

Abstract
Background:
Injuries and illnesses for professional tennis athletes disrupt training, competition, and progression in the sport and represent a major reason for athlete withdrawal or retirement from a tournament. Few descriptive epidemiological studies have focused on these trends in elite tennis athletes.
Purpose:
To examine the causes of professional tennis player withdrawal or retirement from United States Tennis Association (USTA) Pro Circuit tournaments during 2013.
Study Design:
Descriptive epidemiology study.
Level of Evidence:
Level 4.
Methods:
Tournament records from the 2013 USTA Pro Circuit season were retrospectively reviewed for incidences of injury and illness that resulted in athlete withdrawal from the tournament. Data were reported as incidence rates per 1000 match exposures and rate ratios.
Results:
There were 70 medical conditions over the course of 27 competitions (20,988 match exposures), for an overall incidence rate of 3.34 per 1000 match exposures. Women were more likely to injure themselves on clay courts compared with hard courts (rate ratio, 4.67; 95% confidence interval [CI], 1.41-19.85) and in the first half of the season compared with the second half (rate ratio, 3.95; 95% CI, 1.13-21.17). Men had a higher injury rate than women (rate ratio, 1.88; 95% CI, 1.17-3.63), and muscle-/tendon-related injuries were 6 times more likely than all other injuries (95% CI, 2.81-14.69).
Conclusion:
Women were more likely to experience an injury when playing on clay court surfaces, and they also experienced more injuries during the first half of the season. Injury rates for men often peaked during the months that players could qualify for Grand Slam competitions. There was a predominance of injuries in men compared with women.
Keywords: tennis, sports injuries, professional athletes, epidemiology
The United States Tennis Association (USTA) Pro Circuit represents one of the largest tennis tours in the world, with over 1000 athletes competing annually and 89 tournaments held in 2013 alone.1,3 For United States–based athletes, it provides a route for professional players to improve their ranking and qualify for major tennis tournaments while competing domestically.
Injuries or illnesses for professional tennis players disrupt competition, training, and progression in the sport.19,28 Retrospective studies have demonstrated that professional tennis player retirements and withdrawals from competitions have increased in number and frequency over the past decade.5,12,18 Few epidemiological studies have followed professional tennis players to better understand these trends.12,20,25,27 Previous studies have stated that acute injuries are more common in the lower extremity and chronic injuries occur more often in the upper extremity and trunk.25 Additional factors have been suggested to affect injury rates, such as the type of court surface15-17 or time of the year18; however, these factors have yet to be validated. Early research in these areas was limited by the lack of procedural conformity regarding the classification and analysis of medical conditions, which made it difficult to compare studies.4,18 In 2009, an official tennis-specific consensus statement was developed to provide a framework for more objective documentation and analysis of medical conditions.19 A growing number of articles have begun to use this consensus statement, but literature exploring elite-level injuries with this guide remains minimal.12,18,24,25
The purpose of the current study was to examine all the singles and doubles matches from the 2013 USTA Pro Circuit season for injury and illness trends that caused professional tennis players to either withdraw or retire from a match or tournament.
Methods
This study was approved by the Institutional Review Board of the Icahn School of Medicine at Mount Sinai in New York City, New York.
Data Collection
Injury and illness data were collected from 2013 USTA Pro Circuit tournament records, which included men’s and women’s singles and doubles matches during qualifying or main draw weeks of a tournament. Cases were only included if they required an evaluation by a tournament physician (or sports medicine therapist for male athletes) that resulted in either the athlete’s withdrawal from match play or retirement from the tournament. A withdrawal was defined as when a player withdrew from a tournament prior to the start of the competition, and a retirement was defined as when a player was unable to continue playing a match or resume a suspended match after the match had started. Additionally, only cases that occurred while at the tournament, whether during training or match play, were included.
