

SYNOPSIS
Gastrointestinal conditions are prevalent in the population and account for significant morbidity and healthcare costs. Patients with gastrointestinal conditions frequently use integrative medicine. There is growing evidence that integrative medicine approaches can improve symptoms and, in some cases, directly affect physiology and disease course. In this article we review the data on some of the most common and well-studied approaches including mind-body therapies, acupuncture, diet, probiotics, and other dietary supplements and herbs in gastroesophageal reflux disease, inflammatory bowel disease, irritable bowel syndrome, non-alcoholic fatty liver disease, and nausea and vomiting. While clear recommendations can be made for some conditions, in others there are challenges in translating these findings due to small study size, lack of standardization, and trial heterogeneity.
Keywords: Complementary therapies, Integrative medicine, Digestive system diseases, Gastroesophageal reflux disease, Inflammatory bowel disease, Irritable bowel syndrome, Liver disease, Nausea
Introduction
Gastrointestinal (GI) conditions account for substantial morbidity, mortality, and healthcare costs in the US.1 Approximately 42% of the U.S. adult population with GI conditions have used integrative therapies over the course of a given year.2 Interest in, and research on, integrative approaches for addressing GI conditions is growing, in part due to the recognition of the importance of the gut microbiome on human health, the effects of stress on the enteric nervous system, and their interrelationship.3 While an exhaustive review of integrative approaches for managing GI disease is outside of the scope this work, here we focus on the more common and studied approaches for addressing common GI disorders.
Gastroesophageal Reflux Disease
Gastroesophageal reflux disease (GERD) is one of the most prevalent health-related conditions in the Western world with prevalence estimates ranging from 20–40%.4,5 GERD is primarily a clinical diagnosis, characterized by symptoms of heartburn and acid reflux. It is associated with decreased health-related quality of life and significant healthcare costs and lost productivity.6,7 Several integrative therapies may help reduce symptoms.
Acupuncture
Two studies from China suggest that acupuncture (4 points stimulated daily for 6 weeks with a 2–3 day break between each week of stimulation) can significantly reduce esophageal acid and bile reflux and improve GERD-related symptoms.8,9 Another study found that for individuals with ongoing GERD symptoms despite once daily proton pump inhibitor (PPI) therapy, addition of acupuncture (10 sessions over 4 weeks) was more effective than doubling the PPI dose.8,10 Many patients with GERD also have functional dyspepsia, and acupuncture treatment appears to be effective for those symptoms as well, perhaps through a centrally mediated mechanism.11
Mind-Body Therapies
Anxiety and depression are known to increase reports of GERD symptoms, and patients who respond less well to PPI therapy are more likely to suffer from psychological distress.8 In small studies, hypnotherapy, biofeedback, and muscle relaxation techniques have been shown to improve GERD symptoms.8 In a recent randomized controlled trial (RCT) of diaphragmatic breathing exercises for patients with non-erosive GERD, subjects were instructed to practice for 30 minutes daily and were given a recording with instructions and relaxing music.12 After 4 weeks, those practicing the breathing exercises had a significant decrease in esophageal acid exposure by esophageal manometry and improvements in quality of life, whereas there were no changes in the control group. In those still practicing at 9 months, proton pump inhibitor use was decreased.
Herbs and Dietary Supplements
Melatonin is synthesized in the gastrointestinal tract and is an important gut motility signal. Two studies suggest that melatonin may be as or more effective than omeprazole 20 mg in reducing GERD-related symptoms.10 One study examined 3 mg of melatonin daily, the other examined 6 mg of melatonin in combination with several vitamins and amino acids. The only side effect noted in the latter study was somnolence.
STW 5 (Iberogast) is a commercial formula that includes nine botanicals: Iberis amara, Matricaria chamomilla, Carum carvi, Mentha piperita, Glycyrrhiza glabra, Melissa officinalis, Chelidonium majus, Silybum marianum, and Angelica archangelica.10 In three studies of functional dyspepsia that included patients with GERD symptoms, those receiving STW 5 were more likely to have improvement in symptoms than those receiving placebo. STW 5 was most effective for epigastric pain, retrosternal pain, and acid regurgitation. Adverse events were similar to placebo and included dermatitis, angioedema, digestive intolerance, and one case of allergic asthma. The product has been sold in Germany for 40 years and has a good safety profile.
Raft-forming agents include alginate, pectin, and carbenoxolone (a synthetic derivative of glycyrrhizin). When these compounds come in contact with gastric acid, they form polymers and float to the surface of the stomach contents, providing a barrier that protects the esophagus from acid reflux.10 These agents lack major side effects and are useful in treating mild-to moderate GERD.
Some patients take deglycyrhiziniated licorice (DGL), chamomile, slippery elm, marshmallow root, D-limonene, and/or betaine. These products are part of the herbal and naturopathic medicine traditions for GERD treatment, however, there are no rigorous studies evaluating their efficacy. It is important to note that herbs from the mint family (e.g., peppermint, spearmint) can reduce lower esophageal sphincter pressure and may exacerbate reflux.10,13
Nutrition and Lifestyle Interventions
Studies of the effects of diet on heartburn and reflux symptoms have often yielded contradictory results, perhaps because different foods or nutrients exacerbate symptoms in different individuals.10,13 Foods which have been associated with increased GERD-related symptoms include: fatty, fried, and spicy foods, citrus, tomato-based products, and alliums (e.g., onion, garlic). Chocolate, peppermint, coffee, carbonated beverages, and alcohol can all decrease lower esophageal sphincter tone and may play a role. In addition, consumption of fewer meals with a large meal in the evening is associated with increased GERD symptoms.13 Weight loss (obesity increases the risk of GERD) and elevating the head of the bed can help decrease symptoms.10
Summary
There is good evidence for acupuncture, raft-forming agents, Iberogast, weight loss, and elevating the head of the bed for reducing GERD-related symptoms. There is reasonable evidence to consider mind-body approaches (especially if stress may be playing a role), melatonin, and dietary modification.
Inflammatory Bowel Disease
Inflammatory bowel disease (IBD) includes both ulcerative colitis (UC) and Crohn’s disease (CD). Use of integrative medicine among patients with IBD is common, with current or past use ranging from 21–60% of patients.14 The most commonly used modalities are homeopathy, herbal products, and probiotics, followed by specific diets and traditional Chinese medicine (TCM) and acupuncture.15 However, there are few studies for most of these modalities and of those that are available, most are pilot studies with small numbers of subjects. We review the most studied therapies.
