

Abstract
Aims and Objectives:
To assess the body mass index (BMI) status and to correlate between nutritional status and early childhood caries among 3–6-year-old children in Vikarabad, Telangana, India.
Materials and Methods:
A cross-sectional study was conducted among 350 children attending the outpatient department of Pedodontia in Sri Sai College of Dental Surgery, Vikarabad. Caries experience was recorded using dmft index (WHO 1997); various anthropometric measures, such as weight, BMI, and height, were recorded as per the standard guidelines. Pearson correlation coefficient and chi square test were used to determine significant differences. Data were analyzed using the statistical analysis software (SPSS version 17.0 Chicago IL, USA)
Results:
Maximum number of participants (69%) were with normal BMI- for-age followed by underweight, overweight, and obese categories. The mean dmft values for each BMI category among the underweight, normal, overweight, and obese children were 4.9 ± 4.0, 4.6 ± 3.3, 2.7 ± 1.9, and 4.4 ± 3.0, respectively, which was statistically not significant.
Conclusion:
No significant association was found between dmft and BMI-for-age, rather a negative correlation existed between dmft and BMI-for-age (r = −0.023), which was not statistically significant (P = 0.66).
KEYWORDS: Body mass index, early childhood caries, India, nutritional status
INTRODUCTION
Dental caries is a multifactorial disease that affects significant number of populations throughout the world. It is one of the most common chronic childhood disease and can be considered as an epidemic in lower income families and underdeveloped parts of the world.[1] Early childhood caries (ECC) refers to any dental caries in primary dentition. ECC can rapidly destroy the primary dentition of toddlers and small children, and if left untreated, can lead to pain, acute infection, nutritional insufficiencies, and learning and speech problems.[2]
There are many risk factors that contribute to the development of ECC in infants and children. Among other risk factors are dietary habits, feeding practices, socioeconomic condition, oral hygiene practices, salivary flow, and exposure to fluoride, etc.[3]
Nutrition is necessary for the normal growth of an individual, particularly, late growth; and lifespan is significantly influenced by inappropriate nutrient intake. It has now been accepted that nutritional anthropometry has a significant role in the direct assessment of nutritional status in preschool children.[4] Nutritional status of children under 5 years of age in any community is a direct reflection of the stage of development of that community. The national family health survey (NFHS) data showed that 53% of the children in rural areas are underweight, which varies across states. The percentage of underweight children in the country was 53.4 in 1992, which decreased to 45.8 in 1998 and increased again to 47 in 2006.[5] Chronic malnourishment in children is linked to slow cognitive development and serious health consequences later in life that reduce the quality of life. Hence, the present study was undertaken to evaluate the relationship between nutritional status and early childhood caries in Indian children.
MATERIALS AND METHODS
A cross-sectional study was conducted among a sample of patients who visited the outpatient department of Pedodontia in Sri Sai college of Dental Surgery, Vikarabad, Telangana, India. The required sample size was estimated based on the scientific literature on prevalence of ECC in children, which was 37% (Priyadarshini et al, 2011).
The sample size was estimated based on the formula as follows:
n = Z2 × p (1 − p)/ E2
Z = confidence level at 95% (standard value of 1.96)
P = Prevalence of early childhood caries
E = margin of error at 5% (standard value of 0.05)
The minimum sample required was 323, which was rounded to 350 children. The study was conducted for a period of 6 months (January to June 2014).
INCLUSION CRITERIA
3 to 6 year old children who had at least one decayed, missing (due to caries) or filled primary teeth.
Parents who were willing to give written informed consent for the study.
EXCLUSION CRITERIA
Medically compromised children.
Children with physical and mental disabilities.
Uncooperative children/children without parental consent.
The ethical clearance was obtained from the institutional review board (Ethical approval letter no: Regd. No. 33/126/11) prior to the start of the study, and a written informed consent was taken from the parents or caregivers of the children. A pretested questionnaire was administered for the collection of demographic data, feeding practices, and dietary recall, and an oral examination was performed before anthropometric measurements.
ORAL EXAMINATION
The examination for dental caries was carried out on the dental chair, and the caries was diagnosed using WHO criteria (1997) and caries experience was depicted through dmft values, which were equivalent to the DMFT and DMFS indices used for permanent dentition. The American Academy of Pediatric Dentistry (AAPD 2008) defined ECC as the presence of 1 or more decayed (noncavitated or cavitated lesion), missing (due to caries), or filled tooth surfaces in any primary tooth in a child 71 of months age or younger.[6] A single trained and calibrated examiner performed comprehensive clinical examination with the assistance of one recorder. To assess the intraexaminer agreement 10% of the sample was re-examined after 10 days of the first examination (Kappa coefficient = 0.91).
