

Abstract
Background
While it is well known that substance use and gambling overlap, the degree to which this overlap can be explained by shared risk factors has not been fully explored. This study aimed to identify common and unique risk factors for gambling and substance use among young adults.
Methods
Young adults (n=1,019) in a longitudinal study since college entry were interviewed annually. Past-year frequency of seven gambling activities was assessed once (Year 5). Structural equation models evaluated suspected risk factors in two models, one for gambling with substance use as an intermediary variable, and one for substance use with gambling as the intermediary variable.
Results
Sixty percent gambled; 6% gambled weekly or more. Examination of the two structural models supported the existence of significant paths (a) from two of the five substance use variables (alcohol, drugs) to gambling frequency, and (b) from gambling frequency to all five substance use variables. Every risk factor associated with gambling was also associated with one or more substance use variables. Risk factors common to gambling and substance use were sex, race/ethnicity, extracurricular involvement (fraternity/sorority, athletics), impulsive sensation-seeking, and behavioral dysregulation. Risk factors unique to substance use were conduct problems, anxiety, and parent’s history of alcohol and mental health problems.
Conclusions
Gambling and substance use are interrelated, but with incomplete overlap in their respective risk factors. Results underscore the need for longitudinal research to elucidate their distinct etiologies.
Keywords: Alcohol use disorder, college students, drug use, gambling, young adults
1. Introduction
Gambling is a topic of public health concern among college students. Past-year prevalence estimates have ranged from 35% to 87% (Atkinson et al., 2012; Ellenbogen et al., 2008; LaBrie et al., 2003; Seifried et al., 2009; Welte et al., 2008; Wickwire et al., 2008; Wickwire et al., 2007; Winters et al., 1998), depending on how gambling behavior was measured. College students engage in a variety of different gambling activities, including playing the lottery, buying raffle tickets, playing cards for money, betting on sports, and playing sports for money (Barnes et al., 2010). While playing the lottery and card games tend to be the most prevalent among college students (Barnes et al., 2010; Wickwire et al., 2007), the popularity of certain gambling activities varies geographically based on proximity to gambling venues such as casinos and racetracks.
Among college students who do gamble, most do so infrequently. For example, LaBrie et al. (2003) found that while 25% of college students played the lottery, only 1% did so weekly or more. Some college students who gamble much more frequently might be considered problem gamblers. Studies using a standardized instrument to assess problem gambling {e.g., the South Oaks Gambling Screen [SOGS (Lesieur and Blume, 1987)]} have produced estimates ranging from 5% to 14% of college students meeting criteria for problem gambling (Bhullar et al., 2012a; Burger et al., 2006; Engwall et al., 2004; Martin et al., 2012; Weiss, 2010; Wickwire et al., 2008; Winters et al., 1998).
Several cross-sectional studies have focused on the overlap between gambling and substance use among college students and have consistently observed significant positive associations between gambling, problem gambling, and alcohol use (Bhullar et al., 2012b; Engwall et al., 2004; Goudriaan et al., 2009; Huang et al., 2011; LaBrie et al., 2003; Martens et al., 2009; Martin et al., 2014; Stuhldreher et al., 2007; Vitaro et al., 2001). For example, Bhullar et al. (2012b) found that, compared with students who did not meet criteria for binge drinking, binge drinking college students were more likely to participate in poker, Internet gambling, sports betting, and office pools. Similarly, Engwall et al. (2004) found that college student problem gamblers were more likely to be heavy drinkers and experience negative alcohol-related consequences compared with other students. Gambling is also significantly and positively associated with marijuana and other drug use (Engwall et al., 2004; Goudriaan et al., 2009; Huang et al., 2011; LaBrie et al., 2003; Lynch et al., 2004; Stuhldreher et al., 2007; Winters et al., 1998).
One major question is the extent to which the overlap between gambling and substance use can be explained by commonalities in pre-existing risk factors. Examples of shared risk factors for both gambling and substance use include family history, mental health problems, and gender (Barnes et al., 1999; Cook et al., 2015; Mezzich et al., 2001; Vitaro et al., 2014). A recent study utilizing adolescent twin pairs found a significant genetic influence on both gambling and substance use (Vitaro et al., 2014), which is consistent with other research among adults (Slutske et al., 2000; Slutske et al., 2013). Longitudinal data examining gender as a risk factor show an association between gambling problems and incident alcohol dependence among men (Pilver et al., 2013). Affiliation with delinquent peers or poor parental supervision are also common etiological factors to substance use and gambling among adolescents (Vitaro et al., 2001). Several studies show that temperament characteristics such as impulsivity, behavioral dysregulation, and deviance are predictive of both gambling and substance use (Barnes et al., 1999; Leeman et al., 2014; Mezzich et al., 2001; Vitaro et al., 2001).
Of the 11 studies that examine gambling and substance use among college students, only two account for shared risk factors. Winters et al. (1998) evaluated the non-redundant association between drug use and gambling to take into account several possible risk factors, the most significant of which were parental history of problematic gambling, male gender, and illicit drug use more than once per week. LaBrie et al. (2003) found that college students were more likely to gamble if they had families that did not disapprove of drinking, had parents who drank alcohol, and were involved in Greek life or athletics. Some researchers have suggested that excessive alcohol use and gambling might be part of a larger constellation of problem behaviors (Bhullar et al., 2012b; Engwall et al., 2004; Goudriaan et al., 2009; LaBrie et al., 2003; Martens et al., 2009; Stuhldreher et al., 2007; Weiss, 2010).
This study aimed to: 1) document the prevalence of gambling activities among a large sample of college-educated young adults; and 2) examine the independent relationships of several hypothesized risk factors with gambling and five measures of substance use based on two alternative structural models that account for their respective intermediary effects. We hypothesized that both direct and indirect effects would be observed, such that some risk factors would be shared by gambling and substance use simultaneously, while other risk factors would be uniquely associated with either gambling or substance use.
2. Methods
2.1. Study design
Data were gathered as part of the College Life Study, a longitudinal study of health-risk behaviors among a cohort of 1,253 young adults who were originally enrolled as first-year college students. Detailed methodological information has been published previously (Arria et al., 2008; Vincent et al., 2012). Briefly, in 2004, the incoming class of first-year students ages 17 to 19 at a large mid-Atlantic university were invited to complete a short assessment on substance use during high school (N=3,401; 89% response rate). A sample was then recruited for the longitudinal study after oversampling students who had used an illicit drug or nonmedically used a prescription drug at least once during high school. Because virtually all members of the incoming student cohort were assessed at summer orientation, stratified random sampling was possible, as described previously (Arria et al., 2008); no classroom clustering occurred. A two-hour baseline assessment (Year 1) was administered sometime during their first year of college (n=1,253; 87% response rate) and included both structured interview and self-administered modules. These participants were followed up annually in similar assessments, regardless of continued college attendance, with high follow-up rates (91% in Year 2, n=1,142; 81% in Year 5, n=1,019). Participants received cash incentives for each assessment they completed, and informed consent was obtained. Interviewers were trained extensively in confidentiality protection procedures. IRB approval and a federal Certificate of Confidentiality were obtained.
2.2. Participants
The analytic sample was restricted to 1,019 individuals (462 men, 731 non-Hispanic white) who completed the Year 5 assessment, because this was the year in which gambling behaviors were measured. By then, 80% had already graduated from college and 38% were enrolled in graduate school or other coursework. Compared with the 234 individuals who did not complete the Year 5 assessment, the inclusion sample was over-representative of females (55% vs. 38%, p<.001) but similar with respect to race, mother’s education, and neighborhood income during high school. Characteristics of the sample are presented in Table 1.
Table 1.
