

Population-level survival has increased for a number of hematologic malignancies.1–3 Multiple myeloma, in particular, has seen improved survival both in clinical trials4–8 and on the population level.3,9–11 However, it is not known whether the changes in survival for myeloma have extended to other, less common plasma cell or plasmacytoid malignancies such as lymphoplasmacytic lymphoma (LPL, includes Waldenström’s macroglobulinemia (WM)), plasma cell leukemia (PCL), and solitary plasmacytoma (SP). Only a few population level studies of survival are available on LPL,12,13 PCL,14,15 and SP,16 with little information on changes in survival in the past decade.
Prior work on LPL demonstrates a good overall prognosis, with a relative survival (RS) of 78% in the United States of America (USA) from 2001 to 201017 and in Sweden from 2001 to 2005.13 In contrast, one previous study examining survival for patients with SP found no change in survival between 1992 to 1997 and 1998 to 2003.18
Until recently, population-level study of rare malignancies in Germany was difficult as most population-level data were obtained from the Saarland database, which is too small to allow detailed examination of rare cancers. In 2009, a collaborative effort between population-based German cancer registries and the German Cancer Research Center started. This effort has permitted the study of population-level survival in Germany for rare cancers.19,20
Herein, we examine survival for patients with rare plasma cell and plasmacytoid malignancies in Germany compared to that in the USA.
A detailed description of the cancer registries from which data were obtained has been published previously.19,20
ICD-10 codes and ICD-O-3 morphology codes restricted to malignant behavior were used to identify patients with a primary diagnosis of LPL (ICD-10 C88.0 and ICD-O-3 9671/9761), or SP (C90.2/C90.3 and 9731 (intraosseous) or 9734 (extraosseous)) from 1998 to 2012. Patients diagnosed with myeloma (C90.0 and 9732) were examined for comparison. To minimize miscategorization of cases, only cases where the ICD-10 and the ICD-O-3 code agreed were included. Case numbers for PCL were too small to allow for a valid analysis.
Mortality follow up was conducted throughout December 2012 by record linkage with population registries. Patients reported to the registry by death certificate only (DCO) were excluded from the analysis. For some registries, data were available starting only from later years.19,20
In order to compare population-level survival in Germany with survival in the USA, data from the Surveillance, Epidemiology, and End Results (SEER13) database were analyzed21 using the same inclusion criteria and time period as for patients from the German cancer registries.
Five-year RS estimates for the time period from 2003 to 2012 were calculated using period analysis,22 which provides more up-to-date survival estimates than traditional cohort based analysis.23 Period analysis has been previously demonstrated to closely predict the survival later observed for patients during a given period.24,25
Age-adjusted survival estimates were derived by computing weighted averages of age-specific survival estimates using weights according to the International Cancer Survival Standard26 and examined survival by major age groups and by sex. Differences in survival between patients in Germany and the USA were tested for statistical significance using model-based period analysis.27 In model-based analysis, the number of deaths were modeled as a function of the year of follow up, age group, and country by Poisson regression with the logarithm of the person-months at risk as offset.
Trends in survival were examined, comparing 5-year RS for 2003 to 2007 and 2008 to 2012. Differences in survival were tested for statistical significance using model-based period analysis including the following factors: year of follow up, age group, and period of diagnosis.27
RS was calculated as the ratio of observed survival to expected survival. Expected survival was estimated according to the Ederer II method28 using national life tables stratified by age, sex, and calendar year obtained from the German Federal Statistical Office29 (Germany) and sex-, age-, calendar year-, and race-specific life tables published by the Center for Disease Control (USA).30
All calculations were carried out with SAS software (version 9.4, SAS, Carey, NC, USA), using macros developed for standard and model-based period analysis.27,31 A P-value below 5% was considered significant.
