

Abstract
Background:
Tennis elbow is one of the most often diagnosed pathology of the upper extremity and different treatments have been suggested for this disease, so this study was to investigate the effects of extracorporeal shock wave therapy in Tennis elbow treatment.
Materials and Methods:
We design a before and after clinical trial study (registry number: IRCT2012072610405N1) and investigated 40 patients with tennis elbow disease. All patients received 2000 pulses extracorporeal shock wave by piezoelectric device (WOLF Company) daily for one-week. The severity of pain was the primary outcome and measured with visual analogue scale (VAS). Secondary outcome was the ability to perform daily activities using questionnaire’s quick DASH (Disabilities of the Arm, Shoulder and Hand). Primary and secondary outcomes at baseline, 30 and 60 days after intervention were measured.
Results:
The mean age of patients was 43.80±8.97 years and 28 patients (70%) were female. The mean duration of disease was 6.5 ± 7.9 month. The mean score of VAS pain score reduced from 7.25±1.54cm (median=7cm) before treatment to 2.76±2.08cm (median=2cm) at 60 days after the end of treatment (P<0.001). The Quick Dash score reduced significantly from 25.20±5.31 (median=25) before treatment to 8.69±8.32 (median=6) at 60 days after the treatment (P<0.001).
Conclusion:
For newly diagnosed patients with tennis elbow, extracorporeal shock wave therapy can reduce the severity of pain and improve daily activity.
Keywords: Tennis elbow, extracorporeal shock wave, pain, daily activity
1. INTRODUCTION
The prevalence of retinopathy is increasing for substantial part of all sports injuries and occupational disorders (1). Tennis elbow is one of the most often diagnosed pathology of the upper extremity and the incidence of this condition is 1% per 1000 patients per year and its prevalence is 1–3% of adults per year (2). Tennis elbow or lateral epicondylitis of the humerus is tendinosis of the extensor carpi radialis brevis. The principal symptom is pain located at the lateral epicondyle of the humerus and the common extensor origin just distal to it (3).
In the pathogenesis of this condition, Faro and Wolf, reported that there is a shift during the disease process from a phenomenon of inflammation of one of the degeneration of a portion near the extensor tendon origin (4). Clinical criteria diagnosis included: swollen spot on the outer surface of the epicondyle or the sensitivity in the external condyle of the arm, pain in extensor tendon adhesion of origin on external condyle, full extension at the elbow and supination position. Differential diagnosis of elbow pain should also be considered in the diagnosis that there are bursitis, infection, osteoarthritis, gout, cervical radiculopathy and radial tunnel syndrome (5).
Different treatments have been suggested for this disease, include: acupuncture, autologous blood injection in the joint, local corticosteroid injections, wave therapy, iontophoresis, laser, brace, manipulation, oral and topical NSAID, electromagnetic pulse, surgery and ultrasound (6, 7). None of these treatments have not improved the disease fully (5, 8). Extracorporeal shock wave therapy is a treatment that has a longer therapeutic effect (9). Two Meta-analyzes conducted about Extracorporeal shock wave therapy was associated with conflicting results, in meta-analysis studies, Rompe and Maffulli reviewed 10 clinical trials and reported that this method was a useful technique for Tennis elbow (2), but in another, Stasinopoulos and Johnson reviewed 7 clinical trials and reported no beneficial effect of this method (10). Therefore, given that Tennis elbow was one of the common disease of elbow and Extracorporeal shock wave therapy result is controversial, this study was design to investigated the effects of Extracorporeal shock wave therapy on Tennis elbow treatment.
