

Abstract
Purpose
To analyze failure rate in two-year increments to determine if graft choice changed over time and graft failure rate.
Methods
A prospective 2002–2008 database was used to identify risk factors for anterior cruciate ligament retear (ACLR). Subjects who had primary ACLR with no history of contralateral surgery and 2-year follow-up were included. Subjects who underwent a multi-ligament reconstruction were excluded. Graft type, age, sex, smoking status, body mass index, Marx activity level at index surgery, medial and lateral meniscus status at time of ACLR, sport played post-ACLR, and clinical site were evaluated. Analysis was repeated using 2002–2003 (early) and 2007–2008 (late) two-year databases. ANOVA with post-hoc analysis was performed to detect significant differences in age and Marx score by graft type over time.
Results
Two-year follow-up for graft failure was obtained on 2497/2692 (93%) subjects. There were 112/2497 (4.5%) ACLRs identified at two-year follow-up. The only predictor that changed between early/late periods was allograft use. Allograft odds ratio decreased from 13.1 to 9.5 (p<.01). Allografts were used in older patients (31–40 years) and with lower Marx scores (10–8) from early to late periods. Mean age of subjects receiving BTB autografts did not significantly change over time (22.8 to 23.5) Mean age of subjects receiving hamstring autografts fell (27.9 to 25.5). Mean age of subjects receiving allografts rose significantly (31.3 to 39.8, p<.01). Mean Marx score of subjects who received BTB and hamstring autografts did not significantly change over time. Mean Marx score of subjects receiving allografts decreased significantly (p<.01).
Conclusions
After early recognition allograft use in young active patients was a risk factor for retear, graft choice by surgeons changed in the late period to use of allografts in older and less-active patients, which correlated with significant decrease in retear risk.
Level of Evidence
Therapeutic-III, case control study
Introduction
Injuries to the anterior cruciate ligament (ACL) occur in the active general population, but are particularly common in athletes involved in cutting sports1–3. After an ACL injury, the knee has significant risk of functional instability, meniscal tears and subsequent osteoarthritis4. In order to restore knee stability and decrease risk of subsequent injury (e.g. meniscus tears), ACL reconstruction (ACLR) is often performed. Excellent results have been widely reported for ACLR in restoration of knee stability4–6. Despite the high reported success rates, ACLR is not to be taken lightly, as patients must invest a significant amount of time, discomfort, effort and money during the 6 – 12 month recovery period. ACL graft retear after undergoing surgery and rehabilitation is a devastating event for the patient as well as the family, coach, therapist and surgeon. After a tear of an ACL graft, patients often undergo a revision ACLR. In addition to the time, expense and risk of having a revision ACLR, it has been shown that revision ACLRs have inferior results to primary ACLRs7, 8.
Risk factors for tear of the native ACL have been studied and several have been identified. Two of the most commonly reported risk factors are female sex and participation in cutting sports3, 9–11. Other risk factors to have been reported include: posterior tibial slope, notch width, limb alignment and neuromuscular factors2, 10, 12–15. Major risk factors for ACLR graft retear have been identified, presented, and published within a multicenter prospective population11, 16, 17. These risk factors for graft retear were younger age, high activity, and allograft in younger patients. We also showed that the risk of graft retear in the patient with an allograft decreased as the age of the patient increased. Age and activity level were found to be highly collinear, so it can be extrapolated that this result would carry over to activity level as well16. The clinical relevance of being aware of these risk factors are: 1) to better educate patients and surgeons on the expected outcomes of an ACLR, especially graft failure; 2) to counsel patients on post-operative recommendations, and; 3) to facilitate efforts to decrease those risk factors which are modifiable, such as graft choice. The goal of this study was to analyze failure rate in two-year increments to determine if graft choice changed over time and the graft failure rate. We hypothesized that after clinicians were presented with risk factors for subsequent ACL graft failure, clinical decision-making would change and clinical outcomes would subsequently improve.
Methods
After Institutional Review Board approval was granted, data from the prospective database were used to identify the incidence and risk factors for ACLR graft retear. Subjects who had a primary ACL reconstruction at one of 7 sites and performed by one of 17 surgeons involved in the data collection with no history of contralateral knee surgery with 2-year follow-up data were included in the dataset. All patients followed a standardized post-operative rehabilitation protocol. A retear was defined as having to undergo a revision ACL reconstruction. Each time period’s data were prospectively collected in identical fashion from the same set of surgeons with greater than 80% 2-year follow-up. Subjects who underwent a multi-ligament reconstruction (n= 107), had bilateral ACLR (n=23), had an ACL repair (12), or original entry into the database was an ACL revision (n=371) were excluded from the analysis. Graft type (autograft bone-patellar tendon-bone (BTB), autograft hamstring, allograft), age, sex, smoking status, body mass index (BMI), Marx activity rating score18 at time of index surgery, medial and lateral meniscus status at the time of ACLR, sport played post ACLR, and clinical site were evaluated to determine their contribution to graft retear.
Using the statistical software STATA 9.0 (StataCorp LP, College Station, TX) multivariable logistic regression was used to determine if the chosen variables were associated with our primary outcome, ACL graft retear19. Odds ratios and 95% confidence intervals were reported for the variables associated with our outcome. Finally, the analyses were repeated for the two-year time periods at the beginning (enrollment years 2002–2003) and end (enrollment years 2007–2008) of the study timeframe. After analysis of the entire group and due to the smaller size of the “early” (2002–2003) and “late” (2007–2008) groups, the variables analyzed were limited to age, sex, Marx activity level score, and graft type. Chi square and t-tests were performed to test homogeneity between the “early” and “late” groups. Odds ratios and 95% confidence intervals were reported for the variables associated with our outcome. An ANOVA with post-hoc analysis was performed to detect significant differences in age and Marx score at time of index surgery by graft type over time.
