

Abstract
Background
Pancreatic cancer is a biologically aggressive disease with less than 20% of patients suitable for a "curative" surgical resection. This, combined with the poor 5-year survival indicates that effective palliative methods for symptom relief are required. Currently there are no ablative techniques to treat pancreatic cancer in clinical use. Tissue electrolysis is the delivery of a direct current between an anode and cathode to induce localised necrosis. Electrolysis has been shown to be safe and reliable in producing hepatic tissue and tumour ablation in animal models and in a limited number of patients. This study investigates the feasibility of using electrolysis to produce localised pancreatic necrosis in a healthy rat model.
Method
Ten rats were studied in total. Eight rats were treated with variable "doses" of coulombs, and the systemic and local effects were assessed; 2 rats were used as controls.
Results
Seven rats tolerated the procedure well without morbidity or mortality, and one died immediately post procedure. One control rat died on induction of anaesthesia. Serum amylase and glucose were not significantly affected.
Conclusion
Electrolysis in the rat pancreas produced localised necrosis and appears both safe, and reproducible. This novel technique could offer significant advantages for patients with unresectable pancreatic tumours. The next stage of the study is to assess pancreatic electrolysis in a pig model, prior to human pilot studies.
Introduction
Pancreatic cancer is biologically aggressive and the majority of patients present with advanced disease. Radical surgical resection of the pancreas offers the only hope of cure but only 20% of tumours in the head and 3% of tumours elsewhere in the pancreas are suitable for curative resection [1-3]. Many other patients undergo a trial dissection before a palliative surgical procedure is carried out. Locally advanced tumours that involve major blood vessels and metastatic disease are the most common factors that preclude curative resection. Therefore, the mainstay of treatment at present is palliative, directed towards relieving obstructive jaundice, gastric outlet obstruction and pain.
Electrolysis is a simple technique using a direct current passed through a conductive medium between a pair of electrodes, measured in Coulombs (1 Coulomb = 1 ampere × 1 second).Tissue electrolysis produces chemicals at the electrodes [4-6] and the ensuing pH change causes a localised parenchymal necrosis [7]. During the past few years, electrolysis of liver tumours has been extensively investigated at this institution [8-12]. Not only has the process been shown to completely ablate liver tumours in animal models [11] and in humans [13]. It is also safe and predictable in terms of both its inherent tissue destruction and the inability to thrombose or breach large blood vessels in close proximity to the electrolysis [12]. Electrolytic ablation of pancreatic tumours is an entirely novel idea, both for the treatment of pancreatic cancer and for the use of electrolysis. The aim of this study was to assess whether electrolysis of the pancreas gland could be performed in a safe and reproducible manner.
Method
The experiment was approved by the ethics committees of the University of Adelaide and The Queen Elizabeth Hospital. The Direct Current (DC) generator (Bioengineering, Transducers and Signal Processing Research Group, University of Leicester, United Kingdom) was designed to deliver a preset dose of Coulombs, using a continuous current (8 mA) at a variable voltage depending on resistance of the tissue, in accordance with Ohms law (V = IR). The anode and cathode were made from fine platinum wires 0.5 mm in diameter. These were insulated from each other at the proximal end by a semi-rigid plastic sleeve.
Ten SPF female Sprague-Dawley rats were fasted overnight. They were weighed pre-procedure, and anaesthetised using a standard mixture of halothane, nitrous oxide and oxygen. The rats were induced in a perspex box with 3.5% halothane, 1 L/min nitrous oxide and 1 L/min oxygen. Maintenance of anaesthesia was achieved with an inhalation system using 1.5% halothane, 0.5 L/min of nitrous oxide and 0.3 L/min oxygen.
The pancreas was exposed through a midline laparotomy. Swabs were placed around the pancreas to protect the surrounding organs. Two platinum electrodes designated anode and cathode, were inserted into the pancreas at a depth of 2 mm and a separation of 1 mm. A variable dose of Coulombs was delivered, ranging from 0 to 10 Coulombs (Table 1). The control rat underwent the same procedure, but without the delivery of current. Serial blood samples were obtained from the tail vein, pre-operatively then at 1, 4, 24 and 48 hours post-operatively and analysed for amylase and glucose. All rats were sacrificed at 72 hours, weighed and the pancreata removed. This tissue was then fixed in 10% buffered formalin for a minimum of 2 weeks to allow for sufficient fixation. The area of pancreas that had been electrolytically treated was then embedded in paraffin, sectioned and stained with haematoxylin and eosin for histological examination. Electrolytic lesions were graded by a histopathologist who was unaware of the Coulombs administered. The lesions were graded according to the scoring system described by Spormann et al [14], to obtain a comparable histological score (Table 2).