Sample characteristics (n=1,019)
| % (n) | Mean (SD) | |
|---|---|---|
| Substance Use (Year 5) | ||
| Alcohol Use Disorder Risk | 3.0 (1.2) | |
| % No alcohol use during the past year | 3.2 (33) | |
| % Used <5 times during the past year | 2.9 (29) | |
| % Used without DSM-IV problems | 33.4 (340) | |
| % Endorsed some DSM-IV problems | 12.3 (125) | |
| % Met criteria for alcohol abuse | 43.3 (441) | |
| % Met criteria for alcohol dependence | 5.0 (51) | |
| Alcohol use frequency, days in past year | 97.8 (70.6) | |
| Marijuana use frequency, days in past year | 28.2 (69.6) | |
| Tobacco use frequency, days in past year | 41.1 (96.6) | |
| Number of other drugs used, past year | 0.7 (1.2) | |
| Demographics | ||
| Sex (% Male) | 45.3 (462) | |
| Race/Ethnicity (% White, non-Hispanic) | 71.7 (731) | |
| Mother’s education | ||
| High school or less | 15.4 (157) | |
| Some college or technical | 11.7 (119) | |
| Bachelor’s degree | 38.5 (392) | |
| Graduate degree | 34.5 (351) | |
| Father’s education | ||
| High school or less | 16.1 (164) | |
| Some college or technical | 8.1 (82) | |
| Bachelor’s degree | 30.8 (314) | |
| Graduate degree | 45.0 (459) | |
| Current school enrollment (Year 5) | 37.8 (385) | |
| Current salary (Year 5) | ||
| < $10K | 30.8 (314) | |
| $10K to $24,999 | 20.4 (208) | |
| $25K to $49,999 | 34.8 (355) | |
| $50K to $74,999 | 12.6 (128) | |
| $75K or higher | 1.4 (14) | |
| Living situation (% with parent/guardian/relative, Year 5) | 41.4 (422) | |
| Parental History | ||
| Parents’ mental health problems | ||
| Mother (% definite problems) | 14.0 (143) | |
| Father (% definite problems) | 9.4 (96) | |
| Parents’ alcohol problems | ||
| Mother (% possible/definite problems) | 6.3 (64) | |
| Father (% possible/definite problems) | 18.0 (183) | |
| Parents’ drug problems | ||
| Mother (% possible/definite problems) | 2.9 (30) | |
| Father (% possible/definite problems) | 8.9 (91) | |
| Behavioral Disinhibition | ||
| Sensation-seeking score | 3.5 (2.2) | |
| Affective dysregulation score | 23.5 (10.3) | |
| Behavioral dysregulation score | 27.8 (11.7) | |
| Cognitive dysregulation score | 29.0 (8.9) | |
| Childhood conduct problems score | 6.6 (4.6) | |
| Mental Health | ||
| Depression symptoms | 5.3 (5.0) | |
| Anxiety symptoms | 7.5 (6.8) | |
| Extracurricular Involvement | ||
| Fraternity/sorority (% any involvement) | 34.4 (350) | |
| Athletics (% any involvement) | 71.6 (730) |
Note. Substance use was measured in Year 5, concurrently with gambling behaviors (see Figure 2). All other variables shown were assessed during Years 1 through 4, except where noted.
2.3. Measures
2.3.1. Gambling behaviors
Participants were asked in Year 5 how often they engaged in each of seven different gambling activities during the past year: gambling on the Internet, playing cards for money with friends, going to a casino, playing the lottery, betting on sports, betting on horse or dog races, and betting on games of personal skill. Response options (not at all, less than monthly, monthly, weekly, and daily) were scored 0 through 4, and were later summed to create an overall index of gambling frequency (Cronbach’s α=.67). We did not expect to find a large number of problem gamblers among this general college student sample, therefore we opted to assess gambling frequency instead of gambling problems. Gambling frequency was thought to be a good proxy for problem gambling in the future. Items were adapted from prior surveys (Winters et al., 1993).
2.3.2. Tobacco, alcohol, and other drug use
Past-year frequency of use was assessed via a structured interview in Year 5 for alcohol, tobacco, marijuana, and nine other types of illicit drugs (inhalants, hallucinogens, cocaine, amphetamines/methamphetamine, heroin, ecstasy) and prescription drugs used nonmedically (stimulants, analgesics, and tranquilizers). The variables on alcohol, tobacco, and marijuana use frequency were used in the present analyses as self-reported. For the nine other drugs, an index of other drug use was computed as the count of drugs that were used during the past year (0 to 9).
A series of questions (Substance Abuse and Mental Health Services Administration, 2003) assessed the DSM-IV criteria for Alcohol Use Disorders [AUD (American Psychiatric Association, 1994)]. Responses were later consolidated into a six-level variable [did not drink in the past year (0), drank fewer than five times (1), drank but did not endorse any AUD criteria (2), endorsed some AUD criteria but insufficient to meet the definition of alcohol abuse or dependence (3), alcohol abuse (4), alcohol dependence (5)] as an overall indicator of risk for AUD. This variable has demonstrated construct validity in prior studies with this sample (Arria et al., 2014; Arria et al., 2013d).
2.3.3. Demographic characteristics
Race/ethnicity and highest educational attainment of mother and father were self-reported. Sex was coded as observed at Year 1. Salary, school enrollment status, and living situation were assessed in Year 5.
2.3.4. Parental substance use and mental health history
Parental history of problems with alcohol and other drugs was assessed in Year 2 via a self-administered family tree questionnaire (Mann et al., 1985). Due to the small number of individuals endorsing definite parental problems with alcohol or drugs, responses were later consolidated into four dichotomous variables (mother’s alcohol problems, mother’s drug problems, father’s alcohol problems, father’s drug problems) coded as definite or possible problems (1) and no problems (0). Responses of “don’t know” were recoded conservatively as no problems. Parental history of depression and/or anxiety were assessed in a similar fashion in Year 4 and later consolidated into one dichotomous variable for each parent, coded as definite problems (1) and possible or no problems (0) due to the substantial proportion endorsing definite problems.
2.3.5. Behavioral disinhibition
Five measures of behavioral disinhibition were assessed in Year 1. Sensation-seeking was measured via a seven-item subscale of the Zuckerman-Kuhlman Personality Questionnaire (Zuckerman, 2002). The three subscales of the Dysregulation Inventory (Mezzich et al., 2001)—namely affective, behavioral, and cognitive dysregulation—have been validated among this and other college student samples as predictors of substance use disorders and other problem behaviors (Arria et al., 2015; Arria et al., 2013b; Mezzich et al., 2001; O’Grady et al., 2006). Childhood conduct problems were assessed using an adapted version of the conduct disorder screener (Johnson et al., 1995) which asked about 18 different conduct problems that might have occurred during childhood, corresponding to the DSM-IV criteria for conduct disorder (American Psychiatric Association, 1994). Responses were later weighted according to severity and consolidated into a scale score, following standard methods. This variable has been validated among this sample previously (Arria et al., 2013a; Falls et al., 2011; Garnier et al., 2010). Internal consistency among this sample was acceptable for all five scale scores (αs>.75). Convergent validity in relation to substance use and other problem behaviors has been demonstrated previously (Arria et al., 2015, 2016; Arria et al., 2013a; Arria et al., 2013b; Arria et al., 2013c).
2.3.6. Mental health
Symptoms of both depression and anxiety were assessed in Year 1 using the Beck Depression Inventory [BDI (Beck et al., 1979)] and Beck Anxiety Inventory [BAI (Beck et al., 1988)], respectively. The BDI consists of 21 items in each of which the respondent selects one of four statements describing their feelings during the past few days. The BAI asks participants to indicate how much they have been bothered by each of 21 possible symptoms of anxiety during the past week. Scale scores were later summed using standard procedures, and internal consistency was acceptable for both scales (αs>.85).
2.3.7. Extracurricular involvement
Responses to questions about involvement in Greek life and athletics during Years 2 through 5 were consolidated to create two dichotomous variables for fraternity/sorority involvement (i.e., “Greek”) and athletics, coded as regular or irregular involvement (1) and none (0).
