

Abstract
Relative to those with European ancestry, African Americans have an excess incidence of nondiabetic chronic kidney disease predominantly due to two coding renal-risk variants in the apolipoprotein L1 gene (APOL1). This APOL1–kidney disease association is independent of systemic hypertension or blood pressure. Recent reports describe extra-renal effects of the APOL1 G1 and G2 renal-risk variants on cardiovascular disease (CVD), subclinical atherosclerosis, lipoprotein particle concentrations, and survival. However, results have been less consistent than those seen in kidney disease, and the observed APOL1 associations with CVD vary from risk to protective. This manuscript reviews the relationships between APOL1 renal-risk variants and CVD, with an emphasis on study-specific factors that may have contributed to disparate observations. It is possible that APOL1 renal-risk variants impact the systemic vasculature, not only the kidneys. As novel therapies for APOL1-associated nephropathy are developed, APOL1 variant protein effects on large blood vessels and risk of CVD will need to be considered.
Keywords: African Americans, apolipoprotein L1 gene, APOL1, atherosclerosis, cardiovascular disease, chronic kidney disease, myocardial infarction
Introduction
The increased risk of nondiabetic chronic kidney disease (CKD) in African Americans relative to European Americans had long been unexplained.1 In contrast to historic reports suggesting that ethnic differences in systemic blood pressures and socioeconomic factors were major contributors, it is now believed that the majority of this ethnic-specific difference relates to biologic variation in the apolipoprotein L1 gene (APOL1) on chromosome 22q.2,3 This breakthrough linked several previously disparate kidney diseases—including idiopathic focal segmental glomerulosclerosis, HIV-associated collapsing glomerulosclerosis (HIV-associated nephropathy), severe lupus nephritis, sickle cell nephropathy, and hypertension-attributed nephropathy (a primary kidney disease manifesting as focal global glomerulosclerosis with renal interstitial and vascular changes and secondary hypertension)—to a single disease spectrum referred to as APOL1-associated nephropathy.4,5
Several groups have assessed extra-renal effects of APOL1 renal-risk variants on subclinical atherosclerosis (calcified atherosclerotic plaque determined by computed tomography), myocardial infarction (MI), stroke, altered lipoprotein particle concentrations, and participant survival in large trials and cohort studies. In contrast to the consistently observed autosomal recessive APOL1 associations with nondiabetic CKD (risk genotypes include G1G1, G2G2, or G1G2), effects on nonrenal outcomes have been inconsistent, and associations have been reported with recessive and nonrecessive (additive and dominant) genetic models.6 Besides the different cohorts, study designs, and outcomes, APOL1 associations with kidney disease varied between reports and could have impacted findings. This review summarizes published data on the nonrenal vascular effects of the APOL1 G1 and G2 renal-risk variants in the admixed African American population with an emphasis on cardiovascular disease (CVD) phenotypes.
APOL1 and Lipoprotein Particle Concentrations
Given the recent interest in the effects of APOL1 on CVD, it is useful to review studies reporting effects on lipid profiles and lipoprotein particle concentrations. This is especially relevant because APOL1 protein travels in the circulation bound to a subset of trypanosome lytic factors 1 and 2 lipoprotein particles; it does not appear to be bound to typical plasma high-density lipoprotein (HDL) particles as has often been reported.7,8 To date, there is no evidence of association between APOL1 genotypes and circulating APOL1 protein concentrations or components of the standard lipid profile, such as low-density lipoprotein (LDL) cholesterol, HDL cholesterol, or triglycerides.9–13
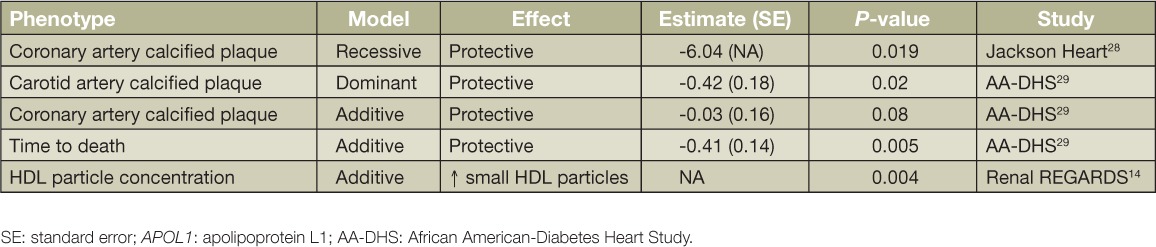
A report of more than 2,000 African American participants in the REGARDS study detected positive association between APOL1 renal-risk variants and small HDL cholesterol particle concentrations.14 The effect of this observation on risk for CVD or MI is currently unknown. APOL1 renal-risk variant effects on macrophage cholesterol efflux and other components of the atherosclerotic process also require further study. Finally, Bentley et al. reported that serum HDL cholesterol relationships with CKD differed in African Americans with and without APOL1 renal-risk variants.11,15 The impact of this finding on clinical CVD outcomes is under study.
