

Abstract
Background
Populations exposed to humanitarian emergencies are particularly vulnerable to mental health problems, including new onset, relapse and deterioration of psychotic disorders. Inadequate care for this group may lead to human rights abuses and even premature death. The WHO Mental Health Gap Action Programme Intervention Guide (mhGAP-IG), and its adaptation for humanitarian settings (mhGAP-HIG), provides guidance for management of mental health conditions by non-specialised healthcare professionals. However, the pharmacological treatment of people with non-affective psychosis who do not improve with mhGAP first-line antipsychotic treatments is not addressed. In order to fill this gap, UNHCR has formulated specific guidance on the second-line pharmacological treatment of non-affective psychosis in humanitarian, non-specialised settings.
Methods
Following the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology, a group of international experts performed an extensive search and retrieval of evidence on the basis of four scoping questions. Available data were critically appraised and summarised. Clinical guidance was produced by integrating this evidence base with context-related feasibility issues, preferences, values and resource-use considerations.
Results
When first-line treatments recommended by mhGAP (namely haloperidol and chlorpromazine) are not effective, no other first-generation antipsychotics are likely to provide clinically meaningful improvements. Risperidone or olanzapine may represent beneficial second-line options. However, if these second-line medications do not produce clinically significant beneficial effects, there are two possibilities. First, to switch to the alternative (olanzapine to risperidone or vice versa) or, second, to consider clozapine, provided that specialist supervision and regular laboratory monitoring are available in the long term. If clinically relevant depressive, cognitive or negative symptoms occur, the use of a selective serotonin reuptake inhibitor may be considered in addition or as an alternative to standard psychological interventions.
Conclusions
Adapting scientific evidence into practical guidance for non-specialised health workers in humanitarian settings was challenging due to the paucity of relevant evidence as well as the imprecision and inconsistency of results between studies. Pragmatic outcome evaluation studies from low-resource contexts are urgently needed. Nonetheless, the UNHCR clinical guidance is based on best available evidence and can help to address the compelling issue of undertreated, non-affective psychosis in humanitarian settings.
Electronic supplementary material
The online version of this article (doi:10.1186/s12916-017-0960-z) contains supplementary material, which is available to authorized users.
Keywords: Global mental health, Humanitarian settings, Antipsychotics, Non-affective psychosis, Translational research, Clinical guidance
Background
There has been a dramatic increase in worldwide humanitarian emergency situations in recent years, provoked by forced displacement related to armed conflicts and persecution as well as to environmental disasters, including drought, flooding and earthquakes. People in such humanitarian settings have elevated risks for the development of mental health issues, which cause additional suffering and constitute major clinical and public health concerns [1–6]. In humanitarian emergencies, mental health issues are at risk of being overlooked [7]. In particular, while many efforts have been made to describe and address stress-related disorders, such as post-traumatic stress disorder, anxiety and emotional disorders, including depression, far less attention has been given to the epidemiological characterisation and clinical management of non-affective psychosis (including schizophrenia) [8–15]. Thus, there is a major treatment gap, particularly considering that epidemiological data suggest that the prevalence of psychotic disorders is heightened in refugees in comparison with both native populations and non-refugee migrants [12], and that, in humanitarian emergencies, people with pre-existing psychosis are particularly vulnerable to relapse and deterioration [16–18]. In humanitarian settings, people with psychotic disorders constitute a significant proportion of the caseload in clinical mental health programmes, with rates ranging from 8.6% to 41.2% of overall mental disorders [19–23]. These individuals are particularly vulnerable to human rights violations, discrimination, social exclusion and even premature death [24–26].
In the last 10 years, efforts have been made to provide non-specialised healthcare professionals with easily accessible tools for managing mental health conditions of high priority. The World Health Organization (WHO) and the United Nations High Commissioner for Refugees (UNHCR) have developed policies and tools to expand access to mental healthcare to underserved populations through the decentralisation of basic mental healthcare and integration of mental health into primary care [27, 28]. In particular, the Mental Health Gap Action Programme Intervention Guide (mhGAP-IG) [29, 30] and the Mental Health Gap Action Programme Humanitarian Intervention Guide (mhGAP-HIG) [31] represent successful examples of this approach. However, neither mhGAP-IG nor mhGAP-HIG address the management of people with long-term, disabling mental disorders, particularly non-affective psychosis, who remain symptomatic after antipsychotic treatment provided according to mhGAP guidelines. Although the number of people with treatment-resistant psychosis may be relatively small, the unmet mental health needs of this group lead to significant social and economic burden for families, health workers, and the wider community. Furthermore, for this population, guidance on subsequent pharmacological options is limited.
In order to fill this gap, UNHCR has recently formulated specific guidance on the pharmacological treatment of non-affective psychosis in humanitarian non-specialised settings. This paper anticipates the methodology employed to evaluate and summarise the best available evidence, and reports on how the evidence was translated into pragmatic guidance for healthcare professionals. The expected impact of the UNHCR guidance in humanitarian settings, as well as the potential obstacles to its effective implementation, are also discussed.
Methods
The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology [32] guided the process from evidence retrieval to the production of a pragmatic guidance for health professionals working in humanitarian settings. A scientific secretariat, represented by the WHO Collaborating Centre for Research and Training in Mental Health and Service Evaluation in Verona, Italy, worked closely with an advisory panel of international experts with in-depth expertise spanning the fields of clinical psychopharmacology, mental health systems and services research in humanitarian settings, health policy development, health economics, and implementation science. According to the GRADE methodology, key scoping questions for this guidance were formulated on the basis of a shared process directly involving in-field experts and practitioners, with a strong emphasis on the role of specific context variables [33]. These scoping questions guided evidence retrieval, critical appraisal and interpretation:
In people with non-affective psychosis who do not improve after treatment with a first-generation antipsychotic (FGA), is switching to another FGA effective and safe?