2.4. Statistical analyses
Structural equation modeling (SEM) was selected as the analytic method of choice for two primary reasons. First, SEM allowed for examination of a model including both an intermediary variable and multiple antecedent variables (the risk factors). Second, SEM allows for testing and examination of fit of both the overall model and each variable in the model. It should be noted that while cross-sectional data obviously constrains the ability to make temporal or causal inferences, the direct and indirect effects of the variables can be evaluated using cross-sectional data. We refrain from formally labeling our approach as a mediation analysis because longitudinal data are preferable for assessing mediation (Kline, 2015). Moreover, by using baseline (or earliest available) measures of our risk factors—rather than subsequent observations that would have been more proximal to the dependent variables measured in Year 5 (gambling, substance use)—our models were designed to emphasize the prospective nature of the hypothesized association between the risk factors and the dependent variables. The purpose of this strategy is to understand which variables might be useful in identifying high-risk students during the first years of college.
The analytic strategy was to evaluate two alternative structural models, hereinafter referred to as Models A and B (see Figures 1a and 1b). The first model (A) examined the associations between the risk factors and the five substance use variables (i.e., AUD risk, alcohol use frequency, marijuana use frequency, tobacco use frequency, and number of other drugs used), both directly and indirectly through their influence on gambling frequency as the intermediary variable. The alternative model (B) examined the direct and indirect relationships between the same risk factors and gambling frequency, with the five substance use variables as intermediary variables. Each model was initially specified as an “indirect” model, such that in the first model (A1), gambling frequency served as the intermediary variable between the risk factors and substance use, and there were no direct paths between the risk factors and substance use, while in the first alternative model (B1), the five substance use variables served as intermediary variables between the risk factors and gambling, and there were no direct paths between the risk factors and gambling. In contrast, the second model (A2) allowed for all direct paths between the risk factors and the five substance use variables to be free and thus estimated and tested for significance, while in the second alternative model (B2), all paths between the risk factors and gambling were specified as free and so were estimated and tested for significance. These second models were then pruned of all their non-significant paths (α=.05) to obtain a more parsimonious model, and the resulting revised models (A3 and B3, respectively) were evaluated. These revised models were then re-fit a final time after additional non-significant paths were eliminated (Models A4 and B4, respectively). Thus, this model fitting approach allowed for the examination of both the direct and indirect effects of the risk factors on the distal effect of gambling or substance use, in which the other variable served as the intermediary variable.
Figure 1.
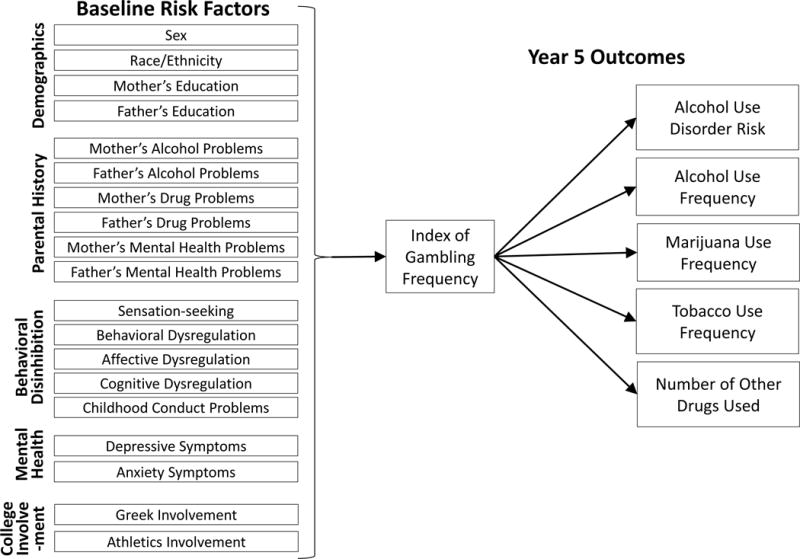
a: Hypothesized model A in which gambling predicts past-year substance use.
Note. In addition to the effects shown, Year 5 salary, Year 5 school enrollment status, and baseline living situation were partialled out as covariates.
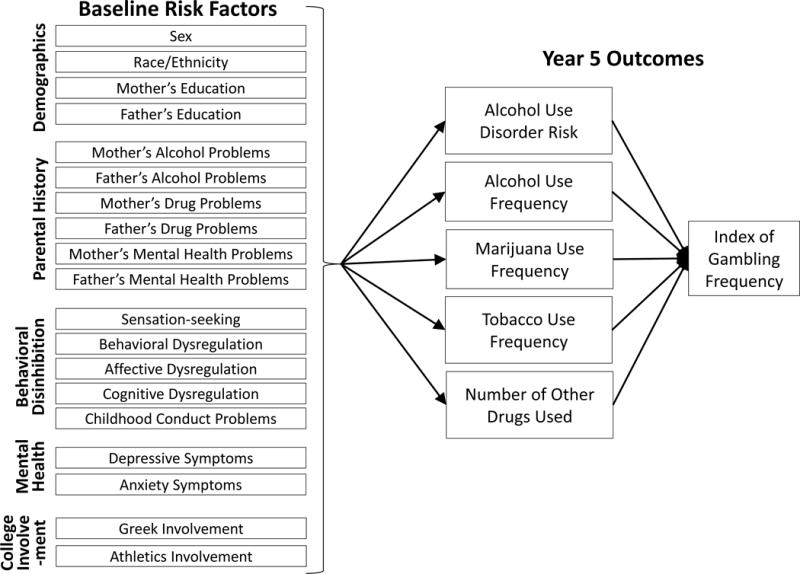
b: Hypothesized model B in which past-year substance use predicts gambling.
Note. In addition to the effects shown, Year 5 salary, Year 5 school enrollment status, and baseline living situation were partialled out as covariates.
The parental history variables were modeled as three latent variables: parental alcohol problems, parental drug problems, and parental mental health problems. Pathways involving multinomial categorical variables (i.e., parents’ education, alcohol problems, and drug problems) were evaluated using χ2 difference tests, given multiple paths associated with these variables. Model fit was evaluated using multiple criteria as per Hu and Bentler’s recommendation (1999), with cutoff values of ≥.95 for Bentler’s comparative fit index (CFI), ≤.06 for the root mean square error of approximation (RMSEA), and ≤.09 for the standardized root mean square residual (SRMSR); χ2 tests of overall model fit were also evaluated. Missing data were minimal (less than 9% for any given variable), and missing values were imputed using EM estimation. Year 5 variables on salary, school enrollment status, and living situation were partialled out as covariates in all models in order to reduce potential confounding of the hypothesized associations between the risk factors and dependent variables; this was important because of the sample’s heterogeneity on these dimensions during their transition from college to post-college life.
3. Results
As shown in Figure 2, 60% of the sample engaged in at least one gambling activity during the past year. Casino gambling (35%) was the most prevalent of the seven gambling activities assessed, followed by playing cards for money with friends (25%), playing the lottery (20%), and betting on sports (20%). Frequent gambling was rare, with 6% gambling weekly or more (i.e., responded “weekly” or “daily” for at least one gambling activity). For any given gambling activity, the proportion who participated on a weekly or daily basis was less than 3%.
Figure 2.