Results
A total of 2692 subjects met all study inclusion/exclusion criteria; 2497/2692 (93%) had 2-year follow-up for graft failure obtained. There were 112/2497 (4.5%) ipsilateral graft retears and 90/2497 (3.6%) contralateral ACL tears identified in the entire group at two-year follow-up. Median time to follow up was 2/4 years (range 2.0 years–3.9 years). The number of subjects and percent graft retears are summarized for the variables tested in aggregate and for each time period in Table 1.
Table 1.
ACL Graft Retears
| 2002–2003 (n=750) | 2007–2008 (n=879) | p | Entire Population (n=2497) | ||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| N | % Retear | N | % Retear | value | N | % Retear | |
| Graft type | <.001 | ||||||
|
| |||||||
| Autograft BTB | 334 | 2.4 | 375 | 3.2 | 1132 | 3.2 | |
| Autograft Hamstring | 269 | 4.1 | 385 | 4.4 | 891 | 4.8 | |
| Allograft | 145 | 11.7 | 109 | 3.7 | 460 | 7.0 | |
|
| |||||||
| Sex | .43 | ||||||
|
| |||||||
| Male | 407 | 5.4 | 494 | 3.8 | 1368 | 4.8 | |
| Female | 343 | 4.1 | 385 | 3.6 | 1129 | 4.2 | |
|
| |||||||
| Smoking Status | .39 | ||||||
|
| |||||||
| No | 602 | 5.5 | 708 | 4.2 | 1995 | 5.2 | |
| Quit | 75 | 2.7 | 98 | 1.0 | 257 | 1.2 | |
| Current | 69 | 1.4 | 66 | 3.0 | 214 | 2.3 | |
|
| |||||||
| Sport post ACLR | .03 | ||||||
|
| |||||||
| None | 123 | 4.9 | 173 | 1.7 | 464 | 3.9 | |
| Football | 84 | 7.1 | 96 | 8.3 | 272 | 6.6 | |
| Basketball | 201 | 4.0 | 181 | 4.4 | 588 | 4.1 | |
| Soccer | 77 | 9.1 | 107 | 6.5 | 275 | 8.4 | |
| Other | 265 | 3.4 | 322 | 2.2 | 898 | 3.2 | |
|
| |||||||
| Medial Meniscus | .29 | ||||||
|
| |||||||
| No Tear | 520 | 5.2 | 588 | 3.9 | 1733 | 4.9 | |
| Tear | 230 | 3.9 | 291 | 3.4 | 764 | 3.5 | |
|
| |||||||
| Lateral Meniscus | .07 | ||||||
|
| |||||||
| No Tear | 503 | 4.8 | 552 | 4.3 | 1617 | 4.6 | |
| Tear | 247 | 4.9 | 327 | 2.8 | 880 | 4.3 | |
|
| |||||||
| 2002–2003 | 2007–2008 | Entire Population | |||||
|
| |||||||
| No Tear | Tear | No Tear | Tear | No Tear | Tear | ||
| x̄ (SD) | x̄ (SD) | x̄ (SD) | |||||
|
| |||||||
| Age | 26.7 (11.1) | 18.3 (5.4) | 26.8 (11.5) | 18.5 (3.7) | .64 | 26.9 (11.4) | 19.1 (6.5) |
|
| |||||||
| BMI | 25.5 (4.7) | 24.3 (4.7) | 25.5 (4.9) | 24.0 (4.5) | .84 | 25.5 (4.8) | 23.9 (4.4) |
|
| |||||||
| Marx Activity Level | 11.2 (5.2) | 14.3 (3.7) | 11.4 (5.2) | 14.4 (4.0) | .54 | 11.3 (5.2) | 14.3 (3.8) |
BTB, bone-patellar tendon-bone; ACLR, anterior cruciate ligament reconstruction; SD, standard deviation
Risk factors for ACL graft retears in entire population
Significant risk factors for ipsilateral ACL graft retear were: use of an allograft (odds ratio: 5.91, p<.01, 95% CI 2.91 – 12.01); younger age (odds ratio: 0.90; p<.01; 95% CI 0.86 – 0.93); and higher Marx activity level score (odds ratio: 1.10; p<.01; 95% CI 1.03 – 1.18). Sex, sport, smoking status, medial or lateral meniscus status and clinical site were not predictors of a graft retear after primary ACLR (p>0.05). This is identical to our previously reported results of the entire group11.
Predictors of ACL graft retears over time
The strength of the risk factors for ACL graft retear were compared between the early (2002–2003) and late (2007–2008) time periods. The early and late groups were statistically similar except for graft type (p<0.001) and sport played post ACLR (p=0.03) (Table 1). Younger age and allograft usage remained significant predictors of graft retear in both time periods (Table 2). The strength of age as a risk factor was not significantly different between the 02–03 and 07–08 time periods with odds ratios of 0.86 and 0.87 respectively. The strength of allograft as a risk factor did change over time. This is discussed below.
Table 2.
