the neural axis, avoiding the need for IT chemotherapy administered via multiple lumbar punctures or ventricular reservoirs. However, toxicity in bone marrow and other organs should be considered.92
High-dose methotrexate
IV MTX is active in primary and secondary CNSL although the optimal dosage is yet to be defined. Doses ≥1 g/m2 achieve tumoricidal levels in brain parenchyma, doses of 8 g/m2 produce higher cytotoxic levels in serum and CSF than IT MTX, and doses of 3 g/m2 are sufficient to treat brain and leptomeningeal disease, without associated IT MTX.91 There is no consensus as to the optimal number of cycles needed, although at least 4 cycles of HD-MTX may be necessary. The toxic effects of HD-MTX should be carefully considered, particularly nephropathy. Advanced age, poor performance status, and renal or liver dysfunction should be considered contraindications for HD-MTX.
Polychemotherapy
A study of patients with PCNSL by Ferreri and colleagues demonstrated a failure-free survival benefit in patients who received HD-MTX plus HD-cytarabine as induction therapy, followed by radiotherapy as consolidation.93 Other anti-lymphoma agents that cross the BBB such as procarbazine or ifosfamide have been used in combination with HD-MTX, and have showed encouraging activity.91,92,94 Immunochemotherapy consisting of HD-MTX, intravenous rituximab, and oral temozolomide may be a feasible option, as demonstrated by Wong and colleagues in a study of PCNSL patients.95
Intensification chemotherapy and autologous hematopoietic stem cell transplantation
High-dose chemotherapy consolidation followed by autologous stem cell transplant (ASCT) rescue is a very promising option in patients with recurrent SCNSL, with better outcomes in patients who achieve CR before transplantation.96
In a German prospective phase II study, HDMTX, ifosfamide, dexamethasone and IT LC followed by HD-cytarabine, thiotepa and IT LC, and, for responding patients, consolidation with BCNU, thiotepa, etoposide, and ASCT rescue, resulted in 50% CR, with a 2-year OS rate of 68% after transplantation.97 In another recent Italian trial, HDMTX and cytarabine, followed by R-HDS (rituximab, cyclophosphamide, cytarabine, and etoposide) supported by ASCT was associated with 63% CR and 5-year OS of 68% for transplanted patients.98 Long-term survival in patients who underwent ASCT has also been reported in a retrospective international multicenter study.99
Other published conditioning regimens include other combinations including cyclophosphamide, carmustine, etoposide, busulfan and thiotepa, with or without rituximab.93,100,101 All such studies demonstrate that significant progress has been made toward cure in this difficult condition that was almost systematically fatal a few years ago.102 Hopefully, new molecules that cross the BBB, like ibrutinib or lenalidomide, might further improve the outcome of these patients.86,87
To our understanding, current treatments for this condition should incorporate multifaceted approaches, such as multi-drug regimens with non-cross resistance and CNS activity, rituximab to improve systemic lymphoma control, IT therapy, and treatment intensification with ASCT.96,101
Intrathecal therapy
IT MTX, cytarabine, and thiotepa can be administered into the spinal fluid, allowing the drug to reach the spinal cord and brain. However, these agents are rapidly cleared from the CSF, requiring administration two or three times a week. IT LC provides sustained concentrations in CSF for 14 days, allowing a more favorable administration schedule.103,104
The superiority of LC over conventional cytarabine in the treatment of lymphomatous meningitis has been demonstrated in a randomized clinical trial,76 and several studies have shown significant efficacy of LC.104–106 In terms of safety, LC should be administered with concurrent dexamethasone therapy,107,108 maintaining an adequate interval between LC administration and that of other potential neurotoxic cytostatic drugs, especially intravenous HD-MTX and HD-cytarabine.78,107
Intraventricular or IT administration of rituximab may be of value in the treatment of patients with recurrent CD20-positive CNSL.80,81 Intraventricular administration of rituximab (10–25 mg) is feasible, has shown encouraging anti-CNSL activity and clinical benefit, and when combined with intraventricular MTX results in improved responses.81
Therapeutic approach
CNS involvement by aggressive lymphoma is an extremely heterogeneous and very complex situation, with many variables determining treatment of choice and outcome, including the B-cell-of-origin subtype.
