

Abstract
Objective:
The aim of this study was to identify the range and frequency of patient-reported barriers and facilitators to antiretroviral treatment (ART) adherence in sub-Saharan Africa (SSA).
Design:
Studies from 2005 to 2016 were identified by searching 10 electronic databases and through additional hand and web-searching.
Methods:
Inclusion criteria were HIV-positive adults taking ART based in any SSA country, qualitative study or quantitative survey and included at least one patient-reported barrier or facilitator to ART adherence. Exclusion criteria were only including data from treatment-naive patients initiating ART, only single-dose treatment, participants residing outside of SSA and reviews.
Results:
After screening 11 283 records, 154 studies (161 papers) were included in this review. Forty-three barriers and 30 facilitators were reported across 24 SSA countries. The most frequently identified barriers across studies were forgetting (n = 76), lack of access to adequate food (n = 72), stigma and discrimination (n = 68), side effects (n = 67) and being outside the house or travelling (n = 60). The most frequently identified facilitators across studies were social support (n = 60), reminders (n = 55), feeling better or healthier after taking ART (n = 35), disclosing their HIV status (n = 26) and having a good relationship with a health provider (n = 22).
Conclusion:
This review addresses the gap in knowledge by collating all the patient-reported barriers and facilitators to ART adherence in SSA. Current barriers measures need to be adapted or new tools developed to include the wide variety of factors identified. The factors that have the greatest impact need to be isolated so interventions are developed that reduce the barriers and enhance the facilitators.
Keywords: Africa South of the Sahara, AIDS, antiretroviral therapy, HIV, medication adherence
Introduction
Nearly 25 million people, 70% of all those living with HIV globally, live in countries in sub-Saharan Africa (SSA) [1]. HIV is a debilitating disease; however, antiretroviral treatment (ART) helps promote effective viral suppression, reduces the risk of transmission and prevents death [2,3]. To ensure positive treatment outcomes, high levels of ART adherence (80–95%) are necessary depending on the regime potency [4–6]; however, a meta-analysis [7] indicated that 23% of Africans were achieving less than 80% adherence, potentially impacting on prognosis.
Mills et al. [3] conducted a systematic review in 2005 of patient-reported barriers and facilitators to ART adherence globally. This review identified important barriers, in both high-income countries (HIC) and low and middle-income countries (LMIC), which included substance abuse, forgetfulness, pill burden, fear of disclosure, falling asleep, decreased quality of life, access to medication, being suspicious of the treatment, work and family responsibilities and complicated regimens; however, only 12 (14.3%) of the studies included were conducted in LMIC of which only five were in SSA. ART availability in SSA has improved since this review was conducted, with 1.3 million patients receiving ART treatment in 2006; a 10-fold increase on patients with access 3 years earlier [8]. The lack of treatment availability would have impacted the number of studies being conducted in this region, which has steadily increased over the past decade.
No facilitators were identified by Mills et al. in LMIC [3]; however, important facilitators were identified, including seeing positive effects of medication, accepting their HIV status, using reminders, having a simple regimen, sense of self-worth and understanding the need for strict adherence. Although some similarities were found between different settings and countries, the review urged the need to determine the patient-important factors for adherence in LMIC [3] due to the number of people living with HIV in these areas and the unique psycho-socio-political environments.
In the past decade, there has been a shift in simply identifying and reporting rates of nonadherence and an increased focus on identifying and addressing barriers and facilitators to ART adherence in LMIC, in particular in SSA [9–11]; therefore, this systematic review is a critical update. The review identifies adult patient-reported barriers and facilitators to ART adherence in SSA from 2005 to 2016 in studies with qualitative and quantitative methodology.
Materials and methods
Search strategy
The review was conducted in-line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) [12]. N.C. performed searches on 10 databases on 24 May 2016: Cochrane Library, MEDLINE (OVID), PsycINFO (OVID), PsycARTICLES (OVID), EMBASE (OVID), Global Health (OVID), CINAHL (EBSCO), International Bibliography of the Social Science (IBSS; Proquest), Applied Social Sciences Index and Abstracts (AIDIA; Proquest) and African Index Medicus (AIM; WHO). Search terms were varied to adapt to the different requirements of the different databases. The search included terms related to HIV, ART, SSA countries and adherence (see supplementary material for full example of search strategy).
All databases were searched from 2005 to 24 May 2016 to investigate the research published since the review by Mills et al. [3]. All records were downloaded into ENDNOTE (X7.4).
Hand-searching, web-searching and forward citation searching were conducted to find other relevant published and unpublished studies. Abstracts from the following international conferences were searched: International AIDS Society (IAS; 2005–2015), Conference on Retroviruses and Opportunistic Infections (CROI; 2014, 2016), AIDS Impact (2009–2015) and International AIDS Conference (2006–2014). For all potentially relevant abstracts, if no published article was found, the authors were contacted for more details if possible. Reference lists of included articles and systematic reviews were searched. Searches in Google Scholar were conducted using search terms such as ‘adherence’, ‘HIV’ and ‘Sub-Saharan Africa’. Forward tracking of the review by Mills et al. [3] was also performed in the Web of Science database.
Study selection
N.C. reviewed all the titles and abstracts of each record to assess potential relevance and M.Ah. examined a random sample (10%) and a concordance rate was measured. Acceptable concordance was predefined as agreement on at least 90%, which is the same as other health reviews [13,14]. N.C. reviewed the full text for any potentially relevant studies to assess eligibility. Eligible studies met the following criteria: based in SSA, original research, any language, qualitative study or quantitative survey and included an adult patient-reported barrier or facilitator to ART adherence. Studies were excluded if they only focused on initiation to ART in treatment-naive participants, only utilized a single dose of ART treatment, for example prophylaxis, only focused on Africans living in a non-SSA country or were only reviews.
Quality assessment
N.C. completed quality assessment for all included studies. M.Ah. assessed a random sample of 30 (15 qualitative and 15 quantitative). The RATS (Relevance, Appropriateness, Transparency, Soundness) measure [15] was used to assess the qualitative studies and a measure developed by Hawker et al. [16] was used to assess the quantitative studies (see supplementary material for further details).
Data extraction
N.C. extracted all the data into a predesigned Excel spreadsheet that was double checked for accuracy. After an initial read of all qualitative papers, a list of all key barriers and facilitators were identified and were combined into themes. N.C., L.D.H. and M.Ab. discussed the themes and any disputes were resolved (see supplementary material for further details on extraction). Due to the considerable heterogeneity of the studies, a meta-analysis was not suitable.
Results
A total of 161 papers involving 154 studies were identified for inclusion. The search of the 10 databases provided a total of 11 283 citations (see Fig. 1). After adjusting for duplicates, 6065 citations remained. Of these, 5266 citations were excluded after reviewing the title and abstracts. The majority of these were excluded (4943; 93.9%) because they were not related to HIV or adherence. The remaining 323 citations (6.1%) were excluded based upon other criteria.
Fig. 1.
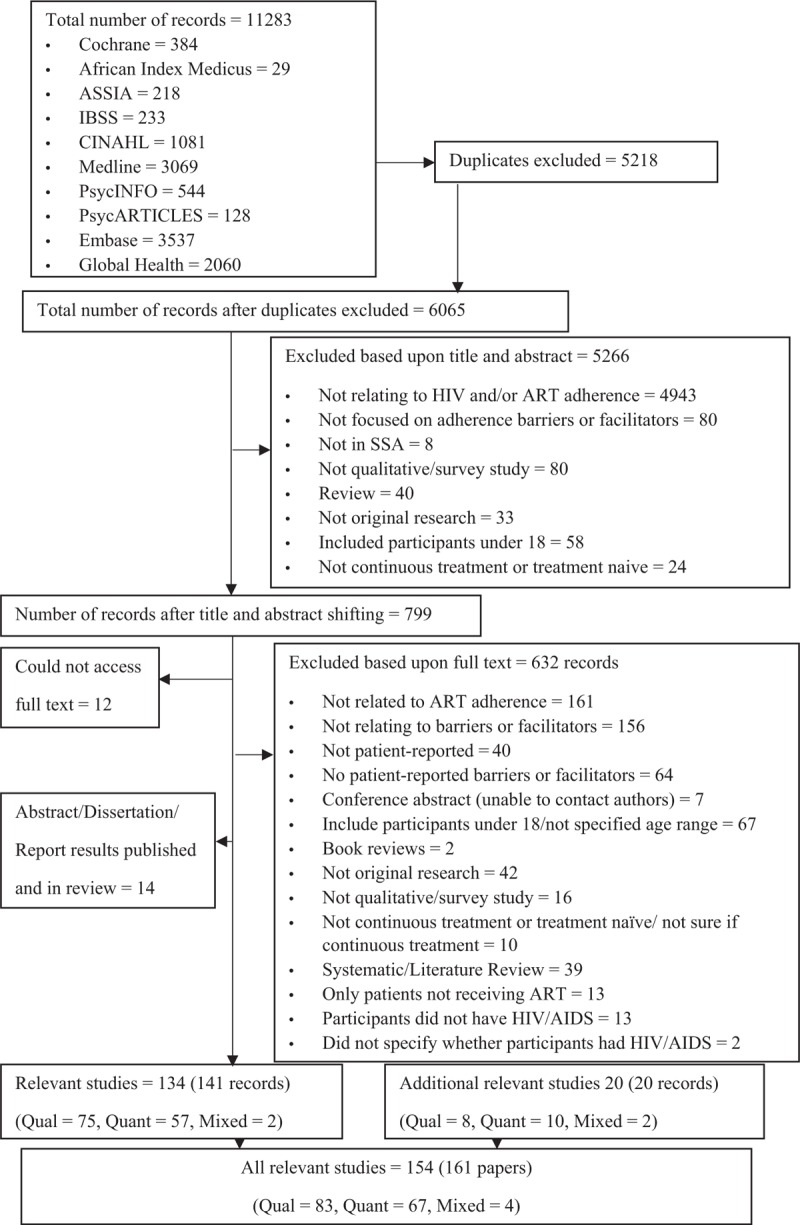
Flowchart.