Are second-generation antipsychotics (SGAs) effective and safe in people with non-affective psychosis who do not improve with FGAs used as first-line treatment?
Which antipsychotic is effective and safe in people with a diagnosis of treatment-resistant non-affective psychosis?
Are antidepressant-antipsychotic combinations effective and safe in people with non-affective psychosis who develop depressive, cognitive and negative symptoms?
In order to address each question, the target populations, settings, interventions and outcomes of interest were characterised by employing a Population, Intervention, Comparison, Outcomes framework. In order to extensively review all available data on the pharmacological treatments of non-affective psychosis, for each Population, Intervention, Comparison, Outcomes table we systematically searched electronic databases (PubMed, PsychINFO, CINHAL, MEDLINE, Web Of Science Core Collection, the Cochrane Central Register of Controlled Trials) to identify the most recent good-quality systematic review for each intervention of interest. We used the terms “psychosis OR psychotic OR schizophrenia” in association with (1) specific search filters for systematic reviews and meta-analyses (http://hiru.mcmaster.ca/hiru/HIRU_Hedges_MEDLINE_Strategies.aspx#Reviews); (2) the specific term identifying the subgroup of interest (e.g. “treatment-resistant”, “negative symptoms”); and (3) the names of the medications of interest. No language restrictions were applied. The last update of the search was performed in January 2017. We included only systematic reviews and/or meta-analysis of randomised controlled trials including adult patients. When more than one review provided data for the same outcome, the most recent and comprehensive review was chosen. When systematic reviews of randomised trials were not available, we searched for the most up-to-date and good quality individual randomised trials and observational studies. The scientific secretariat summarised the results of the included reviews and assessed their quality by employing the Guideline Development Tool [34], an online software that helps produce evidence summaries and healthcare recommendations according to the GRADE approach. The GRADE tables produced are available as Additional file 1. On the basis of evidence summaries, in line with the GRADE methodology, the panel critically discussed the balance between the possible clinical advantages and disadvantages of different treatment options, considering context-related feasibility issues, costs, ethical issues, values, preferences and insights from experts working in low-resource settings. This led to the development of the clinical practice guidance, graphically summarised in Fig. 1. Doses were reported according to licensed doses from the British National Formulary [35]. When the licensed dose range was considered to possibly diverge from that used in common clinical practice, we employed data from the most updated systematic reviews or guidelines. Further, additional clinical annotations (including the use of long-acting formulations and relevant insights on the monitoring and management of adverse events) were derived from the mhGAP and, if needed, from the most updated international guidelines and regulatory documents in order to pragmatically support mental health professionals in routine practice. These pragmatic annotations will be available in the final format of the UNHCR guidance. Additionally, a comprehensive evidence summary reporting each step of this process will be made available online for consultation.
Fig. 1.
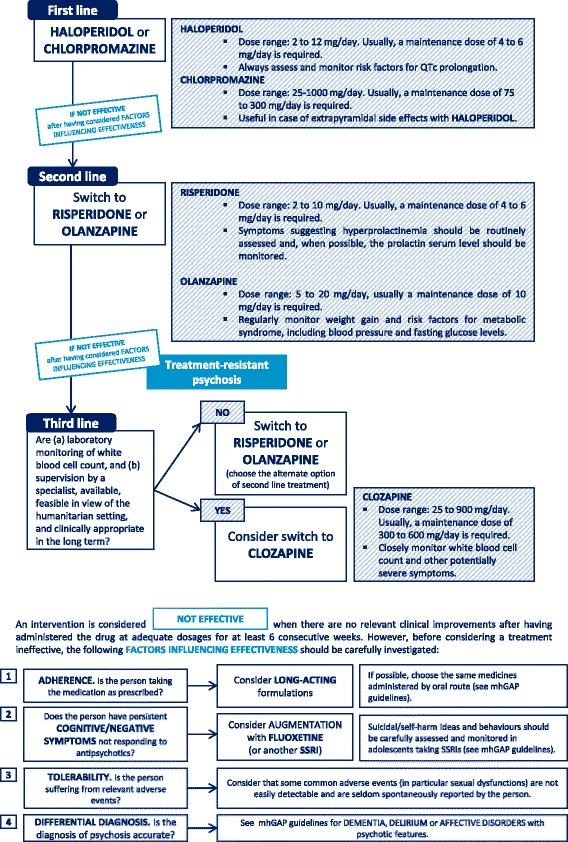
Flow-chart describing the clinical pathway for the choice of antipsychotics
Results
In people with non-affective psychosis who do not improve after treatment with a FGA, is switching to another FGA effective and safe?
Haloperidol and chlorpromazine were used as the reference standard, as these medications are the first-line recommended treatments for patients with non-affective psychosis in the mhGAP guidelines [29, 36].
We did not find studies of SGA intervention in individuals who had failed to improve after treatment with one FGA. Therefore, we included studies conducted in the general population of people suffering from non-affective psychosis. This evidence was rated as indirect (Additional file 1).
According to available evidence, no difference in treatment response was identified between haloperidol and FGAs as a class, and between haloperidol and the following medications considered individually: chlorpromazine, perphenazine, pimozide, fluphenazine and trifluoperazine. Haloperidol showed a slightly better overall acceptability with respect to chlorpromazine, but caused more movement disorders. Perphenazine and FGAs as a class did not show benefits compared with haloperidol in terms of efficacy, acceptability and tolerability. Pimozide, fluphenazine and trifluoperazine did not show benefits over haloperidol in terms of efficacy, while data on acceptability and tolerability were not available.
