

Abstract
Rectal foreign body insertion is a common condition in emergency surgery, which often requires surgical intervention. Here we report a clinical case of rectal foreign body insertion as a rare cause of persistent lumbosacral plexus injury. A 72-year-old man presented to the emergency department complaining of acute bilateral paraplegia with loss of sensation in both legs, as well as total urinary retention. The patient underwent abdominal computed tomography, which showed a rectal foreign body measuring 13 × 11.5 × 10 cm in the lower abdomen and pelvis. Extraluminal assistance through a median laparotomy was required after unsuccessful attempts at transanal recovery alone. After removal of the foreign body, the rectal wall and anorectal sphincter were massively dilated, with severe bruising of the rectal mucosa on proctoscopy. A protective loop-ileostomy was performed.
The sacral plexus is located posteriorly in the pelvis. Physiologically, the nerves are well protected by surrounding anatomical structures. Post-traumatic lumbosacral plexus injuries with paraplegia, urinary retention and anorectal sphincter insufficiency occur quite frequently after heavy traffic accidents. Lumbosacral plexus injury as a result of rectal foreign body insertion is rare. Severe neurological deficits through rectal foreign body insertion are rare but known medical conditions. To the best of our knowledge, this is the first reported case of severe and persistent post-traumatic lumbosacral plexus injury through a rectal foreign body.
Keywords: Rectal foreign body, Neurological deficit, Stenosis, Lumbosacral plexus
Introduction
Rectal foreign body insertion is a common condition in emergency surgery, which often requires surgical intervention. In most cases of anorectal foreign body insertion, the patients are of male gender. It is current standard practice to extract the foreign body using the least invasive approach. Anorectal foreign bodies can usually be removed by hand, by tools such as Kocher clamps or endoscopically. Failing this, emergency laparotomy should be performed. Here, we report a rare clinical presentation of severe and persistent neurological deficits after rectal foreign body insertion.
Case history
A 72-year-old man was admitted to the emergency department of the University Hospital RWTH-Aachen, presenting with acute bilateral paraplegia, loss of sensation in both legs and urinary dysfunction. Initially, the patient reported a fall, omitting to mention the rectal foreign body insertion. X-ray and computed tomography (CT) studies were done to exclude traumatic spinal cord injury. These revealed a foreign body in the lower pelvis measuring 13 × 11.5 × 10 cm, with no signs of spinal cord injury, bowel perforation or bleeding (Fig 1). Extraluminal assistance through a median laparotomy was required after unsuccessful attempts at transanal recovery alone. Concomitant urinary retention was treated by intraoperative insertion of a suprapubic catheter. After removal of the foreign body (Fig 2), rectal wall integrity was tested by transanal application of 400 ml methylene blue. Even though there were no signs of rectal perforation, the rectal wall and anorectal sphincter were massively dilated with a bruised rectal mucosa on proctoscopy. Accordingly, a protective loop ileostomy was performed. Postoperatively, a lesion of the lumbosacral plexus including axonal demyelination damage to the nervus tibialis, nervus suralis and nervus peroneus was diagnosed. As a result, the patient suffered from erectile dysfunction, together with faecal and urinary incontinence. The latter was controlled by a suprapubic catheter. After 23 days of hospitalisation, the patient was discharged and transferred to a neurological rehabilitation centre.
Figure 1.

Plain x-ray of the pelvis showing a rectal foreign body measuring 13 × 11.5 × 10 cm
Figure 2.
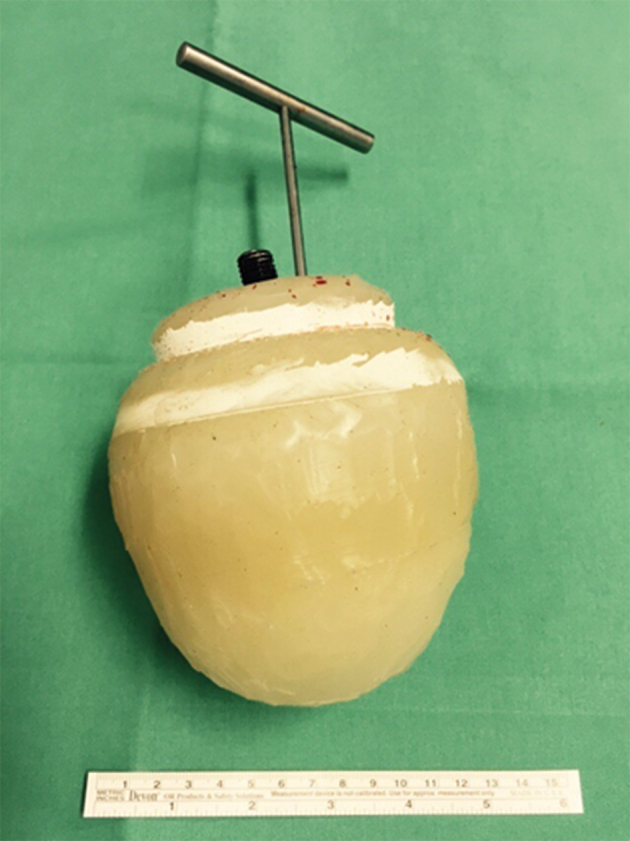
The foreign body as shown after removal. The object itself consisted mainly of a silicon body; the metal handle was screwed to the base during our attempt to recover the object transanally.