2. MATERIAL AND METHODS
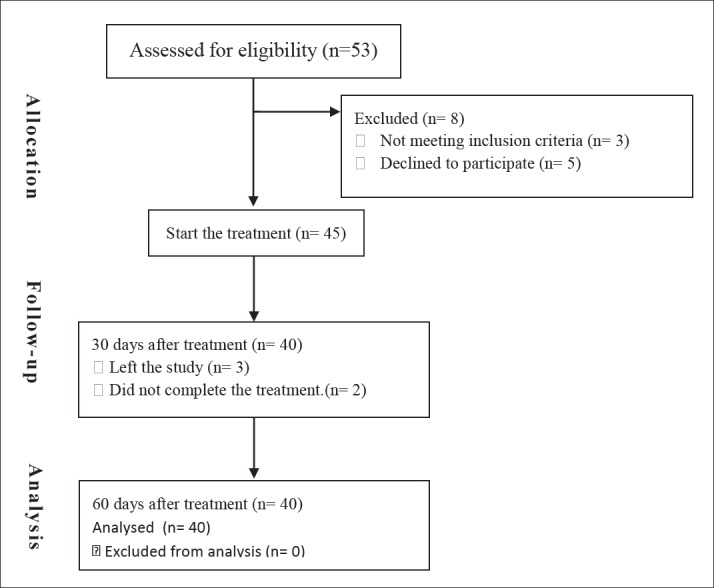
We design a before and after clinical trial study (registry number: IRCT2012072610405N1). The study population was patients with Tennis elbow that referred to the Orthopedics Clinic of Mazandaran University of Medical Sciences. The sample size was calculated by the Cochran formula and 40 subjects that based on a=0.05, P=0.75 and d=0.12 and calculated by the Cochran formula. The diagnosis was based on clinical examination by an orthopedic physician with at least 5 years’ experience. The inclusion criteria were patients of both sexes aged between 20 to 60 years’ old who have had no treatment other than taking analgesia. Exclusion criteria included: evidence of dysfunction of the neck and shoulders, local arthritis, polyarthritis, general neurological disorders, pregnancy, infections, tumors, fractures of the elbow, known hypothyroidism and radial tunnel syndrome. All patients underwent Electromyography and Nerve conduction velocity for exclusion of radial tunnel syndrome. All patients received 2000 pulses extracorporeal shock wave by piezoelectric device (WOLF Company) daily for one-week. The severity of pain in rest was the primary outcome. To assess the pain severity, we asked patients to rate pain they experienced from 1 to 10 and these were recorded as the VAS values. Secondary outcome of the study was the ability to perform daily activities using questionnaire’s quick DASH (Disabilities of the Arm, Shoulder and Hand). The reliability and validity of Persian version of quick DASH questionnaire was approve by Ebrahimzadeh et al. (11). Primary and secondary outcomes at the baseline and 30 and 60 days after intervention were measured (Figure 1). Other variables such as age, sex, duration of illness and the use of analgesia were recorded. This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences.
Figure 1. CONSORT flow diagram.
3. DATA ANALYSIS
Data was analysis by SPSS 18 software. Normality was checked by Kolmogorov Smirnov test. The difference in percentages (quality variables) was analyzed by the Chi-square test and Fisher’s exact test. The mean difference was estimated by the student’s t-test. P-value < 0.05 was considered to be statistically significant.
4. RESULTS
Finally, 40 patients were studied in this trial. The mean age of patients was 43.80±8.97 years (Median=44). 28 patients (70%) were female. The mean duration of disease was 6.58±7.99 months (Standard Error: 1.31, Median=3.96).
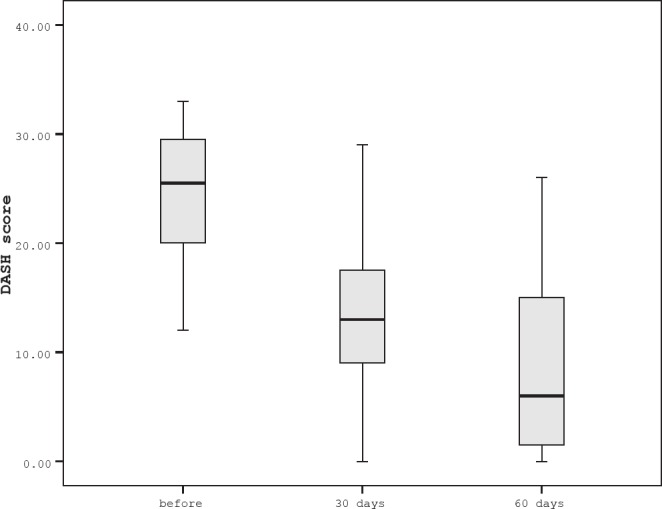
The mean score of VAS was decrease form 7.25±1.54cm (median=7cm) to 4.02±1.64cm (median=4cm) after 30 days (P<0.001) and 2.76±2.08cm (median=2cm) after 60 days (P<0.001) of the treatment (P<0.001). Also, the mean score of DASH at the beginning of study, 30 days and 60 days after treatment were 25.20±5.31 (median=25), 13.53±6.53 (median=13) and 8.69±8.32 (median=6), respectively. Daily activity of patients was significantly improving after the treatment (P<0.001) (Figures 2 and 3). The analgesic consumption was observed in 19 patients (47.5%) at the base line, 9 patients (22.5%) after the 30 days and 6 patients (15%) after the 60 days of study. The shock-wave therapy significantly reduced analgesic consumption (P<0.001). There was not observed any complication.
Figure 2. The VAS score changes before and after extracorporeal shock wave therapy.