The full text of the remaining 799 potentially relevant citations were searched for; however, 12 (1.5%) could not be retrieved. The full texts of the remaining 787 papers were examined in more detail. Fourteen were excluded (1.8%) because the search had identified both published and unpublished formats of the same studies; therefore, the published versions were retained. A further 632 papers (80.3%) were excluded based upon inclusion and exclusion criteria. From the 141 relevant papers (17.9%) identified, 134 relevant studies were included. From the additional searching, a further 20 studies were identified that met the criteria for inclusion. An acceptable concordance of 91.0% was achieved between N.C. and M.Ah. for inclusion of studies.
Overall, 154 studies were eligible of which 83 were qualitative [17–99], 67 were quantitative [100–166] and four were mixed [167–170], which included at least one patient-reported barrier or facilitator in both the qualitative and quantitative studies included in the paper. Three studies were published in French [116,137,149] and a fluent French speaker was utilized to extract the data and translate into English. The remaining studies were published in English.
Description of studies
A total of 37 175 HIV-positive participants were included across all 154 quantitative and qualitative studies of which 36 476 were prescribed ART. Within the 87 qualitative studies, 3247 HIV-positive participants were included of whom 2824 were prescribed ART. Within the 71 quantitative studies, 33 928 HIV-positive participants were included of whom 33 652 were prescribed ART (see supplementary material (Table 3) for a description of each study).
Studies were conducted in 24 countries in SSA with six studies including more than one country [45,64,84,95,124,130]. More than half the studies (59.7%) were conducted across South Africa, Uganda, Ethiopia and Kenya.
Just over half of the qualitative studies conducted semi-structured in-depth interviews (IDIs) (49; 56.3%) [17,20–22,26,27,29,32–37,39–43,45–47,49,51,54–60,62,63,65–67,69–71,78,81,84,85,87–90,95–97,165] with their HIV-positive participants. Eighteen studies (20.7%) used focus group discussions (FDGs) [19,23–25,28,50,53,61,68,73,74,76,77,82,94,98,167,169], 16 used both IDIs and FDGs (18.4%) [18,30,31,38,44,52,64,72,75,79,83,86,92,93,99,170], one used free attitude interviews (FAIs) and FGDs (1.1%) [80], one used group sessions without more detail [168], one used IDIs and life history and illness narratives [48] and one used digital stories [91].
The majority of the quantitative surveys (54; 76.1%) were administered by an interviewer [100,102,104–109,112,113,115–117,119,121–124,128–130,133–137,139,141–150,152–166,168,169], five (7.0%) were self-administered [125,126,132,140,151], one (1.4%) used an audio computer-assisted self-interview [110] and the remaining studies (11; 15.5%) did not specify or it was not clear how the survey was administered [101,103,111,114,118,120,127,131,138,167,170]. No studies indicated clearly that there was a free response option for participants to report the barriers they experienced (for further description on the studies see the supplementary material).
Quality assessment
The qualitative studies showed overall high quality, with 98.9% of studies including all RATS items related to relevance of study question, 72.4% including the item related to appropriateness of qualitative method and 83.5% including all items related to soundness of interpretive approach, with the exception of poor transparency of the procedure (only 55.0% of studies included all items). In particular, studies required more information regarding recruitment (only 23.0% of studies included this), who chose not to participate and why (only 20.7% included this), end of data collection justification (25.0% included this) and researcher bias (16.1% included this). The quantitative studies showed overall fair/good quality (9.2% of studies being assessed as good across categories and 65.9% being assessed as fair), with the exception of the ethics and bias category (49.3% assessed as poor and 12.7% assessed as very poor). Only 5.6% of studies were assessed as good quality in this category, which required papers to include explicit details regarding issues of patient confidentiality, sensitivity and informed consent. Researchers also were required to be reflexive or be aware of any potential bias they may have. One-third of studies (32.4%) acknowledged these issues without including explicit details; however, the majority either briefly mentioned them or did not include them (see supplementary material for further details).
Barriers
Forty-three unique patient-reported barriers were identified in 79 (90.8%) of the qualitative and 68 (95.8%) of the quantitative studies that we developed into nine themes comprising financial constraints, problems with their health provider and other interpersonal relationships, issues regarding medication collection and medication taking, treatment-related challenges, problems with their mental health and well-being and beliefs about HIV and treatment as well as specific beliefs about ART. See Table 1 for a list of the themes and both the barriers and facilitators included within each theme (see supplementary material, for further details including a list of studies that reported each factor as well as the frequency of nonadherent participants within each study that reported each barrier or facilitator if reported).
Table 1.
Barriers and facilitators.
| Themes | Barriers (n of studies that reported factor) | Facilitators (n of studies that reported factor) |
| Financial | Lack of money for transport to ART clinic (32) | Grant or livelihood support (5)d |
| Lack of money for HIV care (19) | Free ART treatment (4) | |
| Do not want to lose disability grant (6)d | ||
| Health provider | Dissatisfaction with HIV/ART information provided (17) | Good relationship with health provider (22)d |
| Experienced negative treatment from clinic staff (10) | Receiving counselling and/or teaching (17) | |
| Unable to gain attention from staff (9) | ||
| Poor relationship with health | ||
| provider (5)d | ||
| Medication taking | Forgetting (76)a | Reminders (55) |
| Lack of access to adequate food (72)b,d | Having a routine (9) | |
| Stigma and discrimination (68) | ART packaging (7) | |
| Outside house or travelling (60)c | Access to food and/or water (6)d | |
| Being busy (30) | Carrying ART whilst out of the house (5) | |
| Run out of ART (26) | ||
| Sleeping (22) | ||
| Difficulty taking ART in private (17)a | ||
| Change in daily routine (15) | ||
| No access to liquids (6)a,d | ||
| Interpersonal relationships | Lack of social support (22)d | Social support (60)a,d |
| Sharing or selling ART (7) | Having disclosed HIV status (26)d | |
| HIV nondisclosure (21)d | Want to live and take care of children (21) | |
| Sex (wives have lack of autonomy) (6) | Attending a support group (11) | |
| Seeing others improve on ART (6) | ||
| Want to look healthy to others (5) | ||
| Staying away from negative relationships (2) | ||
| Mental health and well being | Feeling sick or ill (30)d | Feeling better or healthier (35)f |
| Using alcohol or other substances (27)a | Being able to work again (13) | |
| Feeling better or healthier (26)e | “Normalization’ – feeling the same as others or same as before HIV (8) | |
| Low mood or stress (22)a | Fewer HIV/AIDS-related illnesses (8) | |
| Feeling hopeless (7)d | Prayers or faith in God (8) | |
| Feeling lonely (4) | Being hopeful (6)d | |
| Beliefs about HIV and treatment | Religious beliefs or treatments (27)a | Want to take control of their health (13) |
| Traditional beliefs or medicines (20) | Improved knowledge and understanding of HIV/ART (10) | |
| Fear of cause of HIV (6) | Accept own HIV status (7)d | |
| Denial of HIV status (4)d | ||
| Beliefs about ART | Negative attitude towards treatment | Belief in ART benefit (20)d |
| regime (19) | Do not want to be ill again (14) | |
| ART will not work (7)d | Adherence self-efficacy (8) | |
| ART is harmful (7) | ART helps you look healthy to others (5) | |
| Lack of motivation to take ART (7) | God provided ART (4) | |
| Should not mix ART with other treatments (4) | ||
| Medication collection | Erratic clinic drug supply (22) | |
| Long clinic waiting times (13)a | ||
| Long distance to the clinic (8) | ||
| Unable to get to clinic due to work | ||
| constraints (7) | ||
| Treatment-related factors | Side effects (67)c | |
| Pill burden (20) | ||
| Problem with physical characteristics of | ||
| Pills (4) |
ART, antiretroviral treatment.
aOne mixed-methods study identified the barriers or facilitators in both the qualitative and quantitative components.
bThree mixed-methods studies identified the barriers or facilitators in both the qualitative and quantitative components.
cTwo mixed-methods studies identified the barriers or facilitators in both the qualitative and quantitative components.
dComparable barriers and facilitators across themes.
eSame factor as both a barrier and facilitator.
fSame factor as well as a comparable factor to another barrier or facilitator.
Facilitators
Thirty patient-reported facilitators were identified in 76 (87.4%) of the qualitative and 21 (29.6%) of the quantitative studies. Seventeen facilitators (56.7%) were only identified in the qualitative studies. The facilitators are composed of seven of the same themes as the barriers excluding medication collection and treatment-related factors (see Table 1). Due to the comparable themes, the barriers and facilitators will be described together.
Themes
There were several factors that impacted adherence related to finance as well as each patient's health provider. Within the finance theme, in particular not receiving financial help was a barrier, whereas receiving funds was a benefit. Across studies, the fifth most reported facilitator was having a good relationship with their health provider (n = 22). The opposite was identified as a barrier, however, only by a few studies (n = 5).
Four of the five most-reported barriers across all studies were classified into the medication-taking theme; forgetting (n = 76), lack of access to adequate food (n = 72), stigma and discrimination (n = 68) and being outside the house or travelling (n = 60). Some of these had comparable facilitators, including having reminders to take medication [which was the second most reported facilitator (n = 55)], having access to food or water and carrying ART whilst out of the house, although the latter two were only identified by a small number of studies.
