

Abstract
Objective
Evaluate the effect of providing choice of treatment alternatives to patients who fail to engage in or drop out of intensive outpatient programs (IOPs) for substance dependence.
Methods
Alcohol and/or cocaine dependent patients (N=500) participated in a sequential multiple assignment randomized trial (SMART). Those who failed to engage in IOP at week 2 (N=189) or who dropped out after engagement (N= 84) were randomized to motivational interviewing (MI) telephone calls that focused on engagement in IOP (MI-IOP) or provided a choice of IOP or three treatment options (MI-PC, or patient choice). Those not engaged at both 2 and 8 weeks (N=102) were re-randomized to MI-PC or no further outreach. Outcomes were treatment attendance and measures of alcohol and cocaine use obtained at 1, 2, 3, and 6 months.
Results
MI-PC produced better attendance than comparison conditions in patients who dropped out after initial engagement and in those re-randomized at 8 weeks. However, contrary to study hypotheses, MI-IOP produced significantly better alcohol use outcomes than MI-PC in alcohol dependent patients not engaged at week 2. There were no other significant differences between treatment conditions on other main effect analyses with alcohol or cocaine outcome measures.
Conclusion
Providing treatment options via telephone calls to patients who failed to engage in IOP did not produce better substance use outcomes than outreach calls focused on engagement in IOP. Future research should investigate the potential benefits of choice at other points in treatment (i.e., at intake) or other combinations of treatments.
Keywords: SMART study design, sequential randomization, alcohol dependence, cocaine dependence, treatment choice, motivational interviewing, medication management, CBT, telephone
There is a growing belief that patient preferences should be taken into consideration in the selection of treatment interventions. For example, patient preferences and shared decision making between patients and health care providers figure prominently in current disease management models (Wagner et al., 2001) and in the VA/DoD Substance Use Disorder Clinical Practice Guidelines (2009). Moreover, patients increasingly prefer an active role in treatment decisions (Chewning et al., 2012). Client choice and shared decision making may have a number of benefits, including higher satisfaction, increased treatment completion rates, better adherence, and improved clinical outcomes (Lindhiem, Bennettt, Trentacosta, & McLear, 2014).
Self-Determination Theory (Ryan & Deci, 2000), which has focused on identifying the conditions that facilitate intrinsic or self-motivation, provides a strong theoretical rationale for the importance and impact of client choice in treatment approaches. According to this theory, self-motivation and overall personal well-being require feelings of competence, social relatedness, and autonomy. Notably, competence alone will not increase intrinsic motivation unless it is paired with a sense of autonomy (Ryan & Deci, 2000). In fact, studies have indicated that choice and opportunities for self-direction increase intrinsic motivation by supporting autonomy (Deci & Ryan, 1985). Providing choice in treatment options could therefore be a vehicle for increasing clients’ intrinsic motivation to commit to and persevere with treatment.
However, individuals seeking treatment for substance use disorders typically have little sense of autonomy or choice in the type of treatment they receive. The vast majority of outpatient addiction treatment consists of traditional abstinence-oriented group therapy interventions based on the principles of Alcoholics Anonymous (AA) (McLellan, Carise, & Kleber, 2003). Although this kind of intervention is effective for many individuals, some do not respond well, as evidenced by high dropout rates and mixed substance use outcomes in these programs (SAMHSA, 2008). Moreover, key elements of standard treatment are perceived as problematic by many individuals. A study by Rapp et al. (2006) reported that the most frequently reported barriers to engagement in substance use disorder treatment following an intake appointment were: not liking to talk in groups (36.5%), not liking to talk about one’s personal life with other people (35.6%), difficulty getting to and from treatment (20.2%), belief that one can handle drug use problem without treatment (16.1%), and having had a bad experience in treatment (16%). According to Self-Determination Theory, choice may be particularly important for generating a sense of intrinsic motivation in clients receiving treatments for substance use disorders, which are often prompted by external factors such as pressure from family members, employers, or the criminal justice system (Ryan & Deci, 2000; Wild, Cunningham, & Ryan, 2006).
Research on the impact of choice and shared decision making in medical and psychiatric disorders has yielded mixed findings. In a meta-analysis of 32 studies (84% for medical disorders), preference was generally not related to outcome (King et al., 2005). Conversely, Swift and Callahan (2009) concluded that preference affected both outcome and dropout in 26 studies of treatments for psychiatric and substance use disorders. Moreover, a recent meta-analysis (Lindhiem et al., 2014) with 34 studies (66% for behavioral/psychiatric, 34% for medical disorders) found that clients who were involved in shared decision making, chose a treatment condition, or otherwise received preferred treatments had higher treatment satisfaction and completion rates, and better clinical outcomes than other clients.
There has been comparatively little research on the impact of patient choice on substance use disorder treatment outcomes. Alcohol abusing industrial workers randomized to hospital-based treatment had better drinking outcomes than those randomized to a choice of hospital treatment or AA (Walsh et al., 1991). In comparisons of IOP and residential treatment, cocaine and alcohol outcomes did not differ as a function of whether patients were randomly assigned to treatment condition, or were placed in these settings on the basis of patient or clinician preference (McKay et al., 1995, 1998). Similarly, outcomes of patients with alcohol dependence who received their preferred treatment did not differ from the outcomes of those who did not (Adamson et al., 2005). Conversely, offering alcohol dependent women a choice of individual vs. conjoint treatment increased the probability of entering treatment, although not treatment attendance (McCrady et al., 2011). Cocaine dependent patients allowed to choose the modality of treatment (individual vs. group) had fewer cocaine use days than those who were not give a choice of modality (Sterling et al., 1997). Finally, a shared decision making intervention for substance dependent patients produced better drug use and psychiatric severity outcomes than standard care (Joosten, de Jong, de Weert-van Oene, Sensky, & van der Staak, 2009).
The research literature on patient choice in treatment for substance use disorders has several notable limitations, in addition to the paucity of studies. None of the studies has allowed patients to choose between standard care and other contemporary interventions, such as CBT or addiction medications. Moreover, no study has directly examined the effect of patient choice when providing additional care to individuals who have not responded to standard treatment. This may be particularly important in the treatment of substance use disorders, where only one type of treatment is readily available (i.e., 12-step oriented, group counseling). Finally, prior studies have not examined the timing of patient choice; in other words, whether the potential impact of choice varies as a function of when it is offered.
The goal of the present study was to use a sequential multiple assignment randomized trial (SMART; Murphy et al., 2007) design to test the hypothesis that patients who enter addiction specialty care programs but fail to engage or drop out after a brief period of engagement will have better retention and substance use outcomes if outreach efforts include a choice of treatment options. Participants were recruited when they entered treatment at one of two intensive outpatient programs (IOPs), and their attendance was tracked for 8 weeks. We selected IOPs, as these programs are now the most common form of treatment for individuals with more severe substance use disorders. Patients who failed to engage in IOP by the 2 week point were randomized to two telephone motivational interviewing (MI; Miller & Rollnick, 2013)-based outreach efforts, one of which was focused on helping the patient to engage in the IOP (MI-IOP), whereas the other included a choice of IOP or three other treatment options (MI-PC, or patient choice). The other options were individual cognitive-behavioral therapy (CBT), telephone-based stepped care, and medication management.
