

Abstract
It is unusual but not uncommon for foreign bodies to be missed at bronchoscopy. This case report highlights the importance of the clinical history in the diagnosis of aspirated foreign bodies and the usefulness of chest imaging modalities. A 6-year-old boy presented with recurrent breathlessness and cough of 2 months. He was said to have aspirated the base cap of a pen at about the time symptoms started. He had two sessions of rigid bronchoscopy and a session of flexible bronchoscopy at three different hospitals. He had an initial rigid bronchoscopy which failed to show the foreign body (FB). A chest computerized tomographic scan demonstrated the FB, which was retrieved at combined flexible/rigid bronchoscopy. Although rigid bronchoscopy is the gold standard for managing airway foreign bodies, there remains a false negative rate for this procedure and where necessary, appropriate imaging may compliment rigid bronchoscopy, especially where there is some confusion.
Keywords: Bronchoscopy, foreign body, trachea
Introduction
Foreign body (FB) aspiration is common among children.[1] If not extracted early, they may lead to problems including pneumonia, granuloma, and mucosal erosions which may require hospitalization.[2] Severe complications including pneumomediastinum, pneumothorax, total atelectasis, and FB dislodgement sometimes requiring admission and thoracotomy[3] have also been reported.
Since invention, bronchoscopy has become the gold standard in the diagnosis and extraction of airway FB.[4] Foreign bodies may be missed at bronchoscopy if covered by granulation tissue or multiple with the remaining ones not searched for. This article reports the case of a 6-year-old boy who had three sequential rigid bronchoscopies at three different hospitals which failed to identify the FB. It was finally identified on a chest computerized tomography (CT) scan before extraction at the final rigid bronchoscopy.
Case Report
A 6-year-old boy presented to our hospital with recurring breathlessness and cough of 2 months. He told his parents he accidentally aspirated the base cap of a pen, subsequently developing breathlessness and cough. He was immediately taken to a private health facility where he had an emergency rigid bronchoscopy, but the FB was not found. He was given medications, got slightly better, and discharged home. He re-presented at two tertiary hospitals where repeat bronchoscopies were performed 4 weeks apart which failed to demonstrate any FB. He was diagnosed to have asthma, treated accordingly, and improved symptomatically on bronchodilators.
He was admitted at our hospital following symptom recurrence. A chest x-ray done at presentation appeared normal and repeat rigid bronchoscopy was performed at his parents’ request. A pedunculated subglottic mass was identified and excised. The patient improved remarkably and was discharged home 24 h later. Histology of the mass was reported as fibrocartilaginous tissue devoid of epithelium.
About 2 weeks later, he re-presented with severe respiratory distress. A neck and chest CT was requested which demonstrated a thin mass just above and straddling the carina [Figure 1].
Figure 1.
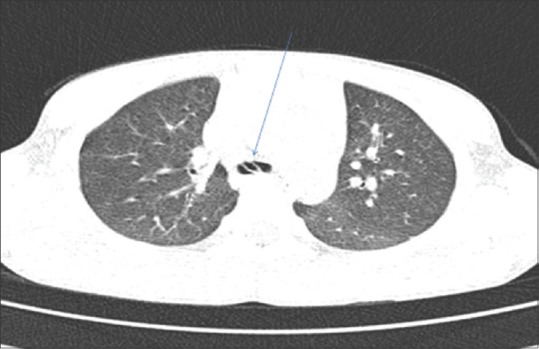
Chest computerized tomography scan showing foreign body located just above the carina (straight arrow)
He had repeat combined flexible and rigid bronchoscopy which identified the FB covered with granulation tissue which was then successfully extracted [Figures 2 and 3]. Postbronchoscopy recovery was uneventful and he was discharged home 24 h later with complete symptom resolution.
Figure 2.

Object removed at bronchoscopy
Figure 3.