Strength of Risk Factors for Graft Tears
| 2002–2003 | 2007–2008 | |||
|---|---|---|---|---|
|
| ||||
| ACL Graft Retear | Odds ratio | p-value | Odds ratio | p-value |
| Age | 0.86 | <.001 | 0.87 | <.001 |
|
| ||||
| Marx Activity Level (t0) | 1.08 | .20 | 1.09 | .18 |
|
| ||||
| Autograft BTB | REF | REF | REF | REF |
| Autograft Hamstring | 2.51 | 0.06 | 1.62 | 0.22 |
| Allograft | 13.13 | <.001 | 9.51 | .002 |
|
| ||||
| Male | REF | REF | REF | REF |
| Female | 0.58 | 0.15 | 0.70 | 0.34 |
BTB, bone-patellar tendon-bone.
Post hoc analysis of change of age and Marx activity rating score by graft type over time
Average age and Marx activity rating score for each 2-year group are summarized in Table 3. The mean age (Figure 1) of subjects receiving BTB autografts did not significantly change over time, whereas the mean age of subjects receiving hamstring autografts fell while the mean age of subjects receiving allografts rose significantly over time (p< 0.01). The mean Marx activity rating score (Figure 2) of subjects who received BTB and hamstring autografts did not significantly change over time, whereas the mean Marx activity rating score of subjects receiving allografts decreased significantly over time (p< .01). Mean age of subjects receiving BTB autografts did not significantly change over time, whereas mean age of subjects receiving hamstring autografts fell, and mean age of subjects receiving allografts rose significantly.
Table 3.
Age and Activity Level of Subgroups
| 2002–2003 | 2007–2008 | |
|---|---|---|
| Age | Mean (SD) | Mean (SD) |
| Autograft BTB | 22.8 (8.9) | 23.5 (9.4) |
| Autograft Hamstring | 27.9 (11.7)† | 25.5 (10.7)† |
| Allograft | 31.3 (12.0)* | 39.8 (10.9)* |
|
| ||
| ACL Graft Retear | ||
|
| ||
| No retear | 26.7 (11.1) | 26.8 (11.5) |
| Retear | 18.2 (5.4) | 18.5 (3.7) |
|
| ||
| Marx Activity Level | Mean (SD) | Mean (SD) |
|
| ||
| Autograft BTB | 12.2 (4.9) | 12.5 (4.9) |
| Autograft Hamstring | 10.9 (5.2) | 11.6 (5.0) |
| Allograft | 10.3 (5.3)# | 8.1 (5.6)# |
|
| ||
| ACL Graft Retear | ||
|
| ||
| No retear | 11.2 (5.2) | 11.4 (5.2) |
| Retear | 14.3 (3.7) | 14.4 (4.0) |
SD = standard deviation; BTB = bone-patellar tendon-bone
Age was significantly different between the 2002–03 and 2007–08 groups (p = 0.01)
Age significantly increased over time (p < .001)
Marx significantly decreased over time (p = 0.001)
Figure 1.
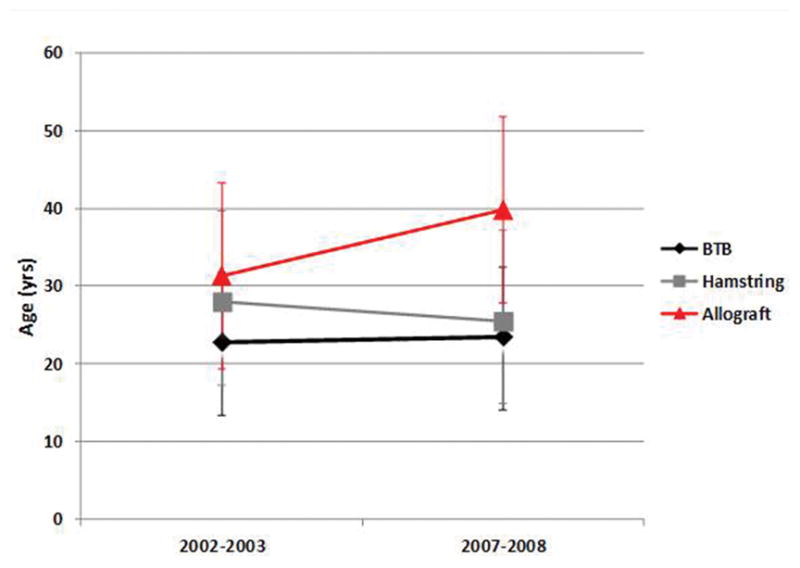
Change in age by graft type over time.
Figure 2.
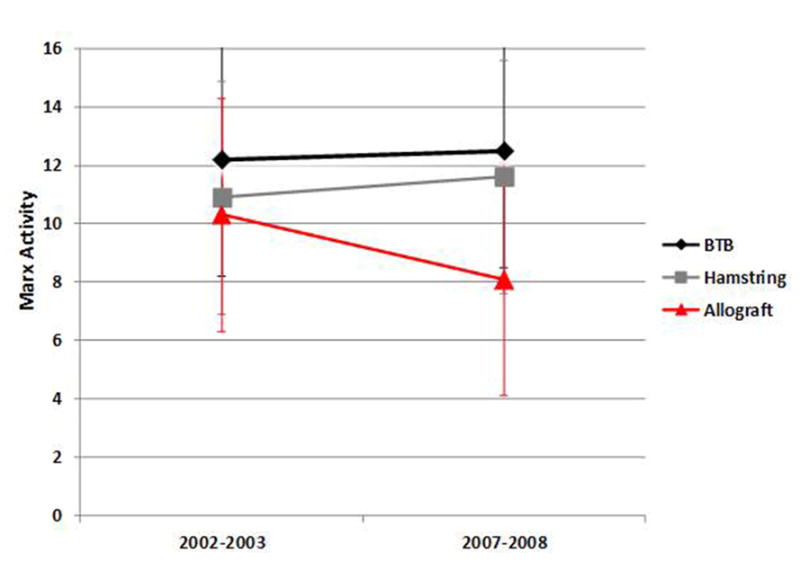
Change in Marx score by graft type over time.