CNS and systemic involvement at diagnosis
Patients with synchronous CNS and systemic aggressive NHL at presentation should receive immunochemotherapy for the systemic disease and CNS-targeted chemotherapy for CNSL. R-CHOP plus HD-MTX followed, in patients with systemic and CNS CR, by etoposide and cytarabine consolidation is one feasible option.91 In cases of lymphomatous meningitis, R-CHOP plus LC is a possible alternative.105
CNS relapse
High-dose chemotherapy followed by ASCT is feasible and effective for recurrent aggressive CNS lymphoma, and is probably the best currently available curative option.97,99
It is important to determine whether the relapse is “MTX-sensitive” or not. In MTX-sensitive patients, HD-MTX administration to achieve maximum cytoreduction is advisable, followed by thiotepa or carmustine-based conditioning regimens and ASCT.91 Patients with MTX-resistant lymphoma or those relapsing within 6 months after consolidation schemas may not be candidates for high-dose rescue strategies. These patients should be included in clinical trials or considered for palliative treatment, according to clinical condition and other clinical or laboratory variables.91
Summary and recommendations for treatment of CNS involvement in DLBCL
Patients with systemic DLBCL and synchronous CNS parenchymatous and/or leptomeningeal lymphoma at diagnosis should be treated with HD-MTX-containing regimens (recommendation 1, level of evidence B). In cases involving leptomeningeal lymphoma, associated IT LC treatment can be administered (recommendation 1, level of evidence B).
In patients not suitable for HD-MTX treatment due to age or comorbidities, we recommend treatment with IT LC (recommendation 1, level of evidence B).
In patients with relapsed DLBCL with good clinical condition and of appropriate age: HD-MTX-based schemes followed, in responding cases, by consolidation with ASCT (recommendation 1, level of evidence B).
Thiotepa and BCNU should be included in the conditioning regimen prior to ASCT (recommendation 1, level of evidence C).
For patients with occult leptomeningeal lymphoma (CC−/FCM+), there is no direct evidence supporting the value of different therapeutic strategies. In these patients, we recommend considering treatment with HD-MTX and/or IT chemotherapy (particularly in patients for whom HD-MTX is not indicated due to age or comorbidities) (recommendation 2, level of evidence C).
In cases of refractoriness or early relapse after HD-MTX: clinical trial or whole brain radiotherapy (recommendation 2, level of evidence C).
Supplementary Material
Acknowledgments
Adelaida Velasco for her editorial assistance and patience in preparing the manuscript.
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/102/2/235
References
- 1.Zhang J, Chen B, Xu X. Impact of rituximab on incidence of and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: a systematic review and meta-analysis. Leuk Lymphoma. 2014;55(3):509–514. [DOI] [PubMed] [Google Scholar]
- 2.Fletcher CD, Kahl BS. Central nervous system involvement in diffuse large B-cell lymphoma: an analysis of risks and prevention strategies in the post-rituximab era. Leuk Lymphoma. 2014;55(10):2228–2240. [DOI] [PubMed] [Google Scholar]
- 3.Feugier P, Virion JM, Tilly H, et al. Incidence and risk factors for central nervous system occurrence in elderly patients with diffuse large-B-cell lymphoma: Influence or rituximab. Ann Oncol. 2004; 15(1):129–133. [DOI] [PubMed] [Google Scholar]
- 4.Boehme V, Schmitz N, Zeynalova S, Loeffler M, Pfreundschuh M. CNS events in elderly patients with aggressive lymphoma treated with modern chemotherapy (CHOP-14) with or without rituximab: An analysis of patients treated in the RICOVER-60 trial of the German High-Grade Non-Hodgkin Lymphoma Study Group (DSHNHL). Blood. 2009; 113(17):3896–3902. [DOI] [PubMed] [Google Scholar]
- 5.Villa D, Connors JM, Shenkier TN, Gascoyne RD, Sehn LH, Savage KJ. Incidence and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: The impact of the addition of rituximab to CHOP chemotherapy. Ann Oncol. 2009;21(5):1046–1052. [DOI] [PubMed] [Google Scholar]
