

Abstract
Multiple myeloma is a very heterogeneous disease with variable survival. Despite recent progress and the widespread use of new agents, patients with relapsed and refractory disease have a poor outcome. Immunomodulatory drugs play a key role in both the front-line and the relapsed/refractory setting. The combination of pomalidomide (POM) and dexamethasone is safe and effective in relapsed and refractory patients, even in those with high-risk cytogenetic features. Furthermore, it can be used in most patients without the need to adjust according to the degree of renal failure. In order to further improve the results, POM-based triplet therapies are currently used. This article highlights the most relevant issues of POM and POM-based combinations in the relapsed/refractory multiple myeloma setting, from a pharmacological and clinical point of view.
Keywords: multiple myeloma, pomalidomide, triplet therapy, dexamethasone
Video abstract
Introduction
Multiple myeloma (MM) is a plasma cell malignancy characterized by the presence of 10% or more clonal plasma cells on bone marrow examination or a biopsy-proven plasmacytoma, and the evidence of a myeloma-defining event, according with the recently established diagnostic criteria.1 These criteria allow early diagnosis and initiation of therapy before end-organ damage. MM should be considered a heterogeneous group of related diseases rather than a single entity.2 Median overall survival (OS) is variable depending on stage, response to therapy, and host-related and tumor-related prognostic factors. Several risk stratification systems have been developed to help estimate the outcome, allowing for a risk-adapted approach.3–6 In recent years, OS is progressively increasing.7 However, MM is still considered incurable in most patients, and 5-year relative survival is only around 40%.8
The treatment of MM has dramatically changed over the past decade due to the widespread use of the new agents and new combinations, better supportive care, and optimized indication of autologous stem cell transplant (ASCT). Both proteasome inhibitors (PIs) like bortezomib as well as immunomodulatory drugs such as thalidomide or lenalidomide are commonly used in the front-line setting. The landscape of MM therapy is increasingly complex with the availability of second-generation PIs (carfilzomib, ixazomib), novel immunomodulatory drugs such as pomalidomide (POM), histone deacetylase inhibitors (panobinostat), monoclonal antibodies (elotuzumab and daratumumab), and other group of drugs.9,10 Cure is currently achievable in a selected group of patients.11,12 In this regard, continuous or early treatment could be new strategies to cure MM.13,14
Given the high rates of complete response (CR) seen with new treatment approaches, new response categories need to be defined that can identify deeper responses than those conventionally defined as CR. Using flow cytometry or gene sequencing as well as sensitive imaging techniques, the International Myeloma Working Group has defined new response categories of minimal residual disease negativity.15
Therefore, achieving a minimal residual diseases-negative response seems to be a prerequisite or mandatory step for curing MM. Outside clinical trials, patients should be treated with the best available regimen from the beginning, in order to reach this response. However, most patients will not reach or maintain a CR, and for those patients the aim will be turning MM into a chronic disease.
The approach to first-line MM therapy is commonly divided into several phases: induction, ASCT, consolidation, and maintenance. Most patients will relapse, and a personalized salvage therapy should be assessed for the management of the disease at this point. The choice of treatment for newly diagnosed MM (NDMM) depends on the eligibility for ASCT. For patients who are eligible for transplant, an upfront ASCT will be planned, ideally after a PI- and immunomodulatory-based induction. On the other hand, the optimal treatment for elderly NDMM should provide a good balance of efficacy and safety.16 Triplet therapy is currently preferred, with doublet therapy reserved for frail patients, but controversy still remains.17 Although the new combinations can achieve a high overall response rate (ORR) with a certain level of CR, most patients will relapse. Therefore, the duration of the response (DOR), progression-free survival (PFS), and the time to the next treatment are key issues.
The presence of baseline high-risk (HR) disease according to fluorescent in situ hybridization has shown a deep prognostic impact. This analysis is mandatory and includes probes to detect the following translocations, deletions, or duplications: t(4;14), t(14;16), del(17p), del(1p), and gain(1q21).18
The management of relapsed and/or refractory MM (RRMM) represents a key point on the overall care for patients and is a critical area of ongoing scientific and clinical research. The prognosis of patients refractory to bortezomib and at least one immunomodulatory drug is extremely poor.19 Treatment is indicated when patients develop symptomatic relapse, a rapidly rising paraprotein level, or extramedullary disease. Specific management recommendations have been provided by the International Myeloma Working Group.20 Similarly, the Mayo Clinic has updated its evidence-based and risk-adapted approach for RRMM patients.21
POM is a third-generation immunomodulatory drug approved in 2013 by the United States Food and Drug Administration (FDA) and the European Medicines Agency in combination with low-dose dexamethasone (d) for MM patients who have received at least two prior therapies (including both lenalidomide and bortezomib) and whose disease progressed after the last treatment. Herein, we review the clinically relevant pharmacological aspects of POM, its clinical development, as well as its evidence-based role in the current approach to MM therapy.