Risk of retear by graft type over time
In 2002–2003, there were 36/750 (4.8%) retears compared to 33/879 (3.8%) in 2007–2008. The odds of retear for allograft subjects was 13.13 times higher compared to BTB autograft in the 2002–2003 group (p<.01) and decreased to 9.51 times higher in the 2007–2008 group (p<.01). The odds ratio between BTB autograft and hamstring autograft was not significantly different in the 2002–2003 (p=.06) or 2007–2008 groups (p=0.22). The only significant change in risk of retear by graft type between the two time periods was in allografts, for which the odd ratio decreased by nearly 28% (13.13 to 9.51) and percentage of retears decreased 68% (11.7 to 3.7). Please see tables 1 and 2. The change in odds ratios over time by graft type are shown in Figure 3.
Figure 3.
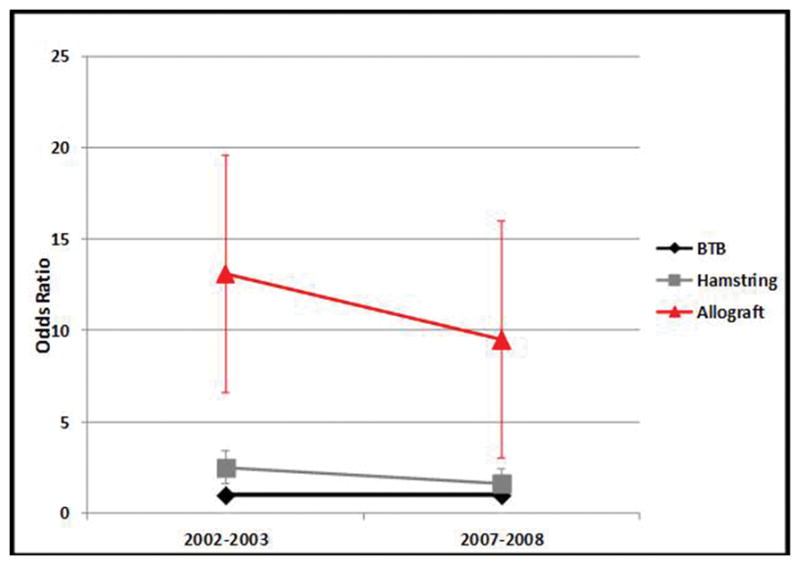
Odds ratio by graft type over time.
Sport
A qualitative review of the sport involved when the ACL retore revealed that in the entire population, 3.9% of those who did not play sports retore their ACL compared to 6.6%, 8.4%, and 4.1% for football, soccer, and basketball respectively. With respect to a change in risk between the early and late time periods, football and basketball did not change (7.1% to 8.3% and 4.0% to 4.4%, respectively), whereas the risk in soccer appeared to drop approximately 29% (9.1% to 6.5%).
Discussion
The current study supports our hypothesis that after clinicians were presented with risk factors for subsequent ACL graft failure, their clinical decisions would change and that the risk factors and clinical results would subsequently change over time. When orthopaedic surgeons were shown high quality prospective evidence that allograft use in younger patients was a major risk factor for subsequent graft failure, their practice patterns changed. They started using allografts in older and less active patients and the odds of graft retears in the allograft patients fell by 27%.
A retear of an otherwise successful ACLR is not only frustrating to all involved, but often necessitates a revision ACLR, which subjects the patient to additional expense, surgical risk, physical therapy and time away from their sport20. It has also been shown that revision ACLRs have inferior results to primary reconstructions7, 8. Understanding the risk of reinjury is important in order to appropriately counsel patients and surgeons on expected long-term results and avoid graft failure by modification of one or more risk factors21–30. Minimization of the risk of ACL graft failure should be a priority of clinicians caring for ACLR patients31.
Allograft vs Autograft
It has been reported by us, others, and confirmed by a meta-analysis that allograft ACLRs have a high retear risk compared to autografts in younger and/or highly active athletes11, 32–38. In this group, the use of allograft tissue (as well as youth and high activity) was a predictor of graft retear in the early time frame. When this became apparent in 2005–6 during the analysis of the 2-year follow-up of the 2002/03 group, it was reported internally to all study surgeons. The analysis of risk of retear by graft type with increasing age, as shown in Figure 4, was presented to the group as well. No formal recommendation of change in practice patterns was done. However, in the population of patients who were given allografts the average age and activity level changed in the subsequent time period. Surgeons started to use allografts in older and less active patients and this correlated with a corresponding decrease in the risk of retear. Over time the standard allograft patient increased in age by 8.5 years and decreased in activity by 2.2 Marx points while his/her risk of retear fell by 27%. This is of interest as it demonstrates that motivated surgeons presented with high quality prospective outcomes data with outstanding follow-up will change their practice patterns to produce better outcomes. Potentially another factor in modifying graft choice was that every surgeon knew his/her failure rate and outcomes in 2007–2008 would be prospectively tracked individually, and no surgeon desires a higher failure rate of ACLR than his/her peers.
Figure 4.
