

Abstract
Background
Type 2 diabetes is a prevalent, chronic disease for which diet is an integral aspect of treatment. In our previous trial, we found that recommendations to follow a very low-carbohydrate ketogenic diet and to change lifestyle factors (physical activity, sleep, positive affect, mindfulness) helped overweight people with type 2 diabetes or prediabetes improve glycemic control and lose weight. This was an in-person intervention, which could be a barrier for people without the time, flexibility, transportation, social support, and/or financial resources to attend.
Objective
The aim was to determine whether an online intervention based on our previous recommendations (an ad libitum very low-carbohydrate ketogenic diet with lifestyle factors; “intervention”) or an online diet program based on the American Diabetes Associations’ “Create Your Plate” diet (“control”) would improve glycemic control and other health outcomes among overweight individuals with type 2 diabetes.
Methods
In this pilot feasibility study, we randomized overweight adults (body mass index ≥25) with type 2 diabetes (glycated hemoglobin [HbA1c] 6.5%-9.0%) to a 32-week online intervention based on our previous recommendations (n=12) or an online diet program based around a plate method diet (n=13) to assess the impact of each intervention on glycemic control and other health outcomes. Primary and secondary outcomes were analyzed by mixed-effects linear regression to compare outcomes by group.
Results
At 32 weeks, participants in the intervention group reduced their HbA1c levels more (estimated marginal mean [EMM] –0.8%, 95% CI –1.1% to –0.6%) than participants in the control group (EMM –0.3%, 95% CI –0.6% to 0.0%; P=.002). More than half of the participants in the intervention group (6/11, 55%) lowered their HbA1c to less than 6.5% versus 0% (0/8) in the control group (P=.02). Participants in the intervention group lost more weight (EMM –12.7 kg, 95% CI –16.1 to –9.2 kg) than participants in the control group (EMM –3.0 kg, 95% CI –7.3 to 1.3 kg; P<.001). A greater percentage of participants lost at least 5% of their body weight in the intervention (10/11, 90%) versus the control group (2/8, 29%; P=.01). Participants in the intervention group lowered their triglyceride levels (EMM –60.1 mg/dL, 95% CI –91.3 to –28.9 mg/dL) more than participants in the control group (EMM –6.2 mg/dL, 95% CI –46.0 to 33.6 mg/dL; P=.01). Dropout was 8% (1/12) and 46% (6/13) for the intervention and control groups, respectively (P=.07).
Conclusions
Individuals with type 2 diabetes improved their glycemic control and lost more weight after being randomized to a very low-carbohydrate ketogenic diet and lifestyle online program rather than a conventional, low-fat diabetes diet online program. Thus, the online delivery of these very low-carbohydrate ketogenic diet and lifestyle recommendations may allow them to have a wider reach in the successful self-management of type 2 diabetes.
Trial Registration
ClinicalTrials.gov NCT01967992; https://clinicaltrials.gov/ct2/show/NCT01967992 (Archived by WebCite at http://www.webcitation.org/6o0fI9Mkq)
Keywords: eHealth, diet, weight loss, type 2 diabetes mellitus
Introduction
Type 2 diabetes mellitus is a rapidly growing chronic disease that affects approximately 22 million people in the United States, for which diet is an integral aspect of treatment [1,2]. Data suggest that very low-carbohydrate diets [3-11], and adequate sleep and physical exercise [12-16] can improve glycemic control and reduce body weight in individuals with type 2 diabetes. Moreover, behavioral adherence strategies, including positive affect regulation and mindful eating strategies, may reduce overall stress, stress-based eating, and depressive symptoms, which can be barriers for following behavioral recommendations [17-19].
In prior research, we found that recommendations to follow a very low-carbohydrate diet and to make lifestyle changes (sleep and exercise recommendations and a package of behavioral adherence strategies based on positive affect regulation and mindfulness) were able to improve glycemic control and reduce body weight in overweight individuals with type 2 diabetes or prediabetes [20]. Although promising, this previous trial was delivered in-person, which is a significant barrier to engagement for people without the time, flexibility, transportation, social support, and/or financial resources to attend. To create a highly disseminable, evidence-based program, we adapted our in-person intervention for online delivery.
In this pilot feasibility and acceptability study, we assessed whether overweight individuals with type 2 diabetes, randomized to receive an online intervention based on our previous trial (recommendations to follow an ad libitum very low-carbohydrate ketogenic diet and other lifestyle changes), would have greater improvements in glycemic control and other health outcomes than participants randomized to a control group, an online diet program based on a plate method diet (the American Diabetes Associations’ “Create Your Plate” diet). To our knowledge, this is the first online randomized controlled trial to teach a very low-carbohydrate ketogenic diet to individuals with type 2 diabetes.
Methods
Participants and Procedure
We conducted a parallel-group, balanced randomization (1:1) trial, approved by the University of California, San Francisco, Institutional Review Board and registered with ClinicalTrials.gov (NCT01967992). The primary outcome measure was glycemic control, operationalized as change in glycated hemoglobin (HbA1c). A key secondary outcome was body weight. Exploratory outcomes were cholesterol, triglycerides, diabetes-related distress, subjective experiences of the diet, and physical side effects.
We recruited participants nationally with online ads (on Craigslist, Backpage, and Facebook), newspaper ads and articles, and radio ads. This allowed us to recruit participants from across the United States. Eligibility criteria included age 18 years or older with a body mass index of ≥25, an elevated HbA1c level diagnostic of type 2 diabetes (6.5%-9%, measured by us at baseline), and regular access to the Internet. To reduce the risk of hypoglycemia, we excluded participants who were taking any diabetes medication other than metformin.
Recruitment materials directed interested participants to a study website to complete an online eligibility questionnaire. Study staff then called potentially eligible participants to assess initial eligibility and describe study procedures. For example, we assessed whether participants were taking any medications for their type 2 diabetes other than metformin. If participants then consented to the full study, they were asked to complete several assessments, all specified in the measures section.
We recruited participants who were ready to make the changes required of the intervention in order to mitigate a potentially high dropout rate. We measured readiness to undertake the intervention [21] with the following item: “If you are eligible for this study you will be asked to...cut out the kinds of cookies, cakes, pasta, pastries, bagels, rice, potatoes, and sugary fruits that some people often eat. Given the description of the dietary changes above, how prepared do you feel to make these changes?” Participants could answer the item from 1 (not at all) to 7 (very much so). Participants were eligible if they rated themselves to be prepared to begin above the midpoint of the scale (5-7). In addition, conscientious people, we reasoned, would be more likely to follow the behavior changes requested by the intervention because conscientiousness has been shown to be positively related to following beneficial health-related behaviors [22]. Participants were eligible if they rated themselves as conscientious on two items [23]: “I see myself as someone who is dependable, self-disciplined” (eligible answers were agree and strongly agree) and “I see myself as someone who is disorganized, careless” (eligible answers were disagree and strongly disagree). We used items from the Yale Food Addiction Scale [24] and the Eating Disorder Diagnostic Scale [25] to screen out participants who had the tendency to be addicted to food or binge eat.
For this study, it was not possible for the participants and staff to be masked to group allocation. Therefore, once all baseline measurements had been completed, study staff randomized participants to one of the two intervention groups by opening the next opaque envelope in a series containing the concealed sequence for randomization, which was created by a statistician using block randomization procedures, with blocks of size randomly allocated to size 2, 4, or 6.
Outcomes were measured at baseline as well as 16 and 32 weeks after baseline. We paid participants US $25 for each assessment at 16 and 32 weeks. Thus, participants could receive up to US $50 over the course of the study.
Intervention
Intervention Group: Very Low-Carbohydrate Ketogenic Diet and Lifestyle Recommendations
We randomized half of participants to receive recommendations on how to eat an ad libitum very low-carbohydrate ketogenic diet, to reduce carbohydrate intake to between 20-50 grams of nonfiber carbohydrates a day with the goal of restricting carbohydrate intake to a level at which a low amount of ketone production is induced, called nutritional ketosis. In this state, the body uses fatty acids instead of carbohydrates as its primary energy source, which do not elevate glucose levels as strongly as carbohydrates [26,27]. To support dietary adherence, we mailed participants in this group urinary acetoacetate (a ketone that can be measured in urine) test kits (KetoStix, Abbott). We asked them to measure their urine for the presence of ketones at least once a week for the first few months of the program.
