

Abstract
Background
The prognostic effect of pretreatment elevated platelet count remains controversial in colorectal cancer patients. We conducted this meta-analysis to evaluate the prognostic impact of it in these patients.
Methods
PubMed, EMBASE and Cochrane Library were searched and studies on the prognostic significance of pretreatment elevated platelet count in colorectal patients were identified. We performed the meta-analysis, using overall survival and disease-free survival as outcomes and presenting data with hazard ratio and its 95% confidence interval. Heterogeneity among studies and publication bias were also evaluated.
Results
Thirty studies were included in the meta-analysis. Compared with normal platelet count, pretreatment elevated platelet count was associated with poorer overall survival (Hazard ratio = 1.837, 95% confidence interval, 1.497 to 2.255, p = 0.000) and poorer disease-free survival (Hazard ratio = 1.635, 95% confidence interval, 1.237 to 2.160, p = 0.001) in patients with colorectal cancer. In subgroup analyses, pretreatment elevated platelet count was also associated with poorer overall survival and disease-free survival in most subgroups.
Conclusion
Pretreatment elevated platelet count was an independent prognostic factor of overall survival and disease-free survival in colorectal cancer patients. Large-scale prospective studies and a validation study are warranted.
Keywords: colorectal cancer, platelet, thrombocytosis, prognosis, meta-analysis
INTRODUCTION
Colorectal cancer is the third most commonly diagnosed cancer in males and the second in females, with an estimated 1.4 million cases and 693,900 deaths occurring in 2012 [1]. Several markers like carcinoembryonic antigen, C-reactive protein, albumin and tumor necrosis factors have been reported as prognostic indicators of outcomes in patients with colorectal cancer. However, it is still difficult to predict the outcome of patients before treatment.
There is a growing body of evidence showing that elevated platelet count or thrombocytosis is associated with outcomes of colorectal cancer [2–10]. Early in 1998, Monreal M et al. reported a significant association between pre-operative platelet count and survival in patients with colorectal cancer. The following studies confirmed this association [2, 3, 5, 6]. However, some other studies failed to demonstrate the association between pretreatment elevated platelet count and outcomes of colorectal cancer [11–16]. Considering the controversial evidence, we conduct a meta-analysis to evaluate whether pretreatment elevated platelet count is a prognostic marker of colorectal cancer.
RESULTS
Study selection
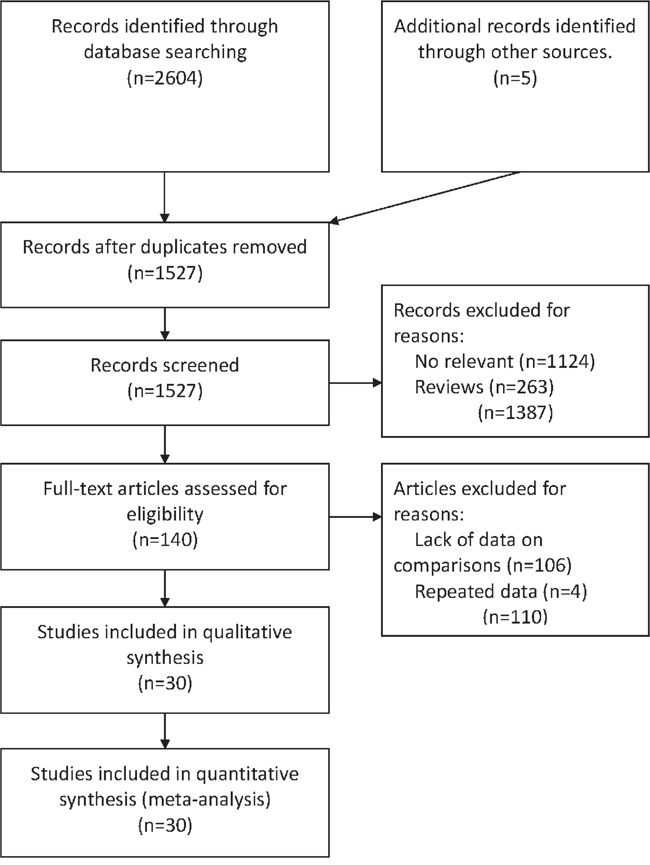
Electronic search identified 2604 potentially relevant references. Additional 5 references were further identified by checking the reference list. 2469 duplicates or clearly irrelevant references were excluded through reading the abstracts. 140 references were read in full and 106 references were excluded for irrelevance or lack of data on comparisons or outcomes. Four references were excluded for repeated data. Finally, 30 references fulfilled the inclusion criteria and provided data for the meta-analysis [2–31] (Figure 1).
Figure 1. Flowchart of the process for the identification of relevant studies.
Characteristics of included studies
All thirty included articles were cohort studies published from 1998 to 2016. This meta-analysis included 9123 patients. The quality score of included studies ranged from 6 to 8 stars. Hazard ratios of overall survival were available in 28 included studies and hazard ratios of disease-free survival were available in 15 included studies. Characteristics of the included studies are listed in Table 1.