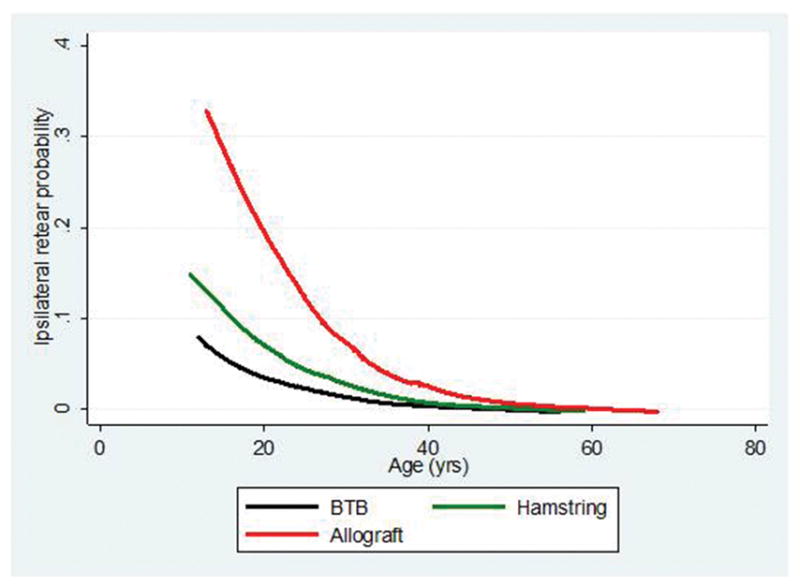
Probability of graft retear as age increases.
Many of the allografts in this group had low dose irradiation to address superficial contamination of the graft. It has been shown in several studies that irradiated allograft with higher doses (>2.5mRad) fail at a high rate16, 39–43. Other studies have shown that allografts, particularly fresh frozen, non-irradiated allografts, have similar retear risk as autografts; however, these studies tended to also have a much older patient group in the allograft group5, 44–51. In the MARS data52 when the extent of low dose versus no irradiation in allograft in revision ACLR was examined, the failure rates between the two were no different. This study has demonstrated that a change in a surgeon’s use of allograft to older patients will significantly decrease their failure risk. Further research into the influence of donor characteristics, processing techniques, tissue type and recipient characteristics on allograft ACLR outcomes should be performed by allograft industry and surgeons who utilize allografts.
Age and Activity Level
Younger age and higher activity at index ACLR were significant predictors of graft retear as previously reported11, 16. In previous studies, authors found that the risk of retear decreased by 9% for each year increase in age and increased by 10% for each increase of a point on the Marx activity scale11, 16. We suspect that the level of returned to activity is the driver of both these findings. Though this current study did not directly measure the returned to level of activity, the activity level at the time of index ACLR has been shown to be a significant predictor of activity level at two years11, 53. We suggest that the returned to level of activity needs to be controlled for in any future analysis of predictors of graft retear.
Sport
The fact that 3.9% of those patients who did not play sports retore their ACL correlates well with the fact that patients with a high Marx activity level who played football and soccer retore at a higher percentage (6.6% and 8.4% respectively). Overall the sport of football, soccer, or basketball in previous multivariable analysis was not a risk factor11. With respect to a change in risk between the early and late time periods, it is interesting that the male dominated sport of football did not change, but the percentage of coed athletes who played soccer decreased by 28.6% between the time periods. This may be explained by a possible disproportionate higher use of allografts in the early time period in which the subsequent decrease in allograft use in the late time period benefited in their retear risk. Another explanation could be a more rigorous use of ACL injury prevention programs in the later time period by female athletes, thus the differential benefit to the coed sport versus football.
Sex
Though being a strong predictor of native ACL injury, in this study female gender was not a risk factor for retear of an ACL graft. This matches reported findings11, 16 and other reports11, 54–57.
Limitations
This study was a retrospective analysis of prospectively collected data, thus it has some of the weaknesses of any retrospective analysis. As far as applicability, this study looked at results from surgeons at seven academic centers and as such, may not be generalizable to a larger more diverse group of surgeons. In this study, retear was defined as having to undergo a revision ACL reconstruction and as such probably under reports graft failures, but the same definition was used in both time frames. In addition, other potential risk factors for graft retear such as tibial slope and graft size were not analyzed as they were not part of the prospective data set.
Conclusions
After early recognition that allograft use in young active patients was a risk factor for graft retear, graft choice by the surgeons changed in the late time period to use of allografts in older and less active patients which correlated with a significant decrease in graft retear risk.
Acknowledgments
Research reported in this publication was partially supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number R01AR053684 (K.P.S.). The content is solely the responsibility of the authors and does not necessarily represent official views of the National Institutes of Health. The project was also supported by the Vanderbilt Sports Medicine Research Fund, which received unrestricted educational gifts from Smith & Nephew Endoscopy and DonJoy Orthopaedics.
We wish to thank the following research coordinators, analysts and support staff from the Multicenter Orthopaedic Outcomes Network (MOON) sites, whose efforts related to regulatory, data collection, subject follow-up, data quality control, analyses, and manuscript preparation have made this consortium successful.
We also thank all the subjects who generously enrolled and participated in this study.
