

Abstract
Background:
Marginal leakage is the important factor influencing the maintenance of dental esthetic.
Aim:
The purpose of this study was to evaluate the relationship between the preparation techniques and type of polymerization techniques on microleakage of composite laminate veneers.
Materials and Methods:
Ninety-one same sized, caries-free human maxillary central incisors were randomly assigned to 13 groups (n = 7) and were designed with four different preparation techniques (window type, feather type, bevel type, and incisal overlap type). One group determined as control group and any preparation was applied. Nanohybrid resin composite was used for restoration. Composite laminate veneers polymerized with three different techniques (direct light curing, indirect polymerization with a combination of pressure, light and heat using a light cup and heat cup, direct polymerization, and additionally heat cured in an oven). The specimens were thermocycled, and then immersed in 5% basic fuchsine solution. Following 24 h, all specimens were immersed in 65% nitric acid solutions for volumetric dye extraction test. Samples diluted with distilled water and centrifuged and microleakage determined by a spectrophotometer.
Statistical Analysis Used:
Data were analyzed with two-way ANOVA and Tukey honest significant difference post hoc multiple comparisons test (P < 0.05).
Results:
For comparing the microleakage value of preparation and polymerization techniques, Window type preparation showed a significant difference in direct polymerization + additional cured group (P < 0.05). Control group was statistically different from the other groups (P < 0.05).
Conclusions:
Window type laminate preparation can be preferred in indirect polymerization technique because it caused less leakage in this present study.
Keywords: Composite laminate veneer, direct polymerization, indirect polymerization, microleakage
Introduction
Lost dental esthetic due to shape, color, position, and structural abnormalities is the crucial problem for patients.[1] The developments of adhesive techniques have increased the use of conservative restoration options for restore the esthetic appearance of the dentition. Composite laminate veneer is preferred because it provides less invasive and more conservative treatment for correction unaesthetic tooth forms, to mask tooth discolorations, and to restore fractured anterior teeth.[2,3,4] However, marginal discoloration, microleakage, wear, and marginal fractures are common problem of composite restorations, and this situation causes reducing the esthetic result over time.[5,6]
One of the widely used techniques for restoring of teeth in clinic is direct preparation. No or minimal tooth preparation, better marginal adaptation, easy intraoral polishing, inexpensive, and no need for an additional adhesive cementing system, easy to repair are some advantages of direct laminate veneers. However, low resistance to fractures and wear, and discoloration are the main disadvantages of this technique.[1,7] The use of indirect polymerization technique is a possible method of minimizing of this disadvantages.[8] Indirect laminate veneers have high resistance against fractures and discoloration compared to direct laminate veneer restoration. Main disadvantages of indirect laminate veneer restorations are higher cost, long chair time, and the necessity of using an adhesive cementing system.[9]
Microleakage is the major problem in clinical dentistry and may predispose a tooth the discoloration, postoperative sensitivity, recurrent caries, and pulpal inflammation.[10] Poor adaptation between the tooth structure and the restorative material is the main cause of microleakage. Volume changes occurring by the oral thermal factors will cause a gap formation and microleakage.[11] Different test methods available to detect microleakage include direct visual examination, and microscopic examination, scanning electron microscopic examination, neutron activation analysis, using air pressure, an electrochemical methodology, and measuring bacteria penetration.[12] However, dye penetration technique is widely preferred method due to easy manipulation, easy analysis of the results and no need for expensive instrumentation.[11]
The purpose of this in vitro study was to evaluate the influence of different polymerization techniques and different laminate preparations techniques on the microleakage of composite laminate veneers. The volumetric microleakage evaluation method used in this study is important because it gives quantitative results.
Materials and Methods
Ninety-one human maxillary central incisors with no caries, cracks or excessive wear extracted for protethic rehabilitation or due to periodontal problems were selected for the study. Tissue and calculus deposits were removed from teeth and teeth stored in a 0.1% chloramine solution. The teeth were divided into four main groups according to preparations techniques [Figure 1]. Group 1: Window type, Group 2: Feather type, Group 3: Bevel type, and Group 4: Incisal overlap type.[10]
Figure 1.