With few exceptions, the GRADE tables showed ‘low’ or ‘very low’ quality for the vast majority of outcomes, mostly due to the indirectness of the evidence, as no data were collected in low-resource settings, and individuals were not included on the basis of being not responsive to haloperidol as first-line treatment. Moreover, many of the included studies had small sample sizes and high attrition rates.
In conclusion, the clinical implication was that it is not possible to identify individual FGAs to recommend when a first-line treatment with haloperidol proves to be ineffective. Common clinical practice would suggest switching to the other most commonly available treatment or chlorpromazine. However, there is still uncertainty and further studies in low-resources/humanitarian settings may provide relevant insights on this issue.
The therapeutic dose of haloperidol may vary between 2 and 12 mg/day, and a maintenance dose of 4 to 6 mg/day is usually required [35, 37, 38]. For chlorpromazine, the dose range is from 25 to 1000 mg/day, with a maintenance dose of 75 to 300 mg/day [29, 35].
Are SGAs effective and safe in people with non-affective psychosis who do not improve with FGAs used as first-line treatment?
Each SGA was compared initially to haloperidol, as the reference standard of first-line FGAs. SGAs that proved to be more effective than haloperidol were then compared to each other (head-to-head) in order to identify possible advantages of one medication over another. We found no data specifically referring to individuals who had already failed to improve after treatment with one FGA. Therefore, studies conducted in the general population of people suffering from non-affective psychosis were used (indirect). Compared to haloperidol, all SGAs considered individually (with the exception of paliperidone, for which no data were available) appeared to cause less sedation and motor symptoms, and had a better overall acceptability profile. Among these medications, only risperidone and olanzapine showed a more favourable efficacy profile in comparison with haloperidol. After having compared these two medications head-to-head, risperidone showed better acceptability and was associated with less weight gain than olanzapine, while olanzapine caused less motor symptoms and prolactin increase.
Indirectness, high attrition rates and imprecise results (due to small sample sizes) contributed to set the quality of the evidence to ‘low’ or ‘very low’ for all of the outcomes of interest. In conclusion, the clinical implication was that risperidone and olanzapine may be chosen as second-line treatments as they are both associated with benefits in comparison with haloperidol in terms of efficacy and overall acceptability in the medium- and long-term. The level of confidence in this clinical implication was judged uncertain. The panel pointed out that the choice between risperidone and olanzapine should be based on specific patient characteristics and the antipsychotic profile, considering that, in general, risperidone may have a slightly better overall tolerability and cause less weight gain compared to olanzapine, while olanzapine is associated with less motor symptoms and prolactin increase compared to risperidone. Further, the choice should take into account availability, affordability and sustainability of provision in the long term, in relation to the setting of care. The therapeutic dose of risperidone may vary between 2 and 10 mg/day, and a maintenance dose of 4 to 6 mg/day is usually required [35, 39], while the dose of olanzapine may vary between 5 and 20 mg/day, and the maintenance dose required is usually 10 mg/day [35].
Which individual antipsychotic is effective and safe in people with a diagnosis of treatment-resistant non-affective psychosis?
For the purposes of this review, individuals were defined as treatment-resistant when at least two adequate trials with different antipsychotics, one of which is a SGA, proved ineffective. This is an adaptation of the definition provided by Suzuki et al. [40]. However, considering the lack of a widely shared consensus on definitions of treatment resistance [41], we included studies of participants with treatment-resistant psychosis even where this definition varied. Compared to FGAs, clozapine appeared to be more effective in terms of clinical improvement, similarly effective in terms of relapse rates, and similarly acceptable and more tolerable in terms of motor symptoms, while blood problems and weight gain were more frequent in patients taking clozapine. In patients with treatment-resistant psychosis, risperidone and olanzapine appeared to be similarly effective and acceptable in comparison with clozapine. Risperidone was associated with less weight gain and sedation, but more motor symptoms, when compared to olanzapine.
Studies comparing clozapine and olanzapine, as well as studies comparing clozapine and risperidone, provided efficacy outcomes of ‘moderate’ quality. By contrast, for most of the other outcomes the quality was ‘low’ or ‘very low’ due to indirectness and high attrition rates.
As a clinical implication, it was concluded that, in patients not improving after at least two antipsychotics (one of which is an SGA) administered at adequate dose and duration, a switch to risperidone or olanzapine (in people with no previous ineffective exposure to these medications) or clozapine may be considered. Almost no evidence exists on other SGAs. The choice to use clozapine must take into account context-related issues, particularly in relation to safety, given that routine clinical and laboratory monitoring (for the risk of life-threatening agranulocytosis, but also for other potentially severe adverse events such as seizures and myocarditis [42]) and supervision by a specialist should be regarded as a fundamental prerequisite.
The therapeutic dose of clozapine may vary between 25 and 900 mg/day, and a maintenance dose of 300 to 600 mg/day is usually required [35, 40, 43].
Are antidepressant-antipsychotic combinations effective and safe in people with non-affective psychosis who develop depressive, cognitive and negative symptoms?
Augmentation strategies of antipsychotic treatment with antidepressants are often considered in the treatment of depressive, cognitive and negative symptoms in people with non-affective psychosis. These symptom dimensions are often overlooked and may be associated with unfavourable outcomes, such as chronic functional impairment and higher suicide risk [44–46]. We therefore retrieved and analysed all available data on augmentation strategies of antipsychotic treatment with antidepressants.