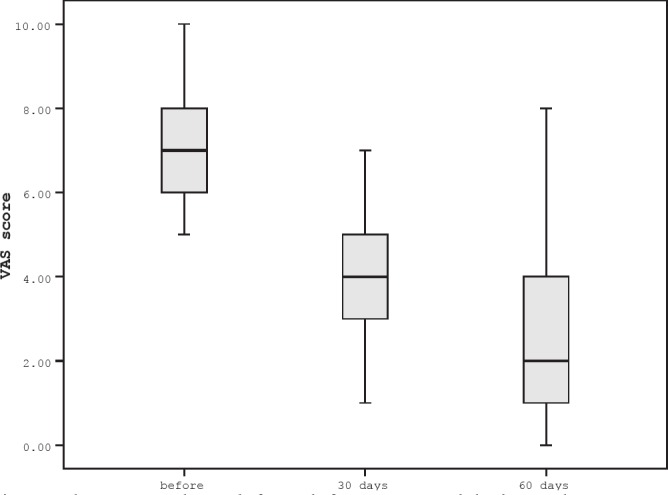
Figure 3. The Quick DASH score changes before and afterextracorporeal shock wave therapy.
5. DISCUSSION
Extracorporeal shock wave therapy for tendinopathy is not widely known among the medical community. It has been thoroughly investigated experimentally during the past decade (2). The objective of the present study was to investigate the effects of extracorporeal shock wave therapy in Tennis elbow treatment and the result show that the mean score of VAS pain score reduced significantly after the treatment. Ozkut et al. treated 13 elbows of 12 patients who did not benefit from conservative therapy for lateral epicondylitis and refused surgical therapy. Under fluoroscopic guidance, extracorporeal shockwave therapy of 1200 pulses at 15-20 KV was administered at a mean of three sessions with two-day intervals. The follow-up period was 12 months. Patients were evaluated using the Roles and Maudsley pain scores. The mean pain score, which was 3.4 before treatment decreased significantly to 2 after treatment (12). Krischek et al treated 30 patients with chronic medial epicondylitis with low-energy shock waves. All patients received 500 impulses of 0.08 mJ/mm2 three times at weekly intervals. At 1-year follow-up, outcome was acceptable in 60% of the patients with tennis elbow and the average relief of pain was 32% (13). Rompe et al, in a systematic review, reported that well-designed randomized controlled trials had provided evidence of the effectiveness of shock wave intervention for tennis elbow (14) Conversely, Stasinopoulos and Johnson in another systematic review reported no beneficial effect of this method (10). Another review shows that high-extracorporeal shock-wave therapy is effective for treating calcific rotator cuff-tendinosis and no evidence were found in the effectiveness of ESWT to treat non-calcific rotator cuff-tendinosis (15). The results of these studies show that extracorporeal shock wave therapy as an alternative can be a beneficial method for treatment of tennis elbow, it seems that these waves stimulates of soft-tissue healing and inhibition of pain receptors, via an unknown mechanism (2). The mechanism of this method is not yet completely understood, but many mechanisms have been described in clarifying its effects, including direct stimulation of healing, neovascularization, direct suppressive effects on nociceptors and a hyper stimulation mechanism that would block the gate control mechanism. It seems that it can increase the number of neovessels at the normal tendon–bone junction, through the release of growth factors and some other active substances (16).
Secondary outcome of the study was the ability to perform daily activities by quick DASH score and the result show that this score reduced significantly after the end of treatment. In the Ozkut et al. study, the mean grip strength of the affected extremities was 82.1% of the normal side at the end of 12 months after treatment with extracorporeal shockwave therapy. At final follow-up, 75% stated that the treatment was beneficial (12). In the Rompe et al study, 78 patients enrolled in a placebo-controlled trial. All patients were tennis players with recalcitrant MRI-confirmed tennis elbow of at least 12 months’ duration. At 3 months, there was a significantly higher improvement in Upper Extremity Function Scale in the intervention group than in the placebo group (17). In another study, Rasmussen et al. 48 patients with chronic Achilles tendinopathy were randomized to receive either active ESWT or sham ESWT over 4 weeks. American Orthopedic Foot and Ankle Society (AOFAS) score were assessed before treatment, during the 4-week treatment period, and at 4, 8, and 12 weeks of follow-up and better results were seen as the intervention group at 8 and 12 weeks of follow-up (18).
In limitation, this treatment in not usable in every center, because it needs specialist. Additionally, this study designed as before and after study and we can’t a placebo group because it is not ethical.
6. CONCLUSION
For newly diagnosed patients with tennis elbow, extracorporeal shock wave therapy can reduce the severity of pain and improve daily activity.
Authors’ contributions:
All the authors were involved during the investigation process in all stages of this study including a primary data collection, analysis and the documentation of the collection.
Funding/Support:
This research was supported financially by the research grant of Mazandaran University of Medical Sciences, Mazandaran, Sari, Iran.
Conflict of interest:
none declared.
