

Abstract
Obstructive sleep apnea (OSA) occurs in 5%-14% of adults but is often undiagnosed. Apneas cause acute physiological changes, including alveolar hypoventilation and pulmonary artery vasoconstriction; they also promote chronic vascular disease secondary to increased platelet adhesiveness, endothelial dysfunction, and accelerated atherosclerosis. The Sleep Heart Health Study demonstrated that OSA is a risk factor for stroke and that an increase of 1 unit in the apnea-hypopnea index increases stroke risk by 6% in men. Patients with OSA frequently have atrial fibrillation (AF). Patients with OSA and AF have an increased incidence of stroke compared with patients with only OSA. The treatment of OSA with CPAP reduces the incidence of stroke and decreases the recurrence rate of AF in patients undergoing pulmonary vein ablation procedures. Undertreated OSA has the potential to complicate the postoperative course of patients undergoing cardiac surgery and increase the frequency of arrhythmias and ischemic events. However, one prospective study demonstrated that OSA did not increase complications during the first 30 days following surgery but increased complications during the long-term follow-up. OSA is associated with increased atherosclerotic coronary disease and the development of coronary events and congestive heart failure. In summary, patients with OSA have an increased frequency of stroke and AF The treatment of these patients with CPAP reduces the frequency of stroke and AF recurrence rate in patients with AF undergoing either medical management or invasive procedures. However, well-designed clinical trials are necessary to answer critical questions regarding the management of OSA in patients with cardiovascular diseases.
Keywords: obstructive sleep apnea, atrial fibrillation, stroke, cardiac surgery, coronary artery disease, outcomes
Introduction
Episodes of partial or complete airway obstruction lasting for >10 s during sleep characterize obstructive sleep apnea (OSA). Symptoms of excessive daytime sleepiness and an apnea-hypopnea index (AHI) of >5 events/h during polysomnography confirm the presence of OSA (1). The prevalence of OSA in the adult population is between 5% and 14%; however, this condition is often undiagnosed because of a lack of awareness and limited access to sleep centers (2, 3).
OSA is associated with cardiovascular diseases. For example, 20% of hypertensive patients have OSA, and a large study of 450 consecutive patients with heart failure estimated that the prevalence of OSA was between 31% and 38% (4, 5). Ventricular arrhythmias and cardiac conduction disorders are frequent in patients with sleep disordered breathing (SDB), and the frequency of arrhythmic events decreases after the treatment of OSA (6). Previous studies have also documented a strong association between OSA and atrial fibrillation (AF) (7). In addition, several studies suggest that there is increased risk of stroke in patients with OSA when they also have AF (8).
This review will address the following questions: 1. Does the presence of OSA in patients with AF increase the incidence of stroke or change the outcome in patients with stroke? 2. Does the presence of OSA in patients with AF change the management of AF or the success of management? 3. Does the presence of OSA in patients undergoing cardiac surgery increase the number of complications? 4. Does the presence of OSA change the management of patients with coronary artery disease (CAD)? This review will not discuss the association between OSA and hypertension or pulmonary hypertension.
Pathophysiological events during apneas at night
Repeated apneas and hypopneas during the night have pronounced physiological effects in patients with OSA (9). Reductions in ventilation cause alveolar hypoxia and hypercapnia. Pulmonary artery pressures increase because of pulmonary artery vasoconstriction related to alveolar hypoxia and because of increased blood return to the right heart secondary to negative intrathoracic pressure. Right ventricular overload can cause paradoxic movement of the intraventricular septum to the left and decrease left ventricular compliance. In addition, the negative intrathoracic pressure increases left ventricular afterload and left ventricular work. These changes can cause transient left ventricular dysfunction. These events are associated with increased sympathetic activity (10). Hypoxia, acidemia, and increased sympathetic activity predispose these patients to arrhythmias at night. Patients with severe OSA defined by an AHI of >30 have more frequent AF, nonsustained ventricular tachycardia, and complex ventricular ectopy than patients with an AHI of <5 (11). These arrhythmias occur more frequently following a respiratory event than during periods of normal respiration in these patients (12). These pathophysiologic events likely contribute to the adverse cardiac outcomes discussed in this review.
Obstructive sleep apnea and stroke
OSA has negative effects on cardiovascular physiology and causes increased platelet adhesiveness, vascular endothelial dysfunction, hypercoagulability, decreased cerebral blood flow, paradoxical embolization, and atherosclerosis. All of these alterations have a potential to put patients at an increased risk of cardiovascular events, including stroke (13). Since 1985, OSA has been studied as a potential risk factor for stroke, and studies in the 1990s have reported that the prevalence of OSA among patients with stroke was >60% (14, 15). However, at that time, it was not clear whether the high prevalence of stroke in patients with OSA was independent of confounders such as obesity, hypertension, and smoking history (16). Moreover, the temporal relationship between OSA and stroke was not determined, and it was not known if OSA preceded the occurrence of stroke.