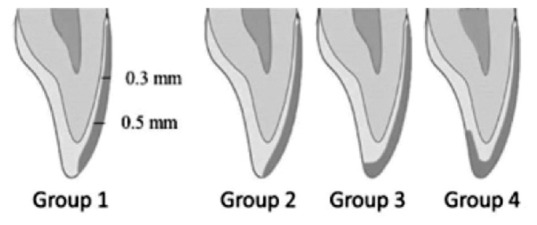
Schematic illustration showing the different preparation techniques in groups. Group 1: Window type, Group 2: Feather type, Group 3: Bevel type, and Group 4: Incisal overlap type
The teeth were prepared with special laminate veneer preparation bur set (Laminate Veneer Set, Axis, Kerr, Teksas, USA). Diamond depth cut burs (M834-016, M834-021, Axis, Teksas, USA) were used to scribe horizontal depth cut grooves on the labial surface for minimal preparations of approximately 0.3 mm in the cervical third and 0.5 mm in the middle and incisal third. All of the grooves were connected with a diamond rotary cutting instrument (H284K-016). The surface was prepared with retouch bur. SF134-014 was used in middle third, SF132-008 and SF379-023 were used in cervical and incisal third.
In the Group 1, 1 mm intact enamel was left in four edges of teeth, and incisal edge was protected.
In the Group 2, the preparation was terminated in incisal edge without shortening incisal edge.
In the Group 3, incisal edge was reduced 1.5 mm, and bucco-palatal bevel was prepared across the full width of the preparation.
In the Group 4, the incisal edge was reduced 2 mm and then the laminate preparation extended onto the palatal aspect of the preparation.
Seven teeth without any treatment were determined as control group.
Materials used in the study are shown in Table 1. Nanohybrid resin composite was used for the preparation of laminates (Clearfil Majesty Esthetic, Kuraray, Okayama, Japan). A1 shade was chosen for standardization. Each of the four main groups was divided into three additional subgroups according to polymerization technique. Devices used for polymerization are shown in Table 2. Subgroup A: Composite laminates were polymerized using direct light curing units. Subgroup B: Composite laminates were polymerized using indirect light + heat + pressure curing units. Subgroup C: Composite laminates were polymerized using direct light curing unit and were placed in an oven for additional polymerization.
Table 1.
Materials, manufacturers, chemical compositions used in this study
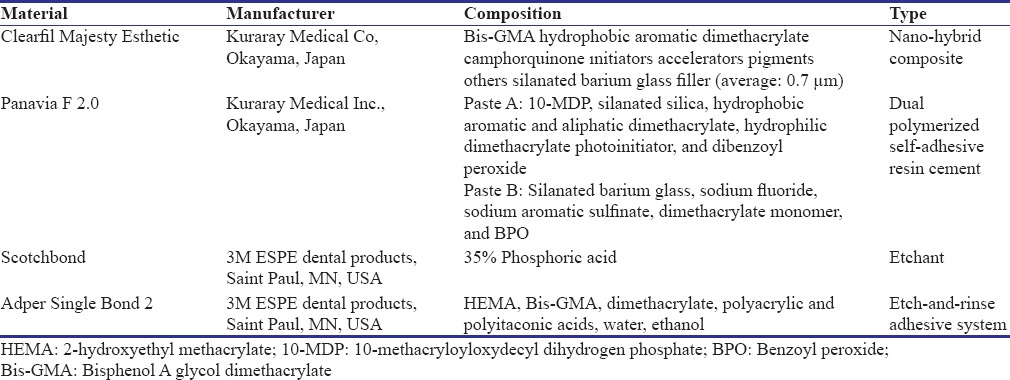
Table 2.
Devices used for polymerization in this study
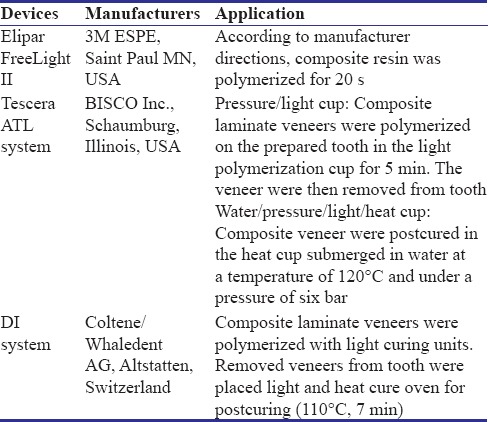
In Subgroup A, after using two-step etch-and-rinse adhesive system (Adper Single Bond 2, 3M ESPE, St. Paul, MN, USA), resin composite was polymerized with light curing units (Elipar FreeLight II, 3M ESPE). The output of the curing light was checked with a radiometer (Hilux UltraPlus Curing Units; Benlioglu Dental, Istanbul, Turkey).
