

Abstract
Objectives:
Risk factors in oral implantology are defined as local or systemic conditions that increase failure rates. The purpose of this paper is to evaluate the long-term survival rate of dental implants placed in patients presenting mechanical risk factors.
Materials and Methods:
This retrospective study was conducted only with patients presenting at least one of the following risk factors were included: Bruxism; crown-to-implant (C/I) ratio <0.8; abutment angulation. The overall implant survival was estimated using Kaplan–Meier analyses. Risk factors for implant failure were identified using the Cox proportional hazard regression models.
Results:
Eighty-nine eligible patients were enrolled in this study: They were both male (n = 56, 62.92%) and female (n = 33, 37.08%), with an average age of 53.24 (23–76 years), with 227 dental implants inserted. The mean follow-up was 13.6 years (range: 10–16 years). The overall 10-year Kaplan–Meier survival estimate with associated 95% confidence intervals was 86.34% (82.8, 87.1). Bruxism was the only variable that showed a statistically significant association with implant failure (P < 0.05) and a hazard ratio of 2.9, while both Crown to-implant and abutment angulations reported lower values of failure (P > 0.05).
Conclusions:
Within the limitations of this study, can be concluded that data suggested an evident relationship between bruxism and dental implant failure but further studies, with a larger sample and a different design are required to assess this relationship.
KEYWORDS: Bruxism, dental implant, implant survival, risk factors
INTRODUCTION
Risk factors in oral implantology are defined as local or systemic conditions that increase failure rates.[1,2] Smoking habit, osteoporosis, coagulation disturbs, and diabetes are considered as general risk factors.[3,4,5]
Failures can be divided into early failures, which are related to the surgical phase, and late failures which occurred during or after the prosthetic phase and the application of an occlusal load.[6,7,8] Early and late failures are associated with different causes: early failures are always biological, resulting in the lack of healing of the peri-implant tissues, without getting a proper, satisfying bone integration with an intimate bone-implant contact.[9,10]
Late failures may be categorized into biological and mechanical. The inflammatory process of peri-implant tissues may determine biological failures together with occlusal overload, resulting in a progressive loss of osseointegration with resorption and apical growth of epithelial tissue may be observed.[11,12] Mechanical failures are determined by wear and sagging of implant-prosthesis mechanical components with possible connection screw loosening or fracture, fixture fracture, abutment or prosthesis fracture.[13,14]
Mechanical risk factors are represented by all situations which expose dental implants to lateral loads: Crown-to-implant (C/I) ratio <0.8; angulation >25°; diameter inferior to the ideal; presence of cantilever, as well as bruxism and clenching para-functional habits.[15,16]
However, to date, most studies evaluating risk factors for implant failure are flawed in terms of their statistical analyses.[17,18,19]
The aim of this paper is to assess the long-term survival rate of dental implants placed in patients presenting mechanical risk factors.
The authors hypothesized that dental implants placed in patients with bruxism and clenching para-functional habits may show higher failure rates, compared to dental implants in patients presenting other mechanical risk factors.
MATERIALS AND METHODS
The sample for this retrospective cohort study was derived from a population of patients presenting at the university's department for implant treatment, between 1998 and 2006.
The following inclusion criteria were applied: Age >18 years, presence of at least one of the following mechanical risk factors (bruxism; C/I ratio <0.8; abutment angolations), Full or partial natural dentition opposing the implants, dental implant supporting only single crown restoration, agreed to participate to the study.
Exclusion from the study was performed in case of uncontrolled systemic disorders; if patients refused to enroll in this survey or in case of missing medical records. The study was approved by the Institution Review Board.
Dental implants placed were all cylindrical, with a surface acid-etched and sanded with aluminum oxide medium grade particles (250 μm).
STUDY VARIABLES
The following study variables were considered:
Bruxism
C/I ratio <0.8 of single tooth implant-supported restorations. The length of the crown and of the implant was measured directly from the radiograph using constant magnification to calculate C/I ratio
Abutment angulations. The need to avoid an adjacent tooth or vital structure may dictate implant angulations during insertion. Data on abutment angulations were recorded from the patient's charts.
The outcome variable of interest was implant failure defined as the removal of the implant. Total survival time was considered the duration of time, expressed in months, from implant placement to implant removal or date of the last follow-up for patients whose implants has not been removed.