Table 1. Characteristics of included studies.
| Study | Number of patients | Tumor type | Disease stage | Cut-off value | Area | Study time | Age (year) | Follow-up (year) | Treatment | Outcome | Quality score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Azab B 2014 [11] | 580 | colorectal cancer | I-IV | tertile | USA | 2005-2011 | 68.6 | 40.5 | surgery or chemotherapy | overall survival, disease-free survival | 6 |
| Baranyai Z 2014 [2] | 336 | colorectal cancer | I-IV | 400 | Hungary | 2001-2011 | 67 | 36.1 | surgery | overall survival, disease-free survival | 8 |
| Carruthers R 2012 [17] | 115 | rectal cancer | I-III | NA | UK | 2000-2005 | 63.8 | 37.1 | chemoradiation and surgery | overall survival, disease-free survival | 6 |
| Chen LL 2016 [3] | 503 | colorectal cancer | I-IV | 300 | China | 2010-2013 | 58 | 33.8 | surgery | overall survival | 7 |
| Choi KW 2014 [12] | 105 | colorectal cancer | I-IV | 400 | Korea | 2005-2008 | 63 | 44 | surgery | overall survival | 7 |
| Cravioto-Villanueva A 2012 [4] | 163 | rectal cancer | I-III | 350 | Mexico | 2000-2007 | 57.6 | 35.4 | chemoradiation and surgery | overall survival | 6 |
| Del Prete M 2015 [18] | 208 | colorectal cancer | IV | 0.54 ULN | Italy | NA | 61 | NA | chemotherapy | overall survival | 6 |
| Guo T 2014 [5] | 310 | colorectal cancer | I-III | 400 | USA | 2004-2013 | 69.9 | NA | NA | overall survival | 6 |
| Jósa V 2015 [19] | 336 | colorectal cancer | I-IV | 400 | Hungary | 2001-2011 | 66.9 | NA | surgery and chemotherapy | overall survival | 6 |
| Jósa V 2015 [19] | 166 | colorectal cancer | IV | 380 | Hungary | 2001-2011 | 62 | 28 | surgery and chemotherapy | overall survival, disease-free survival | 6 |
| Kandemir EG 2005 [7] | 198 | colon cancer | I-II | 400 | Turkey | NA | 57 | 47 | NA | overall survival, disease-free survival | 7 |
| Kaneko M 2012 [20] | 50 | colorectal cancer | IV | 400 | Japan | 2005-2010 | 61 | 17 | chemotherapy | overall survival, | 7 |
| Kawai K 2013 [8] | 108 | rectal cancer | I-IV | 365 | Japan | 2003-2012 | 63.3 | 22.5 | chemoradiation and surgery | disease-free survival | 7 |
| Kim HJ 2015 [9] | 314 | rectal cancer | I-III | 370 | Japan | 2003-2011 | NA | 36 | chemoradiation and surgery | overall survival, disease-free survival | 7 |
| Kozak MM 2015 [21] | 129 | colorectal cancer | I-III | 400 | USA | 2005-2009 | 67 | 24.7 | chemotherapy | overall survival, disease-free survival | 7 |
| Kronborg CS 2015 [13] | 314 | colorectal cancer | IV | 400 | Denmark | 2007-2011 | 64.5 | 21.3 | chemotherapy | overall survival | 7 |
| Lee YS 2016 [22] | 284 | colorectal cancer | II | 450 | Korea | 2003-2009 | 65 | 7.67 | Adjuvant therapy | overall survival, disease-free survival | 8 |
| Lin MS 2012 [23] | 150 | colorectal cancer | I-IV | 300 | China | 2006-2011 | 60.9 | NA | surgery or NA | overall survival | 6 |
| Monreal M 1998 [24] | 180 | colorectal cancer | I-III | quertile | Spain | 1994-1996 | 67 | 13 | surgery and chemotherapy | overall survival | 7 |
| Neal CP 2015 [25] | 302 | colorectal cancer | IV | 400 | UK | 2006-2010 | 64.8 | 29.7 | surgery | overall survival | 7 |
| Paik KY 2014 [26] | 600 | colorectal cancer | I-IV | 400 | Korea | 2006-2009 | 62.3 | 27.4 | surgery | overall survival, disease-free survival | 8 |
| Qiu MZ 2010 [27] | 363 | colorectal cancer | I-IV | 400 | China | 2005-2009 | 56 | 26 | NA | overall survival | 7 |
| Roxburgh CS 2010 [28] | 287 | colon cancer | I-III | 400 | UK | 1997-2005 | NA | 65 | surgery and chemotherapy | overall survival | 7 |
| Sasaki K 2012 [29] | 636 | colorectal cancer | I-IV | 370 | Japan | 2002-2008 | 65.9 | 49.1 | surgery and chemotherapy | overall survival, disease-free survival | 8 |
| Shen L 2014 [14] | 199 | rectal cancer | II-III | 300 | China | 2006-2011 | 55 | 31 | chemoradiation and surgery | overall survival, disease-free survival | 8 |
| Song A 2015 [15] | 177 | colorectal cancer | IV | 400 | South Korea | 2006-2013 | 52 | 3.1 | chemotherapy | overall survival | 7 |
| Toiyama Y 2015 [30] | 89 | rectal cancer | I-III | 300 | Japan | 2001-2012 | 65 | 56 | chemoradiation and surgery | overall survival, disease-free survival | 8 |
| Wan S 2013 [31] | 1513 | colorectal cancer | I-IV | 400 | USA | 1990-2010 | 64.9 | 54 | surgery and chemotherapy | overall survival, disease-free survival | 8 |
| Wei Y 2015 [10] | 286 | colorectal cancer | II-III | 276 | China | 2003-2011 | 62 | 34 | surgery and chemotherapy | disease-free survival | 7 |
| Zhao H 2016 [16] | 122 | colorectal cancer | IV | 300 | China | 2006-2009 | NA | NA | chemotherapy | overall survival | 7 |
NA, not available; ULN, upper limits of normal.