In Subgroup B, resin composite was polymerized with light and heat in a special devices.(Tescera ATL, Bisco, Schaumburg, USA). After polymerization, composite laminates were cemented with resin cement (Panavia F 2.0, Kuraray, New York, USA) according to manufacturer instructions.
In Subgroup C, after composite laminates were polymerized with light curing units (Elipar FreeLight II, 3M ESPE, St. Paul MN, USA), they were exposed additional curing in an oven (Coltene DI 500, Whaledent, Altstatten, Switzerland). After polymerization, composite laminate was cemented with resin cement (Panavia F 2.0, Kuraray, New York, USA) according to manufacturer instructions.
The composite veneers were finished and polished using polishing disks (Sof-Lex, 3M ESPE, St. Paul, MN, USA) of different grain sizes (medium, fine, and extra-fine). After storage for 24 h in distilled water, all specimens were thermocycled by immersion in two water tanks (cold, warm) with temperatures of 5°C and 55°C. The tooth surface was coated with nail varnish to within 1 mm of the laminate veneer margins, then immersed in 5% basic fuchsine solution for 24 h. After that, the samples were rinsed under tap water, and nail varnish was removed by polishing disks. Dye extraction method was used for microleakage evaluation. 1 ml % 65 nitric acid solution was added in experimental tubes. Following that all specimens were immersed in experimental tubes for 3 days to let basic fuchsine within laminates dentin interface diluted in nitric acid. The tubes were centrifuged 14,000 rpm for 5 min, and after that, 100 μL of the supernatant from each was transferred to a plate. The dye absorption was determined by an automatic spectrophotometer at 600 nm wavelength. The results of the spectrophotometer indicate the light absorption of the basic fuchsine in the laminate-tooth interface which is actually showing the microleakage of the restoration.
Data were analyzed by ANOVA and Tukey honest significant difference test. All tests were run at 5% significance level (P < 0.05).
Results
The mean and standard deviation of microleakage value for groups are shown in Table 3. Statistically significant differences between the preparation and polymerization techniques are indicated in the same table. According to microleakage value evaluation for polymerization techniques, there was a significant difference between Group 1A and Group 1C (P = 0.033). Control group was statistically different from the other groups in pairwise comparisons for preparation techniques (P < 0.05). For comparing the microleakage value of preparation and polymerization techniques, as shown in Figure 2, Group 2B and Group 4B indicated more leakage according to dye extraction method. Window type preparation was showed significant difference microleakage value in Subgroup C (P < 0.05). Incisal overlap preparation showed the least leakage in direct polymerization technique, while window type showed lower leakage in indirect polymerization technique.
Table 3.
The means and standard deviations of microleakage level of different groups
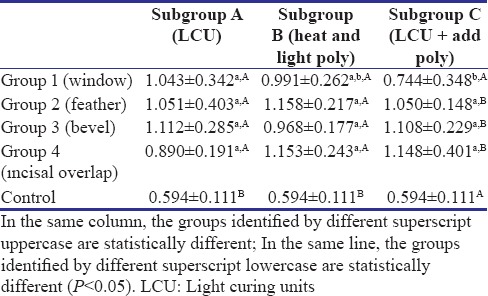
Figure 2.
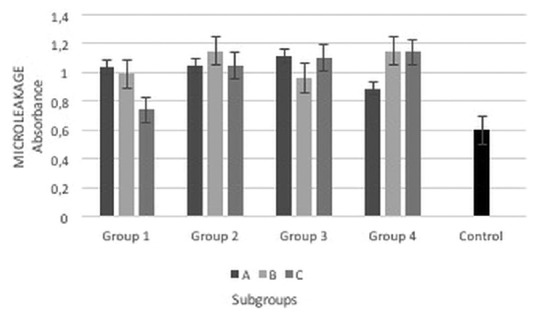
The comparisons of average microleakage in groups by dye extraction method
Discussion
Nowadays, patients demand not only healthy functional dentition but also an esthetic smile. Composite laminate veneers have gained considerable importance to provide increasing esthetic demand and offer a treatment option for a patient with minimal preparation. Prevention of microleakage is very important factor for the longevity of restoration. Obtained data from this study showed that preparation techniques and polymerization techniques demonstrated different effect on microleakage of composite laminate veneers.