Herbal Medicines
Two recent reviews examined herbal products for IBD.14,16 The best evidence is for Plantago ovata and curcumin in UC maintenance therapy and Artemisia absinthium (wormwood) in CD. Aloe vera, Boswellia serrata, wheat grass, Andrographis paniculata, silymarin, cannabis, evening primrose oil, mastic gum, and a few herbal combinations have all been studied but there is insufficient data to make conclusions about effectiveness.
In an open-label trial of 105 patients with UC in remission, Plantago ovata seeds (10g twice daily) were as effective as mesalamine in maintaining remission at 12 months. Subjects receiving Plantago ovata had higher levels of butyrate in their stool. Side effects were few, mainly constipation and bloating.14,16
Curcumin is a phytochemical present in turmeric and has potent anti-inflammatory activity. In a double-blind RCT of 89 patients with quiescent UC, subjects were randomized to curcumin 1 g twice daily or placebo with sulfasalazine or mesalamine. After 6 months, the curcumin group had a significantly lower rate of relapse as well as lower clinical activity index and endoscopic index compared to the placebo group.14,16
Two studies of Artemisia absinthium in patients with active CD have suggested benefit.14,16 In one trial, 40 patients were randomized to receive Artemisia absinthium 500 mg three times daily or placebo in addition to prednisone. After 8 weeks there was near complete clinical remission in 65% of the intervention subjects and none within the placebo group. Artemisia absinthium was also steroid sparing. In another study, Artemisia absinthium treatment was associated with reductions in TNF-α and improvements in quality of life. In both studies, adverse events were similar in the intervention and comparison groups.
Three studies of Tripterygium wilfordii (Thunder God Vine) suggest that it is as or more effective than sulfasalazine or mesalamine for the prevention of post-surgical relapse (clinically and endoscopically) in CD.16 Though well-tolerated in these studies, there is concern about potential side effects and toxicity of the plant.17
Probiotics
Providing recommendations on the use of probiotics in IBD is challenging given the small numbers of subjects in most studies and the wide variety of organisms used. A recent review concluded that evidence suggests that the probiotic combination VSL#3 is effective in inducing remission in mild to moderate UC (alone or combined with conventional therapies) and that E. coli Nissle 1917 strain is effective in maintaining remission in UC.18 There is insufficient data on the use of probiotics in CD to provide recommendations.
Fish oil
Fish oil contains omega-3 fatty acids known to have anti-inflammatory properties. A Cochrane review examining the effects of fish oil on induction of remission in patients with UC concluded that there was insufficient data to determine whether fish oil is effective for inducing remission in ulcerative colitis.19 A more recent Cochrane review examined the evidence for omega-3 fatty acids in maintenance of remission in CD and concluded that based on two large, high quality RCTs, omega-3 fatty acids are likely ineffective.20
Mind-Body Therapies
Studies of several different mind-body interventions including mindfulness-based stress reduction, relaxation therapy, hypnotherapy, and comprehensive lifestyle programs have been studied in patients with UC and CD, mostly in those with inactive disease.16,21 Stress is a risk factor for disease flare. In general these studies suggest improvements in quality of life, and sometimes anxiety and pain, but did not change laboratory parameters or reduce disease activity, though these studies may have been underpowered to detect the latter.
Traditional Chinese Medicine/Acupuncture
Two studies have suggested benefit with acupuncture and moxibustion in patients with active UC or CD with regard to disease activity but did not show improvement in quality of life or symptoms. Additional studies of acupuncture and moxibustion have been conducted but were of such poor methodological quality that no definitive conclusion can be made.14
Nutrition
The internet contains conflicting information on dietary approaches to ameliorate IBD, and data suggests that patients and clinicians have differing attitudes toward the role of diet and dietary modifications.22,23 Importantly, patients with IBD commonly have both protein-energy and micronutrient deficiencies that can adversely affect patient outcomes.24 Epidemiologic studies have suggested that diets high in sucrose, animal fats, and fast foods are risk factors for the development of IBD whereas diets rich in unsaturated fats, fruits, vegetables, and whole grains are protective. Food additives such as maltodextrin, carageenans, titanium dioxide, and aluminum silicates have been shown to injure enterocytes or alter enteric immune responses in animal models. Exclusive enteral nutrition (EEN) has clear benefits for inducing remission in patients with active CD. There is emerging data that the specific carbohydrate diet (eliminates all dietary disaccharides, oligosaccharides, and polysaccharides) and low FODMAP diet (see Table 1) may help reduce symptoms in patients with IBD.25,26 Single studies have demonstrated some improvement with a semi-vegetarian diet, gluten-free diet, or allergen elimination diet. Given the potential for elimination/exclusion diets to exacerbate nutritional deficiencies, we recommend that patients work with a nutritionist or registered dietician who has expertise in helping patients with IBD.
Table 1.
Low and High FODMAP Foods*
| Low FODMAP foods | High FODMAP foods |
|---|---|
| Broccoli | Garlic |
| Cabbage | Onions |
| Carrots | Artichoke |
| Collard greens | Asparagus |
| Kale | Black beans |
| Olives | Cauliflower |
| Radish | Mushrooms |
| Red peppers | Soy beans |
| Spinach | Apples |
| Bananas | Avocado |
| Blueberries | Mango |
| Beef | Wheat |
| Chicken | Cashews |
| Tuna | Rye |
| Gluten-free breads | Granola |
| Alcohol | Honey |
| Coffee | Beer |
| Tofu | Dairy |
For additional information see: http://www.ibsdiets.org/fodmap-diet/fodmap-food-list/
Summary
In UC, there is good evidence for Plantago ovata (10 g twice daily), curcumin (1 g twice daily), and E. coli Nissle 1917 for maintenance therapy and VSL#3 for inducing remission. In active CD there is good evidence for exclusive enteral nutrition and Artemisia absinthium (500 mg three times daily) for inducing remission. In IBD in general, there is reasonable evidence to consider mind-body approaches, acupuncture, the specific-carbohydrate diet, and/or the low FODMAP diet for symptom reduction. Though there is good data for Tripterygium wilfordii in CD, there is concern about potential toxicity and more data is needed.
Irritable Bowel Syndrome
Irritable bowel syndrome (IBS) is a functional bowel disorder (FBD) characterized by chronic abdominal pain and altered bowel habits in the absence of any organic etiology.27 In North America and Europe its prevalence is around 12%.28,29 IBS likely has multifactorial roots related to alterations in gastrointestinal motility, alterations in fecal flora, visceral hypersensitivity, previous infections, inflammation, bacterial overgrowth and food sensitivity.30 IBS accounts for a significant number of primary care visits and up to 50% of all referrals to general gastroenterologists.31 IBS subtypes include IBS with predominant constipation (IBS-C), IBS with predominant diarrhea (IBS-D) and IBS with mixed bowel habits (IBS-M). Certain treatments may work better than others for specific IBS subtypes, however, the integrative medicine literature largely does not distinguish between IBS subtypes.