Interpersonal relationships included the first and fourth most reported facilitators [social support (n = 60) and having disclosed their HIV status (n = 26)]. Both of these included comparable barriers (e.g. lack of social support and HIV nondisclosure) indicating that an absence of these factors is a barrier to adherence.
Mental health and well-being was the only theme to include the same factor as both a barrier and facilitator, feeling better or healthier after ART treatment. This factor was the third most reported facilitator across studies (n = 35), although 26 studies also reported it as a barrier. Another comparable barrier to feeling better was also reported (feeling sick or ill) indicating that the opposite can also hinder adherence. Feeling hopeless and being hopeful were both reported as comparable factors, although only reported in a few studies.
The patients’ beliefs about HIV and treatments theme also included factors that acted as a barrier or facilitator. Both religious and traditional beliefs and treatments were indicated as a barrier to adhering to ART, whilst a patient's desire to take control of their health was a facilitator. Denial of one's own HIV status was reported as a barrier and had a comparable facilitator of accepting one's own HIV status, although these were reported by a small number of studies. Specific beliefs about ART also showed to have an impact on adherence. The belief in the benefit of ART was reported (n = 20) as a facilitator, whereas believing ART will not work was reported as a barrier, but only by seven studies in comparison.
Both medication collection and treatment-related factors only included barriers. The latter theme included the fourth most reported barrier across studies, side effects (n = 67). Erratic clinic drug supply and long waiting times were reported by the most studies as a barrier to ART adherence in the medication collection theme.
Discussion
Summary of evidence
In this systematic review, a total of 43 patient-reported barriers and 30 facilitators to ART adherence were identified in 154 studies across 24 SSA countries. Barriers and facilitators to ART adherence included factors related to participants’ physically taking their ART medication (e.g. unable to take their pills without adequate food or using reminders to remember to take their pills), factors that impacted participants’ physical or mental health (e.g. feeling sick or feeling better after taking ART), factors related to participants’ relationships with other people (e.g. nondisclosure of HIV status to others or social support), factors related to finance (e.g. lack of money for HIV care or free ART treatment), factors related to participants’ health provider including all staff (e.g. experiencing negative treatment from clinic staff or having a good relationship with their health provider), beliefs around HIV and treatments for HIV (e.g. using traditional medicines or accepting own HIV status) and beliefs regarding ART (e.g. ART is harmful or ART is beneficial). Factors related to collecting medication at the clinic (e.g. long waiting times or erratic drug supply) and treatment-related factors (e.g. side effects or pill burden) were only reported as barriers to ART adherence. One factor was both a barrier and facilitator (e.g. feeling better after taking ART), which emphasizes medication-adhering behaviour is not universal and it is necessary to explore this individually. The most frequently identified barriers across studies and methodologies were forgetting, lack of access to adequate food, stigma and discrimination, side effects and being outside the house or travelling. The most frequently identified facilitators across studies and methods were social support, using reminders, feeling better or healthier after taking ART, disclosing their HIV status and having a good relationship with a health provider. This review helps identify the range and frequency of factors that impact ART adherence for patients within a variety of different settings in SSA.
Other systematic reviews have focused on specific types of adherence barriers, including geographic and transport-related barriers in SSA [171], food insecurity [172] and depression and alcohol use in SSA [173]. These reviews are useful because they go in-depth into one type of barrier and they may focus on HIV outcomes other than adherence [171]; however, this review is necessary to give an overview of the many factors that affect ART adherence in SSA.
Frequency across studies does not necessarily equate with importance for individuals; therefore, the most reported factors may not have the greatest impact upon adherence. Unfortunately, the low number of studies that included the nonadherent within-study frequencies means it is difficult to compare the impact of these on adherence. Future studies should include these to allow researchers to ascertain not only the range of factors that affect adherence but also the impact of each.
This review identified 26 barriers that were not previously reported in SSA in the previous systematic review [3], including traditional medicines, religious beliefs or treatments, lack of access to food and sharing medication. These need to be acknowledged when working with people living with HIV in SSA. The five most frequently reported facilitators were included in the previous review [3], showing that there is similarity between patients in HIC and LMIC; however, several others were identified that had not been previously noted, for example financial aid, access to food and water and religious beliefs. This further confirms that there are factors that may be more applicable to LMIC that therefore need particular consideration when designing interventions to improve ART adherence.
Understanding and being aware of these are important for policy makers, researchers and health professionals. Although patients denied missing ART doses to their health professional, if a barrier measure was used, patients would then reveal nonadherence by indicating the barriers that prevent them from adhering [174]. Having a list of barriers that are applicable to the context is essential. There are some differences between HIC and LMIC and this should be reflected in the provisions available for patients. Although general and HIV-specific measures for barriers to adherence do currently exist [175–179], none encompass the wide range of reasons identified in this review. Developing or adapting a measure that can be utilized by health professionals in SSA is necessary. In particular, the most commonly used self-report HIV adherence measure [180] (Adult AIDS Care Trials Group [AACTG]) includes a ‘reasons for nonadherence’ subscale [175] that needs to be adapted if used in SSA to include all relevant factors. To our knowledge, there is not a similar measure for facilitators and research needs to explore whether assessing the facilitators may be equally as helpful as the barriers to reach the level of desired adherence.
Immediate treatment initiation after diagnosis has been shown to have more positive HIV outcomes than later [181,182] and thus may become the recommended start date globally. There are debates in the literature about the practicalities associated with immediate ART initiation [183], including increased burden on the healthcare system, increased frequency of risk behaviours when receiving ART and ethical issues such as resource allocation in low-resource settings [183]. The impact of certain barriers may increase, such as the factors associated with healthcare; therefore, the need to enhance the facilitators will become greater.
Future research needs to help identify the barriers and facilitators that have the greatest impact on adherence and help develop interventions based upon these. Within SSA, there have been several interventions focused on helping participants remember their medication, whereas less have focused on lack of food or stigma [184]. Research needs to explore whether these other interventions would have a greater influence on adherence. In addition, the focus on adherence interventions in SSA has often been observational and more randomized control trials (RCTs) are required [184].
Limitations
Although efforts were made to include all eligible studies, it is possible that not all studies exploring barriers and facilitators to ART adherence in SSA were included, as research from resource-constrained settings may be less likely to be published or not indexed in the major databases [185]. The studies are not easily compared due to the heterogeneity of how factors and adherence were measured. There was a great variety of within-study frequency measurement; therefore, only studies that included the frequency of reporting within nonadherent participants were included. Also, some studies combined separate factors into one, so it was not possible to extract the individual factors. The quality of the studies seemed generally fair; however, there were areas of poor quality. As two measures were utilized in quality assessment, it is not easy to compare the quality across both qualitative and quantitative studies.
The majority of the qualitative studies identified both barriers and facilitators, whereas the majority of the quantitative studies only identified barriers. This bias may have prevented certain facilitators from being identified. Barrier measures or adapted versions [175,177,186–189] were utilized in some surveys that may have caused certain barriers to be reported more frequently; however, other important barriers may have been missed because they were not included.
Conclusion
This review highlights the range and frequency of barriers and facilitators that affect ART adherence in HIV adult patients in SSA. Research needs to help identify which factors have the greatest impact on adherence and develop interventions accordingly. Measures need to be developed or adapted for SSA to include all the relevant factors. Interventions need to be developed that aim to reduce the barriers and enhance the facilitators. By understanding and being able to identify what hurdles a patient experiences and how certain aspects may encourage them to adhere, the focus is now on using this information to help patients achieve optimum ART outcomes.
Acknowledgements
N.C. drafted the protocol including the search strategy and L.D.H and M.Ab. helped develop the final one. N.C. performed the electronic search. N.C. and M.Ah. identified and quality assessed relevant studies. N.C. wrote the first draft. All authors contributed to subsequent drafts. All authors read and approved the final draft. Open access for this article was funded by King's College London.
Conflicts of interest
There are no conflicts of interest.
Supplementary Material
Footnotes
Lyndsay D. Hughes and Melanie Abas contributed equally to the writing of this article.