The IOP option was provided for patients who still preferred IOP, despite failure to engage initially in that approach. Each of the other options was selected to address common criticisms of IOP (Rapp et al., 2006). CBT was included to provide an individual, as opposed to group, approach. Moreover, CBT has a different purported mechanism of action than the traditional AA-oriented approach of the IOP, and therefore might be effective when IOP was not. Telephone stepped care provided a lower intensity, lower burden option for patients who either did not want or had difficulty coming to a clinic-based program three times per week. Finally medication management was included for those who preferred a medical approach that combined pharmacotherapy with a lower level behavioral intervention. It should be noted that all three alternatives to IOP were lower intensity treatment approaches, compared to IOP.
Patients who were engaged in IOP at two weeks were followed for another six weeks. If they stopped attending IOP for two consecutive weeks during that period, they were randomized to receive either MI-IOP or MI-PC. At the 8-week point, patients who had not been engaged at both 2 and 8 weeks were re-randomized to receive either MI-PC or no further outreach efforts. The data analyses compared the two treatment options in patients who were (a) not engaged at 2 weeks, (b) engaged at 2 weeks but disengaged during weeks 3–8, and (c) were not engaged at both week 2 and week 8. The outcomes were measures of alcohol and cocaine use, and weeks of treatment engagement. The MI-PC condition was hypothesized to yield better engagement and substance use outcomes than MI-IOP in the first two analyses, and better engagement and substance use outcomes than no further outreach in the third analysis.
Method
Participants
The participants were 500 adults enrolled in one of two intensive outpatient programs in Philadelphia (a publicly funded program and a Veterans Affairs program) who met criteria for DSM-IV alcohol or cocaine dependence (lifetime or current) and had used alcohol or cocaine within the past 3 months. The other criteria for eligibility were a willingness to participate in research and be randomly assigned; no psychiatric or medical condition that precluded outpatient treatment (i.e., severe dementia, current auditory or visual hallucinations); between the ages of 18 and 65; no regular IV heroin use within the past 12 months; ability to read at approximately the 4th grade level; and at least a minimum degree of stability in living situation (e.g., not living on the street). To facilitate follow-up, participants had to be able to provide the names, addresses, and telephone numbers of at least two contacts.
The study sample was drawn from two parallel studies done concurrently at the same treatment programs that recruited cocaine dependent (N=300) or alcohol dependent (N=200) patients. Given that the studies had the same design, and that 76% of participants in the cocaine study also had alcohol dependence and 40% of those in the alcohol study also had cocaine dependence, the study samples were combined for this report. Of the 500 participants, 428 had alcohol dependence (288 current, 140 lifetime), 409 had cocaine dependence (283 current, 126 lifetime), 195 had current dependence on both alcohol and cocaine, 69 had lifetime dependence on both alcohol and cocaine, 90 had current or lifetime alcohol dependence but no cocaine dependence, and 71 had current or lifetime cocaine dependence but no alcohol dependence.
The participants averaged 48.3 (sd=8.9) years of age and most were male (81%), African American (88.8%), and not currently married (85%). Seventy-seven percent of the participants had completed high school or obtained a GED, and 32% had some post secondary school education. The participants averaged 2.8 (sd= 4.4) prior treatments for alcohol problems, and 3.5 (sd=4.6) treatments for drug problems.
Intensive Outpatient Treatment
Both IOPs provided approximately 9 hours of group-based treatment per week, and patients could typically attend for up to 3 months. Treatment at both sites was focused on overcoming denial, fostering participation in self-help groups, and providing information about the process of addiction and cues to relapse (McKay, Van Horn, Oslin, et al., 2010).
Motivational Interviewing Telephone Calls
Non-engaged patients received two MI (Miller & Rollnick, 2013) telephone sessions of up to one hour each. In the MI-IOP condition, the goal of the sessions was to facilitate re-engagement in IOP. In the MI-PC condition, the goal of the sessions was to help the patient choose and engage in one of the four treatment options outlined earlier. In both treatment conditions, the therapist opened the dialogue by introducing him/herself, orienting the patient to the purpose of the call, and determining whether the patient could participate in the call at that time. Consistent with an MI approach, the style and “spirit” of the intervention was emphasized over specific techniques. However, a typical call included discussion of the reasons the patient sought and discontinued treatment; the patient’s current intentions regarding alcohol and drug use with a focus on increasing motivation to achieve or maintain abstinence; the patient’s thoughts about what might be most helpful at this time; and troubleshooting practical barriers to treatment. In MI-PC, treatment options were then presented, with an effort made to tailor the message to the patient’s stated needs and barriers. Whether or not the patient committed to treatment participation by the end of the call, the therapist offered a follow-up call up to one week later to check in and continue building motivation or troubleshooting as needed.
Treatment Options in MI-PC
Cognitive-behavioral therapy (CBT)
Patients received up to 12 weekly individual CBT sessions (Carroll, 1998), delivered in our clinical research space or at the VAMC.
Telephone stepped care (TSC)
Patients had an initial in person orientation session with their study counselor, followed by weekly telephone calls (20–30 minutes each). Each call began with an assessment of risk and protective factors encountered since the last call, and a discussion of upcoming high-risk situations. This information was used to select a target to be addressed in the remainder of the call, usually the issue most likely to lead to relapse in the following week. A coping response for this issue or situation was then identified and rehearsed (see McKay, Van Horn, & Morrison, 2010). Patients who continued to use alcohol or drugs could be stepped up to more frequent calls or in-person clinic sessions.
Medication management (MM)
Patients met weekly with a nurse, who delivered the manualized protocol (Oslin et al., 2014). Initially, we offered modafinil to patients with cocaine dependence, and naltrexone to those with alcohol dependence. However, after results from two negative modafinil studies were reported early in the recruitment period (Anderson et al., 2009; Dackis et al., 2012), we discontinued this medication. Eighty-six percent of patients in the study were alcohol dependent, and they were offered naltrexone, which has been shown to be effective in reducing heavy drinking (Rosner et al., 2010). Patients who were dependent on cocaine only were offered one of the other three treatment options (e.g., IOP, CBT, or TSC).
Therapists
The MI calls were provided by 5 therapists (two women and three men), each of whom delivered both the IOP and PC forms of the intervention. These therapists also provided the CBT and telephone stepped care when these intervention were selected in MI-PC. Therapists had prior experience with providing outpatient treatment for substance use disorders, ranging from 1 to 20 years. They were previously trained to criterion in delivery of CBT and telephone stepped care in prior studies, and received 2 days of workshop training and ongoing supervision in MI for the present study. Three therapists had MA-level degrees in psychology or social work and two had a Ph.D. in clinical psychology. The behavioral components of the medication management condition were provided by a nurse or psychologist at the VA or our clinical research clinic, with prescriptions for medication provided by a psychiatrist.
Adherence to Treatment Protocols
The MI calls and CBT and telephone-stepped care treatment interventions were audio-taped to facilitate supervision and monitor adherence to the protocol as described in the manuals. Supervision was provided weekly by the study clinical coordinator, and one group supervision session was also held per week in which therapeutic issues were discussed with the senior clinical research staff on the project. Any deviations from the treatment protocol identified by the clinical coordinator were immediately addressed in the weekly supervision meetings.
Approximately 25% of the initial MI calls were rated for adherence using the MI Treatment Integrity rating scales version 3.1.1 (MITI; Moyers, Martin, Manuel, Hendrickson, & Miller, 2005; Moyers, Martin, Manuel, Miller, & Ernst, 2010). MITI ratings include tallies of therapist utterances, simple and complex reflections, MI-adherent and MI-nonadherent behavior, and giving information; and global ratings of evocation, collaboration, autonomy support, empathy, and direction on a scale of 1–5. Ratings are combined into several indices with thresholds representing Basic Competency and Proficiency in MI practice.