Testing
IBS is a diagnosis of exclusion, and alarm features (e.g., nocturnal or progressive abdominal pain or diarrhea, rectal bleeding in the absence of documented bleeding hemorrhoids or anal fissures, unintentional weight loss, or laboratory abnormalities such as anemia, elevated inflammatory markers, or electrolyte disturbances) should always be evaluated.32 Clinicians must also exclude concomitant IBD, infection, malignancy, microscopic colitis, small intestinal bacterial overgrowth (SIBO), lactose or fructose intolerance, and celiac disease among other entities, however, overlap between IBS and these entities does exist.33 Appropriate testing will depend upon the patients’ symptoms and context. Some patients may specifically ask about complete stool analyses, food allergy or food sensitivity tests, and intestinal permeability tests. Food allergy testing is particularly challenging given the potential for false positives and false negatives and requires careful interpretation.34 Providers can consider training in functional medicine to learn more or refer to an integrative medicine center that incorporates functional medicine testing.
Mind-Body Therapies
A meta-analysis of yoga for IBS found significant reductions in bowel symptoms and anxiety, although heterogeneity of controls, multiple sources of potential bias and inadequate reporting of randomization methods tempered this conclusion.35 A meta-analysis evaluating 7 RCTs of hypnosis found a significant improvement in abdominal pain at 3 months though performance bias (salutary effects of the provider-patient interaction) and difficulties with blinding likely contribute to positive effects.36 A larger meta-analysis of psychological therapies (mindfulness, relaxation, cognitive behavioral therapy, hypnosis, and stress reduction techniques) for IBS calculated a pooled risk ratio for improvement of 1.47, favoring psychological therapies.37 These studies were quite heterogeneous with different control arms and criteria for improvement. Meditation and mindfulness-based approaches also show promise in IBS with sustained symptom improvements in abdominal pain, quality of life, and other associated symptoms.21,38,39 Given the favorable safety profile of mind-body therapies and the likelihood that some individuals will derive significant benefit, it is reasonable to recommend such practices for patients with IBS.
Special diets and dietary supplements
The role of nutrition in the pathogenesis and management of IBS has evolved in recent years with increasing evidence supporting the recommendation of various dietary interventions. Notably, patients should be asked about their diet with special attention paid to the ingestion of caffeine, wheat, fruits, vegetables, dairy products, sweetened soft drinks, and chewing gum as these can mimic or exacerbate IBS symptoms.40 Interesting, dietary restriction of gluten globally improves symptoms in IBS patients in whom celiac disease was carefully excluded.41 Mechanistically, it has been shown that gluten alters bowel barrier functions in patients with IBS-D.42
Low FODMAP Diet
FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) are short-chain carbohydrates that are incompletely absorbed in the small intestine, fermented in the colon, and are associated with bloating, diarrhea and abdominal pain. FODMAP reduction decreases the osmotic load and gas production in the distal small bowel and the proximal colon, providing symptomatic relief in patients with IBS. Table 1 lists low and high FODMAP foods. A recent meta-analysis of 6 RCTs and 16 non-randomized studies showed that a low FODMAP diet was associated with reduced abdominal pain, bloating and improvement in overall symptom score.43 Overall, up to 86% of patients with IBS may find improvement in their gastrointestinal symptoms following the diet including those of constipation and flatulence as well as abdominal pain, diarrhea and bloating.44 While a low FODMAP diet appears safe for short-term use, long-term data is lacking and adherence can be challenging. Nutritional intervention by specialized dietitians may improve the success of the low FODMAP diet.
Dietary Fiber
Dietary fiber supplementation has long served as a standard component of IBS management, however, its optimal use can be nuanced given that certain forms of fiber, such as bran, in specific patients may exacerbate abdominal distention and flatulence.45 Additionally, high amounts of dietary fiber can impair absorption of certain medications, thus medications should be taken one hour before or two hours after fiber supplementation.46 Additional information regarding soluble and insoluble fiber is presented in Table 2 and a recent review.47 Fiber should be most often considered in patients with IBS whose predominant symptom is constipation. It is believed that dietary fiber softens stool by drawing in water for easier passage. A recent systematic review and meta-analysis on the effect of fiber supplementation on IBS evaluated 14 RCTs involving 906 subjects and concluded that there was a significant benefit of soluble fiber in IBS with a number needed to treat (NNT) of 7 subjects, however, no benefit was seen with wheat bran.45 However, a Cochrane review evaluating 12 studies found no beneficial effect for bulking agents over placebo in improving abdominal pain, global assessment or symptom scores.48 Interestingly, in constipation, prunes appear superior to psyllium for improving stool frequency and consistency.49
Table 2.
Soluble and Insoluble Fiber
| Soluble Fiber | Insoluble Fiber |
|---|---|
| Absorbs water and reduces glycemic response and plasma cholesterol | Increases fecal bulk and decreases intestinal transit |
| Types include pectins and gums | Types include cellulose and lignin |
Foods high in soluble fiber:
|
Foods high in insoluble fiber:
|
Probiotics
A systematic review of 19 RCTs in 1650 patients with IBS concluded that probiotics were statistically significantly better than placebo with an NNT of 4 subjects.50 However the most effective species and strains are uncertain based on heterogeneity in the studies. A more recent meta-analysis of 1793 patients demonstrated that probiotics reduce pain and global symptom severity in patients with IBS compared to placebo.51 While probiotics are felt to be safe with a generally favorable side effect profile aside from mild gas and bloating, there is a theoretical risk of causing infection in individuals with compromised immune systems.52
Peppermint Oil
Peppermint oil is derived from the peppermint plant and causes relaxation of gastrointestinal smooth muscle through blockade of calcium channels.53 While peppermint oil is generally well tolerated, smooth muscle relaxation can occur at both the intestinal level as well as the lower esophageal sphincter and thus lead to gastroesophageal reflux. Aside from heartburn, common adverse effects may include allergic reactions, blurred vision, perianal burning, nausea, and vomiting.53 At very high doses it has been associated with acute renal failure via interstitial nephritis. It may inhibit the cytochrome P450 1A2 system and thus medication interactions should be evaluated such as those of cyclosporine and statin drugs.53 A meta-analysis of four RCTs with 392 subjects with IBS found peppermint oil to be superior to placebo for global symptom reduction (especially abdominal pain and diarrhea) compared with placebo with an NNT to prevent persistent symptoms of 2.5.54 More recently, a meta-analysis of 9 RCTs with 726 patients showed that peppermint oil was superior to placebo for global improvement of IBS symptoms.55 In this analysis, the reported adverse events in the placebo-controlled studies were mild and transient and included heartburn, dry mouth, belching, peppermint taste, rash, dizziness, headache, increased appetite, and a cold perianal sensation. Peppermint oil is best taken in the form of enteric-coated capsules (containing 0.2 mL of oil) which reduces the risk of heartburn and the recommended dosage for adults is 1–2 capsules three times per day before meals.53
Acupuncture
A clear consensus on the effects of acupuncture in IBS has been challenging due to small, heterogeneous, and methodologically unsound trials. A Cochrane review of 17 RCTs with 1806 subjects found no benefit of acupuncture relative to a credible sham acupuncture control on IBS symptom severity or IBS-related quality of life.56 However, even “sham” acupuncture may have clinical effects as needles are often placed into the skin. Moreover, subgroup analyses revealed that acupuncture was more effective than either pharmacotherapy (RR 1.28, 5 studies, 449 patients) or no specific therapy (RR 2.11, 2 studies, 181 patients). In this analysis, there was one adverse event (i.e. syncope) associated with acupuncture. Other side effects which have been reported are often mild and transient including aching at the sites of needle insertion and dizziness however more serious rare events have been reported including bruising, infection, and bleeding.57
Summary
There is good evidence for mind-body therapies, low FODMAP diet, probiotics, and enteric-coated peppermint oil (0.2 – 0.4 mL three times per day for abdominal pain) for reducing IBS-related symptoms. There is reasonable evidence to consider soluble fiber supplementation (especially for constipation), a trial of gluten elimination, and acupuncture.