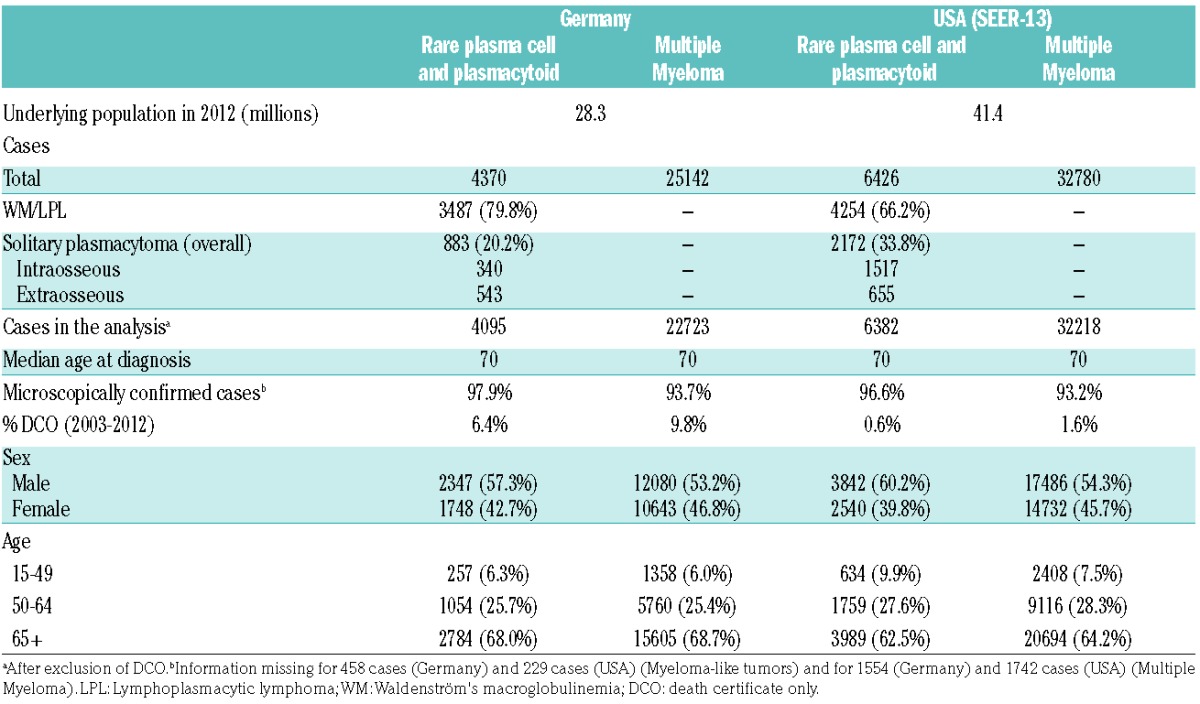
A total of 4,370 cases of patients with rare plasma cell diseases, excluding PCL, were identified in the German cancer database in the period 1998 to 2012 (Table 1). Of these, 6.4% were notified by DCO and were thus excluded. A total of 6,426 cases were identified in the SEER database, with 0.6% of cases excluded for DCO notification. LPL was the more common malignancy, accounting for 79.8% of cases in Germany and 66.2% of cases in the USA. In Germany, 38.5% of SP cases were intraosseous, in the USA, 69.8% were intraosseous. Myeloma was considerably more common, with case numbers of 22,723 and 32,218, respectively, in Germany and the USA (after exclusion of DCO cases). Median age at diagnosis was 70 for both countries.
Table 1.