Procedures
Recruitment
Potential participants at the community program were screened on or within a few days of their intake appointment by the study research technicians. At the VA facility, patients were screened at the first of two group orientation sessions that they attended following their intake appointment, prior to starting in IOP. Those who were eligible at each site completed informed consent procedures, which included a quiz to ensure that they understood the study process. The baseline assessment was initiated and completed after informed consent was obtained. The study was conducted in compliance with the policies of the Institutional Review Boards of the University of Pennsylvania and the Philadelphia VAMC. Participants were recruited between October 2008 and April 2012.
Representativeness of the study sample
Of the 865 patients screened for participation in the study (417 at the community program and 448 at the VA), 500 were eligible and willing to participate and were enrolled in the study (see Figure 1). Reasons for failure to enter the study were: met inclusion criteria but failed to attend first baseline interview (N=92); had not used alcohol or cocaine in the three months prior to baseline (N=76); were injecting opiates in 3 months prior to baseline (N=49); intake date was more than 7 days prior to screening (N=36); not interested in participating (N=29); did not meet DSM-IV criteria for cocaine or alcohol dependence (N=21); already completed study (N=12); participating in other SUD treatment (N=8); not between the ages of 18 and 75 (N=7); unable to read/comprehend (N=7); unable to provide at least three contacts (N=5); considered a prisoner/court appointed to treatment (N=5); prohibited by recovery house from participating in research (N=5); had not been a Philadelphia resident for at least three months prior to baseline (N=4); had an acute medical problem that requires inpatient treatment (N=4); currently participating in another research program (N=4); and had an untreated/poorly managed psychiatric disorder or dementia (N=1).
Figure 1.
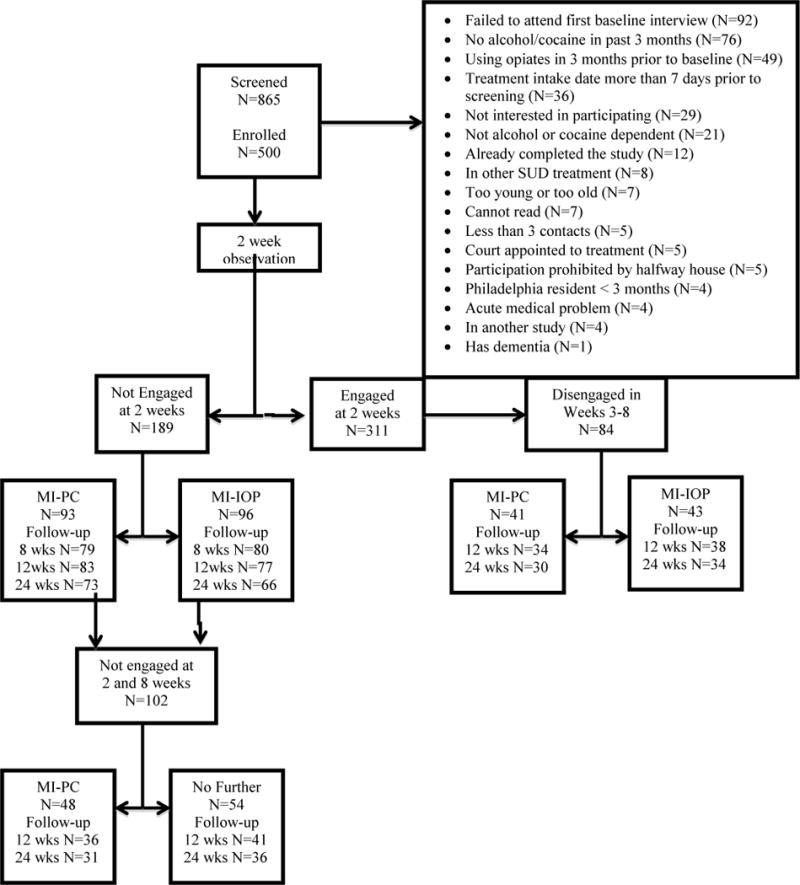
Consort Diagram. MI-PC= Motivational Interviewing-Patient Choice; MI-IOP= Motivational Interviewing-Intensive Outpatient Program. “Follow-up” refers to number of participants providing data at each follow-up point.
Determining engagement status
At the publicly funded program, patients entered the IOP within a few days of intake. Those who failed to attend 2 or more of their IOP sessions in week 2 were considered not engaged at the 2-week point. The intake process at the VA program was more complicated. Following intake, patients were required to attend two weekly orientation sessions before starting in the IOP. Therefore, at the VA, patients who failed to attend the second orientation and the first scheduled IOP session were considered not engaged at 2 weeks. In both programs, initially engaged patients who failed to attend any IOP sessions for two consecutive weeks between weeks 3 and 8 were considered not engaged at that point. Finally, patients who were not engaged at 2 weeks and failed to attend any IOP session in weeks 7 and 8 were considered still not engaged, and were included in the second randomization.
Randomization procedures
Separate randomized allocation schemes were used within each site. In each scheme, a blocked randomization scheme, using blocks of size 30, was used to yield a balanced allocation of participants to the three treatment groups. The study statistician, Kevin G. Lynch, generated the sequences. The assignments were placed in envelopes, and the sequence was concealed until the point of randomization.
Baseline and follow-up assessments
Baseline assessments were administered as soon as possible after informed consent was obtained. The follow-up assessments were conducted at 4, 8, 12, and 24 weeks post baseline. Participants received $30 for completing the baseline research sessions, and $40 per visit for completing each the four follow-up sessions. All study interviews were conducted by research personnel who had received extensive training in the use of the assessment instruments and were closely monitored during the course of the study.
Follow-up rates
The Consort diagram (see Figure 1) presents data on follow-up rates in the 273 participants in the full sample who were classified as disengaged at some point. Analyses compared follow-up rates separately within the alcohol and cocaine dependent samples. Among participants not engaged at 2 weeks, follow-up rates in MI-PC and MI-IOP did not differ (alcohol group p= .57, cocaine group p= .15). Among participants who disengaged between weeks 3 and 8, follow-up rates in MI-PC and MI-IOP did not differ (alcohol group p= .30, cocaine group p= .33). Finally, among those not engaged at 2 and 8 weeks, follow-up rates in MI-PC and no further outreach did not differ (alcohol group p= .72, cocaine group p= .33).
Measures
Psychiatric diagnoses
The Structured Clinical Interview for DSM-IV (SCID) (First et al., 1996) was administered at baseline to to determine cocaine and alcohol substance use disorder diagnoses and rule out any psychiatric disorders that would preclude study participation.
Self-reported alcohol and cocaine use
Time-line follow-back (TLFB) (Sobell, Maisto, Sobell, & Cooper, 1979) calendar assessment techniques were used to gather self-reports of alcohol and cocaine use during the 2 months preceding entrance into IOP and the 24 week follow-up period. In validity studies with drug abusers, TLFB reports of days of cocaine use were highly correlated with urine toxicology results (Ehrman & Robbins, 1994; Fals-Stewart et al., 2000). Moreover, TLFB reports of alcohol use have generally correlated .80 or better with collateral reports (Maisto, Sobell, & Sobell, 1979; Sobell, Sobell, Leo, & Cancilla, 1988; Stout, Beattie, Longabaugh, & Noel, 1989). Self-reports of alcohol use in the context of a research study have been found to have high validity (Babor, Steinberg, Anton, & Del Boca, 2000).