- 6.Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shimazu Y, Notohara K, Ueda Y. Diffuse large B-cell lymphoma with central nervous system relapse: Prognosis and risk factors according to retrospective analysis from a single-center experience. Int J Hematol. 2009;89(5):577–583. [DOI] [PubMed] [Google Scholar]
- 8.Mitrovic Z, Bast M, Bierman PJ, et al. The addition of rituximab reduces the incidence of secondary central nervous system involvement in patients with diffuse large B-cell lymphoma. Br J Haematol. 2012;157(3):401–403. [DOI] [PubMed] [Google Scholar]
- 9.Schmitz N, Zeynalova S, Glass B, et al. CNS disease in younger patients with aggressive B-cell lymphoma: an analysis of patients treated on the Mabthera International Trial and trials of the German High-Grade Non-Hodgkin Lymphoma Study Group. Ann Oncol. 2012;23(5): 1267–1273. [DOI] [PubMed] [Google Scholar]
- 10.Wilson WH, Bromberg JEC, Stetler-Stevenson M, et al. Detection and outcome of occult leptomeningeal disease in diffuse large B-cell lymphoma and Burkitt lymphoma. Haematologica. 2014; 99(7): 1228–1235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mcmillan A, Ardeshna KM, Cwynarski K, Lyttelton M, Mckay P, Montoto S. Guideline on the prevention of secondary central nervous system lymphoma: British Committee for Standards in Haematology. Br J Haematol. 2013;163(2):168–181. [DOI] [PubMed] [Google Scholar]
- 12.van Besien K, Ha CS, Murphy S, et al. Risk factors, treatment, and outcome of central nervous system recurrence in adults with intermediate-grade and immunoblastic lymphoma. Blood. 1998;91(4):1178–1184. [PubMed] [Google Scholar]
- 13.Haioun C, Besson C, Lepage E, et al. Incidence and risk factors of central nervous system relapse in histologically aggressive non-Hodgkin’s lymphoma uniformly treated and receiving intrathecal central nervous system prophylaxis: A GELA study on 974 patients. Ann Oncol. 2000;11(6):685–690. [DOI] [PubMed] [Google Scholar]
- 14.Hollender A, Kvaloy S, Nome O, Skovlund E, Lote K, Holte H. Central nervous system involvement following diagnosis of non-Hodgkin’s lymphoma: A risk model. Ann Oncol. 2002;13(7):1099–1107. [DOI] [PubMed] [Google Scholar]
- 15.Boehme V, Zeynalova S, Kloess M, et al. Incidence and risk factors of central nervous system recurrence in aggressive lymphoma–a survey of 1693 patients treated in protocols of the German High-Grade Non-Hodgkin’s Lymphoma Study Group (DSHNHL). Ann Oncol. 2007;18(1): 149–157. [DOI] [PubMed] [Google Scholar]
- 16.Bernstein SH, Unger JM, Leblanc M, Friedberg J, Miller TP, Fisher RI. Natural history of CNS relapse in patients with aggressive non-Hodgkin’s lymphoma: a 20-year follow-up analysis of SWOG 8516 – the Southwest Oncology Group. J Clin Oncol. 2009;27(1):114–119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kumar A, Vanderplas A, LaCasce AS, et al. Lack of benefit of central nervous system prophylaxis for diffuse large B-cell lymphoma in the rituximab era: findings from a large national database. Cancer. 2012; 118(11):2944–2951. [DOI] [PubMed] [Google Scholar]
- 18.Yamamoto W, Tomita N, Watanabe R, et al. Central nervous system involvement in diffuse large B-cell lymphoma. Eur J Haematol. 2010;85(1):6–10. [DOI] [PubMed] [Google Scholar]
- 19.Zucca E, Conconi A, Mughal TI, et al. Patterns of outcome and prognostic factors in primary large-cell lymphoma of the testis in a survey by the International Extranodal Lymphoma Study Group. J Clin Oncol. 2003;21(1):20–27. [DOI] [PubMed] [Google Scholar]
- 20.Tomita N, Yokoyama M, Yamamoto W, et al. Central nervous system event in patients with diffuse large B-cell lymphoma in the rituximab era. Cancer Sci. 2012; 103(2):245–251. [DOI] [PubMed] [Google Scholar]
- 21.Hosein PJ, Maragulia JC, Salzberg MP, et al. A multicentre study of primary breast diffuse large B-cell lymphoma in the rituximab era. Br J Haematol. 2014; 165(3):358–363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Villa D, Connors JM, Sehn LH, Gascoyne RD, Savage KJ. Diffuse large B-cell lymphoma with involvement of the kidney: Outcome and risk of central nervous system relapse. Haematologica. 2011;96(7): 1002–1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tai WM, Chung J, Tang PL, et al. Central nervous system (CNS) relapse in diffuse large B cell lymphoma (DLBCL): Pre- and post-rituximab. Ann Hematol. 2011; 90(7):809–818. [DOI] [PubMed] [Google Scholar]