Object as seen in its unaltered state
Discussion
FB aspiration is common among children, especially males[5,6,7] and may have life-threatening complications if unextracted.[8]
Since the discovery by Gustav Killian,[9] extraction of tracheobronchial FB has been accomplished with rigid bronchoscopy which is still considered as the gold standard[8,10] with thoracotomy and bronchotomy required in 1–3% of cases.[11] With improved instrumentation, flexible bronchoscopy is rapidly gaining use in airway FB extraction and is now considered by some authors as the first line in airway FB extraction.[12]
Diagnosis of FB aspiration in children is challenging, and there is often a delay in diagnosis and treatment due to factors including physician misdiagnosis, failure by caregivers to seek early medical attention, discharge against medical advice, and others.[13] Although challenging, several tools are available for diagnosis of tracheobronchial FB in children ranging from the patient's clinical presentation, chest X-rays, CT, magnetic resonance imaging, and endoscopy, each having its sensitivity and specificity. Endoscopy has the added advantage of FB visualization and extraction at the same time.
It is uncommon for tracheobronchial FB to be missed at endoscopy, and rarer still, for it to be missed at four consecutive endoscopies at four different centers. The expertise of the endoscopist and functionality of his equipment are important determinants of successful identification and retrieval of the FB. Other possible reasons why FB may be missed at bronchoscopy includes migration during bronchoscopy, especially with inert materials[11,14] when inflammation is minimal and growth of exuberant granulation tissue around the FB[15] which if not completely removed may result in it being missed at bronchoscopy. The surrounding granulation tissue around the FB in this patient may have thus contributed to it being missed. Although our patient had a single FB in the airway, there is a higher likelihood of FB being missed if they are multiple as reported by Gupta and Khanna.[16] Poor instrumentation leads generally to poor outcomes with bronchoscopy; there is, for example, a higher chance of missing a FB with a poor illumination system. The problems with inadequate instrumentation in many centers in our country have been discussed by Falase et al.[8] including widespread lack of video bronchoscopes and optical forceps in most centers. It is possible all these factors with the exception of multiple FB may have contributed to it being missed at four consecutive bronchoscopies. Improvements and acquisition of new bronchoscope technologies such as high-definition optical systems, optical forceps, and video bronchoscopes should reduce the likelihood of missed foreign bodies at bronchoscopy.
This case also highlights the importance of the clinical history in the diagnosis of tracheobronchial FB. Because of the potential problems that may be caused by undiagnosed tracheobronchial FB, every effort should be made to confirm or exclude them.[1] A history of witnessed aspiration by caregivers or children is important and may be sufficient reason to perform a bronchoscopy as between 73% and 98% of patients who had a FB at bronchoscopy had such a history as reported by Passàli et al.,[1,17,18] although Iversen and Klug reported a lower percentage correlation (43%)[19] and Yadav et al. 53.8%.[20] Choking and sudden cough in a child appear to be the most common symptoms associated with bronchoscopically proven FB[1,19,20] as seen in this patient.
The role of the chest CT scan also needs to be discussed as it helped in making the eventual diagnosis of tracheobronchial FB. With plain chest X-rays having a diagnostic accuracy of about 66% for tracheobronchial FB,[21] chest CT has a prominent role to play in the diagnosis of airway FB. Cohen in his study concluded that CT scans may be useful in selected cases of diagnostic dilemmas[22] and Hong et al.[23] reported a sensitivity of spiral CT of 100%, specificity of 66.7%, positive predictive value of 93.3%, and negative predictive value of 100% using virtual bronchoscopy (VB) while Abd El-Gawad et al.[24] reported a sensitivity of 94.4%, specificity of 75%, and accuracy of 90.4%. While we do not routinely do chest CT in patients with suspected tracheobronchial FB, we would consider a chest CT in patients with diagnostic dilemmas as suggested by Cohen based on our experience from this patient.
The advent of VB has improved the diagnostic accuracy of airway FB in children. VB is a noninvasive technique that provides an internal view of the trachea and major bronchi by three-dimensional reconstructions.[25] VB can provide the exact location of an FB. In a study detailing the role of VB in children with suspected FB involving sixty children,[26] rigid bronchoscopy confirmed the results of VB in 59 patients. In the remaining patient, a FB identified at VB was shown to be a thick mucus plug at rigid bronchoscopy. Adaletli et al.[27] also made similar findings concluding that in cases were no obstructive pathology was identified by multidetector CT and VB; bronchoscopy may not be clinically useful.