Design and characteristics
Immunomodulatory drugs
Thalidomide is a (N-ftalimido) glutarimide molecule that was synthesized from glutamic acid in Germany in 1954 and has two enantiomers (as a consequence from the asymmetric carbon atom in position 3 from piperidinedione ring, which further binds with an indole ring). The S-enantiomer of thalidomide exhibits teratogenic effects in humans, while the R-enantiomer is responsible of sedative–hypnotic pharmacological activities. It was used to prevent morning sickness during the first trimester in pregnant women. However, it was withdrawn from market in 1961 because teratogenicity (phocomelia) was associated with its use during pregnancy.22,23 Recently, this drug has received attention due to the discovery of its antiangiogenic and immunomodulatory properties. It was implemented in MM based on the referred potential antiangiogenic effect.24 In 2006, thalidomide was granted approval from FDA for NDMM. Although the cellular pharmacology of thalidomide (and analogs) has been well studied, its mechanism of action was not fully understood until 2010, when the protein CRBN was identified as the molecular target of thalidomide teratogenic effects, acting as a coreceptor of the E3 ubiquitin ligase complex which includes the DDB1 and the CUL4A protein. The absence of CRBN protein is associated with resistance to immunomodulatory drugs.25 CRBN also mediates the costimulatory anti-MM and T activities of lenalidomide and POM.26,27
In order to decrease the side effects of thalidomide and to increase its effectiveness, structure-based drug design has been applied to find a similar mechanism of action. The search of thalidomide analogs with increased immunomodulatory activity and better safety profile led to the testing of thalidomide to which an amino group was added to carbon atom 4 of its phthaloyl moiety, giving rise to 4-amino analogs known as immunomodulatory drugs (Figure 1). These drugs exhibit a superior performance, 50 to 200-fold more potent than thalidomide to stimulate T- and natural killer cells and to reduce plasma cell adhesion to stroma, reducing cytokine production and promoting apoptosis.28 Thalidomide, lenalidominde, and POM are structurally related molecules, sharing a common α-(isoindolinone-2-yl)-glutarimide core. Those analogs with an amino group in position 4 of the isoindolinone or isoindolindione (ftalimide) exhibit a strong inhibition of TNF-α factor.27 Table 1 summarizes some of the characteristics of the immunomodulatory drugs.
Figure 1.
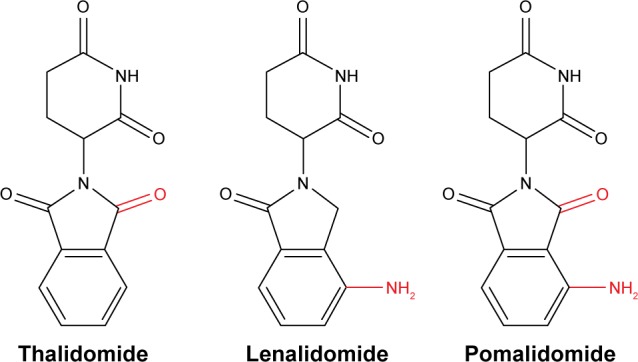
Chemical structure of immunomodulatory drugs.
Note: Common structural features are shown in black.
Table 1.
POM-based triplet therapies in RRMM
| Study | Regimen | n | Phase | Prior lines, m (range) | ORR % | CR % | mPFS months | mOS months |
|---|---|---|---|---|---|---|---|---|
| Baz et al,52 2016 | POMCyd | 34 | 2 | 4 (2–12) | 64.7 | 3 | 9.5 | NR |
| Chari et al,53 2016 | POMCyd | 28 | 2 | 3 | 67 | 10.7 | 14.5 | NR |
| Sriskandarajah et al,50 2017 | POMd (30), POMCyd (9) | 39 | – | 4 (1–8) | 41 | 0 | 5.2 | 13.1 |
| Bringhen et al,55 2016 | KPOMd | 57 | 1/2 | – | 58 | – | 9.5 | NR |
| Hobbs et al,56 2016 | KPOMd | 45 | – | 4 (1–14) | 36 | 9 | 3.3 | 16.1 |
| Krishnan et al,57 2016 | IPOMd | 32 | 1/2 | 3 (1–5) | 45 | 0 | – | – |
| Spencer et al,58 2016 | MPOMd | 38 | 1 | 4 (1–9) | 53 | – | – | – |
| Ocio et al,64 2016 | POMdfil | 14 | 1b/2 | 3.5 (2–6) | 50 | 0 | 7 | – |
| Branca et al,59 2016 | DaraPOMd | 39 | – | 4 | 41 | 5 | – | – |
| Richardson et al,60 2016 | IsaPOMd | 14 | 1b | 4.5 (2–11) | 62 | 7.7 | – | – |
| Chen et al,61 2016 | SelPOMd | 11 | 1b/2 | 5 | 60 | 10 | – | – |
| Badros et al,62 2016 | PemPOMd | 48 | 2 | 3 (2–6) | 56 | 8 | – | – |
| Wilson et al,63 2016 | PemPOMd | 9 | – | ≥5 | 33 | 0 | 1.9 | 56% at 6 months |
Abbreviations: POM, pomalidomide; RRMM, relapsed/refractory multiple myeloma; n, number of patients; m, median; ORR, overall response rate; CR, complete response; PFS, progression-free survival; OS, overall survival; Cy, cyclophosphamide; d, low-dose dexamethasone; K, carfilzomib; I, ixazomib; M, marizomib; fil, filanesib; Dara, daratumumab; Isa, isatuximab; Sel, selinexor; Pem, pembrolizumab; NR, not reached; –, unknown.
POM
POM is a structural analog of thalidomide and lenalidomide with an even stronger activity than the latter ones. It has an additional amino group in the 4th position of the ftaloil ring and differs from lenalidomide in that it also has a a carbonyl group in the ftaloil ring.29 From a chemical point of view, it is a racemic mixture of R- and S-isomers (RS)-4-amino-2-(2,6-dioxopiperidin-3-yl)isoindole-1,3-dione with a molecular weight of 27,324 Da.
Mechanism of action of POM
POM is a 3rd generation immunomodulatory drug with antitumor activity and immunomodulatory and antiangiogenic properties as well as direct antimyeloma activity (Figure 2). Like other drugs in this group, it shows a pleiotropic mechanism of action, aligned with the current cancer therapy approach focused on a triple action: induction of apoptosis against tumor cells, interference of tumor interactions with cellular microenvironment, and improvement of the autoimmune response.
Figure 2.

Schematic representation of the mechanism of action of POM.
Abbreviations: POM, pomalidomide; NK, natural killer.
POM received approval in combination with d for the treatment of patients with RRMM who have received at least two previous lines of therapy, including lenalidomide and bortezomib, and whose disease progressed during last therapy.30
The mechanism of action of POM has not yet been fully elucidated. CRBN has been demonstrated to be the direct target of POM.31 The binding of POM to CRBN promotes the recruitment of IL-2 transcriptional repressors, IKZF1 (Ikaros) and IKZF3 (Aiolos), causing its ubiquitination and further degradation within hours of treatment, and also produces the negative regulation of transcriptional factor IRF4 and MYC within 48 h of treatment.31,32 These findings suggest that POM induces the proteasome degradation mediated by both proteins in T-cells.