Several studies have now provided sufficient evidence to prove that OSA is an independent risk factor for stroke. Four of these studies specifically evaluated stroke as the only endpoint; two studies used composite endpoints, such as cardiovascular events and strokes as well as all-cause death, and not stroke as the only endpoint (13-19). Arzt et al. (13) studied patients aged 30 to 60 years who were followed up for 12 years. They concluded that patients with an AHI of >20 had an increased prevalence of stroke compared with healthy individuals, independent of confounders. They also found that patients with moderate-to-severe OSA had an increased risk of having their first stroke over the next 4 years. However, after adjustment for confounders, this odds ratio was no longer significant. In addition, during the 4-year prospective follow-up, only 14 strokes occurred, limiting the statistical power of the study to detect a significant association between OSA and incident stroke. Shahar et al. (18) studied 6,000 subjects aged >40 years in the Sleep Heart Health Study (SHHS) who underwent overnight polysomnography at home to determine the cross-sectional association between SDB and the self-reported occurrence of stroke. They found a higher prevalence of self-reported stroke among subjects with OSA who had an AHI of >11/h; however, their final model did not adjust for hypertension or body mass index.
Munoz et al. (15) also studied an older population: individuals aged 70-100 years were followed up for 6 years. They found an increased risk of stroke in patients with severe OSA (AHI>30), but they adjusted only for age and sex and for no other confounders (15). Finally, Redline et al. (19) determined the incidence of stroke in a population extracted from the SHHS. Incident stroke was defined as the first occurrence of stroke between the date of the baseline polysomnogram and the end of follow-up of approximately 8 years. A significant positive association between ischemic stroke and AHI was observed in men; moreover, in the mild-to-moderate range (AHI between 5 and 25), each 1-unit increase in AHI increased the stroke risk by 6%. The relationship between AHI and stroke risk persisted after multiple adjustments for confounders. In women, stroke was not significantly associated with AHI quartiles; however, increased risk was observed at an AHI of >25.
Thus, recent studies demonstrate that OSA is an independent risk factor for ischemic stroke and that the risk of stroke is higher in more severe forms of OSA. One study also suggests that OSA might affect recovery from a stroke, possibly because sleep deprivation affects the response to rehabilitation or because nocturnal hypoxemia might impair neuronal healing (20). Mansukhani et al. (20) prospectively studied patients with recent stroke who were screened for OSA using the Berlin Sleep Questionnaire. Seven patients out of 174 in the study had a prior diagnosis of OSA. The 30 day mortality after stroke was five-fold higher in these patients, and OSA was an independent predictor of worse functional outcomes after hospital discharge.
Obstructive sleep apnea, atrial fibrillation, and stroke
A recent population based study demonstrated that OSA may increase the risk of AF by up to four fold; these patients are more likely to develop new onset AF independent of obesity (21, 22). Approximately 32%-49% of patients with AF have documented OSA (17). It has been proposed that OSA causes swings in the intrathoracic pressure during upper airway narrowing, resulting in atrial enlargement and, thus, predisposing the patient to the development of AF (21). In view of this association, studies have been conducted to evaluate the effect of OSA on the frequency of stroke in patients with AF to determine whether patients with OSA and AF have worse outcomes than those with no OSA, and to measure the impact of treatment of sleep apnea on the incidence of stroke in patients with AF
Mansukhani et al. (21) studied patients with newly diagnosed OSA with a sleep study and identified those diagnosed with ischemic stroke during the same timeframe. These authors compared these patients with those who had OSA only and determined the presence of AF. AF was more prevalent in patients with OSA who had had a stroke, and after controlling for confounders, AF was significantly associated with stroke in patients with OSA.
Holmqvist et al. (22) studied the population from the Outcome Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) who had reported AF and OSA. They determined the incidence of stroke, non-nervous systemic embolic events, and TIA in their study population, and also determined the effect of CPAP treatment on these outcomes. They concluded that the risk of death and the composite of cardiovascular death, myocardial infarction, and stroke/TIA were not significantly different between patients with both AF and OSA and patients with only AF, despite the fact that patients in the OSA/AF group were more likely to have a smoking history and higher BMIs. There were no statistically significant differences in mortality rates and major cardiovascular events between patients with OSA treated with CPAP and those without treatment. These results differ from those of Yaranov et al. (23), who performed a retrospective cohort study on patients with AF who had OSA to determine the occurrence of first time stroke (23). They found that the prevalence of stroke was higher in patients with AF and OSA compared with those without OSA (odds ratio for first-time stroke in patients with AF having OSA compared with those without OSA: 3.84, 95% CI: 1.33-11.05). This association remained statistically significant after adjustment for confounders such as BMI, smoking history, hypertension, and age, showing that OSA was an independent risk factor for stroke in patients with AF. Additionally, they found a dose effect relationship between AHI and the incidence of stroke and a decreased likelihood of stroke in patients with OSA who were compliant with CPAP compared with those who were not.