Liver Disease
Non-alcoholic fatty liver disease (NAFLD) is perhaps the most common liver disorder with prevalence estimates over 20% in North America and Europe and growing rates in other countries.58 NAFLD is associated with obesity and metabolic syndrome. Lifestyle modification is critical, however, a growing number of studies suggest potential benefits with herbs and dietary supplements. Less data is available for Hepatitis C and other liver diseases.
Herbal Medicines and Vitamin E
A systematic review of 419 studies of traditional Chinese medicine (TCM) herbal combinations (246 different herbs overall) in patients with NAFLD concluded that overall there were improvements in labs and steatosis on imaging and that TCM provides modest benefit in NAFLD59. A Cochrane review examined 77 RCTs of 6753 participants which included 75 different herbal medicine products.58 Some products had positive effects on liver enzymes (AST, ALT), ultrasound, and CT results. There was no significant different between herbal medicine and control groups in terms of adverse effects. No definitive conclusions could be made due to high risk of bias and the limited number of studies testing individual herbs.
Another review specifically examined silymarin, a lipophilic extract from the milk thistle plant.60 Seven studies of varying doses of silymarin with or without Vitamin E and other anti-oxidants were examined in patients with NAFLD. In one study, 138 patients received treatment or placebo for 12 months. Side effects were mild and included diarrhea, dysgeusia, and pruritus. The authors concluded that there was good clinical evidence for silymarin at 140 mg/day combined with vitamin E in the treatment of NAFLD. A major challenge is that extraction and standardization methods for the compounds used in these studies has not been adequately described. Another meta-analysis concluded that oral silymarin had no benefit on aminotransferase levels or viral load in patients with chronic hepatitis C infection.61 Finally, Vitamin E may improve liver enzymes in NAFLD, non-alcoholic steatohepatitis, and chronic hepatitis C, however, dosing varied greatly in the studies examined.62
Probiotics
A review of probiotic use in patients with a variety of different liver conditions (hepatic encephalopathy, NAFLD, alcoholic liver disease, hepatocellular carcinoma, and patients undergoing liver surgery) concluded that probiotics show promise in reducing the incidence of hepatic encephalopathy, improving serum liver enzymes and inflammatory markers, and reducing post-surgical infections.63 In a review of probiotics for NAFLD, the authors found that probiotic administration reduced serum aminotransferase levels, total cholesterol, TNF-α, and improved insulin resistance.64 Another review of 10 studies of probiotics for NAFLD found similar benefits including improvements in ultrasound-based fatty liver scores.65 However, given the variety of products used, it is unclear which organisms or dose is most effective.
Summary
There is good evidence for weight loss, silymarin (140 mg/day) combined with vitamin E, and probiotics for patients with NAFLD. There is insufficient data to recommend any specific therapy for chronic hepatitis C virus infection.
Nausea and Vomiting
Integrative therapies have been used for the treatment of nausea and vomiting in a variety of settings. Here we present the most studied therapies.
Ginger (Zingiber officinale)
Ginger is one of the most well-known and studied herbal treatments for nausea. Gingerols and shogaols are thought be among its pharmacoactive constituents, and may have anticholinergic and antiserotonergic effects.66 Evidence suggests that ginger may be effective in reducing morning sickness, postoperative nausea and vomiting, and antiretroviral-induced nausea and vomiting.67 Doses range from 1–2 g daily. A meta-analysis of 12 studies concluded that ginger is likely safe and may be effective in reducing nausea associated with pregnancy.68 Another meta-analysis of ginger in pregnancy included 6 studies and 508 subjects and concluded a 5-fold pooled likelihood of improvement with 4 consecutive days of 1 g daily.69 A study of 102 HIV positive patients randomized to ginger or placebo at the initiation of anti-retroviral therapy resulted in 90% of the placebo group experiencing some degree of nausea versus 56% of the ginger group (p=0.001).70 A meta-analysis in chemotherapy-induced nausea and vomiting found no significant difference in the incidence and severity of nausea and vomiting in the ginger groups versus placebo or metoclopramide.71 These results are difficult to interpret as there were only 5 trials and comparison groups included both placebo and active control. Overall, ginger is likely effective for a variety of conditions producing nausea.