POM achieves its antimyeloma action through the negative direct regulation of key functions of tumor cells as well as by blocking the myeloma cell interactions with their microenvironment by modulation of cellular adhesion and reduction of TNF-6, IL-8, and VEGF production. POM induces apoptosis via caspase-8 pathway and exhibits an antiangiogenic activity by inhibiting the secretion of VEGF and bFGF for both myeloma and stroma cells29 and modulating the secretion of various cytokines, blocking the interaction between stroma and myeloma cells. POM also inhibits TNF-α production, which induces IL-6 expression, a growth factor for the proliferation of myeloma cells.33
As stated before, CRBN protein has been identified as the pharmacological target for thalidomide and its analogs, and there is a clear relationship between low CRBN expression and the resistance to these drugs in myeloma. CRBN interacts with interferon regulatory factor 4, which plays a crucial role in the survival of myeloma cells. POM increases proliferation of T-lymphocytes (both CD4 and CD8) and natural killer cells as well as the expression of different costimulating molecules like CD28. Also, it inhibits the production of different proinflammatory cytokines (TNF-α and interleukins IL-1β, IL-6, and IL-12), increasing the levels of other interleukins with anti-inflammatory nature (IL-10). Moreover, POM increases gamma interferon and IL-2 production. POM has been proven to inhibit the growth of tumor cells that show resistance to other antineoplastic drugs, including lenalidomide, and possesses a synergistic effect with d both in lenalidomide-resistant MM cellular therapy lines and in those sensitive to lenalidomide to induce apoptosis in tumor cells.34
POM has also direct antimyeloma activity, blocking the cellular cycle in MM cell lines by increasing the expression level of p21 (WAF-1) by an LSD1-mediated epigenetic mechanism. WAF-1 is a mediator of p53 tumor suppression.35
Finally, MM clinical trials have proved that POM is an efficient drug to overcome resistance to lenalidomide and thalidominde as well as to bortezomib.36
Pharmacokinetics
After administration of a unique oral dose, oral absorption of POM is higher than 70%, and the maximum plasma concentration is reached in 2–3 hours. The area under the curve (AUC) of POM increases, approximately, lineally and proportionally to the dose increments. POM has an accumulation ratio from 27% to 31% in AUC after multiple dose administration. Coadministration with high-fat and high-calorie food reduces its absorption rate, reducing the maximum plasma concentration in 25%, and it also has an effect on the extent of the global absorption, showing a reduction of 8% in AUC. The mean apparent distribution volume of POM is between 62 and 138 liters at steady state. The in vitro binding of the POM enantiomers to the plasmatic proteins in humans is in the range of 12%–14%, and this is not concentration dependent.
The half-life of POM is between 6.5 and 8.0 h, and most of it is eliminated in 48 h.37 POM is primarily eliminated in urine by kidneys (~73%), but is widely metabolized before excretion. Majority of the drug is excreted after cytochrome P450-mediated hydroxylation (CYP1A2 and CYP3A2), and this is followed by that excreted following glucoronidation38 (43% of the dose) and hydrolysis of the glutarimide ring (25%), and finally 10% of the drug is excreted in a nonaltered form. 5-hydroxypomalidomide, an oxidative metabolite, is formed mainly by CYP1A2 and CYP3A4. The hydroxyl metabolites and the hydrolytic by-products are at least 26 times less active than POM in vitro.29,38 POM can be also eliminated by dialysis.38
Clinical development
On February 8, 2013, the FDA approved POM for use in the treatment of patients with RRMM who have received at least two prior therapies, including lenalidomide and bortezomib, and have demonstrated disease progression on or within 60 days of completion of the last therapy. The approval was based on the results of clinical trial CC-4047-MM-002. Start date: June 2008, USA and Canada. Enrollment: 259.
The purpose of the CC-4047-MM-002 study was to determine the maximum tolerated dose (MTD) and effectiveness of POM (CC-4047) alone or in combination with d (POMd) as treatment for patients with RRMM. The primary outcome measure of Phase I was MTD. The trial design had 4 study arms: POM (2, 3, 4 and 5) mg daily on days 1–21 of each 28-day cycle; participants with progressive disease had the option of adding d 40 mg on days 1, 8, 15 and 22 of each 28-day cycle or discontinuing study treatment. The number of participants analyzed were 6, 8, 14 and 10 in each arm (2, 3, 4 and 5 mg POM). The patients with dose-limiting toxicities in cycle 1 were 1, 1, 2 and 4 respectively.
The outcome measures of Phase II were Kaplan–Meier estimates of PFS and percentage of participants with PFS events. The trial design had two arms: POM 4 mg daily on days 1–21 of each 28-day cycle, and the other arm was POMd: POM with the same dose as the first arm and d (dose determined by age: 40 mg for participants ≤75 years of age and 20 mg for participants >75 years of age) on days 1, 8, 15 and 22 of each 28-day cycle. The number of participants was 113 in the POMd arm and 108 in the POM arm. Kaplan–Meier estimates of PFS were 16.6 (95% confidence interval [95% CI], 14.1–21.1) weeks for POMd versus 10.7 (95% CI, 8.3–16.1) weeks for POM. The proportion of participants with PFS events as of the April 1, 2011, (cut-off) was not significantly different between the arms (76.1% in the POMd compared to 75% in the POM arm).
