

Abstract
Background/Aim
To estimate overweight and obesity prevalence trends in Slovenian adolescents entering secondary schools in the years 2004, 2009 and 2014 and differences in the prevalence between different types of secondary schools.
Methods
Data from 17,538 adolescents entering secondary schools (mean age ± standard deviation 15.4 ± 0.5 years) collected during obligatory medical examination in years 2004, 2009 and 2014 was analyzed. Overweight and obesity were defined using International Obesity Task Force criteria.
Results
In 2004-2009 overweight and obesity prevalence increased, especially in males and stabilized thereafter (2009-2014) in both genders. It was significantly higher (p < 0.0001) in those attending secondary vocational and technical/professional versus grammar schools (2009; 28.7 vs. 16.8% overweight females and 31.6 vs. 22.3% overweight males; 2014: 29.7 vs. 17.9% overweight females and 33.6 vs. 20.4% overweight males).
Conclusions
Overweight and obesity prevalence in Slovenian adolescents entering secondary schools stabilized recently. Adolescents attending secondary vocational and technical/professional schools are at an increased risk of overweight and obesity.
Key Words: Overweight, Obesity, Adolescent, Education, Slovenia
Introduction
Obese children and adolescents are prone to develop overweight or obesity in adulthood which is often associated with various obesity-related health complications [1,2]. Significant obesity-related metabolic and non-metabolic complications may however also present in adolescents and even children [1,3]. Obesity in children represents an important public healthcare problem that will become even more significant in the near future should we not turn the current trends in the prevalence of obesity and its complications [1,4].
Overweight and obesity prevalence was increasing in both developed and developing countries until recently, when it plateaued at an unacceptably high level [5,6,7]. Increase in prevalence was also reported in Slovenian children and adolescents [8,9,10]. Recently prevalence of overweight and obesity stabilized in Slovenian 5-year-old children in the period 2001-2009, and in 7-year-old children in the period 1991-2011 in the city of Ljubljana [11,12]. In the same time period prevalence of overweight and obesity however continued to increase in Slovenian adolescents [13].
The aim of this study was to estimate trends in the prevalence of overweight and obesity in Slovenian adolescents entering secondary schools in the years 2004, 2009, and 2014. In addition, differences in the prevalence of overweight and obesity according to the type of secondary schools adolescents were entering was investigated in the years 2009 and 2014.
Material and Methods
Subjects
All students entering secondary schools have an obligatory clinical examination. It is performed by a primary care pediatrician at a local healthcare facility. For the purpose of the study, anonymous data was obtained from primary care pediatricians from all regions of Slovenia that were willing to participate in the study. Data was collected from all adolescents that have had an obligatory clinical examination performed by these pediatricians in the years 2004, 2009, and 2014. In 2014, however, 11 subjects were excluded due to missing data (2 gender, 4 height and weight, 5 age). In 2009, 4 subjects were excluded due to missing data (3 height, 1 weight), 1 due to age < 15 years and 51 due to age > 17 years. In 2004, no subjects were excluded.
The adolescents were measured in their underwear in the morning in a fasted state by a trained medical professional. Height and weight were determined by validated stadiometers and electronic digital scales. Both were rounded to the first decimal place. BMI was calculated as weight (kg) divided by squared height (m).
Overweight and obesity prevalence were calculated using the International Obesity Task Force (IOTF) criteria corresponding to adult's BMI cut-offs of 25 and 30 kg/m2, respectively, at 18 years of age [14]. These criteria define age- and gender-specific cut-off points from 2- to 18-year-old children.
In 2009 and 2014 data, the type of secondary schools adolescents were entering was also recorded. Adolescents were divided into two groups according to the type of secondary school. Adolescents entering academically oriented grammar secondary schools were included into the first group. Adolescents entering other types of secondary schools - vocational schools and technical/professional secondary schools - were included into the second group. Adolescents with missing data on the type of schooling were excluded from the sub-analysis (N = 1,446 in 2009 and N = 879 in 2014). The effective size of the population of students entering secondary schools in Slovenia was obtained for each of the 12 statistical regions and for each gender [15].
Statistical Analysis
Descriptive statistics were calculated for the three survey time points (2004, 2009, and 2014). The results were reported as the number and proportion of subjects that were overweight (including obese) or obese, with 95% confidence interval (95% CI) separately for males and females.
The gender-specific BMI distributions in consecutive years were compared using quantile-quantile (QQ) plots. QQ plots are scatter plots of the quantiles of one distribution against the quantiles of the second distribution and are useful for the assessment of the similarity between two distributions. If two distributions are similar, the points should be close to the identity line. The BMI distributions were compared using Mann-Whitney test.