DATA ANALYSIS
The nonparametric Kaplan–Meier survival analysis was used to estimate implant survival rates, a χ2 test was performed to evaluate statistical association between variables, with a P < 0.05. Risk factors with P < 0.05, based on univariate analyses, were analyzed to obtain a proper hazard ratio using the Cox regression model.
RESULTS
During the study, 1354 implants were placed in 456 patients.
Eighty-nine eligible patients were enrolled in this study: They were both male (n = 56, 62.92%) and female (n = 33, 37.08%), with an average age of 53.24 (23–76 years), with 227 dental implants placed.
The mean follow-up was 13.6 years (range: 10–16 years). Data and demographic of the sample were summarized in Tables 1 and 2.
Table 1.
Sample demographic
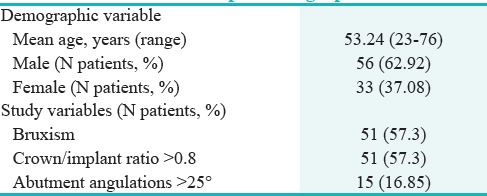
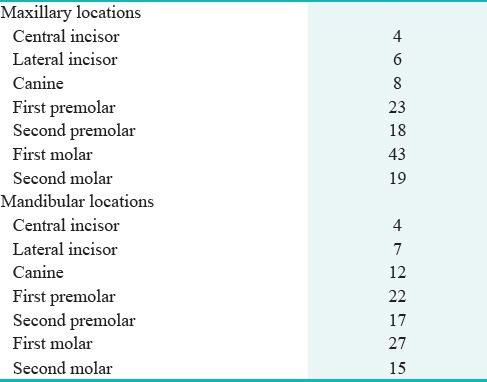
Table 2.
Implant treatment sites
The overall 10-year Kaplan–Meier survival estimate with associated 95% confidence intervals was 86.34% (82.8, 87.1).
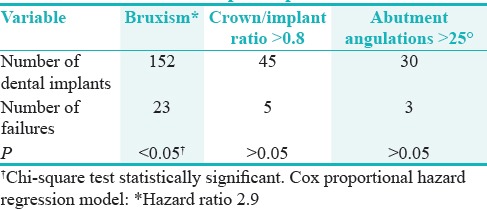
A total of 152 dental implants were placed in patients affected by bruxism, 45 in subjects with a C/I ratio >0.8 and thirty implants had abutments angulated >25° [Table 3]. Bruxism was the only variable that showed a statistically significant association with implant failure (P < 0.05) and a hazard ratio of 2.9, while both C/I ratio and abutment angulations reported lower values of failure (P > 0.05).
Table 3.
Study variables analysis based on number of dental implants placed
DISCUSSION
Dental implants placed in patients affected by bruxism showed statistically significant higher failure rates, compared to other risk factors assessed.
According to our findings, bruxism had a hazard ratio of 2.9 and therefore, may represent a contraindication to implant treatment, although the evidence for this is usually based only on clinical experience and is still controversial.[20,21] Bruxism is considered as one of the possible factors, among others, for temporomandibular pain, tooth wear in the form of attrition and loss of dental implants.[22,23,24] In the present study, bruxism was diagnosed according to the following criteria; tooth wear affecting at least one sextant of the dentition with enamel reduction to dentine and some loss of crown height and/or masseter muscle hypertrophy.[21]
There is no proof that suggests that bruxism can cause an overload of dental implants but Lobbezoo et al. recommended a careful approach when placing implants in patients with this para-functional habit.[15,16]
A recent systematic review by Chrcanovic et al.[22] obtained a risk ratio of 2.93 for dental implants placed in patients with bruxism, a data comparable to our findings.
They compared dental implants inserted in bruxers versus no bruxers and found out only ten studies suitable, all characterized by various biases, such as a low level of specificity and lack of control group.
Data highlighted the lack of appropriate literature on the topic, suggesting the need for further studies, with a larger sample and a different study design.
As for secondary outcome variables, in cases where the quantity of bone is not sufficient for implant insertion and regeneration techniques cannot be implemented, we can use short implants or insert them with a nonideal angulation.[25,26,27,28] According to our results, C/I ratio and abutment angulation resulted not associated with mechanical failure, therefore, not representing a risk factor for long-term survival of dental implants.