Urine toxicology
Urine samples obtained at baseline and at each follow-up point were tested for the cocaine metabolite benzoylecgonine using either the Emit assay system or FPIA analysis (with quantitative output converted to a dichotomous variable).
Outcome measures
The primary outcomes were measures of alcohol and drug use within each 30-day period of the follow-up. For participants with alcohol dependence (N= 428), the outcomes were dichotomous measures of any alcohol and any heavy alcohol use, and continuous measures of percent days alcohol and heavy alcohol use from the TLFB. Heavy alcohol use was defined as ≥ 5 drinks in a day for men, ≥ 4 drinks for women. For participants with cocaine dependence (N= 409), the outcomes were a dichotomous measure of any cocaine use and percent days cocaine use from the TLFB, and cocaine urine toxicology.
Treatment participation
Data on attendance in IOP, MI telephone calls, and additional interventions provide in MI-PC were obtained from counselors reports and review of IOP attendance records. These data were used to construct the primary attendance measure, a binary variable (attended any SUD treatment: yes/no) for each week in the 10 weeks following the week 2 randomization,. Number of sessions of each type of treatment was also calculated.
Data Analyses
Differences between the conditions at baseline were evaluated with one-way nonparametric ANOVAs (continuous measures) and chi-square tests (categorical measures). Treatment differences in number of days on which intensive outpatient treatment sessions were received were also evaluated with one-way ANOVAs.
Generalized estimating equations models (GEE; SAS PROC GENMOD) were used to compare the study groups on the outcomes. Participants with alcohol dependence were included in analyses to predict the alcohol outcomes, and those with cocaine dependence were included in analyses to predict cocaine outcomes. The TLFB data were collapsed into a pre-treatment baseline period (2 months prior to baseline) and six follow-up periods (months 1, 2, 3, 4, 5, and 6). Urine toxicology data were obtained at baseline and 1, 2, 3, and 6 months. Analyses of participants non-engaged at 2 weeks included outcome data collected after that point, analyses of participants disengaged between weeks 3–8 included outcome data from week 8 to week 26, and analyses of those re-randomized at week 8 included outcome data after week 8.
A compound symmetry/exchangeable working covariance structure was used for these models, and empirical standard errors were used for the analyses. Compound symmetry assumes that the within-subject correlation between any two time points is the same, which was a good fit with the data and is a reasonable choice of working correlation matrix within the GEE framework (Fitzmaurice, Laird, & Ware, 2011). Time was modeled as a categorical factor. Dichotomous variables representing site (VA vs. community), study (cocaine vs. alcohol), and substance use diagnosis (current vs. lifetime) were included in each analysis, and any significant interactions between these variables and treatment condition were reported.
Preliminary analyses indicated that at the two randomizations, the treatment conditions did not differ on gender, race, age, or % days alcohol or cocaine use at baseline (all p > .30). Therefore, these variables were not included as covariates in the analyses. Effects of missing outcome data were evaluated by comparing the primary GEE analyses to parallel mixed effects models, which are more sensitive to the effects of missing data; examining relations between baseline study variables and missing data; and conducting pattern mixture analyses.
Results
Engagement Results
Alcohol dependent participants
Of 428 patients with alcohol dependence, 267 were engaged at the two-week point, and 161 were not. Of the 267 patients engaged at 2 weeks, 73 became disengaged between weeks 3 and 8. Of the 161 who were not engaged at 2 weeks, 86 were not engaged at 8 weeks, and were re-randomized.
Cocaine dependent participants
Of 409 patients with cocaine dependence, 250 were engaged at the two-week point, and 159 were not. Of the 250 patients engaged at 2 weeks, 69 became disengaged between weeks 3 and 8. Of the 159 who were not engaged at 2 weeks, 84 were not engaged at 8 weeks, and were re-randomized.
Treatment Selection in MI-PC
Among the 136 patients randomized to MI-PC at week 2 who were disengaged at that point or who disengaged prior to week 8, the most frequent treatments chosen were IOP (N=47) and CBT (N=24). Conversely, very few patients opted for telephone stepped care (N=6), or medication management (N=2). Another 58 patients said they did not wish to continue with any treatment, or were unreachable. Of the 48 patients who were randomized to MI-PC at week 8, 9 selected CBT, 6 selected IOP, 5 selected telephone stepped care, and 3 selected medication management. The other 25 patients did not want further treatment or were not reached.
Motivational Interviewing Adherence Analyses
A convenience sample of 57 initial MI outreach calls of at least 5 minutes’ duration (26 MI-IOP and 31 MI-PC) was rated for adherence to MI style and spirit. Ratings are presented in Table 1. On average, MITI scores met or exceeded Basic Competency thresholds (Moyers et al., 2010). There were no differences between treatment conditions on any of the MITI global scales, behavior count ratios, or underlying behavior counts, with one exception: the frequency of giving information, a behavior count that is not assigned a threshold level nor included in any of the behavior count ratios reflecting MI proficiency. On average, therapists gave information 6.1 (SD = 4.6) times in MI-IOP calls, whereas in MI-PC calls, they gave information 9.4 (SD = 4.9) times, t(55) = −2.60, p = .01, d= .69. P-values for other comparisons ranged from .07 to .98.
Table 1.
Motivational Interviewing treatment fidelity ratings
| Variable | Mean | Standard Deviation |
|---|---|---|
| MITI Global Scales | ||
| Evocation | 4.00 | 0.42 |
| Collaboration | 3.93 | 0.41 |
| Autonomy Support | 3.96 | 0.44 |
| Direction | 4.83 | 0.37 |
| Empathy | 3.95 | 0.34 |
| Spirit Composite | 3.96 | 0.38 |
| MITI Behavior Count Ratios | ||
| Percent Complex Reflections | 55.70 | 14.46 |
| Percent Open Questions | 48.62 | 20.20 |
| Reflection to Question Ratio | 1.23 | 1.09 |
| Percent MI Adherent | 95.23 | 10.67 |
Note: MITI = Motivational Interviewing Treatment Integrity Scales
Treatment Participation
Among patients who were not engaged at week 2, MI-PC and MI-IOP did not differ on number of treatment sessions in weeks 3–12 weeks [m= 3.92 (sd=3.27) in MI-PC vs. m= 3.50 (sd=3.23) in MI-IOP; chi-square (1)= 2.57, p= .11, d= .13]. Among patients who disengaged between weeks 3 and 8, those in MI-PC attended more treatment sessions over weeks 9–12 than those in MI-IOP [m=1.28 (sd=1.55) vs. m= 0.76 (sd=1.25); chi-square (1)= 5.05, p= .02, d= .37]. Among patients disengaged at both weeks 2 and 8, those in MI-PC attended more treatment sessions in weeks 9–12 than those receiving no further outreach, although rates of attendance were very low in both conditions [m= 0.58 (sd=1.11) vs. m= 0.30 (sd= .76); chi-square (1)= 7.79, p= .005, d= .30].
Covariate Effects
There were no significant effects for study (i.e., alcohol vs. cocaine). With regard to site, outcomes for alcohol dependent patients were significantly better in the VA than in the community program on all four alcohol outcomes (disengaged at 2 weeks: p= .006 to .04; disengaged at both 2 and 8 weeks: p= .006 to .04). Site was not significant in any other analysis. Substance use outcomes were consistently worse in those with current, as opposed to lifetime, alcohol or cocaine dependence. For example, in those not engaged at 2 weeks, p values ranged from .006 to .04 for the alcohol measures and from .0001 to .003 for the cocaine measures. However, none of these factors interacted significantly with treatment condition, unless noted below.