There are several points to note regarding the study by Holmqvist et al. (22). First, they used a composite endpoint, not stroke only as Yaranov did (23). Second, patients with OSA were more likely to be on prophylactic anticoagulation despite similar CHADS2 scores. This may have affected the results of this study by decreasing the incidence of stroke in patients with OSA. Third, the diagnosis of OSA was based on medical records and not on sleep study results. Since the prevalence of OSA in this population was lower than expected, it is likely that some patients with OSA were missed or undiagnosed. Finally, patients were only followed up for 2 years, which might not be sufficient time to calculate the actual incidence of events in the groups. The authors also note that compliance and the average number of hours of CPAP use per night in patients undergoing CPAP treatment were not known and that this might have affected the study results.
Since AF is one of the most important preventable causes of ischemic stroke and OSA is now known to be an independent risk factor for ischemic stroke, it has been proposed that OSA should be included in the risk assessment tools used to evaluate the risk of ischemic stroke in patients with AF Chang et al. (24) examined whether or not OSA provided additional predictive value to CHA2DS2-VASc scores to determine the patients may benefit from primary prevention of ischemic stroke. They concluded that adding OSA to the CHA2DS2-VASc score did not improve its predictive value for ischemic stroke in patients with AF This study result was unexpected, and some suggest that the study design was not adequate. First, the study included only patients with severe OSA requiring CPAP This is a smaller subgroup, and treatment with CPAP might ameliorate the impact of OSA on stroke risk and attenuate the risk of stroke in patients with OSA. Second, the authors report similar baseline CHA2DS2- VASc scores for the two groups, even though patients with concomitant AF and OSA had more frequent hypertension, diabetes, CAD, and peripheral arterial disease than patients with AF but without OSA (25).
Effect of obstructive sleep apnea on the management of atrial fibrillation
AF is a common arrhythmia and is common in patients with OSA. Patients with OSA have increased oxidative stress and inflammation, which increases left atrial volume, electroanatomic atrial remodeling, and fibrosis; these, in turn, increase the risk of AF (26, 27). In addition, patients with OSA often have enhanced sympathetic tone with surges in blood pressure during apneic episodes and during arousal periods at the end of obstructive events. This leads to left atrial stretch through pressure and volume overload and diastolic dysfunction, which can trigger AF episodes. Finally, intermittent nocturnal hypercapnia and hypoxemia present in patients with OSA may also increase patient vulnerability to developing AF by increasing the atrial conduction time. These three major mechanisms can limit the efficacy of medical, electrical, and catheter based treatment of AF
The treatment of OSA with continuous airway positive pressure (CPAP) reduces the number of hypoxic and hypercapnic episodes and diminishes the sympathetic tone in patients with OSA. These effects may decrease the recurrence rate of AF episodes regardless of the treatment strategy for AF Fein and coworkers examined the effect of CPAP on AF recurrence in patients with OSA who underwent pulmonary vein isolation. CPAP therapy mitigated the AF recurrence rate and increased AF-free survival in their study (26). The authors concluded that CPAP therapy can improve outcomes with AF ablation procedures and improve patient selection before offering this costly therapy to patients with coexistent AF and OSA. Naruse et al. (28) also evaluated the efficacy of CPAP therapy on recurrences after AF ablation in a prospective study with 153 patients. The authors found that patients with untreated OSA had a higher recurrence of AF after ablation. CPAP therapy in patients with OSA reduced the risk of recurrent AF by 60% (HR 0.41; 95% CI 0.22-0.76; p<0.01). These studies underline the importance of aggressive OSA treatment to improve AF ablation outcomes.
CPAP therapy decreases the left atrial volume index and improves cardiac remodeling; therefore, clinicians might expect CPAP treatment to reduce the rate of recurrent AF episodes (29). However, despite the high prevalence of both OSA and AF as well as the important implications of this association in current clinical practice, a randomized clinical trial specifically designed to determine whether CPAP therapy actually reduces the risk of recurrence of AF has not been done.