Vitamin B6 (pyridoxine)
A study comparing vitamin B6 to ginger found ginger more effective for reducing nausea, but equally effective for reducing vomiting associated with pregnancy.72 Another study found that ginger and vitamin B6 both significantly reduced nausea in pregnancy equivalently.73 A Cochrane review concluded that Vitamin B6 is possibly effective in reducing pregnancy-associated nausea, but that data are insufficient.74 Dosing in studies ranged from 10–25 mg every 8 hours to 50 mg daily. Vitamin B6 has not been extensively studied in other conditions producing nausea. B6 has a long record of safety, however, there are reports of B6 toxicity leading to peripheral neuropathy.75
Aromatherapy
Aromatherapy, typically in the form of ginger or peppermint oil, has also been used to reduce nausea. A recent qualitative review found that these two oils were most commonly used and may be effective, although all studies suffered from significant design flaws.76 A Cochrane review of nine trials (6 RCTs and 3 controlled clinical trials) concluded that isopropyl alcohol was more effective than saline for post-operative nausea but less effective than standard anti-emetics.77 There was insufficient evidence to evaluate studies of peppermint oil. A more recent study randomized 301 patients to normal saline, 70% isopropyl alcohol, ginger oil or a blend of oils including peppermint and they found a significant reduction in nausea and anti-emetic use in the ginger and blend group but not isopropyl alcohol.78
Acupuncture and Acupressure
A reductionist approach to studying acupuncture is difficult because of the nuances of individual treatment and the different points that may be stimulated. Nevertheless, one point in particular, the PC6 point (located 2 . to 3 fingerbreadths from the wrist crease up the arm, see Figure 1), has emerged with the most supportive evidence for use in reducing nausea. A meta-analysis concluded that acupuncture at PC6 is likely effective for reducing post-operative nausea, but that there are insufficient data to support efficacy for other points with or without PC6.79 A Cochrane review of 59 trials involving 7667 subjects examined acupuncture stimulation at PC6 for prevention of post-operative nausea and vomiting.80 The authors found low-quality evidence for efficacy of PC6 over sham, and moderate quality evidence that there was no significant difference between acupressure and anti-emetics. Finally, a recent systematic review evaluating 29 trials of acustimulation (acupressure, acupuncture, auricular stimulation, or moxibustion) in nausea associated with pregnancy found some evidence of benefit, however, the authors urged caution given the heterogeneity of the studies and poor blinding.81
Figure 1.
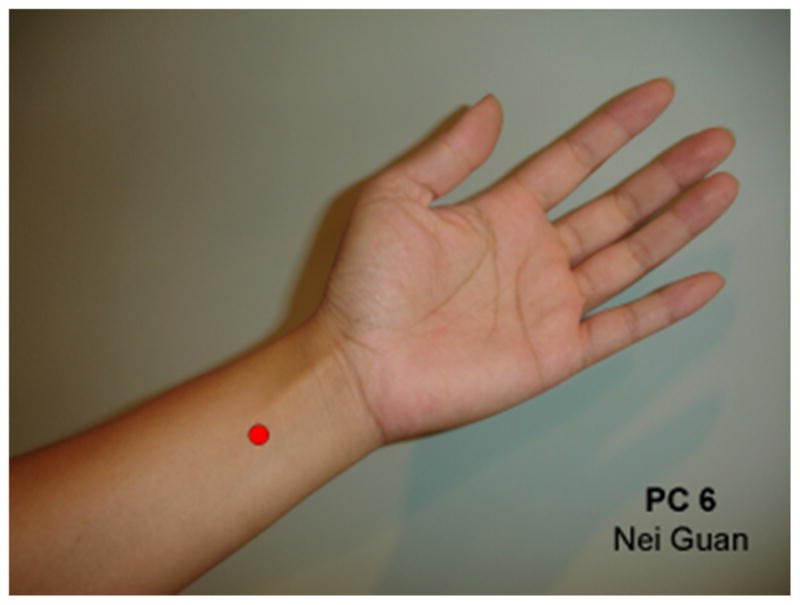
PC6 point.
From Acupressure Point P6: Pericardium 6 or Nei Guan. ExploreIM. UCLA Center for East-West Medicine. Available at: http://exploreim.ucla.edu/self-care/acupressure-point-p6/; with permission.
Summary
There is good evidence for ginger (1–2 g/day) in reducing nausea and vomiting and vitamin B6 (10–25 mg three times a day or 50 mg daily) in reducing nausea and vomiting associated with pregnancy. There is reasonable evidence to consider use of ginger or peppermint oil as aromatherapy or acupuncture.
Conclusion
A growing number of studies support the use of integrative medicine approaches for reducing nausea and vomiting, symptoms associated with GERD, IBD, and IBS, as well as steatosis associated with NALFD. The majority of these approaches have excellent safety profiles and are unlikely to interfere with pharmaceuticals, making them particularly attractive options. In some cases, data suggests that therapies may be broadly beneficial (e.g., probiotics in IBS), but there is yet insufficient information to recommend specific dosing or agents. Categories of integrative medicine approaches that appear to show the most promise in GI conditions include mind-body therapies, acupuncture, diet, probiotics, and specific dietary supplements and herbs.
KEY POINTS.
Patients with gastrointestinal conditions frequently use integrative medicine, and evidence of efficacy of specific therapies for certain conditions is growing
Promising results have been achieved with mind-body therapies, acupuncture, diet, and some dietary supplements including probiotics and specific herbs in distinct gastrointestinal conditions.
The most commonly studied conditions are gastroesophageal reflux disease, inflammatory bowel disease, irritable bowel syndrome, non-alcoholic fatty liver disease, and nausea and vomiting.
Footnotes
DISCLOSURE: Dr. Dossett was supported by K23 AT009218 from the National Center for Complementary and Integrative Health (NCCIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard University and its affiliated academic health care centers or the National Institutes of Health.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Peery AF, Crockett SD, Barritt AS, et al. Burden of Gastrointestinal, Liver, and Pancreatic Diseases in the United States. Gastroenterology. 2015;149(7):1731–1741e3. doi: 10.1053/j.gastro.2015.08.045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dossett ML, Davis RB, Lembo AJ, et al. Complementary and alternative medicine use by US adults with gastrointestinal conditions: Results from the 2012 National Health Interview Survey. Am J Gastroenterol. 2014;109(11):1705–11. doi: 10.1038/ajg.2014.108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Konturek PC, Brzozowski T, Konturek SJ. Stress and the gut: pathophysiology, clinical consequences, diagnostic approach and treatment options. J Physiol Pharmacol Off J Pol Physiol Soc. 2011;62(6):591–9. [PubMed] [Google Scholar]