Adding antidepressants to antipsychotic treatment appeared to be similarly acceptable in comparison with antipsychotics alone, and associated with a statistically relevant benefit on depressive, cognitive and negative symptoms. A ‘low’ and ‘very low’ quality rating was given for all outcomes of interest, due to indirectness, high attrition rates, very small sample sizes and few events for the majority of included studies, which led to imprecise results (Additional file 1).
In conclusion, the clinical implication was that adding one antidepressant to antipsychotic treatment may be considered in the case of clinically relevant depressive, negative or cognitive symptoms. Preference should be given to selective serotonin reuptake inhibitors, including fluoxetine (available widely in generic formulations and included in the WHO essential list of medicines), considering their favourable balance between efficacy and tolerability.
Discussion
Quality shortcomings and implications for research
Translating scientific data on antipsychotics into pragmatic suggestions to be implemented in humanitarian settings carries methodological limitations. For this particular setting, indirectness represented the most pressing quality issue. First, none of the studies included in selected reviews were performed in low-resource settings or in humanitarian contexts (Additional file 1). Data were collected in people from stable, high-income, Western countries, which are often considerably different from humanitarian settings with regards to distribution of risks and mediating factors such as medical conditions (e.g. dehydration, malnutrition, infectious illnesses), exposure to potentially traumatic events, stability of family and social support, and access to complementary healthcare resources (e.g. psychosocial support, rehabilitation and a safe medical environment in case of acute symptoms). Second, studies from high-income, Western countries may not capture culturally specific concepts of distress that are relevant to other countries. In general, it is unclear whether the efficacy of treatments may differ in contexts characterised by on-going, chronic adversities [47–49]. Third, even when supported by sound scientific evidence, some interventions may not be feasible in low-resource settings due to the need for expensive and/or time-consuming practices (e.g. laboratory investigations and specialist oversight needed for clozapine). Fourth, the setting may strongly affect the burden and impact of side effects and adverse events. For example, prolactin increase can be managed with relatively sophisticated interventions in high-income countries, including laboratory monitoring of blood prolactin levels, addition of low doses of aripiprazole to the current antipsychotic medication, or the addition of bromocriptine or cabergoline under specialist supervision [50]. None of these options is likely to be feasible and suitable in humanitarian settings. Finally, focusing on the aim of pragmatically translating available data into a clinical guidance, we included reviews referring to populations for which some degree of heterogeneity cannot be excluded, as in the case of treatment-resistant psychosis.
In general, the overall quality of evidence was low for the majority of outcomes considered. This was due not only to the setting of care (as in the case of indirectness), but also resulted from the internal quality of the included studies. Most studies included small samples and had high attrition rates and a short follow-up period, resulting in both inconsistency of estimates across studies and imprecise estimates (even after the aggregation of results from single studies).
For all these reasons, we urgently need to broaden the evidence base around antipsychotic treatments and include direct evidence from populations in low- and middle-income countries and, where possible, from humanitarian settings, instead of merely extrapolating results from studies in high-income settings [51, 52]. Within the scope of this paper, we see a need for pragmatic research to establish the cost-effectiveness of various SGAs and clozapine.
Given the specific challenges related to conducting research in humanitarian settings, such studies should ideally have the form of randomised pragmatic trials focused on issues such as feasibility and cost-effectiveness [53, 54]. This review suggests that the introduction of clozapine as a third step in a treatment protocol could yield significant benefits. However, there is considerable uncertainty about the routine use of clozapine in low- and middle-income countries, mostly because of the risk of serious, and sometimes life-threatening, side effects [55, 56].
Implications for practice and policy
In recent years, strong emphasis has been placed on addressing mental health issues in low-resource and humanitarian contexts in a timely manner, not only to improve the quality of life for people suffering from mental illness, but also as a necessary step to achieve global health and development goals [57, 58]. The growing number of humanitarian and emergency settings, many of which develop into protracted crises that take years if not decades to resolve, should prompt global health researchers to explicitly take these settings into consideration. The proposed algorithm (Fig. 1) is aimed at optimising not only the quality of treatments, but also the timeliness of care for people with non-affective psychosis, considering that early intervention is widely recognised as an essential precondition for achieving higher response rates and better functioning outcomes [59]. This algorithm shows relevant differences if compared with current guidelines developed for general settings of care in high-income countries [60–63], which confirms how, starting from the same evidence base, clinical decisions can radically differ in relation to context-related preferences, values, feasibility and cost-effectiveness considerations.
Among possible obstacles preventing this guidance from having an effective impact, it should be acknowledged that accurate psychiatric assessment and differential diagnosis might be particularly challenging for non-specialised health workers, especially in emergency and humanitarian contexts. This is generally true for mental health, but particularly relevant for the area of psychosis. For example, the onset of non-affective psychosis is often preceded by non-specific symptoms, such as perplexity, obsessive-compulsive manifestations and sub-threshold mood alterations, whose recognition is challenging even for trained psychiatrists [64]. In addition, in contexts with high levels of disorders related to extreme stress, pre-psychotic stages can be misdiagnosed as mood disorders. At the same time, severe mood or post-traumatic disorders with psychotic features can be mistaken for prodromal psychosis. This is particularly relevant if we consider that culturally related manifestations often include mood episodes with psychotic features [65–67]. Furthermore, the most appropriate options for an effective implementation of mental health recommendations into clinical practice remain unclear [68], and this issue results particularly challenging for humanitarian, low-resources settings [69, 70]. Therefore, although guidance on psychopharmacology can notably improve the effectiveness and timeliness of interventions in humanitarian settings, this tool alone cannot be considered as exhaustive. Sustainable improvements in the quality of treatments for people with severe mental illness need to be supported by a broader cultural and structural change in health systems on multiple levels [71–73].