Table 1.
Dose of Coulombs delivered to rats
| Dose Of Coulombs | Number Of Rats | Deaths |
| (mA/sec) | ||
| 0 (control) | 2 | 1+ |
| 2 | 1 | |
| 4 | 1 | |
| 6 | 2 | |
| 8 | 2 | |
| 10 | 2 | 1* |
+ During anaesthetic induction * Under anaesthetic on completion of electrolysis
Table 2.
Histological scoring of pancreatitis
| Oedema |
| 1 = Mild |
| 2 = Moderate |
| 3 = Severe |
| Inflammatory Infiltrate |
| 1 = Mild |
| 2 = Moderate |
| 3 = Severe |
| Fat Necrosis |
| 3 = Mild |
| 5 = Moderate |
| 7 = Severe |
| Parenchymal Necrosis |
| 3 = Singular |
| 5 = Sub lobular <1/3 |
| 7 = Lobular >1/3 |
| Haemorrhage |
| 3 = Mild |
| 5 = Moderate |
| 7 = Severe |
Ref:Spormann Pathol Res Pract 1989 184: 507–13
Results
Median pre-procedure weight of the rats was 250 gm, (range 242–257 gm). There was no weight loss in any of the rats prior to tissue harvesting.
Of the 2 control rats, one animal died on induction of anaesthetic before any procedure had been performed, and the other tolerated the laparotomy and sham procedure without any side effects. In the treatment group, eight rats received between 2 to 10 Coulombs. One rat died immediately post electrolysis whilst under general anaesthetic. Seven rats survived with no morbidity or mortality. All eight animals that survived appeared clinically well, and were all eating and drinking within 2 hours of the procedure. On dissection of the pancreas gland an area of necrosis was evident on all the treated organs.
Blood results
The control group showed no significant change in amylase concentration (Figure 1). The treatment group revealed a transient hyperamylasaemia, peaking at approximately 4 hours which was not dose related and was not statistically significant.
Figure 1.
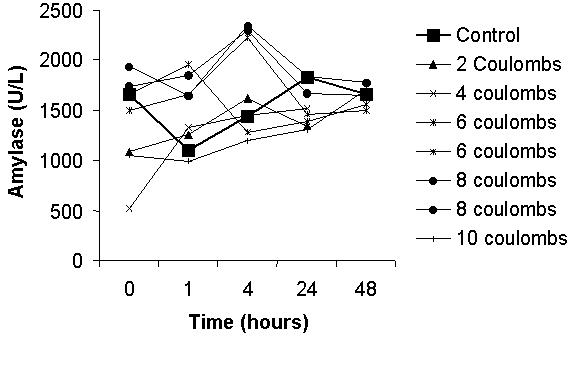
Serum amylase plotted against time (in hours)
Glucose levels were essentially unchanged in the control and treatment rats over the period of investigation (Figure 2).
Figure 2.
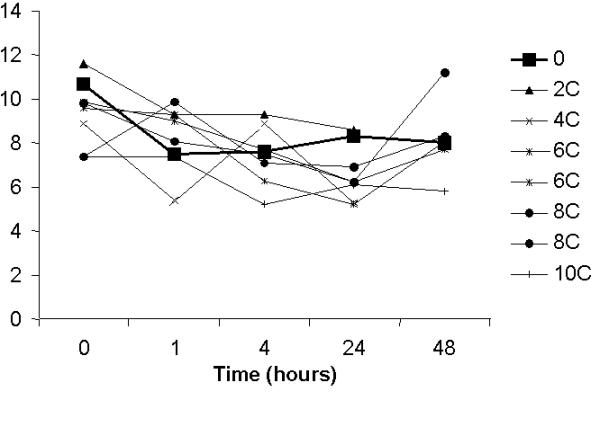
Serum glucose levels plotted against time (in hours)
Histology
On harvesting, a localised necrotic electrolytic lesion was macroscopically visible in all specimens of the pancreas (Figure 3), with no evidence of bowel perforations, fluid collections or haemorrhage. The necrotic lesion itself was difficult to measure due to the mucinous nature of the rat pancreas gland. The ablated region was surrounded by discoloured pancreatic tissue. There was a small area of inflammation (brown in colour) around the necrotic region, which was graded using the histological score, this was not proportional to the electrolytic dose (Figure 4). The inflammation did not extend through the pancreas.