Effect of obstructive sleep apnea on outcomes postcardiac surgery
SDB is relatively common in patients with CAD and can potentially have adverse effects during the postoperative period following cardiac surgery. Uchoa et al. (30) studied the effects of OSA on cardiovascular events following coronary artery bypass surgery in 67 patients. The AHI was >15 events/h in 56% of these patients. There were no differences in all-cause death, myocardial infarction, repeat revascularization, or cerebrovascular events in patients with OSA during the first 30 days following surgery. However, there was a significant increase in the composite cardiovascular event score during prolonged follow-up in these patients (mean, 4.5 years). Patients with OSA had more frequent revascularization (19% vs. 0%), episodes of typical angina (30% vs. 7%), and AF (22% vs. 0%). These patients did not undergo any treatment during the follow-up because of financial constraints related to government insurance. Mooe et al. (31) monitored 121 consecutive patients during hospitalization following coronary bypass surgery. Patients with an AHI of >5 had a nonsignificant increase in AF during the postoperative period. Patients with an oxygen desaturation index (ODI) of >5 episodes/h had a statistically significant increase in AF (39% vs. 18%, p=0.02). Multivariate analysis indicated that increased age and an abnormal ODI increased the risk of AF in the postoperative period. Unosawa did postoperative portable monitoring for SDB and cardiac arrhythmias in 89 patients during the postoperative period following cardiac surgery (32). Twenty-six patients (29.2%) had an AHI of >15. These patients did not have a significant increase in the frequency of AF but did have more frequent premature ventricular contractions than patients without SDB (AHI<15). In addition, maximum daytime and nighttime heart rates were significantly higher in the frequent SDB group during the postoperative period. The studies report mixed results on the effect of OSA in postoperative cardiac patients. Patients with coronary disease are likely to have a higher frequency of OSA. This may result in nocturnal hypoxemia during the postoperative period, particularly if the patient receives narcotics for postoperative pain. However, the postoperative state might alter the frequency of AHI secondary to changes in respiratory drive, and routine management protocols with oxygen and/or noninvasive ventilation may reduce the degree of hypoxemia and AHI. Therefore, physicians caring for postoperative cardiac patients who have adverse events, particularly AF, should consider the possibility of untreated sleep apnea as a factor in these complications. During long-term follow-up, these patients will likely require evaluation for OSA and treatment if the AHI is high.
Effect of obstructive sleep apnea on coronary artery disease
Patients with CAD have an increased frequency of OSA (33-35). Several studies have reported a positive association between the severity of sleep apnea and the extent of coronary artery calcification (CAC) based on electron beam computed tomography (35, 36). Inami et al. (36) studied 83 patients and found that the severity of SDB was associated with the severity of the coronary atherosclerotic burden using coronary angiography and the Gensini score. Even in stable patients with CAD, they found that the severity of SDB was associated with increased levels of NT-proBNP and hs-TnT cardiac markers, suggesting ongoing silent myocardial stress and injury. Sorajja et al. (37) studied 202 patients without clinical coronary disease and found a strong association between OSA and subclinical CAD. OSA was directly associated with the extent and severity of CAC, and this association was independent of traditional coronary disease risk factors.
Several studies have concluded that OSA is an independent risk factor for the development of incident CAD (33, 37-39). However, in some studies, the findings were equivocal, and the results could not be generalized to all populations, particularly women of any age and men aged >70 years (40, 41). The prospective longitudinal Sleep Health Heart Study found that OSA was a significant predictor of the development of CAD and CHF in men between the ages of 40 and 70 years but not in women or older men (40, 41). Middle aged men with an AHI of >30 had a 68% greater chance of developing coronary heart disease defined by myocardial infarction, revascularization, or cardiac death than those with AHI<5.
The mechanisms that contribute to the pathogenesis of CAD in patients with OSA are multifactorial. Endothelial dysfunction, systemic inflammation, oxidative stress, hypoxia-induced sympathetic activation, and metabolic dysregulation lead to hypertension and atherosclerosis as well as promote coronary artery damage (35, 36, 38, 42, 43). This association between OSA and CAD has significant treatment implications. Patients with CAD and untreated OSA had a worse prognosis (38, 44). Patients with OSA treated with CPAP had improvement in their coronary health (34, 35, 45-47). Liu reported that 3 months of treatment with noninvasive ventilation improved ventricular dimensions and left ventricular ejection fractions and also reduced pro-brain natriuretic peptide levels (47).
In summary, OSA has a strong association with CAD, and treatment of OSA has the potential to improve outcomes in patients with CAD.
Discussion
OSA is a relatively common condition in adults and has definite adverse effects on the cardiovascular system (Table 1) (2, 3). These effects include acute effects associated with alveolar hypoventilation during apnea and the associated changes in pulmonary artery pressures and left ventricular function (9). OSA also has chronic effects on arterial vessels secondary to changes in coagulation and accelerated atherosclerosis. OSA increases the frequency of stroke even after adjustment for other confounding medical disorders (15, 19). Patients with AF have an increased frequency of OSA, and patients with both disorders have an increased incidence of stroke. The treatment of patients with OSA and AF with CPAP can reduce the frequency of stroke (21, 22). OSA complicates the management of AF and appears to increase recurrence rates. Better management of OSA with CPAP can reduce these recurrence rates (28). OSA has the potential to increase complications during the postoperative period in patients undergoing cardiac surgery. In-hospital management of these patients may minimize adverse effects related to OSA; however, these patients appear to have more frequent complications during the long-term follow-up if OSA is undertreated (30). Patients with CAD and OSA have more frequent cardiac events (40, 41). In summary, OSA has important adverse consequences in patients with common cardiovascular disorders. Clinicians need to consider this diagnosis while managing these patients, and treatment with CPAP has the potential to reduce the complexity of management, the frequency of incident stroke, and the frequency of recurrent stroke and recurrent AF in these patients. Screening for OSA may involve questionnaires, such as the Berlin questionnaire, portable home polysomnography, or formal overnight polysomnography in sleep centers, in patients with symptoms suggesting sleep apnea.