- 24.MacKintosh FR, Colby TV, Podolsky WJ, et al. Central nervous system involvement in non-Hodgkin’s lymphoma: an analysis of 105 cases. Cancer. 1982;49(3):586–595. [DOI] [PubMed] [Google Scholar]
- 25.Murawski N, Held G, Ziepert M, et al. The role of radiotherapy and intrathecal CNS prophylaxis in extralymphatic craniofacial aggressive B-cell lymphomas. Blood. 2014; 124(5):720–728. [DOI] [PubMed] [Google Scholar]
- 26.Lee G, Go S, Kim S, et al. Clinical outcome and prognosis of patients with primary sinonasal tract diffuse large B-cell lymphoma treated with rituximab-cyclophosphamide, doxorubicin, vincristine and prednisone chemotherapy: a study by the Consortium for Improving Survival of Lym. Leuk Lymphoma. 2015;56(4):1020–1026. [DOI] [PubMed] [Google Scholar]
- 27.Schmitz N, Zeynalova S, Nickelsen M, Ziepert M, Pfreundschuh M, Glass B, L M. A new prognostic model to assess the risk of CNS disease in patients with aggressive B-cell lymphoma. Hematol Oncol. 2013; 31(S1):96–150.22961993 [Google Scholar]
- 28.Schmitz N, Zeynalova S, Nickelsen M, et al. CNS International Prognostic Index: A Risk Model for CNS Relapse in Patients With Diffuse Large B-Cell Lymphoma Treated With R-CHOP. J Clin Oncol. 2016; 34(26):3150–3156. [DOI] [PubMed] [Google Scholar]
- 29.Savage KJ, Slack GW, Mottok A, et al. The impact of dual expression of MYC and BCL2 by immunohistochemistry on the risk of CNS relapse in DLBCL. Blood. 2016; 127(18):2182–2189. [DOI] [PubMed] [Google Scholar]
- 30.Scott BJ, Douglas VC, Tihan T, Rubenstein JL, Josephson SA. A systematic approach to the diagnosis of suspected central nervous system lymphoma. JAMA Neurol. 2013; 70(3):311–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chamberlain MC, Sandy AD, Press GA. Leptomeningeal metastasis: a comparison of gadolinium-enhanced MR and contrast-enhanced CT of the brain. Neurology. 1990;40(3 Pt 1):435–438. [DOI] [PubMed] [Google Scholar]
- 32.Abrey LE, Batchelor TT, Ferreri AJM, et al. Report of an international workshop to standardize baseline evaluation and response criteria for primary CNS lymphoma. J Clin Oncol. 2005; 23(22): 5034–5043. [DOI] [PubMed] [Google Scholar]
- 33.Freilich RJ, Krol G, DeAngelis LM. Neuroimaging and cerebrospinal fluid cytology in the diagnosis of leptomeningeal metastasis. Ann Neurol. 1995;38(1):51–57. [DOI] [PubMed] [Google Scholar]
- 34.Pauls S, Fischer AC, Brambs HJ, Fetscher S, Höche W, Bommer M. Use of magnetic resonance imaging to detect neoplastic meningitis: Limited use in leukemia and lymphoma but convincing results in solid tumors. Eur J Radiol. 2012;81(5):974–978. [DOI] [PubMed] [Google Scholar]
- 35.Johnson BA, Fram EK, Johnson PC, Jacobowitz R. The variable MR appearance of primary lymphoma of the central nervous system: Comparison with histopathologic features. Am J Neuroradiol. 1997; 18(3):563–572. [PMC free article] [PubMed] [Google Scholar]
- 36.Geppert M, Ostertag CB, Seitz G, Kiessling M. Glucocorticoid therapy obscures the diagnosis of cerebral lymphoma. Acta Neuropathol. 1990;80(6):629–634. [DOI] [PubMed] [Google Scholar]
- 37.Dethy S, Goldman S, Blecic S, Luxen A, Levivier M, Hildebrand J. Carbon-11-methionine and fluorine-18-FDG PET study in brain hematoma. J Nucl Med. 1994;35(7):1162–1166. [PubMed] [Google Scholar]
- 38.Tsuyuguchi N, Sunada I, Ohata K, et al. Evaluation of treatment effects in brain abscess with positron emission tomography: comparison of fluorine-18-fluorodeoxyglucose and carbon-11-methionine. Ann Nucl Med. 2003;17(1):47–51. [DOI] [PubMed] [Google Scholar]
- 39.Baraniskin A, Deckert M, Schulte-Altedorneburg G, Schlegel U, Schroers R. Current strategies in the diagnosis of diffuse large B-cell lymphoma of the central nervous system. Br J Haematol. 2012; 156(4):421–432. [DOI] [PubMed] [Google Scholar]