Figure 3.

Pancreas after harvest showing electrolytic lesion
Figure 4.
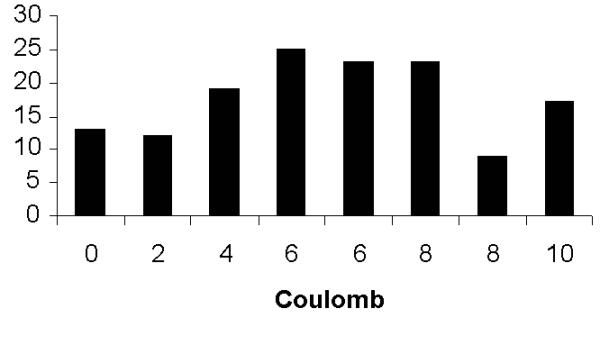
Histological grading graph.
Discussion
Pancreatic carcinoma has a poor prognosis, and involvement of major blood vessels and metastatic disease are the most common factors that preclude curative resection [1,15]. Therefore, the mainstay of treatment at present is palliative, and there has been little advancement in new palliative treatments in the last few decades. Symptoms requiring palliation include anorexia, nausea, vomiting, weight loss and epigastric and back pain [15,16]. Nausea and vomiting are due to mechanical and functional impairment of gastric and duodenal emptying. Pain results from malignant involvement of the splanchnic plexus, or from obstruction to the pancreatic duct. Biliary obstruction may cause jaundice often associated with intractable pruritus. Most symptoms are progressive and reflect locally advanced disease at presentation. A proportion of patients undergo attempted resection but at the time of operation the presence of local and/or distant disease, and invasion of the major vessels, prevents any surgical resection, and palliation is resorted to. Surgical palliation consists of biliary, and or gastric bypass,and an increasing number of patients are undergoing this form of treatment [17]. Palliation is also possible by endoscopic stenting of the obstructed common bile duct [18]. The ideal palliation would include the relief of pain, jaundice and gastro-duodenal obstruction, to improve quality of life measures with minimum morbidity. Local tumour destruction by electrolysis may not affect the overall tumour biology but may ameliorate the mass effect of the tumour, decrease tumour burden and destroy afferent nerves and could be performed at the time of biliary by-pass.
There are several ablative techniques that are currently being investigated and employed mainly for liver tumours. Several of these techniques rely on a direct thermal insult to cause local tissue ablation. These include interstitial laser therapy [19], radiofrequency ablation [20], and cryotherapy [21]. Thermal ablative techniques have limitations, particularly related to cytokine release in "cryoshock phenomenon"[22,23] and charring in the heat methods [24]. Pancreatic cryotherapy has been reported in a single study, but the data reported was inadequate to make any conclusions [25]. A recent report of radiofrequency ablation in the porcine pancreas has shown this to be feasible and safe [26].
Electrolysis has the potential to be adapted for pancreatic tissue ablation. A direct current is passed through a conductive medium between a pair of electrodes. Platinum electrodes appear ideal as they are relatively inert, but also have potential anti-neoplastic properties in the formation of platinum salts [27-29]. Tissue electrolysis produces sodium hydroxide and hydrogen at the cathode (alkaline), and hydrochloric acid and chlorine gas at the anode (acidic) [4-6]. The significant pH changes produced by electrolysis are cytotoxic and cause localised tissue necrosis [7]. Electrolytic ablation does not rely on a thermal effect [8,30].
The hypothesis of this study was that electrolytic destruction of the pancreas would result in a localised pancreatitis. The extent and severity of this was assessed in the experiment using blood and histological analysis.