We also suggested that participants in the intervention group follow lifestyle recommendations, including behavioral adherence strategies aimed at increasing positive affect regulation [18] and mindful eating based largely on the Mindfulness-Based Eating Awareness Training program [19,28], using handouts and lesson content adapted from our in-person intervention. Specific topics included setting attainable goals; scheduling, noticing, and savoring positive events; developing self-compassion; practicing positive reappraisal, gratitude, and acts of kindness; being aware of one’s personal strengths; and being mindful of hunger, fullness, cravings, taste satisfaction, and triggers for overeating. Moreover, starting in week 6, the lessons discussed the importance of physical activity and sleep as well as encouraged participants to increase their level of physical activity and amount of sleep. We chose to include a comprehensive program of behavioral support in this intervention group in order to enhance the likelihood of finding an impact of our previously successful in-person program using an online format.
We emailed participants in this group new lessons weekly for the first 16 weeks and then every two weeks for the remaining 16 weeks of the study. The lessons in the first 16 weeks included short videos created for the study about all of the study components (about 5-15 minutes long, with audio narration over videos with white text, images, and a black background), with printable handouts and links to online resources, such as recipes and recipe books. The lessons in the last 16 weeks did not include study-specific videos, only printable handouts and links to online resources.
Control Group: American Diabetes Associations’ “Create Your Plate” Diet
This dietary intervention, our control group, was slightly different from the one we had originally used in our in-person intervention because we received feedback that the previous “carbohydrate counting” intervention was difficult for participants to follow. Instead, we randomized half of participants to a diet program based around a plate method diet, the American Diabetes Associations’ “Create Your Plate” diet, a low-fat diet that emphasizes green vegetables, lean protein sources, and somewhat limited starchy and sweet foods. All proportions are based on a 9-inch plate: half the plate is filled with nonstarchy vegetables, one-quarter with carbohydrates, and one-quarter with lean proteins [29]. We taught this group using short videos created for the study (approximately 5-10 minutes long), with printable handouts and links to online resources, such as links to online recipes and recipe books. We chose to include just the standard dietary information in this group, and not all the extra behavioral help, in order to have this condition be a minimal dietary control group. We emailed participants in this group new lessons weekly for the first 4 weeks and then every 4 weeks thereafter. This group did not get the positive affect regulation and mindful eating materials.
All participants in both groups could contact the first author by phone or email as needed with questions. A coauthor (SK) was on-call by pager for any urgent medical concerns. All regularly planned emails were sent automatically by custom software, which allowed us to ensure that the emails arrived to participants in a timely manner and removed the need for study staff to oversee this process.
Measures
All measures were assessed at baseline before randomization and at 16 and 32 weeks after the intervention began.
Metabolic Measures
We assessed HbA1c as well as fasted low- and high-density lipoprotein cholesterol (LDL and HDL) and triglycerides at a commercial Clinical Laboratory Improvement Amendments-certified laboratory (LabCorp; Laboratory Corporation of America Holdings, Burlington, NC, USA).
Body Weight
Participants recruited at the start of the study had their body weight measured at a US HealthWorks Medical Group (Valencia, CA, USA) location, near wherever they lived. Due to measurement concerns (eg, participants were asked their weight instead of actually being weighed), we then mailed the participants the EatSmart Digital Bathroom Scale. At each critical time point, participants emailed study staff a photo of their feet and digitally displayed weight while they stood on the digital scale.
Psychological Self-Report
Participants completed the Diabetes Distress Scale [30], a measure of upset related to having diabetes. We assessed the subjective experience of each diet by asking, “How much do you like how you feel on your diet?” and “How much do you think your diet has improved your physical health?” all rated from 1 (not at all) to 7 (very much so). We further asked, “How often do you cheat on your diet?” rated from 1 (not at all) to 7 (very often) and “How hard is it to stay on your diet?” rated from 1 (not at all) to 7 (very difficult).
We measured depressive symptoms with a 20-item scale, the Center for Epidemiologic Studies Depression Scale (CESD) [31], with higher scores reflecting greater symptoms over the past week. Following past research, we also separately examined four items that tap into positive affect, including “I felt hopeful about the future” and “I was happy.” Higher scores reflect greater positive affect.
Participants completed the Modified Differential Emotions Scale (mDES) [32], which gauges negative and positive mood. This version of the mDES asked participants to recall the past week and rate how often they had experienced particular emotions, rated from 1 (not at all) to 9 (all the time). The positive emotions subscale consists of amusement, awe, compassion, contentment, gratitude, hope, interest, happy, love, and pride. The negative emotions subscale consists of anger, contempt, disgust, embarrassment, anxiety, guilt, sadness, boredom, and loneliness.
Physical Self-Report
We assessed physical symptoms with an adaptation of the Health Symptom Checklist, a short, face-valid measure of physical symptoms [33], rated from 1 (not at all) to 4 (very often) for how often over the past week they had experienced a variety of physical symptoms. We used a subscale of the Short Form Health Survey [34], a well-validated and extensively used measure of health-related quality of life, to assess vitality (energy and fatigue).
Dietary Self-Report
We assessed dietary composition using the free online application MyFitnessPal [35], which has a vast database of foods and has been or is being used in other clinical trials [36-38]. Even so, its database is partially user-generated and results may be prone to error. Therefore, the dietary self-report results should not be considered validated. At each of the main time points, participants reported on what they had eaten over two weekdays and one weekend day, which we then averaged into one composite measure.
Statistical Analyses
The primary statistical analyses were performed using Stata IC software version 14.1 (StataCorp LP, College Station, TX, USA) setting two-tailed alpha to reject the null hypothesis at .05. Our experimental design randomized participants to one of two groups (intervention: n=12; control: n=13) participating in a 32-week online dietary and lifestyle intervention designed for weight and HbA1c reductions with primary outcomes (HbA1c and body weight) measured at three time points (baseline, week 16, week 32). All our main outcomes were continuously scaled and were appropriately analyzed with parametric statistical techniques, and all statistical assumptions were tested prior to interpreting results. The data met the distributional requirements for the techniques employed without requiring data transformations, model adjustments (eg, random slope terms, heteroscedasticity adjustments), or nonlinear modeling.
Participants’ repeated measures outcomes were submitted to separate mixed-effects linear regression analyses with fixed effect terms comparing baseline (preintervention) to each of the two subsequent observations made postintervention (weeks 16 and 32), the main effect for group, and most importantly, the simple interaction effects comparing the relative change by group at each postintervention assessment, relative to baseline. Random y-intercept terms were included to accommodate for the repeated measures experimental design. Our analysis of total caloric intake, net carbohydrates, fat, and sugar required log transformations prior to analysis to normalize model residuals; out of a total possible 63 observations, we eliminated one triglyceride, two LDL, and one calorie observations that were overly influential outliers.
For all the self-reported ratings of the subjective experience of the diet, we assessed differences between the groups using Cohen d. For all results involving ratios, we used a two-tailed Fisher exact test to assess significance. Means and confidence intervals are reported in their original units for all variables.
Results
We enrolled and randomized 25 participants to the intervention (n=12) or control (n=13) group (Figure 1). A large number of individuals who took our initial online survey were ineligible because they did not have type 2 diabetes (n=249), were taking diabetes medications other than metformin (n=404), or had definite plans to begin taking insulin (n=35). Randomized participants included men and women, of several different types of ethnic and racial backgrounds (although about half were white), with an average duration of diagnosed type 2 diabetes of approximately 5 years, and a mean baseline HbA1c of approximately 7% (Table 1).
Figure 1.