In order to collect more data for POMd, a new phase III clinical trial was designed, CC-4047-MM-003. The purpose of this study was to compare efficacy and safety of POMd versus high-dose d in subjects with RRMM. The short name for this study is NIMBUS, and the number of subjects enrolled is 455. Although resistance to high-dose d in the last line of therapy was considered an exclusion criterion, nearly all patients who were enrolled had failed prior steroid-based treatment. As of February 2017, the study is ongoing, but not recruiting participants. In this study, the experimental arms were treated as follows: POMd, POM 4 mg on days 1–21 of each 28-day treatment cycle and 40 mg d days 1, 8, 15 and 22 of a 28-day cycle until disease progression. Subjects older than 75 years old had a reduction to 20 mg d (on the same days; ie, 1, 8, 15 and 22). The active comparator arm was treated as follows: 40 mg/d in 1–4, 9–12, 17–20 of 28 day cycle until disease progression. The primary outcome measured was PFS, and other secondary outcome measures were analyzed. The PFS for POMd was 15.7 weeks (95% CI, 13.0–20.1), versus 8.0 weeks (95% CI, 7.0–9.0) for the high-dose d arm.
As of February 2017, there are 2,100 clinical trials registered in ClinicalTrials.gov studying the condition MM or RRMM, 125 using POM as drug, and 78 clinical trials with POM for MM or RRMM condition, which amounts to only 3.7% of the overall studies in MM. These trials have been designed either to compare the toxicity and/or efficacy of other drugs with POM-based combinations, and enrollment is planned for 13,613 participants. Now, only 6 of them have results. The evolution of POM-based clinical trials is shown in Figure 3.
Figure 3.

Number of POM-based clinical trials by trimesters.
Note: *Data registered until February 27th 2017.
Abbreviation: POM, pomalidomide.
The current role of POM in the MM therapy
The evidence-based impact of any drug on the outcome of MM must be placed in the context of the relative role of several well-established tumor and host-related prognostic factors. On the other hand, only a few drugs have shown a certain level of anti-MM activity to allow its use as monotherapy.39,40 Therefore, the relative influence of each drug in a given combination must be taken into account in the final outcome.
In the NDMM setting, the current approach is using the best available regimen. For instance, a triplet regimen including bortezomib, lenalidomide, and d41 is recommended by the Mayo Clinic as front-line therapy,42 but this combination is still not allowed in many countries. Until now, POM has not been approved for the first-line therapy. Therefore, we will now focus on the use of POM-based combinations in RRMM.
For RRMM patients, the characteristics of the relapse, the critical assessment of the previous treatment, along with the best response achieved and its duration are key issues to guide the best approach. The armamentarium against MM has grown rapidly in recent years. There are several new combinations, such as daratumumab, lenalidomide, and d43 that have been recently approved by the FDA and show impressive results.
The choice of the best therapy at any stage of the MM evolution is challenging, owing to local availability of drug, regulatory health care issues, the impact on quality of life, and cost-effectiveness analysis. The evidence supporting clinical decisions come from both clinical trials and population-based studies. Studies on real-life RRMM patients have demonstrated the importance of optimization and personalization of any line of therapy in order to maximize the risk–benefit ratio. In this regard, it is well known that the sooner a given combination is used, the better the response and DOR. Therefore, the best option for the second-line therapy is increasingly complex. Taking into consideration the overall outcome, the correct sequencing of treatment is a major issue.
The most remarkable aspects about the use of POM-based combinations in RRMM will be highlighted next.
Several phase I clinical trials evaluated the efficacy and safety of POM monotherapy in heavily pretreated patients (median prior lines of therapy, 3–6), with encouraging ORR rates ranging from 25% to 54%.44
The use of POMd in phase II studies showed an improvement in the ORR. Lacy et al45 reported the first phase II study in 60 patients with no more than 3 prior lines of therapy. The patients in this study were treated with 2 mg/d of POM daily and 40 mg/wk of d. After a median follow-up of 27.2 months, the ORR was 65% and median DOR was 21.3 months. Importantly, PFS did not differ between HR and standard-risk patients.
The MM-002 study showed that the MTD of POM was 4 mg/d.46 ORR was 33%, and there was a significant improvement compared to PFS seen with POM alone.47
San Miguel et al48 in the MM-003 study compared POMd with high-dose d in patients in whom treatment with bortezomib and lenalidomide had been exhausted, showing that POMd significantly prolonged median PFS and OS compared with therapy with high-dose d.
There are some real-world studies on the use of POM containing regimens in RRMM.
Maciocia et al49 have shown similar results to MM-003 with the use of POMd in 85 real-world patients in UK, with 5 and 13 months of PFS and OS respectively, but a remarkable 52.9% ORR. Sriskandarajah et al50 showed an ORR of 41% in 39 patients, of whom 30 received POMd and 9 received POM, cyclophosphamide (Cy), and d (POMCyd), with a median of 4 prior lines of therapy. The median PFS was 5.2 (95% CI, 2.6–7.8) months, and OS was 13.1 months (95% CI, 9.1–17.1). Interestingly, the presence of HR cytogenetics had no impact on outcome, and neither did the number of lines of prior therapies. In contrast, the number of cycles delivered did have an impact on OS, with patients receiving 5 or more cycles demonstrating a significant benefit compared to patients who received less than 5 cycles.
The outcome of patients treated with POMd is still poor. Therefore, POMd has been combined with other drugs in triplet therapy. The most promising combinations are summarized in Table 1.
Clarithromycin has been used in association with lenalidomide and d. Likewise, Mark et al51 showed an ORR of 60% in 46 patients with POMd and clarithromycin.
POMCyd is an effective, all-oral regimen for RRMM, as has been demonstrated in two recent phase II studies using 4 mg/d of POM. Baz et al52 showed a 64.7% ORR and PFS of 9.5 months (95% CI, 4.6–14) in 34 evaluable patients, whereas Chari et al53 reported 67% ORR and PFS of 14.5 months in 28 patients. Previously, Larocca et al54 performed a phase 1/2 study, but the dose level of 2.5 mg/d of POM was defined as the MTD, and so the ORR was only 51%.