Urinary incontinence resolved completely after 8 months and the suprapubic catheter could be removed. In the later postoperative course, the patient also developed lower rectum stenosis. This condition could, however, be managed interventionally with repeat endoscopic balloon dilatations. An ileostomy reversal was performed 14 months after the initial surgery, without complications. Anal sphincter atony and neurological deficits of the lower extremity were, however, still evident at this time.
Discussion
The lumbosacral plexus lies posteriorly in the pelvis, with the sigmoid colon located in front of it. Physiologically, the nerves are well protected by the surrounding anatomical structures.1 In our case, a massive dilatation of the rectum with concomitant compression injury of the lumbosacral plexus led to persistent neurological deficits. Post-traumatic lumbosacral plexus injuries with paraplegia, urinary retention and anorectal sphincter insufficiency occur more frequently as a result of heavy traffic accidents and are quite unusual after rectal foreign body insertion.2 Nerve surgery is a treatment option in early traumatic nerve injuries but is often associated with poor clinical outcome. Neurological rehabilitation is the predominant treatment of choice.2 In most cases of anorectal foreign body insertion, the patients are of male gender and the mean age is 44 years.3 Typically, these patients are oligosymptomatic, presenting with mild abdominal and/or rectal pain, usually without anal bleeding.4 It is current standard practice to extract the foreign body using the least invasive approach.3 Often, anorectal foreign bodies can be removed manually using instruments, such as Kocher clamps, or endoscopically.
If signs of bowel perforation are present, such as peritonitis or free air on imaging studies, or if the foreign body cannot be removed through less traumatic techniques, an emergency laparotomy is the treatment of choice.3 In most cases of anorectal foreign bodies, the long-term complication rate is low.5 There are very few reports of stenosis or incontinence as sequelae of an anorectal foreign body.5 Rectal stenosis is most commonly a complication of colorectal operations and/or chronic inflammatory bowel disease.6
Conclusion
Severe complications as a result of rectal foreign body insertion are rare. In our case, however, the patient suffered from serious neurological symptoms and incontinence, which persisted more than 18 months after the incident. To the best of our knowledge, this is the first reported case of severe and persistent post-traumatic lumbosacral plexus injury through a rectal foreign body.
References
- 1.Neufeld EA, Shen PY, Nidecker AE et al. MR imaging of the lumbosacral plexus: a review of techniques and pathologies. J Neuroimaging 2015; (5): 691–703. [DOI] [PubMed] [Google Scholar]
- 2.Garozzo D, Zollino G, Ferraresi S. In lumbosacral plexus injuries can we identify indicators that predict spontaneous recovery or the need for surgical treatment? Results from a clinical study on 72 patients. J Brachial Plex Peripher Nerve Inj 2014; (1): 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cologne KG, Ault GT. Rectal foreign bodies: what is the current standard? Clin Colon Rectal Surg 2012; (4): 214–218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Akhtar MA, Arora PK. Case of unusual foreign body in the rectum. Saudi J Gastroenterol 2009; (2): 131–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ooi BS, Ho YH, Eu KW et al. Management of anorectal foreign bodies: a cause of obscure anal pain. Aust N Z J Surg 1998; (12): 852–855. [DOI] [PubMed] [Google Scholar]
- 6.Ragg J, Garimella V, Cast J et al. Balloon dilatation of benign rectal anastomotic strictures: a review. Dig Surg 2012; (4): 287–291. [DOI] [PubMed] [Google Scholar]