Prognostic impact of pretreatment elevated platelet count on overall survival
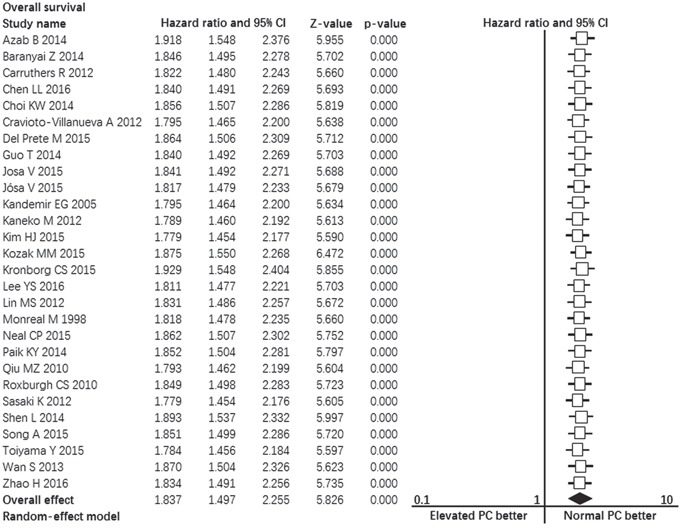
Twenty-eight studies contributed data to the analyses of overall survival [2-7, 9, 11-31]. Significant heterogeneity was found among studies (I2 = 81%, p = 0.000, Figure 2). Random-effect model was used. The pooled hazard ratio estimate showed that patients with pretreatment elevated platelet count had poorer overall survival compared with normal platelet count (HR = 1.837, 95% confidence interval, 1.497 to 2.255, p = 0.000, Figure 2).
Figure 2. Forest plot showing the prognostic effect of pretreatment elevated platelet count on overall survival of colorectal cancer patients.
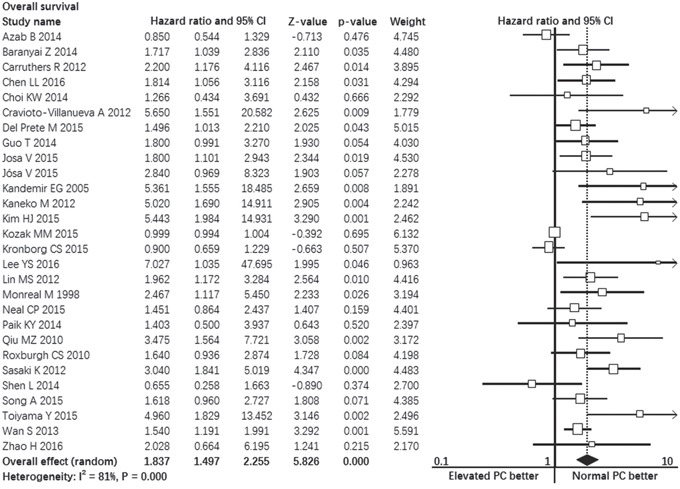
*CI: Confidence interval.
We performed subgroup analyses on confounding factors such as disease stage, cancer type, cut-off values, etc. The results consistently showed that patients with pretreatment elevated platelet count had poorer overall survival compared with normal platelet count in most subgroups: multivariate analysis subgroup (p = 0.000), univariate analysis subgroup (p = 0.000), preoperative subgroup (p = 0.000), metastatic disease subgroup (p = 0.027), stage I-III disease subgroup (p = 0.000), rectal cancer subgroup (p = 0.009), cut-off value ≥ 400 subgroup (p = 0.000), 300 ≤ cut-off value < 400 subgroup (p = 0.000), cut-off value < 300 subgroup (p = 0.043). In colon cancer subgroup, overall survival of patients with pretreatment elevated platelet count had no difference with patients with normal platelet count (p = 0.099). The detailed results of subgroup analyses were summarized in Table 2.
Table 2. Summarized results of meta-analysis.
| Outcomes | Subgroups | Analysis Model | Studies | Heterogeneity | Hazard Ratio | 95% Confidence Interval | P-value | ||
|---|---|---|---|---|---|---|---|---|---|
| P-value | I-square % | ||||||||
| Overall survival | total | random | 28 | 0.000 | 81.006 | 1.837 | 1.497 | 2.255 | 0.000 |
| multivariable | random | 11 | 0.000 | 68.792 | 2.122 | 1.508 | 2.985 | 0.000 | |
| univariable | fixed | 8 | 0.162 | 33.341 | 1.675 | 1.331 | 2.108 | 0.000 | |
| preoperative | random | 20 | 0.000 | 83.380 | 2.015 | 1.547 | 2.625 | 0.000 | |
| metastatic disease | random | 6 | 0.021 | 62.204 | 1.503 | 1.047 | 2.157 | 0.027 | |
| stage I-III disease | random | 11 | 0.000 | 82.555 | 2.330 | 1.461 | 3.715 | 0.000 | |
| rectal cancer | random | 5 | 0.008 | 70.832 | 2.796 | 1.286 | 6.078 | 0.009 | |
| colon cancer | random | 2 | 0.088 | 65.731 | 2.594 | 0.837 | 8.035 | 0.099 | |
| cut-off value ≥ 400 × 109 / L | random | 15 | 0.000 | 77.687 | 1.633 | 1.284 | 2.077 | 0.000 | |
| 300 ≤ cut-off value < 400 × 109 / L | random | 9 | 0.038 | 51.062 | 2.467 | 1.685 | 3.612 | 0.000 | |
| cut-off value < 300 × 109 / L | - | 1 | - | - | 1.496 | 1.013 | 2.210 | 0.043 | |
| Disease-free survival | total | random | 15 | 0.000 | 82.195 | 1.635 | 1.237 | 2.160 | 0.001 |
