

Abstract
The present study examines whether early adolescents’ self-efficacy beliefs about anger regulation mediate the relation between parents’ self-efficacy beliefs about anger regulation and early adolescents’ internalizing and externalizing problems. Participants were 534 early adolescents (T1: M age = 10.89, SD = .70; 50% female), their mothers (n = 534), and their fathers (n = 431). Families were drawn from Colombia, Italy, and the USA. Follow-up data were obtained two (T2) and three (T3) years later. At T1 and T3, parents’ self-efficacy beliefs were self-reported and internalizing and externalizing problems were assessed via mothers’, fathers’, and early adolescents’ reports. At T2, early adolescents’ self-efficacy beliefs were self-reported Within the overall sample, mothers with higher self-efficacy beliefs about anger regulation had children with similar beliefs. Early adolescents’ low self-efficacy beliefs were associated with higher internalizing and externalizing problems.
Keywords: Self-efficacy, Anger regulation, Internalizing, Externalizing, Adolescence, Cross-cultural
1. Introduction
The transition to adolescence is associated with substantial increases in the prevalence of a wide range of externalizing and internalizing problems that have long-term implications for both physical and mental health in adulthood (Costello, Copeland, & Angold, 2011). Indeed, many psychiatric diseases in adulthood are preceded by mental illness before the age of 18 years (e.g., Kim-Cohen et al., 2003). Thus, there is a need to understand determinants of early adolescents’ mental health. The present study examined one potentially important determinant of early adolescents’ mental health—self-efficacy beliefs about emotion regulation. Given that such self-efficacy beliefs and the prevalence of mental health disorders vary widely across cultures, we gathered data from parents and children in three countries: Colombia, Italy, and the USA. Understanding the determinants of early adolescents’ mental health problems across three countries could inform international intervention efforts aimed at improving future generations’ psychological well-being.
1.1. Adolescent psychopathology across cultures in times of change
To begin, it is important to note that prevalence rates of mental health problems among adults from Colombia, Italy, and the USA vary widely, ranging from 10% to 25% in Colombia, from 1% to 12% in Italy, and from 20% to 31% in the USA (Kessler et al., 2007; Polanczyk, Salum, Sugaya, Caye, & Rohde, 2015). Given strong relations between mental health in adolescence and adulthood, it seems reasonable to assume that adolescent mental health problems have roughly similar variability in these three countries.
Furthermore, the frequency of mental health problems in adolescence varies across time. For example, internalizing problems have increased in recent decades in the Netherlands (e.g., Tick, Van Der Ende, & Verhulst, 2007), Greece (Fichter, Xepapadakos, Quadflieg, Georgopoulou, & Fthenakis, 2004), Sweden (Kosidou et al., 2010), and the USA (Achenbach, Dumenci, & Rescorla, 2003). Externalizing problems appear to vary across time as well (e.g., Collishaw, Maughan, Natarajan, & Pickles, 2010). For example, externalizing symptoms among adolescents in the USA increased between the 1970s and 1980s and then declined in the 1990s (e.g., Achenbach et al., 2003). This preliminary evidence suggests that mental health symptoms among adolescents vary by culture and across time. Given this variability, it is important to examine determinants of adolescents’ internalizing and externalizing problems within current cultural contexts.
1.2. Self-efficacy beliefs about emotion regulation
Self-efficacy beliefs about emotion regulation are potential determinants of early adolescents’ internalizing and externalizing problems (e.g., Bandura, Caprara, Barbaranelli, Gerbino, & Pastorelli, 2003; Caprara, Gerbino, Paciello, Di Giunta, & Pastorelli, 2010). Emotion regulation involves initiating, avoiding, inhibiting, maintaining, or modulating feelings and related physiological processes, cognitions, and behaviors in the service of accomplishing goals and adhering to social expectations (e.g., Eisenberg & Spinrad, 2004). The assessment of emotion regulation often measures what individuals actually do or report they would do to modulate their emotional experiences. It is equally important to understand what individuals believe themselves capable of doing in response to their emotional experiences. Self-efficacy beliefs about emotion regulation measure how well people believe they can control emotional experiences, including exerting control over the origins and intensity of, reactions to, and consequences of one’s own emotions (Bandura et al., 2003). Thus, one’s self-efficacy beliefs about emotion regulation likely impact many aspects of one’s response to emotionally evocative situations, including the interpretation of situations, the expression of emotion, choice of regulatory strategies, and evaluations of consequences (e.g., Bandura, 1986; Caprara, Di Giunta, Pastorelli, & Eisenberg, 2013). Given the substantial effects self-efficacy beliefs about emotion regulation likely have on emotion regulation (e.g., Caprara, Vecchione, Barbaranelli, & Alessandri, 2013; Di Giunta et al., 2017), it is important to understand predictors and outcomes of such beliefs.