POMd has been combined with several new PIs. Preliminary results of the combination of weekly carfilzomib with POMd in an Italian phase I/II trial55 showed a double median PFS in comparison with the MM-003. However, the same regimen in the real-world setting as reported by Hobbs et al56 showed a short PFS of only 3.3 months. Krishnan et al57 reported an ORR of 58% in patients with HR cytogenetics by using the all-oral ixazomib-POMd regimen. Spencer et al58 also showed promising activity in heavily pretreated HR RRMM patients by using the combination of marizomib and POMd.
Branca et al59 used daratumumab in combination with POMd in 39 real-life patients with four prior lines of therapy, showing an ORR of 41% and 5% CR. In the same way, Richardson et al60 reported preliminary promising results in a phase 1b trial with isatuximab, another anti-CD38 monoclonal antibody, and POMd.
The all-oral combination of selinexor, a first-in-class selective inhibitor of nuclear export, with POMd has demonstrated in a phase 1/2 trial61 a 60% ORR. Responses were rapid in onset, and 10% CR was achieved.
Pembrolizumab, a programmed death 1 blocking antibody, has been used in combination with POMd in a phase II trial62 showing an ORR of 56% with 8% CR. Median DOR for responding patients was 8.8 months. The addition of pembrolizumab to POMd in a population heavily treated with POMd previously63 still achieved a 33% ORR.
In Spain, a four-drug all-oral combination including POMCyd and clarithromycin is currently being used as a clinical protocol, with promising preliminary results. Moreover, a phase I clinical trial combining POM with nivolumab and d, with or without elotuzumab, is ongoing. On the other hand, Ocio et al64 showed in a phase Ib/II trial that filanesib, a kinesin spindle protein inhibitor, is a good partner for combination with POMd, achieving 50% ORR and 100% disease control rate in refractory MM patients.
Finally, a high level of synergy has been shown between POM and citarinostat (ACY-241),65 a selective histone deacetylase 6 inhibitor, in both in vitro and in vivo preclinical models.
The STRATUS (MM-010)66 study assessed POMd in the largest cohort of patients with RRMM to date. This phase 3b study supports POMd as a standard of care for patients with RRMM, showing an ORR of 32.6% and 4.6 months of median PFS. This doublet is generally well tolerated.
The safety profile of POMd was highlighted in the pivotal MM-003 trial. Only 4% of patients in the POMd group discontinued treatment because of treatment-related adverse events. The most common grade 3–4 adverse events were cytopenias (neutropenia 48%, anemia 33%, and thrombocytopenia 22%), infections (30%), and pneumonia (13%). Only 1% of patients developed grade 3 or greater neuropathy. With thromboprophylaxis, the incidence of deep-vein thrombosis and pulmonary embolism was 2% (1% grade 3–4). The most common cause of death was progression. Infection was the second most common cause of death, but accounted for more deaths in the control arm of the trial. A similar safety profile was observed in the MM-010 trial.
Treatment-related toxicities are usually easily managed using treatment interruption, dose modification, prophylactic therapies, and transfusions.67 POMd is safe and effective for patients with moderate renal impairment (creatinine clearance ≥30 to <60 mL/min).68
POMd is also active and well tolerated in patients with HR disease, particularly in those with del(17p).69,70 POMd leads to significant improvement in health-related quality of life.71
The optimal sequence of therapy, the best clinical target, the identification of biomarkers of response, and the best POM-based combination remain to be defined.
Conclusion
Despite significant advances, almost all patients with MM will eventually relapse. The evolving approach to RRMM therapy is increasingly complex, even with the growing number of regimens available. Some POM-based all-oral triplet therapies, particularly POMCyd, have become a standard of care in RRMM, focusing on the third line of treatment. New POM-based combinations are expected to play an important role in the coming years in the RRMM setting.
Footnotes
Disclosure
R Ríos-Tamayo has received honoraria and participated in advisory boards for Amgen, Janssen, Celgene, Takeda, and Bristol-Myers Squibb. The author has no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. The authors report no other conflicts of interest in this work.
References
- 1.Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538–e548. doi: 10.1016/S1470-2045(14)70442-5. [DOI] [PubMed] [Google Scholar]
- 2.Rajkumar SV. Multiple myeloma: 2016 update on diagnosis, risk-stratification, and management. Am J Hematol. 2016;91(7):719–734. doi: 10.1002/ajh.24402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chng WJ, Dispenzieri A, Chim CS, et al. IMWG consensus on risk stratification in multiple myeloma. Leukemia. 2014;28(2):269–277. doi: 10.1038/leu.2013.247. [DOI] [PubMed] [Google Scholar]
- 4.Usmani SZ, Rodríguez-Otero P, Bhutani M, Mateos MV, San Miguel J. Definign and treating high-risk multiple myeloma. Leukemia. 2015;29(11):2119–2125. doi: 10.1038/leu.2015.209. [DOI] [PubMed] [Google Scholar]