| multivariable | random | 6 | 0.000 | 90.188 | 2.166 | 1.234 | 3.802 | 0.007 | |
| univariable | random | 9 | 0.008 | 61.329 | 1.377 | 0.992 | 1.909 | 0.056 | |
| preoperative | random | 14 | 0.000 | 83.175 | 1.751 | 1.287 | 2.384 | 0.000 | |
| metastatic disease | - | 1 | - | - | 0.850 | 0.540 | 1.320 | 0.459 | |
| stage I-III disease | random | 8 | 0.000 | 78.468 | 1.697 | 1.154 | 2.495 | 0.007 | |
| rectal cancer | Fixed | 5 | 0.194 | 34.037 | 1.588 | 1.175 | 2.147 | 0.003 | |
| colon cancer | - | 1 | - | - | 4.102 | 1.822 | 9.235 | 0.001 | |
| cut-off value ≥ 400 × 109 / L | random | 6 | 0.000 | 81.695 | 1.589 | 0.989 | 2.555 | 0.056 | |
| 300 ≤ cut-off value < 400 × 109 / L | Fixed | 6 | 0.076 | 49.840 | 2.030 | 1.599 | 2.578 | 0.000 | |
| cut-off value < 300 × 109 / L | - | 1 | - | - | 1.853 | 1.236 | 2.780 | 0.003 | |
Prognostic impact of pretreatment elevated platelet count on disease-free survival
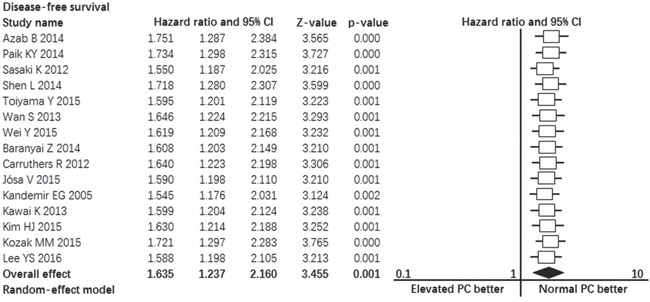
Fifteen studies contributed data to the analyses of disease-free survival. Significant heterogeneity was found among studies (I2 = 82%, p = 0.000, Figure 3). Random-effect model was used. The pooled hazard ratio estimate showed that patients with pretreatment elevated platelet count had poorer disease-free survival compared with normal platelet count (HR = 1.635, 95% confidence interval, 1.237 to 2.160, p = 0.001, Figure 3).
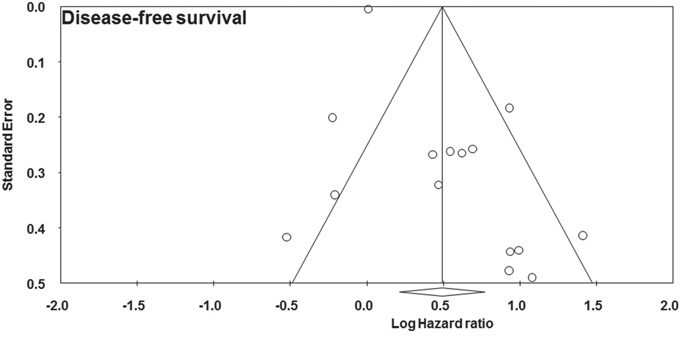
Figure 3. Forest plot showing the prognostic effect of pretreatment elevated platelet count on disease-free survival of colorectal cancer patients.
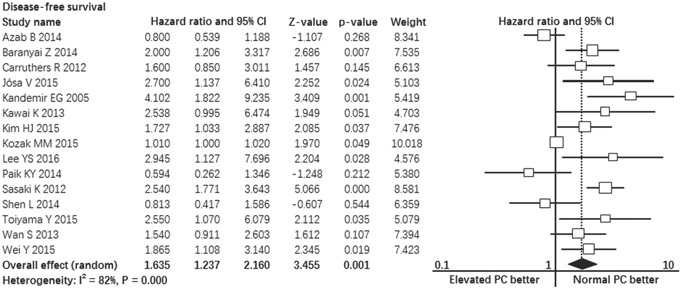
*CI: Confidence interval.
The results of subgroup analyses revealed that colorectal patients with pretreatment elevated platelet count had poorer disease-free survival compared with normal platelet count in the following subgroups: multivariate analysis subgroup (p = 0.007), preoperative subgroup (p = 0.000), stage I-III disease subgroup (p = 0.007), rectal cancer subgroup (p = 0.003), colon cancer subgroup (p = 0.001), 300 ≤ cut-off value < 400 subgroup (p = 0.000), cut-off value < 300 subgroup (p = 0.003). In three subgroups, patients with pretreatment elevated platelet count had similar disease-free survival compared with patients with normal platelet count: univariate analysis subgroup (p = 0.056), cut-off value ≥ 400 subgroup (p = 0.056) and metastatic disease subgroup (all patients received R0 resection of primary and metastasis tumors) (p = 1.320). The detailed results of subgroup analyses were summarized in Table 2.
Publication bias
Visual inspection of the funnel plot for overall survival and disease-free survival outcomes did not show the typically asymmetry associated with publication bias (Figure 4, Figure 5). Evidence of publication bias was also not seen with the Begg's tests of overall survival (p = 0.441) and disease-free survival (p = 1.000).
Figure 4. Funnel plot showing the publication bias of overall survival.