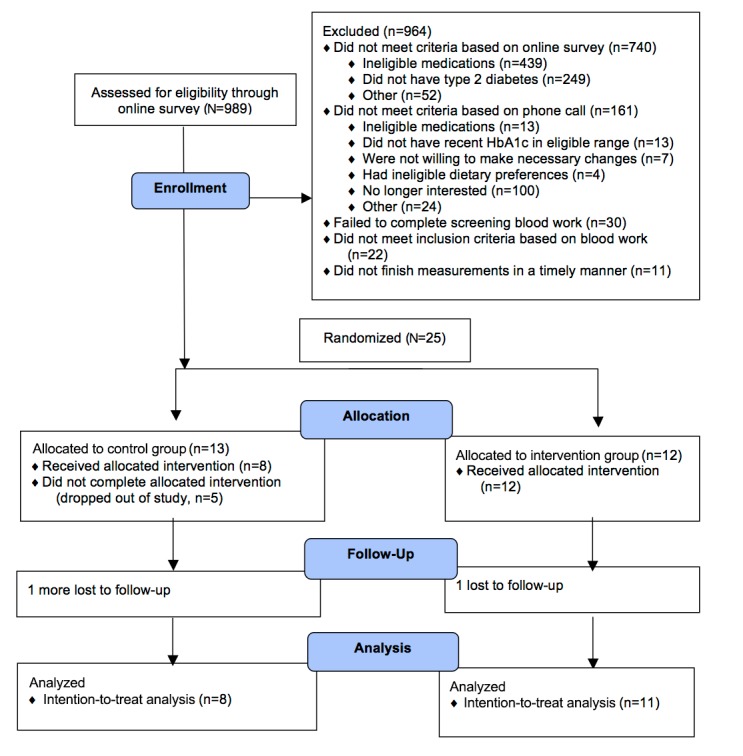
Study participant flowchart for online study.
Table 1.
Baseline participant characteristics (N=25).
| Baseline characteristics | Intervention group (n=12) | Control group (n=13) | |
| Sex, n (%) | |||
| Male | 6 (50) | 4 (31) | |
| Female | 6 (50) | 9 (69) | |
| Age (years), mean (SD) | 53.0 (10.2) | 58.2 (6.7) | |
| Race/Ethnicity, n (%) | |||
| Asian/Pacific Islander | 2 (17) | 2 (15) | |
| Black | 3 (25) | 0 (0) | |
| White | 7 (58) | 8 (62) | |
| Latino/a | 2 (17) | 5 (38) | |
| Duration of diabetes (years), mean (SD) | 5.3 (4.1) | 5.7 (3.7) | |
| HbA1c (%), mean (SD) | 7.1 (0.4) | 7.2 (0.3) | |
| Weight (kg), mean (SD) | 109.7 (24.9) | 90.9 (16.4) | |
| Triglycerides (mg/dL), mean (SD) | 174.1 (79.4) | 151.5 (87.1) | |
| HDL cholesterol (mg/dL), mean (SD) | 45.7 (15.0) | 53.9 (12.7) | |
| LDL cholesterol (mg/dL), mean (SD) | 96.9 (30.4) | 90.5 (29.0) | |
| Diabetes-related distress, mean (SD) | 1.9 (0.8) | 2.4 (1.2) | |
| CES-Depression, mean (SD) | 10.5 (7.7) | 9.8 (7.4) | |
| CES-D Positive Affect, mean (SD) | 10.2 (2.3) | 10.2 (2.2) | |
| DES Negative Affect, mean (SD) | 2.8 (1.3) | 2.7 (1.4) | |
| DES Positive Affect, mean (SD) | 6.5 (1.1) | 6.2 (1.5) | |
| Vitality (SF-36 subscale), mean (SD) | 53.3 (16.4) | 49.2 (20.1) | |
| Total kilocalories, mean (SD) | 1768.5 (626.6) | 1749.1 (322.2) | |
| Total grams of nonfiber carbohydrates, mean (SD) | 163.6 (86.7) | 152.0 (58.9) | |
| Total grams of fat, mean (SD) | 77.1 (41.4) | 81.3 (27.3) | |
| Total grams of protein, mean (SD) | 83.3 (18.0) | 74.5 (17.2) | |
| Total grams of sugar, mean (SD) | 50.6 (33.8) | 44.9 (23.8) | |
Trial retention differed by group. Dropout was higher in the control group: 16-week dropout for the intervention group was zero of 12 (0%) and 5 of 13 (39%) for the control group (P=.04); 32-week dropout for the intervention group was 1 of 12 (8%) and 6 of 13 (46%) for the control group (P=.07). One participant in each group reported experiencing an event that they believed was caused by hypoglycemia (one in the control group was likely from eating very few calories and the other in the intervention group was after taking a dose of metformin).
Metabolic Measures
Glycated Hemoglobin
There were significantly greater reductions in HbA1c for the intervention group relative to the control group at both 16 (P=.01) and 32 (P=.002) weeks. Reductions in HbA1c were approximately twice as large in the intervention versus the control group (intervention group: estimated marginal mean [EMM] –0.9% at 16 weeks and EMM –0.8% at 32 weeks; control group: EMM –0.5% at 16 weeks and EMM –0.4% at 32 weeks; Table 2,Figure 2). At both 16 and 32 weeks, a greater percentage of participants in the intervention group lowered their HbA1c to less than 6.5%, the cutoff for type 2 diabetes, compared to the percentage of participants in the control group (intervention group: 9/12, 75% at 16 weeks and 6/11, 55% at 32 weeks; control group: 1/8, 13% at 16 weeks and 0/8, 0% at 32 weeks; Table 3). We redid these analyses using participants’ baseline body weight as covariates in the model. The results were nearly identical; therefore, we present the simpler unadjusted model.
Table 2.
Estimated marginal mean (EMM) changes from baseline to 16 and 32 weeks.a
| Outcomes | Intervention group, EMM (95% CI)b | Control group, EMM (95% CI)c | Difference between groups, EMM (95% CI) | P | |
| HbA1c (%) | |||||
| 16 weeks | –0.9 (–1.1, –0.6) | –0.5 (–0.8, –0.2) | –0.4 (–0.7, –0.1) | .01 | |
| 32 weeks | –0.8 (–1.1, –0.6) | –0.3 (–0.6, 0.0) | –0.5 (–0.8, –0.2) | .002 | |
| Weight (kg) | |||||
| 16 weeks | –8.5 (–11.9, –5.2) | –3.9 (–8.0, 0.2) | –4.6 (–8.8, –0.4) | .03 | |
| 32 weeks | –12.7 (–16.1, –9.2) | –3.0 (–7.3, 1.3) | –9.6 (–14.0, –5.3) | <.001 | |
| Triglycerides (mg/dL) | |||||
| 16 weeks | –35.5 (–65.7, –5.2) | –17.4 (–55.2, 20.4) | –18.1 (–56.1, 19.9) | .35 | |
| 32 weeks | –60.1 (–91.3, –28.9) | –6.2 (–46.0, 33.6) | –53.9 (–93.6, –14.2) | .01 | |
| HDL cholesterol (mg/dL) | |||||
| 16 weeks | 1.4 (–2.7, 5.6) | –0.3 (–5.3, 4.8) | 1.7 (–3.4, 6.8) | .52 | |
| 32 weeks | 4.8 (0.5, 9.1) | 0.6 (–4.7, 5.9) | 4.1 (–1.2, 9.5) | .13 | |
| LDL cholesterol (mg/dL) | |||||
| 16 weeks | –0.8 (–10.9, 9.4) | 1.5 (–11.7, 14.7) | –2.2 (–15.3, 10.8) | .74 | |
| 32 weeks | –0.3 (–10.8, 10.3) | –6.1 (–19.9, 7.7) | 5.9 (–7.8, 19.5) | .40 | |
| Diabetes-related distress | |||||
| 16 weeks | –0.5 (–0.8, –0.1) | –0.3 (–0.7, 0.1) | –0.1 (–0.6, 0.3) | .49 | |
| 32 weeks | –0.4 (–0.8, 0.0) | –0.4 (–0.8, 0.0) | 0.0 (–0.5, 0.5) | .98 | |
| CES-Depression | |||||
| 16 weeks | –3.7 (–7.8, 0.5) | 0.8 (–3.7, 5.4) | –4.5 (–9.3, 0.4) | .07 | |
| 32 weeks | –0.6 (–5.0, 3.7) | –1.0 (–6.0, 4.0) | –0.4 (–4.8, 5.6) | .88 | |