Alcohol Outcomes in Alcohol Dependent Patients
Among patients who were not engaged at 2 weeks, those in MI-IOP were less likely than those in MI-PC to have months with any drinking days during the follow-up (OR= 0.40, p= .0007) and to have months with any heavy drinking days (OR= 0.33, p= .0001) (see Table 2). Rates of any and heavy drinking in a given month were about 20–25 percentage points lower in MI-IOP than in MI-PC at each point in the follow-up (see Figure 2). Frequencies of drinking days (d= −.39, beta= −1.08, p= .01) and heavy drinking days (d= −.40, beta= −1.09, p= .003) were also lower in MI-IOP than in MI-PC (See Table 1 and Figure 3). Among the 73 initially engaged patients who disengaged between weeks 3–8, MI-IOP and MI-PC did not differ on any of the outcomes (see Table 2).
Table 2.
Treatment group comparisons in alcohol dependent patients
| Group | Outcome | N | Chi-Square | P | OR/BETA(d) | CI |
|---|---|---|---|---|---|---|
| Not en-gaged at 2 weeks | Any Drinking | 161 | 11.41 | .0007 | 0.40 | 0.23 0.68 |
| Any Heavy Drinking | 161 | 14.50 | .0001 | 0.33 | 0.19 0.58 | |
| % Days Drinking | 161 | 6.74 | .009 | −1.08 (d= −.39) | −1.87 −0.29 | |
| % Days Heavy Drinking | 161 | 8.60 | .003 | −1.09 (d= −.40) | −1.80 −0.39 | |
| Disengaged weeks 3–8 | Any Drinking | 73 | 2.00 | .16 | 0.54 | 0.23 1.27 |
| Any Heavy Drinking | 73 | 0.85 | .36 | 0.67 | 0.29 1.54 | |
| % Days Drinking | 73 | 1.44 | .23 | −0.84 (d= −.32) | −2.20 0.52 | |
| % Days Heavy Drinking | 73 | 2.54 | .10 | −1.03 (d= −.39 | −2.26 0.21 | |
| Disengaged at weeks 2 and 8 | Any Drinking | 86 | 0.07 | .79 | 1.12 | 0.48 2.60 |
| Any Heavy Drinking | 86 | 0.57 | .45 | 1.43 | 0.58 3.54 | |
| % Days Drinking | 86 | 0.30 | .58 | −0.34 (d= −.25) | −1.52 0.85 | |
| % Days Heavy Drinking | 86 | 0.00 | .97 | 0.02 (d= −.04) | −1.10 1.14 |
Treatment contrasts for MI-IOP vs. MI-PC coded as MI-IOP=1; MI-PC=0. Contrasts for MI-PC vs. no further outreach coded as MI-PC=1; no further outreach= 0.
Models include binary indicators of Site (VA versus nonVA), Study (P01 versus P60), and a nominal indicator for study month.
Effect sizes are indicated by Odds Ratios (OR) for the dichotomous outcomes and BETA and Cohen’s d values for continuous outcomes. CI= confidence intervals
Figure 2.
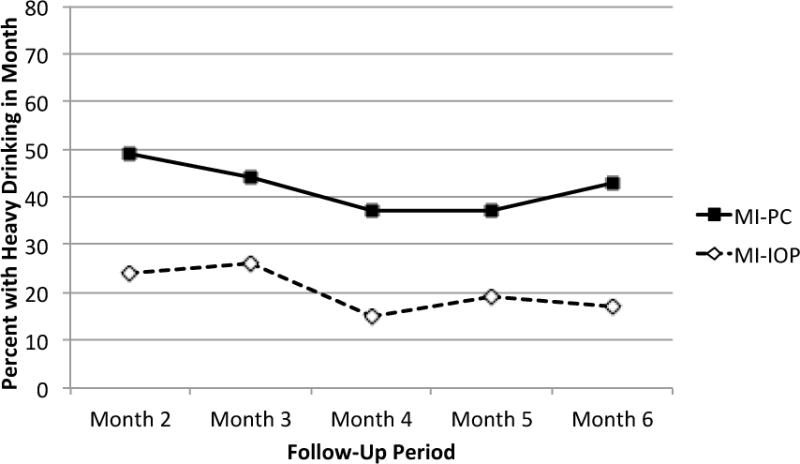
Rates of any heavy drinking days in the prior 30 days in alcohol dependent patients not engaged at 2 weeks. MI-PC= Motivational Interviewing-Patient Choice; MI-IOP= Motivational Interviewing- Intensive Outpatient Program
Figure 3.
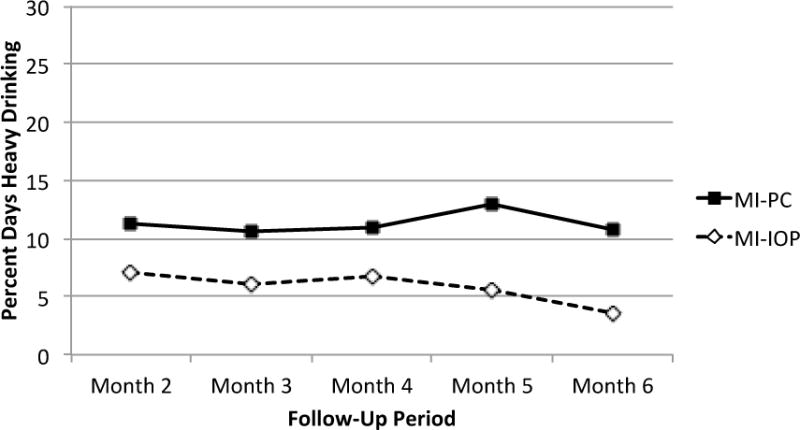
Frequency of heavy drinking days in the prior 30 days in alcohol dependent patients not engaged at 2 weeks. MI-PC= Motivational Interviewing-Patient Choice; MI-IOP= Motivational Interviewing- Intensive Outpatient Program
In the 86 patients who were disengaged at both week 2 and week 8, there were no significant treatment condition main effects on the alcohol outcomes (See Table 2). However, the treatment condition × time interactions were significant with any heavy drinking [chi-square (3)=8.50, p= .04] and frequency of drinking days [chi-square (3)= 9.37, p= .02] and reached the level of a trend with any drinking [chi-square (3)= 7.17, p= .07] and frequency of heavy drinking days [chi-square (3)= 6.96, p= .07]. In the two significant interactions, MI-PC produced worse drinking outcomes than no further outreach initially (i.e., months 3 and 4 with any heavy drinking; month 3 with drinking days), but better outcomes than no further outreach in subsequent months (i.e., months 5 and 6 for any heavy drinking; months 4, 5, and 6 for days drinking). These results suggested a delayed onset of treatment effects. However, none of the treatment group comparisons at any of the time points was significant (i.e., all p> .05).
In addition, a significant treatment × alcohol dependence diagnosis interaction [chi-square (1)= 4.56, p= .03] was obtained on presence of any drinking days, in which MI-PC was superior to no further outreach in patients with only a lifetime dependence diagnosis (OR=0.19, p=0.08), whereas the reverse was true for those with a current diagnosis (OR=1.85, p=0.22). A similar interaction [chi-square (1)= 3.90, p= .05] was obtained on presence of heavy drinking days: MI-PC was superior to no further outreach in patients with only a lifetime dependence diagnosis (OR=0.22, p=0.16), whereas the reverse was true for those with a current diagnosis (OR=2.14, p=0.15). This treatment × alcohol dependence diagnosis interaction was not significant with frequency of any (p= .11) or heavy (p= .12) drinking days, although similar patterns were observed for these outcomes.