This study presents an evaluation of implant survival in patients with mechanical risk factors, especially bruxism, showing results similar to Chrcanovic et al.[22] However, the long-term follow-up (up to 16 years) and the large number of dental implants placed in bruxers (implant failure: 23/152, hazard ratio 2.9) characterized our study as one of the few in literature with the consistent sample and observation period.
According to the authors, further studies, with a prospective design and a control group (bruxers vs. no bruxers) are necessary to address the relevant question: How bruxism affect dental implant survival?
Literature available is made by retrospective cohort studies, included this study, with a high risk of bias and difficult interpretation of results. Another important flaw of current literature available is generated by the difficulty to establish a “definite” diagnosis of bruxism and by the status of opposing dentition, which needs to be taken into account, as well as implant characteristics (length/diameter/surface).
CONCLUSIONS
Within the limitations of this study, can be concluded that data suggested an evident relationship between bruxism and dental implant failure but further studies, with a larger sample and a different design are required to assess this relationship.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986;1:11–25. [PubMed] [Google Scholar]
- 2.Misch CE. The effect of bruxism on treatment planning for dental implants. Dent Today. 2002;21:76–81. [PubMed] [Google Scholar]
- 3.Manzano G, Montero J, Martín-Vallejo J, Del Fabbro M, Bravo M, Testori T. Risk factors in early implant failure: A meta-analysis. Implant Dent. 2016;25:272–80. doi: 10.1097/ID.0000000000000386. [DOI] [PubMed] [Google Scholar]
- 4.Rosella D, Papi P, Giardino R, Cicalini E, Piccoli L, Pompa G. Medication-related osteonecrosis of the jaw: Clinical and practical guidelines. J Int Soc Prev Community Dent. 2016;6:97–104. doi: 10.4103/2231-0762.178742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pompa G, Bignozzi I, Cristalli MP, Quaranta A, Di Carlo S, Annibali S. Bisphosphonate and osteonecrosis of the jaw: The oral surgeon's perspective. Eur J Inflamm. 2012;10:11–23. [Google Scholar]
- 6.Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur J Oral Sci. 1998;106:527–51. doi: 10.1046/j.0909-8836..t01-2-.x. [DOI] [PubMed] [Google Scholar]
- 7.Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis. Eur J Oral Sci. 1998;106:721–64. doi: 10.1046/j.0909-8836..t01-6-.x. [DOI] [PubMed] [Google Scholar]
- 8.Mencio F, De Angelis F, Papi P, Rosella D, Pompa G, Di Carlo S. A randomized clinical trial about presence of pathogenic microflora and risk of peri-implantitis: Comparison of two different types of implant-abutment connections. Eur Rev Med Pharmacol Sci. 2017;21:1443–51. [PubMed] [Google Scholar]
- 9.De Angelis F, Papi P, Mencio F, Rosella D, Di Carlo S, Pompa G. Implant survival and success rates in patients with risk factors: Results from a long-term retrospective study with a 10 to 18 years follow-up. Eur Rev Med Pharmacol Sci. 2017;21:433–7. [PubMed] [Google Scholar]
- 10.Quaranta A, Piattelli A, Scarano A, Quaranta M, Pompa G, Iezzi G. Light-microscopic evaluation of the dimensions of peri-implant mucosa around immediately loaded and submerged titanium implants in monkeys. J Periodontol. 2008;79:1697–703. doi: 10.1902/jop.2008.070631. [DOI] [PubMed] [Google Scholar]
- 11.Masuelli L, Pompa G, Fabrizi M, Quaranta A, Vozza I, Piccoli L, et al. Patients with peri-implantitis, unlike those with a healthy periimplant microenvironment, display antibodies to more than one heat shock protein (HSP 27, HSP 65 and HSP 90) linear epitope. Eur J Inflamm. 2011;9:257–67. [Google Scholar]