Conclusions
Underdiagnosed and undertreated non-affective psychosis is a compelling issue for health workers in humanitarian and emergency settings. By conducting an appraisal of the best evidence base, the present UNHCR guidance attempts to pragmatically address this treatment gap. The adaptation of available scientific evidence to inform clinical practice in humanitarian settings has proved particularly challenging mainly due to indirectness of data, which needs to be urgently supplemented by large and pragmatic in-field clinical research. Hopefully, the implementation of this pragmatic guidance may notably improve cost-effectiveness and timeliness of pharmacological interventions in the context of wide and multilevel actions towards better practices and policies for people with psychosis.
Acknowledgements
The authors wish to thank Fuad Almossa, Sabah Aziz, Boris Budosan, Dan Cohen, Asis K. Das, Carolina Echeverri, Mohamed Elshazly, Saeed Farooq, Fikirte Girma, Julius Muron and Benyam Worku, who provided useful feedback as external reviewers.
Funding
This guidance was commissioned to the WHO Collaborating Center of Verona and funded by UNHCR.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study. Details of the search and GRADE tables will be made available online for consultation.
Abbreviations
- FGAs
First-generation antipsychotics
- GRADE
Grading of recommendations, assessment, development and evaluation
- mhGAP-HIG
Mental Health Gap Action Programme Humanitarian Intervention Guide
- mhGAP-IG
Mental Health Gap Action Programme Intervention Guide
- SGAs
Second-generation antipsychotics
- UNHCR
United Nations High Commissioner for Refugees
- WHO
World Health Organization
Additional file
Online supplemental material - PICO tables and GRADE tables produced for each scoping question. (DOCX 169 kb)
Authors’ contributions
GO, CB and PV conceived the content and methodology for producing the guidance. GO and CB performed the search for evidence and rated its quality by applying the GRADE methodology. As part of the experts’ panel, DS, JE, SC and LJ provided feedback on the relevance of the document contents and its clinical applicability throughout each phase, and discussed advantages and disadvantages of each intervention in order to shape the final guidance. CH provided extensive support and conceptual advice in characterising the clinical implications of the guidance. GO wrote the first draft of the manuscript, which was critically revised and finally approved by CB, CH, DS, JE, SC, LJ and PV.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1186/s12916-017-0960-z) contains supplementary material, which is available to authorized users.
Contributor Information
Giovanni Ostuzzi, Phone: +39 045 812 4063, Email: giovanni.ostuzzi@gmail.com.
Corrado Barbui, Email: corrado.barbui@univr.it.
Charlotte Hanlon, Email: charlotte.hanlon@kcl.ac.uk.
Sudipto Chatterjee, Email: sudipto_dr@yahoo.com.au.
Julian Eaton, Email: julian.eaton@cbm.org.
Lynne Jones, Email: lynnemyfanwy@gmail.com.
Derrick Silove, Email: d.silove@unsw.edu.au.
Peter Ventevogel, Email: ventevog@unhcr.org.
References
- 1.Mollica RF, Cardozo BL, Osofsky HJ, Raphael B, Ager A, Salama P. Mental health in complex emergencies. Lancet. 2004;364:2058–67. doi: 10.1016/S0140-6736(04)17519-3. [DOI] [PubMed] [Google Scholar]
- 2.IASC. Inter-Agency Contingency Planning Guidelines for Humanitarian Assistance. 2007. https://interagencystandingcommittee.org/node/2902. Accessed 27 Oct 2017.
- 3.Steel Z, Chey T, Silove D, Marnane C, Bryant RA, van Ommeren M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta-analysis. JAMA. 2009;302:537–49. doi: 10.1001/jama.2009.1132. [DOI] [PubMed] [Google Scholar]
- 4.Tol WA, Barbui C, Galappatti A, Silove D, Betancourt TS, Souza R, et al. Mental health and psychosocial support in humanitarian settings: linking practice and research. Lancet. 2011;378:1581–91. doi: 10.1016/S0140-6736(11)61094-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Roberts B, Browne J. A systematic review of factors influencing the psychological health of conflict-affected populations in low- and middle-income countries. Glob Public Health. 2011;6:814–29. doi: 10.1080/17441692.2010.511625. [DOI] [PubMed] [Google Scholar]
- 6.Kane JC, Luitel NP, Jordans MJD, Kohrt BA, Weissbecker I, Tol WA. Mental health and psychosocial problems in the aftermath of the Nepal earthquakes: findings from a representative cluster sample survey. Epidemiol Psychiatr Sci. 2017. doi:10.1017/S2045796016001104. [DOI] [PMC free article] [PubMed]
- 7.Ventevogel P, van Ommeren M, Schilperoord M, Saxena S. Improving mental health care in humanitarian emergencies. Bull World Health Organ. 2015;93:666–666A. doi: 10.2471/BLT.15.156919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nosè M, Turrini G, Imoli M, Ballette F, Ostuzzi G, Cucchi F, et al. Prevalence and correlates of psychological distress and psychiatric disorders in asylum seekers and refugees resettled in an Italian catchment area. J Immigr Minor Health. 2017. doi:10.1007/s10903-017-0629-x. [DOI] [PubMed]