APOL1 and Subclinical Calcified Atherosclerotic Plaque
Calcified plaque in the coronary arteries (CAC), as well as in the aorta and carotid arteries, is widely recognized to be a marker of subclinical atherosclerosis and is associated with heightened risk for CVD events and death.16–18 The higher risk for CVD in individuals with higher CAC is observed in members of all ethnic groups. In contrast to European Americans, African Americans have markedly lower levels of CAC despite the presence of more severe conventional CVD risk factors such as higher blood pressure, LDL cholesterol, albuminuria, and blood sugars in populations with diabetes.19–22 The population-based Multi-Ethnic Study of Atherosclerosis (MESA) and the African American-Diabetes Heart Study (AA-DHS) both revealed that African Americans who had higher levels of CAC had higher percentages of European ancestry.23,24 This demonstrates that African ancestry is protective from the development of subclinical CVD and CAC, whereas European ancestry contributes to risk. This effect is contrary to the APOL1-associated risk for CKD based on positive selection for trypanolytic variants of sub-Saharan African origin. It further demonstrates that, in addition to the environment, biologic variation or inherited factors contribute to the risks of CVD and CKD.
The clinical relevance of lower levels of CAC in African Americans was evident in studies where both African and European Americans had equivalent access to healthcare. In contrast to the general population, where African Americans have greater risk for CVD than European Americans, African Americans with type 2 diabetes treated by the Veteran's Administration and Kaiser Permanente had 50% lower rates of MI than European Americans.25,26 Similar lower rates of MI and improved survival rates are seen in African Americans with end-stage kidney disease receiving renal replacement therapy through the Centers for Medicare and Medicaid Services.27 Therefore, the lower levels of CAC in African Americans relative to European Americans have biologic relevance once the confounding effects of environmental factors, including “differential access to healthcare,” are considered.
The Jackson Heart Study (JHS) and AA-DHS measured calcified atherosclerotic plaque with computed tomography in the large blood vessels of African Americans and tested for genetic association with APOL1 (Table 1). APOL1 renal-risk variants were associated with lower levels of calcified atherosclerotic plaque in the left main coronary arteries in JHS and with lower levels of calcified plaque in multiple vascular beds in AA-DHS, with results consistent across studies.28,29 Calcified plaque associations in AA-DHS were strongest in additive and dominant genetic models, whereas JHS reported an association in a recessive model. In the JHS, the significant association between CAC and APOL1 persisted when removing participants with CKD, supporting a true protective effect of renal-risk variants on subclinical CVD. Despite concordance between calcified plaque associations with APOL1 in the AA-DHS sample with type-2 diabetes (717 participants with measured CAC) and JHS (1,959 participants; number with CAC not provided), discordant effects of APOL1 on clinical CVD events were observed despite the expected protection from CVD and MI in those with lower levels of calcified atherosclerotic plaque in the coronary arteries and aorta.
Table 1.
APOL1 associations with subclinical cardiovascular disease and related phenotypes.