Case numbers and characteristics of examined malignancies in Germany and the USA from 1998 to 2012
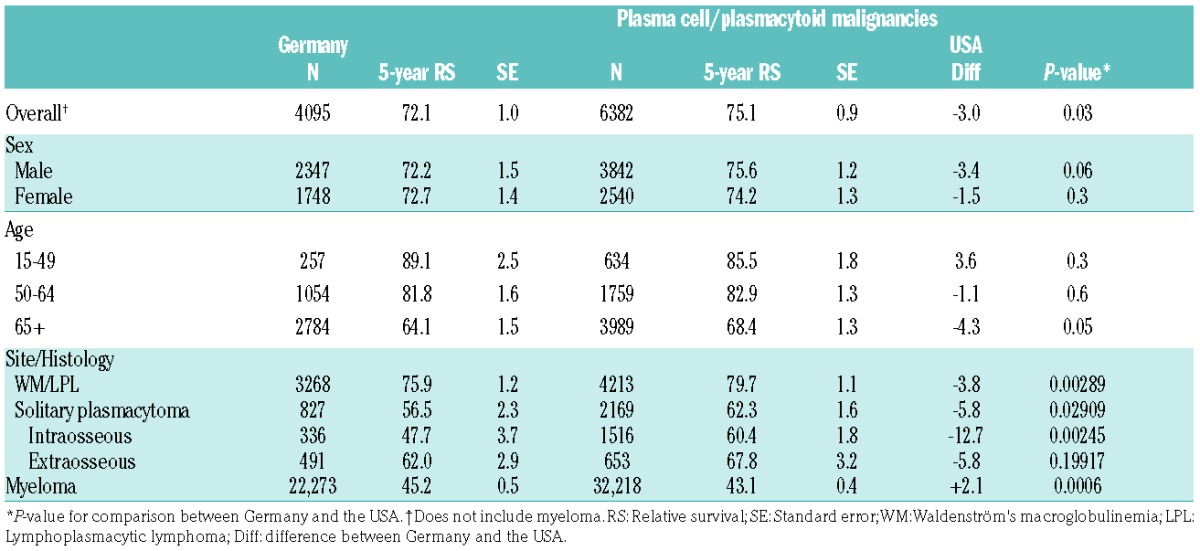
Overall age-adjusted 5-year RS of patients with rare plasma cell and plasmacytoid conditions in Germany was 72.1%, but survival varied by specific condition (Table 2). Survival estimates were similar for men and women. Survival decreased with age in both countries, but a steeper decline was observed in Germany. Five-year RS for LPL was 75.9% in Germany. Patients with SP had a 5-year RS of 56.5%, with a lower survival for intraosseous (47.7%) versus extraosseous (62.0%). Five-year RS for patients with LPL were similar in the USA (79.7%). Five-year RS estimates for patients with SP were higher at 62.3%, with survival for patients with intraosseous SP at 60.4% and extraosseous SP at 67.8%. Five-year RS for patients with myeloma was 45.2% in Germany and 43.1% in the USA.
Table 2.
Five year age-adjusted and age-specific relative survival by diagnosis, age, and location from 2003 to 2012.
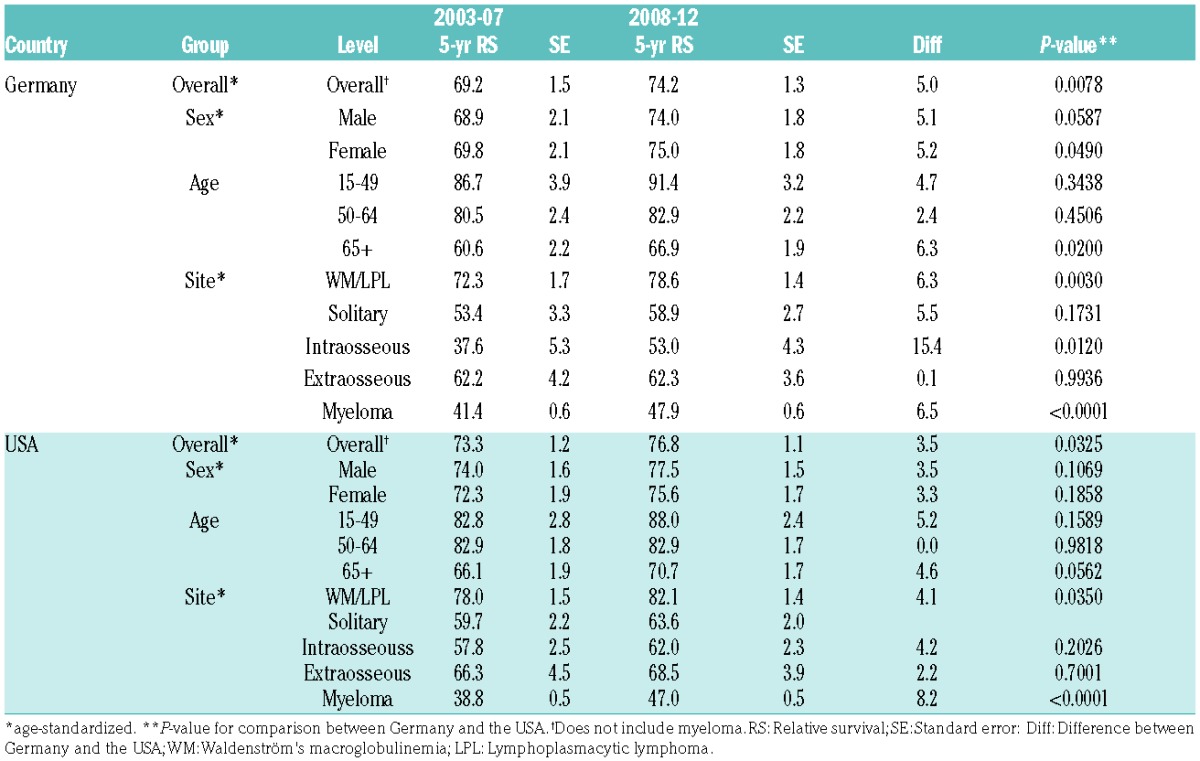
Survival trends were examined between 2003 to 2007 and 2008 to 2012 (Table 3). Five-year age-adjusted RS for patients with LPL/SP increased in Germany, from 69.2% between 2003 and 2007 to 74.2% in the period 2008 to 2012. In the USA, overall 5-year age-adjusted RS for these conditions went from 73.3% to 76.8%. Similar increases were seen for both men and women. The largest increase in survival was observed for patients aged 65+ in Germany (+6.3% units). When individual conditions were considered, rather substantial increases were seen in Germany, at +6.3% units for LPL and +5.5% units for SP. The increase in survival was mainly due to increases in survival for patients with intraosseous SP, for whom an increase of +15.4% units was observed. In the USA, a trend towards increased survival was likewise observed, at +4.1% units for LPL and +3.9% units for SP, with small increases observed for both subtypes. Survival for patients with myeloma increased by 6.5% units in Germany and 8.2% units in the USA.
Table 3.
Changes in age-standardized and age-specific 5-year survival for rare plasma cell and plasmacytoid malignancies between 2003 and 2007 and 2008 and 2012 by country, sex, age, and histology.