To take the sampling scheme into account, the proportion estimates were obtained for each of the statistical regions, and the overall estimate was defined as their weighted average (the weights being the proportion of students effectively enrolled in each region, for each year and gender). To take into account that the sampling fraction was large, a finite population correction was applied; the correction guarantees that the standard errors are estimated correctly when the population is not infinite, and in practice it reduces the standard errors by a factor equal to √((N - n)) ⁄ ((N - 1)), where n and N are the sizes of the sample and of the population, respectively. Standard errors, 95% CI, and p values were based on hypergeometric distribution for the region-specific estimates and on normal approximation for the overall estimates. Unweighted estimates were also derived. The comparisons between vocational and technical/professional schools versus grammar schools were based on unweighted estimates; the p values were obtained using the chi-square test, and the 95% CI were based on normal approximation.
The R statistical program was used for statistical analysis [16]. The Sprop function included in the sampling book R package was used to obtain the results corrected for the finite population.
Results
Altogether 17,538 (8,437 females) adolescents entering secondary schools were included in the study. The prevalence of overweight and obesity in the year 2004 has been reported previously [13]. The sample included 10.1% of all students entering secondary schools in Slovenia in 2004, 31.6% in 2009, and 40.6% in 2014. Descriptive statistics data are presented in table 1.
Table 1.
Overweight/obesity prevalence and auxologic data in adolescent females and males in the years 2004, 2009 and 2014
| 2004 |
2009 |
2014 |
Δ 2009 – 2004*
|
Δ 2014 – 2009*
|
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| females (n = 1,412, 53%) | males (n= 1,229,47%; | females) (n = 3,500, 51%) | males (n = 3,361, 49%) | females (n = 3,525, 44%) | males (n = 4,511, 56%; | females | males | females | males | |
| Age, years | 15.66 ± 0.60 | 15.74 ± 0.68 | 15.13 ± 0.38 | 15.16 ± 0.41 | 15.55 ± 0.49 | 15.60 ± 0.57 | ||||
|
| ||||||||||
| BMI, kg/m2 | 21.34 ± 3.39 | 21.53 ± 3.35 | 21.99 ± 3.88 | 22.40 ± 4.22 | 22.03 ± 3.88 | 22.40 ±4.23 | ||||
|
| ||||||||||
| Overweight prevalence, % (95% CI) | 18.6 (16.5–20.7) | 20.6 (18.1–23.1) | 21.0 (19.8–22.3) | 29.4 (27.9–30.9) | 23.4 (22.1–24.7) | 28.6 (27.5–29.8) | 2.4 (0.0–4.9) p = 0.052 | 8.8 (5.9–11.7) p < 0.001 | 2.4 (0.6–4.1) p = 0.010 | –0.8 (–2.7 to 1.1) p = 0.424 |
|
| ||||||||||
| Obesity prevalence, % (95% CI) | 3.5 (2.5–4.6) | 3.0 (2.1–4.0) | 5.7 (5.0–6.5) | 9.3 (8.3–10.3) | 5.6 (4.9–6.3) | 9.2 (8.5–10.0) | 2.2 (0.9–3.4) p <0.001 | 6.3 (4.9–7.6) p < 0.001 | –0.1 (–1.1 to 0.9) p = 0.790 | –0.1 (–1.3 to 1.1) p = 0.925 |
Estimated difference of proportions (95% CI, p value).
Trends in Overweight and Obesity Prevalence from 2004 to 2014
There was an increase in the prevalence of overweight in the period 2004-2009, being more profound in males than in females (table 1). It however stabilized in the period 2009-2014, especially in males (table 1). Obesity prevalence increased significantly from 2004 to 2009 for both females and males, and stabilized in the period 2009-2014 (table 1).
Males were more prone to be overweight than females in the years 2009 and 2014 : 8.4 (6.4-10.3, p < 0.001) versus 5.2 (3.5-7.0, p < 0.001) (estimated difference of proportions (95% CI, p value)). In addition, males were also more prone than females to be obese in years the 2009 and 2014: 3.6 (2.4-4.8), p < 0.001 versus 3.7 (2.7-3.7, p < 0.001).
Similar results were obtained with the unweighted estimates (within 0.5 percentage points for obesity and 1.5 percentage points for overweight, complete data not shown).
Trends in BMI Distribution in Males and Females from 2004 to 2014
In addition to trends in the prevalence of overweight and obesity, we have also investigated the pattern of BMI distribution within the population. Distribution of central BMI values (mean and median) changed modestly in the selected time period (fig. 1). There was however a change towards an increased prevalence of adolescents with very high BMI values from 2004 to 2009 for both females and males and for males from 2009 to 2014, but not for females (fig. 1). Overall, the 2004 and 2009 gender-specific BMI distributions were significantly different (p < 0.001 for both genders), while the 2009 and 2014 BMI distributions were not (p = 0.72 and 0.91 for females and males, respectively).
Fig. 1.