References
- 1.Agel J, Arendt EA, Bershadsky B. Anterior cruciate ligament injury in national collegiate athletic association basketball and soccer: a 13-year review. The American journal of sports medicine. 2005;33:524–530. doi: 10.1177/0363546504269937. [DOI] [PubMed] [Google Scholar]
- 2.Anderson AF, Dome DC, Gautam S, Awh MH, Rennirt GW. Correlation of anthropometric measurements, strength, anterior cruciate ligament size, and intercondylar notch characteristics to sex differences in anterior cruciate ligament tear rates. The American journal of sports medicine. 2001;29:58–66. doi: 10.1177/03635465010290011501. [DOI] [PubMed] [Google Scholar]
- 3.Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. The American journal of sports medicine. 1995;23:694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- 4.Spindler KP, Kuhn JE, Freedman KB, Matthews CE, Dittus RS, Harrell FE., Jr Anterior cruciate ligament reconstruction autograft choice: bone-tendon-bone versus hamstring: does it really matter? A systematic review. The American journal of sports medicine. 2004;32:1986–1995. doi: 10.1177/0363546504271211. [DOI] [PubMed] [Google Scholar]
- 5.Poehling GG, Curl WW, Lee CA, et al. Analysis of outcomes of anterior cruciate ligament repair with 5-year follow-up: allograft versus autograft. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2005;21:774–785. doi: 10.1016/j.arthro.2005.04.112. [DOI] [PubMed] [Google Scholar]
- 6.Gobbi A, Francisco R. Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: a prospective clinical investigation. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2006;14:1021–1028. doi: 10.1007/s00167-006-0050-9. [DOI] [PubMed] [Google Scholar]
- 7.Wright R, Spindler K, Huston L, et al. Revision ACL reconstruction outcomes: MOON cohort. The journal of knee surgery. 2011;24:289–294. doi: 10.1055/s-0031-1292650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wright RW, Gill CS, Chen L, et al. Outcome of revision anterior cruciate ligament reconstruction: a systematic review. The Journal of bone and joint surgery. American volume. 2012;94:531–536. doi: 10.2106/JBJS.K.00733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gwinn DE, Wilckens JH, McDevitt ER, Ross G, Kao TC. The relative incidence of anterior cruciate ligament injury in men and women at the United States Naval Academy. The American journal of sports medicine. 2000;28:98–102. doi: 10.1177/03635465000280012901. [DOI] [PubMed] [Google Scholar]
- 10.Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: Part 1, mechanisms and risk factors. The American journal of sports medicine. 2006;34:299–311. doi: 10.1177/0363546505284183. [DOI] [PubMed] [Google Scholar]
- 11.Kaeding CC, Pedroza AD, Reinke EK, Huston LJ, Spindler KP. Risk Factors and Predictors of Subsequent ACL Injury in Either Knee After ACL Reconstruction: Prospective Analysis of 2488 Primary ACL Reconstructions From the MOON Cohort. The American journal of sports medicine. 2015;43:1583–1590. doi: 10.1177/0363546515578836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Oates KM, Van Eenenaam DP, Briggs K, Homa K, Sterett WI. Comparative injury rates of uninjured, anterior cruciate ligament-deficient, and reconstructed knees in a skiing population. The American journal of sports medicine. 1999;27:606–610. doi: 10.1177/03635465990270051001. [DOI] [PubMed] [Google Scholar]
- 13.Orchard J, Seward H, McGivern J, Hood S. Intrinsic and extrinsic risk factors for anterior cruciate ligament injury in Australian footballers. The American journal of sports medicine. 2001;29:196–200. doi: 10.1177/03635465010290021301. [DOI] [PubMed] [Google Scholar]
- 14.Rozzi SL, Lephart SM, Gear WS, Fu FH. Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. The American journal of sports medicine. 1999;27:312–319. doi: 10.1177/03635465990270030801. [DOI] [PubMed] [Google Scholar]
- 15.Sward P, Kostogiannis I, Roos H. Risk factors for a contralateral anterior cruciate ligament injury. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2010;18:277–291. doi: 10.1007/s00167-009-1026-3. [DOI] [PubMed] [Google Scholar]
- 16.Kaeding CC, Aros B, Pedroza A, et al. Allograft Versus Autograft Anterior Cruciate Ligament Reconstruction: Predictors of Failure From a MOON Prospective Longitudinal Cohort. Sports health. 2011;3:73–81. doi: 10.1177/1941738110386185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wright RW, Dunn WR, Amendola A, et al. Risk of tearing the intact anterior cruciate ligament in the contralateral knee and rupturing the anterior cruciate ligament graft during the first 2 years after anterior cruciate ligament reconstruction: a prospective MOON cohort study. The American journal of sports medicine. 2007;35:1131–1134. doi: 10.1177/0363546507301318. [DOI] [PubMed] [Google Scholar]
- 18.Marx RG, Stump TJ, Jones EC, Wickiewicz TL, Warren RF. Development and evaluation of an activity rating scale for disorders of the knee. The American journal of sports medicine. 2001;29:213–218. doi: 10.1177/03635465010290021601. [DOI] [PubMed] [Google Scholar]
- 19.Mickey RM, Greenland S. The impact of confounder selection criteria on effect estimation. American journal of epidemiology. 1989;129:125–137. doi: 10.1093/oxfordjournals.aje.a115101. [DOI] [PubMed] [Google Scholar]
- 20.Goddard M, Salmon L, Waller A, Papapetros E, Pinczewski LA. Incidence of graft rupture 15 years after bilateral anterior cruciate ligament reconstructions: a case-control study. The bone & joint journal. 2013;95-b:798–802. doi: 10.1302/0301-620X.95B6.30841. [DOI] [PubMed] [Google Scholar]