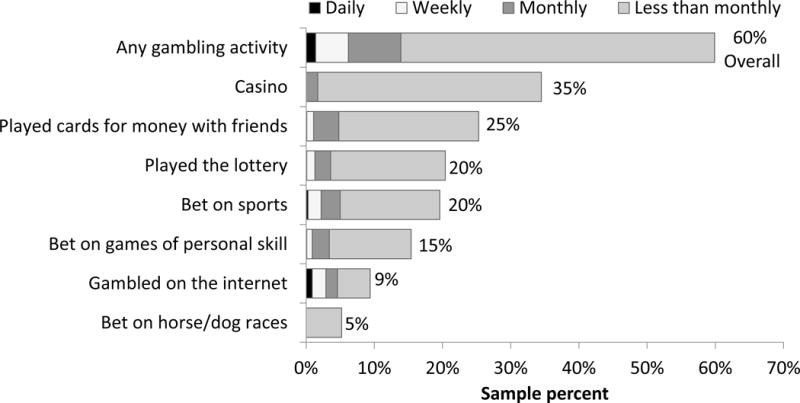
Prevalence and frequency of seven different gambling activities during the past year (n=1,109).
3.1. Structural models
Overall fit was acceptable for both of the final re-fit models (see Table 2). In the model in which gambling functioned as the intermediary variable between the risk factors and substance use outcomes (Model A), gambling was significantly associated with all five outcomes tested (see Figure 3). In the alternative model (B) in which gambling functioned as the outcome variable, alcohol use frequency and number of other drugs used were the only two substance use variables with significant indirect effects between the risk factors and gambling. Results of both models are discussed below in relation to the direct and indirect effects of the hypothesized risk factors on the respective outcome variables.
Table 2.
Summary of model fit for two sets of structural models
| Χ2 (df) | Bentler CFI | RMSEA | SRMSR | |
|---|---|---|---|---|
| Model A: Gambling → Substance use | ||||
| Model A1 | 295.57 (115) | .9633 | .0393 | .0317 |
| Model A2 | n/a | n/a | n/a | n/a |
| Model A3 | 116.10 (103) | .9973 | .0112 | .0164 |
| Model A4 | 117.93 (104) | .9972 | .0115 | .0159 |
| Model B: Substance use → Gambling | ||||
| Model B1 | 217.07 (23) | .9606 | .0912 | .0231 |
| Model B2 | n/a | n/a | n/a | n/a |
| Model B3 | 110.42 (102) | .9983 | .0090 | .0160 |
| Model B4 | 116.68 (106) | .9978 | .0100 | .0161 |
Note. Fit statistics are not provided for Models A2 and B2 as they were just-identified models and as such, the fit of the model to the data is perfect.
Figure 3.
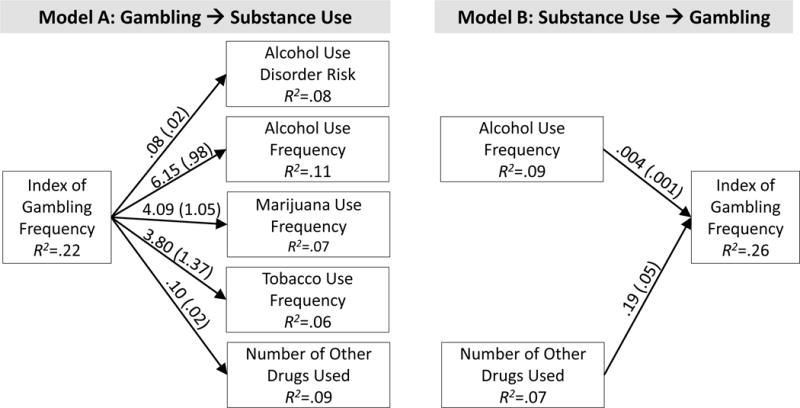
Results of two alternative structural models in which (A) gambling predicts past-year substance use, and (B) past-year substance use predicts gambling [b(SE)].
Note. All pathways shown were statistically significant (p<.05). All non-significant pathways were omitted. Pathways between the risk factors (shown in Figures 1a and 1b) and the outcome variables shown here have been omitted for ease of presentation; see Table 3 for comprehensive results of both models. In addition to the effects shown, Year 5 salary, Year 5 school enrollment status, and baseline living situation were partialled out as covariates.
3.2. Hypothesized risk factors related to neither gambling nor substance use
Five of the hypothesized risk factors we tested (mother’s education, mother’s and father’s drug problems, affective dysregulation, cognitive dysregulation) were omitted from both models because they had no significant associations with dependent variables.
3.3. Risk factors independently associated with both gambling and substance use
Involvement in Greek organizations had significant direct effects on both gambling and two of the five substance use variables tested, and these effects were not appreciably different between the two models (see Table 3). In the model in which gambling was the intermediary variable, the direct effect of Greek involvement on gambling was positive (b=.35, SE=.13). A very similar result was obtained in the model where gambling was the outcome (b=.28, SE=.13), even accounting for the modest indirect effect of Greek involvement via substance use (b=.094, SE=.026). Similarly, Greek involvement’s direct effect on alcohol use frequency was significant when alcohol was the intermediary variable (b=12.39, SE=4.00) or the outcome (b=9.92, SE=3.96), and its indirect effect on alcohol use via gambling was much more modest by comparison (b=2.13, SE=.86). By contrast, across the two models, the effects of Greek involvement on AUD, marijuana use frequency, and number of other drugs used were completely accounted for by gambling. Interestingly, Greek involvement functioned as a protective factor for tobacco use frequency, again via mechanisms that appeared to be distinct from its contribution to gambling, as evidenced by its direct association with less frequent tobacco use in both models (b=−15.58, SE=6.00, and b=−18.52, SE=5.97, respectively).
Table 3.
Direct and indirect contributions of hypothesized risk factors to gambling and substance use variables [b(SE)]
| Index of Gambling Frequency | Alcohol Use Disorder Risk | Alcohol Use Frequency | Marijuana Use Frequency | Number of Other Illicit Drugs Used | Tobacco Use Frequency | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intermediary Variable |
Outcome | Intermediary Variable |
Outcome | Intermediary Variable |
Outcome | Intermediary Variable |
Outcome | Intermediary Variable |
Outcome | Intermediary Variable |
Outcome | |||||||
|
| ||||||||||||||||||
| Direct | Direct | Indirect
via Alcohol Frequency and/ or Other Drugs |
Direct | Direct | Indirect via Gambling |
Direct | Direct | Indirect via Gambling |
Direct | Direct | Indirect via Gambling |
Direct | Direct | Indirect via Gambling |
Direct | Direct | Indirect via Gambling |
|
| Risk Factors | ||||||||||||||||||
| Independently associated with both gambling and substance use | ||||||||||||||||||
| Greek Involvement | 0.35 (0.13) | 0.28 (0.13) | 0.094 (0.026) | 0.028 (0.012) | 12.39 (4.00) | 9.92 (3.96) | 2.13 (0.86) | 1.42 (0.64) | 0.21 (0.06) | 0.04 (0.01) | −15.58 (6.00) | −18.52 (5.97) | ns | |||||
| Athletics Involvement | 0.50 (0.14) | 0.47 (0.14) | 0.062 (0.025) | 0.23 (0.08) | 0.23 (0.08) | 0.040 (0.014) | 14.17 (4.76) | 12.54 (4.63) | 3.06 (1.01) | 2.04 (0.79) | 0.05 (0.02) | 1.89 (0.87) | ||||||
| Associated primarily with substance use but not gambling | ||||||||||||||||||
| Father’s Alcohol Problems | ns | ns | 16.37 (7.46) | 17.54 (7.45) | ||||||||||||||
| Mother’s Alcohol Problems | −17.72 (7.40) | −17.36 (7.42) | ns | 11.77 (11.74) | ||||||||||||||
| Childhood Conduct Problems | 0.016 (0.007) | 0.019 (0.007) | 1.09 (0.48) | 0.017 (0.008) | ||||||||||||||
| Father’s Mental Health Problems | ns | 15.53 (7.23) | 15.66 (7.19) | 0.26 (0.12) | ns | ns | ns | |||||||||||
| Mother’s Mental Health Problems | ns | 19.25 (6.09) | 18.91 (6.06) | 0.20 (0.10) | ns | 32.58 (8.48) | 32.54 (8.47) | |||||||||||
| Anxiety Symptoms | 0.011 (0.005) | |||||||||||||||||
| Depressive Symptoms | −0.005 (0.002) | −1.05 (0.38) | −1.02 (0.37) | |||||||||||||||
| Shared associations with both gambling and substance use | ||||||||||||||||||
| Sex | 1.65 (0.13) | 1.58 (0.13) | 0.102 (0.030) | 0.21 (0.08) | 0.13 (0.03) | 12.26 (4.36) | 10.17 (1.81) | 20.65 (4.16) | 9.50 (4.12) | 6.77 (1.82) | 0.26 (0.07) | 0.17 (0.03) | 6.28 (2.32) | |||||
| Race/Ethnicity | 0.29 (0.14) | 0.09 (0.03) | 0.160 (0.078) | ns | 19.97 (4.55) | 15.63 (4.24) | 1.80 (0.89) | ns | 0.030 (0.015) | ns | ||||||||
| Behavioral Dysregulation | 0.014 (0.005) | 0.017 (0.005) | 0.0011 (0.0005) | 0.084 (0.036) | −0.43 (0.19) | 0.056 (0.026) | −0.010 (0.003) | 0.0014 (0.0006) | 0.052 (0.028) | |||||||||
| Sensation-seeking | 0.076 (0.029) | 0.040 (0.008) | 0.072 (0.017) | 0.065 (0.017) | 0.0061 (0.0027) | 4.52 (0.97) | 3.95 (0.96) | 0.47 (0.20) | 2.84 (0.98) | 2.58 (1.03) | 0.31 (0.14) | 0.11 (0.02) | 0.11 (0.02) | 0.008 (0.003) | 7.10 (1.36) | 6.53 (1.38) | ns | |
Note. AUD=Alcohol Use Disorder. All results shown were statistically significant (p<.05). Non-significant pathways that were omitted during the model fitting process are represented by empty cells. Race/ethnicity was parameterized as minority vs. non-Hispanic White.