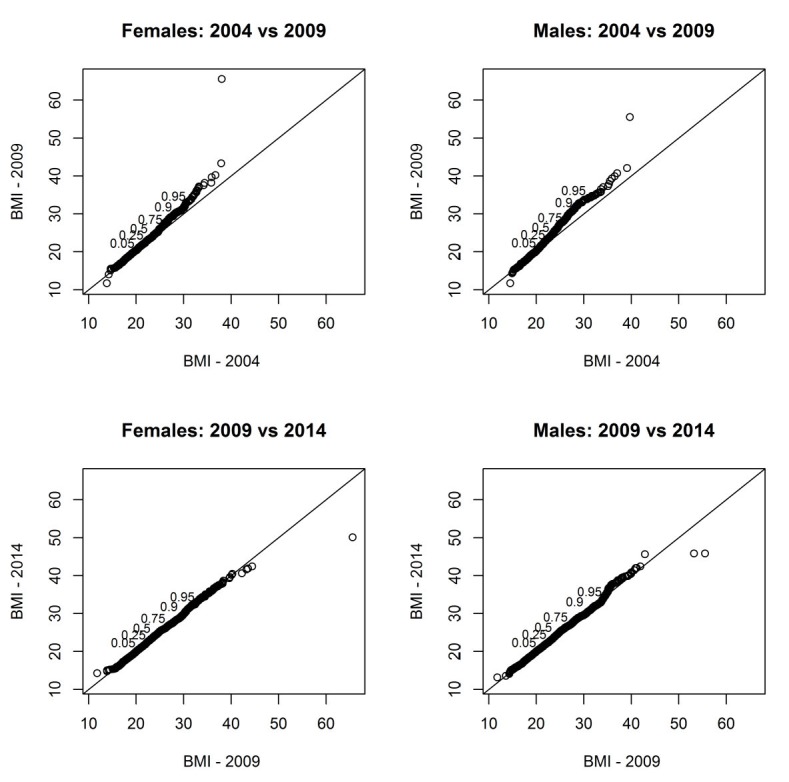
Quantile to quantile plots of observed BMI in adolescent males and females in the period 2004-2014 (pairwise comparisons). The numbers in the plots indicate the ordinate position of the corresponding quantile of the distribution plotted on the ordinate axis, e.g., in the first plot 0.5 is plotted on the ordinate where the median of the distribution of BMI for year 2004 is 21.3.
Overweight and Obesity Prevalence in Relation to the Type of Secondary School
As presented in table 2, the prevalence of overweight and obesity was higher in both males and females attending vocational and technical/professional secondary schools. All differences (for both obesity and overweight within each gender and year) were significant (p < 0.0001).
Table 2.
Overweight and obesity prevalence in adolescent females and males according to the type of secondary school they are attending in years 2009 and 2014
| School | 2009 |
2014 |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| females |
males |
females |
males |
|||||||||
| grammar (n = 1,371, 39%) | non-grammar (n = 1,259, 36%) | Δ non-grammar – grammar | grammar (n = 820, 24%) | non-grammar (n = 1,946, 58%) | Δ non-gramma –grammar | r grammar (n = 1549, 44%) | non-grammar (n = 1,585, 45 %) | Δ non-grammar – grammar | grammar (n = 939, 21%) | non-grammar (n = 3,060, 68%) | Δ non-grammar – grammar | |
| Over-weight | 16.8 (14.9–19.0) | 28.7 (26.3–31.3) | 11.9 (8.6–15.2) p < 0.001 | 22.3 (19.6–25.4) | 31.6 (29.6–33.7) | 9.3 (5.7–12.9) p < 0.001 | 17.9 (16.1–20.0) | 29.7 (27.5–32.0) | 11.8 (8.8–14.8) p < 0.001 | 20.4 (17.9–23.1) | 33.6 (31.9–35.3) | 13.2 (10.0–16.3) p < 0.001 |
|
| ||||||||||||
| Obesity | 4.2 (3.3–5.5) | 8.6 (7.1–10.3) | 4.4 (2.4–6.3) p < 0.001 | 5.3 (3.9–7.1) | 11.2(9.9–12.7) | 5.9 (3.8–8.1) p < 0.001 | 3.3 (2.5–4.3) | 7.8 (6.5–9.2) | 4.4 (2.8–6.1) p < 0.001 | 4.0 (2.9–5.5) | 12.0 (10.9–13.3) | 8.0 (6.2–9.8) p < 0.001 |
Overweight and obesity prevalence is expressed as percentage and 95% confidence interval. Non-grammar school includes vocational and technical/professional schools. Δ – difference.
Discussion
Trends in overweight and obesity prevalence in Slovenian adolescents entering secondary schools were estimated by analyzing data from 10% of adolescents entering secondary schools in Slovenia in 2004, 32% in 2009, and 41% in 2014 [15]. One of the main findings was that overweight and obesity prevalence increased from 2004 to 2009 (being more profound in males) and then stabilized from 2009 to 2014.
In the time period 2001-2002, Slovenia ranked in the middle of the 34 countries (including several European countries, USA, Canada, and Israel) participating in the Health Behaviour in School-Aged Children (HBSC) survey with an overweight (including obesity) prevalence of 14.9% in 10- to 16-year-old adolescents (girls and boys) which was determined using self-reported data [17]. In 2010, according to the IOTF criteria and based on measured weight, 22.5% of girls and 31.7% of boys aged 10-12 years in Slovenia were overweight or obese, which is similar to our results (table 1) [18]. Also in 2010, it was estimated that 21.2% of boys and 13.5% of girls aged 14 years in the capital city of Ljubljana were overweight according to IOTF criteria [12]. These data are further supported by the data from the HBSC survey performed in the period 2009-2010 where it was estimated that 13% of girls and 23% of boys were overweight or obese. Slovenia ranked in the upper third of countries participating in the study [19].