Cocaine Outcomes in Cocaine Dependent Patients
Among patients who were not engaged at 2 weeks, MI-IOP and MI-PC did not differ on months with any self-reported cocaine use (OR= 0.66, p= .13), frequency of cocaine use (d= −.04, beta= −0.13, p= .75) or on cocaine urine toxicology outcomes (OR=1.05, p= .86) (See Table 3). Among the 69 patients who disengaged between weeks 3–8, the treatment conditions did not differ on months with any self-reported cocaine use (OR= 0.83, p= .71), frequency of cocaine use (d= −.37, beta= −0.84, p= .16), or cocaine urine toxicology (OR= 1.05, p= .74) (see Table 3).
Table 3.
Treatment group comparisons in cocaine dependent patients
| Group | Outcome | N | Chi-Square | P | OR/BETA(d) | CI |
|---|---|---|---|---|---|---|
| Not engaged at 2 weeks | Any Cocaine Use | 159 | 2.25 | .13 | 0.66 | 0.38 1.14 |
| % Days cocaine use | 159 | 0.10 | .75 | −0.13 (d= −.04) | −0.94 0.60 | |
| Cocaine urine toxicology | 159 | 0.03 | .86 | 1.05 | 0.61 1.80 | |
| Disengaged weeks 3–8 | Any Cocaine Use | 69 | 0.14 | .71 | 0.83 | 0.33 2.12 |
| % Days cocaine | 69 | 2.02 | .16 | −0.84 (d= −.37) | −1.98 0.30 | |
| Cocaine urine toxicology | 69 | 0.13 | .74 | 1.17 | 0.50 2.77 | |
| Disengaged at weeks 2 and 8 | Any Cocaine Use | 84 | 0.85 | .36 | 1.48 | 0.64 3.40 |
| % Days cocaine | 84 | 0.65 | .42 | 0.60 (d= .22) | −0.85 2.04 | |
| Cocaine urine toxicology | 84 | 2.20 | .14 | 2.00 | 0.82 – 4.91 |
Treatment contrasts for MI-IOP vs. MI-PC coded as MI-IOP=1; MI-PC=0. Contrasts for MI-PC vs. no further outreach coded as MI-PC=1; no further outreach= 0.
Models include binary indicators of Site (VA versus nonVA), Study (P01 versus P60), and a nominal indicator for study month.
Effect sizes are indicated by Odds Ratios (OR) for the dichotomous outcomes and BETA and Cohen’s d values for continuous outcomes. CI= confidence intervals
In the 84 patients who were disengaged at both week 2 and week 8, there were no significant treatment condition main effects on self-reported months with any cocaine use (OR= 1.48, p = .36), frequency of cocaine use (d= .22, beta= 0.60, p= .42), or cocaine urine toxicology (OR = 2.00, p= .13) (See Table 3). The interaction between treatment condition and cocaine dependence diagnosis reached the level of a trend with any cocaine use [chi-square (1)= 3.18, p= .07], but did not approach significance with frequency of cocaine use (p= .16) or with cocaine urine toxicology (p= .79). The interactions between treatment condition and time did not approach significance with any of the three outcome measures (p ≥ .23).
Analyses with Participants with Alcohol and Cocaine Dependence
The analyses described above were repeated with the 338 participants who were dependent on both alcohol and cocaine. The results were very similar to what was obtained in separate analyses of alcohol and cocaine dependent patients. In participants who were not engaged at 2 weeks, alcohol use outcomes were significantly better in MI-IOP than in MI-PC, with effect sizes similar to those in alcohol dependent participants only. There were no significant treatment group differences in the analyses of alcohol use outcomes in participants who engaged initially but dropped out in weeks 3–8 and in those who were not engaged at weeks 2 and 8, or in any of the analyses of cocaine use outcomes.
Missing Data Analyses
These analyses revealed little evidence of any effects due to missing data. Mixed effects models, which are more sensitive to missing data than GEE, generated the same results as the GEE analyses reported here, with one exception: a significant treatment group × time interaction (p= .04) on any heavy drinking in participants not engaged at 2 and 8 weeks was no longer significant in the mixed effects model (p= .14). All the pattern mixture models yielded non-significant results, with one analysis reaching the level of a trend (p= .06). This analysis suggested the effect on any heavy drinking days favoring MI-IOP over MI-PC in alcohol dependent participants not engaged at week 2 was somewhat larger in those with one or more missing follow-ups than in those who completed all follow-ups. No significant associations were found between baseline study variables and follow-up status.
Discussion
This study employed a sequential multiple assignment randomized trial (SMART; Murphy et al., 2007) design to evaluate the efficacy of providing a choice of alternative treatments to alcohol and cocaine dependent patients who failed to engage in IOP or who engaged but subsequently dropped out. In SMART designs, non-responders are randomized to two or more alternative conditions that either augment the current treatment or switch the patient to different treatment alternatives. Patients who are still not responding after the first randomization are re-randomized to other possible treatment options. Experimental procedures are therefore used to determine the best modification for patients who are not responding. The design in this study featured elements of both effectiveness and efficacy research, in that participants were recruited from “real world” treatment programs but the additional treatment elements (e.g., MI, CBT, Telephone stepped care, and medication management) were provided by research therapists/clinicians at alternative locations.
We hypothesized that providing motivational interviewing outreach telephone calls that gave patients a choice of several treatment options would produce better treatment attendance and substance use outcomes than MI calls focused on re-engagement in IOP. Contrary to our predictions, there was no advantage to MI with patient choice with regard to substance use outcomes, either for participants not engaged at 2 weeks, those who were initially engaged but dropped out between weeks 3 and 8, or for those disengaged at both week 2 and 8. In fact, with alcohol dependent participants, alcohol use outcomes in some analyses favored the condition focused on re-engagement in IOP. Moreover, providing choice to those not engaged at two weeks did not produce better treatment attendance than efforts to engage in IOP only, although there was better attendance in the choice conditions for those who disengaged between weeks 3 and 8.
It is conceivable that providing patients with choice of treatments could lead to higher rates of attendance but poorer substance use outcomes, if the alternative treatments were somehow more appealing or less burdensome, but not as strong therapeutically. There are hints of this in the present study, with some analyses indicating higher attendance rates in MI-PC. However, the number of sessions attended by those who disengaged between weeks 3 and 8 was low in both MI-PC and MI-IOP, and the difference likely not clinically significant. Therefore, the results across attendance and substance use measures indicate no real advantage to the choice condition.
We found that disengaged patients in the choice condition were most likely to select IOP over the other alternatives in the menu, and that there was virtually no interest in either telephone-based step care or medication management. The most popular treatment choice in patients who were contacted was IOP (60%), followed by CBT (30%). About half of the patients who were not engaged at both 2 and 8 weeks and were randomized to MI-PC at 8 weeks could not be reached or refused further treatment (52%). However, among the patients who did make a choice at that point, there was more balance in treatments selected.
It should be noted that most participants had been treated multiple times in traditional treatment programs. Offering other treatments with different orientations may have been confusing, or counterproductive in some other way. There is some evidence for such an effect. In the NIDA Cocaine Collaborative Study (Crits-Christoph et al., 1999), participants who received individual and group counseling of the same orientation (i.e., 12-step focused) had better outcomes than those who received 12-step oriented group counseling coupled with either cognitive or psychodynamic therapy. Of course it is possible that offering patients a choice of interventions when they first enter treatment might improve engagement and substance use outcomes, although this was not addressed in the present study.