Non-effective seal at restoration margins may cause to marginal staining, postoperative sensitivity, and recurrent caries as a result of bacterial penetration.[13] Marginal integrity is the most important criteria for evaluating a restoration's success.[14] Different test methods have been used for years to understand fluid flow and marginal integrity of composites cohesive and adhesive natures in vitro. In general, dye penetration has been considered as the most frequently used method. However, subjectivity of readings is the limitations of these test methods.[13,15] In this present study, dye extraction method was used, and the volume of penetrated dye was measured as a quantitative using a spectrophotometer.
Polymerization shrinkage, nonretentive tooth preparation, weak cement, malocclusion, excessive forces of mastication affect the microleakage.[16] Indirect restorations are expected to show better marginal integrity. Poor marginal integrity can appear due to polymerization shrinkage or removal of the luting cement. In indirect restorations, the composite resin is polymerized before placement for prevention of polymerization shrinkage.[14] However, the type of luting agent and its mechanical properties have a significant effect on microleakage.[17,18] The thickness of resin luting agent is the another risk factor. Thicker luting agent may occur crack and leakage as a result of a poorly fitting veneer.[19] In this present study, comparing the results of dye extraction, indirect polymerization technique was showed significant difference only in Group 1. In the other groups, indirect and direct techniques showed same values. It may be explained by properties of luting agent. Aschenbrenner et al.[20] detected small marginal cement deterioration with microscopic analysis after removal of excess cement with a hand instrument. This situation may cause dye entry to gap formation. Gerdolle et al.[8] reported in their study that due to the difference in thermal expansion between luting agent and tooth, the thermal cycling of a restoration between high and low temperatures may cause deterioration of the bond between the luting agent and tooth.
Tooth preparation is known as one of the most critical steps in the use of laminate veneers. In the literature, widely accepted designs are the window preparation, feather preparation, bevel preparation, and the incisal overlap preparation.[21,22] Pini et al.,[23] reported that the preparation design should allow an optimum marginal adaptation of the final laminate veneer restoration. The incisal preparation design is the controversial subject in the literature.[24] Some authors recommend an incisal overlap preparation as the standard procedure for laminate veneers,[25] while others do not.[26] Window preparation design protect natural enamel over the incisal edge. However, incisal finish line can be difficult to hide.
Preparation depth is desirable to remain within enamel. Dentin tends to expose in the cervical and proximal area because the enamel is thinnest in this areas.[22] In bonded restorations, the enamel margins are less susceptible to leakage than dentinal margins, because of resin-based restorative materials bond well with acid-etched enamel.[27,28] In recent studies reported that laminate preparation where located in aprismatic enamel or dentin cause mikroleakage at the cervical margin and the microleakage at cervical margin was greater than at the incisal margin.[22,26] 0.5 mm tissue reduction in cervical region is associated with dentinal exposure and this situation may increase the risk of lost marginal seal.[26,29] Therefore, in this study all margins of laminate preparation were placed in enamel. Depth cut burs were used for prevention of over preparation, and all preparation finish line were located 1.0 mm close the gingival margin. Hekimoglu et al.[26] reported in their study, and the window preparation type was more effective in terms of prevention of microleakage than the overlapped type laminates. In another study concluded that the incisal overlap design showed more microleakage when compared with the window preparation. This can be attributed to the shrinkage of materials and leading to marginal gap formation at the linguoincisal edge.[30] In this present study, window type preparation was showed lower microleakage value in Subgroup C.
Concerning the limitations of this study, the cemented composite laminate veneers were not exposed to mechanical cycling, and all groups exposed only thermocycling in the laboratory. As this might not replicate the actual situations present in routine clinical practice, further studies are recommended.