APOL1 Renal-Risk Variants and Cardiovascular Disease
APOL1-Associated Risk for Cardiovascular Disease and Incident Myocardial Infarction
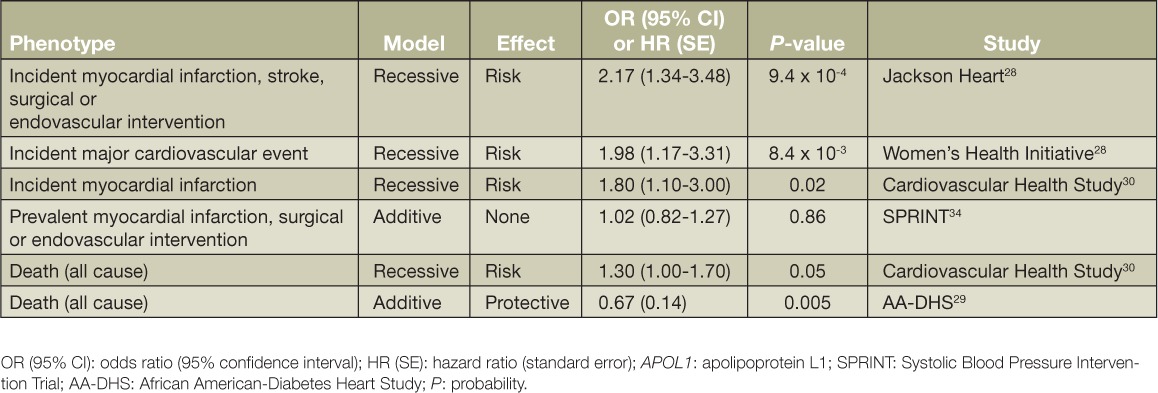
Three studies identified an increased risk for CVD or incident MI among African Americans with two APOL1 renal-risk variants (Table 2); however, APOL1 was significantly associated with the presence of kidney disease and/or albuminuria in all three reports.28,30 Although adjustment for CKD was performed, it remains uncertain whether kidney disease, a powerful risk factor for MI, could have confounded results.31 The initial report by Ito et al. assessed the JHS and African American participants in the Women's Health Initiative (WHI).28 With the large size of these studies and the national representation of the WHI, CVD events were adjudicated and expected to be highly accurate. Participants with two APOL1 renal-risk variants in both studies had higher rates of incident MI, stroke, and surgical or endovascular intervention even after statistical adjustment for CKD. Women's Health Initiative participants did not have computed tomography scans to measure CAC or subclinical atherosclerosis. As noted above, JHS participants with two APOL1 renal-risk variants had significantly lower levels of CAC. Therefore, the paradoxical observation of a lower CAC despite higher CVD rates led the authors to speculate that novel mechanisms might have contributed to CVD outcomes. As stated above, the possibility that CKD was a confounder in this surprising finding may not have been fully excluded by statistical adjustment. In the Cardiovascular Health Study (CHS), Mukamal et al. analyzed incident MI related to APOL1 in African American participants with a mean age of 73 years.30 As in JHS and WHI, CVD events were adjudicated. Again, the presence of two APOL1 renal-risk variants was associated with albuminuria (but not estimated glomerular filtration rate) and MI; association with CVD persisted after adjustment for albuminuria. Therefore, JHS, WHI, and CHS all reported positive association between two APOL1 renal-risk variants and adjudicated CVD events or MI and also with CKD or albuminuria.28,30
Table 2.
APOL1 associations with major cardiovascular events and death.
APOL1-Associated Protection from Death and CVD Events
Consistent findings in JHS, WHI, and CHS provide reassurance as to detected associations. However, it is difficult to completely exclude the confounding effects of APOL1-associated CKD on risk for MI. Although the African American Study of Kidney Disease and Hypertension (AASK) was not designed or powered to demonstrate the risk of MI or death, APOL1 was strongly associated with renal outcomes (doubling of serum creatinine concentration or initiation of dialysis),32 yet very few deaths were recorded in this population with advanced CKD despite their high risk for CVD.33 This suggests that APOL1 might not be associated with a markedly heightened risk for CVD.
In AA-DHS, all participants had type 2 diabetes, and APOL1 was not associated with diabetic kidney disease. As opposed to conclusions drawn from JHS, AA-DHS linked participant survival in the Social Security Death Index (SSDI) to genotypes (Table 2). In agreement with the APOL1 association with lower levels of calcified atherosclerotic plaque (and lack of confounding by nephropathy association), increasing numbers of APOL1 renal-risk variants were associated with longer survival (additive genetic model).29 As with adjudicated events in JHS and CHS, results were likely accurate given that outcomes were assessed using the SSDI. Although results differed from those in JHS and CHS, AA-DHS evaluated a uniformly diabetes-affected cohort at high risk for CVD, and kidney disease phenotypes (albuminuria and eGFR) did not confound results. Therefore, there are potential explanations for the different directions of association between AA-DHS and the other reports.