The number of matches per tournament was determined by reviewing the draw sheet of each tournament found on the International Tennis Federation website.26 Following the tennis-specific consensus statement developed by Pluim et al,19 match exposures (MEs) were calculated for each tournament. As defined in the consensus statement, an ME is “play (including on-court warm-up) between competing players.”19 Thus, final MEs were calculated by using 2 MEs for a singles match (2 players per match) and 4 MEs for a doubles match (4 players per match). Court type and MEs were found on the USTA website.1,3
Injury Classification
Data were classified following the consensus statement.19 Using this system, medical conditions were categorized by manner of onset (acute or gradual) as well as by type and location. Injury types included bone, joint (nonbone) and ligament, muscle and tendon, skin, nervous system, or other. Injury locations included 5 main regions: head/neck, upper extremities, lower extremities, trunk, and unspecified. Illnesses were classified according to the organ system affected (ie, cardiovascular, respiratory, etc) or manner of contagion (ie, allergic, environmental, etc). Additionally, the term “medical condition” was adopted as a term that encompassed both injuries and illnesses, following the methods of previous studies.12,19
Data Analysis
Data are reported as injury rates per 1000 MEs with their corresponding 95% confidence intervals (CIs). This method of reporting injury rates has been used in previous research using the consensus statement.8,18,25,27 Additionally, injury rate ratios with their corresponding 95% CIs are also reported, as described by Knowles et al.9 Differences between injury rates were calculated and assessed for statistical significance using accepted statistical methods.23 All statistical analyses were performed using MedCalc Statistical Software (version 15.10.0). For analyzing the differences between injury rates, statistical significance was set at P < 0.05, and for analyzing injury rate ratios, statistical significance was defined as when the lower limit of the 95% CI was greater than 1.00.
To determine whether injury rates occur more frequently at specific points throughout the season, the data were analyzed by individual months as well as by 6-month blocks that delineated the first half and second half of the season. The first half of the season was measured from January through June, while the second half represented July through December. Injury rates during these time points were calculated using the number of injuries and the number of MEs either within a given month or the first or second half of the season.
Results
In 2013, the USTA held 89 Pro Circuit tournaments—47 men’s tournaments and 42 women’s tournaments—totaling 20,988 MEs. Of those, there were 27 competitions (18 men’s and 9 women’s) in which athletes withdrew or retired because of injury or illness. A total of 70 medical condition cases resulting in retirement or withdrawal were identified. The average age of injured athletes was 24.4 ± 4.3 and 22.3 ± 3.9 years for men and women, respectively. Injuries accounted for 80% of overall medical conditions and occurred at a rate 4 times higher than that of illnesses (95% CI, 2.20-7.78). Muscle/tendon injuries overall occurred at a rate 6 times higher than all other injury types combined (95% CI, 2.81-14.69) (Table 1).