- 9.Shawyer F, Enticott JC, Block AA, Cheng I, Meadows GN. The mental health status of refugees and asylum seekers attending a refugee health clinic including comparisons with a matched sample of Australian-born residents. BMC Psychiatry. 2017;17:76. doi: 10.1186/s12888-017-1239-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kirmayer LJ, Narasiah L, Munoz M, Rashid M, Ryder AG, Guzder J, et al. Common mental health problems in immigrants and refugees: general approach in primary care. CMAJ. 2011;183:E959–67. doi: 10.1503/cmaj.090292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Murray KE, Davidson GR, Schweitzer RD. Review of refugee mental health interventions following resettlement: best practices and recommendations. Am J Orthopsychiatry. 2010;80:576–85. doi: 10.1111/j.1939-0025.2010.01062.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dapunt J, Kluge U, Heinz A. Risk of psychosis in refugees: a literature review. Transl Psychiatry. 2017;7:e1149. doi: 10.1038/tp.2017.119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Priebe S, Giacco D, El-Nagib R. Public health aspects of mental health among migrants and refugees: a review of the evidence on mental health care for refugees, asylum seekers and irregular migrants in the WHO European region. Geneva: World Health Organization; 2016. [PubMed] [Google Scholar]
- 14.Miller KE, Rasmussen A. The mental health of civilians displaced by armed conflict: an ecological model of refugee distress. Epidemiol Psychiatr Sci. 2017;26:129–38. doi: 10.1017/S2045796016000172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Coldiron ME, Llosa AE, Roederer T, Casas G, Moro M. Brief mental health interventions in conflict and emergency settings: an overview of four medecins sans frontieres - France programs. Confl Health. 2013;7:23. doi: 10.1186/1752-1505-7-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Llosa AE, van Ommeren M, Kolappa K, Ghantous Z, Souza R, Bastin P, et al. A two-phase approach for the identification of refugees with priority need for mental health care in Lebanon: a validation study. BMC Psychiatry. 2017;17:28. doi: 10.1186/s12888-016-1154-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hollander A, Dal H, Lewis G, Magnusson C, Kirkbride JB, Dalman C. Refugee migration and risk of schizophrenia and other non-affective psychoses: cohort study of 1.3 million people in Sweden. BMJ. 2016;352:i1030. doi: 10.1136/bmj.i1030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Katona C. Non-affective psychosis in refugees. BMJ. 2016;352:i1279. doi: 10.1136/bmj.i1279. [DOI] [PubMed] [Google Scholar]
- 19.Jones L, Asare J, Elmasri M, Mohanraj A. Mental health in disaster settings. BMJ. 2007;335:679–80. doi: 10.1136/bmj.39329.580891.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Humayun A, Azad N, Haq I, Khan FR, Ahmad A, Farooq RK. Mental health and psychosocial support for the internally displaced persons in Bannu, Pakistan. Intervention. 2016;14:33–49. doi: 10.1097/WTF.0000000000000105. [DOI] [Google Scholar]
- 21.Rose N, Hughes P, Ali S, Jones L. Integrating mental health into primary health care settings after an emergency. Intervention. 2011;9(3):211–24. [Google Scholar]
- 22.Ventevogel P, Ndayisaba H, Van De Put W. Psychosocial assistance and decentralized mental health care in post-conflict Burundi (2000–2008) Intervention. 2011;9:315–31. [Google Scholar]
- 23.Kane JC, Ventevogel P, Spiegel P, Bass JK, van Ommeren M, Tol WA. Mental, neurological, and substance use problems among refugees in primary health care: analysis of the health information system in 90 refugee camps. BMC Med. 2014;12:228. doi: 10.1186/s12916-014-0228-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Silove D, Ekblad S, Mollica R. The rights of the severely mentally ill in post-conflict societies. Lancet. 2000;355:1548–9. doi: 10.1016/S0140-6736(00)02177-2. [DOI] [PubMed] [Google Scholar]
- 25.Jones L, Asare JB, El Masri M, Mohanraj A, Sherief H, van Ommeren M. Severe mental disorders in complex emergencies. Lancet. 2009;374:654–61. doi: 10.1016/S0140-6736(09)61253-8. [DOI] [PubMed] [Google Scholar]
- 26.Galletly CA. Premature death in schizophrenia: bridging the gap. Lancet Psychiatry. 2017;4:263–5. doi: 10.1016/S2215-0366(17)30079-2. [DOI] [PubMed] [Google Scholar]
- 27.World Health Organization. Mental Health Action Plan 2013–2020. 2013. http://www.who.int/mental_health/publications/action_plan/en/. Accessed 27 Oct 2017.
- 28.United Nations High Commissioner for Refugees. Global Strategy for Public Health 2014–2018. 2014. http://www.unhcr.org/530f12d26.pdf. Accessed 27 Oct 2017.
- 29.World Health Organization. mhGAP Intervention Guide for Mental, Neurological and Substance Use Disorders in Non-Specialized Health Settings: Mental Health Gap Action Programme (mhGAP). 2016. http://www.who.int/mental_health/mhgap/mhGAP_intervention_guide_02/en/. Accessed 27 Oct 2017. [PubMed]
- 30.Dua T, Barbui C, Patel AA, Tablante EC, Thornicroft G, Saxena S. Discussion of the updated WHO recommendations for mental, neurological, and substance use disorders. Lancet Psychiatry. 2016;3:1008–12. doi: 10.1016/S2215-0366(16)30184-5. [DOI] [PubMed] [Google Scholar]
- 31.World Health Organization & United Nations High Commissioner for Refugees. mhGAP Humanitarian Intervention Guide. Clinical Management of Mental, Neurological and Substance Use Conditions in Humanitarian Emergencies. 2015. http://www.who.int/mental_health/publications/mhgap_hig/en/. Accessed 27 Oct 2017.