Body mass index (BMI) is a measure of body fat based on the results of which the individual may be categorized under obese or underweight. In children and teens, BMI keeps on changing continuously as they grow and mature and varies between boys and girls of the same age. BMI in children is not only age specific but also gender specific.
Height and weight measurements were recorded for all the children who participated in the study. Weight of each child, barefoot with light clothing, was measured to the nearest 0.1 kg using a portable glass digital electronic personal weighing scale (Nova BGS-1238, Nova weigh suppliers, Ludhiana, Punjab), which was calibrated before use. For height, the investigator used a height measuring rod with a movable head board; it was measured to the nearest 0.1 cm using a mobile stadiometer (Seca 214 height rod, size 205 cm, SCORPIA India Medicare Pvt. Ltd. Ghaziabad, India), which was standardized at the National Institute of Nutrition (NIN) Hyderabad. The investigator was trained by the anthropologist at the National Institute of Nutrition (NIN). BMI was recorded by the examiner among 15 children who were not included in the study. Then, it was recorded by the anthropologist on the same individuals, and the interexaminer variability was calculated. A Kappa value of 0.86 was obtained for interobserver agreement.
For calculating BMI, the following formula was used.
BMI = Weight in Kg/(Height in m)2
The value obtained was then plotted on age and gender specific percentile curves given by the centers for disease control and prevention (CDC), and the children were categorized into four groups based on their BMI percentiles as follows:[7]
Underweight group children with BMI-for-age less than 5th percentile.
Normal group children with BMI-for-age greater than or equal to 5th percentile and less than 85th percentile.
Overweight group children with BMI-for-age greater than or equal to 85th percentile and less than 95th percentile.
Obese group children with BMI greater than or equal to 95th percentile.
STATISTICAL ANALYSIS
Chi-square test was done for assessing differences between qualitative variables. Pearson correlation coefficient test was used to evaluate the relation between BMI and dmft. All statistical analyses were performed using SPSS software (17.0, Chicago IL, USA). P value of <0.05 was considered statistically significant.
RESULTS
Out of 350 children, 188 were males and 162 were females, and 17.4% belonged to the 3-year-old group, 28% to 4-year-old, 34.4% to 5-year-old, and 20.2% to 6-year-old group [Table 1]. Table 2 shows the distribution of children based on the mean dmft in various BMI-for-age categories. The mean dmft values for each BMI category among the underweight, normal, overweight, and obese children were 4.9 ± 4.0, 4.6 ± 3.3, 2.7 ± 1.9, and 4.4 ± 3.0, respectively. The mean BMI of the total sample was 14.7 ± 1.4, respectively.
Table 1.
Distribution of children according to age and gender
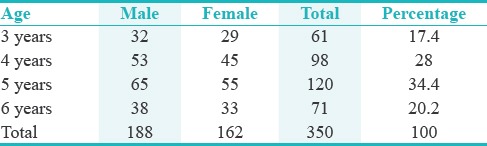
Table 2.
Distribution of children based on mean dmft in various BMI-for-age categories

Table 3 shows the comparison between nutritional status and dmft. There was a negative correlation between nutritional status and dmft (r = −0.023, P =0.665), and this relation was not of statistically significant.
Table 3.
Pearson correlation analysis between BMI and dmft
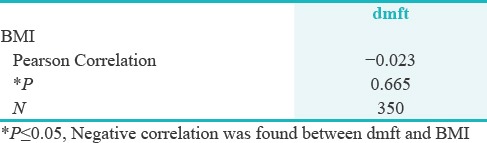
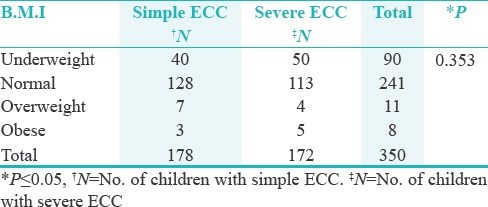
Table 4 shows the distribution of children based on BMI and early childhood caries. Of the 350 children, 178 had simple ECC and 172 had severe ECC. Of the 178 simple ECC children, 40 (22.4%) were underweight, 128 (71.9%) were normal, 7 (3.9%) were overweight, and 3 (1.6%) were obese. Of the 172 severe ECC children, 50 (29%) were underweight, 113 (65.6%) were normal, 4 (2.3%) were overweight, and 5 (2.9%) were obese. There was no statistical significant difference between ECC and BMI-for-age categories (P =0.353).
Table 4.