Finally, the Systolic Blood Pressure Intervention Trial (SPRINT) enrolled only nondiabetic individuals, many with mild-to-moderate CKD and low level proteinuria (albuminuria below 1,000 mg/day); recruitment specifically targeted the elderly and those with prevalent CVD.34 SPRINT saw weak association between APOL1 and CKD in 2,571 African American participants but observed no evidence of association between APOL1 and prevalent CVD. This was despite large numbers of SPRINT participants with CVD. However, results were cross-sectional. Longitudinal associations will soon be assessed, as SPRINT was halted prematurely due to beneficial effects of a lower systolic blood pressure goal on primary CVD outcomes.
Therapeutic Considerations
As targeted therapies for APOL1-associated nephropathy are likely to be developed in the near future, it is critical to elucidate whether the CVD effects of APOL1 renal-risk variants increase or decrease the risk of cardiac events. Kidney transplantation studies suggest that the nephropathy risk from APOL1 renal-risk appears principally related to intrinsic gene expression in cells of the kidney and not to circulating APOL1 protein.35–37 However, it is unknown whether vascular gene expression or circulating proteins are involved in the cardiovascular effects of APOL1. Circulating APOL1 protein concentration does not appear to be dependent on APOL1 renal-risk variant genotypes.7,38 APOL1 messenger RNA and protein have been detected in vascular cells, which supports the potential for a local vascular effect as with nephropathy risk.39,40
If APOL1 renal-risk alleles exhibit opposing effects on CVD and nephropathy risk, an effect supported by AA-DHS, treatments that improve renal outcomes might have the potential to aggravate CVD. In contrast, if reports from JHS, WHI, and CHS are correct and APOL1 renal-risk alleles increase the risk for CVD independently from nephropathy, treatments for APOL1-associated kidney disease could also improve cardiac outcomes. The conflicting data on APOL1 associations with increased cardiovascular events (JHS, WHI, and CHS), lower levels of CAC (JHS and AA-DHS), and reduced rates of death (AA-DHS) require additional studies to reach a consensus. Ideally, future analyses can be performed in populations with recent African ancestry where APOL1 is not (or only weakly) associated with nephropathy to limit confounding between CKD and CVD. This remains a fertile area of research and holds great importance for individuals who possess recent African ancestry.
Key Points
Apolipoprotein L1 gene (APOL1) renal-risk genotypes contribute to approximately 40% of cases of end-stage kidney disease in the African American population.
Associations between APOL1 renal-risk variants with cardiovascular disease and mortality are less consistent than those with nephropathy.
As targeted therapies for APOL1-associated kidney disease are developed, additional studies are required to clearly elucidate the vascular effects of its renal-risk variants.
Conflict of Interest Disclosure
Wake Forest University Health Sciences and Barry I. Freedman have filed for a patent related to APOL1 genetic testing. Dr. Freedman receives research funding from Novartis and is a consultant for Ionis Pharmaceuticals and AstraZeneca.