- 32.Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, Schunemann HJ. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–6. doi: 10.1136/bmj.39489.470347.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ostuzzi G, Bighelli I, Carrara B, Dusi N, Imperadore G, Lintas C, et al. Making the use of psychotropic drugs more rational through the development of GRADE recommendations in specialist mental healthcare. Int J Ment Health Syst. 2013;7:14. doi: 10.1186/1752-4458-7-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.McMaster University. GRADEpro GDT: GRADEpro Guideline Development Tool. 2015. https://gradepro.org/. Accessed 27 Oct 2017.
- 35.British National Formulary: Joint Formulary Committee. September 2015-March 2016. 70th ed. London: British Medical Association; 2015.
- 36.WHO. Mental Health Gap Action Programme. In Individuals with Psychotic Disorders (Including Schizophrenia), are Antipsychotic Drugs Safe and Effective? 2012. http://www.who.int/mental_health/mhgap/evidence/resource/psychosis_q1.pdf?ua=1. Accessed 27 Oct 2017.
- 37.Geddes J, Freemantle N, Harrison P, Bebbington P. Atypical antipsychotics in the treatment of schizophrenia: systematic overview and meta-regression analysis. BMJ. 2000;321:1371–6. doi: 10.1136/bmj.321.7273.1371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Donnelly L, Rathbone J, Adams CE. Haloperidol dose for the acute phase of schizophrenia. Cochrane Database Syst Rev. 2013;8:CD001951. doi: 10.1002/14651858.CD001951.pub2. [DOI] [PubMed] [Google Scholar]
- 39.Li C, Xia J, Wang J. Risperidone dose for schizophrenia. Cochrane Database Syst Rev. 2009;4:CD007474. doi: 10.1002/14651858.CD007474.pub2. [DOI] [PubMed] [Google Scholar]
- 40.Suzuki T, Remington G, Mulsant BH, Uchida H, Rajji TK, Graff-Guerrero A, et al. Defining treatment-resistant schizophrenia and response to antipsychotics: a review and recommendation. Psychiatry Res. 2012;197:1–6. doi: 10.1016/j.psychres.2012.02.013. [DOI] [PubMed] [Google Scholar]
- 41.Howes OD, McCutcheon R, Agid O, de Bartolomeis A, van Beveren NJ, Nico JM, Birnbaum ML, et al. Treatment-resistant schizophrenia: treatment response and resistance in psychosis (TRRIP) working group consensus guidelines on diagnosis and terminology. Am J Psychiatry. 2017;174:216–29. doi: 10.1176/appi.ajp.2016.16050503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Remington G, Agid O, Foussias G, Ferguson L, McDonald K, Powell V. Clozapine and therapeutic drug monitoring: is there sufficient evidence for an upper threshold? Psychopharmacology (Berl) 2013;225:505–18. doi: 10.1007/s00213-012-2922-7. [DOI] [PubMed] [Google Scholar]
- 43.Freudenreich O, McEvoy J. Guidelines for Prescribing Clozapine in Schizophrenia. 2015. http://www.uptodate.com/contents/guidelines-for-prescribing-clozapine-in-schizophrenia#H350566201. Accessed 27 Oct 2017.
- 44.van Os J, Kapur S. Schizophrenia. Lancet. 2009;374:635–45. doi: 10.1016/S0140-6736(09)60995-8. [DOI] [PubMed] [Google Scholar]
- 45.Helfer B, Samara MT, Huhn M, Klupp E, Leucht C, Zhu Y, et al. Efficacy and safety of antidepressants added to antipsychotics for schizophrenia: a systematic review and meta-analysis. Am J Psychiatry. 2016;173:876–86. doi: 10.1176/appi.ajp.2016.15081035. [DOI] [PubMed] [Google Scholar]
- 46.Acosta FJ, Siris SG, Diaz E, Salinas M, Del Rosario P, Hernandez JL. Suicidal behavior in schizophrenia and its relationship to the quality of psychotic symptoms and insight - a case report. Psychiatr Danub. 2012;24:97–9. [PubMed] [Google Scholar]
- 47.Tol WA, Barbui C, Bisson J, Cohen J, Hijazi Z, Jones L, et al. World health organization guidelines for management of acute stress, PTSD, and bereavement: key challenges on the road ahead. PLoS Med. 2014;11:e1001769. doi: 10.1371/journal.pmed.1001769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Tay AK, Rees S, Chen J, Kareth M, Lahe S, Kitau R, et al. Associations of conflict-related trauma and ongoing stressors with the mental health and functioning of West Papuan refugees in Port Moresby, Papua New Guinea (PNG) PLoS One. 2015;10:e0125178. doi: 10.1371/journal.pone.0125178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Kohrt BA, Rasmussen A, Kaiser BN, Haroz EE, Maharjan SM, Mutamba BB, et al. Cultural concepts of distress and psychiatric disorders: literature review and research recommendations for global mental health epidemiology. Int J Epidemiol. 2014;43:365–406. doi: 10.1093/ije/dyt227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Taylor D, Paton C, Kapur S. The maudsley prescribing guidelines in psychiatry. 12. Chichester: Wiley-Blackwell; 2015. [Google Scholar]
- 51.Purgato M, Adams C, Barbui C. Schizophrenia trials conducted in African countries: a drop of evidence in the ocean of morbidity? Int J Ment Health Syst. 2012;6:9. doi: 10.1186/1752-4458-6-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Patel V, Araya R, Chatterjee S, Chisholm D, Cohen A, de Silva M, et al. Treatment and prevention of mental disorders in low-income and middle-income countries. Lancet. 2007;370:991–1005. doi: 10.1016/S0140-6736(07)61240-9. [DOI] [PubMed] [Google Scholar]
- 53.IASC. IASC Recommendations for Conducting Ethical Mental Health and Psychosocial Research in Emergency Settings. 2014. https://interagencystandingcommittee.org/node/9061. Accessed 27 Oct 2017.