Five additional independent variables that were tested and found to be non-significant in both models were omitted from this table (mother’s education, mother’s and father’s drug problems, affective dysregulation, cognitive dysregulation), as was father’s education, for which only one hypothesized path was significant (to gambling, Model B only).
Athletics involvement had independent contributions to gambling, alcohol use frequency, and AUD risk, as evidenced by significant direct paths that were not attenuated by the inclusion of indirect paths. For example, athletics involvement had significant direct effects on gambling in both models (b=.50, SE=.14 and b=.47, SE=.14, respectively), but its indirect effect on gambling via substance use was much smaller (b=.062, SE=.025). Similarly, its direct effect on AUD risk (b=.23, SE=.08 in both models) was unchanged regardless of the modest indirect effect via gambling (b=.040, SE=.014), and the pattern was similar for alcohol use frequency. By contrast, the effects of athletics involvement on tobacco and marijuana use frequency, and number of other drugs used were entirely accounted for by gambling.
3.4. Risk factors accounting for “shared” variance in gambling and substance use
Four of the hypothesized risk factors we tested (i.e., sex, race/ethnicity, sensation-seeking, behavioral dysregulation) exhibited direct associations with both gambling and substance use that were accounted for, partially or completely, by each other, respectively. For example, male sex was directly associated with gambling in both models (b=1.65, SE=.13, and b=1.58, SE=.13, respectively), and had an additional indirect effect on gambling via alcohol use frequency and number of other drugs used (b=.10, SE=.03). Although male sex was also directly and independently associated with each of the substance use variables, these effects were all partially (for marijuana use frequency) or completely (for AUD risk, alcohol use frequency, number of other drugs used) attenuated in the model that included the indirect effect of sex via gambling. The sole exception to this pattern was tobacco use frequency, for which sex had an indirect effect via gambling (b=6.28, SE=2.32) but no direct effects in either model.
With respect to race/ethnicity, being White was associated with both more frequent alcohol use and more frequent gambling. The direct effect of race/ethnicity on gambling (b=.29, SE=.14) was completely attenuated by the inclusion of its indirect effect via alcohol and drug use (b=.09, SE=.03), whereas its direct effect on alcohol frequency (b=19.97, SE=4.55) was only slightly attenuated (b=15.63, SE=4.24) by the inclusion of the indirect effect through gambling (b=1.80, SE=.89). The effects of race/ethnicity on the other four substance variables (i.e., AUD risk, marijuana use frequency, tobacco use frequency, number of other drugs used) were all either absent or entirely accounted for by gambling.
Sensation-seeking was directly associated with every substance use variable in both models, and had additional indirect effects in the model in which gambling was an intermediary variable. However, the direct effect of sensation-seeking on gambling (b=.076, SE=.029) was completely attenuated by including its indirect path via alcohol use frequency and number of other drugs (b=.040, SE=.008).
The direct effect of behavioral dysregulation on more frequent gambling was significant in both models (b=.014, SE=.005 and b=.017, SE=.005, respectively) but did not flow through substance use (as evidenced by the absence of any significant indirect effect in the model where gambling was the outcome). Conversely, for three of the substance use outcomes (AUD risk, alcohol use frequency, tobacco use frequency), the influence of behavioral dysregulation was solely indirect via gambling (b=.0011, SE=.0005; b=.084, SE=.036; and b=.052, SE=.028, respectively), and no direct effects were observed. Behavioral dysregulation exhibited similar indirect effects (via gambling) on marijuana use frequency (b=.056, SE=.026) and number of other drugs used (b=.0014, SE=.0006); unexpectedly, however, these indirect effects were outweighed by predominant direct effects in the opposite direction (b=−.43, SE=.19 and b=−.01, SE=.003, respectively), such that the total effect of behavioral dysregulation on both marijuana (b=−.37, SE=.19) and other drug use (b=−.0083, SE=.0033) was protective (total effects not shown in a table).
3.5. Risk factors associated with substance use but not gambling
Six of the hypothesized risk factors we tested were significantly associated with one or more of the substance use variables, but had no significant direct or indirect effects on gambling in either model: childhood conduct problems, anxiety symptoms, mother’s and father’s mental health problems, and mother’s and father’s alcohol problems. Childhood conduct problems were directly associated with higher AUD risk, more marijuana use, and a greater number of other drugs used, but not with alcohol or tobacco frequency. Anxiety symptoms were directly associated with a greater number of other drugs used, but not with any of the other substance use outcomes. Mental health problems in either parent were directly associated with more marijuana and other drug use, and maternal (but not paternal) mental health problems with more frequent tobacco use. Both paternal and maternal alcohol problems were directly associated with more frequent tobacco use.
Unexpectedly, two of the hypothesized risk factors we tested functioned as protective factors. First, mother’s alcohol problems were directly associated with less frequent marijuana use, despite functioning simultaneously as a risk factor for tobacco use (see above). Second, depressive symptoms were directly associated with less frequent alcohol use and did not function as risk factor for any of the outcomes we tested.
4. Discussion
4.1. Gambling
Past-year gambling was fairly common among this sample of recent college students (60%), with casino gambling being the most prevalent gambling activity (35%). Because participants were followed up even after they left the home university, it is impossible to say what each individual’s proximity to a casino might have been during Year 5; however, to the extent that students were likely to have remained nearby, it might be useful to note that the nearest casinos were located approximately 2 hours’ drive from the university. The finding that 6% of the sample gambled on a weekly basis or more is comparable with prior research (LaBrie et al., 2003).
Consistent with the literature, individuals who gambled were more likely to be male, athletes, and involved with a Greek organization during college (Barnes et al., 2010; LaBrie et al., 2003; Stuhldreher et al., 2007). Not surprisingly, gambling behavior was more frequent at higher levels of behavioral dysregulation. An important contribution of this study is the finding that a reasonably large proportion of the variance in gambling frequency (R2=.26) could be accounted for by a relatively small number of risk factors. Aside from sex and race differences, the main predictors of gambling were behavioral dysregulation and college involvement variables (i.e., athletics, fraternity/sorority), with an additional contribution from sensation-seeking that flowed through more frequent drinking and number of other drugs used.