In the period 2009-2014, however, overweight and obesity prevalence trends in Slovenian adolescents stabilized. Similar trends were recently determined in Germany where overweight and obesity in children/adolescents aged 4-16 years stabilized already in the years 2004 and 2008 [20] and in the USA where obesity in 2- to 19-year-old children remained stable between 2007 and 2008 as well as 2009 and 2010 [21]. In England overweight and obesity prevalence stabilized between 2004 and 2013 in younger children but still increased in 11- to 15-year-old children, although to a lesser extent [22]. Despite the stabilization of overweight and obesity prevalence, Slovenia ranks in the group of countries with the highest prevalence of overweight and obesity in adolescents in Europe [23].
Data on nutritional habits or physical activity of the subjects were unfortunately not collected in the present study. Therefore, we can only speculate on the reasons why the prevalence of overweight and obesity increased in Slovenian adolescents in the period 2004-2009.
Increased energy intake is suspected to be a major cause for the obesity pandemic in children and adolescents, i.e., a diet high in energy, saturated fats, carbohydrates, sugar-sweetened drinks, and low in fiber [24,25,26]. It was determined that in years 2003-2005 Slovenian adolescents did not meet minimal standards for the intake of vegetables, grains, fish and plant oils, and also fruits in boys [27]. Intake of sugar-sweetened beverages was determined to be extremely high, ranking at the top of international scale of sugar-sweetened beverages intake in 2010 [28]. This was especially evident in boys when compared to girls, possibly explaining the more profound increase in the prevalence of overweight and obesity in adolescent boys when compared to girls in the present study [27,28]. It was also estimated that Slovenian adolescents, based on food frequency questionnaire and 3-day weighted dietary protocol, consumed excessive amounts of free sugars, especially in liquid form [29]. Some adolescents did tend to underreport and overreport their energy intake but it was assessed that the assessment of the diet of the whole group was valid [30].
In addition only 44% of children had regular breakfast during the working week in this time period, which ranked Slovenian adolescents at the very bottom of the international scale of regular breakfast consumption [28]. Having breakfast is associated with higher diet quality and lower prevalence of adiposity [31].
Recently a stabilization of obesity in 5-year-old children in Slovenia was reported. It was speculated that this might be caused by new national nutritional guidelines for the preparation of meals in kindergartens and schools, with decreased total fat and carbohydrate intake [11]. More than 75% of 5-year-old Slovenian children visit kindergartens, where they receive up to 4 meals per day [11]. A significantly lower percentage of Slovenian adolescents had regular meals in schools in this time period [32].
In addition to unhealthy diet, physical inactivity is also a major contributor to the development of overweight and obesity in children and adolescents [33,34,35]. Adolescents from Northern and Central Europe tend to be more physically active than those from Southern Europe, where overweight and obesity prevalence is higher [23,36]. According to self-reported data from the HBSC study there has been a decline in regular physical activity in Slovenian adolescents in the period 2002-2010 [28]. A decrease in motor abilities in Slovenian 6- to 18-year-old children and adolescents was determined by objectively measured motor abilities [37]. In addition to nutritional causes this could significantly contribute to the increased prevalence of overweight and obesity in Slovenian adolescents.
Our results indicate that not only the prevalence of obesity but also that of adolescents with very high BMI values increased (fig. 1). This change was more evident in adolescent boys than girls. Similar observations were made in North America, several European countries, Australia, and New Zeeland [21,38,39,40]. A proposed explanation is that children with a genetic predisposition for obesity are especially susceptible to the environmental risk factors causing obesity, with boys being more sensitive than girls [39].
The prevalence of adolescents that drink sugar-sweetened beverages however decreased in the period 2010-2014. The decrease was more significant in adolescent boys - from 48.8% in 2010 to 28% in 2014, than in girls - from 39.2% to 22.7% [28]. This may be attributed to campaigns targeting intake of sugar-sweetened beverages by informing children, parents and educational professionals about negative health effects of sugar-sweetened beverages and advantages of drinking plain water [41]. In addition, the percent of adolescents that regularly eat breakfast increased [28]. Not eating breakfast regularly is associated with higher risk of obesity [31]. On the other side it is possible to decrease this risk by targeted interventions [42]. Regular physical activity plays an prominent role in obesity prevention [35]. In this respect it is important to acknowledge the possible effect of the Healthy Lifestyle Project on the stabilization of overweight and obesity prevalence in Slovenia. This project has been offering children and adolescents aged 6-15 years additional sports activities for several years in all regions of Slovenia [43].