Plasma cell or lymphoplasmacytic malignancies occur in both Germany and the USA, with incidences of <1/100,000. Five-year RS increased for patients with LPL in both Germany and the USA. Smaller increases were observed for SP.
Treatment for patients with myeloma has changed greatly, with new medications becoming available in the first4–8 and second decades of the 21st century.32–34
While treatment options have not changed as drastically for LPL, new treatment options have recently become available. Rituximab, proteasome inhibitors, and stem cell transplantation have been successfully incorporated into the treatment of WM/LPL.35–37
The treatment for SP continues to be radiation +/− surgery.38,39 Although excellent results are obtained for most patients, a certain number will progress to myeloma.40 Conversely, because myeloma often develops in those patients who previously had SP, improvements in the treatment of myeloma may improve the long-term survival for patients initially diagnosed with SP. Improved imaging modalities to visualize SP may result in earlier diagnosis.41 Finally, the observed survival differences might be related to better case identification.
Small differences in survival between Germany and the USA were observed. The reasons for these differences cannot be definitively stated here as the databases lack information on disease, treatment, and patient characteristics. Examination of more granular data may be helpful in distinguishing the etiology of the differences.
Strengths of our study include the use of two very large cancer databases which allowed for the examination of population level survival in these rare cancers. In addition, the use of period analysis allowed for the most up-to-date evaluation of survival possible.
When evaluating our results, some limitations should be considered. First, even with the use of the large combined German and SEER databases, the case numbers were small. Second, no information on chemotherapy is included in either database. Third, the DCO rate is higher in Germany, potentially leading to an overestimation of survival in Germany. We addressed this issue by calculating a plausibility range.42,43 The plausibility range for 5-year RS was 63.6–68.6% for those with LPL/SP and 42.3–45.2% for those with myeloma, suggesting a minimal effect.