Despite the fact that naltrexone has been shown to be effective, in the context of a more substantial treatment such as IOP or CBT (Rosner et al., 2010) or in medication management as was offered here (Oslin et al., 2014), there is very little use of the medication in substance use disorder treatment (Harris et al., 2012; Heinrich & Hill, 2008). The low rates of prescribing naltrexone for patients with alcohol use disorders has been seen as a function of program structural issues, or providers’ lack of knowledge about the effectiveness of the medication or belief that it is not effective (Heinrich & Hill, 2008; Oser & Roman, 2007). However, the findings of the current study suggest that low uptake of naltrexone may also be due in part to lack of enthusiasm for the medication in those seeking treatment for alcohol use disorders.
Overall, the results did not support further efforts to re-engage patients who were not engaged at both 2 and 8 weeks. It is likely that our difficulty in contacting these patients and delivering further treatments to them at that point contributed to the lack of efficacy. Interestingly, significant or trend-level interactions obtained with both the alcohol and cocaine dependent patients on some outcomes suggested that further outreach efforts yielded benefits with patients who had prior but not current dependence at entrance to IOP. This raises the possibility that a second attempt to engage less severe patients via telephone outreach efforts is beneficial, but that such efforts do not help those with more severe substance use problems at intake to treatment, possibly because they are not intensive enough for this group. There was also some evidence of a delayed effect favoring a second outreach effort in the alcohol dependent patients, as indicated by significant or trend level group by time interactions. However, these diagnosis and time moderator effects should be interpreted very cautiously, as none of the treatment condition contrasts at any time point reached the .05 level of significance.
This study had a number of significant limitations. The sample consisted primarily of African American men, and the results may not generalize to other patient groups. However, it should be noted that the African American sample is also a strength with regard to diversity. As was discussed earlier, choice of treatments was not offered at intake, but rather after patients had already started (or failed to start) IOP, and the alternative treatments were not provided at the IOP or by the IOP staff. Using IOP counselors to deliver the alternative treatments and providing them at the IOP may have led to different results. Moreover, we did not offer combination treatments as options, such as receiving CBT and medication management, and patients were not offered the option of staying with IOP and adding one of the other three treatments. These factors may have reduced the likelihood of treatment effects favoring choice, and the willingness of participants to try interventions other than IOP.
Finally, the study design did not include a no outreach control condition for the analyses with patients who were not engaged at 2 weeks or with those who dropped out between weeks 3 and 8. Therefore, we cannot determine whether either MI-IOP or MI-PC was better than no outreach in patients who were disengaged at these points. It is clear that treatment choice is a very complicated issue, and that there are many potential treatment options that could be considered as well as other designs with which they could be studied. The impact of choice becomes even more complicated within a SMART study, with repeated randomizations.
Public Health Significance.
The results of this study indicated that individuals who failed to engage in intensive outpatient programs (IOP) for substance use disorders had better drinking outcomes if outreach attempts focused on engagement in the IOP, rather than on offering several treatment options in addition to IOP. Therefore, providing treatment choice to non-engaged patients did not lead to better outcomes.
Acknowledgments
This research was supported by grants P01 AA016821 from the National Institute on Alcohol Abuse and Alcoholism, and P60 DA05186 and K24 DA029062 from the National Institute on Drug Abuse. Additional support was provided by the Center of Excellence in Substance Abuse Treatment and Education of the Department of Veterans Affairs. We thank the management and clinical staffs at Presbyterian Hospital and the Philadelphia VAMC Addictions Recovery Unit for collaborating on this research project and providing access to patients in their programs. We also thank our team of counselors and research technicians who carried out the study.
References
- Adamson SJ, Sellman JD, Dore GM. Therapy preference and treatment outcome in clients with mild to moderate alcohol dependence. Drug and Alcohol Review. 2005;24:209–216. doi: 10.1080/09595230500167502. [DOI] [PubMed] [Google Scholar]
- Anderson AL, Reid MS, Li SH, Holmes T, Shemanski L, Slee A, et al. Modafinil for the treatment of cocaine dependence. Drug & Alcohol Dependence. 2009;104:133–139. doi: 10.1016/j.drugalcdep.2009.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Babor TF, Steinberg K, Anton R, Del Boca F. Talk is cheap: Measuring drinking outcomes in clinical trials. Journal of Studies on Alcohol. 2000;61:55–63. doi: 10.15288/jsa.2000.61.55. [DOI] [PubMed] [Google Scholar]
- Carroll KM. A cognitive-behavioral approach: Treating cocaine addiction. Rockville, MD: National Institute on Drug Abuse; 1998. (NIH publication 98-4308). [Google Scholar]
- Chewning B, Bylund CL, Shah B, Arora NK, Gueguen JA, Makoul G. Patient preference for shared decisions: A systematic review. Patient Education and Counseling. 2012;86:9–18. doi: 10.1016/j.pec.2011.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crits-Christoph P, Liqueland L, Blaine J, Frank A, Luborsky L, Onken LS, et al. Psychosocial treatments for cocaine dependence: National Institute on Drug Abuse Collaborative Cocaine Treatment Study. Archives of General Psychiatry. 1999;56:493–502. doi: 10.1001/archpsyc.56.6.493. [DOI] [PubMed] [Google Scholar]
- Dackis CA, Kampman KM, Lynch KG, Plebani J, Pettinati HM, Sparkman T, et al. A double-blind, placebo-controlled trial of modafinil for cocaine dependence. J Subst Abuse Treat. 2012;43:303–312. doi: 10.1016/j.jsat.2011.12.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deci EL, Ryan RM. Intrinsic motivation and self-determination in human behavior. New York: Plenum; 1985. [Google Scholar]
- Ehrman RN, Robbins SJ. Reliability and validity of six-month timeline reports of cocaine and heroin use in a methadone population. Journal of Consulting and Clinical Psychology. 1994;62:843–850. doi: 10.1037//0022-006x.62.4.843. [DOI] [PubMed] [Google Scholar]
- Fals-Stewart W, O’Farrell TJ, Freitas TT, McFarlin SK, Rutigliano P. The timeline followback reports of psychoactive substance use by drug-abusing patients: Psychometric properties. Journal of Consulting and Clinical Psychology. 2000;68:134–144. doi: 10.1037//0022-006x.68.1.134. [DOI] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for DSM-IV Axis I Disorders—patient edition (SCID-I/P, version 2.0) Biometrics Research Department, New York State Psychiatric Institute; NY: 1996. [Google Scholar]
- Fitzmaurice GM, Laird NM, Ware JH. Applied Longitudinal Analysis. 2nd. John Wiley & Sons; Hoboken, New Jersey: 2011. [Google Scholar]