References
- 1.Joint United Nations Programme on HIV/AIDS (UNAIDS). The Gap report. 2014; Geneva: UNAIDS, http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_en.pdf [Google Scholar]
- 2.World Health Organisation (WHO). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. 2013; Geneva: World Health Organisation, http://www.who.int/hiv/pub/guidelines/arv2013/download/en/ [PubMed] [Google Scholar]
- 3.Mills EJ, Nachega JB, Bangsberg DR, Singh S, Rachlis B, Wu P, et al. Adherence to HAART: a systematic review of developed and developing nation patient-reported barriers and facilitators. PLoS Med 2006; 3:e438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hardon AP, Akurut D, Comoro C, Ekezie C, Irunde HF, Gerrits T, et al. Hunger, waiting time and transport costs: time to confront challenges to ART adherence in Africa. AIDS Care 2007; 19:658–665. [DOI] [PubMed] [Google Scholar]
- 5.Orrell C, Bangsberg DR, Badri M, Wood R. Adherence is not a barrier to successful antiretroviral therapy in South Africa. AIDS 2003; 17:1369–1375. [DOI] [PubMed] [Google Scholar]
- 6.Bangsberg DR. Less than 95% adherence to nonnucleoside reverse-transcriptase inhibitor therapy can lead to viral suppression. Clin Infect Dis 2006; 43:939–941. [DOI] [PubMed] [Google Scholar]
- 7.Mills EJ, Nachega JB, Buchan I, Orbinski J, Attaran A, Singh S, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: a meta-analysis. JAMA 2006; 296:679–690. [DOI] [PubMed] [Google Scholar]
- 8.Ojikutu B, Makadzange AT, Gaolathe T. Scaling up ART treatment capacity: lessons learned from South Africa, Zimbabwe, and Botswana. Curr HIV/AIDS Rep 2008; 5:94–98. [DOI] [PubMed] [Google Scholar]
- 9.Mayston R, Kinyanda E, Chishinga N, Prince M, Patel V. Mental disorder and the outcome of HIV/AIDS in low-income and middle-income countries: a systematic review. AIDS 2012; 26:S117–S135. [DOI] [PubMed] [Google Scholar]
- 10.Langebeek N, Gisolf EH, Reiss P, Vervoort SC, Thóra B, Richter C, et al. Predictors and correlates of adherence to combination antiretroviral therapy (cART) for chronic HIV infection: a meta-analysis. BMC Med 2014; 12:142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Merten S, Kenter E, McKenzie O, Musheke M, Ntalasha H, Martin-Hilber A. Patient-reported barriers and drivers of adherence to antiretrovirals in sub-Saharan Africa: a meta-ethnography. Trop Med Int Health 2010; 15:16–33. [DOI] [PubMed] [Google Scholar]
- 12.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009; 151:264–269. [DOI] [PubMed] [Google Scholar]
- 13.Leamy M, Bird V, Le Boutillier C, Williams J, Slade M. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis. Brit J Psychiatry 2011; 199:445–452. [DOI] [PubMed] [Google Scholar]
- 14.Slade M, Leamy M, Bacon F, Janosik M, Le Boutillier C, Williams J, et al. International differences in understanding recovery: systematic review. Epidemiol Psychiatr Sci 2012; 21:353–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Clark J. How to peer review a qualitative manuscript. Peer Rev Health Sci 2003; 2:219–235. [Google Scholar]
- 16.Hawker S, Payne S, Kerr C, Hardey M, Powell J. Appraising the evidence: reviewing disparate data systematically. Qual Health Res 2002; 12:1284–1299. [DOI] [PubMed] [Google Scholar]
- 17.Aransiola J, Imoyera W, Olowookere S, Zarowsky C. Living well with HIV in Nigeria? Stigma and survival challenges preventing optimum benefit from an ART clinic. Glob Health Promot 2014; 21:13–22. [DOI] [PubMed] [Google Scholar]
- 18.Arem H, Nakyanjo N, Kagaayi J, Mulamba J, Nakigozi G, Serwadda D, et al. Peer health workers and AIDS care in Rakai, Uganda: a mixed methods operations research evaluation of a cluster-randomized trial. AIDS Patient Care STDs 2011; 25:719–724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Asgary R, Antony S, Grigoryan Z, Aronson J. Community perception, misconception, and discord regarding prevention and treatment of infection with human immunodeficiency virus in Addis Ababa, Ethiopia. Am J Trop Med Hygiene 2014; 90:153–159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Aspeling HE, van Wyk NC. Factors associated with adherence to antiretroviral therapy for the treatment of HIV-infected women attending an urban care facility. Int J Nurs Pract 2008; 14:3–10. [DOI] [PubMed] [Google Scholar]
- 21.Audu B, Morgan R, Rutter P. Qualitative exploration of the relationship between HIV/AIDS patients’ experiences of clinical services and treatment adherence at Maitama District Hospital, Abuja, Nigeria. AIDS Care 2014; 26:270–273. [DOI] [PubMed] [Google Scholar]
- 22.Axelsson JM, Hallager S, Barfod TS. Antiretroviral therapy adherence strategies used by patients of a large HIV clinic in Lesotho. J Health Popul Nutr 2015; 33:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Baghazal AA. Factors influencing adherence to antiretroviral therapy at a general hospital in Mombasa, Kenya [Master's thesis]. University of the Western Cape; 2011. http://hdl.handle.net/11394/2570. [Google Scholar]
- 24.Balcha TT, Jeppsson A, Bekele A. Barriers to antiretroviral treatment in Ethiopia: a qualitative study. J Int Assoc Phys AIDS Care 2011; 10:119–125. [DOI] [PubMed] [Google Scholar]
- 25.Beyene KA, Gedif T, Gebre-Mariam T, Engidawork E. Highly active antiretroviral therapy adherence and its determinants in selected hospitals from south and central Ethiopia. Pharmacoepidemiol Drug Saf 2009; 18:1007–1015. [DOI] [PubMed] [Google Scholar]
- 26.Bezabhe WM, Chalmers L, Bereznicki LR, Peterson GM, Bimirew MA, Kassie DM. Barriers and facilitators of adherence to antiretroviral drug therapy and retention in care among adult HIV-positive patients: a qualitative study from Ethiopia. PLoS One 2014; 9:e97353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bhagwanjee A, Govender K, Akintola O, Petersen I, George G, Johnstone L, Naidoo K. Patterns of disclosure and antiretroviral treatment adherence in a South African mining workplace programme and implications for HIV prevention. Afr J AIDS Res 2011; 10:291–391. [DOI] [PubMed] [Google Scholar]
- 28.Boateng D, Kwapong GD, Agyei-Baffour P. Knowledge, perception about antiretroviral therapy (ART) and prevention of mother-to-child-transmission (PMTCT) and adherence to ART among HIV positive women in the Ashanti Region, Ghana: a cross-sectional study. BMC Women's Health 2013; 13:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bohle LF, Dilger H, Groß U. HIV-serostatus disclosure in the context of free antiretroviral therapy and socio-economic dependency: experiences among women living with HIV in Tanzania. Afr J AIDS Res 2014; 13:215–227. [DOI] [PubMed] [Google Scholar]
- 30.Byron E, Gillespie S, Nangami M. Integrating nutrition security with treatment of people living with HIV: lessons from Kenya. Food Nutr Bull 2008; 29:87–97. [DOI] [PubMed] [Google Scholar]
- 31.Campbell C, Scott K, Skovdal M, Madanhire C, Nyamukapa C, Gregson S. A good patient? How notions of ‘a good patient’ affect patient-nurse relationships and ART adherence in Zimbabwe. BMC Infect Dis 2015; 15:404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Chileshe M, Bond VA. Barriers and outcomes: TB patients co-infected with HIV accessing antiretroviral therapy in rural Zambia. AIDS Care 2010; 22:51–59. [DOI] [PubMed] [Google Scholar]
- 33.Daftary A, Padayatchi N. Social constraints to TB/HIV healthcare: accounts from coinfected patients in South Africa. AIDS Care 2012; 24:1480–1486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Dahab M, Charalambous S, Hamilton R, Fielding K, Kielmann K, Churchyard GJ, et al. That is why I stopped the ART’: patients’ & providers’ perspectives on barriers to and enablers of HIV treatment adherence in a South African workplace programme. BMC Public Health 2008; 8:63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Dawson-Rose C, Gutin SA, Cummings B, Jaiantilal P, Johnson K, Mbofana F. ART adherence as a key component of prevention with persons living with HIV in Mozambique. J Assoc Nurses AIDS Care 2016; 27:44–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.de Sumari-de Boer IM, van den Boogaard J, Ngowi KM, Semvua HH, Kiwango KW, Aarnoutse RE, et al. Feasibility of real time medication monitoring among HIV infected and TB patients in a resource-limited setting. AIDS Behav 2016; 20:1097–1107. [DOI] [PubMed] [Google Scholar]
- 37.Duwell MM, Knowlton AR, Nachega JB, Efron A, Goliath R, Morroni C, et al. Patient-nominated, community-based HIV treatment supporters: patient perspectives, feasibility, challenges, and factors for success in HIV-infected South African adults. AIDS Pat Care STDs 2013; 27:96–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Elwell K. Facilitators and barriers to treatment adherence within PMTCT programs in Malawi. AIDS Care 2016; 28:971–975. [DOI] [PubMed] [Google Scholar]
- 39.Foster SD, Nakamanya S, Kyomuhangi R, Amurwon J, Namara G, Amuron B, et al. The experience of ’medicine companions’ to support adherence to antiretroviral therapy: quantitative and qualitative data from a trial population in Uganda. AIDS Care 2010; 22:35–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Frank J, Duncan N. Speaking to experts and patients: recommendations for improving antiretroviral therapy (ART) adherence. Health SA Gesondheid 2009; 14:1–9. [Google Scholar]