Table 1.
Descriptive and incidence data for injury classification, type, and location for men, women, and overall in the USTA during the year 2013 a
| Men (11,972 MEs) |
Women (9,016 MEs) |
Overall (20,988 MEs) |
IRR | 95% CI | Comparison | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Cases | IR | 95% CI | Total Cases | IR | 95% CI | Total Cases | IR | 95% CI | ||||
| Total cases | 51 | 4.26 b | 3.09 to 5.43 | 19 | 2.11 | 1.16 to 3.05 | 70 | 3.34 | 2.55 to 4.12 | 2.02 c | 1.17 to 3.63 | M vs W |
| Type of departure | ||||||||||||
| Withdrawal | 20 | 1.67 b | 0.94 to 2.40 | 4 | 0.44 | 0.01 to 0.88 | 24 | 1.14 | 0.69 to 1.60 | 3.77 c | 1.26 to 15.15 | M vs W |
| Retirement | 31 | 2.59 | 1.68 to 3.50 | 15 | 1.66 | 0.82 to 2.51 | 46 | 2.19 | 1.56 to 2.83 | 1.56 | 0.82 to 3.10 | M vs W |
| Reason for departure | ||||||||||||
| Injury | 40 | 3.34 b | 2.31 to 4.28 | 16 | 1.77 | 0.91 to 2.64 | 56 | 2.67 | 1.97 to 3.37 | 1.88 c | 1.03 to 3.60 | M vs W |
| Illness | 11 | 0.92 | 0.38 to 1.46 | 3 | 0.33 | −0.04 to 0.71 | 14 | 0.67 | 0.32 to 1.02 | 2.76 | 0.73 to 15.41 | M vs W |
| Type of medical condition | ||||||||||||
| Acute | 34 | 2.84 | 1.89 to 3.79 | 15 | 1.66 | 0.82 to 2.51 | 49 | 2.33 | 1.68 to 2.99 | 1.71 | 0.91 to 3.37 | M vs W |
| Gradual | 16 | 1.34 b | 0.68 to 1.99 | 4 | 0.44 | 0.01 to 0.88 | 20 | 0.95 | 0.54 to 1.37 | 3.01 | 0.97 to 12.38 | M vs W |
| No data | 1 | 0.08 | −0.08 to 0.25 | 0 | 0.00 | 0.00 to 0.00 | 1 | 0.05 | −0.05 to 0.14 | n/a | n/a | |
| Injury location | ||||||||||||
| Head/neck | 2 | 0.17 | −0.06 to 0.40 | 0 | 0.00 | 0.00 to 0.00 | 2 | 0.10 | −0.04 to 0.23 | n/a | n/a | |
| Upper extremity | 10 | 0.84 | 0.32 to 1.35 | 4 | 0.44 | 0.01 to 0.88 | 14 | 0.67 | 0.32 to 1.02 | 1.88 | 0.54 to 8.22 | M vs W |
| Lower extremity | 19 | 1.59 b | 0.87 to 2.30 | 5 | 0.55 | 0.07 to 1.04 | 24 | 1.14 | 0.69 to 1.60 | 2.86 c | 1.03 to 9.81 | M vs W |
| Trunk | 9 | 0.75 | 0.26 to 1.24 | 7 | 0.78 | 0.20 to 1.35 | 16 | 0.76 | 0.39 to 1.14 | 1.03 | 0.33 to 3.12 | W vs M |
| Injury type | ||||||||||||
| Bone | 0 | 0.00 | 0.00 to 0.00 | 3 | 0.33 | −0.04 to 0.71 | 3 | 0.14 | −0.02 to 0.30 | n/a | n/a | |
| Joint/ligament | 3 | 0.25 | −0.03 to 0.53 | 1 | 0.11 | −0.11 to 0.33 | 4 | 0.19 | 0.00 to 0.38 | 2.26 | 0.18 to 118.6 | M vs W |
| M/T | 36 | 3.01 b | 2.02 to 3.99 | 12 | 1.33 | 0.58 to 2.08 | 48 | 2.29 | 1.64 to 2.93 | 2.26 c | 1.15 to 4.77 | M vs W |
| Skin | 0 | 0.00 | 0.00 to 0.00 | 0 | 0.00 | 0.00 to 0.00 | 0 | 0.00 | 0.00 to 0.00 | n/a | n/a | |
| CNS/PNS | 0 | 0.00 | 0.00 to 0.00 | 0 | 0.00 | 0.00 to 0.00 | 0 | 0.00 | 0.00 to 0.00 | n/a | n/a | |
| Other | 1 | 0.08 | −0.08 to 0.25 | 0 | 0.00 | 0.00 to 0.00 | 1 | 0.05 | −0.05 to 0.14 | n/a | n/a | |
| All other injury typesd | 4 | 0.33 | 0.01 to 0.66 | 4 | 0.44 | 0.01 to 0.88 | 8 | 0.38 | 0.12 to 0.65 | 6.00 c | 2.81 to 14.69 | M/T vs all other injury types |
CNS/PNS, central nervous system/peripheral nervous system; IR, injury rate per 1000 MEs; IRR, injury rate ratio; M, men; MEs, match exposures; M/T, muscle/tendon; n/a, not applicable; USTA, United States Tennis Association; W, women.
Comparison column describes the 2 variables being compared: first variable as numerator and also having a higher IR than the second variable. Medical conditions include both injuries and illnesses.
Significant difference compared with women (P < 0.05).