- 40.Balmaceda C, Gaynor JJ, Sun M, Gluck JT, DeAngelis LM. Leptomeningeal tumor in primary central nervous system lymphoma: Recognition, significance, and implications. Ann Neurol. 1995;38(2):202–209. [DOI] [PubMed] [Google Scholar]
- 41.Fine HA, Mayer RJ. Primary central nervous system lymphoma. Ann Intern Med. 1993; 119(11):1093–1104. [DOI] [PubMed] [Google Scholar]
- 42.Hegde U, Filie A, Little RF, et al. High incidence of occult leptomeningeal disease detected by flow cytometry in newly diagnosed aggressive B-cell lymphomas at risk for central nervous system involvement: The role of flow cytometry versus cytology. Blood. 2005;105(2):496–502. [DOI] [PubMed] [Google Scholar]
- 43.Glantz MJ, Cole BF, Glantz LK, et al. Cerebrospinal fluid cytology in patients with cancer: minimizing false-negative results. Cancer. 1998;82(4):733–739. [DOI] [PubMed] [Google Scholar]
- 44.Glass JP, Melamed M, Chernik NL, Posner JB. Malignant cells in cerebrospinal fluid (CSF): the meaning of a positive CSF cytology. Neurology. 1979;29(10):1369–1375. [DOI] [PubMed] [Google Scholar]
- 45.Quijano S, Lopez A, Sancho JM, et al. Identification of leptomeningeal disease in aggressive B-Cell non-Hodgkin’s lymphoma: Improved sensitivity of flow cytometry. J Clin Oncol. 2009; 27(9):1462–1469. [DOI] [PubMed] [Google Scholar]
- 46.Sancho JM, Orfao A, Quijano S, et al. Clinical significance of occult cerebrospinal fluid involvement assessed by flow cytometry in non-Hodgkin’s lymphoma patients at high risk of central nervous system disease in the rituximab era. Eur J Haematol. 2010;85(4):321–328. [DOI] [PubMed] [Google Scholar]
- 47.Finn WG, Peterson LC, James C, Goolsby CL. Enhanced detection of malignant lymphoma in cerebrospinal fluid by multiparameter flow cytometry. Am J Clin Pathol. 1998;110(3):341–346. [DOI] [PubMed] [Google Scholar]
- 48.French CA, Dorfman DM, Shaheen G, Cibas ES. Diagnosing lymphoproliferative disorders involving the cerebrospinal fluid: Increased sensitivity using flow cytometric analysis. Diagn Cytopathol. 2000; 23(6):369–374. [DOI] [PubMed] [Google Scholar]
- 49.Roma AA, Garcia A, Avagnina A, Rescia C, Elsner B. Lymphoid and myeloid neoplasms involving cerebrospinal fluid: Comparison of morphologic examination and immunophenotyping by flow cytometry. Diagn Cytopathol. 2002;27(5):271–275. [DOI] [PubMed] [Google Scholar]
- 50.Subirá D, Górgolas M, Castañón S, et al. Advantages of flow cytometry immunophenotyping for the diagnosis of central nervous system non-Hodgkin’s lymphoma in AIDS patients. HIV Med. 2005;6(1):21–26. [DOI] [PubMed] [Google Scholar]
- 51.Benevolo G, Stacchini A, Spina M, et al. Final results of a multicenter trial addressing role of CSF flow cytometric analysis in NHL patients at high risk for CNS dissemination. Blood. 2012;120(16):3222–3228. [DOI] [PubMed] [Google Scholar]
- 52.de Jongste AH, Kraan J, Van Den Broek PD, et al. Use of TransFixTM cerebrospinal fluid storage tubes prevents cellular loss and enhances flow cytometric detection of malignant hematological cells after 18 hours of storage. Cytom Part B - Clin Cytom. 2014;86(4):272–279. [DOI] [PubMed] [Google Scholar]
- 53.van Dongen JJM, Lhermitte L, Böttcher S, et al. EuroFlow antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive and malignant leukocytes. Leukemia. 2012; 26(9):1908–1975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Blakeley J, Laterra J. Neoplastic and Paraneoplastic Disorders. In: Irani DN, editor. Cerebrospinal Fluid in Clinical Practice. Philadelphia: Saunders; 2009. p. 233–247. [Google Scholar]
- 55.Chamberlain MC, Glantz M, Groves MD, Wilson WH. Diagnostic Tools for Neoplastic Meningitis: Detecting Disease, Identifying Patient Risk, and Determining Benefit of Treatment. Semin Oncol. 2009; 36(4 Suppl 2):S35–S45. [DOI] [PubMed] [Google Scholar]
- 56.Gleissner B, Siehl J, Korfel A, Reinhardt R, Thiel E. CSF evaluation in primary CNS lymphoma patients by PCR of the CDR III IgH genes. Neurology. 2002;58(3):390–396. [DOI] [PubMed] [Google Scholar]
- 57.Muniz C, Martin-Martin L, Lopez A, et al. Contribution of cerebrospinal fluid sCD19 levels to the detection of CNS lymphoma and its impact on disease outcome. Blood. 2014;123(12):1864–1869. [DOI] [PubMed] [Google Scholar]