In caerulein-induced pancreatitis in rats serial serum amylase has shown a 2 to 5 fold increase from the control value [31]. The hyperamylasemia with a proportion of the animals in this study (at approximately 4 hours) was not statistically significant in a paired T-test comparing the pre-electrolytic samples, with the 4 hour samples (Sig 2-tailed = 0.72).
Serum glucose would be expected to rise in severe pancreatitis according to Ranson's criteria [32] but this was not demonstrated in this study where it was relatively unchanged throughout all the animals.
The histology of the sections was quantified using a point score originally described by Spormann et al [14]. Electrolysis of the pancreas gland produced a region of necrosis. There was a localised region of pancreatitis around the electrolysis site, but this was not throughout the gland. It shows there is a generalised increase in the cumulative score although this was not dose related and was not significantly different from the control value.
The dismal outcome of pancreatic cancer and the need for low morbidity palliation has prompted the investigation of electrolysis as a possible method of palliation by tumour ablation. This study has demonstrated that electrolysis in the rat pancreas produce localised necrosis that appears both safe and reproducible. This pilot study was performed in only a small number of animals, but all animal deaths were believed to be related to the anaesthesia. All the rats that survived recovered well following electrolysis. The study indicates that localised pancreatic ablation is feasible with electrolysis. There was a localised region of pancreatitis around the site of necrosis, but there were no systemic complications of electrolysis in this model. The next stage is to extensively investigate pancreatic electrolysis in a large animal model, to assess the short and long-term effects, prior to human pilot studies. In the larger animal model, a larger volume of tissue can be ablated with higher doses of Coulombs. Previous studies have shown that dose of Coulombs delivered is proportional to the volume of necrosis produced [9]. This study investigated the effects of electrolytic ablation in healthy pancreatic tissue, as this would have a greater tendency to become inflamed than that of tumour and thus cause a pancreatitis. A future area of study could investigate the effect of electrolysis in rodent pancreatic tumour model [33-36]. This study was performed on the minium number of animals as a pilot study to show feasibility, but obviously the technique needs to be performed on a greater number of large animal models whose pancreatic anatomy is more similar to that of humans. This novel technique could offer significant advantages for patients with unresectable pancreatic tumours.
Competing interests
None declared.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Contributor Information
Beverley G Fosh, Email: foshy@hotmail.com.
Jonathon Guy Finch, Email: guy@guyfinch.fsnet.co.uk.
Adrian A Anthony, Email: Adrian.Anthony@nwahs.sa.gov.au.
Michael Texler, Email: Michael.Texler@IMVS.sa.gov.au.
Guy J Maddern, Email: guy.maddern@adelaide.edu.au.
References
- Bramhall SR, Allum WH, Jones AG, Allwood A, Cummins C, Neoptolemos JP. Treatment and survival in 13,560 patients with pancreatic cancer, and incidence of the disease, in the West Midlands: an epidemiological study [see comments]. Br J Surg. 1995;82:111–115. doi: 10.1002/bjs.1800820137. [DOI] [PubMed] [Google Scholar]