4.2. Gambling and substance use
Findings underscore the interrelatedness of gambling and substance use—independent of the effects of their shared risk factors. Longitudinal studies are needed to determine the direction of this relationship and evaluate whether, for example, involvement in either substance use or gambling might contribute to the escalation of the other. Moreover, given the large number of risk factors that were evaluated, it is apparent that gambling and substance use among this sample were partially but not entirely attributable to a shared propensity for risky behaviors. Rather than finding a preponderance of indirect effects of the risk factors through the hypothesized intermediary variables to the more distal outcome (i.e., through gambling to substance use, or through substance use to gambling), in both models, we observed a large number of significant direct pathways between the risk factors and the more distal outcome variable(s).
4.3. Risk factors
Of the 19 hypothesized risk factors we tested, five (mother’s education, mother’s and father’s drug problems, affective dysregulation, cognitive dysregulation) did not significantly predict any of the gambling or substance use variables, either directly or indirectly, in the context of our two alternative models. This result contradicts prior findings that negative affect is associated with gambling (Atkinson et al., 2012) and parental substance use is predictive of substance use in offspring (Biederman et al., 2000). The fact that our measure of parent substance use problems was very simple and self-reported by the young adult could account for this discrepancy. In contrast, other risk factors had direct associations exclusively with either substance use or gambling. Specifically, six risk factors (childhood conduct problems, anxiety symptoms, mother’s and father’s mental health problems, mother’s and father’s alcohol problems) were directly associated with one or more substance use variables but not with gambling. A possible explanation for the parental factors might be that certain environmental factors, such as family influence, predict substance use but not problem gambling (Vitaro et al., 2001; Vitaro et al., 2014). On the other hand, behavioral dysregulation was the sole variable that was directly associated with gambling but none of the substance use variables. Still other risk factors had significant direct effects on both gambling and substance use—namely, Greek affiliation contributed directly to gambling and alcohol use frequency, and athletics involvement contributed directly to gambling, alcohol use frequency, and AUD risk. Taken together, these findings clarify previous literature (Engwall et al., 2004; LaBrie et al., 2003; Stuhldreher et al., 2007; Weiss, 2010) by suggesting that involvement in Greek life and/or athletics might contribute independently to both more frequent gambling and greater alcohol involvement via mechanisms that are largely separate.
With respect to indirect effects, none of the risk factors we tested were indirectly associated with gambling via substance use, unless they were also indirectly associated with one or more substance use variables via gambling. We identified five such variables (Greek involvement, athletics involvement, sex, sensation-seeking, race/ethnicity) that had significant indirect associations with both gambling and one or more substance use variables. On the other hand, one risk factor (behavioral dysregulation) had significant indirect effects on substance use via its influence on gambling, but had no corresponding indirect effect on gambling via substance use. Overall, given how few variables were exclusively associated with gambling either directly or indirectly, the present findings illustrate the preponderance of overlap between the risk factors for gambling with those for substance use.
In general, the results expand our understanding of the independent and overlapping relationships of several risk factors with substance use and gambling. Results support the notion that the association between gambling and substance use is partially attributable to shared variance in certain risk factors (sex, race/ethnicity, sensation-seeking, behavioral dysregulation). Still other risk factors (childhood conduct problems, anxiety, family history) exhibited more specificity in relation to substance use, in that they were not independently associated with gambling after accounting for all the other effects in our models. Interestingly, both of the extracurricular involvement variables (Greek, athletics) accounted for distinct, non-overlapping variance in both gambling and alcohol-related variables—suggesting the possible existence of separate underlying mechanisms—in addition to some shared variance between gambling and less prevalent types of substance use behavior.
4.4. Limitations
The study is limited by the cross-sectional nature of the relationships between the gambling and substance use variables. Also, we did not account for possible changes in risk factors during college. Future research analyzing such relationships prospectively is needed to understand any underlying temporality, such as whether or not gambling behaviors might play a role in the persistence of substance use during the post-college period. To aid in the identification of treatment targets, future studies could focus on assessing underlying processes such as delay discounting, which has been shown in prior studies to be related to problem gambling (Steward et al., 2017). Moreover, our sample size was not sufficient to assess the differential associations between separate gambling activities and substance use. Findings might not be comparable with other studies of college students, as the majority of the subjects in this study had graduated from college at the time of follow-up. Given that students were sampled from a single university, results might not be generalizable to students attending other types of institutions (e.g., small private colleges). Despite the large number of risk factors assessed, data were not available on some potentially important variables found to be significant in prior studies, such as parents’ history of gambling problems or competitive personality (Burger et al., 2006; King et al., 2010; Weinstock et al., 2008; Wickwire et al., 2008; Winters et al., 1998). Given the slight underrepresentation of men in our analytic sample, coupled with the finding that men gambled more frequently than women, it is likely that our results might have underestimated the extent of gambling in the target population.
4.5. Implications
The observed interrelationships between gambling, substance use, and risk factors that are common to both extend prior literature showing that gambling and substance use tend to co-occur, and therefore could be addressed simultaneously in prevention activities aimed at reducing young adults’ involvement in high-risk activities. Given that college environments create a relatively captive audience for screening and intervention in emerging adulthood, it might be worthwhile for colleges to be vigilant about the relationship between gambling and excessive drinking and to identify and intervene with students at risk for one or both issues.
On the other hand, the observed specificity of several risk factors as predictors of substance use but not gambling (i.e., childhood conduct problems, anxiety symptoms, family history) highlights the possibility that gambling is not necessarily equivalent to a generalized “problem behavior” profile. To the extent that such distinctions might reflect meaningful differences in the etiology of gambling vis a vis substance use, they likely translate to important differences in both prevention and intervention approaches. For example, the observed absence of any relationship of parental problems (alcohol, mental health) with gambling in the context of our models suggests that family-based approaches for intervening with high-risk youth might not be effective for reducing students’ gambling, even though they appear to be promising for substance use (Abar et al., 2014; Brooks-Russell et al., 2015; Dishion et al., 2003). A possible explanation is that parents view substance use as a greater problem than gambling (Campbell et al., 2011) and might be more permissive of gambling behavior than of substance use.
Considering that commercial gambling venues (e.g., casinos, racetracks) might provide opportunities for excessive drinking, research should focus on the potential impact of expanding such venues, especially in communities near college campuses. Moreover, outside of commercial gambling establishments, research is needed to understand how the social nature of some private gambling activities (e.g., poker nights) might promote concomitant excessive drinking and drug use among college students. The present findings highlight the need for researchers to account for a variety of risk factors simultaneously to more fully understand the development of gambling problems and substance use.
Acknowledgments
Funding for this study was provided by the National Institute on Drug Abuse (R01DA14845, Dr. Arria, PI) and the Maryland Department of Health and Mental Hygiene via the Maryland Center of Excellence on Problem Gambling. Neither the National Institute on Drug Abuse nor the Maryland Department of Health and Mental Hygiene had any further role in the study design; in the collection, management, analysis, and interpretation of the data; in the writing of the manuscript; or in the decision to submit the paper for publication.