- 12.Chen H, Liu N, Xu X, Qu X, Lu E. Smoking, radiotherapy, diabetes and osteoporosis as risk factors for dental implant failure: A meta-analysis. PLoS One. 2013;8:e71955. doi: 10.1371/journal.pone.0071955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Danesh-Sani SA. Maintaining osseointegration: Understanding, preventing, and treating risk factors for peri-implant diseases. J Contemp Dent Pract. 2016;17:711–2. doi: 10.5005/jp-journals-10024-1917. [DOI] [PubMed] [Google Scholar]
- 14.Mencio F, Papi P, Di Carlo S, Pompa G. Salivary bacterial leakage into implant-abutment connections: Preliminary results of an in vitro study. Eur Rev Med Pharmacol Sci. 2016;20:2476–83. [PubMed] [Google Scholar]
- 15.Jacobs R, De Laat A. Bruxism and overload of periodontium and implants. Ned Tijdschr Tandheelkd. 2000;107:281–4. [PubMed] [Google Scholar]
- 16.Lobbezoo F, Van Der Zaag J, Naeije M. Bruxism: Its multiple causes and its effects on dental implants – An updated review. J Oral Rehabil. 2006;33:293–300. doi: 10.1111/j.1365-2842.2006.01609.x. [DOI] [PubMed] [Google Scholar]
- 17.Lobbezoo F, Brouwers JE, Cune MS, Naeije M. Dental implants in patients with bruxing habits. J Oral Rehabil. 2006;33:152–9. doi: 10.1111/j.1365-2842.2006.01542.x. [DOI] [PubMed] [Google Scholar]
- 18.Chuang SK, Wei LJ, Douglass CW, Dodson TB. Risk factors for dental implant failure: a strategy for the analysis of clustered failure-time observations. J Dent Res. 2002;81:572–7. doi: 10.1177/154405910208100814. [DOI] [PubMed] [Google Scholar]
- 19.Chuang SK, Tian L, Wei LJ, Dodson TB. Kaplan-Meier analysis of dental implant survival: a strategy for estimating survival with clustered observations. J Dent Res. 2001;80:2016–20. doi: 10.1177/00220345010800111301. [DOI] [PubMed] [Google Scholar]
- 20.Yadav K, Nagpal A, Agarwal SK, Kochhar A. Intricate assessment and evaluation of effect of bruxism on long-term survival and failure of dental implants: A comparative study. J Oral Rehabil. 2016;43:813–23. doi: 10.5005/jp-journals-10024-1910. [DOI] [PubMed] [Google Scholar]
- 21.Chrcanovic BR, Kisch J, Albrektsson T, Wennerberg A. Bruxism and dental implant failures: A multilevel mixed effects parametric survival analysis approach. J Oral Rehabil. 2016;43:813–823. doi: 10.1111/joor.12431. [DOI] [PubMed] [Google Scholar]
- 22.Chrcanovic BR, Albrektsson T, Wennerberg A. Bruxism and dental implants: A meta-analysis. Implant Dent. 2015;24:505–16. doi: 10.1097/ID.0000000000000298. [DOI] [PubMed] [Google Scholar]
- 23.Baqain ZH, Moqbel WY, Sawair FA. Early dental implant failure: risk factors. Br J Oral Maxillofac Surg. 2012;50:239–43. doi: 10.1016/j.bjoms.2011.04.074. [DOI] [PubMed] [Google Scholar]
- 24.Clark D, Levin L. Dental implant management and maintenance: How to improve long-term implant success? Quintessence Int. 2016;47:417–23. doi: 10.3290/j.qi.a35870. [DOI] [PubMed] [Google Scholar]
- 25.Tran DT, Gay IC, Diaz-Rodriguez J, Parthasarathy K, Weltman R, Friedman L. Survival of dental implants placed in grafted and nongrafted bone: A retrospective study in a university setting. Int J Oral Maxillofac Implants. 2016;31:310–7. doi: 10.11607/jomi.4681. [DOI] [PubMed] [Google Scholar]
- 26.Cassetta M, Pompa G, Di Carlo S, Piccoli L, Pacifici A, Pacifici L. The influence of smoking and surgical technique on the accuracy of mucosa-supported stereolithographic surgical guide in complete edentulous upper jaws. Eur Rev Med Pharmacol Sci. 2012;16:1546–53. [PubMed] [Google Scholar]
- 27.Annibali S, Cristalli MP, Dell'Aquila D, Bignozzi I, La Monaca G, Pilloni A. Short dental implants: a systematic review. J Dent Res. 2012;91:25–32. doi: 10.1177/0022034511425675. [DOI] [PubMed] [Google Scholar]
- 28.Mangano F, Frezzato I, Frezzato A, Veronesi G, Mortellaro C, Mangano C. The Effect of Crown-to-Implant Ratio on the Clinical Performance of Extra-Short Locking-Taper Implants. J Craniofac Surg. 2016;27:675–681. doi: 10.1097/SCS.0000000000002562. [DOI] [PubMed] [Google Scholar]