| CESD Positive Affect | |||||
| 16 weeks | 8.4 (–5.3, 22.2) | –4.4 (–19.1, 10.3) | 12.9 (–2.9, 28.7) | .11 | |
| 32 weeks | 0.5 (–13.6, 14.8) | 7.2 (–9.0, 23.4) | –6.6 (–23.5, 10.3) | .45 | |
| DES Negative Affect | |||||
| 16 weeks | –0.7 (1.5, 0.1) | –0.1 (–0.9, 0.8) | –0.6 (–1.5, 0.3) | .19 | |
| 32 weeks | –0.4 (–1.2, 0.4) | –0.7 (–1.6, 0.2) | 0.3 (0.5, –0.6) | .49 | |
| DES Positive Affect | |||||
| 16 weeks | 0.5 (–0.3, 1.4) | –0.2 (–1.1, 0.7) | 0.7 (–0.3, 1.7) | .15 | |
| 32 weeks | 0.4 (–0.5, 1.2) | 0.3 (–0.7, 1.2) | 0.1 (–0.9, 1.1) | .82 | |
| Vitality (SF-36 subscale) | |||||
| 16 weeks | 13.3 (2.5, 24.02) | 2.3 (–9.4, 13.9) | 11.0 (–1.4, 23.4) | .08 | |
| 32 weeks | 9.2 (–1.9, 20.4) | 11.0 (–1.8, 23.8) | –1.8 (–15.1, 11.6) | .80 | |
| Total kilocalories | |||||
| 16 weeks | –362.9 (–634.7, –91.1) | –300.8 (–594.3, –7.4) | –62.1 (–376.0, 251.7) | .65 | |
| 32 weeks | –439.3 (–719.4, –159.3) | –216.6 (–559.2, 125.9) | –222.7 (–569.9, 124.5) | .13 | |
| Total grams of nonfiber carbohydrates | |||||
| 16 weeks | –123.2 (–167.2, –79.2) | –27.03 (–75.4, 21.3) | –19.2 (–147.4, –44.9) | <.001 | |
| 32 weeks | –122.7 (–167.9, –77.5) | –14.8 (–71.0, 41.5) | –107.9 (–164.6, –51.3) | <.001 | |
| Total grams of fat | |||||
| 16 weeks | –7.8 (–36.3, 20.7) | –18.7 (–48.8, 11.4) | 10.9 (–21.7, 43.4). | .42 | |
| 32 weeks | –4.0 (–33.2, 25.3) | –23.7 (–58.5, 11.1) | 19.8 (–15.9, 55.5) | .13 | |
| Total grams of protein | |||||
| 16 weeks | –0.5 (–14.0, 13.0) | –0.2 (–15.3, 14.9) | –0.3 (–16.2, 15.6) | .97 | |
| 32 weeks | –1.6 (–15.5, 12.3) | –0.1 (–17.7, 17.6) | –1.5 (–19.2, 16.1) | .86 | |
| Total grams of sugar | |||||
| 16 weeks | –37.2 (–53.8, –20.5) | –4.4 (–22.9, 14.1) | –32.7 (–52.3, –13.2) | <.001 | |
| 32 weeks | –32.5 (–49.7, –15.4) | –0.3 (–21.9, 21.3) | –32.2 (–53.9, –10.6) | <.001 | |
a Data are estimated marginal means and 95% confidence intervals by linear mixed-effects model analysis.
b Total analyzed in intervention group: n=12 for week 16 and n=11 for week 32.
c Total analyzed in control group: n=9 for week 16 and n=8 for week 32.
Figure 2.
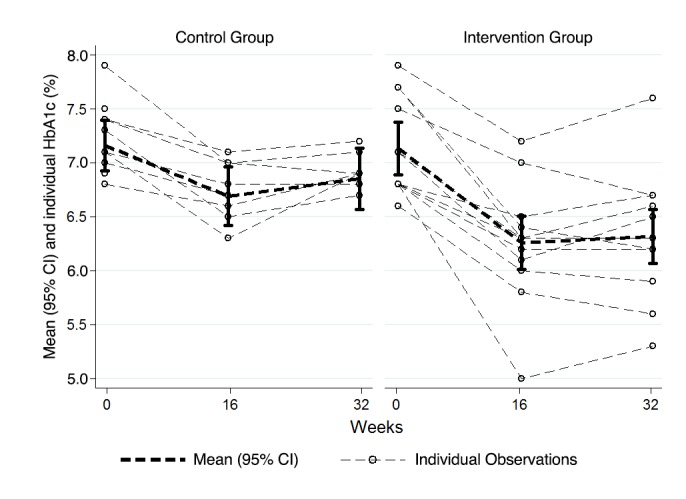
Mean and individual body weight (in kilograms) for the intervention and control groups at baseline and at 16 and 32 weeks. Bars represent 95% confidence intervals of the mean. Dashed lines reflect individual participants; darker lines represent each group mean.
Table 3.
Percentage of people meeting HbA1c and weight change thresholds.
| HbA1c and weight outcomes | Intervention groupa | Control groupb | Difference between groups | P | |
| Participants with final HbA1c<6.5%, n (%) | |||||
| 16 weeks | 9 (75%) | 1 (13%) | .02 | ||
| 32 weeks | 6 (55%) | 0 (0%) | .02 | ||
| Weight (% of initial weight), mean (SD) | |||||
| 16 weeks | –7.8 (3.6) | –4.2 (3.7) | –3.6 (–7.1, –0.1) | .04 | |
| 32 weeks | –12.0 (7.3) | –2.5 (4.6) | –9.5 (–16.1, –2.9) | .01 | |
| Participants achieving a 5% weight loss, n (%) | |||||
| 16 weeks | 10 (83%) | 3 (38%) | .06 | ||
| 32 weeks | 10 (90%) | 2 (29%) | .01 | ||
a Total in intervention group: n=12 at 16 weeks and n=11 at 32 weeks.
b Total in control group: n=8 at 16 weeks and n=8 at 32 weeks for participants with HbA1c <6.5%, and n=7 at 32 weeks for participants achieving a 5% weight loss.
Body Weight
We also found significantly greater reductions in body weight for participants in the intervention group relative to the control group at weeks 16 (P=.03) and 32 (P<.001). For example, at 32 weeks, participants in the intervention group lost more weight (EMM –12.7 kg, 95% CI –16.1 to –9.2 kg) than participants in the control group (EMM –3.0 kg, 95% CI –7.3 to 1.3 kg; P<.001) (Table 2,Figure 3). At both 16 and 32 weeks, more than double the percentage of participants in the intervention group lost at least 5% of their body weight compared participants in the control group (intervention group: 10/12, 83.3% at 16 weeks and 10/11, 90.1% at 32 weeks; control group: 3/8, 37.5% at 16 weeks and 2/8, 28.6% at 32 weeks; Table 3).
Figure 3.
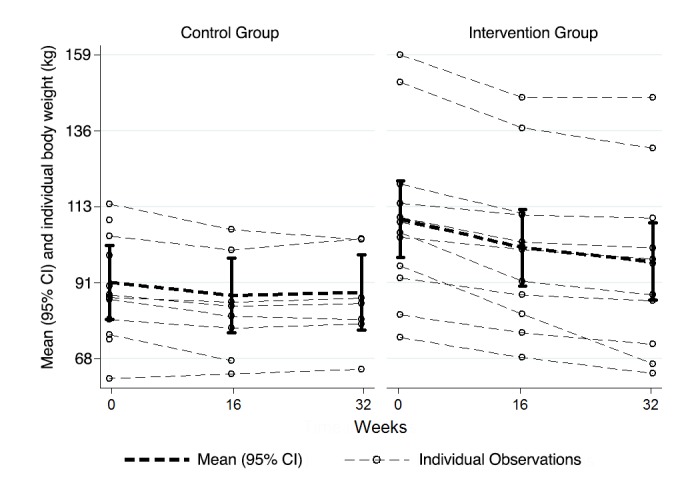
Mean and individual body weight (in kilograms) for the intervention and control groups at baseline and at 16 and 32 weeks. Bars represent 95% confidence intervals of the mean. Dashed lines reflect individual participants; darker lines represent each group mean.
We examined the intersection of weight and HbA1c changes over time for each participant (Figure 4). Participants in the intervention group tended to show strong downward and leftward trajectories, especially from baseline to 16 weeks, reflecting a strong initial loss in weight and HbA1c, whereas those trajectories reflected less simultaneous change for most participants in the control group.
Figure 4.