Conclusions
Based on the findings of this in vitro study, the following conclusions were drawn:
All preparation and polymerization techniques caused microleakage when compared with control groups (P < 0.05)
Incisal overlap preparation can be preferred in direct polymerization because it showed less leakage according to the other preparation techniques
In window type preparation, application light curing + additional polymerization showed lower microleakage than the other preparation technique
Indirect polymerization technique did not show differences according to direct polymerization technique in all groups except window type preparation (P > 0.05).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Korkut B, Yanıkoğlu F, Günday M. Direct composite laminate veneers: Three case reports. J Dent Res Dent Clin Dent Prospects. 2013;7:105–11. doi: 10.5681/joddd.2013.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bagis B, Aydoğan E, Bagis YH. Direct restorative treatment of missing maxillary laterals with composite laminate veneer: A case report. Open Dent J. 2008;2:93–5. doi: 10.2174/1874210600802010093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Begum Z, Chheda P, Shruthi CS, Sonika R. Effect of ceramic thickness and luting agent shade on the color masking ability of laminate veneers. J Indian Prosthodont Soc. 2014;14:46–50. doi: 10.1007/s13191-014-0362-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Turkaslan S, Tezvergil-Mutluay A, Bagis B, Shinya A, Vallittu PK, Lassila LV, et al. Effect of intermediate fiber layer on the fracture load and failure mode of maxillary incisors restored with laminate veneers. Dent Mater J. 2008;27:61–8. doi: 10.4012/dmj.27.61. [DOI] [PubMed] [Google Scholar]
- 5.Mahrous AI, Eltiti HA, Ahmed IM, Alagha EI. Effect of different gingival margin restorations of class II cavities on microleakage: An in-vitro study. Electron Physician. 2015;7:1435–40. doi: 10.19082/1435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gupta KV, Verma P, Trivedi A. Evaluation of microleakage of various restorative materials. J Life Sci. 2011;3:29–33. [Google Scholar]
- 7.Hemmings KW, Darbar UR, Vaughan S. Tooth wear treated with direct composite restorations at an increased vertical dimension: Results at 30 months. J Prosthet Dent. 2000;83:287–93. doi: 10.1016/s0022-3913(00)70130-2. [DOI] [PubMed] [Google Scholar]
- 8.Gerdolle DA, Mortier E, Loos-Ayav C, Jacquot B, Panighi MM. In vitro evaluation of microleakage of indirect composite inlays cemented with four luting agents. J Prosthet Dent. 2005;93:563–70. doi: 10.1016/j.prosdent.2005.04.004. [DOI] [PubMed] [Google Scholar]
- 9.Gresnigt MM, Kalk W, Ozcan M. Randomized controlled split-mouth clinical trial of direct laminate veneers with two micro-hybrid resin composites. J Dent. 2012;40:766–75. doi: 10.1016/j.jdent.2012.05.010. [DOI] [PubMed] [Google Scholar]
- 10.Priyalakshmi S, Manish R. A review on marginal deterioration of composite restoration. J Dent Med Sci. 2014;13:6–9. [Google Scholar]
- 11.Shih WY. Microleakage in different primary tooth restorations. J Chin Med Assoc. 2016;79:228–34. doi: 10.1016/j.jcma.2015.10.007. [DOI] [PubMed] [Google Scholar]
- 12.de Santi Alvarenga FA, Pinelli C, Monteiro Loffredo Lde C. Reliability of marginal microleakage assessment by visual and digital methods. Eur J Dent. 2015;9:1–5. doi: 10.4103/1305-7456.149628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gorucu J, Gurgan S, Cakir FY, Bicer CO, Gorucu H. The effect of different preparation and etching procedures on the microleakage of direct composite veneer restorations. Photomed Laser Surg. 2011;29:205–11. doi: 10.1089/pho.2009.2752. [DOI] [PubMed] [Google Scholar]