Significant rate ratio (95% CI >1.00).
Additional category added to the original table.
Gender Differences
Men had over twice the overall rate of injury compared with women (P < 0.05) and they also had over 3 times the injury rate that resulted in withdrawal from a match (P < 0.05) (Table 1). Men were also more likely than women to leave a match because of injury (P < 0.05), had nearly 3 times the rate of lower limb injuries (P < 0.05), and had over twice the injury rate of muscles/tendons (P < 0.05) compared with women (Table 1).
Acute Versus Gradual-Onset Medical Conditions
Acute medical conditions occurred at a rate over twice that of gradual-onset medical conditions (95% CI, 1.43-4.35), and caused retirement from tournaments at a rate 3 times that of gradual-onset medical conditions (95% CI, 1.53-6.76) (Table 2). Acute injuries had 3 times the rate of occurrence in the lower limb compared with gradual-onset injuries (P < 0.05) (Table 2) and had twice the rate of injury to muscles/tendons compared with gradual-onset injuries (P < 0.05) (Table 2). The only instance in which gradual-onset injuries had a significantly higher rate than acute injuries was with respect to recurrent injuries, as defined by a medical condition of the same type and at the same site linked to an index medical condition and which occurs after a player’s return to full participation from the index medical condition,19 where it was over 3 times as likely (P < 0.05) (Table 2).
Table 2.
Descriptive and incidence data for injury classification, type, and location for acute and gradual-onset injuries in the USTA during the year 2013
| Acute (20,988 MEs) |
Gradual-Onset (20,988 MEs) |
IRR | 95% CI | Comparison | |||||
|---|---|---|---|---|---|---|---|---|---|
| Total Cases | IR | 95% CI | Total Cases | IR | 95% CI | ||||
| Total cases a | 49 | 2.33 b | 1.68 to 2.99 | 20 | 0.95 | 0.54 to 1.37 | 2.45 c | 1.43 to 4.35 | Acute vs gradual |
| Type of departure | |||||||||
| Withdrawal | 15 | 0.71 | 0.35 to 1.08 | 9 | 0.43 | 0.15 to 0.71 | 1.67 | 0.68 to 4.32 | Acute vs gradual |
| Retirement | 34 | 1.62 b | 1.08 to 2.16 | 11 | 0.52 | 0.21 to 0.83 | 3.09 c | 1.53 to 6.76 | Acute vs gradual |
| Reason for departure | |||||||||
| Injury | 36 | 1.72 b | 1.15 to 2.28 | 19 | 0.91 | 0.50 to 1.31 | 1.89 c | 1.06 to 3.50 | Acute vs gradual |
| Illness | 13 | 0.62 b | 0.28 to 0.96 | 1 | 0.05 | −0.05 to 0.14 | 13.00 c | 1.95 to 552.47 | Acute vs gradual |
| Recurrence | |||||||||
| Yes | 4 | 0.19 | 0.00 to 0.38 | 13d | 0.62 | 0.28 to 0.96 | 3.25 c | 1.004 to 13.68 | Gradual vs acute |
| No | 45 | 2.14 b | 1.52 to 2.77 | 7 | 0.33 | 0.09 to 0.58 | 6.43 c | 2.88 to 16.90 | Acute vs gradual |
| Injury location | |||||||||
| Head/neck | 2 | 0.10 | −0.04 to 0.23 | 0 | 0.00 | 0.00 to 0.00 | n/a | n/a | |
| Upper extremity | 5 | 0.24 | 0.03 to 0.45 | 8 | 0.38 | 0.12 to 0.65 | 1.60 | 0.46 to 6.22 | Gradual vs acute |
| Lower extremity | 18 | 0.86 b | 0.46 to 1.25 | 6 | 0.29 | 0.06 to 0.51 | 3.00 c | 1.14 to 9.23 | Acute vs gradual |