- 41.Gachanja G, Burkholder GJ. A model for HIV disclosure of a parent's and/or a child's illness. Peer J 2016; 4:e1662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Goudge J, Ngoma B. Exploring antiretroviral treatment adherence in an urban setting in South Africa. J Public Health Policy 2011; 32:S52–S64. [DOI] [PubMed] [Google Scholar]
- 43.Govender V, Fried J, Birch S, Chimbindi N, Cleary S. Disability Grant: a precarious lifeline for HIV/AIDS patients in South Africa. BMC Health Serv Res 2015; 15:227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Grant E, Logie D, Masura M, Gorman D, Murray SA. Factors facilitating and challenging access and adherence to antiretroviral therapy in a township in the Zambian Copperbelt: a qualitative study. AIDS Care 2008; 20:1155–1160. [DOI] [PubMed] [Google Scholar]
- 45.Gusdal AK, Obua C, Andualem T, Wahlstrom R, Tomson G, Peterson S, et al. Voices on adherence to ART in Ethiopia and Uganda: a matter of choice or simply not an option?. AIDS Care 2009; 21:1381–1387. [DOI] [PubMed] [Google Scholar]
- 46.Hussen SA, Tsegaye M, Argaw MG, Andes K, Gilliard D, del Rio C. Spirituality, social capital and service: factors promoting resilience among Expert Patients living with HIV in Ethiopia. Global Public Health 2014; 9:286–298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Izugbara CO, Wekesa E. Beliefs and practices about antiretroviral medication: a study of poor urban Kenyans living with HIV/AIDS. Sociol Health Illness 2011; 33:869–883. [DOI] [PubMed] [Google Scholar]
- 48.Jones C. ‘If i take my pills i’ll go hungry’: the choice between economic security and HIV/AIDS treatment in Grahamstown, South Africa. Ann Anthropol Pract 2011; 35:67–80. [Google Scholar]
- 49.Karanja SW. Factors influencing adherence to antiretroviral Medications among patients living with HIV in Kenya [Master's thesis]. University of Nairobi; 2013. http://erepository.uonbi.ac.ke/handle/11295/60397 [Accessed 25 May 2016]. [Google Scholar]
- 50.Khalid FJ. Adherence to antiretroviral therapy and associated factors among HIV and AIDS patients at Mnazi Mmoja Hospital, Zanzibar [Master's thesis]; 2012. http://41.204.187.24:8080/handle/123456789/1010 [Accessed 25 May 2016]. [Google Scholar]
- 51.Kidia K, Machando D, Bere T, Macpherson K, Nyamayaro P, Potter L, et al. ‘I was thinking too much’: experiences of HIV-positive adults with common mental disorders and poor adherence to antiretroviral therapy in Zimbabwe. Trop Med Int Health 2015; 20:903–913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kuteesa MO, Seeley J, Cumming RG, Negin J. Older people living with HIV in Uganda: understanding their experience and needs. Afr J AIDS Res 2012; 11:295–305. [DOI] [PubMed] [Google Scholar]
- 53.Lifson AR, Demissie W, Tadesse A, Ketema K, May R, Yakob B, et al. Barriers to retention in care as perceived by persons living with HIV in rural Ethiopia: focus group results and recommended strategies. J Int Assoc Provid AIDS Care 2013; 12:32–38. [DOI] [PubMed] [Google Scholar]
- 54.Lyimo RA, de Bruin M, van den Boogaard J, Hospers HJ, van der Ven A, Mushi D. Determinants of antiretroviral therapy adherence in northern Tanzania: a comprehensive picture from the patient perspective. BMC Public Health 2012; 12:716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.MacLachlan EW, Potter K, Hamunime N, Shepard-Perry MG, Uusiku J, Simwanza R, et al. We are now free to speak’: qualitative evaluation of an education and empowerment training for HIV patients in Namibia. PLoS One 2016; 11:e0153042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Maixenchs M, Boene H, Anselmo R, Mindu C, Alonso P, Menéndez C, et al. Post-ART symptoms were not the problem: a qualitative study on adherence to ART in HIV-infected patients in a Mozambican Rural Hospital. PLoS One 2015; 10:e0137336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Makua T. Reduced adherence to antiretroviral therapy among patients on antiretroviral therapy in Limpopo province, South Africa. Afr J Phys Health Educ Recreat Dance 2015; 21:107–114. [Google Scholar]
- 58.Martin F, Kiwanuka T, Kawuma R, Zalwango F, Seeley J. Tasks and strategies of self-management of living with antiretroviral therapy in Uganda. AIDS Patient Care STDs 2013; 27:697–706. [DOI] [PubMed] [Google Scholar]
- 59.Masquillier C, Wouters E, Mortelmans D, van Wyk B. On the road to HIV/AIDS competence in the household: building a health-enabling environment for people living with HIV/AIDS. Int J Environ Res Public Health 2015; 12:3264–3292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Mbonye M, Seeley J, Ssembajja F, Birungi J, Jaffar S. Adherence to antiretroviral therapy in Jinja, Uganda: a six-year follow-up study. PLoS One 2013; 8:e78243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Mbuagbaw L, Bonono-Momnougui RC, Thabane L. Considerations in using text messages to improve adherence to highly active antiretroviral therapy: a qualitative study among clients in Yaounde, Cameroon. HIV/AIDS (Auckland, NZ) 2012; 4:45–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Mendelsohn JB, Rhodes T, Spiegel P, Schilperoord M, Burton JW, Balasundaram S, et al. Bounded agency in humanitarian settings: a qualitative study of adherence to antiretroviral therapy among refugees situated in Kenya and Malaysia. Soc Sci Med 2014; 120:387–395. [DOI] [PubMed] [Google Scholar]
- 63.Mfecane S. Negotiating therapeutic citizenship and notions of masculinity in a South African village. Afr J AIDS Res 2011; 10:129–138. [DOI] [PubMed] [Google Scholar]
- 64.Mkandawire-Valhmu L, Kako PM, Kibicho JW. Perceptions of the character of God as narrated by East African women living with HIV. J Christ Nurs 2012; 29:164–172. [DOI] [PubMed] [Google Scholar]
- 65.Moiloa EM. Nonadherence to ART medication regimens among people living with HIV, who are registered with Leratong hospital in Gauteng province, South Africa [Master's thesis]. Stellenbosch: Stellenbosch University; 2012. http://scholar.sun.ac.za/handle/10019.1/19924 [Accessed 25 May 2016]. [Google Scholar]
- 66.Musumari PM, Feldman MD, Techasrivichien T, Wouters E, Ono-Kihara M, Kihara M. ’If I have nothing to eat, I get angry and push the pills bottle away from me’: a qualitative study of patient determinants of adherence to antiretroviral therapy in the Democratic Republic of Congo. AIDS Care 2013; 25:1271–1277. [DOI] [PubMed] [Google Scholar]
- 67.Mutabazi-Mwesigire D, Seeley J, Martin F, Katamba A. Perceptions of quality of life among Ugandan patients living with HIV: a qualitative study. BMC Public Health 2014; 14:113–118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Nachega JB, Knowlton AR, Deluca A, Schoeman JH, Watkinson L, Efron A, et al. Treatment supporter to improve adherence to antiretroviral therapy in HIV-infected South African adults: a qualitative study. J Acquir Immune Defic Syndr 2006; 43:S127–S133. [DOI] [PubMed] [Google Scholar]
- 69.Nagata JM, Magerenge RO, Young SL, Oguta JO, Weiser SD, Cohen CR. Social determinants, lived experiences, and consequences of household food insecurity among persons living with HIV/AIDS on the shore of Lake Victoria, Kenya. AIDS Care 2012; 24:728–736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Nam SL, Fielding K, Avalos A, Dickinson D, Gaolathe T, Geissler PW. The relationship of acceptance or denial of HIV-status to antiretroviral adherence among adult HIV patients in urban Botswana. Soc Sci Med 2008; 67:301–310. [DOI] [PubMed] [Google Scholar]
- 71.Ngarina M, Popenoe R, Kilewo C, Biberfeld G, Ekstrom AM. Reasons for poor adherence to antiretroviral therapy postnatally in HIV-1 infected women treated for their own health: experiences from the Mitra Plus study in Tanzania. BMC Public Health 2013; 13:450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Nsimba SE, Irunde H, Comoro C. Barriers to ARV adherence among HIV/AIDS positive persons taking antiretroviral therapy in two Tanzanian regions 8-12 months after program initiation. J AIDS Clin Res 2010; 1:111. [Google Scholar]
- 73.Nyanzi-Wakholi B, Lara AM, Watera C, Munderi P, Gilks C, Grosskurth H. The role of HIV testing, counselling, and treatment in coping with HIV/AIDS in Uganda: a qualitative analysis. AIDS Care 2009; 21:903–908. [DOI] [PubMed] [Google Scholar]
- 74.Nyanzi-Wakholi B, Medina Lara A, Munderi P, Gilks C. on behalf of the Dart Trial Team. The charms and challenges of antiretroviral therapy in Uganda: the DART experience. AIDS Care 2012; 24:137–142. [DOI] [PubMed] [Google Scholar]
- 75.Okoror TA, Falade CO, Olorunlana A, Walker EM, Okareh OT. Exploring the cultural context of HIV stigma on antiretroviral therapy adherence among people living with HIV/AIDS in Southwest Nigeria. AIDS Patient Care STDs 2013; 27:55–64. [DOI] [PubMed] [Google Scholar]
- 76.Olupot-Olupot P, Katawera A, Cooper C, Small W, Anema A, Mills E. Adherence to antiretroviral therapy among a conflict-affected population in Northeastern Uganda: a qualitative study. AIDS 2008; 22:1882–1884. [DOI] [PubMed] [Google Scholar]
- 77.Omotala OFI. Knowledge, attitude and practice of antiretroviral therapy among adult hiv patients attending a tertiary hospital in Nigeria [Master's thesis]; 2015. http://repository.unn.edu.ng:8080/xmlui/handle/123456789/1294 [Accessed 25 May 2016]. [Google Scholar]