Table 1.
Important articles on associations between OSA and CVDs used in this review
| Clinical diagnosis | Study | Outcome |
|---|---|---|
| Stroke (19) | 5422 participants, untreated OSA, median follow-up 8.7 years | 193 strokes; 4.4 strokes per 1000 person-years; OAHI >19 in men resulted in R: 2.86 after adjustment; non-significant HR in women |
| Stroke with AF (23) | 332 patients with AF, 85.2% with OSA | 22.9% had stroke; OR: 3.65 with OSA; increased stroke with CHADS2 score 0 & 1; more likely in CPAP non-compliant patients |
| AF management (28) | 153 patients with AF, 116 with OSA, median follow-up 18.8 months after ablation | 51 patients with recurrence; OSA increased recurrence (HR 2.61, P<0.05); CPAP decreased recurrence (HR 0.41, P<0.01) |
| Coronary artery disease (40) | 4422 subjects with median follow-up 8.7 years | 473 incident coronary events; in men <70 years the HR was 1.10 per 10 unit increase in AHI; no increase in older men or women; 308 cases of CHF; HR: 1.13 per 10 unit increase in AHI in men all ages; no increase in women |
| Cardiac surgery (30) | 67 patients with coronary surgery, 57% had AHI >15 | No increase in complications during first 30 days following surgery; significant increase in composite cardiac event score during 4.5 year follow-up |
AF - atrial fibrillation; CHF - congestive heart failure; CVD - cardiovascular disorders; HR - hazard ratio; OAHI - obstructive apnea-hypopnea index; OR - odds ratio; OSA - obstructive sleep apnea
The association between OSA and cardiovascular disorders discussed in this review has important clinical implications for patients. AF and CAD clearly impact longevity and quality of life, and the management of these disorders frequently requires complicated medication regimens and/or invasive procedures. We need more definitive information on the contribution of OSA to outcomes in these patients based on trials that are randomized and controlled as much as possible (Fig. 1). The definition of clinically important AHI in these patients is unknown, and the study design should consider the following questions: 1. Is the diagnosis of OSA sufficient to identify patients at risk of cardiovascular complications? 2. Is there a linear relationship between AHI and the frequency of cardiovascular complications? 3. Is there an AHI threshold that identifies patients at an increased risk of complications? 4. Do patients with apneas and daytime sleepiness have more complications than patients with apneas but no sleepiness? 5. Does the oxygen desaturation index (i.e., the degree of hypoxemia) help predict complications? Randomized controlled trials are possible in the management of patients with AF and stroke. For example, patients with AF scheduled for ablation procedures can undergo polysomnography. Patients with elevated AHI defined by an AHI of >15 can undergo CPAP titration and treatment for 4-8 weeks prior to the ablation procedure. The control group may be merely observed. Following ablation, patients may continue treatment or remain under observation. Follow-up studies may determine the success rate for ablation, the frequency of recurrence, and the impact of CPAP treatment on these outcomes. Patients with stroke are frequently referred to rehabilitation centers posthospitalization. These patients can undergo portable polysomnography within 7 days postdischarge and be randomized into two groups. Some patients with an AHI of >15 can start CPAP treatment. The control group may have no therapy directed at OSA. Polysomnography can be repeated after 4-8 weeks in the control group to determine the percentage of patients with resolved OSA following acute stroke and the percentage of patients with persistent OSA. The latter group could be randomized into treatment and observation groups to determine the frequency of recurrent stroke and transient ischemic events as well as clinical outcomes. The design of these clinical trials will depend on case load and resources.
Figure 1.