- Connolly MM, Dawson PJ, Michelassi F, Moossa AR, Lowenstein F. Survival in 1001 patients with carcinoma of the pancreas. Ann Surg. 1987;206:366–373. doi: 10.1097/00000658-198709000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michelassi F, Erroi F, Dawson PJ, Pietrabissa A, Noda S, Handcock M, Block GE. Experience with 647 consecutive tumors of the duodenum, ampulla, head of the pancreas, and distal common bile duct. Ann Surg. 1989;210:544–556. doi: 10.1097/00000658-198910000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Samuelsson L, Jonsson L, Lamm IL, Linden CJ, Ewers SB. Electrolysis with different electrode materials and combined with irradiation for treatment of experimental rat tumors. Acta Radiol. 1990;32:178–181. [PubMed] [Google Scholar]
- Samuelsson L, Jonsson L. Electrolyte destruction of lung tissue. Electrochemical aspects. Acta Radiol. 1980;21:711–714. doi: 10.1177/028418518002100604. [DOI] [PubMed] [Google Scholar]
- Grossi EA, Parish MA, Kralik MR, Glassman LR, Esposito RA, Ribakove GH, Galloway AC, Colvin SB. Direct-current injury from external pacemaker results in tissue electrolysis [published erratum appears in Ann Thorac Surg 1994 Apr;57(4):1053] [see comments]. Ann Thorac Surg. 1993;56:156–157. doi: 10.1016/0003-4975(93)90422-e. [DOI] [PubMed] [Google Scholar]
- Hagedorn R, Fuhr G. Steady state electrolysis and isoelectric focusing. Electrophoresis. 1990;11:281–289. doi: 10.1002/elps.1150110402. [DOI] [PubMed] [Google Scholar]
- Baxter PS, Wemyss-Holden SA, Dennison AR, Maddern GJ. Electrochemically induced hepatic necrosis: the next step forward in patients with unresectable liver tumours? Aust N Z J Surg. 1998;68:637–640. doi: 10.1111/j.1445-2197.1998.tb04833.x. [DOI] [PubMed] [Google Scholar]
- Robertson GS, Wemyss-Holden SA, Dennison AR, Hall PM, Baxter P, Maddern GJ. Experimental study of electrolysis-induced hepatic necrosis. Br J Surg. 1998;85:1212–1216. doi: 10.1046/j.1365-2168.1998.00806.x. [DOI] [PubMed] [Google Scholar]
- Wemyss-Holden SA, Robertson GS, Dennison AR, Vanderzon PS, Hall PM, Maddern GJ. A new treatment for unresectable liver tumours: long-term studies of electrolytic lesions in the pig liver. Clin Sci (Colch) 2000;98:561–567. doi: 10.1042/CS19990298. [DOI] [PubMed] [Google Scholar]
- Wemyss-Holden SA, Robertson GS, Dennison AR, de la MHP, Fothergill JC, Jones B, Maddern GJ. Electrochemical Lesions in the Rat Liver Support Its Potential for Treatment of Liver Tumors. J Surg Res. 2000;93:55–62. doi: 10.1006/jsre.2000.5910. [DOI] [PubMed] [Google Scholar]
- Wemyss-Holden SA, de la MHP, Robertson GS, Dennison AR, Vanderzon PS, Maddern GJ. The safety of electrolytically induced hepatic necrosis in a pig model. Aust N Z J Surg. 2000;70:607–612. doi: 10.1046/j.1440-1622.2000.01907.x. [DOI] [PubMed] [Google Scholar]
- Berry DP, Dennison AR, Ward R, Maddern GJ. Electrolytic ablation of colorectal liver metastases-1 year follow-up. Digestive Surgery. [DOI] [PubMed]
- Spormann H, Sokolowski A, Letko G. Experimental acute pancreatitis – a quantification of dynamics at enzymic and histomorphologic levels. Pathol Res Pract. 1989;185:358–362. doi: 10.1016/S0344-0338(89)80013-5. [DOI] [PubMed] [Google Scholar]
- Andersson A, Bergdahl L. Carcinoma of the pancreas. Am Surg. 1976;42:173–177. [PubMed] [Google Scholar]
- Lillemoe KD, Barnes SA. Surgical palliation of unresectable pancreatic carcinoma. Surg Clin North Am. 1995;75:953–968. doi: 10.1016/s0039-6109(16)46739-3. [DOI] [PubMed] [Google Scholar]
- Watanapa P, Williamson RC. Surgical palliation for pancreatic cancer: developments during the past two decades. Br J Surg. 1992;79:8–20. doi: 10.1002/bjs.1800790105. [DOI] [PubMed] [Google Scholar]
- Lichtenstein DR, Carr-Locke DL. Endoscopic palliation for unresectable pancreatic carcinoma. Surg Clin North Am. 1995;75:969–988. doi: 10.1016/s0039-6109(16)46740-x. [DOI] [PubMed] [Google Scholar]
- Germer CT, Albrecht D, Roggan A, Isbert C, Buhr HJ. Experimental study of laparoscopic laser-induced thermotherapy for liver tumours. Br J Surg. 1997;84:317–320. doi: 10.1046/j.1365-2168.1997.02567.x. [DOI] [PubMed] [Google Scholar]