When examining self-efficacy beliefs about emotion regulation, it is important to consider the type of emotion being experienced. Caprara and colleagues (e.g., Caprara et al., 2008; Caprara, Di Giunta, et al., 2013; Caprara, Vecchione, et al., 2013) found empirical support for examining self-efficacy beliefs separately by emotion (e.g., irritability/anger, depression/sadness, positive emotions). Self-efficacy beliefs about anger are especially important to understand, given the significant public health burden associated with anger during adolescence (e.g., Brotman, Kircanski, & Leibenluft, 2017). Childhood clinical disorders that have anger as a central feature have extremely high comorbidity rates (e.g., Nock, Kazdin, Hiripi, & Kessler, 2007). Anger alone is associated with several mental disorders, many of which do not include anger as a key symptom (e.g., social phobia, specific phobia, anxiety and mood disorders; Stringaris, Cohen, Pine, & Leibenluft, 2009). Furthermore, anger during adolescence predicts maladjustment in adulthood Copeland, Shanahan, Egger, Angold, & Costello, 2014; Pickles et al., 2010; Stringaris et al., 2009). Given the cross-diagnostic and long-term impact of anger during adolescence, it is crucial to understand mechanisms associated with its regulation.
1.3. Relating parental self-efficacy beliefs about emotion regulation to adolescents’ self-efficacy beliefs about emotion regulation
One potentially important predictor of adolescents’ self-efficacy beliefs about emotion regulation is their parents’ self-efficacy beliefs about their own emotion regulation. Although there is no direct evidence on this link, general theories on self-efficacy beliefs provide theoretical support for such as association. According to Bandura (1997), self-efficacy beliefs develop from four potential sources: mastery experiences, modeling, social persuasion, and interpretations of one’s physiological and affective experiences.
Eisenberg, Cumberland, and Spinrad (1998) were among the earliest theorists to propose a model of how children’s emotion-related outcomes (e.g., the experience, comprehension, expression, and regulation of emotion) are socialized within the family context. One pathway in their model suggests that parents’ emotion-related beliefs impact children’s cognitions about emotion and its regulation (sometimes through mediating variables such as emotion-related parenting practices and child arousal). Morris, Silk, Steinberg, Myers, and Robinson (2007) expanded on Eisenberg et al.’s (1998) work, proposing three mechanisms that explain how family environments affect children’s development of emotion regulation skills. One of the mechanisms proposed by Morris et al. (2007) is observational learning/modeling, whereby adolescents learn emotion-related self-regulation skills by watching their parents’ own skills in action (see also Denham, Mitchell-Copeland, Strandberg, Auerbach, & Blair, 1997). In other words, parents’ personal emotional tendencies can implicitly teach adolescents which emotions and self-management strategies are appropriate. By observing their parents’ reactions to provocative emotional situations, children learn what is ‘expected’ of them in analogous situations they encounter. This line of thinking can readily be expanded to include self-efficacy beliefs about emotion regulation. Parents who do not believe they can regulate their own emotions might implicitly teach their children similar beliefs. After regularly witnessing their parents’ low self-efficacy beliefs about emotion regulation, children may eventually come to believe that similar cognitions are expected of them and that they are incapable of dealing with their own emotions. Thus, parental self-efficacy beliefs about emotion regulation might be important predictors of early adolescents’ self-efficacy beliefs about emotion regulation.
1.4. Self-efficacy beliefs about emotion regulation and adolescents’ psychological adjustment
Externalizing and internalizing problems might be important outcomes of early adolescents’ self-efficacy beliefs about emotion regulation. Poor self-efficacy beliefs about emotion regulation have been related to anxiety, depression, and externalizing symptoms (Bandura et al., 2003; Valois, Zullig, & Hunter, 2015; Zullig, Teoli, & Valois, 2014). Regarding self-efficacy beliefs about anger regulation specifically, Caprara et al. (2008), Caprara, Di Giunta, et al. (2013) and Caprara, Vecchione, et al. (2013) found that greater self-efficacy beliefs about anger regulation were moderately associated with less irritability, aggression, and anxiety-depression among young adults. Among pre-adolescents from Italy, the USA, and Colombia, Di Giunta et al. (2017) found that greater self-efficacy beliefs about anger regulation were associated with fewer concurrent externalizing symptoms. This preliminary evidence suggests that externalizing and internalizing problems might be important outcomes of self-efficacy beliefs about emotion regulation, especially about anger regulation.