A significantly lower prevalence of overweight and obesity was estimated in adolescents attending grammar schools, compared to those attending secondary vocational and technical/professional schools in the years 2009 and 2014 (table 2). There are limited data on the association between type of school children/adolescents are attending and the overweight and obesity prevalence; however, differences between girls attending secondary grammar schools versus those attending vocational and technical/professional secondary schools were already reported in 2004. At that time girls attending grammar secondary schools were taller, lighter, had smaller skin fold thickness, and achieved better results in motor tests [44]. Children attending secondary vocational schools have poorer academic results when compared to those attending grammar schools. There is a negative association between overweight and obesity prevalence in children and their academic results [45,46]. Obese adolescents have higher probability of being enrolled in a school with lower level of education [45]. Academic results are associated with socioeconomic status and directly or indirectly with overweight and obesity. Adolescents attending schools with lower socioeconomic status have a higher BMI when compared to those attending schools with higher socioeconomic status, e.g. private schools [47]. Altogether, overweight and obesity prevalence is associated with adolescent's academic results and socioeconomic status. Therefore specifically targeted interventions, taking into account adolescent's academic and socioeconomic status, need to be strictly implemented for adolescents attending secondary vocational and technical/professional schools in Slovenia.
One of the strengths of the presented study is that a large sample of adolescents from all regions of Slovenia was analyzed. This was especially true for samples from 2009 (32%) and 2014 (41%), and thus the main conclusions of the study were derived for the time period 2009-2014. For the sample estimates to be as representative as possible of the population values the proportion estimates were obtained for each of the statistical regions and the overall estimate was defined as their weighted average (the weights being the proportion of students effectively enrolled in each region, for each year and gender). Another strength is that anthropometric measurements were performed by trained medical professionals using validated stadiometers and electronic digital scales.
Several limitations also have to be acknowledged. The measurements were not limited to one season only, but were performed from September to May of the following year, and this could have an effect on the reported results as it is known that there is a seasonal variability in nutritional status. In addition, data on nutritional and physical activity habits were not collected making a discussion on possible causes of estimated changes and differences in overweight and obesity prevalence speculative. Determination of these causes was however not an aim of the study.
Conclusions
Overweight and obesity prevalence increased in Slovenian adolescents entering secondary schools in the period 2004-2009. Thereafter, prevalence of overweight and obesity stabilized in the period 2009-2014, similarly to several other developed countries. Adolescent boys seem to be at particularly high risk for developing overweight and obesity, when compared to adolescent girls.
Adolescents entering vocational and technical/professional secondary schools are at an increased risk for overweight and obesity when compared to adolescent entering grammar schools. Specifically targeted intervention, such as healthy and regular meals, regular and appropriate physical activity and educational programs about healthy lifestyle provided by the school, should therefore be strictly implemented, especially in this population.
Disclosure Statement
The authors declare that they have no conflict of interest.
Acknowledgments
This study was supported in part by the Slovenian Research Agency grants P3-0343 and J3-6798.
The study protocol was approved by the National Medical Ethics Committee (#25/10/09). All procedures performed in the study were in accordance with the 1964 Helsinki declaration and its later amendments.
Authors would like to acknowledge the efforts of all primary care pediatricians and their teams that were involved in the collection of the data: Andrenšek Alenka, Cajnkar Kac Miroslava, Dimc Orhideja, Golnar Andreja, Goršič-Frank Mojca, Goste Ksenija, Gracar Irena, Grgič Martina, Gusič Irena, Hočevar Nives, Horvat Alenka, Ivankovič-Kacjan Mojca, Jagrič Friškovec Anita, Jerman Gorišek Lea, Kerin Grošelj Marija, Klemenčič Irena, Klim Janusz, Kocjan Melanja, Kocjan Mirjana, Kodrin Pušnik Janeta, Kolar Božena, Kolman Krapež Irena, Komen Odineja, Kozorog Ksenija, Krajnik Valentič Bernarda, Kržišnik Irena, Kvas Kučič Branka, Laktič Romana, Levstek Plut Maruška, Lovše Eva, Lovšin Salmič Kristina, Miklavič Breda, Orehek-Kirbis Marta, Pečnik Gerlec Miroslava, Petrović Nenad, Rančigaj-Žabkar Marija, Rojko Irena, Schweiger Nemanič Janja, Škulj Aleksandra, Trupac Paola, Vidmar Romič Milena, Žagar Slana Alenka.
K.S. contributed to conception and design of the study, collection of the data, interpretation of the results, and drafting the article. L.L. contributed to analysis and interpretation of data and drafting the article. T.B. contributed to conception and design of the study, collection of the data, interpretation of the results, and critical revision of the manuscript. P.K. contributed to conception and design of the study, interpretation of the results, and critical revision of the manuscript.