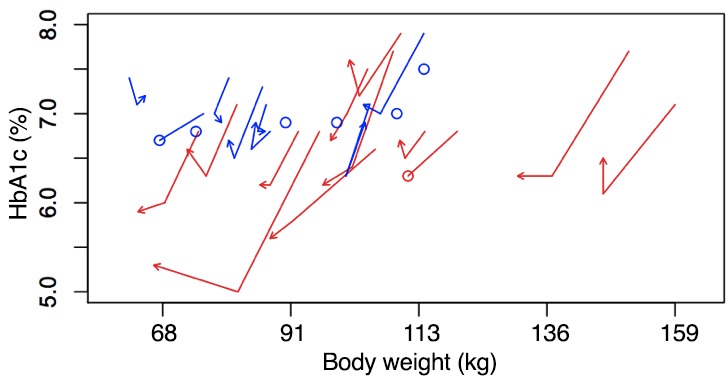
Body weight and HbA1c plotted for each participant separately for each of the three time periods (0, 16, and 32 weeks). Red lines represent the intervention participants; blue lines represent the control participants. Lines that end in an O reflect dropouts (and missing data). Lines that end in an arrow show participants who completed the study.
Cholesterol and Triglycerides
The intervention was also more effective at reducing triglycerides from baseline relative to the control; however, the effect was significant only at the 32-week time point (P=.01). Both HDL and LDL data revealed no effects between groups or differences from baseline within each group.
Psychological Self-Report
Diabetes-Related Distress
We found no statistically significant effects on this measure in the intervention group relative to the control group (Table 2).
Depressive Symptoms, Affect, and Vitality
We found no statistically significant effects on these measures in the intervention group relative to the control group (Table 2).
Subjective Experience of the Diets
Compared to the control group, participants in the intervention group rated themselves as less likely to cheat on their assigned diet at 16 and 32 weeks, with a large effect size of at least a Cohen d=–1.0 (Table 4). Participants in the intervention group also rated their diet less difficult to stick to, better liked how they felt on the diet, and were more likely to think that their diet improved their physical health, all with medium to large effect sizes.
Table 4.
Self-reported ratings of subjective experience of the diets.
| Self-reported ratings | Intervention group, mean (SD) | Control group, mean (SD) | Cohen d between groups | |
| Overall self-rating of how much they like how they feel on the diet | ||||
| 16 weeks | 5.9 (1.1) | 5.2 (1.3) | 0.6 | |
| 32 weeks | 6.2 (1.0) | 4.9 (2.3) | 0.8 | |
| Overall self-rating of how much they think the diet improved their physical health | ||||
| 16 weeks | 6.2 (1.0) | 5.3 (1.8) | 0.6 | |
| 32 weeks | 6.2 (0.9) | 5.1 (2.5) | 0.5 | |
| Overall self-rating of likelihood of cheating on diet | ||||
| 16 weeks | 2.7 (1.4) | 3.9 (0.9) | –1.0 | |
| 32 weeks | 3.4 (1.1) | 5.0 (0.8) | –1.7 | |
| Overall self-rating of difficulty of staying on diet | ||||
| 16 weeks | 2.7 (1.5) | 4.0 (1.3) | –0.9 | |
| 32 weeks | 3.2 (1.5) | 4.0 (1.7) | –0.5 | |
Physical Self-Report
Compared to participants in the control group, participants in the intervention group reported greater reductions in headache symptoms, bloating, and gas at week 16, as well as greater increases in constipation symptoms at week 16 (all with a large Cohen d effect size of at least 0.9 between groups; Multimedia Appendices 1 and 2.
Dietary Self-Reports
At both 16 and 32 weeks, compared to the control group, the intervention group reported eating fewer grams of nonfiber carbohydrates and grams of sugar. Grams of fat and protein did not show any group effects (Table 2).
The dietary measurements suggest that participants in both groups were, on average, adherent to their assigned diet. Participants in the intervention group ate the recommended daily grams of nonfiber carbohydrates and participants in the control group ate an expected percentage of their total calories from carbohydrates. In the intervention group, daily grams of nonfiber carbohydrates lowered from a mean of 163.6 (SD 86.7) grams at baseline to a mean of 40.4 (SD 45.9) grams at 16 weeks and a mean of 43.5 (SD 33.9) grams at 32 weeks, suggesting that participants were, on average, adherent to their assigned intervention diet. Although participants in the control group were not asked to reach a particular daily target for grams of nonfiber carbohydrates, their daily intake lowered from a mean of 152.0 (SD 58.9) grams at baseline to a mean of 127.1 (SD 40.2) grams at 16 weeks and a mean of 144.8 (SD 33.7) grams at 32 weeks.
In the intervention group, the mean percentage of calories from total carbohydrates changed from a baseline mean of 39.6% (SD 10.4%) to a mean of 15.5% (SD 13.0%) at 16 weeks and a mean of 18.5% (SD 12.8%) at 32 weeks. In the control group, the mean percentage of calories from total carbohydrates changed from a baseline mean of 37.6% (SD 10.3%) to a mean of 40.9% (SD 6.3%) at 16 weeks and a mean of 43.0% (SD 9.1%) at 32 weeks. This percentage of calories from carbohydrates in the both groups suggest that participants were, on average, adherent their assigned control diet; the overall target of percentage of calories from carbohydrates was expected to be approximately less than 20% in the intervention group and about 50% in the control group.
Medication Changes
The changes in metformin dosages were similar between groups. At 32 weeks, in the intervention group, metformin medications was decreased in one participant, increased in two participants, and unchanged in eight participants. In the control group, metformin dosage was decreased in two participants, increased in one participant, and unchanged in four participants. We had limited room to see differences in medication changes because we only enrolled participants on metformin, a drug that is safe enough and has a low enough risk of hypoglycemia that physicians do not quickly change its dosage.
Discussion
Principal Results
Our results show that participants randomly assigned to the very low-carbohydrate ketogenic diet and lifestyle recommendations (intervention) group had a variety of health benefits including lower HbA1c, body weight, and triglyceride levels, compared to those assigned to the control group (the plate method diet).
Our results are similar to those from our previous in-person trial of these very low-carbohydrate ketogenic diet and lifestyle recommendations. This online study differed from the in-person one due to its recruitment approach (national for this online study; in San Francisco, CA, for the in-person study), and allowable diabetes medications (none or just metformin for this online study; none, metformin, and/or sulfonylureas or dipeptidyl peptidase-4 inhibitor for the in-person study). These differences suggest that the online program might be applicable to overweight individuals with type 2 diabetes living across the United States, not currently taking multiple medications for their diabetes, who are motivated to make dietary changes, and have access to the Internet.
Limitations
The ability to generalize from the results of this study is limited by its size, targeted population, and length of follow-up time. We had to screen a large number of participants in order to find eligible participants. Of those screened, 26% filled out the online survey but did not have type 2 diabetes (according to their own self-report), 47% were taking or planning to take medications that made them ineligible, 10% were not interested once they heard more about the study from the study staff online, and only a few (<1%) reported having dietary preferences counter to those on the possible assigned diets. A larger trial with a longer follow-up is needed to better understand the durability of the effects on glycemic control and weight in a broader population.
By the end of the trial, we retained 92% of participants in the intervention group, compared to 54% of the control group. This difference could have been because the intervention group’s program had more sessions and included behavioral adherence strategies, which may have made their program more engaging. In addition, glycemic control and weight loss were lower in the intervention group; some participants in the control group expressed frustration that their glycemic control or weight loss was not as much as they would like, and thus they decided to not continue with the control program. Participants in the intervention group rated themselves as less likely to cheat on their assigned diet, compared to participants in the control group. Perhaps this difference in likelihood to cheat also suggests that the intervention program was easier to adhere to (possibly due to the diet or possibly due to the extra supports included in the intervention program).
Comparison With Prior Work
An innovative aspect of this program was remote monitoring of glycemic control, body weight, and other outcomes, suggesting that although these online program participants never met the researchers or study staff in-person, we were still able to measure and improve outcomes. Several other online interventions have successfully improved glycemic control and reduced body weight in adults, although their ability to retain participants was mixed. For example, one online program for individuals with prediabetes was based on the Diabetes Prevention Program, and it likely taught participants a lower-calorie, lower-fat diet, although this is not explicitly mentioned in the publication. After 12 months, participants’ HbA1c was reduced by 0.4% and they had lost 4.8% of body weight. However, only 45% of 220 participants had follow-up HbA1c values [39]. In a completely online program for overweight individuals that taught participants to follow a lower-calorie and lower-fat diet, participants in the active intervention group lost a mean 5.6% of their body weight 6 months after baseline. Of 77 participants assigned to the active intervention group, 70% were retained [40].