- Harris AHS, Oliva E, Bowe T, Humphreys KN, Kivlahan DR, Trafton JA. Pharmacotherapy of alcohol use disorders in the Veterans Health Administration: Patterns of receipt and persistence. Psychiatric Services. 2012;63:679–685. doi: 10.1176/appi.ps.201000553. [DOI] [PubMed] [Google Scholar]
- Heinrich CJ, Hill CJ. Role of state policies in the adoption of naltrexone for substance abuse treatment. Health Research and Educational Trust. 2008;43:951–970. doi: 10.1111/j.1475-6773.2007.00812.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joosten EAG, de Jong CAJ, de Weert-van Oene GH, Sensky T, van der Staak CPF. Shared decision making reduces drug use and psychiatric severity in substance-dependent patients. Psychotherapy and Psychosomatics. 2009;78:245–253. doi: 10.1159/000219524. [DOI] [PubMed] [Google Scholar]
- King M, Nazareth I, Lampe F, Bower P, Chandler M, Morou M, et al. Impact of participant and physician intervention preferences on randomized trials. JAMA. 2005;293:1089–1099. doi: 10.1001/jama.293.9.1089. [DOI] [PubMed] [Google Scholar]
- Lindhiem O, Bennett CB, Trentacosta CJ, McLear C. Client preferences affect treatment satisfaction, completion, and clinical outcomes. Clinical Psychology Review. 2014;34:506–517. doi: 10.1016/j.cpr.2014.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maisto SA, Sobell LC, Sobell MB. Comparison of alcoholics' self-reports of drinking behavior with reports of collateral informants. Journal of Consulting and Clinical Psychology. 1979;47:106–122. [PubMed] [Google Scholar]
- McCrady BS, Epstein EE, Cook S, Jensen NK, Ladd BO. What do women want? Alcohol treatment choices, treatment entry, and retention. Psychology of Addictive Behaviors. 2011;25:521–529. doi: 10.1037/a0024037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKay JR, Alterman AI, McLellan AT, Boardman C, Mulvaney F, O’Brien CP. Random versus non-random assignment in the evaluation of treatment for cocaine abusers. Journal of Consulting and Clinical Psychology. 1998;66:697–701. doi: 10.1037//0022-006x.66.4.697. [DOI] [PubMed] [Google Scholar]
- McKay JR, Alterman AI, McLellan AT, Snider EC, O’Brien CP. The effect of random versus nonrandom assignment in a comparison of inpatient and day hospital rehabilitation for male alcoholics. Journal of Consulting and Clinical Psychology. 1995;63:70–78. doi: 10.1037//0022-006x.63.1.70. [DOI] [PubMed] [Google Scholar]
- McKay JR, Van Horn D, Morrison R. Telephone continuing care for adults. Center City MN: Hazelden Foundation Press; 2010. [Google Scholar]
- McKay JR, Van Horn D, Oslin D, Lynch KG, Ivey M, Ward K, Drapkin M, Becher J, Coviello D. A randomized trial of extended telephone-based continuing care for alcohol dependence: Within treatment substance use outcomes. Journal of Consulting and Clinical Psychology. 2010;78:912–923. doi: 10.1037/a0020700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLellan AT, Carise D, Kleber HD. The national addiction treatment infrastructure: Can it support the public’s demand for quality care? Journal of Substance Abuse Treatment. 2003;25:117–121. [PubMed] [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Helping people change. 3rd. New York: Guilford Press; 2013. [Google Scholar]
- Moyers TB, Martin T, Manuel JK, Hendrickson SML, Miller WR. Assessing competence in the use of motivational interviewing. Journal of Substance Abuse Treatment. 2005;28(1):19–26. doi: 10.1016/j.jsat.2004.11.001. [DOI] [PubMed] [Google Scholar]
- Moyers TB, Martin T, Manuel JK, Miller WR, Ernst D. Revised global scales: Motivational Interviewing Treatment Integrity 3.1.1. University of New Mexico Center on Alcoholism, Substance Abuse, and Addictions; Albuquerque, NM: 2010. (MITI 3.1.1) [Google Scholar]
- Murphy SA, Lynch KG, McKay JR, Oslin DW, Ten Have TR. Developing adaptive treatment strategies in substance abuse research. Drug and Alcohol Dependence. 2007;88:S24–S30. doi: 10.1016/j.drugalcdep.2006.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oser CB, Roman PM. Organizational-level predictors of adoption across time: Naltrexone in private substance-use disorder treatment centers. Journal of Studies on Alcohol and Drugs. 2007;68:852–861. doi: 10.15288/jsad.2007.68.852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oslin DW, Lynch KG, Maisto SA, Lantinga LJ, McKay JR, Possemato K, et al. A randomized clinical trial of alcohol care management delivered in VA primary care clinics versus specialty care addiction treatment. Journal of General Internal Medicine. 2014 doi: 10.1007/s11606-013-2625-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rösner S, Hackl-Herrwerth A, Leucht S, Vecchi S, Srisurapanont M, Soyka M. Opioid antagonists for alcohol dependence. Cochrane Database Syst Rev. 2010;(12):CD001867. doi: 10.1002/14651858.CD001867.pub3. [DOI] [PubMed] [Google Scholar]
- Rapp RC, Xu J, Carr CA, Lane DT, Wang J, Carlson R. Treatment barriers identified by substance abusers assessed at a central intake. Journal of Substance Use Disorders. 2006;30:227–235. doi: 10.1016/j.jsat.2006.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist. 2000;55:68–78. doi: 10.1037//0003-066x.55.1.68. [DOI] [PubMed] [Google Scholar]
- Sobell LC, Maisto SA, Sobell MB, Cooper AM. Reliability of alcohol abusers' self-reports of drinking behavior. Behavior Research and Therapy. 1979;17:157–160. doi: 10.1016/0005-7967(79)90025-1. [DOI] [PubMed] [Google Scholar]
- Sobell LC, Sobell MB, Leo GI, Cancilla A. Reliability of a timeline method: Assessing normal drinkers' reports of recent drinking and a comparative evaluation across several populations. British Journal of Addictions. 1988;83:393–402. doi: 10.1111/j.1360-0443.1988.tb00485.x. [DOI] [PubMed] [Google Scholar]
- Sterling RC, Gotheil E, Glassman SD, Weinstein SP, Serota RD. Patient treatment and compliance: Data from a substance abuse treatment program. American Journal on Addictions. 1997;6:168–176. [PubMed] [Google Scholar]
- Stout RL, Beattie MC, Longabaugh R, Noel N. Factors affecting correspondence between patient and significant other reports of drinking [abstract] Alcoholism: Clinical and Experimental Research. 1989;12:336. [Google Scholar]
- Substance Abuse and Mental Health Services Administration, Office of Applied Studies0. Discharges from substance abuse treatment services. Rockville, MD: U.S. Department of Health and Human Services; 2008. Treatment Episode Data Set (TEDS): 2005. (DASIS Series S-41; DHHS Publication No SMA 08 4314). [Google Scholar]
- Swift JK, Callahan JL. The impact of client treatment preference on outcome: A meta-analysis. Journal of Clinical Psychology. 2009;65:368–381. doi: 10.1002/jclp.20553. [DOI] [PubMed] [Google Scholar]
- VA/DoD Clinical Practice Guideline: Management of Substance Use Disorder (SUD) Version 2. Department of Veterans Affairs, Department of Defense; 2009. http://www.healthquality.va.gov/guidelines/MH/sud/ [Google Scholar]
- Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving chronic illness care: Translating evidence into action. Health Affairs. 2001;20:64–78. doi: 10.1377/hlthaff.20.6.64. [DOI] [PubMed] [Google Scholar]
- Walsh DC, Hingson RW, Merrigan SJ, Levenson SM, Cupples LA, Heeren T, et al. A randomized trial of treatment options for alcohol abusing workers. New England Journal of Medicine. 1991;325:775–782. doi: 10.1056/NEJM199109123251105. [DOI] [PubMed] [Google Scholar]
- Wild TC, Cunningham JA, Ryan RM. Social pressure, coercion, and client engagement at treatment entry: A self-determination theory perspective. Addictive Behaviors. 2006;31:1858–1872. doi: 10.1016/j.addbeh.2006.01.002. [DOI] [PubMed] [Google Scholar]