| Trunk | 11 | 0.52 | 0.21 to 0.83 | 5 | 0.24 | 0.03 to 0.45 | 2.20 | 0.70 to 8.08 | Acute vs gradual |
| Injury type | |||||||||
| Bone | 1 | 0.05 | −0.05 to 0.14 | 2 | 0.10 | −0.04 to 0.23 | 2.00 | 0.10 to 117.99 | Gradual vs acute |
| Joint/ligament | 2 | 0.10 | −0.04 to 0.23 | 2 | 0.10 | −0.04 to 0.23 | 1.00 | n/a | |
| Muscle/tendon | 32 | 1.52 b | 1.00 to 2.05 | 15 | 0.71 | 0.35 to 1.08 | 2.13 c | 1.12 to 4.24 | Acute vs gradual |
| Skin | 0 | 0.00 | 0.00 to 0.00 | 0 | 0.00 | 0.00 to 0.00 | n/a | n/a | |
| CNS/PNS | 0 | 0.00 | 0.00 to 0.00 | 0 | 0.00 | 0.00 to 0.00 | n/a | n/a | |
| Other | 1 | 0.05 | 0.28 to 0.96 | 0 | 0.00 | 0.00 to 0.00 | n/a | n/a | |
CNS/PNS, central nervous system/peripheral nervous system; IR, injury rate per 1000 MEs; IRR, injury rate ratio; MEs, match exposures; n/a, not applicable; USTA, United States Tennis Association.
Onset was not specified for 1 case.
Significant difference compared with gradual-onset (P < 0.05).
Significant rate ratio (95% CI >1.00).
Significant difference compared with acute (P < 0.05).
Court Types
Across the entire season, all tournaments were played on either hard or clay courts. On hard courts, men were 4 times more likely to injure themselves compared with women (95% CI, 1.57-18.65) (Table 3). When comparing the 2 court surfaces, women were more than 4 times as likely to injure themselves on clay courts compared with hard courts (95% CI, 1.41-19.85) (Table 3).
Table 3.
Descriptive and incidence data for court type and time of year for men, women, and overall in the USTA during the year 2013 a
| Men (11,972 MEs) | Women (9,016 MEs) | Overall (20,988 MEs) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clay/hard court MEs | 5,782/6,190 | 3,528/5,488 | 9,310/11,678 | |||||||||
| Jan-Jun/Jul-Dec MEs | 5,982/5,990 | 5,178/3,838 | 11,160/9,828 | |||||||||
| Total Cases | IR | 95% CI | Total Cases | IR | 95% CI | Total Cases | IR | 95% CI | IRR | 95% CI | Comparison | |
| Court type (injuries only) | ||||||||||||
| Clay | 19 | 3.29 | 1.81 to 6.00 | 12 | 3.4 | 1.48 to 6.34 | 31 | 3.33 | 2.16 to 5.89 | 1.04 | 0.46 to 2.25 | M vs W |
| Hard | 21 | 3.39 b | 1.84 to 6.15 | 4 | 0.73 | −0.38 to 3.26 | 25 | 2.14 | 1.09 to 4.64 | 4.65 c | 1.57 to 18.65 | M vs W |
| 4.67 c | 1.41 to 19.85 | Clay vs hard (women only) | ||||||||||
| Time of year (medical conditions) d | ||||||||||||
| Jan-Jun | 20 | 3.34 | 1.88 to 4.81 | 16 | 3.09 | 1.58 to 4.60 | 36 | 3.23 | 2.17 to 4.28 | 1.08 | 0.53 to 2.23 | M vs W |
| Jul-Dec | 30 | 5.01 b | 3.22 to 6.80 | 3 | 0.78 | −0.10 to 1.67 | 33 | 3.36 | 2.21 to 4.50 | 6.41 c | 2.00 to 32.81 | M vs W |
| 3.95 c | 1.13 to 21.17 | Jan-Jun v Jul-Dec (women) | ||||||||||
IR, injury rate per 1000 MEs; IRR, injury rate ratio; M, men; MEs, match exposures; USTA, United States Tennis Association; W, women.
Comparison column describes the 2 variables being compared: first variable as numerator and also having a higher IR than the second variable. Medical conditions include both injuries and illnesses.