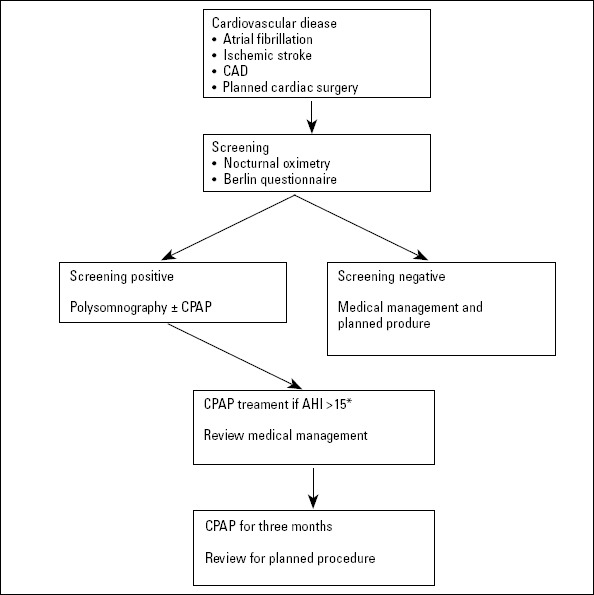
OSA screening and management in patients with selected cardiovascular diseases
*An argument could be made for an AHI>5
Pastori et al. (48) recently reported a prospective study involving 1019 patients with AF All patients were treated with oral vitamin K antagonists and had a median follow-up of 34 months. These patients had 111 cardiovascular events during follow-up for an event rate of 3.43%/year, which was much higher than the stroke and transient ischemic attack event rate (0.96%/year). Multivariate analysis indicated that age, smoking, history of cerebrovascular or cardiac events, metabolic syndrome, heart failure, and male sex predicted these events. These authors concluded that metabolic syndrome is a common clinical feature in patients with AF that increases their risk of cardiovascular events. They encourage a holistic approach to the management of these patients to reduce cardiovascular complications. However, they did not consider the possibility of OSA as a contributing factor. Because of the strong association between metabolic syndrome and OSA, this study suggests that this holistic approach should depend on medication as well as include a careful assessment of OSA, particularly in patients with AF (48). This study suggests that there are opportunities for improving outcomes in patients with chronic cardiovascular disease having OSA, if well-designed studies provide conclusive management strategies.
Acknowledgements:
We greatly appreciate the assistance of Cihan Çevik MD and Alejandro Velasco MD in the development of the manuscript.
References
- 1.Somers VK, White DIP, Amin R, Abraham WT, Costa IF, Culebras A, et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. J Am Coll Cardiol. 2008;52:686–717. doi: 10.1016/j.jacc.2008.05.002. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 2.Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177:1006–14. doi: 10.1093/aje/kws342. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Young T, Evans L, Finn L, Palta M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep. 1997;20:705–6. doi: 10.1093/sleep/20.9.705. [DOI] [PubMed] [Google Scholar]
- 4.Lavie P, Ben-Yosef R, Rubin AE. Prevalence of sleep apnea syndrome among patients with essential hypertension. Am Heart J. 1984;108:373–6. doi: 10.1016/0002-8703(84)90628-8. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 5.Sin DD, Fitzgerald F, Parker JD, Newton G, Floras JS, Bradley TD. Risk factors for central and obstructive sleep apnea in 450 men and women with congestive heart failure. Am J Respir Crit Care Med. 1999;160:1101–6. doi: 10.1164/ajrccm.160.4.9903020. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 6.Guilleminault C, Connolly SJ, Winkle RA. Cardiac arrhythmia and conduction disturbances during sleep in 400 patients with sleep apnea syndrome. Am J Cardiol. 1983;52:490–4. doi: 10.1016/0002-9149(83)90013-9. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 7.Gami AS, Pressman G, Caples SM, Kanagala R, Gard JJ, Davison DE, et al. Association of atrial fibrillation and obstructive sleep apnea. Circulation. 2004;110:364–7. doi: 10.1161/01.CIR.0000136587.68725.8E. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 8.Velasco A, Nugent K. Should we treat nonsleepy patients with obstructive sleep apnea and atrial fibrillation with CPAP? J Clin Sleep Med. 2013;9:1235–6. doi: 10.5664/jcsm.3254. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ismail K, Roberts K, Manning P, Manley C, Hill NS. OSA and pulmonary hypertension. time for a new look. Chest. 2015;147:847–61. doi: 10.1378/chest.14-0614. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 10.Tamisier R, Tan CO, Pepin JL, Levy P, Taylor JA. Blood Pressure Increases in OSA due to Maintained Neurovascular Sympathetic Transduction: Impact of CPAP Sleep 2015. doi: 10.5665/sleep.5252. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mehra R, Benjamin EJ, Sahar E, Gottlieb DJ, Nawabit R, Kirchner HL, et al. Association of nocturnal arrhythmias with sleep-disordered breathing: The Sleep Heart Health Study. Am J Respir Crit Care Med. 2006;173:910–6. doi: 10.1164/rccm.200509-1442OC. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Monahan K, Storfer-Isser A, Mehra R, Shahar E, Mittleman M, Rottman J, et al. Triggering of nocturnal arrhythmias by sleep disordered breathing events. J Am Coll Cardiol. 2009;54:1797–804. doi: 10.1016/j.jacc.2009.06.038. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Arzt M, Young T, Finn L, Skatrud JB, Bradley TD. Association of sleep-disordered breathing and the occurrence of stroke. Am J Respir Crit Care Med. 2005;172:1447–51. doi: 10.1164/rccm.200505-702OC. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034–41. doi: 10.1056/NEJMoa043104. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 15.Munoz R, Duran-Cantolla J, Matinez-Vila E, Gallego J, Rubio R, Aizpuru F, et al. Severe sleep apnea and risk of ischemic stroke in the elderly. Stroke. 2006;37:2317–21. doi: 10.1161/01.STR.0000236560.15735.0f. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 16.Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. doi: 10.1016/S0140-6736(05)71141-7. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 17.Yazdan-Ashoori P, Baranchuk A. Obstructive sleep apnea may increase the risk of stroke in AF patients: refining the CHADS2 score. Int J Cardiol. 2011;146:131–3. doi: 10.1016/j.ijcard.2010.10.104. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 18.Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163:19–25. doi: 10.1164/ajrccm.163.1.2001008. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 19.Redline S, Yenokyan G, Gottlieb DJ, Shahar E, O’Connor GT, Resnick HE, et al. Obstructive sleep apnea-hypopnea and incident stroke the sleep heart health study. Am J Respir Crit Care Med. 2010;182:269–77. doi: 10.1164/rccm.200911-1746OC. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mansukhani MR, Bellolio MF, Kolla BP, Enduri S, Somers VK, Stead LG. Worse outcome after stroke in patients with obstructive sleep apnea: an observational cohort study. J Stroke Cerebrovasc Dis. 2011;20:401–5. doi: 10.1016/j.jstrokecerebrovasdis.2010.02.011. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 21.Mansukhani MP, Calvin AD, Kolla BIP, Brown RD, Jr, Lipford MC, Somers VK, et al. The association between atrial fibrillation and stroke in patients with obstructive sleep apnea: a population-based case-control study. Sleep Med. 2013;14:243–6. doi: 10.1016/j.sleep.2012.08.021. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Holmqvist F, Guan N, Zhu Z, Kowey PR, Allen LA, Fonarow GC, et al. Impact of obstructive sleep apnea and continuous positive airway pressure therapy on outcomes in patients with atrial fibrillation-Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) Am Heart J. 2015;169:647–54. doi: 10.1016/j.ahj.2014.12.024. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 23.Yaranov DM, Smyrlis A, Usatii N, Butler A, Petrini JR, Mendez J, et al. Effect of obstructive sleep apnea on frequency of stroke in patients with atrial fibrillation. Am J Cardiol. 2015;115:461–5. doi: 10.1016/j.amjcard.2014.11.027. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 24.Chang CC, Chiu CC, Chiang CH, Huang CC, Chan WL, Huang PH, et al. Obstructive sleep apnea and the risk of ischemic stroke in patients with atrial fibrillation. Int J Cardiol. 2015;181:144–6. doi: 10.1016/j.ijcard.2014.12.019. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 25.Kalemci S, Altun I, Akın F, Biteker M. Obstructive sleep apnea and stroke risk in atrial fibrillation: Is there a correlation or not? Int J Cardiol. 2015;184:306. doi: 10.1016/j.ijcard.2015.02.065. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 26.Fein AS, Shvilkin A, Shah D, Haffajee CI, Das S, Kumar K, et al. Treatment of obstructive sleep apnea reduces the risk of atrial fibrillation recurrence after catheter ablation. J Am Coll Cardiol. 2013;62:300–5. doi: 10.1016/j.jacc.2013.03.052. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 27.Romero-Corral A, Somers VK, Pellikka PA. Decreased right and left ventricular myocardial performance in obstructive sleep apnea. Chest. 2007;132:1863–70. doi: 10.1378/chest.07-0966. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 28.Naruse Y, Tada H, Satoh M, Yanagihara M, Tsuneoka H, Hirata Y, et al. Concomitant obstructive sleep apnea increases the recurrence of atrial fibrillation following radiofrequency catheter ablation of atrial fibrillation: clinical impact of continuous positive airway pressure therapy. Heart Rhythm. 2013;10:331–7. doi: 10.1016/j.hrthm.2012.11.015. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 29.Colish J, Walker JR, Elmayergi N, Almutairi S, Alharbi F, Lytwyn M, et al. Obstructive sleep apnea: effects of continuous positive airway pressure on cardiac remodeling as assessed by cardiac biomarkers, echocardiography, and cardiac MRI. Chest. 2012;141:674–81. doi: 10.1378/chest.11-0615. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 30.Uchoa CH, Danzi-Soares Nde J, Nunes FS, de Souza AA, Nerbass FB, Pedrosa RP, et al. Impact of OSA on cardiovascular events after coronary artery bypass surgery. Chest. 2015;147:1352–60. doi: 10.1378/chest.14-2152. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 31.Mooe T, Gullsby S, Rabben T, Eriksson P. Sleep-disordered breathing: a novel predictor of atrial fibrillation after coronary artery bypass surgery. Coron Artery Dis. 1996;7:475–8. [CrossRef] [PubMed] [Google Scholar]