Distribution of children based on BMI to ECC
DISCUSSION
The present study was undertaken to assess the association between nutritional status and EC in 3–6-year-old children. The mean dmft was slightly higher in the underweight category (4.9 ± 4.0) compared to the normal and obese category, which indicates that underweight children were more prone to dental caries, which is in accordance with the studies done by Prasanth et al.[8] and Parkar et al.[9] This might be because the children might have chronic nutritional stress due to poor economic status and lack of awareness regarding oral and general health. Contradictory to this result, Sharma and Hegde[10] and Willershausen et al.[11] showed that high BMI was associated with dental caries in primary school children.
The results of this study revealed that maximum number of participants had normal BMI for age (69%), which was in accordance with the studies done by Ahmed et al.[12] and Sudhakar et al.[13] However, in contrast with the study conducted by Narang et al.[14] and Koksal et al.[15] who reported that maximum number of children were underweight, which might be due to the social class difference among children and study setting done in schools (Public and private). In the present study, there was no significant association between BMI for age (i.e. either in normal, underweight, overweight, and obese category) and ECC, which was similar to the studies done by Chen et al.[16] and Sheller et al.[17] In severe early childhood caries, the BMI percentiles had no correlation with dmft or pulp involvement of teeth in 2–5-year-old children.
Pearson correlation coefficient test was done to assess any relation between dmft and BMI. Negative correlation was found between nutritional status and ECC among children (r = −0.023), which was similar to the studies done by Ambarkova et al.[18] (r = −0.1105) and Yadav et al.[19] This might be because high percentage of decayed component (untreated caries) cause toothache, thus reducing food intake leading to low weight gain. Second, the low percentage of obese children (2%) found in this sample could also have biased the results towards a negative correlation. However, the decayed component was higher in the obese category which requires attention. In contrast, studies done by Aluckal et al.,[20] Alswata et al.,[21] and Davidson et al.[22] showed a positive relationship between nutritional status and caries.
The most obvious limitation of the study is its cross-sectional design as cause-effect cannot be established. Thus, relationships among variables must be interpreted with caution. A large sample size with longitudinal design and random sampling would have shown any positive associational between nutritional status and caries. Despite the limitations, this study found that ECC can be a risk factor in underweight children. Exploring the relation between nutritional status and dental caries is controversial.[23] Undeniably, it is likely that not a single common risk factor plays a role in the relationship between ECC and BMI but rather a complex interface of dietary pattern, oral hygiene practices, and genetic aspects that determine both caries and alterations in BMI.
CONCLUSION
From the results of this study, it can be concluded that maximum numbers of participants (69%) had normal BMI-for-age followed by underweight, overweight and obese categories. Mean dmft was slightly higher in the underweight category (4.9 ± 4.0) when compared to the normal category (4.6 ± 3.3) and the lowest mean was reported in the overweight category (2.7 ± 1.9); however, it was not statistically significant (P = 0.202). No significant association was found between dmft and BMI (P = 0.35) rather a negative correlation existed between dmft and BMI-for-age (r = −0.023), which was not statistically significant (P = 0.66).
The greatest portion of the total dmft score was decayed, which suggests an urgent improvement in the preventive dental care policies. Preventive programs should be conducted in schools and continuous education should be given to parents regarding dietary practices and oral hygiene to reduce the prevalence of both the diseases.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
ACKNOWLEDGEMENT
We sincerely thank Sree Ramakrishna garu (Community studies wing, NIN Hyderabad) in guiding us to record the nutritional status.
REFERENCES
- 1.Mohammadi TM, Zainab Hossienian Z, Bakhteyar M. The association of body mass index with dental caries in an Iranian sample of children. J Oral Health Oral Epidemiol. 2012;1:29–35. [Google Scholar]
- 2.Nunn ME, Braunstein NS, Krall Kaye EA, Dietrich T, Garcia RA, Henshaw MM. Healthy Eating Index is a Predictor of Early Childhood Caries. J Dent Res. 2009;88:361–6. doi: 10.1177/0022034509334043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Colak H, Dulgeril CT, Dalli M, Hamidi MM. Early childhood caries update: A review of causes, diagnoses, and treatments. J Nat Sc Biol Med. 2013;4:29–38. doi: 10.4103/0976-9668.107257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Priyadarshini HR, Hiremath SS, Puranik M, Rudresh SM, Nagaratnamma T. Prevalence of early childhood caries among preschool children of low socioeconomic status in Bangalore city, India. J Int Soc Prevent Communit Dent. 2011;1:27–30. doi: 10.4103/2231-0762.86384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Srivastava A, Mahmood SE, Srivastava PM, Shrotriya VP, Kumar B. Nutritional status of school-age children – A scenario of urban slums in India. Arch Public Health. 2012;70:1–8. doi: 10.1186/0778-7367-70-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.AAPD (American Academy of Pediatric Dentistry) Policy on Early Childhood Caries (ECC): classifications, consequences, and preventive strategies. [Last Accessed on 2016 Jul 3]. Available at: http://www.aapd.org/media/Policies_Guidelines/D_ECC.pdf . [PubMed]
- 7.Centers for Disease Control and Prevention. Growth charts body mass index for age percentiles, boys and girls. [Last accessed on 8th August 2016]. Available from: http://www.cdc.gov/bmi/bmimeans.htm .