Significant difference compared with women (P < 0.05).
Significant rate ratio (95% CI >1.00).
Date of injury missing for 1 of the men’s injuries.
Time of Year
Women were nearly 4 times more likely to sustain an injury in the first half of the season compared with the second half (95% CI, 1.13-21.17) (Table 3). Conversely, men had over 6 times the injury rate during the second half of the year compared with women (95% CI, 2.00-32.81) (Table 3). Injury rates and number of MEs per month for both men and women can be seen in Figure 1. The shaded areas in this figure represent the time period during which players may qualify to enter 1 of the 4 major Grand Slam competitions, which occurs between 28 and 42 days prior to the first Monday of the competition.2
Figure 1.
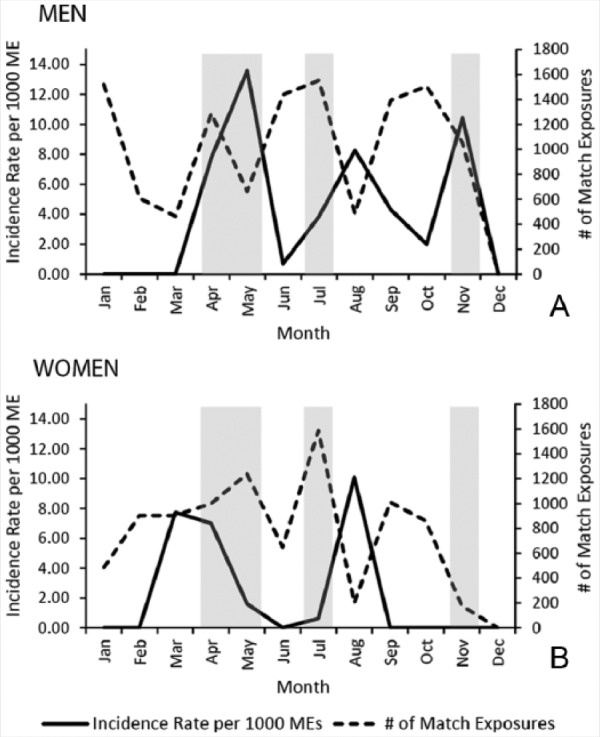
Incidence rate per 1000 match exposures (MEs) of injuries and illnesses as well as the number of match exposures per month for men (A) and women (B). Shaded areas represent the time periods during which players may enter 1 of the 4 Grand Slam competitions, either through the main draw (42 days prior to the first Monday of the competition) or by competing in a qualification tournament (28 days prior to the first Monday of the competition).
Discussion
Previous research has focused mainly on injuries and illnesses that occurred either at a single competition over several years or only included singles matches, which limits the generalizability of the data and prohibits a deeper understanding of injury trends among professional tennis athletes reported in some studies.12,17,25,27 Extensive research has been devoted to injuries in recreational or youth tennis athletes, but because of the significant differences in play time, support, and routines, the extrapolation of findings from these previous studies to professional players is limited.6,8,11,20,21
This study yielded results consistent with various injury trends identified in prior research that has utilized the consensus statement. For example, injuries, as opposed to illnesses, accounted for 80% of all medical conditions in this study, similar to a previous finding of 78%.18 Several inconsistencies with recent studies, however, were also identified, such as the finding that the overall injury rate in men was nearly twice that of women. A study of the injury trends at the US Open between 1994 and 2009 by Sell et al25 also found higher injury rates in men compared with women; however, a study utilizing data from the Association of Tennis Professionals and the Women’s Tennis Association between the years 2001 and 2012 by Okholm Kryger et al18 found that women had higher injury rates compared with men. Thus, while the consensus statement has streamlined the reporting of tennis injuries, there remains discordance in important injury trends.