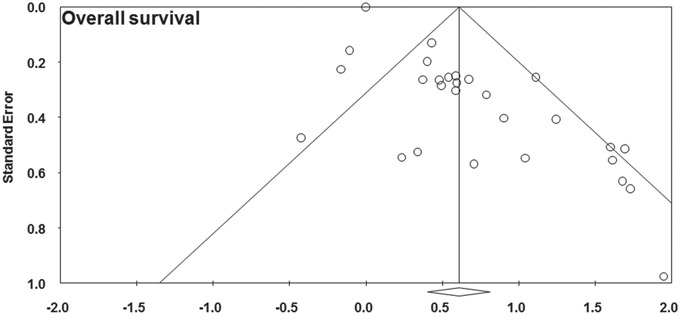
Figure 5. Funnel plot showing the publication bias of disease-free survival.
Sensitivity analyses
The result of Sensitivity analyses demonstrated that no individual study had excessive influence on the stability of the pooled effect of comparisons for overall survival (Figure 6) and disease-free survival (Figure 7). The result of this meta-analysis is robust.
Figure 6. Forest plot showing the sensitivity analyses of overall survival.
*CI: Confidence interval
Figure 7. Forest plot showing the sensitivity analyses of disease-free survival.
*CI: Confidence interval
DISCUSSION
Elevated platelet count or thrombocytosis is observed in patients with various kinds of cancer and reported inversely correlated with survival [24, 32–36]. It was reported that nearly 10% to 30% of patients with colorectal cancer had elevated platelet count before treatment and worse survival than those with normal platelet count [2-5, 7, 9, 21]. In our study, the results demonstrated that elevated platelet count was associated with shorter overall survival and disease-free survival in patients with colorectal cancer. Subgroup analyses demonstrated that the impact of elevated platelet count are consistent in different disease stages, tumor locations and analysis models. The result of our study is robust. This evidence indicated that platelet could be a simple and robust prognostic marker to identify high risk patients. Those patients should be taken into account to receive adjuvant therapy or maybe anti-platelet medications. There have been accumulating evidence that postdiagnosis aspirin therapy can improve overall survival of patients with colorectal cancer in recent years [37].
It is noteworthy that the cut-off values applied in included studies were not unified. Most studies used 400 × 109/L as cut-off value and some studies used 300 × 109/L. The optimal cut-off value, however, was not validated in previous studies. The subgroup analyses reached consistent results among different cut-off value subgroup. The cut-off value ≥ 400 × 109 / L and between 300 and 400 can both distinguished patients well by overall survival and disease-free survival. Only in cut-off value ≥ 400 × 109 / L subgroup, platelet count failed to predict the disease-free survival of patients (p = 0.056, Table 2). Regarding this, it may be reasonable to suggest that the cut-off value between 300 and 400 × 109 / L be applied in further investigation.
The mechanisms of tumor-related elevated platelet count or thrombocytosis remain undetermined. One of the potential hypotheses is that thrombocytosis is usually associated with inflammatory cytokines induced by interactions between tumor and host. Among these cytokines, IL-6, having multiple functions in many physiological conditions, plays a very important role in the formation of thrombocytosis [38]. By stimulating differentiation of megakaryocytes to platelets in the bone marrow, IL-6 induced thrombocytosis in various malignancies [39]. For another explanation of cancer-associated thrombocytosis, tumor can stimulate activation of platelet. As reported in several studies that cancer cells can secrete vascular endothelial growth factor to stimulates megakaryocyte differentiation [40]. For the prognostic association between elevated platelet count and patients' outcomes, there is a most widely accepted hypothesis that activated platelets contribute to the tumor growth, angiogenesis and metastasis by releasing various cytokines with inflammatory, proliferative and angiogenic activity [41–43]. With regard to tumor metastasis, platelets can cover and protect circulating tumor cells from the host's immune system. With these underlying mechanisms, platelets may be a direct or indirect target for cancer therapy.
There are some limitations of this study. First, our analysis is based on low-level evidence retrospective studies, in most of which some important confounders were not well adjusted, such as tumor stage, therapeutic strategy or ratio of colon and rectal cancer. The result of subgroup analysis, however, demonstrated that the negative prognostic significance of thrombocytosis on overall survival and disease-free survival was consistent between groups. Subgroup analysis according to therapeutic strategies was not performed because of insufficient data. Second, the sample size of some included studies were very small. The results of subgroup analyses still confirm the prognostic significance of thrombocytosis. Third, although the platelet count is easy to measure, its utility as a clinical prognostic marker could be affected by some other conditions, such as thrombosis, coronary disease, splenic disease, myeloproliferative disease, blood coagulation disorders, iron deficiency anemia and drugs. Actually, some heterogeneity was unexplainable.
In conclusion, our study demonstrated that the pretreatment elevated platelet count was an independent prognostic factor of overall survival and disease-free survival in colorectal cancer patients. It may make sense that patients with elevated platelet count should receive intensive treatment or anti-platelet therapy. And large-scale prospective studies and a validation study are warranted to confirm its prognostic significance and determine the optimal platelet cut-off value.
MATERIALS AND METHODS
Eligibility criteria
This meta-analysis was performed according to the statement of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [44]. Cohort studies, being published from inception to July 9, 2016, which reported comparisons of overall survival or disease-free survival between colorectal cancer patients with pretreatment elevated platelet count and those patients with pretreatment normal platelet count. The study participants had been pathologically diagnosed colorectal cancer patients.
Search strategy
An electronic search in PubMed, EMBASE and the Cochrane Library were conducted from inception to July 9, 2016. The following key words in combination as medical subject heading terms and text words were used: “colorectal cancer” and “platelet” or “thrombocytosis”. Potentially relevant articles were identified by reading titles and abstracts. The full texts of the relevant articles were read to determine whether they met the inclusion criteria. The references were also searched to identify relevant studies.