Not all online trials are effective. In an online self-management program for individuals with type 2 diabetes that recommended “healthy eating,” participants in the active intervention groups (with or without extra follow-up calls and visits) had not significantly reduced their HbA1c levels or lost weight at 12 months after baseline. Of 331 participants assigned to either intervention group, 72% were retained [41]. In an online self-care intervention for individuals with type 2 diabetes that also recommended “healthy eating,” participants assigned to the active intervention group did not show changes in their HbA1c at 6 months after baseline. Of 491 participants who began the program, 80% had 6-month outcome data [42]. Thus, the retention rate of our active intervention group (92%) was good compared to other previous online trials, as was our ability to bring about changes in glycemic control and weight in that group.
In previous trials of very low-carbohydrate diet programs in adults with type 2 diabetes that were at least 3 months or longer [7,38,43-58], researchers followed participants for a mean of 12 months. All interventions were in-person. On average, HbA1c dropped 1.0% (median –0.8%). Both mean and median body weight lost was –8%. Thus, the results from our online very low-carbohydrate intervention program replicate or improve on past results, given the fact that HbA1c dropped by 0.8% and body weight reduced by 12.0%.
Conclusions
Our results lend continued support for the idea that our program’s recommendations to follow a very low-carbohydrate ketogenic diet and make lifestyle changes is promising and can bring about improved health outcomes in overweight individuals with type 2 diabetes. Future work should examine how robust these results are with larger, more diverse participants; determine whether more robust psychological or other intervention support could improve dietary adherence; track whether the positive health effects are sustained over time; and, through more thorough implementation research, whether and how such an online intervention can dovetail with existing in-person health care teams. The online delivery of this approach gives it the potential to have wider impact in the treatment of type 2 diabetes.
Acknowledgments
Thanks very much to our dedicated participants as well as Patricia Moran and Michael Cohn for their help. The research was supported by a grant from the Mount Zion Health Fund. Laura Saslow and Ashley Mason were supported by National Institutes of Health (NIH) grant T32AT003997 from the National Center for Complementary and Integrative Health (NCCIH). Laura Saslow was also supported by funding from the William K Bowes, Jr Foundation and the NIH (K01 from the National Institute of Diabetes and Digestive and Kidney Diseases, DK107456). Ashley Mason was also supported by the NIH (K23 from the National Heart, Lung, and Blood Institute, HL133442). Judith Moskowitz was supported by NIH grant K24 MH093225 from the National Institute of Mental Health. Frederick Hecht was supported by NIH grant K24 AT007827 from NCCIH. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Abbreviations
- CESD
Center for Epidemiologic Studies Depression Scale
- HbA1c
glycated hemoglobin
- HDL
high-density lipoprotein
- LDL
low-density lipoprotein
- mDES
Modified Differential Emotions Scale
Baseline values of physical symptoms.
Change in symptoms from baseline.
Footnotes
Conflicts of Interest: Frederick Hecht is on the Scientific Advisory Board for Virta Health. No other author declares any conflict of interest.
References
- 1.American DA. Economic costs of diabetes in the US in 2012. Diabetes Care. 2013 Apr;36(4):1033–1046. doi: 10.2337/dc12-2625. http://europepmc.org/abstract/MED/23468086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, Lin JK, Farzadfar F, Khang Y, Stevens GA, Rao M, Ali MK, Riley LM, Robinson CA, Ezzati M, Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Glucose) National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet. 2011 Jul 2;378(9785):31–40. doi: 10.1016/S0140-6736(11)60679-X. [DOI] [PubMed] [Google Scholar]
- 3.Feinman RD, Pogozelski WK, Astrup A, Bernstein RK, Fine EJ, Westman EC, Accurso A, Frassetto L, Gower BA, McFarlane SI, Nielsen JV, Krarup T, Saslow L, Roth KS, Vernon MC, Volek JS, Wilshire GB, Dahlqvist A, Sundberg R, Childers A, Morrison K, Manninen AH, Dashti HM, Wood RJ, Wortman J, Worm N. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition. 2015 Jan;31(1):1–13. doi: 10.1016/j.nut.2014.06.011. http://linkinghub.elsevier.com/retrieve/pii/S0899-9007(14)00332-3. [DOI] [PubMed] [Google Scholar]
- 4.Volek JS, Phinney SD, Forsythe CE, Quann EE, Wood RJ, Puglisi MJ, Kraemer WJ, Bibus DM, Fernandez ML, Feinman RD. Carbohydrate restriction has a more favorable impact on the metabolic syndrome than a low fat diet. Lipids. 2009 Apr;44(4):297–309. doi: 10.1007/s11745-008-3274-2. [DOI] [PubMed] [Google Scholar]
- 5.Ruskin DN, Masino SA. The nervous system and metabolic dysregulation: emerging evidence converges on ketogenic diet therapy. Front Neurosci. 2012;6:33. doi: 10.3389/fnins.2012.00033. doi: 10.3389/fnins.2012.00033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bistrian BR, Blackburn GL, Flatt JP, Sizer J, Scrimshaw NS, Sherman M. Nitrogen metabolism and insulin requirements in obese diabetic adults on a protein-sparing modified fast. Diabetes. 1976 Jun;25(6):494–504. doi: 10.2337/diab.25.6.494. [DOI] [PubMed] [Google Scholar]
- 7.Dashti HM, Mathew TC, Khadada M, Al-Mousawi M, Talib H, Asfar SK, Behbahani AI, Al-Zaid NS. Beneficial effects of ketogenic diet in obese diabetic subjects. Mol Cell Biochem. 2007 Aug;302(1-2):249–256. doi: 10.1007/s11010-007-9448-z. [DOI] [PubMed] [Google Scholar]
- 8.Kirk JK, Graves DE, Craven TE, Lipkin EW, Austin M, Margolis KL. Restricted-carbohydrate diets in patients with type 2 diabetes: a meta-analysis. J Am Diet Assoc. 2008 Jan;108(1):91–100. doi: 10.1016/j.jada.2007.10.003. [DOI] [PubMed] [Google Scholar]
- 9.Nielsen JV, Joensson E. Low-carbohydrate diet in type 2 diabetes. Stable improvement of bodyweight and glycemic control during 22 months follow-up. Nutr Metab (Lond) 2006;3:22. doi: 10.1186/1743-7075-3-22. http://nutritionandmetabolism.biomedcentral.com/articles/10.1186/1743-7075-3-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Accurso A, Bernstein RK, Dahlqvist A, Draznin B, Feinman RD, Fine EJ, Gleed A, Jacobs DB, Larson G, Lustig RH, Manninen AH, McFarlane SI, Morrison K, Nielsen JV, Ravnskov U, Roth KS, Silvestre R, Sowers JR, Sundberg R, Volek JS, Westman EC, Wood RJ, Wortman J, Vernon MC. Dietary carbohydrate restriction in type 2 diabetes mellitus and metabolic syndrome: time for a critical appraisal. Nutr Metab (Lond) 2008;5:9. doi: 10.1186/1743-7075-5-9. http://nutritionandmetabolism.biomedcentral.com/articles/10.1186/1743-7075-5-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Santos FL, Esteves SS, da Costa PA, Yancy WS, Nunes JP. Systematic review and meta-analysis of clinical trials of the effects of low carbohydrate diets on cardiovascular risk factors. Obes Rev. 2012 Nov;13(11):1048–1066. doi: 10.1111/j.1467-789X.2012.01021.x. [DOI] [PubMed] [Google Scholar]