- 5.Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International staging system for multiple myeloma: A report From International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863–2869. doi: 10.1200/JCO.2015.61.2267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Palumbo A, Bringhen S, Mateos MV, et al. Geriatric assessment predicts survival and toxicities in elderly myeloma patients: an International Myeloma Working Group report. Blood. 2015;125(13):2068–2074. doi: 10.1182/blood-2014-12-615187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ríos-Tamayo R, Sánchez MJ, Puerta JM, et al. Trends in survival of multiple myeloma: A thirty-year population-based study in a single institution. Cancer Epidemiol. 2015;39(5):693–699. doi: 10.1016/j.canep.2015.08.002. [DOI] [PubMed] [Google Scholar]
- 8.De Angelis R, Sant M, Coleman MP, et al. Cancer survival in Europe 1999–2007 by country and age: results of EUROCARE-5-a population-based study. Lancet Oncol. 2014;15(1):23–34. doi: 10.1016/S1470-2045(13)70546-1. [DOI] [PubMed] [Google Scholar]
- 9.Ocio EM, Richardson PG, Rajkumar SV, et al. New drugs and novel mechanisms of action in multiple myeloma in 2013: a report of the International Myeloma Working Group (IMWG) Leukemia. 2014;28(3):525–542. doi: 10.1038/leu.2013.350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Anderson KC. Progress and paradigms in multiple myeloma. Clin Cancer Res. 2016;22(22):5419–5427. doi: 10.1158/1078-0432.CCR-16-0625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Alexanian R, Delasalle K, Wang M, et al. Curability of multiple myeloma. Bone Marrow Res. 2012:916479. doi: 10.1155/2012/916479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Barlogie B, Mitchell A, van Rhee F, et al. Curing myeloma at last: defining criteria and providing the evidence. Blood. 2014;124(20):3043–3051. doi: 10.1182/blood-2014-07-552059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Salem KZ, Ghobrial IM. The road to cure in multiple myeloma starts with smoldering disease. Expert Opin Orphan Drugs. 2015;3(6):653–661. doi: 10.1517/21678707.2015.1036740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Palumbo A, Gay F, Cavallo F, et al. Continuous therapy versus fixed duration of therapy in patients with newly diagnosed multiple myeloma. J Clin Oncol. 2015;33(30):3459–3466. doi: 10.1200/JCO.2014.60.2466. [DOI] [PubMed] [Google Scholar]
- 15.Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328–e346. doi: 10.1016/S1470-2045(16)30206-6. [DOI] [PubMed] [Google Scholar]
- 16.Mateos MV, Ocio EM, Paiva B, et al. Treatment for patients with newly diagnosed multiple myeloma in 2015. Blood Reviews. 2015;29(6):387–403. doi: 10.1016/j.blre.2015.06.001. [DOI] [PubMed] [Google Scholar]
- 17.Magarotto V, Bringhen S, Offidani M, et al. Triplet vs doublet lenalidomide-containing regimens for the treatment of elderly patients with newly diagnosed multiple myeloma. Blood. 2016;127(9):1102–1108. doi: 10.1182/blood-2015-08-662627. [DOI] [PubMed] [Google Scholar]
- 18.Rajan AM, Kumar S. Interpretation of cytogenetic results in multiple myeloma for clinical practice. Blood Cancer Journal. 2015;5:e365. doi: 10.1038/bcj.2015.92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kumar SK, Lee JH, Lahuerta JJ, et al. Risk of progression and survival in multiple myeloma relapsing after therapy with IMiDs and bortezomib: a multicenter international myeloma working group study. Leukemia. 2012;26(1):149–157. doi: 10.1038/leu.2011.196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Laubach J, Garderet L, Mahindra A, et al. Management of relapsed multiple myeloma: recommendations of the International Myeloma Working Group. Leukemia. 2016;30(5):1005–1017. doi: 10.1038/leu.2015.356. [DOI] [PubMed] [Google Scholar]
- 21.Dingli D, Ailawadhi S, Bergsagel L, et al. Therapy for relapsed multiple myeloma: Guidelines from the Mayo stratification for myeloma and risk-adapted therapy. Mayo Clin Proc. 2017;92(4):578–598. doi: 10.1016/j.mayocp.2017.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ito T, Ando H, Handa H. Teratogenic effects of thalidomide: molecular mechanisms. Cell Mol Life Sci. 2011;68(9):1569–1579. doi: 10.1007/s00018-010-0619-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chang X, Zhu Y, Shi C, Stewart AK. Mechanism of immunomodulatory drugs’ action in the treatment of multiple myeloma. Acta Biochim Biophys Sin. 2014;46:240–253. doi: 10.1093/abbs/gmt142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rajkumar SV, Witzig TE. A review of angiogenesis and antiangiogenic therapy with thalidomide in multiple myeloma. Cancer Treat Rev. 2000;26(5):351–362. doi: 10.1053/ctrv.2000.0188. [DOI] [PubMed] [Google Scholar]
- 25.Wang M, Dimopoulos MA, Chen C, et al. Lenalidomide plus dexamethasone is more effective than dexamethasone alone in patients with relapsed or refractory multiple myeloma regardless of prior thalidomide exposure. Blood. 2008;112(12):4445–4451. doi: 10.1182/blood-2008-02-141614. [DOI] [PubMed] [Google Scholar]
- 26.Ito T, Ando H, Suzuki T, et al. Identification of a primary target of thalidomide teratogenicity. Science. 2010;327:1345–1350. doi: 10.1126/science.1177319. [DOI] [PubMed] [Google Scholar]
- 27.Ruchelman AL, Man HW, Zhang W, et al. Isosteric analogs of lenalidomide and pomalidomide: Synthesis and biological activity. Bioorg Med Chem Lett. 2013;23(1):360–365. doi: 10.1016/j.bmcl.2012.10.071. [DOI] [PubMed] [Google Scholar]
- 28.Gandhi AK, Kang J, Capone L, et al. Dexamethasone synergizes with lenalidomide to inhibit multiple myeloma tumor growth, but reduces lenalidomide-induced immunomodulation of T and NK cell function. Curr Cancer Drug Targets. 2010;10(2):155–167. doi: 10.2174/156800910791054239. [DOI] [PubMed] [Google Scholar]