- 21.Barber-Westin SD, Noyes FR. Objective criteria for return to athletics after anterior cruciate ligament reconstruction and subsequent reinjury rates: a systematic review. The Physician and sportsmedicine. 2011;39:100–110. doi: 10.3810/psm.2011.09.1926. [DOI] [PubMed] [Google Scholar]
- 22.Borchers JR, Pedroza A, Kaeding C. Activity level and graft type as risk factors for anterior cruciate ligament graft failure: a case-control study. The American journal of sports medicine. 2009;37:2362–2367. doi: 10.1177/0363546509340633. [DOI] [PubMed] [Google Scholar]
- 23.Chen JL, Allen CR, Stephens TE, et al. Differences in mechanisms of failure, intraoperative findings, and surgical characteristics between single- and multiple-revision ACL reconstructions: a MARS cohort study. The American journal of sports medicine. 2013;41:1571–1578. doi: 10.1177/0363546513487980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kamien PM, Hydrick JM, Replogle WH, Go LT, Barrett GR. Age, graft size, and Tegner activity level as predictors of failure in anterior cruciate ligament reconstruction with hamstring autograft. The American journal of sports medicine. 2013;41:1808–1812. doi: 10.1177/0363546513493896. [DOI] [PubMed] [Google Scholar]
- 25.Ma Y, Ao YF, Yu JK, Dai LH, Shao ZX. Failed anterior cruciate ligament reconstruction: analysis of factors leading to instability after primary surgery. Chinese medical journal. 2013;126:280–285. [PubMed] [Google Scholar]
- 26.Magnussen RA, Taylor DC, Toth AP, Garrett WE. ACL graft failure location differs between allografts and autografts. Sports medicine, arthroscopy, rehabilitation, therapy & technology : SMARTT. 2012;4:22. doi: 10.1186/1758-2555-4-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Mariscalco MW, Flanigan DC, Mitchell J, et al. The influence of hamstring autograft size on patient-reported outcomes and risk of revision after anterior cruciate ligament reconstruction: a Multicenter Orthopaedic Outcomes Network (MOON) Cohort Study. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2013;29:1948–1953. doi: 10.1016/j.arthro.2013.08.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Morgan JA, Dahm D, Levy B, Stuart MJ. Femoral tunnel malposition in ACL revision reconstruction. The journal of knee surgery. 2012;25:361–368. doi: 10.1055/s-0031-1299662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rahr-Wagner L, Thillemann TM, Pedersen AB, Lind MC. Increased risk of revision after anteromedial compared with transtibial drilling of the femoral tunnel during primary anterior cruciate ligament reconstruction: results from the Danish Knee Ligament Reconstruction Register. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2013;29:98–105. doi: 10.1016/j.arthro.2012.09.009. [DOI] [PubMed] [Google Scholar]
- 30.Tiamklang T, Sumanont S, Foocharoen T, Laopaiboon M. Double-bundle versus single-bundle reconstruction for anterior cruciate ligament rupture in adults. The Cochrane database of systematic reviews. 2012;11:Cd008413. doi: 10.1002/14651858.CD008413.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Crawford SN, Waterman BR, Lubowitz JH. Long-term failure of anterior cruciate ligament reconstruction. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2013;29:1566–1571. doi: 10.1016/j.arthro.2013.04.014. [DOI] [PubMed] [Google Scholar]
- 32.Barrett GR, Luber K, Replogle WH, Manley JL. Allograft anterior cruciate ligament reconstruction in the young, active patient: Tegner activity level and failure rate. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2010;26:1593–1601. doi: 10.1016/j.arthro.2010.05.014. [DOI] [PubMed] [Google Scholar]
- 33.Guo L, Yang L, Duan XJ, et al. Anterior cruciate ligament reconstruction with bone-patellar tendon-bone graft: comparison of autograft, fresh-frozen allograft, and gamma-irradiated allograft. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2012;28:211–217. doi: 10.1016/j.arthro.2011.08.314. [DOI] [PubMed] [Google Scholar]
- 34.Krych AJ, Jackson JD, Hoskin TL, Dahm DL. A meta-analysis of patellar tendon autograft versus patellar tendon allograft in anterior cruciate ligament reconstruction. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2008;24:292–298. doi: 10.1016/j.arthro.2007.08.029. [DOI] [PubMed] [Google Scholar]
- 35.Pallis M, Svoboda SJ, Cameron KL, Owens BD. Survival comparison of allograft and autograft anterior cruciate ligament reconstruction at the United States Military Academy. The American journal of sports medicine. 2012;40:1242–1246. doi: 10.1177/0363546512443945. [DOI] [PubMed] [Google Scholar]
- 36.Papageorgiou CD, Ma CB, Abramowitch SD, Clineff TD, Woo SL. A multidisciplinary study of the healing of an intraarticular anterior cruciate ligament graft in a goat model. The American journal of sports medicine. 2001;29:620–626. doi: 10.1177/03635465010290051501. [DOI] [PubMed] [Google Scholar]
- 37.van Eck CF, Schkrohowsky JG, Working ZM, Irrgang JJ, Fu FH. Prospective analysis of failure rate and predictors of failure after anatomic anterior cruciate ligament reconstruction with allograft. The American journal of sports medicine. 2012;40:800–807. doi: 10.1177/0363546511432545. [DOI] [PubMed] [Google Scholar]
- 38.Wasserstein D, Sheth U, Cabrera A, Spindler KP. A Systematic Review of Failed Anterior Cruciate Ligament Reconstruction With Autograft Compared With Allograft in Young Patients. Sports health. 2015;7:207–216. doi: 10.1177/1941738115579030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ellis HB, Matheny LM, Briggs KK, Pennock AT, Steadman JR. Outcomes and revision rate after bone-patellar tendon-bone allograft versus autograft anterior cruciate ligament reconstruction in patients aged 18 years or younger with closed physes. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2012;28:1819–1825. doi: 10.1016/j.arthro.2012.06.016. [DOI] [PubMed] [Google Scholar]