Court Types
Women were more likely to injure themselves on clay courts compared with hard courts. Conversely, Okholm Kryger et al18 found that female athletes were more likely to sustain an injury on hard courts compared with clay courts. Previous research has largely attributed the difference in injury rates on hard versus clay courts to frictional differences.4,7,16 These conflicting findings indicate that surface friction may not be the only factor determining a court’s effect on athlete injury. Recent reports have found that clay courts actually increase the length of rallies and effective playing time, which decreases the effective recovery time and results in an overall higher demand for athletes, as evidenced by elevated heart rates and lactate concentrations during play on clay courts.13,14,22 Perhaps overtraining, athlete fatigue, and volume of play, which have already been positively correlated with increased injury rates in elite athletes, are also necessary factors to consider.10
Time of Year
For men, injury rates peaked during the months of April, May, and November, which coincide with the months during which players may qualify for entry into 1 of the 4 major Grand Slam competitions (Figure 1). This finding contradicts data by Okholm Kryger et al18 that identified no significant difference in the monthly trend of injuries in men. This inconsistency could be explained by the differences in profiles between the Association of Tennis Professionals athletes used in that study and the athletes in this study. Players competing in USTA Pro Circuit futures and challenger tournaments are younger developmentally than athletes competing in Association of Tennis Professionals tournaments.
Male injury rates often peaked during months that contained the fewest number of MEs (Figure 1). Conversely, injury rates often reached troughs during months that contained the highest number of MEs.
Study Limitations
This study analyzes withdrawals and retirements over a 1-year period; sample sizes are limited for some of the analyses. Tournament records were occasionally nonuniform as the records were being completed by multiple different tournament physicians. Both men and women had to have their withdrawal/retirement form filled out by the tournament physician. Additionally, the sports medicine therapist was also permitted to fill out the form for the men. This may have led to the increase in the men’s injury rate leading to withdrawal or retirement in comparison to the women’s rate. Injury rates should be reported as a function of playing time given the variation in match length between men and women.19 However, this was not possible given the retrospective nature of the study.
Conclusion
Women were 4 times more likely to sustain an injury on clay courts compared with hard courts and in the first half of the year compared with the second half. Injury rates for men often peaked during the months that they can qualify for Grand Slam tournaments. Men had a higher injury rate than women.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1.2013 Men’s Pro Circuit Tournament Information. https://www.usta.com/Pro-Tennis/Pro-Circuit/2013_mens_pro_circuit_tournaments__january/. Accessed September 7, 2015.
- 2.2013 Official Grand Slam Rule Book. London, England: Grand Slam Committee; 2013. [Google Scholar]
- 3.2013 Women’s Pro Circuit Tournament Information. United States Tennis Association. https://www.usta.com/Pro-Tennis/Pro-Circuit/2013_womens_pro_circuit_tournaments__january/. Accessed September 7, 2015.
- 4. Abrams GD, Renstrom PA, Safran MR. Epidemiology of musculoskeletal injury in the tennis player. Br J Sports Med. 2012;46:492-498. [DOI] [PubMed] [Google Scholar]
- 5. Breznik K, Batagelj V. Retired matches among male professional tennis players. J Sports Sci Med. 2012;11:270-278. [PMC free article] [PubMed] [Google Scholar]
- 6. Bylak J, Hutchinson MR. Common sports injuries in young tennis players. Sports Med. 1998;26:119-132. [DOI] [PubMed] [Google Scholar]