Quality assessment
For cohort studies, the 9-star Newcastle-Ottawa Scale was used to assess the risk of bias [45]. This scale is an 8-item instrument that allows for assessment of patient population and selection, study comparability, follow-up, and outcome. Interpretation of the scale is performed by awarding points for high-quality elements. Studies with 5 or more stars were defined as high-quality studies and were included.
Statistical analyses
Data was extracted using a unified form and study information including author name, study year, study area, sample size, hazard ratio of overall survival or disease-free survival were collected. If the hazard ratio was not reported in the original article, we would calculate hazard ratio from reported data according to the methods described by Tierney et al [46]. Statistical heterogeneity among studies was examined using the Cochrane Q test by calculating the I2 value [47]. The I2 value greater than 50% or p value less than 0.05 were considered to represent significant heterogeneity. The pooled hazard ratio and the 95% confidence interval were calculated using the Z test. The pooled hazard ratio and the 95% confidence interval were calculated using the Mantel-Haenszel formula (fixed-effect model) when heterogeneity was not detected (p > 0.05), or using the DerSimonian-Laird formula (random-effect model) when heterogeneity was significant (p < 0.05) [48]. Publication bias was evaluated using the funnel plot and the Begg's test [49]. Influence analyses were conducted to access how robust the pooled estimators were by removing individual studies. An individual study was suspected of excessive influence if the point estimate of its omitted analysis was outside the 95% confidence interval of the combined analysis. Statistical analyses were performed with Comprehensive Meta Analysis professional version 2.2 (Biostat Inc, Englewood NJ, www.meta-analysis.com).
ACKNOWLEDGMENTS AND FUNDING
This research was supported by Provincial Research Project for Health Care of Cadres in Sichuan, China (Grant No. Chuan Gan Yan 2013-802).
Abbreviations
- CI
Confidence interval
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Footnotes
CONFLICTS OF INTEREST
The authors declared no competing financial interest.
Authors' contributions
Conception/Design: Ting Wang, Yu Long. Data analysis and statistical guidance: Yu Long, Qian Gao, Chengya Zhou. Manuscript writing: Ting Wang, Yu Long. Final approval of the manuscript: Ting Wang, Yu Long, Chengya Zhou, Qian Gao.
REFERENCES
- 1.Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. doi: 10.3322/caac.21262. [DOI] [PubMed] [Google Scholar]
- 2.Baranyai Z, Krzystanek M, Josa V, Dede K, Agoston E, Szasz AM, Sinko D, Szarvas V, Salamon F, Eklund AC, Szallasi Z, Jakab F. The comparison of thrombocytosis and platelet-lymphocyte ratio as potential prognostic markers in colorectal cancer. Thromb Haemost. 2014;111:483–90. doi: 10.1160/TH13-08-0632. [DOI] [PubMed] [Google Scholar]
- 3.Chen LL, Zhang L, Li YL, Li XL, Liu WH, Yan J, Yang YF. [Association of preoperative platelet count with the prognosis of patients with colorectal cancer]. [Article in Chinese] Nan Fang Yi Ke Da Xue Xue Bao. 2016;36:482–7. [PubMed] [Google Scholar]
- 4.Cravioto-Villanueva A, Luna-Perez P, Gutierrez-de la Barrera M, Martinez-Gomez H, Maffuz A, Rojas-Garcia P, Perez-Alvarez C, Rodriguez-Ramirez S, Rodriguez-Antezana E, Ramirez-Ramirez L. Thrombocytosis as a predictor of distant recurrence in patients with rectal cancer. Arch Med Res. 2012;43:305–11. doi: 10.1016/j.arcmed.2012.06.008. [DOI] [PubMed] [Google Scholar]
- 5.Guo T, Krzystanek M, Szallasi Z, Szallasi A. Thrombocytosis portends adverse prognostic significance in patients with stage II colorectal carcinoma. F1000Res. 2014;3:180. doi: 10.12688/f1000research.4856.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Josa V, Krzystanek M, Vass T, Lang T, Juhasz V, Szilagyi K, Tihanyi B, Harsanyi L, Szallasi Z, Salamon F, Baranyai Z. Thrombocytosis of Liver Metastasis from Colorectal Cancer as Predictive Factor. Pathol Oncol Res. 2015;21:991–7. doi: 10.1007/s12253-015-9925-8. [DOI] [PubMed] [Google Scholar]
- 7.Kandemir EG, Mayadagli A, Karagoz B, Bilgi O, Turken O, Yaylaci M. Prognostic significance of thrombocytosis in node-negative colon cancer. J Int Med Res. 2005;33:228–35. doi: 10.1177/147323000503300211. [DOI] [PubMed] [Google Scholar]
- 8.Kawai K, Kitayama J, Tsuno NH, Sunami E, Watanabe T. Thrombocytosis before pre-operative chemoradiotherapy predicts poor response and shorter local recurrence-free survival in rectal cancer. Int J Colorectal Dis. 2013;28:527–35. doi: 10.1007/s00384-012-1594-4. [DOI] [PubMed] [Google Scholar]