Conclusion
Diagnosis of tracheobronchial FB bodies in children may be difficult. A negative bronchoscopy usually should rule out foreign bodies. If symptoms however persist, a chest CT may greatly contribute in resolving the dilemma.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Passàli D, Lauriello M, Bellussi L, Passali GC, Passali FM, Gregori D. Foreign body inhalation in children: An update. Acta Otorhinolaryngol Ital. 2010;30:27–32. [PMC free article] [PubMed] [Google Scholar]
- 2.Rodríguez H, Cuestas G, Botto H, Nieto M, Cocciaglia A, Passali D, et al. Complications in children from foreign bodies in the airway. Acta Otorrinolaringol Esp. 2016;67:93–101. doi: 10.1016/j.otorri.2015.01.003. [DOI] [PubMed] [Google Scholar]
- 3.Oliveira CF, Almeida JF, Troster EJ, Vaz FA. Complications of tracheobronchial foreign body aspiration in children: Report of 5 cases and review of the literature. Rev Hosp Clin Fac Med Sao Paulo. 2002;57:108–11. doi: 10.1590/s0041-87812002000300005. [DOI] [PubMed] [Google Scholar]
- 4.Rodrigues AJ, Oliveira EQ, Scordamaglio PR, Gregório MG, Jacomelli M, Figueiredo VR. Flexible bronchoscopy as the first-choice method of removing foreign bodies from the airways of adults. J Bras Pneumol. 2012;38:315–20. doi: 10.1590/s1806-37132012000300006. [DOI] [PubMed] [Google Scholar]
- 5.Ahmed AO, Shuiabu IY. Inhaled foreign bodies in a paediatric population at AKTH Kano-Nigeria. Niger Med J. 2014;55:77–82. doi: 10.4103/0300-1652.128178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Adegboye V, Adebo OA. Epidemiology of tracheobronchial foreign bodies in Ibadan. Niger J Clin Pract. 2001;4:51–3. [Google Scholar]
- 7.Onotai L, Ebong ME. The pattern of foreign body impactions in the tracheobronchial tree in the University of Port Harcourt Teaching Hospital. Port Harcourt Med J. 2011;5:130–5. [Google Scholar]
- 8.Falase B, Sanusi M, Majekodunmi A, Ajose I, Oke D. Preliminary experience in the management of tracheobronchial foreign bodies in Lagos, Nigeria. Pan Afr Med J. 2013;15:31. doi: 10.11604/pamj.2013.15.31.2710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Becker HD. A short history of bronchoscopy. In: Ernst A, editor. Introduction to Bronchoscopy. Cambridge: Cambridge University Press; 2009. [Google Scholar]
- 10.Mallick MS. Tracheobronchial foreign body aspiration in children: A continuing diagnostic challenge. Afr J Paediatr Surg. 2014;11:225–8. doi: 10.4103/0189-6725.137330. [DOI] [PubMed] [Google Scholar]
- 11.Kikuchi R, Isowa N, Tokuyasu H, Kawasaki Y. Intraoperative migration of a nail from the left B10b to the main bronchus. Interact Cardiovasc Thorac Surg. 2007;6:92–3. doi: 10.1510/icvts.2006.144683. [DOI] [PubMed] [Google Scholar]
- 12.Tang LF, Xu YC, Wang YS, Wang CF, Zhu GH, Bao XE, et al. Airway foreign body removal by flexible bronchoscopy: Experience with 1027 children during 2000-2008. World J Pediatr. 2009;5:191–5. doi: 10.1007/s12519-009-0036-z. [DOI] [PubMed] [Google Scholar]
- 13.Saquib Mallick M, Rauf Khan A, Al-Bassam A. Late presentation of tracheobronchial foreign body aspiration in children. J Trop Pediatr. 2005;51:145–8. doi: 10.1093/tropej/fmh103. [DOI] [PubMed] [Google Scholar]