- Curley SA, Izzo F, Delrio P, Ellis LM, Granchi J, Vallone P, Fiore F, Pignata S, Daniele B, Cremona F. Radiofrequency ablation of unresectable primary and metastatic hepatic malignancies: results in 123 patients. Ann Surg. 1999;230:1–8. doi: 10.1097/00000658-199907000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seifert JK, Junginger T, Morris DL. A collective review of the world literature on hepatic cryotherapy. J R Coll Surg Edinb. 1998;43:141–154. [PubMed] [Google Scholar]
- Seifert JK, Morris DL. World survey on the complications of hepatic and prostate cryotherapy. World J Surg. 1999;23:109–114. doi: 10.1007/s002689900617. [DOI] [PubMed] [Google Scholar]
- Blackwell TS, Debelak JP, Venkatakrishnan A, Schot DJ, Harley DH, Pinson CW, Williams P, Washington K, Chtristman JW, Chapman WC. Acute lung injury after hepatic cryoablation: correlation with NF-kappa B activation and cytokine production. Surgery. 1999;126:518–526. doi: 10.1067/msy.2099.99676. [DOI] [PubMed] [Google Scholar]
- Goldberg SN, Gazelle GS, Solbiati L, Livraghi T, Tanabe KK, Hahn PF, Mueller PR. Ablation of liver tumors using percutaneous RF therapy. AJR Am J Roentgenol. 1998;170:1023–1028. doi: 10.2214/ajr.170.4.9530053. [DOI] [PubMed] [Google Scholar]
- Walzel C. [Cryosurgical treatment of tumors]. Chirurg. 1976;47:289–93. [PubMed] [Google Scholar]
- Merkle EM, Haaga JR, Duerk JL, Jacobs GH, Brambs HJ, Lewin JS. MR imaging-guided radio-frequency thermal ablation in the pancreas in a porcine model with a modified clinical C-arm system. Radiology. 1999;213:461–467. doi: 10.1148/radiology.213.2.r99nv21461. [DOI] [PubMed] [Google Scholar]
- Mortensen BT, Bojsen J. Evidence for growth inhibition by platinum electrodes at low current levels. J Biomed Eng. 1982;4:103–106. doi: 10.1016/0141-5425(82)90069-3. [DOI] [PubMed] [Google Scholar]
- Rosenberg B, VanCamp V. Inhibition of Cell Division in Escherichia Coli by Electrolysis Products from a Platinum Electrode. Nature. 1965:698–699. doi: 10.1038/205698a0. [DOI] [PubMed] [Google Scholar]
- Rosenberg B, VanCamp L, Trosko JE, Mansour VH. Platinum compounds: a new class of potent antitumour agents. Nature. 1969;222:385–386. doi: 10.1038/222385a0. [DOI] [PubMed] [Google Scholar]
- Heiberg E, Nalesnik WJ, Janney C. Effects of varying potential and electrolytic dosage in direct current treatment of tumors. Acta Radiol. 1991;32:174–177. [PubMed] [Google Scholar]
- Hofbauer B, Friess H, Weber A, Baczako K, Kisling P, Schilling M, Uhl W, Dervenis C, Büchler MW. Hyperlipaemia intensifies the course of acute oedematous and acute necrotising pancreatitis in the rat. Gut. 1996;38:753–758. doi: 10.1136/gut.38.5.753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ranson JH, Rifkind KM, Roses DF, Fink SD, Eng K, Localio SA. Objective early identification of severe acute pancreatitis. Am J Gastroenterol. 1974;61:443–451. [PubMed] [Google Scholar]
- Schwarz RE, McCarty TM, Peralta EA, Diamond DJ, Ellenhorn JD. An orthotopic in vivo model of human pancreatic cancer. Surgery. 1999;126:562–567. doi: 10.1067/msy.2099.100267. [DOI] [PubMed] [Google Scholar]
- Pour P, Kruger FW, Althoff J, Cardesa A, Mohr U. Cancer of the pancreas induced in the Syrian golden hamster. Am J Pathol. 1974;76:349–358. [PMC free article] [PubMed] [Google Scholar]
- Longnecker DS. Animal model of human disease. Carcinoma of the pancreas in azaserine-treated rats. Am J Pathol. 1981;105:94–96. [PMC free article] [PubMed] [Google Scholar]
- Longnecker DS, Roebuck BD, Yager JD, Jr, Lilja HS, Siegmund B. Pancreatic carcinoma in azaserine-treated rats: induction, classification and dietary modulation of incidence. Cancer. 1981;47:1562–1572. doi: 10.1002/1097-0142(19810315)47:6+<1562::aid-cncr2820471419>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]