- 12.Markwald RR, Melanson EL, Smith MR, Higgins J, Perreault L, Eckel RH, Wright KP. Impact of insufficient sleep on total daily energy expenditure, food intake, and weight gain. Proc Natl Acad Sci U S A. 2013 Apr 2;110(14):5695–5700. doi: 10.1073/pnas.1216951110. http://www.pnas.org/cgi/pmidlookup?view=long&pmid=23479616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Broussard JL, Ehrmann DA, Van CE, Tasali E, Brady MJ. Impaired insulin signaling in human adipocytes after experimental sleep restriction: a randomized, crossover study. Ann Intern Med. 2012 Oct 16;157(8):549–557. doi: 10.7326/0003-4819-157-8-201210160-00005. http://europepmc.org/abstract/MED/23070488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Spiegel K, Knutson K, Leproult R, Tasali E, Van Cauter E. Sleep loss: a novel risk factor for insulin resistance and Type 2 diabetes. J Appl Physiol (1985) 2005 Nov;99(5):2008–2019. doi: 10.1152/japplphysiol.00660.2005. http://jap.physiology.org/cgi/pmidlookup?view=long&pmid=16227462. [DOI] [PubMed] [Google Scholar]
- 15.Spiegel K, Tasali E, Penev P, Van CE. Brief communication: sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann Intern Med. 2004 Dec 7;141(11):846–850. doi: 10.7326/0003-4819-141-11-200412070-00008. [DOI] [PubMed] [Google Scholar]
- 16.Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. 2006 Mar 14;174(6):801–809. doi: 10.1503/cmaj.051351. http://www.cmaj.ca/cgi/pmidlookup?view=long&pmid=16534088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Saslow L, Cohn M, Moskowitz J. Positive affect interventions to reduce stress: harnessing benefit while avoiding Pollyanna. In: Gruber J, Moskowitz J, editors. The Light and Dark Sides of Positive Emotion. New York: Oxford University Press; 2014. Jan 23, pp. 515–532. [Google Scholar]
- 18.Daubenmier J, Kristeller J, Hecht FM, Maninger N, Kuwata M, Jhaveri K, Lustig RH, Kemeny M, Karan L, Epel E. Mindfulness intervention for stress eating to reduce cortisol and abdominal fat among overweight and obese women: an exploratory randomized controlled study. J Obes. 2011;2011:651936. doi: 10.1155/2011/651936. doi: 10.1155/2011/651936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Daubenmier J, Moran PJ, Kristeller J, Acree M, Bacchetti P, Kemeny ME, Dallman M, Lustig RH, Grunfeld C, Nixon DF, Milush JM, Goldman V, Laraia B, Laugero KD, Woodhouse L, Epel ES, Hecht FM. Effects of a mindfulness-based weight loss intervention in adults with obesity: a randomized clinical trial. Obesity (Silver Spring) 2016 Apr;24(4):794–804. doi: 10.1002/oby.21396. http://europepmc.org/abstract/MED/26955895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Saslow LR, Kim S, Daubenmier JJ, Moskowitz JT, Phinney SD, Goldman V, Murphy EJ, Cox RM, Moran P, Hecht FM. A randomized pilot trial of a moderate carbohydrate diet compared to a very low carbohydrate diet in overweight or obese individuals with type 2 diabetes mellitus or prediabetes. PLoS One. 2014;9(4):e91027. doi: 10.1371/journal.pone.0091027. http://dx.plos.org/10.1371/journal.pone.0091027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.LaBrie JW, Quinlan T, Schiffman JE, Earleywine ME. Performance of alcohol and safer sex change rulers compared with readiness to change questionnaires. Psychol Addict Behav. 2005 Mar;19(1):112–115. doi: 10.1037/0893-164X.19.1.112. [DOI] [PubMed] [Google Scholar]
- 22.Bogg T, Roberts BW. Conscientiousness and health-related behaviors: a meta-analysis of the leading behavioral contributors to mortality. Psychol Bull. 2004 Nov;130(6):887–919. doi: 10.1037/0033-2909.130.6.887. [DOI] [PubMed] [Google Scholar]
- 23.Gosling SD, Rentfrow PJ, Swann WB. A very brief measure of the Big-Five personality domains. J Res Pers. 2003 Dec;37(6):504–528. doi: 10.1016/S0092-6566(03)00046-1. [DOI] [Google Scholar]
- 24.Gearhardt AN, Corbin WR, Brownell KD. Preliminary validation of the Yale Food Addiction Scale. Appetite. 2009 Apr;52(2):430–436. doi: 10.1016/j.appet.2008.12.003. [DOI] [PubMed] [Google Scholar]
- 25.Stice E, Telch CF, Rizvi SL. Development and validation of the Eating Disorder Diagnostic Scale: a brief self-report measure of anorexia, bulimia, and binge-eating disorder. Psychol Assess. 2000 Jun;12(2):123–131. doi: 10.1037//1040-3590.12.2.123. [DOI] [PubMed] [Google Scholar]
- 26.Garber AJ, Menzel PH, Boden G, Owen OE. Hepatic ketogenesis and gluconeogenesis in humans. J Clin Invest. 1974 Oct;54(4):981–989. doi: 10.1172/JCI107839. http://europepmc.org/abstract/MED/4430728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Forsythe CE, Phinney SD, Fernandez ML, Quann EE, Wood RJ, Bibus DM, Kraemer WJ, Feinman RD, Volek JS. Comparison of low fat and low carbohydrate diets on circulating fatty acid composition and markers of inflammation. Lipids. 2008 Jan;43(1):65–77. doi: 10.1007/s11745-007-3132-7. [DOI] [PubMed] [Google Scholar]
- 28.Kristeller JL, Wolever RQ. Mindfulness-based eating awareness training for treating binge eating disorder: the conceptual foundation. Eat Disord. 2011;19(1):49–61. doi: 10.1080/10640266.2011.533605. [DOI] [PubMed] [Google Scholar]
- 29.Wolff K, Cavanaugh K, Malone R, Hawk V, Gregory BP, Davis D, Wallston K, Rothman RL. The Diabetes Literacy and Numeracy Education Toolkit (DLNET): materials to facilitate diabetes education and management in patients with low literacy and numeracy skills. Diabetes Educ. 2009;35(2):233–238. doi: 10.1177/0145721709331945. http://europepmc.org/abstract/MED/19240246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Polonsky WH, Fisher L, Earles J, Dudl RJ, Lees J, Mullan J, Jackson RA. Assessing psychosocial distress in diabetes: development of the diabetes distress scale. Diabetes Care. 2005 Mar;28(3):626–631. doi: 10.2337/diacare.28.3.626. [DOI] [PubMed] [Google Scholar]
- 31.Roberts RE, Vernon SW. The Center for Epidemiologic Studies Depression Scale: its use in a community sample. Am J Psychiatry. 1983 Jan;140(1):41–46. doi: 10.1176/ajp.140.1.41. [DOI] [PubMed] [Google Scholar]
- 32.Fredrickson BL, Tugade MM, Waugh CE, Larkin GR. What good are positive emotions in crises? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J Pers Soc Psychol. 2003 Feb;84(2):365–376. doi: 10.1037//0022-3514.84.2.365. http://europepmc.org/abstract/MED/12585810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bartone PT, Ursano RJ, Wright KM, Ingraham LH. The impact of a military air disaster on the health of assistance workers. A prospective study. J Nerv Ment Dis. 1989 Jun;177(6):317–328. doi: 10.1097/00005053-198906000-00001. [DOI] [PubMed] [Google Scholar]
- 34.Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992 Jun;30(6):473–483. [PubMed] [Google Scholar]
- 35.Yusof A, Iahad N. Review on online and mobile weight loss management system for overcoming obesity. International Conference on Computer & Information Science (ICCIS); June 12-14, 2012; Kuala Lumpur, Malaysia. 2012. pp. 198–203. https://www.researchgate.net/publication/239524687_Review_on_Online_and_Mobile_Weight_Loss_Management_System_for_Overcoming_Obesity. [DOI] [Google Scholar]