- 9.Kim HJ, Choi GS, Park JS, Park S, Kawai K, Watanabe T. Clinical significance of thrombocytosis before preoperative chemoradiotherapy in rectal cancer: predicting pathologic tumor response and oncologic outcome. Ann Surg Oncol. 2015;22:513–9. doi: 10.1245/s10434-014-3988-8. [DOI] [PubMed] [Google Scholar]
- 10.Wei Y, Liang Z, Hong C, Luo D, Cai Z, Guan H, Zeng Z, Yang Z, Luo P, Tan Z. [Impact of platelet count on prognosis of stage II-III colorectal cancer receiving adjuvant chemotherapy]. [Article in Chinese] Zhonghua Wei Chang Wai Ke Za Zhi. 2015;18:1261–4. [PubMed] [Google Scholar]
- 11.Azab B, Mohammad F, Shah N, Vonfrolio S, Lu W, Kedia S, Bloom SW. The value of the pretreatment neutrophil lymphocyte ratio vs. platelet lymphocyte ratio in predicting the long-term survival in colorectal cancer. Cancer Biomark. 2014;14:303–12. doi: 10.3233/CBM-140416. [DOI] [PubMed] [Google Scholar]
- 12.Choi KW, Hong SW, Chang YG, Lee WY, Lee B, Paik IW, Lee H. Inflammation-based score (Glasgow prognostic score) as an independent prognostic factor in colorectal cancer patients. Ann Surg Treat Res. 2014;86:309–13. doi: 10.4174/astr.2014.86.6.309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kronborg CS, Jensen AR. Prognostic factors for overall survival in metastatic colorectal cancer using a stop-and-go FLIRI-based treatment strategy. Int J Colorectal Dis. 2015;30:1059–65. doi: 10.1007/s00384-015-2264-0. [DOI] [PubMed] [Google Scholar]
- 14.Shen L, Zhang H, Liang L, Li G, Fan M, Wu Y, Zhu J, Zhang Z. Baseline neutrophil-lymphocyte ratio (>/=2.8) as a prognostic factor for patients with locally advanced rectal cancer undergoing neoadjuvant chemoradiation. Radiat Oncol. 2014;9:295. doi: 10.1186/s13014-014-0295-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Song A, Eo W, Lee S. Comparison of selected inflammation-based prognostic markers in relapsed or refractory metastatic colorectal cancer patients. World J Gastroenterol. 2015;21:12410–20. doi: 10.3748/wjg.v21.i43.12410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhao H, Wang Y, Yu J, Wei F, Cao S, Zhang X, Dong N, Li H, Ren X. Autologous Cytokine-Induced Killer Cells Improves Overall Survival of Metastatic Colorectal Cancer Patients: Results From a Phase II Clinical Trial. Clin Colorectal Cancer. 2016 doi: 10.1016/j.clcc.2016.02.005. [DOI] [PubMed] [Google Scholar]
- 17.Carruthers R, Tho LM, Brown J, Kakumanu S, McCartney E, McDonald AC. Systemic inflammatory response is a predictor of outcome in patients undergoing preoperative chemoradiation for locally advanced rectal cancer. Colorectal Dis. 2012;14:e701–7. doi: 10.1111/j.1463-1318.2012.03147.x. [DOI] [PubMed] [Google Scholar]
- 18.Del Prete M, Giampieri R, Loupakis F, Prochilo T, Salvatore L, Faloppi L, Bianconi M, Bittoni A, Aprile G, Zaniboni A, Falcone A, Scartozzi M, Cascinu S. Prognostic clinical factors in pretreated colorectal cancer patients receiving regorafenib: implications for clinical management. Oncotarget. 2015;6:33982–92. doi: 10.18632/oncotarget.5053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Josa V, Krzystanek M, Eklund AC, Salamon F, Zarand A, Szallasi Z, Baranyai Z. Relationship of postoperative thrombocytosis and survival of patients with colorectal cancer. Int J Surg. 2015;18:1–6. doi: 10.1016/j.ijsu.2015.03.005. [DOI] [PubMed] [Google Scholar]
- 20.Kaneko M, Nozawa H, Sasaki K, Hongo K, Hiyoshi M, Tada N, Murono K, Nirei T, Kawai K, Sunami E, Tsuno NH, Kitayama J. Elevated neutrophil to lymphocyte ratio predicts poor prognosis in advanced colorectal cancer patients receiving oxaliplatin-based chemotherapy. Oncology. 2012;82:261–8. doi: 10.1159/000337228. [DOI] [PubMed] [Google Scholar]
- 21.Kozak MM, von Eyben R, Pai JS, Anderson EM, Welton ML, Shelton AA, Kin C, Koong AC, Chang DT. The Prognostic Significance of Pretreatment Hematologic Parameters in Patients Undergoing Resection for Colorectal Cancer. Am J Clin Oncol. 2015 doi: 10.1097/COC.0000000000000183. [DOI] [PubMed] [Google Scholar]
- 22.Lee YS, Suh KW, Oh SY. Preoperative thrombocytosis predicts prognosis in stage II colorectal cancer patients. Ann Surg Treat Res. 2016;90:322–7. doi: 10.4174/astr.2016.90.6.322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lin MS, Huang JX, Zhu J, Shen HZ. Elevation of platelet count in patients with colorectal cancer predicts tendency to metastases and poor prognosis. Hepatogastroenterology. 2012;59:1687–90. doi: 10.5754/hge12277. [DOI] [PubMed] [Google Scholar]
- 24.Monreal M, Fernandez-Llamazares J, Pinol M, Julian JF, Broggi M, Escola D, Abad A. Platelet count and survival in patients with colorectal cancer--a preliminary study. Thromb Haemost. 1998;79:916–8. [PubMed] [Google Scholar]
- 25.Neal CP, Cairns V, Jones MJ, Masood MM, Nana GR, Mann CD, Garcea G, Dennison AR. Prognostic performance of inflammation-based prognostic indices in patients with resectable colorectal liver metastases. Med Oncol. 2015;32:144. doi: 10.1007/s12032-015-0590-2. [DOI] [PubMed] [Google Scholar]