- 58.Kiewe P, Fischer L, Martus P, Thiel E, Korfel A. Meningeal dissemination in primary CNS lymphoma: Diagnosis, treatment, and survival in a large monocenter cohort. Neuro Oncol. 2010;12(4):409–417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Roy S, Josephson SA, Fridlyand J, et al. Protein biomarker identification in the CSF of patients with CNS lymphoma. J Clin Oncol. 2008;26(1):96–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Baraniskin A, Kuhnhenn J, Schlegel U, et al. Identification of microRNAs in the cerebrospinal fluid as marker for primary diffuse large B-cell lymphoma of the central nervous system. Blood. 2011;117(11):3140–3146. [DOI] [PubMed] [Google Scholar]
- 61.Kersten MJ, Evers LM, Dellemijn PL, et al. Elevation of cerebrospinal fluid soluble CD27 levels in patients with meningeal localization of lymphoid malignancies. Blood. 1996;87(5):1985–1989. [PubMed] [Google Scholar]
- 62.Fischer L, Korfel A, Pfeiffer S, et al. CXCL13 and CXCL12 in central nervous system lymphoma patients. Clin Cancer Res. 2009; 15(19):5968–5973. [DOI] [PubMed] [Google Scholar]
- 63.Viaccoz A, Ducray F, Tholance Y, et al. CSF neopterin level as a diagnostic marker in primary central nervous system lymphoma. Neuro Oncol. 2015; 17(11):1497–1503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Chihara D, Oki Y, Matsuo K, et al. Incidence and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: analyses with competing risk regression model. Leuk Lymphoma. 2011;52(12):2270–2275. [DOI] [PubMed] [Google Scholar]
- 65.Siegal T, Goldschmidt N. CNS prophylaxis in diffuse large B-cell lymphoma: If, when, how and for whom? Blood Rev. 2012; 26(3):97–106. [DOI] [PubMed] [Google Scholar]
- 66.Sancho JM, Morgades M, Alonso N, et al. Prospective study on the practice of central nervous system prophylaxis and treatment in non-Hodgkin’s lymphoma in Spain. Med Clin (Barc). 2008;131(12):441–446. [DOI] [PubMed] [Google Scholar]
- 67.Cheung CW, Burton C, Smith P, Linch DC, Hoskin PJ, Ardeshna KM. Central nervous system chemoprophylaxis in non-Hodgkin lymphoma: Current practice in the UK. Br J Haematol. 2005;131(2):193–200. [DOI] [PubMed] [Google Scholar]
- 68.Ghose A, Kundu R, Latif T. Prophylactic CNS directed therapy in systemic diffuse large B cell lymphoma. Crit Rev Oncol Hematol. 2014;91(3):292–303. [DOI] [PubMed] [Google Scholar]
- 69.Fleischhack G, Jaehde U, Bode U. Pharmacokinetics following intraventricular administration of chemotherapy in patients with neoplastic meningitis. Clin Pharmacokinet. 2005;44(1):1–31. [DOI] [PubMed] [Google Scholar]
- 70.Arkenau H-T, Chong G, Cunningham D, et al. The role of intrathecal chemotherapy prophylaxis in patients with diffuse large B-cell lymphoma. Ann Oncol. 2007;18(3): 541–545. [DOI] [PubMed] [Google Scholar]
- 71.Tilly H, Lepage E, Coiffier B, et al. Intensive conventional chemotherapy (ACVBP regimen) compared with standard CHOP for poor-prognosis aggressive non-Hodgkin lymphoma. Blood. 2003;102(13): 4284–4289. [DOI] [PubMed] [Google Scholar]
- 72.Vitolo U, Chiappella A, Ferreri AJM, et al. First-line treatment for primary testicular diffuse large B-cell lymphoma with rituximab-CHOP, CNS prophylaxis, and contralateral testis irradiation: Final results of an international phase II trial. J Clin Oncol. 2011;29(20):2766–2772. [DOI] [PubMed] [Google Scholar]
- 73.Tomita N, Kodama F, Kanamori H, Motomura S, Ishigatsubo Y. Prophylactic intrathecal methotrexate and hydrocortisone reduces central nervous system recurrence and improves survival in aggressive non-Hodgkin lymphoma. Cancer. 2002; 95(3):576–580. [DOI] [PubMed] [Google Scholar]
- 74.Wilson WH, Dunleavy K, Pittaluga S, et al. Phase II study of dose-adjusted EPOCH and rituximab in untreated diffuse large B-cell lymphoma with analysis of germinal center and post-germinal center biomarkers. J Clin Oncol. 2008;26(16):2717–2724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Récher C, Coiffier B, Haioun C, et al. Intensified chemotherapy with ACVBP plus rituximab versus standard CHOP plus rituximab for the treatment of diffuse large B-cell lymphoma (LNH03-2B): An open-label randomised phase 3 trial. Lancet. 2011;378(9806):1858–1867. [DOI] [PubMed] [Google Scholar]