REFERENCES
- 1.Ackermann PW, Renström P. Tendinopathy in sport. Sports Health. 2012;4(3):193–201. doi: 10.1177/1941738112440957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Speed C, Nichols D, Richards C, Humphreys H, Wies J, Burnet S, et al. Extracorporeal shock wave therapy for lateral epicondylitis–a double blind randomized controlled trial. Journal of orthopaedic research. 2002;20(5):895–8. doi: 10.1016/S0736-0266(02)00013-X. [DOI] [PubMed] [Google Scholar]
- 3.Crowther M, Bannister G, Huma H, Rooker G. A prospective, randomised study to compare extracorporeal shock-wave therapy and injection of steroid for the treatment of tennis elbow. Bone and Joint Journal. 2002;84(5):678–9. doi: 10.1302/0301-620x.84b5.12741. [DOI] [PubMed] [Google Scholar]
- 4.Faro F, Wolf JM. Lateral epicondylitis: review and current concepts. Journal of hand surgery. 2007;32(8):1271–9. doi: 10.1016/j.jhsa.2007.07.019. [DOI] [PubMed] [Google Scholar]
- 5.Flatt AE. 4. Vol. 21. Baylor University Medical Center; 2008. Tennis elbow; p. 400. Proceedings. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kaeding C, Best TM. Tendinosis pathophysiology and nonoperative treatment. Sports Health. 2009;1(4):284–92. doi: 10.1177/1941738109337778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Andres BM, Murrell GA. Treatment of tendinopathy: what works, what does not, and what is on the horizon. Clinical orthopaedics and related research. 2008;466(7):1539–54. doi: 10.1007/s11999-008-0260-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Oron A, Schwarzkopf R, Loebenberg M. Tennis elbow (lateral epicondylitis)–assessment and treatment. Harefuah. 2008;147(4):340–3. [PubMed] [Google Scholar]
- 9.Ozturan KE, Yucel I, Cakici H, Guven M, Sungur I. Autologous blood and corticosteroid injection and extracoporeal shock wave therapy in the treatment of lateral epicondylitis. Orthopedics. 2010;33(2) doi: 10.3928/01477447-20100104-09. [DOI] [PubMed] [Google Scholar]
- 10.Stasinopoulos D, Johnson M. Effectiveness of extracorporeal shock wave therapy for tennis elbow (lateral epicondylitis) British journal of sports medicine. 2005;39(3):132–6. doi: 10.1136/bjsm.2004.015545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ebrahimzadeh MH, Moradi A, Vahedi E, Kachooei AR, Birjandinejad A. Validity and reliability of the Persian version of shortened disabilities of the arm, shoulder and hand questionnaire (quick-DASH) International journal of preventive medicine. 2015;6 doi: 10.4103/2008-7802.160336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ozkut AT, Kilinçoğlu V, Ozkan NK, Eren A, Ertaş M. Extracorporeal shock wave therapy in patients with lateral epicondylitis. Acta orthopaedica et traumatologica turcica. 2007;41(3):207–10. [PubMed] [Google Scholar]
- 13.Krischek O, Hopf C, Nafe B, Rompe J-D. Shock-wave therapy for tennis and golfer’s elbow–1 year follow-up. Archives of orthopaedic and trauma surgery. 1999;119(1):62–6. doi: 10.1007/s004020050356. [DOI] [PubMed] [Google Scholar]
- 14.Rompe J, Theis C, Maffulli N. Shock wave treatment for tennis elbow. Der Orthopade. 2005;34(6):567–70. doi: 10.1007/s00132-005-0805-x. [DOI] [PubMed] [Google Scholar]
- 15.Huisstede BM, Gebremariam L, van der Sande R, Hay EM, Koes BW. Evidence for effectiveness of Extracorporal Shock-Wave Therapy (ESWT) to treat calcific and non-calcific rotator cuff tendinosis–a systematic review. Manual therapy. 2011;16(5):419–33. doi: 10.1016/j.math.2011.02.005. [DOI] [PubMed] [Google Scholar]
- 16.Notarnicola A, Moretti B. The biological effects of extracorporeal shock wave therapy (ESWT) on tendon tissue. Muscles, ligaments and tendons journal. 2012;2(1):33. [PMC free article] [PubMed] [Google Scholar]
- 17.Rompe JD, Decking J, Schoellner C, Theis C. Repetitive low-energy shock wave treatment for chronic lateral epicondylitis in tennis players. The American journal of sports medicine. 2004;32(3):734–43. doi: 10.1177/0363546503261697. [DOI] [PubMed] [Google Scholar]
- 18.Rasmussen S, Christensen M, Mathiesen I, Simonson O. Shockwave therapy for chronic Achilles tendinopathy: a double-blind, randomized clinical trial of efficacy. Acta Orthopaedica. 2008;79(2):249–56. doi: 10.1080/17453670710015058. [DOI] [PubMed] [Google Scholar]