References
- Abar CC, Turrisi R, Mallett KA. Differential trajectories of alcohol-related behaviors across the first year of college by parenting profiles. Psychol Addict Behav. 2014;28:53–61. doi: 10.1037/a0032731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV. American Psychiatric Press; Washington, DC: 1994. [Google Scholar]
- Arria AM, Caldeira KM, O′Grady KE, Vincent KB, Fitzelle DB, Johnson EP, Wish ED. Drug exposure opportunities and use patterns among college students: Results of a longitudinal prospective cohort study. Subst Abus. 2008;29:19–38. doi: 10.1080/08897070802418451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Vincent KB, Winick ER, Baron RA, O’Grady KE. Discontinuous college enrollment: Associations with substance use and mental health. Psychiatr Serv. 2013a;64:165–172. doi: 10.1176/appi.ps.201200106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Garnier-Dykstra LM, Caldeira KM, Vincent KB, Winick ER, O’Grady KE. Drug use patterns and continuous enrollment in college: Results from a longitudinal study. J Stud Alcohol Drugs. 2013b;74:71–83. doi: 10.15288/jsad.2013.74.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Garnier-Dykstra LM, Cook ET, Caldeira KM, Vincent KB, Baron RA, O’Grady KE. Drug use patterns in young adulthood and post-college employment. Drug Alcohol Depend. 2013c;127:23–30. doi: 10.1016/j.drugalcdep.2012.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Wilcox HC, Caldeira KM, Vincent KB, Garnier-Dykstra LM, O’Grady KE. Dispelling the myth of “smart drugs”: Cannabis and alcohol use problems predict nonmedical use of prescription stimulants for studying. Addict Behav. 2013d;38:1643–1650. doi: 10.1016/j.addbeh.2012.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Vincent KB, Bugbee BA, O′Grady KE. False identification use among college students increases the risk of alcohol use disorder: Results of a longitudinal study. Alcohol Clin Exp Res. 2014;38:834–843. doi: 10.1111/acer.12261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Bugbee BA, Vincent KB, O′Grady KE. The academic consequences of marijuana use during college. Psychol Addict Behav. 2015;29:564–575. doi: 10.1037/adb0000108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Bugbee BA, Vincent KB, O′Grady KE. Energy drink use patterns among young adults: Associations with drunk driving. Alcohol Clin Exp Res. 2016;40:2456–2466. doi: 10.1111/acer.13229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Atkinson J, Sharp C, Schmitz J, Yaroslavsky I. Behavioral activation and inhibition, negative affect, and gambling severity in a sample of young adult college students. J Gambl Stud. 2012;28:437–449. doi: 10.1007/s10899-011-9273-x. [DOI] [PubMed] [Google Scholar]
- Barnes GM, Welte JW, Hoffman JH, Dintcheff BA. Gambling and alcohol use among youth: Influences of demographic, socialization, and individual factors. Addict Behav. 1999;24(99):749–767. 00048–9. doi: 10.1016/S0306-4603. [DOI] [PubMed] [Google Scholar]
- Barnes GM, Welte JW, Hoffman JH, Tidwell MCO. Comparisons of gambling and alcohol use among college students and noncollege young people in the United States. J Am Coll Health. 2010;58:443–452. doi: 10.1080/07448480903540499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive therapy of depression. The Guilford Press; New York, NY: 1979. [Google Scholar]
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: Psychometric properties. J Consult Clin Psychol. 1988;56:893–897. doi: 10.1037//0022-006X.56.6.893. [DOI] [PubMed] [Google Scholar]
- Bhullar N, Simons L, Joshi K. The significance of gender and ethnicity in collegiate gambling and drinking. Addict Disord Their Treat. 2012a;11:154–164. doi: 10.1097/ADT.0b013e31822f9ca9. [DOI] [Google Scholar]
- Bhullar N, Simons L, Joshi K, Amoroso K. The relationship among drinking games, binge drinking and gambling activities in college students. J Alcohol Drug Educ. 2012b;56:58–84. [Google Scholar]
- Biederman J, Faraone SV, Monuteaux MC, Feighner JA. Patterns of alcohol and drug use in adolescents can be predicted by parental substance use disorders. Pediatrics. 2000;106:792–797. doi: 10.1542/peds.106.4.792. [DOI] [PubMed] [Google Scholar]
- Brooks-Russell A, Conway KP, Liu D, Xie Y, Vullo GC, Li K, Iannotti RJ, Compton W, Simons-Morton B. Dynamic patterns of adolescent substance use: Results from a nationally representative sample of high school students. J Stud Alcohol Drugs. 2015;76:962–970. doi: 10.15288/jsad.2015.76.962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burger TD, Dahlgren D, MacDonald CD. College students and gambling: An examination of gender differences in motivation for participation. Coll Stud J. 2006;40:704–714. [Google Scholar]
- Campbell C, Derevensky J, Meerkamper E, Cutajar J. Parents’ perceptions of adolescent gambling: A Canadian national study. Journal of Gambling Issues. 2011:36–53. doi: 10.4309/jgi.2011.25.4. [DOI] [Google Scholar]
- Cook S, Turner NE, Ballon B, Paglia-Boak A, Murray R, Adlaf EM, Ilie G, den Dunnen W, Mann RE. Problem gambling among Ontario students: Associations with substance abuse, mental health problems, suicide attempts, and delinquent behaviours. J Gambl Stud. 2015;31:1121–1134. doi: 10.1007/s10899-014-9483-0. [DOI] [PubMed] [Google Scholar]
- Dishion TJ, Nelson SE, Kavanagh K. The family check-up with high-risk young adolescents: Preventing early-onset substance use by parent monitoring. Behav Ther. 2003;34:553–571. doi: 10.1016/S0005-7894(03)80035-7. [DOI] [Google Scholar]
- Ellenbogen S, Jacobs D, Derevensky J, Gupta R, Paskus T. Gambling behavior among college student-athletes. J Appl Sports Psychol. 2008;20:349–362. doi: 10.1080/10413200802056685. [DOI] [Google Scholar]
- Engwall D, Hunter R, Steinberg M. Gambling and other risk behaviors on university campuses. J Am Coll Health. 2004;52:245–255. doi: 10.3200/JACH.52.6.245-256. [DOI] [PubMed] [Google Scholar]
- Falls BJ, Wish ED, Garnier LM, Caldeira KM, O’Grady KE, Vincent KB, Arria AM. The association between early conduct problems and early marijuana use in college students. J Child Adolesc Subst Abuse. 2011;20:221–236. doi: 10.1080/1067828X.2011.581900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garnier LM, Arria AM, Caldeira KM, Vincent KB, O′Grady KE, Wish ED. Sharing and selling of prescription medications in a college student sample. J Clin Psychiatry. 2010;71:262–269. doi: 10.4088/JCP.09m05189ecr. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goudriaan AE, Slutske WS, Krull JL, Sher KJ. Longitudinal patterns of gambling activities and associated risk factors in college students. Addiction. 2009;104:1219–1232. doi: 10.1111/j.1360-0443.2009.02573.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6:1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- Huang JH, Jacobs DF, Derevensky JL. DSM-based problem gambling: Increasing the odds of heavy drinking in a national sample of U.S. college athletes? J Psychiatr Res. 2011;45:302–308. doi: 10.1016/j.jpsychires.2010.07.001. [DOI] [PubMed] [Google Scholar]
- Johnson EO, Arria AM, Borges G, Ialongo N, Anthony JC. The growth of conduct problem behaviors from middle childhood to early adolescence: Sex differences and the suspected influence of early alcohol use. J Stud Alcohol. 1995;56:661–671. doi: 10.15288/jsa.1995.56.661. [DOI] [PubMed] [Google Scholar]