- 54.Chiumento A, Rahman A, Frith L, Snider L, Tol WA. Ethical standards for mental health and psychosocial support research in emergencies: review of literature and current debates. Global Health. 2017;13:8. doi: 10.1186/s12992-017-0231-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Farooq S, Taylor M. Clozapine: dangerous orphan or neglected friend? Br J Psychiatry. 2011;198:247–9. doi: 10.1192/bjp.bp.110.088690. [DOI] [PubMed] [Google Scholar]
- 56.Remington G, Lee J, Agid O, Takeuchi H, Foussias G, Hahn M, et al. Clozapine’s critical role in treatment resistant schizophrenia: ensuring both safety and use. Expert Opin Drug Saf. 2016;15:1193–203. doi: 10.1080/14740338.2016.1191468. [DOI] [PubMed] [Google Scholar]
- 57.Collins PY, Insel TR, Chockalingam A, Daar A, Maddox YT. Grand challenges in global mental health: integration in research, policy, and practice. PLoS Med. 2013;10:e1001434. doi: 10.1371/journal.pmed.1001434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Miranda JJ, Patel V. Achieving the millennium development goals: does mental health play a role? PLoS Med. 2005;2:e291. doi: 10.1371/journal.pmed.0020291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Singh SP. Early intervention in psychosis. Br J Psychiatry. 2010;196:343–5. doi: 10.1192/bjp.bp.109.075804. [DOI] [PubMed] [Google Scholar]
- 60.Moore TA, Buchanan RW, Buckley PF, Chiles JA, Conley RR, Crismon ML, et al. The Texas medication algorithm project antipsychotic algorithm for schizophrenia: 2006 update. J Clin Psychiatry. 2007;68:1751–62. doi: 10.4088/JCP.v68n1115. [DOI] [PubMed] [Google Scholar]
- 61.Buchanan RW, Kreyenbuhl J, Kelly DL, Noel JM, Boggs DL, Fischer BA, et al. The 2009 schizophrenia PORT psychopharmacological treatment recommendations and summary statements. Schizophr Bull. 2010;36:71–93. doi: 10.1093/schbul/sbp116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Hasan A, Falkai P, Wobrock T, Lieberman J, Glenthøj B, Gattaz WF, et al. World federation of societies of biological psychiatry (WFSBP) guidelines for biological treatment of schizophrenia - a short version for primary care. Int J Psychiatry Clin Pract. 2017;21:82–90. doi: 10.1080/13651501.2017.1291839. [DOI] [PubMed] [Google Scholar]
- 63.NICE. Psychosis and Schizophrenia in Adults: Prevention and Management. 2014. https://www.nice.org.uk/guidance/cg178. Accessed 27 Oct 2017.
- 64.Iyer SN, Boekestyn L, Cassidy CM, King S, Joober R, Malla AK. Signs and symptoms in the pre-psychotic phase: description and implications for diagnostic trajectories. Psychol Med. 2008;38:1147–56. doi: 10.1017/S0033291708003152. [DOI] [PubMed] [Google Scholar]
- 65.Adeponle AB, Groleau D, Kirmayer LJ. Clinician reasoning in the use of cultural formulation to resolve uncertainty in the diagnosis of psychosis. Cult Med Psychiatry. 2015;39:16–42. doi: 10.1007/s11013-014-9408-5. [DOI] [PubMed] [Google Scholar]
- 66.Zouari N, Aloulou J, Siala M, Ben Mahmoud S, Zouari L, Maalej M. Aspects culturels dans la depression masquee par des symptomes psychotiques. Encéphale. 2010;36:504–9. doi: 10.1016/j.encep.2010.03.002. [DOI] [PubMed] [Google Scholar]
- 67.Nygaard M, Sonne C, Carlsson J. Secondary psychotic features in refugees diagnosed with post-traumatic stress disorder: a retrospective cohort study. BMC Psychiatry. 2017;17:5. doi: 10.1186/s12888-016-1166-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Bighelli I, Ostuzzi G, Girlanda F, Cipriani A, Becker T, Koesters M, Barbui C. Implementation of treatment guidelines for specialist mental health care. Cochrane Database Syst Rev. 2016;12:CD009780. doi: 10.1002/14651858.CD009780.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Schafer A, Snider L, Sammour R. A reflective learning report about the implementation and impacts of psychological first Aid (PFA) in Gaza. Disaster Health. 2016;3:1–10. doi: 10.1080/21665044.2015.1110292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Tol WA, Patel V, Tomlinson M, Baingana F, Galappatti A, Silove D, et al. Relevance or excellence? setting research priorities for mental health and psychosocial support in humanitarian settings. Harv Rev Psychiatry. 2012;20:25–36. doi: 10.3109/10673229.2012.649113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Ventevogel P. Integration of mental health into primary healthcare in low-income countries: avoiding medicalization. Int Rev Psychiatry. 2014;26:669–79. doi: 10.3109/09540261.2014.966067. [DOI] [PubMed] [Google Scholar]
- 72.Saxena S. Challenges and opportunities in global mental health: a perspective from WHO. Epidemiol Psychiatr Sci. 2016;25:495–8. doi: 10.1017/S2045796016000536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Saraceno B, Barbui C. Global mental health: achievements, concerns and (unanswered) questions. Epidemiol Psychiatr Sci. 2016;25:493–4. doi: 10.1017/S2045796016000548. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study. Details of the search and GRADE tables will be made available online for consultation.