- 4.Cohen E, Bolus R, Khanna D, et al. GERD symptoms in the general population: prevalence and severity versus care-seeking patients. Dig Dis Sci. 2014;59(10):2488–96. doi: 10.1007/s10620-014-3181-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Agreus L, Svardsudd K, Talley NJ, et al. Natural history of gastroesophageal reflux disease and functional abdominal disorders: a population-based study. Am J Gastroenterol. 2001;96(10):2905–14. doi: 10.1111/j.1572-0241.2001.04680.x. [DOI] [PubMed] [Google Scholar]
- 6.Tack J, Becher A, Mulligan C, et al. Systematic review: the burden of disruptive gastro-oesophageal reflux disease on health-related quality of life. Aliment Pharmacol Ther. 2012;35(11):1257–66. doi: 10.1111/j.1365-2036.2012.05086.x. [DOI] [PubMed] [Google Scholar]
- 7.Rubenstein JH, Chen JW. Epidemiology of gastroesophageal reflux disease. Gastroenterol Clin North Am. 2014;43(1):1–14. doi: 10.1016/j.gtc.2013.11.006. [DOI] [PubMed] [Google Scholar]
- 8.Maradey-Romero C, Kale H, Fass R. Nonmedical therapeutic strategies for nonerosive reflux disease. J Clin Gastroenterol. 2014;48(7):584–9. doi: 10.1097/MCG.0000000000000125. [DOI] [PubMed] [Google Scholar]
- 9.Zhang C, Qin Y, Guo B. Clinical study on the treatment of gastroesophageal reflux by acupuncture. Chin J Integr Med. 2010;16(4):298–303. doi: 10.1007/s11655-010-0516-y. [DOI] [PubMed] [Google Scholar]
- 10.Patrick L. Gastroesophageal reflux disease (GERD): a review of conventional and alternative treatments. Altern Med Rev J Clin Ther. 2011;16(2):116–33. [PubMed] [Google Scholar]
- 11.Ford AC, Moayyedi P. Dyspepsia. Curr Opin Gastroenterol. 2013;29(6):662–8. doi: 10.1097/MOG.0b013e328365d45d. [DOI] [PubMed] [Google Scholar]
- 12.Eherer AJ, Netolitzky F, Hogenauer C, et al. Positive effect of abdominal breathing exercise on gastroesophageal reflux disease: a randomized, controlled study. Am J Gastroenterol. 2012;107(3):372–8. doi: 10.1038/ajg.2011.420. [DOI] [PubMed] [Google Scholar]
- 13.Jarosz M, Taraszewska A. Risk factors for gastroesophageal reflux disease: the role of diet. Przeglaąd Gastroenterol. 2014;9(5):297–301. doi: 10.5114/pg.2014.46166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Langhorst J, Wulfert H, Lauche R, et al. Systematic review of complementary and alternative medicine treatments in inflammatory bowel diseases. J Crohns Colitis. 2015;9(1):86–106. doi: 10.1093/ecco-jcc/jju007. [DOI] [PubMed] [Google Scholar]
- 15.Joos S. Review on efficacy and health services research studies of complementary and alternative medicine in inflammatory bowel disease. Chin J Integr Med. 2011;17(6):403–9. doi: 10.1007/s11655-011-0758-3. [DOI] [PubMed] [Google Scholar]
- 16.Triantafyllidi A, Xanthos T, Papalois A, et al. Herbal and plant therapy in patients with inflammatory bowel disease. Ann Gastroenterol Q Publ Hell Soc Gastroenterol. 2015;28(2):210–20. [PMC free article] [PubMed] [Google Scholar]
- 17.Thunder God Vine. NCCIH; [Accessed on August 16, 2016]. Available at: https://nccih.nih.gov/health/tgvine. [Google Scholar]
- 18.Cammarota G, Ianiro G, Cianci R, et al. The involvement of gut microbiota in inflammatory bowel disease pathogenesis: potential for therapy. Pharmacol Ther. 2015;149:191–212. doi: 10.1016/j.pharmthera.2014.12.006. [DOI] [PubMed] [Google Scholar]
- 19.De Ley M, de Vos R, Hommes DW, et al. Fish oil for induction of remission in ulcerative colitis. Cochrane Database Syst Rev. 2007;(4):CD005986. doi: 10.1002/14651858.CD005986.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lev-Tzion R, Griffiths AM, Leder O, et al. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev. 2014;(2):CD006320. doi: 10.1002/14651858.CD006320.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kuo B, Bhasin M, Jacquart J, et al. Genomic and clinical effects associated with a relaxation response mind-body intervention in patients with irritable bowel syndrome and inflammatory bowel disease. PloS One. 2015;10(4):e0123861. doi: 10.1371/journal.pone.0123861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hou JK, Lee D, Lewis J. Diet and inflammatory bowel disease: review of patient-targeted recommendations. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2014;12(10):1592–600. doi: 10.1016/j.cgh.2013.09.063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Holt DQ, Strauss BJ, Moore GT. Patients with inflammatory bowel disease and their treating clinicians have different views regarding diet. J Hum Nutr Diet Off J Br Diet Assoc. 2016 doi: 10.1111/jhn.12400. [DOI] [PubMed] [Google Scholar]
- 24.Wędrychowicz A, Zając A, Tomasik P. Advances in nutritional therapy in inflammatory bowel diseases: Review. World J Gastroenterol. 2016;22(3):1045–66. doi: 10.3748/wjg.v22.i3.1045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Shah ND, Parian AM, Mullin GE, et al. Oral Diets and Nutrition Support for Inflammatory Bowel Disease: What Is the Evidence? Nutr Clin Pract Off Publ Am Soc Parenter Enter Nutr. 2015;30(4):462–73. doi: 10.1177/0884533615591059. [DOI] [PubMed] [Google Scholar]
- 26.Lee D, Albenberg L, Compher C, et al. Diet in the pathogenesis and treatment of inflammatory bowel diseases. Gastroenterology. 2015;148(6):1087–106. doi: 10.1053/j.gastro.2015.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Mearin F, Lacy BE, Chang L, et al. Bowel Disorders. Gastroenterology. 2016 doi: 10.1053/j.gastro.2016.02.031. [DOI] [PubMed] [Google Scholar]
- 28.Wilson S, Roberts L, Roalfe A, et al. Prevalence of irritable bowel syndrome: a community survey. Br J Gen Pract J R Coll Gen Pract. 2004;54(504):495–502. [PMC free article] [PubMed] [Google Scholar]
- 29.Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a metaanalysis. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2012;10(7):712–721e4. doi: 10.1016/j.cgh.2012.02.029. [DOI] [PubMed] [Google Scholar]
- 30.Deiteren A, de Wit A, van der Linden L, et al. Irritable bowel syndrome and visceral hypersensitivity : risk factors and pathophysiological mechanisms. Acta Gastro-Enterol Belg. 2016;79(1):29–38. [PubMed] [Google Scholar]
- 31.Everhart JE, Renault PF. Irritable bowel syndrome in office-based practice in the United States. Gastroenterology. 1991;100(4):998–1005. doi: 10.1016/0016-5085(91)90275-p. [DOI] [PubMed] [Google Scholar]