- 78.Pyne-Mercier LD, John-Stewart GC, Richardson BA, Kagondu NL, Thiga J, Noshy H, et al. The consequences of postelection violence on antiretroviral HIV therapy in Kenya. AIDS Care 2011; 23:562–568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Rasschaert F, Telfer B, Lessitala F, Decroo T, Remartinez D, Biot M, et al. A qualitative assessment of a community antiretroviral therapy group model in Tete, Mozambique. PLoS One 2014; 9:e91544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Ross AJ, Aung M, Campbell L, Ogunbanjo GA. Factors that positively influence adherence to antiretroviral therapy by HIV and/or AIDS patients and their caregivers. Afr J Primary Healthcare Fam Med 2011; 3:196. [Google Scholar]
- 81.Russell S, Martin F, Zalwango F, Namukwaya S, Nalugya R, Muhumuza R, et al. Finding meaning: HIV self-management and wellbeing among people taking antiretroviral therapy in Uganda. PLoS One 2016; 11:e0147896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Salmen CR, Hickey MD, Fiorella KJ, Omollo D, Ouma G, Zoughbie D, et al. Wan Kanyakla’(We are together): Community transformations in Kenya following a social network intervention for HIV care. Soc Sci Med 2015; 147:332–340. [DOI] [PubMed] [Google Scholar]
- 83.Sanjobo N, Frich JC, Fretheim A. Barriers and facilitators to patients’ adherence to antiretroviral treatment in Zambia: a qualitative study. Sahara J 2008; 5:136–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Selman L, Simms V, Penfold S, Powell RA, Mwangi-Powell F, Downing J, et al. ’My dreams are shuttered down and it hurts lots’-a qualitative study of palliative care needs and their management by HIV outpatient services in Kenya and Uganda. BMC Palliat Care 2013; 12:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Shalihu N, Pretorius L, van Dyk A, Vander Stoep A, Hagopian A. Namibian prisoners describe barriers to HIV antiretroviral therapy adherence. AIDS Care 2014; 26:968–975. [DOI] [PubMed] [Google Scholar]
- 86.Siril H, Fawzi MCS, Todd J, Wyatt M, Kilewo J, Ware N, et al. Hopefulness fosters affective and cognitive constructs for actions to cope and enhance quality of life among people living with HIV in Dar Es Salaam, Tanzania. J Int Assoc Provid AIDS Care 2014; [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Siu GE, Seeley J, Wight D. Dividuality, masculine respectability and reputation: how masculinity affects men's uptake of HIV treatment in rural eastern Uganda. Soc Sci Med 2013; 89:45–52. [DOI] [PubMed] [Google Scholar]
- 88.Tilahun HA, Mariam DH, Tsui AO. Effect of perceived stigma on adherence to highly active antiretroviral therapy and self-confidence to take medication correctly in Addis Ababa, Ethiopia. J HIV/AIDS Soc Serv 2012; 11:346–362. [Google Scholar]
- 89.Tiruneh YM, Wilson IB. What time is it? Adherence to antiretroviral therapy in Ethiopia. AIDS Behav 2016; 20:2662–2673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Tomori C, Kennedy CE, Brahmbhatt H, Wagman JA, Mbwambo JK, Likindikoki S, et al. Barriers and facilitators of retention in HIV care and treatment services in Iringa, Tanzania: the importance of socioeconomic and sociocultural factors. AIDS Care 2014; 26:907–913. [DOI] [PubMed] [Google Scholar]
- 91.Treffry-Goatley A, Lessells R, Sykes P, Bärnighausen T, de Oliveira T, Moletsane R, et al. Understanding specific contexts of antiretroviral therapy adherence in rural South Africa: a thematic analysis of digital stories from a community with high HIV prevalence. PLoS One 2016; 11:e0148801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Treves-Kagan S, Steward WT, Ntswane L, Haller R, Gilvydis JM, Gulati H, et al. Why increasing availability of ART is not enough: a rapid, community-based study on how HIV-related stigma impacts engagement to care in rural South Africa. BMC Public Health 2016; 16:87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.van Loggerenberg F, Gray D, Gengiah S, Kunene P, Gengiah TN, Naidoo K, et al. A qualitative study of patient motivation to adhere to combination antiretroviral therapy in South Africa. AIDS Patient Care STDs 2015; 29:299–306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Walstrom P, Operario D, Zlotnick C, Mutimura E, Benekigeri C, Cohen MH. ’I think my future will be better than my past’: examining support group influence on the mental health of HIV-infected Rwandan women. Global Public Health 2013; 8:90–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Ware NC, Idoko J, Kaaya S, Biraro IA, Wyatt MA, Agbaji O, et al. Explaining adherence success in sub-Saharan Africa: an ethnographic study. PLoS Med 2009; 6:e1000011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Watt MH, Maman S, Earp JA, Eng E, Setel PW, Golin CE, et al. It's all the time in my mind’: facilitators of adherence to antiretroviral therapy in a Tanzanian setting. Soc Sci Med 2009; 68:1793–1800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Weiser SD, Tuller DM, Frongillo EA, Senkungu J, Mukiibi N, Bangsberg DR. Food insecurity as a barrier to sustained antiretroviral therapy adherence in Uganda. PLoS One 2010; 5:e10340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Woolgar HL, Mayers PM. The perceived benefit of the disability grant for persons living with HIV in an informal settlement community in the Western Cape, South Africa. J Assoc Nurses AIDS Care 2014; 25:589–602. [DOI] [PubMed] [Google Scholar]
- 99.Zunner B, Dworkin SL, Neylan TC, Bukusi EA, Oyaro P, Cohen CR, et al. HIV, violence and women: unmet mental healthcare needs. J Affect Disord 2015; 174:619–626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Alemu H, Haile Mariam D, Tsui AO, Shewamare A. Correlates of highly active antiretroviral therapy adherence among urban Ethiopian clients. Afr J AIDS Res 2011; 10:263–270. [DOI] [PubMed] [Google Scholar]
- 101.Amberbir A, Woldemichael K, Getachew S, Girma B, Deribe K. Predictors of adherence to antiretroviral therapy among HIV-infected persons: a prospective study in Southwest Ethiopia. BMC Public Health 2008; 8:265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Avong YK, van Wyk B, Njab J, Abimiku AG, Ndembi N, Okuma J, et al. Adherence to anti-retroviral therapy in north central Nigeria. Curr HIV Res 2015; 13:268–278. [DOI] [PubMed] [Google Scholar]
- 103.Bajunirwe F, Arts EJ, Tisch DJ, King CH, Debanne SM, Sethi AK. Adherence and treatment response among HIV-1-infected adults receiving antiretroviral therapy in a rural government hospital in southwestern Uganda. J Int Assoc Physicians AIDS Care 2009; 8:139–147. [DOI] [PubMed] [Google Scholar]
- 104.Benzekri NA, Sambou J, Diaw B, Sall EHI, Sall F, Niang A, et al. High prevalence of severe food insecurity and malnutrition among HIV-infected adults in Senegal, West Africa. PLoS One 2015; 10:e0141819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Bhat VG, Ramburuth M, Singh M, Titi O, Antony AP, Chiya L, et al. Factors associated with poor adherence to antiretroviral therapy in patients attending a rural health centre in South Africa. Eur J Clin Microbiol Infect Dis 2010; 29:947–953. [DOI] [PubMed] [Google Scholar]
- 106.Byakika-Tusiime J, Oyugi JH, Tumwikirize WA, Katabira ET, Mugyenyi PN, Bangsberg DR. Adherence to HIV antiretroviral therapy in HIV+ Ugandan patients purchasing therapy. Int J STD AIDS 2005; 16:38–41. [DOI] [PubMed] [Google Scholar]
- 107.Chabikuli NO, Datonye DO, Nachega J, Ansong D. Adherence to antiretroviral therapy, virologic failure and workload at the Rustenburg Provincial Hospital. South Afr Fam Pract 2010; 52:350–355. [Google Scholar]
- 108.Crankshaw T, Corless IB, Giddy J, Nicholas PK, Eichbaum Q, Butler LM. Exploring the patterns of use and the feasibility of using cellular phones for clinic appointment reminders and adherence messages in an antiretroviral treatment clinic, Durban, South Africa. AIDS Pat Care STDs 2010; 24:729–734. [DOI] [PubMed] [Google Scholar]
- 109.Demessie R, Mekonnen A, Amogne W, Shibeshi W. Knowledge and adherence to antiretroviral therapy among adult people living with HIV/AIDS at Tikur Anbessa Specialized Hospital, Ethiopia. Int J Basic Clin Pharmacol 2014; 3:320–330. [Google Scholar]
- 110.Dewing S, Mathews C, Lurie M, Kagee A, Padayachee T, Lombard C. Predictors of poor adherence among people on antiretroviral treatment in Cape Town, South Africa: a case-control study. AIDS Care 2015; 27:342–349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Do NT, Phiri K, Bussmann H, Gaolathe T, Marlink RG, Wester CW. Psychosocial factors affecting medication adherence among HIV-1 infected adults receiving combination antiretroviral therapy (cART) in Botswana. AIDS Res Hum Retroviruses 2010; 26:685–691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Dyrehave C, Rasmussen DN, Hønge BL, Jespersen S, Correia FG, Medina C, et al. Nonadherence is associated with lack of HIV-related knowledge: a cross-sectional study among HIV-infected individuals in Guinea-Bissau. J Int Assoc Provid AIDS Care 2016; 15:350–358. [DOI] [PubMed] [Google Scholar]
- 113.Ebuy H, Yebyo H, Alemayehu M. Level of adherence and predictors of adherence to the Option B+ PMTCT programme in Tigray, northern Ethiopia. Int J Infect Dis 2015; 33:123–129. [DOI] [PubMed] [Google Scholar]
- 114.Eholie SP, Tanon A, Polneau S, Ouiminga M, Djadji A, Kangah-Koffi C, et al. Field adherence to highly active antiretroviral therapy in HIV-infected adults in Abidjan, Cote d’Ivoire. J Acquir Immune Defic Syndr 2007; 45:355–358. [DOI] [PubMed] [Google Scholar]