Finally, there is a risk of miscoding of these malignancies. We attempted to minimize this risk by using both ICD-10 and ICD-O-3 codes and including only cases where the ICD-10 and ICD-O-3 codes agreed, but cannot rule out the possibility of misclassification in both fields.
In conclusion, 5-year survival for LPL and SP has increased in the early 21st century, but not to the same extent that it has for myeloma. Only small differences in survival were observed between Germany and the USA. Further research into the optimal treatment for these malignancies may result in better survival.
Supplementary Material
Acknowledgments
Members of the GEKID Cancer Survival Working Group: Karla Geiss, Martin Meyer (Cancer Registry of Bavaria), Andrea Eberle, Sabine Luttmann (Cancer Registry of Bremen), Roland Stabenow (Cancer Registry of Berlin and the New Federal States), Stefan Hentschel, Alice Nennecke (Hamburg Cancer Registry); Joachim Kieschke, Eunice Sirri (Cancer Registry of Lower Saxony), Bernd Holleczek (Saarland Cancer Registry), Katharina Emrich (Cancer Registry of Rhineland-Palatinate), Hiltraud Kajüter, Volkmar Mattauch (Cancer Registry of North Rhine-Westphalia), Alexander Katalinic, Nora Eismann (Cancer Registry of Schleswig-Holstein), Benjamin Barnes, Klaus Kraywinkel (Robert Koch Institute, Berlin), Hermann Brenner, Lina Jansen, and Janick Weberpals (German Cancer Research Center).
Footnotes
Funding: this work was supported in part by a grant from the German Cancer Aid (Deutsche Krebshilfe, no. 108257) and a visiting scientist grant from the German Cancer Research Center to DP.
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Pulte D, Redaniel MT, Jansen L, Brenner H, Jeffreys M. Recent trends in survival of adult patients with acute leukemia: overall improvements, but persistent and partly increasing disparity in survival of patients from minority groups. Haematologica. 2013;98(2):222–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pulte D, Jansen L, Castro FA, Brenner H. Changes in the survival of older patients with hematologic malignancies in the early 21st century. Cancer. 2016;122(13):2031–2040. [DOI] [PubMed] [Google Scholar]
- 3.Sant M, Minicozzi P, Mounier M, et al. Surival for haematological malignancies in Europe between 1997 and 2008 by region and age: results of EUROCARE-5, a population-based study. Lancet Oncol. 2014;15(9):931–942. [DOI] [PubMed] [Google Scholar]
- 4.Weber DM, Chen C, Niesvizky R, et al. Lenalidomide plus dexamethasone for relapsed multiple myeloma in North America. N Engl J Med. 2007;357(2):2133–2142. [DOI] [PubMed] [Google Scholar]
- 5.Palumbo A, Bringhen S, Larocca A, et al. Brotezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: updated follow-up and improved survival. J Clin Oncol. 2014;32(7):634–640 [DOI] [PubMed] [Google Scholar]
- 6.Nooka AK, Kaufman JL, Behera M, et al. Bortezomib-containing induction regimens in transplant-eligible myeloma patients: a meta-analysis of phase 3 randomized clinical trials. Cancer. 2013; 119(23):4119–4128. [DOI] [PubMed] [Google Scholar]
- 7.Mateos MV, Hernandez MT, Giraldo P, et al. lenalidomide plus dexamethasone for high-risk smoldering multiple myeloma. N Engl J Med. 2013;369(5):438–447. [DOI] [PubMed] [Google Scholar]
- 8.San Miguel JF, Schlag R, Khuageva NK, et al. Bortezomib plus melphelan and prednisone for initial treatment of multiple myeloma. N Engl J Med. 2008;359(9):906–917. [DOI] [PubMed] [Google Scholar]
- 9.Pulte D, Jansen L, Castro FA, et al. Trends in survival of multiple myeloma patients in Germany and the United States in the first decade of the 21st century. Br J Haematol. 2015;171(2):189–196. [DOI] [PubMed] [Google Scholar]
- 10.Pulte D, Redaniel MT, Brenner H, Jansen L, Jeffreys M. Recent improvement in survival of patients with multiple myeloma: variation by ethnicity. Leuk Lymphoma. 2014;55(5):1083–1089. [DOI] [PubMed] [Google Scholar]
- 11.Fujisawa M, Suehara Y, Fukumoto K, Takeuchi M, Matsue K. Changes in survival rate of multiple myeloma after introduction of bortezomib: a single institution experience over 20 years. Ann Hematol. 2016;95(1):63–72. [DOI] [PubMed] [Google Scholar]