- 32.Unosawa S, Sezai A, Akahoshi T, Niino T, Shimura K, Shiono M, et al. Arrhythmia and sleep-disordered breathing in patients undergoing cardiac surgery. J Cardiol. 2012;60:61–5. doi: 10.1016/j.jjcc.2012.01.012. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 33.Mooe T, Rabben T, Wiklund U, Franklin KA, Eriksson P. Sleep-disordered breathing in men with coronary artery disease. Chest. 1996;109:659–63. doi: 10.1378/chest.109.3.659. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 34.Peker Y, Kraiczi H, Hedner J, Loth S, Johansson A, Bende M. An independent association between obstructive sleep apnoea and coronary artery disease. Eur Respir J. 1999;14:179–84. doi: 10.1034/j.1399-3003.1999.14a30.x. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 35.Somers VK, White DP, Amin R, Abraham WT, Costa F, Culebras A, et al. Sleep apnea and cardiovascular disease: an American Heart Association/american College Of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council On Cardiovascular Nursing. In collaboration with the National Heart, Lung, and Blood Institute National Center on Sleep Disorders Research (National Institutes of Health) Circulation. 2008;118:1080–111. doi: 10.1161/CIRCULATIONAHA.107.189375. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 36.Inami T, Seino Y, Otsuka T, Yamamoto M, Kimata N, Murakami D, et al. Links between sleep disordered breathing, coronary atherosclerotic burden, and cardiac biomarkers in patients with stable coronary artery disease. J Cardiol. 2012;60:180–6. doi: 10.1016/j.jjcc.2012.03.003. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 37.Sorajja D, Gami AS, Somers VK, Behrenbeck TR, Garcia-Touchard A, Lopez-Jimenez F. Independent association between obstructive sleep apnea and subclinical coronary artery disease. Chest. 2008;133:927–33. doi: 10.1378/chest.07-2544. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.McNicholas WT, Bonsigore MR. Sleep apnoea as an independent risk factor for cardiovascular disease: current evidence, basic mechanisms and research priorities. Eur Respir J. 2007;29:156–78. doi: 10.1183/09031936.00027406. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 39.Schafer H, Koehler U, Ewig S, Hasper E, Tasci S, Luderitz B. Obstructive sleep apnea as a risk marker in coronary artery disease. Cardiology. 1999;92:79–84. doi: 10.1159/000006952. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 40.Gottlieb DJ, Yenokyan G, Newman AB, O’Connor GT, Punjabi NM, Quan SF, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation. 2010;122:352–60. doi: 10.1161/CIRCULATIONAHA.109.901801. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Newman AB, Nieto FJ, Guidry U, Lind BK, Redline S, Pickering TG, et al. Relation of sleep-disordered breathing to cardiovascular disease risk factors: the Sleep Heart Health Study. Am J Epidemiol. 2001;154:50–9. doi: 10.1093/aje/154.1.50. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 42.Namtvedt SK, Hisdal J, Randby A, Agewall S, Stranden E, Somers VK, et al. Impaired endothelial function in persons with obstructive sleep apnoea: impact of obesity. Heart. 2013;99:30–4. doi: 10.1136/heartjnl-2012-303009. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 43.Sanchez-de-la-Torre M, Campos-Rodriguez F, Barbe F. Obstructive sleep apnoea and cardiovascular disease. Lancet Respir Med. 2013;1:61–72. doi: 10.1016/S2213-2600(12)70051-6. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 44.Mooe T, Franklin KA, Holmstrom K, Rabben T, Wiklund U. Sleep-disordered breathing and coronary artery disease: long-term prognosis. Am J Respir Crit Care Med. 2001;164:1910–3. doi: 10.1164/ajrccm.164.10.2101072. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 45.Çifçi N, Uyar M, Elbek O, Süyür H, Ekinci E. Impact of CPAP treatment on cardiac biomarkers and pro-BNP in obstructive sleep apnea syndrome. Sleep Breath. 2010;14:241–4. doi: 10.1007/s11325-009-0306-y. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 46.Einvik G, Rosjo H, Randby A, Namtvedt SK, Hrubos-Strom H, Brynildsen J, et al. Severity of obstructive sleep apnea is associated with cardiac troponin I concentrations in a community-based sample: data from the Akershus Sleep Apnea Project. Sleep. 2014;37:1111–6. doi: 10.5665/sleep.3772. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Liu X, Feng L, Cao G, Huang H, Xu Q, Yu J, et al. Cardiac structure and function improvements in coronary artery disease combined with severe obstructive sleep apnea/hypopnea syndrome patients via noninvasive positive pressure ventilation therapy. Coron Artery Dis. 2014;25:516–20. doi: 10.1097/MCA.0000000000000129. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 48.Pastori D, Pignatelli P, Angelico F, Farcomeni A, Del Ben M, Vicario T, et al. Incidence of myocardial infarction and vascular death in elderly patients with atrial fibrillation taking anticogulants: relationship to atherosclerotic risk factors. Chest. 2015;147:1644–50. doi: 10.1378/chest.14-2414. [CrossRef] [DOI] [PubMed] [Google Scholar]