1.5. Culture and self-efficacy beliefs about emotion regulation
Evidence indicates that there are both differences and similarities among cultures in the emotional significance assigned to situations, the ways in which emotions are conveyed, and the ways in which people deal with situations that elicit emotion (Kitayama, Markus, & Kurokawa, 2000; Markus & Kitayama, 1991; Mesquita, 2001). For example, adults from collectivist cultures scored higher on suppression when compared to adults from individualistic cultures (Matsumoto, Yoo, & Fontaine, 2008). Young adults from Hong Kong used more maladaptive (e.g., self-blame, other-blame, and catastrophizing) and fewer adaptive (e.g., positive reappraisal and acceptance) strategies than those from North America (Wong, 2009). In a study of European countries, individuals from northern Europe (Germany and Netherlands) used fewer maladaptive strategies to handle negative emotions and engaged in more adaptive emotion expression when compared to individuals from southern and eastern Europe (Spain, Italy, Portugal, and Hungary; Potthoff et al., 2016).
The above-noted cross-cultural differences in emotion regulation might influence how self-efficacy beliefs about emotion regulation are developed, structured, and exercised (Bandura, 2002). Despite this proposition, we are not aware of any studies examining cross-cultural differences in the association between self-efficacy beliefs about emotion regulation and youths’ adjustment or in the association between parents’ and adolescents’ self-efficacy beliefs about emotion regulation.
1.6. The present study
This longitudinal study examined whether early adolescents’ self-efficacy beliefs about anger regulation mediated the relation between parents’ self-efficacy beliefs about anger regulation and adolescents’ internalizing and externalizing problems (see Fig. 1). We had three main hypotheses: (a) adolescents with lower self-efficacy about anger regulation would have more internalizing and externalizing symptoms; (b) mothers and fathers with lower self-efficacy beliefs about anger regulation would have offspring with lower self-efficacy beliefs about anger regulation; (c) adolescents’ self-efficacy beliefs about anger regulation would mediate the relation between parents’ self-efficacy beliefs about anger regulation and adolescents’ internalizing and externalizing symptoms.
Fig. 1.
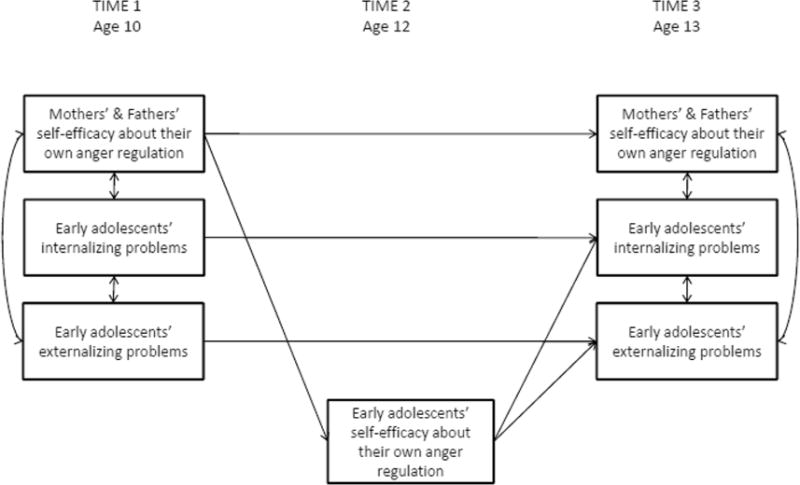
Graphical depiction of the main paths included in the conceptual model. Note. We also anticipated bidirectional paths between parents’ self-efficacy beliefs about anger regulation and early adolescent adjustment. We fit two developmental path analyses models to examine the conceptual model. In the first path analysis, parents’ reports of early adolescents’ adjustment were considered; in the second path analysis, self-reports of early adolescents’ adjustment were considered.