- 26.Paik KY, Lee IK, Lee YS, Sung NY, Kwon TS. Clinical implications of systemic inflammatory response markers as independent prognostic factors in colorectal cancer patients. Cancer Res Treat. 2014;46:65–73. doi: 10.4143/crt.2014.46.1.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Qiu MZ, Yuan ZY, Luo HY, Ruan DY, Wang ZQ, Wang FH, Li YH, Xu RH. Impact of pretreatment hematologic profile on survival of colorectal cancer patients. Tumour Biol. 2010;31:255–60. doi: 10.1007/s13277-010-0024-x. [DOI] [PubMed] [Google Scholar]
- 28.Roxburgh CS, Wallace AM, Guthrie GK, Horgan PG, McMillan DC. Comparison of the prognostic value of tumour- and patient-related factors in patients undergoing potentially curative surgery for colon cancer. Colorectal Dis. 2010;12:987–94. doi: 10.1111/j.1463-1318.2009.01961.x. [DOI] [PubMed] [Google Scholar]
- 29.Sasaki K, Kawai K, Tsuno NH, Sunami E, Kitayama J. Impact of preoperative thrombocytosis on the survival of patients with primary colorectal cancer. World J Surg. 2012;36:192–200. doi: 10.1007/s00268-011-1329-7. [DOI] [PubMed] [Google Scholar]
- 30.Toiyama Y, Inoue Y, Kawamura M, Kawamoto A, Okugawa Y, Hiro J, Saigusa S, Tanaka K, Mohri Y, Kusunoki M. Elevated platelet count as predictor of recurrence in rectal cancer patients undergoing preoperative chemoradiotherapy followed by surgery. Int Surg. 2015;100:199–207. doi: 10.9738/INTSURG-D-13-00178.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wan S, Lai Y, Myers RE, Li B, Hyslop T, London J, Chatterjee D, Palazzo JP, Burkart AL, Zhang K, Xing J, Yang H. Preoperative platelet count associates with survival and distant metastasis in surgically resected colorectal cancer patients. J Gastrointest Cancer. 2013;44:293–304. doi: 10.1007/s12029-013-9491-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Zeimet AG, Marth C, Muller-Holzner E, Daxenbichler G, Dapunt O. Significance of thrombocytosis in patients with epithelial ovarian cancer. Am J Obstet Gynecol. 1994;170:549–54. doi: 10.1016/s0002-9378(94)70225-x. [DOI] [PubMed] [Google Scholar]
- 33.Ikeda M, Furukawa H, Imamura H, Shimizu J, Ishida H, Masutani S, Tatsuta M, Satomi T. Poor prognosis associated with thrombocytosis in patients with gastric cancer. Ann Surg Oncol. 2002;9:287–91. doi: 10.1007/BF02573067. [DOI] [PubMed] [Google Scholar]
- 34.Gao J, Zhang HY, Xia YF. Increased platelet count is an indicator of metastasis in patients with nasopharyngeal carcinoma. Tumour Biol. 2013;34:39–45. doi: 10.1007/s13277-012-0508-y. [DOI] [PubMed] [Google Scholar]
- 35.Silvis SE, Turkbas N, Doscherholmen A. Thrombocytosis in patients with lung cancer. JAMA. 1970;211:1852–3. [PubMed] [Google Scholar]
- 36.Symbas NP, Townsend MF, El-Galley R, Keane TE, Graham SD, Petros JA. Poor prognosis associated with thrombocytosis in patients with renal cell carcinoma. BJU Int. 2000;86:203–7. doi: 10.1046/j.1464-410x.2000.00792.x. [DOI] [PubMed] [Google Scholar]
- 37.Li P, Wu H, Zhang H, Shi Y, Xu J, Ye Y, Xia D, Yang J, Cai J, Wu Y. Aspirin use after diagnosis but not prediagnosis improves established colorectal cancer survival: a meta-analysis. Gut. 2015;64:1419–25. doi: 10.1136/gutjnl-2014-308260. [DOI] [PubMed] [Google Scholar]
- 38.Sierko E, Wojtukiewicz MZ. Platelets and angiogenesis in malignancy. Semin Thromb Hemost. 2004;30:95–108. doi: 10.1055/s-2004-822974. [DOI] [PubMed] [Google Scholar]
- 39.Imai T, Koike K, Kubo T, Kikuchi T, Amano Y, Takagi M, Okumura N, Nakahata T. Interleukin-6 supports human megakaryocytic proliferation and differentiation in vitro. Blood. 1991;78:1969–74. [PubMed] [Google Scholar]
- 40.Troxler M, Dickinson K, Homer-Vanniasinkam S. Platelet function and antiplatelet therapy. Br J Surg. 2007;94:674–82. doi: 10.1002/bjs.5852. [DOI] [PubMed] [Google Scholar]
- 41.Dineen SP, Roland CL, Toombs JE, Kelher M, Silliman CC, Brekken RA, Barnett CC., Jr The acellular fraction of stored platelets promotes tumor cell invasion. J Surg Res. 2009;153:132–7. doi: 10.1016/j.jss.2008.04.013. [DOI] [PubMed] [Google Scholar]
- 42.Kut C, Mac Gabhann F, Popel AS. Where is VEGF in the body? A meta-analysis of VEGF distribution in cancer. Br J Cancer. 2007;97:978–85. doi: 10.1038/sj.bjc.6603923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Sledge GW., Jr Vascular endothelial growth factor in breast cancer: biologic and therapeutic aspects. Semin Oncol. 2002;29:104–10. doi: 10.1053/sonc.2002.34062. [DOI] [PubMed] [Google Scholar]
- 44.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25:603–5. doi: 10.1007/s10654-010-9491-z. [DOI] [PubMed] [Google Scholar]
- 46.Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8:16. doi: 10.1186/1745-6215-8-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 48.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 49.Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–101. [PubMed] [Google Scholar]