- 32.Ford AC, Bercik P, Morgan DG, et al. Validation of the Rome III criteria for the diagnosis of irritable bowel syndrome in secondary care. Gastroenterology. 2013;145(6):1262–1270e1. doi: 10.1053/j.gastro.2013.08.048. [DOI] [PubMed] [Google Scholar]
- 33.Schmulson MW, Chang L. Diagnostic approach to the patient with irritable bowel syndrome. Am J Med. 1999;107(5A):20S–26S. doi: 10.1016/s0002-9343(99)00278-8. [DOI] [PubMed] [Google Scholar]
- 34.Stukus DR, Mikhail I. Pearls and Pitfalls in Diagnosing IgE-Mediated Food Allergy. Curr Allergy Asthma Rep. 2016;16(5):34. doi: 10.1007/s11882-016-0611-z. [DOI] [PubMed] [Google Scholar]
- 35.Schumann D, Anheyer D, Lauche R, et al. Effect of Yoga in the Therapy of Irritable Bowel Syndrome: A Systematic Review. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2016 doi: 10.1016/j.cgh.2016.04.026. [DOI] [PubMed] [Google Scholar]
- 36.Lee HH, Choi YY, Choi M-G. The Efficacy of Hypnotherapy in the Treatment of Irritable Bowel Syndrome: A Systematic Review and Meta-analysis. J Neurogastroenterol Motil. 2014;20(2):152–62. doi: 10.5056/jnm.2014.20.2.152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ford AC, Quigley EMM, Lacy BE, et al. Effect of antidepressants and psychological therapies, including hypnotherapy, in irritable bowel syndrome: systematic review and meta-analysis. Am J Gastroenterol. 2014;109(9):1350–1365. doi: 10.1038/ajg.2014.148. quiz 1366. [DOI] [PubMed] [Google Scholar]
- 38.Aucoin M, Lalonde-Parsi M-J, Cooley K. Mindfulness-based therapies in the treatment of functional gastrointestinal disorders: a meta-analysis. Evid-Based Complement Altern Med ECAM. 2014;2014:140724. doi: 10.1155/2014/140724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Lakhan SE, Schofield KL. Mindfulness-based therapies in the treatment of somatization disorders: a systematic review and meta-analysis. PloS One. 2013;8(8):e71834. doi: 10.1371/journal.pone.0071834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006;130(5):1480–91. doi: 10.1053/j.gastro.2005.11.061. [DOI] [PubMed] [Google Scholar]
- 41.Biesiekierski JR, Newnham ED, Irving PM, et al. Gluten causes gastrointestinal symptoms in subjects without celiac disease: a double-blind randomized placebo-controlled trial. Am J Gastroenterol. 2011;106(3):508–514. doi: 10.1038/ajg.2010.487. quiz 515. [DOI] [PubMed] [Google Scholar]
- 42.Vazquez-Roque MI, Camilleri M, Smyrk T, et al. A controlled trial of gluten-free diet in patients with irritable bowel syndrome-diarrhea: effects on bowel frequency and intestinal function. Gastroenterology. 2013;144(5):903–911e3. doi: 10.1053/j.gastro.2013.01.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Marsh A, Eslick EM, Eslick GD. Does a diet low in FODMAPs reduce symptoms associated with functional gastrointestinal disorders? A comprehensive systematic review and meta-analysis. Eur J Nutr. 2016;55(3):897–906. doi: 10.1007/s00394-015-0922-1. [DOI] [PubMed] [Google Scholar]
- 44.Nanayakkara WS, Skidmore PM, O’Brien L, et al. Efficacy of the low FODMAP diet for treating irritable bowel syndrome: the evidence to date. Clin Exp Gastroenterol. 2016;9:131–42. doi: 10.2147/CEG.S86798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Moayyedi P, Quigley EMM, Lacy BE, et al. The effect of fiber supplementation on irritable bowel syndrome: a systematic review and meta-analysis. Am J Gastroenterol. 2014;109(9):1367–74. doi: 10.1038/ajg.2014.195. [DOI] [PubMed] [Google Scholar]
- 46.Michelfelder AJ, Lee KC, Bading EM. Integrative medicine and gastrointestinal disease. Prim Care. 2010;37(2):255–67. doi: 10.1016/j.pop.2010.02.003. [DOI] [PubMed] [Google Scholar]
- 47.Mudgil D, Barak S. Composition, properties and health benefits of indigestible carbohydrate polymers as dietary fiber: a review. Int J Biol Macromol. 2013;61:1–6. doi: 10.1016/j.ijbiomac.2013.06.044. [DOI] [PubMed] [Google Scholar]
- 48.Ruepert L, Quartero AO, de Wit NJ, et al. Bulking agents, antispasmodics and antidepressants for the treatment of irritable bowel syndrome. Cochrane Database Syst Rev. 2011;(8):CD003460. doi: 10.1002/14651858.CD003460.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lever E, Cole J, Scott SM, et al. Systematic review: the effect of prunes on gastrointestinal function. Aliment Pharmacol Ther. 2014;40(7):750–8. doi: 10.1111/apt.12913. [DOI] [PubMed] [Google Scholar]
- 50.Moayyedi P, Ford AC, Talley NJ, et al. The efficacy of probiotics in the treatment of irritable bowel syndrome: a systematic review. Gut. 2010;59(3):325–32. doi: 10.1136/gut.2008.167270. [DOI] [PubMed] [Google Scholar]
- 51.Didari T, Mozaffari S, Nikfar S, et al. Effectiveness of probiotics in irritable bowel syndrome: Updated systematic review with meta-analysis. World J Gastroenterol. 2015;21(10):3072–84. doi: 10.3748/wjg.v21.i10.3072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Boyle RJ, Robins-Browne RM, Tang MLK. Probiotic use in clinical practice: what are the risks? Am J Clin Nutr. 2006;83(6):1256-1264-1447. doi: 10.1093/ajcn/83.6.1256. [DOI] [PubMed] [Google Scholar]
- 53.Kligler B, Chaudhary S. Peppermint oil. Am Fam Physician. 2007;75(7):1027–30. [PubMed] [Google Scholar]
- 54.Ford AC, Talley NJ, Spiegel BMR, et al. Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: systematic review and meta-analysis. BMJ. 2008;337:a2313. doi: 10.1136/bmj.a2313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Khanna R, MacDonald JK, Levesque BG. Peppermint oil for the treatment of irritable bowel syndrome: a systematic review and meta-analysis. J Clin Gastroenterol. 2014;48(6):505–12. doi: 10.1097/MCG.0b013e3182a88357. [DOI] [PubMed] [Google Scholar]