- 12.Castillo JJ, Olszewski AJ, Kanan S, Meid K, Hunter ZR, Treon SP. Overall survival and competing risks of death in patients with Waldenström macroglobulinemia: an analysis of the Surveillance, Epidemiology, and End Results database. Br J Haematol. 2015; 169(1):81–89. [DOI] [PubMed] [Google Scholar]
- 13.Kristinsson SY, Eloranta S, Dickman PW, et al. Patterns of survival in lymphoplasmacytic lymphoma/Waldenström macroglobulinemia: a population-based study of 1,555 patients diagnosed in Sweden from 1980 to 2005. Am J Hematol. 2013;8(1):60–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gonsalves WI, Rajkumar SV, Go RS, et al. Trends in survival of patients with primary plasma cell leukemia: a population-based analysis. Blood. 2014;124(6):907–912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Iriuchishima H, Ozaki S, Konishi J, et al. Primary plasma cell leukemia in the era of novel agents: a multicenter study of the Japanese Society of Myeloma. Acta Haematol. 2016;135(2):113–121. [DOI] [PubMed] [Google Scholar]
- 16.Katodritou E, Terpos E, Symeonidis AS, et al. Clinical features, outcome, and prognostic factors for survival and evolution to multiple myeloma of solitary plasmacytomas: a report of the Greek myeloma study group of 97 patients. Am J Hematol. 2014;89(8):803–808. [DOI] [PubMed] [Google Scholar]
- 17.Castillo JJ, Olszewski AJ, Cronin AM, Hunter ZR, Treon SP. Survival trends in Waldenström macroglobulinemia: an analysis of the Surveillance, Epidemiology, and End Results database. Blood. 2014; 123(25):3999–4000. [DOI] [PubMed] [Google Scholar]
- 18.Dores GM, Landgren O, McGLynn KA, Curtis RE, Linet MS, Devesa SS. Plasmacytoma of bone, extramedullary plasmacytoma, and multiple myeloma: incidence and survival in the United States, 1992–2004. Br J Haematol. 2009;144(1):86–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jansen L, Castro FA, Gondos A, et al. Recent cancer survival in Germany: An analysis of common and less common cancers. Int J Cancer. 2015;136(11):2649–2658. [DOI] [PubMed] [Google Scholar]
- 20.Hiripi E, Gondos A, Emrich K, et al. Survival from common and rare cancers in Germany in the early 21st century. Ann Oncol. 2012;23(2):472–479. [DOI] [PubMed] [Google Scholar]
- 21.Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) Research Data (1973–2013), National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2016, based on the November 2015 submission.
- 22.Brenner H, Gefeller O, Hakulinen T. Period analysis for up-to-date cancer survival data: theory, empirical evaluation, computational realization and applications. Eur J Cancer. 2004;40:326–335. [DOI] [PubMed] [Google Scholar]
- 23.Brenner H, Gefeller O. An alternative approach to monitoring cancer patient survival. Cancer. 1996;78(9):2004–2010 [PubMed] [Google Scholar]
- 24.Brenner H, Soederman B, Hakulinen T. Use of period analysis for providing more up-to-date estimates of long-term survival rates: empirical evaluation among 370,000 cancer patients in Finland. Int J Epidemiol. 2002;31(2):456–462. [PubMed] [Google Scholar]
- 25.Brenner H, Hakulinen T. Up-to-date long-term survival curves of patients with cancer by period analysis. J Clin Oncol. 2002;20(3):826–832. [DOI] [PubMed] [Google Scholar]
- 26.Corazziari I, Quinn M, Capocaccia R. Standard cancer patient population for age standardizing survival ratios. Eur J Cancer. 2004; 40:2307–2316. [DOI] [PubMed] [Google Scholar]
- 27.Brenner H. and Hakulinen T. Up-to-date and precise estimates of cancer patient survival: model-based period analysis. Am J Epidemiol. 2006;164(7):689–696. [DOI] [PubMed] [Google Scholar]
- 28.Ederer F, H H. Instructions to IBM 650 programmers in processing survival computations. Bethesda, MD: National Cancer Institute; 1959. [Google Scholar]
- 29.Federal Statistical Office Germany: GENESIS-Online database. Available from https://www-genesis.destatis.de/genesis/online. Last accessed September 2016.