- 40.Kraeutler MJ, Bravman JT, McCarty EC. Bone-patellar tendon-bone autograft versus allograft in outcomes of anterior cruciate ligament reconstruction: a meta-analysis of 5182 patients. The American journal of sports medicine. 2013;41:2439–2448. doi: 10.1177/0363546513484127. [DOI] [PubMed] [Google Scholar]
- 41.Mehta VM, Mandala C, Foster D, Petsche TS. Comparison of revision rates in bone-patella tendon-bone autograft and allograft anterior cruciate ligament reconstruction. Orthopedics. 2010;33:12. doi: 10.3928/01477447-20091124-15. [DOI] [PubMed] [Google Scholar]
- 42.Rappe M, Horodyski M, Meister K, Indelicato PA. Nonirradiated versus irradiated Achilles allograft: in vivo failure comparison. The American journal of sports medicine. 2007;35:1653–1658. doi: 10.1177/0363546507302926. [DOI] [PubMed] [Google Scholar]
- 43.Stringham DR, Pelmas CJ, Burks RT, Newman AP, Marcus RL. Comparison of anterior cruciate ligament reconstructions using patellar tendon autograft or allograft. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 1996;12:414–421. doi: 10.1016/s0749-8063(96)90034-1. [DOI] [PubMed] [Google Scholar]
- 44.Chang SK, Egami DK, Shaieb MD, Kan DM, Richardson AB. Anterior cruciate ligament reconstruction: allograft versus autograft. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2003;19:453–462. doi: 10.1053/jars.2003.50103. [DOI] [PubMed] [Google Scholar]
- 45.Indelicato PA, Linton RC, Huegel M. The results of fresh-frozen patellar tendon allografts for chronic anterior cruciate ligament deficiency of the knee. The American journal of sports medicine. 1992;20:118–121. doi: 10.1177/036354659202000204. [DOI] [PubMed] [Google Scholar]
- 46.Lamblin CJ, Waterman BR, Lubowitz JH. Anterior cruciate ligament reconstruction with autografts compared with non-irradiated, non-chemically treated allografts. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2013;29:1113–1122. doi: 10.1016/j.arthro.2013.01.022. [DOI] [PubMed] [Google Scholar]
- 47.Lawhorn KW, Howell SM, Traina SM, Gottlieb JE, Meade TD, Freedberg HI. The effect of graft tissue on anterior cruciate ligament outcomes: a multicenter, prospective, randomized controlled trial comparing autograft hamstrings with fresh-frozen anterior tibialis allograft. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2012;28:1079–1086. doi: 10.1016/j.arthro.2012.05.010. [DOI] [PubMed] [Google Scholar]
- 48.Mariscalco MW, Magnussen RA, Mehta D, Hewett TE, Flanigan DC, Kaeding CC. Autograft versus nonirradiated allograft tissue for anterior cruciate ligament reconstruction: a systematic review. The American journal of sports medicine. 2014;42:492–499. doi: 10.1177/0363546513497566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mayr HO, Willkomm D, Stoehr A, et al. Revision of anterior cruciate ligament reconstruction with patellar tendon allograft and autograft: 2- and 5-year results. Archives of orthopaedic and trauma surgery. 2012;132:867–874. doi: 10.1007/s00402-012-1481-z. [DOI] [PubMed] [Google Scholar]
- 50.Scheffler SU, Schmidt T, Gangey I, Dustmann M, Unterhauser F, Weiler A. Fresh-frozen free-tendon allografts versus autografts in anterior cruciate ligament reconstruction: delayed remodeling and inferior mechanical function during long-term healing in sheep. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2008;24:448–458. doi: 10.1016/j.arthro.2007.10.011. [DOI] [PubMed] [Google Scholar]
- 51.Shino K, Inoue M, Horibe S, Hamada M, Ono K. Reconstruction of the anterior cruciate ligament using allogeneic tendon. Long-term followup. The American journal of sports medicine. 1990;18:457–465. doi: 10.1177/036354659001800502. [DOI] [PubMed] [Google Scholar]
- 52.Group M. Effect of graft choice on the outcome of revision anterior cruciate ligament reconstruction in the Multicenter ACL Revision Study (MARS) Cohort. The American journal of sports medicine. 2014;42:2301–2310. doi: 10.1177/0363546514549005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Dunn WR, Spindler KP. Predictors of activity level 2 years after anterior cruciate ligament reconstruction (ACLR): a Multicenter Orthopaedic Outcomes Network (MOON) ACLR cohort study. The American journal of sports medicine. 2010;38:2040–2050. doi: 10.1177/0363546510370280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Barber-Westin SD, Noyes FR, Andrews M. A rigorous comparison between the sexes of results and complications after anterior cruciate ligament reconstruction. The American journal of sports medicine. 1997;25:514–526. doi: 10.1177/036354659702500415. [DOI] [PubMed] [Google Scholar]
- 55.Ferrari JD, Bach BR, Jr, Bush-Joseph CA, Wang T, Bojchuk J. Anterior cruciate ligament reconstruction in men and women: An outcome analysis comparing gender. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2001;17:588–596. doi: 10.1053/jars.2001.24686. [DOI] [PubMed] [Google Scholar]
- 56.Ryan J, Magnussen RA, Cox CL, Hurbanek JG, Flanigan DC, Kaeding CC. ACL reconstruction: do outcomes differ by sex? A systematic review. The Journal of bone and joint surgery. American volume. 2014;96:507–512. doi: 10.2106/JBJS.M.00299. [DOI] [PubMed] [Google Scholar]
- 57.Salmon L, Russell V, Musgrove T, Pinczewski L, Refshauge K. Incidence and risk factors for graft rupture and contralateral rupture after anterior cruciate ligament reconstruction. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2005;21:948–957. doi: 10.1016/j.arthro.2005.04.110. [DOI] [PubMed] [Google Scholar]