References
- 1. United States Renal Data System. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2014. USRDS annual data report: an overview of the epidemiology of kidney disease in the United States; 2014. [Google Scholar]
- 2. Genovese G, Friedman DJ, Ross MD, . et al. Association of trypanolytic ApoL1 variants with kidney disease in African Americans. Science. 2010. August 13; 329( 5993): 841– 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Tzur S, Rosset S, Shemer R, . et al. Missense mutations in the APOL1 gene are highly associated with end stage kidney disease risk previously attributed to the MYH9 gene. Hum Genet. 2010. September; 128( 3): 345– 50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Freedman BI. APOL1 and kidney disease: new insights leading to novel therapies. Am J Kidney Dis. 2015. July; 66( 1): 9– 11. [DOI] [PubMed] [Google Scholar]
- 5. Palmer ND, Freedman BI.. APOL1 and Progression of Nondiabetic Nephropathy. J Am Soc Nephrol. 2013. September; 24( 9): 1344– 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Lipkowitz MS. Apolipoprotein L1: from obscurity to consistency to controversy. Kidney Int. 2015. January; 87( 1): 14– 7. [DOI] [PubMed] [Google Scholar]
- 7. Weckerle A, Snipes JA, Cheng D, . et al. Characterization of circulating APOL1 protein complexes in African Americans. J Lipid Res. 2016. January; 57( 1): 120– 30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Samanovic M, Molina-Portela MP, Chessler AD, Burleigh BA, Raper J.. Trypanosome lytic factor, an antimicrobial high-density lipoprotein, ameliorates Leishmania infection. PLoS Pathog. 2009. January; 5( 1): e1000276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Mukamal KJ, Tremaglio J, Friedman DJ, . et al. APOL1 Genotype, Kidney and Cardiovascular Disease, and Death in Older Adults. Arterioscler Thromb Vasc Biol. 2016. February; 36( 2): 398– 403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Foster MC, Coresh J, Fornage M, . et al. APOL1 variants associate with increased risk of CKD among African Americans. J Am Soc Nephrol. 2013. September; 24( 9): 1484– 91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Bentley AR, Divers J, Shriner D, . et al. APOL1 G1 genotype modifies the association between HDLC and kidney function in African Americans. BMC Genomics. 2015. May 30; 16: 421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Friedman DJ, Kozlitina J, Genovese G, Jog P, Pollak MR.. Population-based risk assessment of APOL1 on renal disease. J Am Soc Nephrol. 2011. November; 22( 11): 2098– 2105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Freedman BI, Langefeld CD, Murea M. et al. Apolipoprotein L1 nephropathy risk variants associate with HDL subfraction concentration in African Americans. Nephrol Dial Transplant. 2011; 26: 3805– 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Gutierrez OM, Judd SE, Irvin MR, . et al. APOL1 nephropathy risk variants are associated with altered high-density lipoprotein profiles in African Americans. Nephrol Dial Transplant. 2016. April; 31( 4): 602– 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Bentley AR, Doumatey AP, Chen G, . et al. Variation in APOL1 Contributes to Ancestry-Level Differences in HDLc-Kidney Function Association. Int J Nephrol. 2012; 2012: 748984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Detrano R, Guerci AD, Carr JJ, . et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008. March 27; 358( 13): 1336– 45. [DOI] [PubMed] [Google Scholar]
- 17. Budoff MJ, McClelland RL, Chung H, . et al. Reproducibility of coronary artery calcified plaque with cardiac 64-MDCT: the Multi-Ethnic Study of Atherosclerosis. AJR Am J Roentgenol. 2009. March; 192( 3): 613– 7. [DOI] [PubMed] [Google Scholar]
- 18. Budoff MJ, Young R, Lopez VA, . et al. Progression of coronary calcium and incident coronary heart disease events: MESA Multi-Ethnic Study of Atherosclerosis. J Am Coll Cardiol. 2013. March 26; 61( 12): 1231– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Bild DE, Detrano R, Peterson D, . et al. Ethnic differences in coronary calcification: the Multi-Ethnic Study of Atherosclerosis MESA. Circulation. 2005. March 15; 111( 10): 1313– 20. [DOI] [PubMed] [Google Scholar]
- 20. Lee TC, O'Malley PG, Feuerstein I, Taylor AJ.. The prevalence and severity of coronary artery calcification on coronary artery computed tomography in black and white subjects. J Am Coll Cardiol. 2003. January 1; 41( 1): 39– 44. [DOI] [PubMed] [Google Scholar]
- 21. Freedman BI, Hsu FC, Langefeld CD, . et al. The impact of ethnicity and sex on subclinical cardiovascular disease: the Diabetes Heart Study. Diabetologia. 2005. December; 48( 12): 2511– 8. [DOI] [PubMed] [Google Scholar]