- 115.Elul B, Basinga P, Nuwagaba-Biribonwoha H, Saito S, Horowitz D, Nash D, et al. High levels of adherence and viral suppression in a nationally representative sample of HIV-infected adults on antiretroviral therapy for 6, 12 and 18 months in Rwanda. PLoS One 2013; 8:e53586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Essomba EN, Adiogo D, Koum DC, Amang B, Lehman LG, Coppieters Y. [Factors associated with nonadherence of adults infected with HIV on antiretroviral therapy in a referral hospital in Douala]. Pan Afr Med J 2015; 20:412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Eyassu MA. Adherence to antiretroviral therapy among HIV and AIDS patients at the Kwa-Thema Clinic in the Gauteng Province, South Africa [Master's thesis]. University of Limpopo; 2015. http://ulspace.ul.ac.za/handle/10386/1218 [Accessed 25 May 2016]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Garang PG, Odoi RA, Kalyango JN. Adherence to antiretroviral therapy in conflict areas: a study among patients receiving treatment from Lacor Hospital, Uganda. AIDS Patient Care STDs 2009; 23:743–747. [DOI] [PubMed] [Google Scholar]
- 119.Georgette N, Siedner MJ, Zanoni B, Sibaya T, Petty CR, Carpenter S, et al. The acceptability and perceived usefulness of a weekly clinical SMS program to promote hiv antiretroviral medication adherence in Kwazulu-Natal, South Africa. AIDS Behav 2016; 20:2629–2638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Goar SG, Audu MD, Aagbir M, Matawal B. Substance abuse and adherence to antiretroviral therapy among patients attending clinic at a specialist hospital in Jos, Nigeria. Afr J Drug Alcohol Studies 2015; 14:37–47. [Google Scholar]
- 121.Guiro AK, Traore A, Somda A, Huang SL. Attitudes and practices towards HAART among people living with HIV/AIDS in a resource-limited setting in northern Burkina Faso. Public Health 2011; 125:784–790. [DOI] [PubMed] [Google Scholar]
- 122.Habib AG, Abdulmumini M, Dalhat MM, Hamza M, Iliyasu G. Anti-retroviral therapy among HIV infected travelers to Hajj Pilgrimage. J Travel Med 2010; 17:176–181. [DOI] [PubMed] [Google Scholar]
- 123.Hong SY, Fanelli TJ, Jonas A, Gweshe J, Tjituka F, Sheehan HM, et al. Household food insecurity associated with antiretroviral therapy adherence among HIV-infected patients in Windhoek, Namibia. J Acquir Immune Defic Syndr 2014; 67:e115–e122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Jaquet A, Ekouevi DK, Bashi J, Aboubakrine M, Messou E, Maiga M, et al. Alcohol use and nonadherence to antiretroviral therapy in HIV-infected patients in West Africa. Addiction 2010; 105:1416–1421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Jeneke JM. The effect of poor adherence to treatment of people living with HIV/AIDS [Master's thesis]. University of Stellenbosch; 2011. http://scholar.sun.ac.za/handle/10019.1/6848 [Accessed 25 May 2016]. [Google Scholar]
- 126.Kamau TM, Olsen VG, Zipp GP, Clark M. The effectiveness of social resource intervention to promote adherence to HIV medication in a multidisciplinary care setting in Kenya. Int J STD AIDS 2012; 23:843–848. [DOI] [PubMed] [Google Scholar]
- 127.Ketema AK, Weret ZS. Assessment of adherence to highly active antiretroviral therapy and associated factors among people living with HIV at Debrebrihan Referral Hospital and Health Center, northeast Ethiopia: a cross-sectional study. HIV/AIDS Res Palliat Care 2015; 7:75–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Kingori C, Reece M, Obeng S, Murray M, Shacham E, Dodge B, et al. Impact of internalized stigma on HIV prevention behaviors among HIV-infected individuals seeking HIV care in Kenya. AIDS Patient Care STDs 2012; 26:761–768. [DOI] [PubMed] [Google Scholar]
- 129.Kip E, Ehlers VJ, van der Wal DM. Patients’ adherence to anti-retroviral therapy in Botswana. J Nurs Scholarsh 2009; 41:149–157. [DOI] [PubMed] [Google Scholar]
- 130.Koole O, Denison JA, Menten J, Tsui S, Wabwire-Mangen F, Kwesigabo G, et al. Reasons for missing antiretroviral therapy: results from a multicountry study in Tanzania, Uganda, and Zambia. PLoS One 2016; 11:e0147309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Kunutsor S, Evans M, Thoulass J, Walley J, Katabira E, Newell JN, et al. Ascertaining baseline levels of antiretroviral therapy adherence in Uganda: a multimethod approach. J Acquir Immune Defic Syndr 2010; 55:221–224. [DOI] [PubMed] [Google Scholar]
- 132.Kyajja R, Muliira JK, Ayebare E. Personal coping strategies for managing the side effects of antiretroviral therapy among patients at an HIV/AIDS clinic in Uganda. Afr J AIDS Res 2010; 9:205–211. [DOI] [PubMed] [Google Scholar]
- 133.Lencha B, Hasen K, Getachew T, Abdi M, Habtamu M. Adherence to antiretroviral therapy and associated factors among people living with HIV/AIDS at Gobba Hospital, Southeast Ethiopia: an institutional based study. Qual Primary Care 2015; 23:336–341. [Google Scholar]
- 134.Letta S, Demissie A, Oljira L, Dessie Y. Factors associated with adherence to Antiretroviral Therapy (ART) among adult people living with HIV and attending their clinical care, Eastern Ethiopia HIV/AIDS. BMC Int Health Human Rights 2015; 15:33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Malangu NG. Self-reported adverse effects as barriers to adherence to antiretroviral therapy in HIV-infected patients in Pretoria. South Afr Fam Pract 2008; 50:49–49b. [Google Scholar]
- 136.Markos E, Worku A, Davey G. Adherence to ART in PLWHA and Yirgalem Hospital, South Ethiopia. Ethiopian J Health Develop 2009; 22:174–179. [Google Scholar]
- 137.Mbopi-Kéou F-X, Monebenimp F. [Study of factors related to adherence to antiretroviral therapy among patients followed at HIV/AIDS Unit in the District Hospital of Dschang Cameroon]. Pan Afr Med J 2012; 12:55. [PMC free article] [PubMed] [Google Scholar]
- 138.Moremi GS. Barriers to antiretroviral adherence of HIV/AIDS patients under the Wellness Programme in Mogwase Health Centre [Master's thesis]. Stellenbosch University; 2012. http://scholar.sun.ac.za/handle/10019.1/20016 [Accessed 25 May 2016]. [Google Scholar]
- 139.Musumari PM, Wouters E, Kayembe PK, Nzita MK, Mbikayi SM, Suguimoto SP, et al. Food insecurity is associated with increased risk of nonadherence to antiretroviral therapy among HIV-infected adults in the Democratic Republic of Congo: a cross-sectional study. PLoS One 2014; 9:e85327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Nduaguba O, Soremekun R, Olugbake O, Barner JC. The relationship between patient-related factors and medication adherence among Nigerian patients taking highly active antiretroviral therapy. Value Health 2015; 18:A241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Nghoshi S. Assessment of determinants and levels of adherence to antiretroviral therapy in HIV-infected people in Opuwo district, Kunene region, Namibia [Master's thesis]. University of Namibia; 2016. http://41.205.129.132/handle/11070/1703 [Accessed 25 May 2016]. [Google Scholar]
- 142.Nozaki I, Dube C, Kakimoto K, Yamada N, Simpungwe JB. Social factors affecting ART adherence in rural settings in Zambia. AIDS Care 2011; 23:831–838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Nwauche CA, Erhabor O, Ejele OA, Akani CI. Adherence to antiretroviral therapy among HIV-infected subjects in a resource-limited setting in the Niger Delta of Nigeria. Afr J Health Sci 2006; 13:13–17. [Google Scholar]
- 144.Ohene SA, Addo NA, Zigah F, Newman M, Lartey M, Romero MA, et al. Evaluation of antiretroviral therapy (ART) provision in an early cohort of patients initiating ART in Ghana. Pan Afr Med J 2013; 16:117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Oku AO, Owoaje ET, Ige OK, Oyo-ita A. Prevalence and determinants of adherence to HAART amongst PLHIV in a tertiary health facility in south-south Nigeria. BMC Infect Dis 2013; 13:401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Oku AO, Owoaje ET, Oku OO, Monjok E. Prevalence and determinants of adherence to highly active antiretroviral therapy amongst people living with HIV/AIDS in a rural setting in south-south Nigeria. Afr J Reprod Health 2014; 18:133–143. [PubMed] [Google Scholar]
- 147.Omole MK, Adisa R. Investigation of factors affecting medication adherence among people living with HIV/AIDs under Nongovernmental organization in Ibadan city, Nigeria. J Pharm Biomed Sci 2012; 21:1–5. [Google Scholar]
- 148.Onyango DO. Barriers to antiretroviral treatment adherence among HIV infected tuberculosis patients in Jaramogi Oginga Odinga Teaching and Referral Hospital Kisumu, Kenya [Master's thesis]. University of Nairobi; 2013. http://erepository.uonbi.ac.ke/handle/11295/56548 [Accessed 25 May 2016]. [Google Scholar]
- 149.Oumar AA, Dao S, Diamoutene A, Coulibaly S, Koumare B, Maiga II, et al. [Factors associated with antiretroviaral treatment observance at Point ‘G’ hospital] [French]. Le Mali Med 2007; 22:18–21. [PubMed] [Google Scholar]
- 150.Oyore J, Mwanzo I, Orago A, Odhiambo-Otieno G. Determinants of adherence to antiretroviral therapy (ART) among patients attending public and private health facilities in Nairobi, Kenya. J AIDS HIV Res Vol 2013; 5:70–74. [Google Scholar]
- 151.Pefura-Yone EW, Soh E, Kengne AP, Balkissou AD, Kuaban C. Nonadherence to antiretroviral therapy in Yaounde: prevalence, determinants and the concordance of two screening criteria. J Infect Public Health 2013; 6:307–315. [DOI] [PubMed] [Google Scholar]
- 152.Peltzer K, Preez NF, Ramlagan S, Fomundam H, Anderson J. Traditional complementary and alternative medicine and antiretroviral treatment adherence among HIV patients in Kwazulu-Natal, South Africa. Afr J Tradit Complement Altern Med 2010; 7:125–137. [PMC free article] [PubMed] [Google Scholar]