References
- 1.Cali AMG, Caprio S. Obesity in children and adolescents. J Clin Endocrinol Metabol. 2008;93((11 suppl 1)):s31–s36. doi: 10.1210/jc.2008-1363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Starc G, Strel J. Tracking excess weight and obesity from childhood to young adulthood: a 12-year prospective cohort study in Slovenia. Public Health Nutr. 2011;14:49–55. doi: 10.1017/S1368980010000741. [DOI] [PubMed] [Google Scholar]
- 3.Maggio AB, Martin XE, Saunders Gasser C, Gal-Duding C, Beghetti M, Farpour-Lambert NJ, Chamay-Weber C. Medical and non-medical complications among children and adolescents with excessive body weight. BMC Pediatr. 2014;14:232. doi: 10.1186/1471-2431-14-232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Farpour-Lambert NJ, Baker JL, Hassapidou M, Holm JC, Nowicka P, O'Malley G, Weiss R. Childhood obesity is a chronic disease demanding specific health care - a position statement from the Childhood Obesity Task Force (COTF) of the European Association for the Study of Obesity (EASO) Obes Facts. 2015;8:342–349. doi: 10.1159/000441483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF, Abraham JP, Abu-Rmeileh NM, Achoki T, AlBuhairan FS, Alemu ZA, Alfonso R, Ali MK, Ali R, Guzman NA, Ammar W, Anwari P, Banerjee A, Barquera S, Basu S, Bennett DA, Bhutta Z, Blore J, Cabral N, Nonato IC, Chang JC, Chowdhury R, Courville KJ, Criqui MH, Cundiff DK, Dabhadkar KC, Dandona L, Davis A, Dayama A, Dharmaratne SD, Ding EL, Durrani AM, Esteghamati A, Farzadfar F, Fay DF, Feigin VL, Flaxman A, Forouzanfar MH, Goto A, Green MA, Gupta R, Hafezi-Nejad N, Hankey GJ, Harewood HC, Havmoeller R, Hay S, Hernandez L, Husseini A, Idrisov BT, Ikeda N, Islami F, Jahangir E, Jassal SK, Jee SH, Jeffreys M, Jonas JB, Kabagambe EK, Khalifa SE, Kengne AP, Khader YS, Khang YH, Kim D, Kimokoti RW, Kinge JM, Kokubo Y, Kosen S, Kwan G, Lai T, Leinsalu M, Li Y, Liang X, Liu S, Logroscino G, Lotufo PA, Lu Y, Ma J, Mainoo NK, Mensah GA, Merriman TR, Mokdad AH, Moschandreas J, Naghavi M, Naheed A, Nand D, Narayan KM, Nelson EL, Neuhouser ML, Nisar MI, Ohkubo T, Oti SO, Pedroza A, Prabhakaran D, Roy N, Sampson U, Seo H, Sepanlou SG, Shibuya K, Shiri R, Shiue I, Singh GM, Singh JA, Skirbekk V, Stapelberg NJ, Sturua L, Sykes BL, Tobias M, Tran BX, Trasande L, Toyoshima H, van de Vijver S, Vasankari TJ, Veerman JL, Velasquez-Melendez G, Vlassov VV, Vollset SE, Vos T, Wang C, Wang X, Weiderpass E, Werdecker A, Wright JL, Yang YC, Yatsuya H, Yoon J, Yoon SJ, Zhao Y, Zhou M, Zhu S, Lopez AD, Murray CJ, Gakidou E. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013:a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. doi: 10.1016/S0140-6736(14)60460-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1:11–25. doi: 10.1080/17477160600586747. [DOI] [PubMed] [Google Scholar]
- 7.Wabitsch M, Moss A, Kromeyer-Hauschild K. Unexpected plateauing of childhood obesity rates in developed countries. BMC Med. 2014;12:17. doi: 10.1186/1741-7015-12-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kovač M, Leskošek B, Strel J. Overweight and obesity trends in Slovenian boys from 1991 to 2006. Acta Univ Palacki Olomuc. 2008;38:17–25. [Google Scholar]
- 9.Leskošek B, Strel J, Kovač M. Overweight and obesity in Slovenian schoolgirls, 1991-2006. Coll Antropol. 2010;34:1303–1308. [PubMed] [Google Scholar]
- 10.Kovač M, Jurak G, Leskošek B. The prevalence of excess weight and obesity in Slovenian children and adolescents from 1991 to 2011. Anthropol Notebooks. 2012;18:91–103. [Google Scholar]
- 11.Sedej K, Kotnik P, Avbelj Stefanija M, Grošelj U, Širca Čampa A, Lusa L, Battelino T, Bratina N. Decreased prevalence of hypercholesterolaemia and stabilisation of obesity trends in 5-year-old children: possible effects of changed public health policies. Eur J Endocrinol. 2014;170:293–300. doi: 10.1530/EJE-13-0566. [DOI] [PubMed] [Google Scholar]
- 12.Kovač M, Jurak G, Zaletelj Kragelj L, Leskošek B. The secular trend in the prevalence of overweight and obesity in the population of primary school children from Ljubljana (Slovenia) Slov J Pub Health. 2014;53:188–198. [Google Scholar]
- 13.Avbelj M, Saje-Hribar N, Seher-Zupančič M, Brcar P, Kotnik P, Iršič A, Bratanič N, Kržišnik C, Battelino T. Prevalenca čezmerne prehranjenosti in debelosti med pet let starimi otroki in 15 oziroma 16 let starimi mladostnicami in mladostniki v Sloveniji (Prevalence of overweight and obesity among 5 year old children and 15 and 16 year old adolescents in Slovenia) Zdrav Vestn. 2005;74:753–59. [Google Scholar]
- 14.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320:1240–1243. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Statistični urad Republike Slovenije Število in delež dijakov in vajencev vpisanih v 1. letnik programov srednješolskega izobraževanja po regijah, Ljubljana, 2015. (Statistical office of Republic of Slovenia: Number and percentage of high school students enrolled in first year of high school by region, Ljubljana, 2015).