- 29.Terpos E, Kanellias N, Christoulas D, et al. Pharmacologic and pharmacokinetic properties of pomalidomide. OncoTargets and Therapy. 2013;6:531–538. doi: 10.2147/OTT.S34498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Richardson PG, Siegel DS, Vij R, et al. Pomalidomide alone or in combination with low-dose dexamethasone in relapsed and refractory multiple myeloma: a randomized phase 2 study. Blood. 2014;123:1826–1832. doi: 10.1182/blood-2013-11-538835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lopez-Girona A, Mendy D, Ito T, et al. Cereblon is a direct protein target for immunomodulatory and antiproliferative activities of lenalidomide and pomalidomide. Leukemia. 2012;26:2326–2335. doi: 10.1038/leu.2012.119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Krönke J, Udeshi ND, Narla A, et al. Lenalidomide causes selective degradation of IKZF1 and IKZF3 in multiple myeloma cells. Science. 2014;343(6168):301–305. doi: 10.1126/science.1244851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pan B, Lentzsch S. The application and biology of immunomodulatory drugs (IMiDs) in cancer. Pharmacol Ther. 2012;136(1):56–68. doi: 10.1016/j.pharmthera.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 34.Rychak E, Mendy D, Shi T, et al. Pomalidomide in combination with dexamethasone results in synergistic anti-tumour responses in pre-clinical models of lenalidomide-resistant multiple myeloma. Br J Haematol. 2016;172(6):889–901. doi: 10.1111/bjh.13905. [DOI] [PubMed] [Google Scholar]
- 35.Escoubet-Lozach L, Lin IL, Jensen-Pergakes K, et al. Pomalidomide and lenalidomide induce p21 WAF-1 expression in both lymphoma and multiple myeloma through a LSD1-mediated epigenetic mechanism. Cancer Res. 2009;69(18):7347–7356. doi: 10.1158/0008-5472.CAN-08-4898. [DOI] [PubMed] [Google Scholar]
- 36.Schey S, Ramasamy K. Pomalidomide therapy for myeloma. Expert Opin Investig Drugs. 2011;20(5):691–700. doi: 10.1517/13543784.2011.567265. [DOI] [PubMed] [Google Scholar]
- 37.Offidani M, Corvatta L, Caraffa P, et al. Pomalidomide for the treatment of relapsed-refractory multiple myeloma: a review of biological and clinical data. Expert Rev Anticancer Ther. 2014;14(5):499–510. doi: 10.1586/14737140.2014.906904. [DOI] [PubMed] [Google Scholar]
- 38.Hoffmann M, Kasserra C, Reyes J, et al. Absorption, metabolism and excretion of [14C] pomalidomide in humans following oral administration. Cancer Chemother Pharmacol. 2013;71(2):489–501. doi: 10.1007/s00280-012-2040-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kortuem KM, Zidich K, Schuster SR, et al. Activity of 129 single-agent drugs in 228 phase I and II clinical trials in multiple myeloma. Clin Lymphoma Myeloma Leuk. 2014;14(4):284–290. doi: 10.1016/j.clml.2013.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rajan AM, Kumar S. New investigational drugs with single-agent activity in multiple myeloma. Blood Cancer J. 2016;6:e451. doi: 10.1038/bcj.2016.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Durie BGM, Hoering A, Abidi MH, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. Lancet. 2017;389(10068):519–527. doi: 10.1016/S0140-6736(16)31594-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kapoor P, Rajkumar SV. Multiple myeloma in 2016: fresh perspectives on treatment and moments of clarity. Nature Rew Clin Oncol. 2017;14(2):73–74. doi: 10.1038/nrclinonc.2016.221. [DOI] [PubMed] [Google Scholar]
- 43.Dimopoulos MA, Oriol A, Nahi H, et al. Daratumumab, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2016;375(14):1319–1331. doi: 10.1056/NEJMoa1607751. [DOI] [PubMed] [Google Scholar]
- 44.Richardson PG, Mark TM, Lacy MQ. Pomalidomide: New immunomodulatory agent with potential antiproliferative effects. Crit Rev Oncol Hemat. 2013;88(Suppl 1):S36–S44. doi: 10.1016/j.critrevonc.2013.02.001. [DOI] [PubMed] [Google Scholar]
- 45.Lacy MQ, Hayman SR, Gertz MA, et al. Pomalidomide (CC4047) plus low-dose dexamethasone as therapy for relapsed multiple myeloma. J Clin Oncol. 2009;27(30):5008–5014. doi: 10.1200/JCO.2009.23.6802. [DOI] [PubMed] [Google Scholar]
- 46.Richardson PG, Siegel D, Baz R, et al. Phase 1 study of pomalidomide MTD, safety, and efficacy in patients with refractory multiple myeloma who have received lenalidomide and bortezomib. Blood. 2013;121(11):1961–1967. doi: 10.1182/blood-2012-08-450742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Richardson PG, Siegel DS, Vij R, et al. Pomalidomide alone or in combination with low-dose dexamethasone in relapsed and refractory multiple myeloma: a randomized phase 2 study. Blood. 2014;123(12):1826–1832. doi: 10.1182/blood-2013-11-538835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.San Miguel J, Weisel K, Moreau P, et al. Pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone alone for patients with relapsed and refractory multiple myeloma (MM-003): a randomised, open-label, Phase 3 trial. Lancet Oncol. 2013;14(11):1055–1066. doi: 10.1016/S1470-2045(13)70380-2. [DOI] [PubMed] [Google Scholar]
- 49.Maciocia N, Melville A, Maciocia PM, et al. Real-world use of pomalidomide and dexamethasone in double refractory multiple myeloma: a multicentre UK experience. Blood. 2016;128(22) abstract 3312. [Google Scholar]
- 50.Sriskandarajah P, Pawlyn C, Mohammed K, et al. The efficacy and tolerability of pomalidomide in relapsed/refractory myeloma patients in a “real-world” study: the Royal Marsden Hospital experience. Leuk Lymphoma. 2017;58(2):494–497. doi: 10.1080/10428194.2016.1198957. [DOI] [PubMed] [Google Scholar]