- 153.Potchoo Y, Tchamdja K, Balogou A, Pitche VP, Guissou IP, Kassang EK. Knowledge and adherence to antiretroviral therapy among adult people living with HIV/AIDS treated in the healthcare centers of the association ‘Espoir Vie Togo’ in Togo, West Africa. BMC Clin Pharmacol 2010; 10:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Salami AK, Fadeyi A, Ogunmodede JA, Desalu O. Factors influencing adherence to antiretroviral medication in Ilorin, Nigeria. J Int Assoc Physicians AIDS Care 2010; 9:191–195. [DOI] [PubMed] [Google Scholar]
- 155.Sam OB. Factors that constrain adherence to antiretroviral therapy among HIV positive patients in the Sekondi-Takoradi Metropolis [Master's thesis]. Kwame Nkrumah University of Science and Technology, Ghana; 2015. http://ir.knust.edu.gh/handle/123456789/7724 [Accessed 25 May 2016]. [Google Scholar]
- 156.Sasaki Y, Kakimoto K, Dube C, Sikazwe I, Moyo C, Syakantu G, et al. Adherence to antiretroviral therapy (ART) during the early months of treatment in rural Zambia: influence of demographic characteristics and social surroundings of patients. Ann Clin Microbiol Antimicrob 2012; 11:34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Senkomago V, Guwatudde D, Breda M, Khoshnood K. Barriers to antiretroviral adherence in HIV-positive patients receiving free medication in Kayunga, Uganda. AIDS Care 2011; 23:1246–1253. [DOI] [PubMed] [Google Scholar]
- 158.Talam NC, Gatongi P, Rotich J, Kimaiyo S. Factors affecting antiretroviral drug adherence among HIV/AIDS adult patients attending HIV/AIDS clinic at Moi Teaching and Referral Hospital, Eldoret, Kenya. East Afr J Public Health 2008; 5:74–78. [PubMed] [Google Scholar]
- 159.Tessema B, Biadglegne F, Mulu A, Getachew A, Emmrich F, Sack U. Magnitude and determinants of nonadherence and nonreadiness to highly active antiretroviral therapy among people living with HIV/AIDS in Northwest Ethiopia: a cross - sectional study. AIDS Res Ther 2010; 7:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Tsega B, Srikanth BA, Shewamene Z. Determinants of nonadherence to antiretroviral therapy in adult hospitalized patients, Northwest Ethiopia. Patient Prefer Adherence 2015; 9:373–380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Van Oosterhout JJ, Bodasing N, Kumwenda JJ, Nyirenda C, Mallewa J, Cleary PR, et al. Evaluation of antiretroviral therapy results in a resource-poor setting in Blantyre, Malawi. Trop Med Int Health 2005; 10:464–470. [DOI] [PubMed] [Google Scholar]
- 162.Wakibi SN, Ng’ang’a ZW, Mbugua GG. Factors associated with nonadherence to highly active antiretroviral therapy in Nairobi, Kenya. AIDS Res Ther 2011; 8:43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Watt MH, Maman S, Golin CE, Earp JA, Eng E, Bangdiwala SI, et al. Factors associated with self-reported adherence to antiretroviral therapy in a Tanzanian setting. AIDS Care 2010; 22:381–389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Weidle PJ, Wamai N, Solberg P, Liechty C, Sendagala S, Were W, et al. Adherence to antiretroviral therapy in a home-based AIDS care programme in rural Uganda. Lancet 2006; 368:1587–1594. [DOI] [PubMed] [Google Scholar]
- 165.Kekwaletswe CT, Morojele NK. Alcohol use, antiretroviral therapy adherence, and preferences regarding an alcohol-focused adherence intervention in patients with human immunodeficiency virus. Patient Prefer Adherence 2014; 8:401–413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Tadesse S, Tadesse A, Wubshet M. Adherence to antiretroviral treatment and associated factors among people living with HIV/AIDS in Northwest Ethiopia. J Trop Dis 2014; 2:1000133. [Google Scholar]
- 167.Amankwah AK. Facilitators and barriers to antiretroviral therapy adherence among HIV/AIDS patients: a multi-case study of Sunyani regional and municipal hospitals [Master's thesis]. University of Ghana; 2015. http://ugspace.ug.edu.gh/handle/123456789/8158 [Accessed 25 May 2016]. [Google Scholar]
- 168.Jones D, Zulu I, Mumbi M, Chitalu N, Vamos S, Gomez J, et al. Strategies for living with the challenges of HIV and antiretroviral use in Zambia. Int Elect J Health Educ 2009; 12:1–18. [Google Scholar]
- 169.Sisay WA, Alemayehu AA. Determinants of adherence to antiretroviral therapy drugs in the phase of rapid scale-up of antiretroviral treatment in sub-Saharan Africa: the case of Ethiopia. In: Fetene GT, Mesfin R. Antiretroviral treatment in sub-Saharan Africa. Challenges and prospects. Ethiopia: Organisation for Social Science Research in Eastern and Southern Africa (OSSREA); 2013. pp. 87–112. [Google Scholar]
- 170.Vyankandondera J, Mitchell K, Asiimwe-Kateera B, Boer K, Mutwa P, Balinda J-P, et al. Antiretroviral therapy drug adherence in Rwanda: perspectives from patients and healthcare workers using a mixed-methods approach. AIDS Care 2013; 25:1504–1512. [DOI] [PubMed] [Google Scholar]
- 171.Lankowski AJ, Siedner MJ, Bangsberg DR, Tsai AC. Impact of geographic and transportation-related barriers on HIV outcomes in sub-Saharan Africa: a systematic review. AIDS Behav 2014; 18:1199–1223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172.Singer AW, Weiser SD, McCoy SI. Does food insecurity undermine adherence to antiretroviral therapy? A systematic review. AIDS Behav 2015; 19:1510–1526. [DOI] [PubMed] [Google Scholar]
- 173.Nakimuli-Mpungu E, Bass JK, Alexandre P, Mills EJ, Musisi S, Ram M, et al. Depression, alcohol use and adherence to antiretroviral therapy in sub-Saharan Africa: a systematic review. AIDS Behav 2012; 16:2101–2118. [DOI] [PubMed] [Google Scholar]
- 174.Kremer H, Ironson G. To tell or not to tell: why people with HIV share or don’t share with their physicians whether they are taking their medications as prescribed. AIDS Care 2006; 18:520–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175.Chesney MA, Ickovics J, Chambers D, Gifford A, Neidig J, Zwickl B, et al. Self-reported adherence to antiretroviral medications among participants in HIV clinical trials: the AACTG adherence instruments. AIDS Care 2000; 12:255–266. [DOI] [PubMed] [Google Scholar]
- 176.Coetzee B, Kagee A. The development of an inventory to assess the structural barriers to clinic attendance and pill-taking amongst users of antiretroviral therapy. AIDS Behav 2013; 17:319–328. [DOI] [PubMed] [Google Scholar]
- 177.Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care 1986; 24:67–74. [DOI] [PubMed] [Google Scholar]
- 178.Mannheimer S, Friedland G, Matts J, Child C, Chesney M. The consistency of adherence to antiretroviral therapy predicts biologic outcomes for human immunodeficiency virus—infected persons in clinical trials. Clin Infect Dis 2002; 34:1115–1121. [DOI] [PubMed] [Google Scholar]
- 179.Mannheimer S, Mukherjee R, Hirschhorn L, Dougherty J, Celano S, Ciccarone D, et al. The CASE adherence index: a novel method for measuring adherence to antiretroviral therapy. AIDS Care 2006; 18:853–861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180.Simoni JM, Kurth AE, Pearson CR, Pantalone DW, Merrill JO, Frick PA. Self-report measures of antiretroviral therapy adherence: a review with recommendations for HIV research and clinical management. AIDS Behav 2006; 10:227–245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Group ISS. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med 2015; 2015:795–807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182.Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med 2011; 365:493–505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183.Kulkarni SP, Shah KR, Sarma KV, Mahajan AP. Clinical uncertainties, health service challenges, and ethical complexities of HIV ‘test-and-treat’: a systematic review. Am J Public Health 2013; 103:e14–e23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184.Barnighausen T, Chaiyachati K, Chimbindi N, Peoples A, Haberer J, Newell ML. Interventions to increase antiretroviral adherence in sub-Saharan Africa: a systematic review of evaluation studies. Lancet Infect Dis 2011; 11:942–951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185.Govindasamy D, Ford N, Kranzer K. Risk factors, barriers and facilitators for linkage to antiretroviral therapy care: a systematic review. AIDS 2012; 26:2059–2067. [DOI] [PubMed] [Google Scholar]
- 186.Catz SL, Kelly JA, Bogart LM, Benotsch EG, McAuliffe TL. Patterns, correlates, and barriers to medication adherence among persons prescribed new treatments for HIV disease. Health Psychol 2000; 19:124. [PubMed] [Google Scholar]
- 187.Coetzee B, Kagee A. The development of an inventory to assess the structural barriers to clinic attendance and pill-taking amongst users of antiretroviral therapy. AIDS Behav 2013; 17:319–328. [DOI] [PubMed] [Google Scholar]
- 188.The LifeWindows Project Team. The LifeWindows Information Motivation Behavioral Skills ART Adherence Questionnaire (LW-IMB-AAQ) Center for Health, Intervention, and Prevention. University of Connecticut; 2006. http://chipcontent.chip.uconn.edu/chipweb/documents/Research/F_LWIMBARTQuestionnaire.pdf [Accessed 30 May 2016]. [Google Scholar]
- 189.Svarstad BL, Chewning BA, Sleath BL, Claesson C. The Brief Medication Questionnaire: a tool for screening patient adherence and barriers to adherence. Patient Educ Couns 1999; 37:113–124. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.