- 7. Damm L, Low D, Richardson A, Clarke J, Carre M, Dixon S. The effects of surface traction characteristics on frictional demand and kinematics in tennis. Sports Biomech. 2013;12:389-402. [DOI] [PubMed] [Google Scholar]
- 8. Jayanthi NA, O’Boyle J, Durazo-Arvizu RA. Risk factors for medical withdrawals in United States Tennis Association junior national tennis tournaments: a descriptive epidemiologic study. Sports Health. 2009;1:231-235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Knowles SB, Marshall SW, Guskiewicz KM. Issues in estimating risks and rates in sports injury research. J Athl Train. 2006;41:207-215. [PMC free article] [PubMed] [Google Scholar]
- 10. Koutedakis Y, Sharp NC. Seasonal variations of injury and overtraining in elite athletes. Clin J Sport Med. 1998;8:18-21. [DOI] [PubMed] [Google Scholar]
- 11. Kovacs M, Ellenbecker B, Kibler W, Roetert E, Lubbers P. Injury trends in American competitive junior tennis players. J Med Sci Tennis. 2014;19:19-23. [Google Scholar]
- 12. Maquirriain J, Baglione R. Epidemiology of tennis injuries: an eight-year review of Davis Cup retirements. Eur J Sport Sci. 2015;16:266-270. [DOI] [PubMed] [Google Scholar]
- 13. Martin C, Thevenet D, Zouhal H, et al. Effects of playing surface (hard and clay courts) on heart rate and blood lactate during tennis matches played by high-level players. J Strength Cond Res. 2011;25:163-170. [DOI] [PubMed] [Google Scholar]
- 14. Murias JM, Lanatta D, Arcuri CR, Laiño FA. Metabolic and functional responses playing tennis on different surfaces. J Strength Cond Res. 2007;21:112-117. [DOI] [PubMed] [Google Scholar]
- 15. Nigg BM, Segesser B. The influence of playing surfaces on the load on the locomotor system and on football and tennis injuries. Sports Med. 1988;5:375-385. [DOI] [PubMed] [Google Scholar]
- 16. Nigg BM, Yeadon MR. Biomechanical aspects of playing surfaces. J Sports Sci. 1987;5:117-145. [DOI] [PubMed] [Google Scholar]
- 17. O’Donoghue P, Ingram B. A notational analysis of elite tennis strategy. J Sports Sci. 2001;19:107-115. [DOI] [PubMed] [Google Scholar]
- 18. Okholm Kryger K, Dor F, Guillaume M, et al. Medical reasons behind player departures from male and female professional tennis competitions. Am J Sports Med. 2015;43:34-40. [DOI] [PubMed] [Google Scholar]
- 19. Pluim BM, Fuller CW, Batt ME, et al. Consensus statement on epidemiological studies of medical conditions in tennis, April 2009. Br J Sports Med. 2009;43:893-897. [DOI] [PubMed] [Google Scholar]
- 20. Pluim BM, Staal JB, Windler GE, Jayanthi N. Tennis injuries: occurrence, aetiology, and prevention. Br J Sports Med. 2006;40:415-423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Reid M, Schneiker K. Strength and conditioning in tennis: current research and practice. J Sci Med Sport. 2008;11:248-256. [DOI] [PubMed] [Google Scholar]
- 22. Reid MM, Duffield R, Minett GM, Sibte N, Murphy AP, Baker J. Physiological, perceptual, and technical responses to on-court tennis training on hard and clay courts. J Strength Cond Res. 2013;27:1487-1495. [DOI] [PubMed] [Google Scholar]
- 23. Sahai H, Khurshid A. Statistics in Epidemiology: Methods, Techniques, and Applications. 1st ed. Boca Raton, FL: CRC Press; 1996. [Google Scholar]
- 24. Sell K, Hainline B, Yorio M, Kovacs M. Illness data from the US Open tennis championships from 1994 to 2009. Clin J Sport Med. 2013;23:25-32. [DOI] [PubMed] [Google Scholar]
- 25. Sell K, Hainline B, Yorio M, Kovacs M. Injury trend analysis from the US Open tennis championships between 1994 and 2009. Br J Sports Med. 2014;48:546-551. [DOI] [PubMed] [Google Scholar]
- 26.Tournament Calendar. International Tennis Federation. http://www.itftennis.com/procircuit/tournaments/men’s-calendar.aspx. http://www.itftennis.com/procircuit/tournaments/women’s-calendar.aspx. Accessed September 7, 2015.
- 27. Winge S, Jorgensen U, Nielsen AL. Epidemiology of injuries in Danish championship tennis. Int J Sports Med. 1989;10:368-371. [DOI] [PubMed] [Google Scholar]
- 28. Young JA, Pain MD, Pearce AJ. Experiences of Australian professional female tennis players returning to competition from injury. Br J Sports Med. 2007;41:806-811. [DOI] [PMC free article] [PubMed] [Google Scholar]