- 16.R Development Core Team . R: A Language and Environment for Statistical Computing. Vienna: the R Foundation for Statistical Computing; 2011. [Google Scholar]
- 17.Janssen I, Katzmarzyk PT, Boyce WF, Vereecken C, Mulvihill C, Roberts C, Currie C, Pickett W, Health Behaviour in School-Aged Children Obesity Working Group Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes Rev. 2005;6:123–132. doi: 10.1111/j.1467-789X.2005.00176.x. [DOI] [PubMed] [Google Scholar]
- 18.Brug J, van Stralen MM, Te Velde SJ, Chinapaw MJ, De Bourdeaudhuij I, Lien N, Bere E, Maskini V, Singh AS, Maes L, Moreno L, Jan N, Kovacs E, Lobstein T, Manios Y. Differences in weight status and energy-balance related behaviors among schoolchildren across Europe: the ENERGY-project. PLoS ONE. 2012;7:e34742. doi: 10.1371/journal.pone.0034742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Currie C, Zanotti C, Morgan A, Currie D, de Looze M, Samdal O, Smith ORF. Health Behaviour in School-Aged Children (HBSC) study: International Report from the 2009/2010 Survey. Copenhagen: WHO Regional Office for Europe, (Health Policy for Children and Adolescents); 2012. Social Determinants of Health and Well-Being among Young People. pp. 115–118. [Google Scholar]
- 20.Blüher S, Meigen C, Gausche R, Keller E, Pfäffle R, Sabin M, Werther G, Odeh R, Kiess W. Age-specific stabilization in obesity prevalence in German children: a cross-sectional study from 1999 to 2008. Int J Pediatr Obes. 2011;6:e199–e206. doi: 10.3109/17477166.2010.526305. [DOI] [PubMed] [Google Scholar]
- 21.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999-2010. JAMA. 2012;307:483–490. doi: 10.1001/jama.2012.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Van Jaarsveld CHM, Gulliford MC. Childhood obesity trends from primary care electronic health records in England between 1994 and 2013:population-based cohort study. Arch Dis Child. 2015;100:214–219. doi: 10.1136/archdischild-2014-307151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Grammatikopoulou MG, Poulimeneas D, Gounitsioti IS, Gerothanasi K, Tsigga M, Kiranas E. Prevalence of simple and abdominal obesity in Greek adolescents: the ADONUT study. Clin Obes. 2014;4:303–308. doi: 10.1111/cob.12070. [DOI] [PubMed] [Google Scholar]
- 24.Ambrosini GL, Emmett PM, Northstone K, Howe LD, Tilling K, Jebb SA. Identification of a dietary pattern prospectively associated with increased adiposity during childhood and adolescence. Int J Obes. 2012;36:1299–1305. doi: 10.1038/ijo.2012.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: a systematic review. Am J Clin Nutr. 2006;84:274–288. doi: 10.1093/ajcn/84.1.274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zheng M, Rangan A, Olsen NJ, Bo Andersen L, Wedderkopp N, Kristensen P, Grøntved A, Ried-Larsen M, Lempert SM, Allman-Farinelli M, Heitmann BL. Sugar-sweetened beverages consumption in relation to changes in body fatness over 6 and 12 years among 9-year-old children: the European Youth Heart Study. Eur J Clin Nutr. 2014;68:77–83. doi: 10.1038/ejcn.2013.243. [DOI] [PubMed] [Google Scholar]
- 27.Kobe H, Štimec M, Ribič CH, Fidler Mis N. Food intake in Slovenian adolescents and adherence to the Optimized Mixed Diet: a nationally representative study. Public Health Nutr. 2012;15:600–608. doi: 10.1017/S1368980011002631. [DOI] [PubMed] [Google Scholar]
- 28.Jeriček Klanšček H, Koprivnikar H, Drev A, Pucelj V, Zupanič T, Britovšek K. Z zdravjem povezano vedenje v šolskem obdobju med mladostniki v Sloveniji (Health behaviour in school period among adolescents in Slovenia). Ljubljana: National Institute of Public Health of the Republic of Slovenia; 2014. [Google Scholar]
- 29.Fidler Mis N, Kobe H, Štimec M. Dietary intake of macro-and micronutrients in Slovenian adolescents: comparison with reference values. Ann Nutr Metab. 2012;61:305–313. doi: 10.1159/000342469. [DOI] [PubMed] [Google Scholar]
- 30.Kobe H, Kržišnik C, Fidler Mis N. Under-and over-reporting of energy intake in Slovenian adolescents. J Nutr Educ Behav. 2012;44:574–583. doi: 10.1016/j.jneb.2010.02.015. [DOI] [PubMed] [Google Scholar]
- 31.Rampersaud GC, Pereira MA, Girard BL, Adams J, Metzl JD. Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J Am Diet Assoc. 2005;105:743–760. doi: 10.1016/j.jada.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 32. Statistical Office of Republic of Slovenia Prebivalec Slovenije poje jabolk in medu več, mlečnih in žitnih izdelkov pa manj kot prebivalec (Inhabitant of Slovenia eats more apples and honey and less milk and grain products than EU inhabitant). EU28, 2014. www.stat.si/StatWeb/glavnanavigacija/podatki/prikazistaronovico?IdNovice=6652 (last accessed July 14, 2016).