- 8.Prashanth ST, Babu V, Kumar VD, Amitha HA. Comparison of Association of Dental Caries in Relation with Body Mass Index (BMI) in Government and Private School Children. J Dent Sci Res. 2011;2:22–6. [Google Scholar]
- 9.Parkar SM, Chokshi M. Exploring the association between dental caries and body mass index in public school children of Ahmedabad city, Gujarat. SRM J Res Dent Sci. 2013;4:101–5. [Google Scholar]
- 10.Sharma A, Hegde AM. Relationship between body mass index, caries experience and dietary preferences in children. J Clin Pediatr Dent. 2009;34:49–52. doi: 10.17796/jcpd.34.1.17364206hqm0477h. [DOI] [PubMed] [Google Scholar]
- 11.Willerhausen B, Blettner M, Kasaj A, Hohenfellner K. Association between body mass index and dental health in 1,290 children of elementary schools in a German city. Clin Oral Invest. 2007;11:195–200. doi: 10.1007/s00784-007-0103-6. [DOI] [PubMed] [Google Scholar]
- 12.Ahmed TE, Abuaffan AH. Correlation between body mass index and dental caries among a sample of Sudanese children. Braz Dent Sci. 2015;18:42–1. [Google Scholar]
- 13.Sudhakar K, Shanthi PR, Fareed N, Sudhir KM. Relationship between dentition status and body mass index among 5-15 year old group of children of an orphanage in Nellore city. J Indian Assoc Public Health Dent. 2010;15:45–9. [Google Scholar]
- 14.Narang R, Saha S, Jagannath GV, Sahana S, Kumari M, Shafaat M. Nutritional status and caries experience among 12 to 15 yrs old school going children of Lucknow. J Int Dent Med Res. 2012;5:30–5. [Google Scholar]
- 15.Koksal E, Tekcicek M, Yalcin SS, Tugrul B, Yalcin S, Pekcan G. Association between anthropometric measurements and dental caries in Turkish school children. Cent Eur J Public Health. 2011;19:147–51. doi: 10.21101/cejph.a3648. [DOI] [PubMed] [Google Scholar]
- 16.Chen W, Chen P, Chen SC, Shih WT, Hu HC. Lack of association between obesity and dental caries in three-year-old children. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 1998;39:109–11. [PubMed] [Google Scholar]
- 17.Sheller B, Churchill SS, Williams BJ, Davidson B. Body mass index of children with severe early childhood caries. Pediatr Dent. 2009;31:216–21. [PubMed] [Google Scholar]
- 18.Ambarkova V, Bakracevska G. Relating Dental Caries Experience with Body Mass Index among Primary School Children from Ohrid City – A Pilot Study. Aperito J Oral Health Dent. 2015;1:1–3. [Google Scholar]
- 19.Yadav PK, Saha S, Jagannath GV, Singh S. Developmental defects of enamel with dental caries and nutritional status. J Clin Diagn Res. 2015;9:71–4. doi: 10.7860/JCDR/2015/13401.6681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Aluckal E, Anzil KSA, Baby M, George EK, Lakshmanan S, Chikkanna S. Association between body mass index and dental caries among Anganwadi children of Belgaum City, India. J Contemp Dent Pract. 2016;17:844–8. doi: 10.5005/jp-journals-10024-1941. [DOI] [PubMed] [Google Scholar]
- 21.Alswata K, Mohameda WS, Wahabb MA, Aboelilb AA. The association between body mass index and dental caries: Cross-sectional study. J Clin Med Res. 2016;8:147–52. doi: 10.14740/jocmr2433w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Davidson K, Schroth RJ, Levi JA, Yaffe AB, Mittermuller BA, Sellers EAC. Higher body mass index associated with severe early childhood caries. BMC Pediatr. 2016;16:137–44. doi: 10.1186/s12887-016-0679-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Edalat A, Abbaszadeh M, Eesvandi M, Heidari A. The Relationship of Severe Early Childhood Caries and Body Mass Index in a Group of 3- to 6-year-old Children in Shiraz. J Dent Shiraz Univ Med Sci. 2014;15:68–73. [PMC free article] [PubMed] [Google Scholar]