- 14.Oviawe O, Abhulimhen-Iyoha BI, Obaseki DE. Migrating foreign body in the tracheobronchial tree of childen: Report of two cases. Niger Postgrad Med J. 2011;18:154–7. [PubMed] [Google Scholar]
- 15.Fang YF, Hsieh MH, Chung FT, Huang YK, Chen GY, Lin SM, et al. Flexible bronchoscopy with multiple modalities for foreign body removal in adults. PLoS One. 2015;10:e0118993. doi: 10.1371/journal.pone.0118993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gupta SC, Khanna S. Multiple foreign bodies in the tracheobronchial tree. Indian J Otolaryngol Head Neck Surg. 1999;51(Suppl 1):51–4. doi: 10.1007/BF03001555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tong YH, Lau CC. Airway foreign body: A difficult and often neglected diagnosis in asthmatic child in emergency department. Hong Kong J Emerg Med. 2002;9:217–20. [Google Scholar]
- 18.Banerjee A, Rao KS, Khanna SK, Narayanan PS, Gupta BK, Sekar JC, et al. Laryngo-tracheo-bronchial foreign bodies in children. J Laryngol Otol. 1988;102:1029–32. doi: 10.1017/s0022215100107170. [DOI] [PubMed] [Google Scholar]
- 19.Iversen RH, Klug TE. Need for more clear parental recommendations regarding foreign body aspiration in children. Dan Med J. 2012;59:A4498. [PubMed] [Google Scholar]
- 20.Yadav SP, Singh J, Aggarwal N, Goel A. Airway foreign bodies in children: Experience of 132 cases. Singapore Med J. 2007;48:850–3. [PubMed] [Google Scholar]
- 21.Asif M, Haroon T, Qureshi WU, Jamil M, Malik S, Ghani R. Correlation of operative findings with pre-operative clinical signs and analysis of x-rays in patients with airway foreign bodies. J Ayub Med Coll Abbottabad. 2010;22:32–4. [PubMed] [Google Scholar]
- 22.Cohen S, Avital A, Godfrey S, Gross M, Kerem E, Springer C. Suspected foreign body inhalation in children: What are the indications for bronchoscopy? J Pediatr. 2009;155:276–80. doi: 10.1016/j.jpeds.2009.02.040. [DOI] [PubMed] [Google Scholar]
- 23.Hong SJ, Goo HW, Roh JL. Utility of spiral and cine CT scans in pediatric patients suspected of aspirating radiolucent foreign bodies. Otolaryngol Head Neck Surg. 2008;138:576–80. doi: 10.1016/j.otohns.2007.12.039. [DOI] [PubMed] [Google Scholar]
- 24.Abd El-Gawad EA, Ibrahim MA, Mubarak YS. Tracheobronchial foreign body aspiration in infants and children: Diagnostic utility of multidetector CT with emphasis on virtual bronchoscopy. Egypt J Radiol Nucl Med. 2014;45:1141–6. [Google Scholar]
- 25.Haliloglu M, Ciftci AO, Oto A, Gumus B, Tanyel FC, Senocak ME, et al. CT virtual bronchoscopy in the evaluation of children with suspected foreign body aspiration. Eur J Radiol. 2003;48:188–92. doi: 10.1016/S0720-048X(02)00295-4. [DOI] [PubMed] [Google Scholar]
- 26.Behera G, Tripathy N, Maru YK, Mundra RK, Gupta Y, Lodha M. Role of virtual bronchoscopy in children with a vegetable foreign body in the tracheobronchial tree. J Laryngol Otol. 2014;128:1078–83. doi: 10.1017/S0022215114002837. [DOI] [PubMed] [Google Scholar]
- 27.Adaletli I, Kurugoglu S, Ulus S, Ozer H, Elicevik M, Kantarci F, et al. Utilization of low-dose multidetector CT and virtual bronchoscopy in children with suspected foreign body aspiration. Pediatr Radiol. 2007;37:33–40. doi: 10.1007/s00247-006-0331-y. [DOI] [PubMed] [Google Scholar]