- 76.Glantz MJ, LaFollette S, Jaeckle KA, et al. Randomized trial of a slow-release versus a standard formulation of cytarabine for the intrathecal treatment of lymphomatous meningitis. J Clin Oncol. 1999;17(10): 3110–3116. [DOI] [PubMed] [Google Scholar]
- 77.Corazzelli G, Frigeri F, Russo F, et al. RD-CODOX-M/IVAC with rituximab and intrathecal liposomal cytarabine in adult Burkitt lymphoma and “unclassifiable” highly aggressive B-cell lymphoma. Br J Haematol. 2012;156(2):234–244. [DOI] [PubMed] [Google Scholar]
- 78.de la Fuente A, Salar A, Panizo C, et al. Efficacy and Safety of Liposomal Cytarabine as Intrathecal Prophylaxis in Patients with Diffuse Large B Cell Lymphoma at High Risk of CNS Involvement: A Multicentric Study Including 80 Patients in Spain. Blood. 2009; 114(22):1663. [Google Scholar]
- 79.González-Barca E, Canales M, Salar A, et al. Central nervous system prophylaxis with intrathecal liposomal cytarabine in a subset of high-risk patients with diffuse large B-cell lymphoma receiving first line systemic therapy in a prospective trial. Ann Hematol. 2016;95(6):893–899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Schulz H, Pels H, Schmidt-Wolf I, Zeelen U, Germing U, Engert A. Intraventricular treatment of relapsed central nervous system lymphoma with the anti-CD20 antibody rituximab. Haematologica. 2004; 89(6):753–754. [PubMed] [Google Scholar]
- 81.Rubenstein JL, Li J, Chen L, et al. Multicenter phase 1 trial of intraventricular immunochemotherapy in recurrent CNS lymphoma. Blood. 2013;121(5):745–751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Vassal G, Valteau D, Bonnay M, Patte C, Aubier F, Lemerle J. Cerebrospinal fluid and plasma methotrexate levels following high-dose regimen given as a 3-hour intravenous infusion in children with nonHodgkin’s lymphoma. Pediatr Hematol Oncol. 1990; 7(1):71–77. [DOI] [PubMed] [Google Scholar]
- 83.Abramson JS, Hellmann M, Barnes JA, et al. Intravenous methotrexate as central nervous system (CNS) prophylaxis is associated with a low risk of CNS recurrence in high-risk patients with diffuse large B-cell lymphoma. Cancer. 2010;116(18):4283–4290. [DOI] [PubMed] [Google Scholar]
- 84.Holte H, Leppä S, Björkholm M, et al. Dose-densified chemoimmunotherapy followed by systemic central nervous system prophylaxis for younger high-risk diffuse large B-cell/follicular grade 3 lymphoma patients: Results of a phase II Nordic lymphoma group study. Ann Oncol. 2013; 24(5):1385–1392. [DOI] [PubMed] [Google Scholar]
- 85.Adde M, Enblad GG, Hagberg H, Sundstrom C, Laurell A, Sundström C. Outcome for young high-risk aggressive B-cell lymphoma patients treated with CHOEP-14 and rituximab (R-CHOEP-14). Med Oncol. 2006;23(2):283–293. [DOI] [PubMed] [Google Scholar]
- 86.Bernard S, Goldwirt L, Amorim S, et al. Activity of ibrutinib in mantle cell lymphoma patients with central nervous system relapse. Blood. 2015; 126(14):1695–1698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Houillier C, Choquet S, Touitou V, et al. Lenalidomide monotherapy as salvage treatment for recurrent primary CNS lymphoma. Neurology. 2015;84(3):325–326. [DOI] [PubMed] [Google Scholar]
- 88.Avilés A, Jesús Nambo M, Neri N. Central nervous system prophylaxis in patients with aggressive diffuse large B cell lymphoma: an analysis of 3,258 patients in a single center. Med Oncol. 2013;30(2):520. [DOI] [PubMed] [Google Scholar]
- 89.Cheah CY, Herbert KE, O’Rourke K, et al. A multicentre retrospective comparison of central nervous system prophylaxis strategies among patients with high-risk diffuse large B-cell lymphoma. Br J Cancer. 2014; 111(6):1072–1079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Graber JJ, Omuro A. Primary central nervous system lymphoma: is there still a role for radiotherapy? Curr Opin Neurol. 2011;24(6):633–640. [DOI] [PubMed] [Google Scholar]