- 22. Carnethon MR, Bertoni AG, Shea S, . et al. Racial/Ethnic differences in subclinical atherosclerosis among adults with diabetes: the multiethnic study of atherosclerosis. Diabetes Care. 2005. November; 28( 11): 2768– 70. [DOI] [PubMed] [Google Scholar]
- 23. Wassel CL, Pankow JS, Peralta CA, Choudhry S, Seldin MF, Arnett DK.. Genetic ancestry is associated with subclinical cardiovascular disease in African-Americans and Hispanics from the multi-ethnic study of atherosclerosis. Circ Cardiovasc Genet. 2009. December; 2( 6): 629– 36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Divers J, Palmer ND, Lu L, . et al. Admixture mapping of coronary artery calcified plaque in African Americans with type 2 diabetes. Circ Cardiovasc Genet. 2013. February 1; 6( 1): 97– 105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Karter AJ, Ferrara A, Liu JY, Moffet HH, Ackerson LM, Selby JV.. Ethnic disparities in diabetic complications in an insured population. JAMA. 2002. May 15; 287( 19): 2519– 27. [DOI] [PubMed] [Google Scholar]
- 26. Young BA, Maynard C, Boyko EJ.. Racial differences in diabetic nephropathy, cardiovascular disease, and mortality in a national population of veterans. Diabetes Care. 2003. August; 26( 8): 2392– 9. [DOI] [PubMed] [Google Scholar]
- 27. Young BA, Rudser K, Kestenbaum B, Seliger SL, Andress D, Boyko EJ.. Racial and ethnic differences in incident myocardial infarction in end-stage renal disease patients: The USRDS. Kidney Int. 2006. May 1; 69( 9): 1691– 8. [DOI] [PubMed] [Google Scholar]
- 28. Ito K, Bick AG, Flannick J, . et al. Increased burden of cardiovascular disease in carriers of APOL1 genetic variants. Circ Res. 2014. February 28; 114( 5): 845– 50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Freedman BI, Langefeld CD, Lu L, . et al. APOL1 associations with nephropathy, atherosclerosis, and all-cause mortality in African Americans with type 2 diabetes. Kidney Int. 2015. January; 87( 1): 176– 81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Mukamal KJ, Tremaglio J, Friedman DJ, . et al. APOL1 Genotype, Kidney and Cardiovascular Disease, and Death in Older Adults. Arterioscler Thromb Vasc Biol. 2016. February; 36( 2): 398– 403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Weiner DE, Tighiouart H, Amin MG, . et al. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol. 2004. May; 15( 5): 1307– 15. [DOI] [PubMed] [Google Scholar]
- 32. Appel LJ, Wright JT Jr, Greene T, . et al.; African American Study of Kidney Disease and Hypertension Collaborative Research Group Long-term effects of renin-angiotensin system-blocking therapy and a low blood pressure goal on progression of hypertensive chronic kidney disease in African Americans. Arch Intern Med. 2008. April 28; 168( 8): 832– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Alves TP, Wang X, Wright JT Jr, . et al. Rate of ESRD exceeds mortality among African Americans with hypertensive nephrosclerosis. J Am Soc Nephrol. 2010. August; 21( 8): 1361– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Langefeld CD, Divers J, Pajewski NM, . et al. Apolipoprotein L1 gene variants associate with prevalent kidney but not prevalent cardiovascular disease in the Systolic Blood Pressure Intervention Trial. Kidney Int. 2015. January; 87( 1): 169– 75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Reeves-Daniel AM, Depalma JA, Bleyer AJ, . et al. The APOL1 gene and allograft survival after kidney transplantation. Am J Transplant. 2011. May; 11( 5): 1025– 30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Freedman BI, Julian BA, Pastan SO, . et al. Apolipoprotein L1 gene variants in deceased organ donors are associated with renal allograft failure. Am J Transplant. 2015. June; 15( 6): 1615– 22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Freedman BI, Pastan SO, Israni AK, . et al. APOL1 Genotype and Kidney Transplantation Outcomes From Deceased African American Donors. Transplantation. 2016. January; 100( 1): 194– 202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Bruggeman LA, O'Toole JF, Ross MD, . et al. Plasma apolipoprotein L1 levels do not correlate with CKD. J Am Soc Nephrol. 2014. March; 25( 3): 634– 44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Madhavan SM, O'Toole JF, Konieczkowski M, Ganesan S, Bruggeman LA, Sedor JR.. APOL1 localization in normal kidney and nondiabetic kidney disease. J Am Soc Nephrol. 2011. November; 22( 11): 2119– 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Ma L, Shelness GS, Snipes JA, . et al. Localization of APOL1 protein and mRNA in the human kidney: nondiseased tissue, primary cells, and immortalized cell lines. J Am Soc Nephrol. 2015. February; 26( 2): 339– 48. [DOI] [PMC free article] [PubMed] [Google Scholar]