- 51.Mark T, Rodriguez M, Shah M, et al. ClaPD (Clarithromycin/[Biaxin®], Pomalidomide, Dexamethasone) therapy in relapsed or refractory multiplemyeloma. Blood. 2011;118(21) abstract 635. [Google Scholar]
- 52.Baz RC, Martin TG, 3rd, Lin HY, et al. Randomized multicenter phase 2 study of pomalidomide, cyclophosphamide, and dexamethasone in relapsed refractory myeloma. Blood. 2016;127(21):2561–2568. doi: 10.1182/blood-2015-11-682518. [DOI] [PubMed] [Google Scholar]
- 53.Chari A, Cho HJ, Parekh S, et al. A phase II study of pomalidomide, daily low dose oral cyclophosphamide, and dexamethasone in relapsed/refractory multiple myeloma. Blood. 2016;128(22) abstract 4520. [Google Scholar]
- 54.Larocca A, Montefusco V, Bringhen S, et al. Pomalidomide, cyclophosphamide, and prednisone for relapsed/refractory multiple myeloma: a multicenter phase 1/2 open-label study. Blood. 2013;122(16):2799–2806. doi: 10.1182/blood-2013-03-488676. [DOI] [PubMed] [Google Scholar]
- 55.Bringhen S, Magarotto V, Liberati AM, et al. A multicenter, open label phase I/II study of carfilzomib, pomalidomide and dexanethasone in relapsed and/or refractory multiple myeloma (MM) patients. Blood. 2016;128(22) abstract 1145. [Google Scholar]
- 56.Hobbs M, Paludo J, Fonder A, et al. Efficacy of carfilzomib (K), pomalidomide (P), and dexamethasone (d) in heavily pretreated patients with relapsed/refractory multiple myeloma (RRMM) in a real world setting. Blood. 2016;128(22) abstract 3337. [Google Scholar]
- 57.Krishnan A, Kapoor P, Palmer J, et al. A phase I/II trial of Ixazomib (Ix), Pomalidomide (POM), and Dexamethasone (DEX), in relapsed/refractory (R/R) multiple myeloma (MM) patients: Responses in double/triple refractory myeloma and poor risk cytogenetics. Blood. 2016;128(22) abstract 3316. [Google Scholar]
- 58.Spencer A, Harrison S, Laubach JP, et al. Pmd-107: marizomib, pomalidomide and low dose-dexamethasone combination study in relapsed/refractory multiple myeloma ( NCT02103335): Full enrollment results from a phase-1 multicenter, open label study. Blood. 2016;128(22) abstract 3326. [Google Scholar]
- 59.Branca A, Buros A, Yoon D, et al. Daratumumab single agent and daratumumab plus pomalidomide and dexametasone in relapsed/refractory multiple myeloma: A real life retrospective evaluation. Blood. 2016;128(22) abstract 4516. [Google Scholar]
- 60.Richardson PG, Mikhael J, Usmani SZ, et al. Preliminary results from a phase Ib study of isatuximab in combination with pomalidomide and dexamethasone in relapsed and refractory multiple myeloma. Blood. 2016;128(22) abstract 2123. [Google Scholar]
- 61.Chen C, Kotb R, Sebag M, et al. Selinexor shows synergy in combination with pomalidomide and low dose dexamethasone in patients with relapsed/refractory multiple myeloma. Blood. 2016;128(22) abstract 3330. [Google Scholar]
- 62.Badros AZ, Hyjek E, Lesokhin AM, et al. Pembrolizumab in combination with pomalidomide and dexamethasone for relapsed/refractory multiple myeloma (RRMM) Blood. 2016;128(22) abstract 490. [Google Scholar]
- 63.Wilson L, Cohen AD, Weiss BM, et al. Pembrolizumab in combination with pomalidomide and dexamethasone (PEMBRO/POM/DEX) for pomalidomide exposed relapsed or refractory multiple myeloma. Blood. 2016;128(22) abstract 2119. [Google Scholar]
- 64.Ocio EM, Motlló C, Rodríguez-Otero P, et al. Safety and efficacy of filanesib in combination with pomalidomide and dexamethasone in refractory MM patients. Phase Ib/II Pomdefil clinical trial conducted by the Spanish MM Group. Blood. 2016;128(22) doi: 10.1111/bjh.16788. abstract 4503. [DOI] [PubMed] [Google Scholar]
- 65.North BJ, Almeciga-Pinto I, Tamang D, et al. Enhacement of pomalidomide anti-tumor response with ACY-241, a selective HDAC6 inhibitor. Plos One. 2017;12(3):e0173507. doi: 10.1371/journal.pone.0173507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Dimopoulos MA, Palumbo A, Corradini P, et al. Safety and efficacy of pomalidomide plus low-dose dexamethasone in STRATUS (MM-010): a phase 3b study in refractory multiple myeloma. Blood. 2016;128(4):497–503. doi: 10.1182/blood-2016-02-700872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Jones JR, Pawlyn C, Davies FE, Morgan GJ. The safety of pomalidomide for the treatment of multiple myeloma. Expert Opinion on Drug Safety. 2016;15(4):535–547. doi: 10.1517/14740338.2016.1154039. [DOI] [PubMed] [Google Scholar]
- 68.Siegel DS, Weisel KC, Dimopoulos MA, et al. Pomalidomide plus low-dose dexamethasone in patients with relapsed/refractory multiple myeloma and moderate renal impairment: a pooled analysis of three clinical trials. Leuk Lymphoma. 2016;57(12):2833–2838. doi: 10.1080/10428194.2016.1177181. [DOI] [PubMed] [Google Scholar]
- 69.Leleu X, Karlin L, Macro M, et al. Pomalidomide plus low-dose Dexamethasone in Multiple Myeloma with deletion 17p and/or translocation (4;14). IFM 2010-02. Blood. 2015;125(9):1411–1417. doi: 10.1182/blood-2014-11-612069. [DOI] [PubMed] [Google Scholar]
- 70.Dimopoulos MA, Weisel KC, Song KW, et al. Cytogenetics and long-term survival of patients with refractory or relapsed and refractory multiple myeloma treated with pomalidomide and low-dose dexamethasone. Haematologica. 2015;100(10):1327–1333. doi: 10.3324/haematol.2014.117077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Song KW, Dimopoulos MA, Weisel KC, et al. Health-related quality of life from the MM-003 trial of pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone in relapsed and/or refractory multiple myeloma. Haematologica. 2015;100(2):e63–e67. doi: 10.3324/haematol.2014.112557. [DOI] [PMC free article] [PubMed] [Google Scholar]