- 30.Arias E. United States life tables, 2000. 2002, Natl Vit Stat Rep. 1–39. [PubMed] [Google Scholar]
- 31.Brenner H, Gefeller O, Hakulinen T. A computer program for period analysis of cancer patients survival. Eur J Cancer. 2002;38:690–695. [DOI] [PubMed] [Google Scholar]
- 32.San Miguel J, Weisel K, Moreau P, et al. Pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone alone for patients with relapsed and refractory multiple myeloma (MM-003): a randomised, open-label, phase 3 trial. Lancet Oncol. 2013;14(11):1055–1066. [DOI] [PubMed] [Google Scholar]
- 33.Stewart AK, Rajkmar SV, Dimopoulos MA, et al. Carfilzomib, lenalidomide, and dexamethasone for relapsed mulitple myeloma. N Engl J Med. 2015;372(2):142–152. [DOI] [PubMed] [Google Scholar]
- 34.Nooka AK, Kastritis E, Dimopoulos MA, Lonial S. Treatment options for relapsed and refractory mulitple myeloma. Blood. 2015;125(20):3085–3099. [DOI] [PubMed] [Google Scholar]
- 35.Gertz MA, Rue M, Blood E, Kaminer LS, Vesole DH, Greippo PR. Multicenter phase 2 trial of rituximab for Waldenström’s macroglobulinemia (WM): an Eastern Cooperative Oncology Group Study (E3A98). Leuk Lymphoma. 2004;45(10):2047–2055. [DOI] [PubMed] [Google Scholar]
- 36.Treon SP, Ioakimidis L, Soumerai JD, et al. Primaryy therapy of Waldenström macroglobulinemia with bortezomib, dexamethasone, and rituximab: WMCTG clincial trial 05-180. J Clin Oncol. 2009; 27(23):3830–3835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kyriakou C, Canalas C, Sibon D, et al. High-dose therapy and autologous stem-cell transplantation for Waldenström macroglobulinemia: the Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. J Clin Oncol. 2010;28(13):2227–2232. [DOI] [PubMed] [Google Scholar]
- 38.Li QW, Niu SQ, Wang HY, et al. Radiotherapy alone is associated with improved outcomes over surgery in the management of solitary plasmacytoma. Asian Pac J Cancer Prev. 2015;16(9):3741–3745. [DOI] [PubMed] [Google Scholar]
- 39.Weber DM. Solitary bone and extramedullary plasmacytoma. Hematology Am Soc Hematol Educ Program. 2005:373–376. [DOI] [PubMed] [Google Scholar]
- 40.Reed V, Shah J, Medeiros LJ, et al. Solitary plasmacytomas: outcomes and prognostic factors after definitive radiation therapy. Cancer. 2011;117(19):4468–4474. [DOI] [PubMed] [Google Scholar]
- 41.Caers J, Withof N, Hillengass J, et al. The role of positron tomography-computed tomography and magnetic resonance imaging in diagnosis and follow up of multiple myeloma. Haematologica. 2014;99(4):629–637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Berrino F, Esteve J, Coleman MP. Basic issues in estimating and comparing the survival of cancer patients. IARC Sci Publ. 1995;1–14. [PubMed] [Google Scholar]
- 43.Brenner H, Holleczek B. Deriving valid population-based cancer survival estimates in the presence of nonnegligible proportions of cancers notified by death certificate only. Cancer Epidemiol Biomarkers Prev. 2011;20(12):2480–2486. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.