- 36.Laing BY, Mangione CM, Tseng C, Leng M, Vaisberg E, Mahida M, Bholat M, Glazier E, Morisky DE, Bell DS. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: a randomized, controlled trial. Ann Intern Med. 2014 Nov 18;161(10 Suppl):S5–S12. doi: 10.7326/M13-3005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Taylor RW, Roy M, Jospe MR, Osborne HR, Meredith-Jones KJ, Williams SM, Brown RC. Determining how best to support overweight adults to adhere to lifestyle change: protocol for the SWIFT study. BMC Public Health. 2015;15:861. doi: 10.1186/s12889-015-2205-4. http://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-015-2205-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Willis EA, Szabo-Reed AN, Ptomey LT, Steger FL, Honas JJ, Al-Hihi EM, Lee R, Vansaghi L, Washburn RA, Donnelly JE. Distance learning strategies for weight management utilizing social media: A comparison of phone conference call versus social media platform. Rationale and design for a randomized study. Contemp Clin Trials. 2016 Feb 12;47:282–288. doi: 10.1016/j.cct.2016.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sepah SC, Jiang L, Peters AL. Translating the diabetes prevention program into an online social network: validation against CDC standards. Diabetes Educ. 2014 Apr 10;40(4):435–443. doi: 10.1177/0145721714531339. [DOI] [PubMed] [Google Scholar]
- 40.Thomas JG, Leahey TM, Wing RR. An automated internet behavioral weight-loss program by physician referral: a randomized controlled trial. Diabetes Care. 2015 Jan;38(1):9–15. doi: 10.2337/dc14-1474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Glasgow RE, Kurz D, King D, Dickman JM, Faber AJ, Halterman E, Woolley T, Toobert DJ, Strycker LA, Estabrooks PA, Osuna D, Ritzwoller D. Twelve-month outcomes of an Internet-based diabetes self-management support program. Patient Educ Couns. 2012 Apr;87(1):81–92. doi: 10.1016/j.pec.2011.07.024. http://europepmc.org/abstract/MED/21924576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Lorig K, Ritter PL, Laurent DD, Plant K, Green M, Jernigan VB, Case S. Online diabetes self-management program: a randomized study. Diabetes Care. 2010 Jun;33(6):1275–1281. doi: 10.2337/dc09-2153. http://europepmc.org/abstract/MED/20299481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Mayer SB, Jeffreys AS, Olsen MK, McDuffie JR, Feinglos MN, Yancy WS. Two diets with different haemoglobin A1c and antiglycaemic medication effects despite similar weight loss in type 2 diabetes. Diabetes Obes Metab. 2014 Jan;16(1):90–93. doi: 10.1111/dom.12191. http://europepmc.org/abstract/MED/23911112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Stern L, Iqbal N, Seshadri P, Chicano KL, Daily DA, McGrory J, Williams M, Gracely EJ, Samaha FF. The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: one-year follow-up of a randomized trial. Ann Intern Med. 2004 May 18;140(10):778–785. doi: 10.7326/0003-4819-140-10-200405180-00007. [DOI] [PubMed] [Google Scholar]
- 45.Samaha FF, Iqbal N, Seshadri P, Chicano KL, Daily DA, McGrory J, Williams T, Williams M, Gracely EJ, Stern L. A low-carbohydrate as compared with a low-fat diet in severe obesity. N Engl J Med. 2003 May 22;348(21):2074–2081. doi: 10.1056/NEJMoa022637. [DOI] [PubMed] [Google Scholar]
- 46.Hussain TA, Mathew TC, Dashti AA, Asfar S, Al-Zaid N, Dashti HM. Effect of low-calorie versus low-carbohydrate ketogenic diet in type 2 diabetes. Nutrition. 2012 Oct;28(10):1016–1021. doi: 10.1016/j.nut.2012.01.016. [DOI] [PubMed] [Google Scholar]
- 47.Yancy WS, Foy M, Chalecki AM, Vernon MC, Westman EC. A low-carbohydrate, ketogenic diet to treat type 2 diabetes. Nutr Metab (Lond) 2005 Dec 01;2:34. doi: 10.1186/1743-7075-2-34. https://nutritionandmetabolism.biomedcentral.com/articles/10.1186/1743-7075-2-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Westman EC, Yancy WS, Mavropoulos JC, Marquart M, McDuffie JR. The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus. Nutr Metab (Lond) 2008;5:36. doi: 10.1186/1743-7075-5-36. http://nutritionandmetabolism.biomedcentral.com/articles/10.1186/1743-7075-5-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Shai I, Schwarzfuchs D, Henkin Y, Shahar DR, Witkow S, Greenberg I, Golan R, Fraser D, Bolotin A, Vardi H, Tangi-Rozental O, Zuk-Ramot R, Sarusi B, Brickner D, Schwartz Z, Sheiner E, Marko R, Katorza E, Thiery J, Fiedler GM, Blüher M, Stumvoll M, Stampfer MJ, Dietary Intervention Randomized Controlled Trial (DIRECT) Group Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med. 2008 Jul 17;359(3):229–241. doi: 10.1056/NEJMoa0708681. [DOI] [PubMed] [Google Scholar]
- 50.Daly ME, Paisey R, Paisey R, Millward BA, Eccles C, Williams K, Hammersley S, MacLeod KM, Gale TJ. Short-term effects of severe dietary carbohydrate-restriction advice in Type 2 diabetes--a randomized controlled trial. Diabet Med. 2006 Jan;23(1):15–20. doi: 10.1111/j.1464-5491.2005.01760.x. [DOI] [PubMed] [Google Scholar]
- 51.Tay J, Luscombe-Marsh ND, Thompson CH, Noakes M, Buckley JD, Wittert GA, Yancy WS, Brinkworth GD. Comparison of low- and high-carbohydrate diets for type 2 diabetes management: a randomized trial. Am J Clin Nutr. 2015 Oct;102(4):780–790. doi: 10.3945/ajcn.115.112581. [DOI] [PubMed] [Google Scholar]
- 52.Yancy WS, Vernon MC, Westman EC. A pilot trial of a low-carbohydrate, ketogenic diet in patients with type 2 diabetes. Metab Syndr Relat Disord. 2003 Sep;1(3):239–243. doi: 10.1089/154041903322716723. [DOI] [PubMed] [Google Scholar]
- 53.Davis NJ, Tomuta N, Schechter C, Isasi CR, Segal-Isaacson CJ, Stein D, Zonszein J, Wylie-Rosett J. Comparative study of the effects of a 1-year dietary intervention of a low-carbohydrate diet versus a low-fat diet on weight and glycemic control in type 2 diabetes. Diabetes Care. 2009 Jul;32(7):1147–1152. doi: 10.2337/dc08-2108. http://europepmc.org/abstract/MED/19366978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Dyson PA, Beatty S, Matthews DR. A low-carbohydrate diet is more effective in reducing body weight than healthy eating in both diabetic and non-diabetic subjects. Diabet Med. 2007 Dec;24(12):1430–1435. doi: 10.1111/j.1464-5491.2007.02290.x. [DOI] [PubMed] [Google Scholar]
- 55.Vernon MC, Mavropoulos J, Transue M, Yancy WS, Westman EC. Clinical experience of a carbohydrate-restricted diet: effect on diabetes mellitus. Metab Syndr Relat Disord. 2003 Sep;1(3):233–237. doi: 10.1089/154041903322716714. [DOI] [PubMed] [Google Scholar]
- 56.Iqbal N, Vetter ML, Moore RH, Chittams JL, Dalton-Bakes CV, Dowd M, Williams-Smith C, Cardillo S, Wadden TA. Effects of a low-intensity intervention that prescribed a low-carbohydrate vs a low-fat diet in obese, diabetic participants. Obesity (Silver Spring) 2010 Sep;18(9):1733–1738. doi: 10.1038/oby.2009.460. doi: 10.1038/oby.2009.460. [DOI] [PubMed] [Google Scholar]
- 57.Nielsen JV, Joensson EA. Low-carbohydrate diet in type 2 diabetes: stable improvement of bodyweight and glycemic control during 44 months follow-up. Nutr Metab (Lond) 2008;5:14. doi: 10.1186/1743-7075-5-14. http://nutritionandmetabolism.biomedcentral.com/articles/10.1186/1743-7075-5-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Guldbrand H, Dizdar B, Bunjaku B, Lindström T, Bachrach-Lindström M, Fredrikson M, Ostgren CJ, Nystrom FH. In type 2 diabetes, randomisation to advice to follow a low-carbohydrate diet transiently improves glycaemic control compared with advice to follow a low-fat diet producing a similar weight loss. Diabetologia. 2012 Aug;55(8):2118–2127. doi: 10.1007/s00125-012-2567-4. http://europepmc.org/abstract/MED/22562179. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Baseline values of physical symptoms.
Change in symptoms from baseline.