- 33.Chaput JP, Lambert M, Mathieu ME, Tremblay MS, O'Loughlin J, Tremblay A. Physical activity vs. sedentary time: independent associations with adiposity in children. Pediatr Obes. 2012;7:251–258. doi: 10.1111/j.2047-6310.2011.00028.x. [DOI] [PubMed] [Google Scholar]
- 34.Ness AR, Leary SD, Mattocks C, Blair SN, Reilly JJ, Wells J, Ingle S, Tilling K, Smith GD, Riddoch C. Objectively measured physical activity and fat mass in a large cohort of children. PLoS Med. 2007;4:e97. doi: 10.1371/journal.pmed.0040097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hills AP, Andersen LB, Byrne NM. Physical activity and obesity in children. Br J Sports Med. 2011;45:866–870. doi: 10.1136/bjsports-2011-090199. [DOI] [PubMed] [Google Scholar]
- 36.Ruiz JR, Ortega FB, Martínez-Gómez D, Labayen I, Moreno LA, De Bourdeaudhuij I, Manios Y, Gonzalez-Gross M, Mauro B, Molnar D, Widhalm K, Marcos A, Beghin L, Castillo MJ, Sjöström M, HELENA Study Group Objectively measured physical activity and sedentary time in European adolescents: the HELENA study. Am J Epidemiol. 2011;174:173–184. doi: 10.1093/aje/kwr068. [DOI] [PubMed] [Google Scholar]
- 37.Starc G, Strel J, Kovač M. Telesni in gibalni razvoj slovenskih otrok in mladine v številkah: šolsko leto 2007/2008 (Physical and motor development of Slovenian children and adolescents in numbers: school year 2007/2008). Ljubljana: Faculty of Sport, University of Ljubljana; 2010. [Google Scholar]
- 38.Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303:242–249. doi: 10.1001/jama.2009.2012. [DOI] [PubMed] [Google Scholar]
- 39.Beyerlein A, Toschke AM, von Kries R. Risk factors for childhood overweight: shift of the mean body mass index and shift of the upper percentiles: results from a cross-sectional study. Int J Obes. 2010;34:642–648. doi: 10.1038/ijo.2009.301. [DOI] [PubMed] [Google Scholar]
- 40.Bibiloni MDM, Pons A, Tur JA. Prevalence of overweight and obesity in adolescents: a systematic review. ISRN Obes. 2013;2013:392747. doi: 10.1155/2013/392747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Fidler Mis N. Projekt zmanjšanje pitja pijač z dodanim sladkorjem pri otrocih, mladostnikih in ogroženih odraslih (Project of decreasing sugar sweetened beverages drinking among children, adolescents and adults at risk). www.vodazmaga.si/wp-content/uploads/2012/10/Oprojektupodrobno.pdf (last accessed July 14, 2016).
- 42.Ask AS, Hernes S, Aarek I, Johannessen G, Haugen M. Changes in dietary pattern in 15 year old adolescents following a 4 month dietary intervention with school breakfast-a pilot study. Nutr J. 2006;5:33. doi: 10.1186/1475-2891-5-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Zdrav življenjski slog 2014-2015 (Healthy lifestyle 2014-2015) www.zsrs-planica.si/zdrav-zivljenjski-slog/ (last accessed July 14, 2016)
- 44.Kovač M. When social becomes biological: the effect of different physical education curricula on motor and physical development of high-school girls. AnthropolNotebooks. 2006;12:97–112. [Google Scholar]
- 45.Do YK, Finkelstein EA. Adolescent weight status and self-reported school performance in South Korea. J Obes. 2011;2011:798409. doi: 10.1155/2011/798409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Taras H, Potts-Datema W. Obesity and student performance at school. J Sch Health. 2005;75:291–295. doi: 10.1111/j.1746-1561.2005.00040.x. [DOI] [PubMed] [Google Scholar]
- 47.Richmond TK, Subramanian SV. School level contextual factors are associated with the weight status of adolescent males and females. Obesity (Silver Spring) 2008;16:1324–1330. doi: 10.1038/oby.2008.48. [DOI] [PMC free article] [PubMed] [Google Scholar]