- 91.Rubenstein JL, Gupta NK, Mannis GN, LaMarre AK, Treseler P. How I treat CNS lymphomas. Blood. 2013;122(14): 2318–2330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Fischer L, Korfel A, Kiewe P, Neumann M, Jahnke K, Thiel E. Systemic high-dose methotrexate plus ifosfamide is highly effective for central nervous system (CNS) involvement of lymphoma. Ann Hematol. 2009;88(2):133–139. [DOI] [PubMed] [Google Scholar]
- 93.Ferreri AJ, Reni M, Foppoli M, et al. High-dose cytarabine plus high-dose methotrexate versus high-dose methotrexate alone in patients with primary CNS lymphoma: a randomised phase 2 trial. Lancet. 2009; 374(9700):1512–1520. [DOI] [PubMed] [Google Scholar]
- 94.Bokstein F, Lossos A, Lossos IS, Siegal T. Central nervous system relapse of systemic non-Hodgkin’s lymphoma: results of treatment based on high-dose methotrexate combination chemotherapy. Leuk Lymphoma. 2002;43(3):587–593. [DOI] [PubMed] [Google Scholar]
- 95.Wong ET, Tishler R, Barron L, Wu JK. Immunochemotherapy with rituximab and temozolomide for central nervous system lymphomas. Cancer. 2004;101(1):139–145. [DOI] [PubMed] [Google Scholar]
- 96.Bierman P, Giglio P. Diagnosis and treatment of central nervous system involvement in non-Hodgkin’s lymphoma. Hematol Oncol Clin North Am. 2005; 19(4):597–609. [DOI] [PubMed] [Google Scholar]
- 97.Korfel A, Elter T, Thiel E, et al. Phase II study of central nervous system (CNS)-directed chemotherapy including high-dose chemotherapy with autologous stem cell transplantation for CNS relapse of aggressive lymphomas. Haematologica. 2013; 98(3):364–370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Ferreri AJM, Donadoni G, Cabras MG, et al. High doses of antimetabolites followed by high-dose sequential chemoimmunotherapy and autologous stem-cell transplantation in patients with systemic B-cell lymphoma and secondary CNS involvement: Final results of a multicenter phase II trial. J Clin Oncol. 2015; 33(33):3903–3910. [DOI] [PubMed] [Google Scholar]
- 99.Bromberg JE, Doorduijn JK, Illerhaus G, et al. Central nervous system recurrence of systemic lymphoma in the era of stem cell transplantation - An international primary central nervous system lymphoma study group project. Haematologica. 2013; 98(5):808–813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Rubenstein JL, Hsi ED, Johnson JL, et al. Intensive chemotherapy and immunotherapy in patients with newly diagnosed primary CNS lymphoma: CALGB 50202 (Alliance 50202). J Clin Oncol. 2013; 31(25):3061–3068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Tarella C, Zanni M, Magni M, et al. Rituximab improves the efficacy of high-dose chemotherapy with autograft for high-risk follicular and diffuse large B-cell lymphoma: A multicenter Gruppo Italiano Terapie Innnovative nei Linfomi survey. J Clin Oncol. 2008;26(19):3166–3175. [DOI] [PubMed] [Google Scholar]
- 102.Schmitz N, Wu HS. Advances in the Treatment of Secondary CNS Lymphoma. J Clin Oncol. 2015;33(33):3851–3853. [DOI] [PubMed] [Google Scholar]
- 103.Kim S, Khatibi S, Howell SB, McCully C, Balis FM, Poplack DG. Prolongation of drug exposure in cerebrospinal fluid by encapsulation into DepoFoam. Cancer Res. 1993; 53(7):1596–1598. [PubMed] [Google Scholar]
- 104.Howell SB. Liposomal cytarabine for the treatment of lymphomatous meningitis. Biol Ther Lymphoma. 2003;6:10–14. [Google Scholar]
- 105.Garcia-Marco JA, Panizo C, Garcia ES, et al. Efficacy and safety of Liposomal cytarabine in lymphoma Patients with central nervous system involvement from lymphoma. Cancer. 2009;115(9):1892–1898. [DOI] [PubMed] [Google Scholar]
- 106.Gökbuget N, Hartog CM, Bassan R, et al. Liposomal cytarabine is effective and tolerable in the treatment of central nervous system relapse of acute lymphoblastic leukemia and very aggressive lymphoma. Haematologica. 2011;96(2):238–244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.DepoCyte: Summary of product characteristics [Internet]. European Medicines Agency. [cited 2016 Apr 1]. Available from: www.ema.europe.eu/ema/
- 108.Sanchez-Gonzalez B, Llorente A, Sancho JM, et al. A new modified prophylactic scheme against liposomal cytarabine-induced arachnoiditis in adult patients with lymphoma. Leuk Lymphoma. 2013; 54(4):892–893. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.