- King SM, Abrams K, Wilkinson T. Personality, Gender, and Family History in the Prediction of College Gambling. J Gambl Stud. 2010;26:347–359. doi: 10.1007/s10899-009-9163-7. [DOI] [PubMed] [Google Scholar]
- Kline RB. The meditation myth. Basic and Applied Social Psychology. 2015;37:202–213. doi: 10.1080/01973533.2015.1049349. [DOI] [Google Scholar]
- LaBrie RA, Shaffer HJ, LaPlante DA, Wechsler H. Correlates of college student gambling in the United States. J Am Coll Health. 2003;52:53–62. doi: 10.1080/07448480309595725. [DOI] [PubMed] [Google Scholar]
- Leeman RF, Hoff RA, Krishnan-Sarin S, Patock-Peckham JA, Potenza MN. Impulsivity, sensation-seeking, and part-time job status in relation to substance use and gambling in adolescents. J Adolesc Health. 2014;54:460–466. doi: 10.1016/j.jadohealth.2013.09.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lesieur HR, Blume SB. The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. Am J Psychiatry. 1987;144:1184–1188. doi: 10.1176/ajp.144.9.1184. [DOI] [PubMed] [Google Scholar]
- Lynch WJ, Maciejewski PK, Potenza MN. Psychiatric correlates of gambling in adolescents and young adults grouped by age at gambling onset. Arch Gen Psychiatry. 2004;61:1116–1122. doi: 10.1001/archpsyc.61.11.1116. [DOI] [PubMed] [Google Scholar]
- Mann RE, Sobell LC, Sobell MB, Pavan D. Reliability of a family tree questionnaire for assessing family history of alcohol problems. Drug Alcohol Depend. 1985;15(85):61–67. 90030–4. doi: 10.1016/0376-8716. [DOI] [PubMed] [Google Scholar]
- Martens MP, Rocha TL, Cimini MD, Diaz-Myers A, Rivero EM, Wulfert E. The co-occurrence of alcohol use and gambling activities in first-year college students. J Am Coll Health. 2009;57:597–602. doi: 10.3200/JACH.57.6.597-602. [DOI] [PubMed] [Google Scholar]
- Martin RJ, Usdan S, Turner L. Three-month study of college student disordered gambling using the Transtheoretical Model: Findings and lessons learned. Coll Stud J. 2012;46:764–775. [Google Scholar]
- Martin RJ, Usdan S, Cremeens J, Vail-Smith K. Disordered gambling and co-morbidity of psychiatric disorders among college students: An examination of problem drinking, anxiety and depression. J Gambl Stud. 2014;30:321–333. doi: 10.1007/s10899-013-9367-8. [DOI] [PubMed] [Google Scholar]
- Mezzich AC, Tarter RE, Giancola PR, Kirisci L. The dysregulation inventory: A new scale to assess the risk for substance use disorder. J Child Adolesc Subst Abuse. 2001;10:35–43. doi: 10.1300/J029v10n04_04. [DOI] [Google Scholar]
- O′Grady KE, Arria AM, Caldeira KM, Wish ED. Alcohol abuse and dependence in college students: Associations with depression, anxiety, and behavioral dysregulation. Research Society on Alcoholism; Baltimore, MD: 2006. [Google Scholar]
- Pilver CE, Libby DJ, Hoff RA, Potenza MN. Gender differences in the relationship between gambling problems and the incidence of substance-use disorders in a nationally representative population sample. Drug Alcohol Depend. 2013;133:204–211. doi: 10.1016/j.drugalcdep.2013.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seifried C, Krenzelok A, Turner BA, Brett M. The prevalence of gambling in college: A review of literature, convenience sample, and recommendations. ICHPER-SD J Res. 2009;4:13–20. [Google Scholar]
- Slutske WS, Eisen S, True WR, Lyons MJ, Goldberg J, Tsuang M. Common genetic vulnerability for pathological gambling and alcohol dependence in men. Arch Gen Psychiatry. 2000;57:666–673. doi: 10.1001/archpsyc.57.7.666. doi:10-1001/pubs.Arch. Gen Psychiatry-ISSN-0003-990x-57-7-yoa9396. [DOI] [PubMed] [Google Scholar]
- Slutske WS, Ellingson JM, Richmond-Rakerd LS, Zhu G, Martin NG. Shared genetic vulnerability for disordered gambling and alcohol use disorder in men and women: Evidence from a national community-based Australian twin study. Twin Res Hum Genet. 2013;16:525–534. doi: 10.1017/thg.2013.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steward T, Mestre-Bach G, Fernandez-Aranda F, Granero R, Perales JC, Navas JF, Soriano-Mas C, Bano M, Fernandez-Formoso JA, Martin-Romera V, Menchon JM, Jimenez-Murcia S. Delay discounting and impulsivity traits in young and older gambling disorder patients. Addict Behav. 2017;71:96–103. doi: 10.1016/j.addbeh.2017.03.001. [DOI] [PubMed] [Google Scholar]
- Stuhldreher WL, Stuhldreher TJ, Forrest KYZ. Gambling as an emerging health problem on campus. J Am Coll Health. 2007;56:75–88. doi: 10.3200/JACH.56.1.75-88. [DOI] [PubMed] [Google Scholar]
- National Survey on Drug Use and Health Questionnaire. Rockville, MD: Office of Applied Studies; Substance Abuse and Mental Health Services Administration 2003–2002. [Google Scholar]
- Vincent KB, Kasperski SJ, Caldeira KM, Garnier-Dykstra LM, Pinchevsky GM, O’Grady KE, Arria AM. Maintaining superior follow-up rates in a longitudinal study: Experiences from the College Life Study. Int J Mult Res Approach. 2012;6:56–72. doi: 10.5172/mra.2012.6.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vitaro F, Brendgen M, Ladouceur R, Tremblay RE. Gambling, delinquency, and drug use during adolescence: Mutual influences and common risk factors. J Gambl Stud. 2001;17:171–190. doi: 10.1023/a:1012201221601. [DOI] [PubMed] [Google Scholar]
- Vitaro F, Hartl AC, Brendgen M, Laursen B, Dionne G, Boivin M. Genetic and environmental influences on gambling and substance use in early adolescence. Behav Genet. 2014;44:347–355. doi: 10.1007/s10519-014-9658-6. [DOI] [PubMed] [Google Scholar]
- Weinstock J, Whelan JP, Meyers A. College students' gambling behavior: When does it become harmful? J Am Coll Health. 2008;56:513–522. doi: 10.3200/JACH.56.5.513-522. [DOI] [PubMed] [Google Scholar]
- Weiss S. Cross-addiction on campus: More problems for student-athletes. Subst Use Misuse. 2010;45:1525–1541. doi: 10.3109/10826081003682297. [DOI] [PubMed] [Google Scholar]
- Welte JW, Barnes GM, Tidwell MC, Hoffman JH. The prevalence of problem gambling among U.S. adolescents and young adults: Results from a national survey. J Gambl Stud. 2008;24:119–133. doi: 10.1007/s10899-007-9086-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wickwire EM, Jr, Whelan JP, West R, Meyers A, McCausland C, Leullen J. Perceived availability, risks, and benefits of gambling among college students. J Gambl Stud. 2007;23:395–408. doi: 10.1007/s10899-007-9057-5. [DOI] [PubMed] [Google Scholar]
- Wickwire EM, Jr, McCausland C, Whelan JP, Luellen J, Meyers AW, Studaway A. Environmental correlates of gambling behavior among college students: A partial application of problem behavior theory to gambling. J Coll Stud Dev. 2008;49:459–475. doi: 10.1353/csd.0.0030. [DOI] [Google Scholar]
- Winters KC, Stinchfield RD, Fulkerson J. Toward the development of an adolescent gambling problem severity scale. J Gambl Stud. 1993;9:63–84. doi: 10.1007/BF01019925. [DOI] [Google Scholar]
- Winters KC, Bengston P, Dorr D, Stinchfield R. Prevalence and risk factors of problem gambling among college students. Psychol Addict Behav. 1998;12:127–135. doi: 10.1037/0893-164X.12.2.127. [DOI] [Google Scholar]
- Zuckerman M. Zuckerman-Kuhlman Personality Questionnaire (ZKPQ): An alternative five-factorial model. In: de Raad B, Perugini M, editors. Big Five Assessment. Hogrefe & Huber; Seattle, WA: 2002. pp. 377–396. [Google Scholar]