- 14.Dukic W, Dukic OL, Milardovic S, Delija B. Clinical evaluation of indirect composite restorations at baseline and 36 months after placement. Oper Dent. 2010;35:156–64. doi: 10.2341/09-133-C. [DOI] [PubMed] [Google Scholar]
- 15.Mirra AE, El-Mahalawy S. Fracture strength and microleakage of laminate veneer. Cairo Dent J. 2009;25:245–54. [Google Scholar]
- 16.Bhandari S, Aras M, Chitre V. An in vitro evaluation of the microleakage under complete metal crowns using three adhesive luting cements. J Indian Prosthodont Soc. 2012;12:65–71. doi: 10.1007/s13191-011-0109-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gu XH, Kern M. Marginal discrepancies and leakage of all-ceramic crowns: Influence of luting agents and aging conditions. Int J Prosthodont. 2003;16:109–16. [PubMed] [Google Scholar]
- 18.White SN, Ingles S, Kipnis V. Influence of marginal opening on microleakage of cemented artificial crowns. J Prosthet Dent. 1994;71:257–64. doi: 10.1016/0022-3913(94)90464-2. [DOI] [PubMed] [Google Scholar]
- 19.Magne P, Kwon KR, Belser UC, Hodges JS, Douglas WH. Crack propensity of porcelain laminate veneers: A simulated operatory evaluation. J Prosthet Dent. 1999;81:327–34. doi: 10.1016/s0022-3913(99)70277-5. [DOI] [PubMed] [Google Scholar]
- 20.Aschenbrenner CM, Lang R, Handel G, Behr M. Analysis of marginal adaptation and sealing to enamel and dentin of four self-adhesive resin cements. Clin Oral Investig. 2012;16:191–200. doi: 10.1007/s00784-010-0501-z. [DOI] [PubMed] [Google Scholar]
- 21.Li Z, Yang Z, Zuo L, Meng Y. A three-dimensional finite element study on anterior laminate veneers with different incisal preparations. J Prosthet Dent. 2014;112:325–33. doi: 10.1016/j.prosdent.2013.09.023. [DOI] [PubMed] [Google Scholar]
- 22.Walls AW, Steele JG, Wassell RW. Crowns and other extra-coronal restorations: Porcelain laminate veneers. Br Dent J. 2002;193:73–6. doi: 10.1038/sj.bdj.4801489. 79. [DOI] [PubMed] [Google Scholar]
- 23.Pini NP, Aguiar FH, Lima DA, Lovadino JR, Terada RS, Pascotto RC, et al. Advances in dental veneers: Materials, applications, and techniques. Clin Cosmet Investig Dent. 2012;4:9–16. doi: 10.2147/CCIDEN.S7837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Coachman C, Gurel G, Calamita M, Morimoto S, Paolucci B, Sesma N, et al. The influence of tooth color on preparation design for laminate veneers from a minimally invasive perspective: Case report. Int J Periodontics Restorative Dent. 2014;34:453–9. doi: 10.11607/prd.1900. [DOI] [PubMed] [Google Scholar]
- 25.Cötert HS, Dündar M, Oztürk B. The effect of various preparation designs on the survival of porcelain laminate veneers. J Adhes Dent. 2009;11:405–11. [PubMed] [Google Scholar]
- 26.Hekimoglu C, Anil N, Yalçin E. A microleakage study of ceramic laminate veneers by autoradiography: Effect of incisal edge preparation. J Oral Rehabil. 2004;31:265–9. doi: 10.1046/j.0305-182X.2003.01220.x. [DOI] [PubMed] [Google Scholar]
- 27.Erkut S, Caglar A, Yilmaz B, Küçükeşmen HC, Ozdemir E. Microleakage of different provisionalization techniques for class I inlays. J Dent Sci. 2013;8:1–7. [Google Scholar]
- 28.Wahab FK, Shaini FJ, Morgano SM. The effect of thermocycling on microleakage of several commercially available composite class V restorations in vitro. J Prosthet Dent. 2003;90:168–74. doi: 10.1016/s0022-3913(03)00300-7. [DOI] [PubMed] [Google Scholar]
- 29.Ferrari M, Patroni S, Balleri P. Measurement of enamel thickness in relation to reduction for etched laminate veneers. Int J Periodontics Restorative Dent. 1992;12:407–13. [PubMed] [Google Scholar]
- 30.Shetty A, Kaiwar A, Shubhashini N, Ashwini P, Naveen D, Adarsha M, et al. Survival rates of porcelain laminate restoration based on different incisal preparation designs: An analysis. J Conserv Dent. 2011;14:10–5. doi: 10.4103/0972-0707.80723. [DOI] [PMC free article] [PubMed] [Google Scholar]