- 56.Manheimer E, Cheng K, Wieland LS, et al. Acupuncture for treatment of irritable bowel syndrome. Cochrane Database Syst Rev. 2012;(5):CD005111. doi: 10.1002/14651858.CD005111.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Wu J, Hu Y, Zhu Y, et al. Systematic Review of Adverse Effects: A Further Step towards Modernization of Acupuncture in China. Evid-Based Complement Altern Med ECAM. 2015;2015:432467. doi: 10.1155/2015/432467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Liu ZL, Xie LZ, Zhu J, et al. Herbal medicines for fatty liver diseases. Cochrane Database Syst Rev. 2013;(8):CD009059. doi: 10.1002/14651858.CD009059.pub2. [DOI] [PubMed] [Google Scholar]
- 59.Shi K-Q, Fan Y-C, Liu W-Y, et al. Traditional Chinese medicines benefit to nonalcoholic fatty liver disease: a systematic review and meta-analysis. Mol Biol Rep. 2012;39(10):9715–22. doi: 10.1007/s11033-012-1836-0. [DOI] [PubMed] [Google Scholar]
- 60.Milosević N, Milanović M, Abenavoli L, et al. Phytotherapy and NAFLD--from goals and challenges to clinical practice. Rev Recent Clin Trials. 2014;9(3):195–203. [PubMed] [Google Scholar]
- 61.Yang Z, Zhuang L, Lu Y, et al. Effects and tolerance of silymarin (milk thistle) in chronic hepatitis C virus infection patients: a meta-analysis of randomized controlled trials. BioMed Res Int. 2014;2014:941085. doi: 10.1155/2014/941085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Ji H-F, Sun Y, Shen L. Effect of vitamin E supplementation on aminotransferase levels in patients with NAFLD, NASH, and CHC: results from a meta-analysis. Nutr Burbank Los Angel Cty Calif. 2014;30(9):986–91. doi: 10.1016/j.nut.2014.01.016. [DOI] [PubMed] [Google Scholar]
- 63.Minemura M, Shimizu Y. Gut microbiota and liver diseases. World J Gastroenterol. 2015;21(6):1691–702. doi: 10.3748/wjg.v21.i6.1691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Ma Y-Y, Li L, Yu C-H, et al. Effects of probiotics on nonalcoholic fatty liver disease: a meta-analysis. World J Gastroenterol. 2013;19(40):6911–8. doi: 10.3748/wjg.v19.i40.6911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Paolella G, Mandato C, Pierri L, et al. Gut-liver axis and probiotics: their role in non-alcoholic fatty liver disease. World J Gastroenterol. 2014;20(42):15518–31. doi: 10.3748/wjg.v20.i42.15518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Abdel-Aziz H, Windeck T, Ploch M, et al. Mode of action of gingerols and shogaols on 5-HT3 receptors: binding studies, cation uptake by the receptor channel and contraction of isolated guinea-pig ileum. Eur J Pharmacol. 2006;530(1–2):136–43. doi: 10.1016/j.ejphar.2005.10.049. [DOI] [PubMed] [Google Scholar]
- 67.Marx W, Kiss N, Isenring L. Is ginger beneficial for nausea and vomiting? An update of the literature. Curr Opin Support Palliat Care. 2015;9(2):189–95. doi: 10.1097/SPC.0000000000000135. [DOI] [PubMed] [Google Scholar]
- 68.Viljoen E, Visser J, Koen N, et al. A systematic review and meta-analysis of the effect and safety of ginger in the treatment of pregnancy-associated nausea and vomiting. Nutr J. 2014;13:20. doi: 10.1186/1475-2891-13-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Thomson M, Corbin R, Leung L. Effects of ginger for nausea and vomiting in early pregnancy: a meta-analysis. J Am Board Fam Med JABFM. 2014;27(1):115–22. doi: 10.3122/jabfm.2014.01.130167. [DOI] [PubMed] [Google Scholar]
- 70.Dabaghzadeh F, Khalili H, Dashti-Khavidaki S, et al. Ginger for prevention of antiretroviral-induced nausea and vomiting: a randomized clinical trial. Expert Opin Drug Saf. 2014;13(7):859–66. doi: 10.1517/14740338.2014.914170. [DOI] [PubMed] [Google Scholar]
- 71.Lee J, Oh H. Ginger as an antiemetic modality for chemotherapy-induced nausea and vomiting: a systematic review and meta-analysis. Oncol Nurs Forum. 2013;40(2):163–70. doi: 10.1188/13.ONF.163-170. [DOI] [PubMed] [Google Scholar]
- 72.Ensiyeh J, Sakineh M. Comparing ginger and vitamin B6 for the treatment of nausea and vomiting in pregnancy: a randomised controlled trial. Midwifery. 2009 doi: 10.1016/j.midw.2007.10.013. [DOI] [PubMed] [Google Scholar]
- 73.Sripramote M, Lekhyananda N. A randomized comparison of ginger and vitamin B6 in the treatment of nausea and vomiting of pregnancy. J Med Assoc Thail Chotmaihet Thangphaet. 2003;86(9):846–53. [PubMed] [Google Scholar]
- 74.Matthews A, Haas DM, O’Mathuna DP, et al. Interventions for nausea and vomiting in early pregnancy. Cochrane Database Syst Rev. 2015;(9):CD007575. doi: 10.1002/14651858.CD007575.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kulkantrakorn K. Pyridoxine-induced sensory ataxic neuronopathy and neuropathy: revisited. Neurol Sci Off J Ital Neurol Soc Ital Soc Clin Neurophysiol. 2014;35(11):1827–30. doi: 10.1007/s10072-014-1902-6. [DOI] [PubMed] [Google Scholar]
- 76.Lua P, Zakaria N. A brief review of current scientific evidence involving aromatherapy use for nausea and vomiting. J Altern. 2012 doi: 10.1089/acm.2010.0862. [DOI] [PubMed] [Google Scholar]
- 77.Hines S, Steels E, Chang A, et al. Aromatherapy for treatment of postoperative nausea and vomiting. Cochrane Libr. 2012 doi: 10.1002/14651858.CD007598.pub2. [DOI] [PubMed] [Google Scholar]
- 78.Hunt R, Dienemann J, Norton HJ, et al. Aromatherapy as treatment for postoperative nausea: a randomized trial. Anesth Analg. 2013;117(3):597–604. doi: 10.1213/ANE.0b013e31824a0b1c. [DOI] [PubMed] [Google Scholar]
- 79.Cheong KB, Zhang J, Huang Y, et al. The effectiveness of acupuncture in prevention and treatment of postoperative nausea and vomiting--a systematic review and meta-analysis. PloS One. 2013;8(12):e82474. doi: 10.1371/journal.pone.0082474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Lee A, Chan SKC, Fan LTY. Stimulation of the wrist acupuncture point PC6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2015;(11):CD003281. doi: 10.1002/14651858.CD003281.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Van den Heuvel E, Goossens M, Vanderhaegen H, et al. Effect of acustimulation on nausea and vomiting and on hyperemesis in pregnancy: a systematic review of Western and Chinese literature. BMC Complement Altern Med. 2016;16:13. doi: 10.1186/s12906-016-0985-4. [DOI] [PMC free article] [PubMed] [Google Scholar]