We gathered data when children were 10, 12 and 13 years old. We collected parental self-efficacy beliefs as well as internalizing and externalizing problems (assessed via multiple reporters) at ages 10 and 13 and self-efficacy beliefs at age 12. Considering theoretical models (Eisenberg et al., 1998; Morris et al., 2007) regarding bidirectional associations between parents’ personality and child adjustment, on one hand, and child’s personality and child adjustment, on the other hand, we investigated the following direct associations: (1) from mothers’ and fathers’ self-efficacy about anger regulation to child adjustment and from child adjustment to mothers’ and fathers’ self-efficacy; (2) from child’s self-efficacy to child adjustment and from child adjustment to child self-efficacy.
Finally, we expected that the hypothesized relations between self-efficacy beliefs about anger regulation and youths’ adjustment to be largely invariant across countries, child gender, and child age. If confirmed, such finding would support the broad generalizability of parent-early adolescent transmission of self-efficacy beliefs about emotion regulation consistent with existing evidence on the parent-child transmission of emotion regulation (Bandura, 1997; Bridgett, Burt, Edwards, & Deater-Deckard, 2015; Eisenberg et al., 1998; Morris et al., 2007). If relations differ across countries, the universality of this theoretical model would not be supported, making it important to examine factors accounting for the cultural differences.
2. Method
2.1. Sample
Participants were recruited from the longitudinal study entitled Parenting Across Cultures (e.g., Lansford et al., 2014). An overarching goal was to include cultural groups that were diverse on several socio-demographic dimensions, including predominant ethnicity, predominant religion, economic indicators, and indices of child well-being. For example, on the Human Development Index, a composite indicator of a country’s status with respect to health, education, and income, participating countries had a rank of 5 for United States, 28 for Italy, and 98 for Colombia, out of 187 countries with available data (UNDP, 2012). However, it is important to note that our samples were convenience samples and were therefore not nationally representative. Participants included 534 youth (T1: M age = 10.89, SD = .70; 50% female; T2: M age = 12.82, SD = .66; T3: M age = 13.70, SD = .67), their mothers (n = 534), and their fathers (n = 431). Families were drawn from Medellín, Colombia; Naples, Italy; Rome, Italy; and Durham, North Carolina, United States (European Americans, African Americans, and Hispanic Americans). Fig. 1 summarizes sample sizes for each site separately for mothers, fathers, and early adolescents at each time-point. On average, parental reporters had 12 years of education (top section of Table 1). Details about maternal and paternal educational level, marital status, and number of siblings for each group are reported in Supplemental Table S1). Over 81% of mothers, 77% of fathers, and 81% of children from the initial sample of the Parenting Across Cultures Study provided data at T1. Retention rates within the current study were highest for mothers and adolescents (over 90%) and lowest for fathers (≥73%) (see Fig. 2).
Table 1.
Descriptive statistics and internal consistencies of the examined variables for the total sample.
| N | M | SD | Kurtosis | Skewness | |
|---|---|---|---|---|---|
| Early adolescents’ age-T1 | 556 | 10.89 | 0.70 | 0.33 | −0.14 |
| Parental years of education-T1 | 556 | 12.43 | 4.82 | 0.01 | −0.12 |
| Mothers’ self-efficacy beliefs about their own anger regulation | |||||
| Mother report; T1 | 534 | 3.41 | 0.87 | −0.21 | −0.47 |
| Mother report; T3 | 533 | 3.37 | 0.86 | −0.09 | −0.44 |
| Fathers’ self-efficacy beliefs about their own anger regulation | |||||
| Father report; T1 | 431 | 3.93 | 1.57 | 1.98 | 4.56 |
| Father report; T3 | 383 | 3.50 | 0.80 | −0.31 | −0.08 |
| Early adolescents’ self-efficacy beliefs about their own anger regulation | |||||
| Self report; T2 | 524 | 3.18 | 0.75 | −0.11 | 0.02 |
| Early adolescent internalizing problems | |||||
| Parent report; T1 | 536 | 0.30 | 0.21 | 1.24 | 2.78 |
| Parent report; T3 | 538 | 0.30 | 0.21 | 1.29 | 3.45 |
| Self report; T1 | 533 | 0.40 | 0.26 | 0.63 | −0.15 |
| Self report; T3 | 534 | 0.44 | 0.30 | 0.84 | 0.72 |
| Early adolescent externalizing problems | |||||
| Parent report; T1 | 536 | 0.29 | 0.21 | 1.62 | 4.96 |
| Parent report; T3 | 538 | 0.28 | 0.21 | 1.47 | 3.45 |
| Self report; T1 | 534 | 0.30 | 0.23 | 1.54 | 4.08 |
| Self report; T3 | 534 | 0.34 | 0.23 | 1.01 | 1.14 |
Fig. 2.
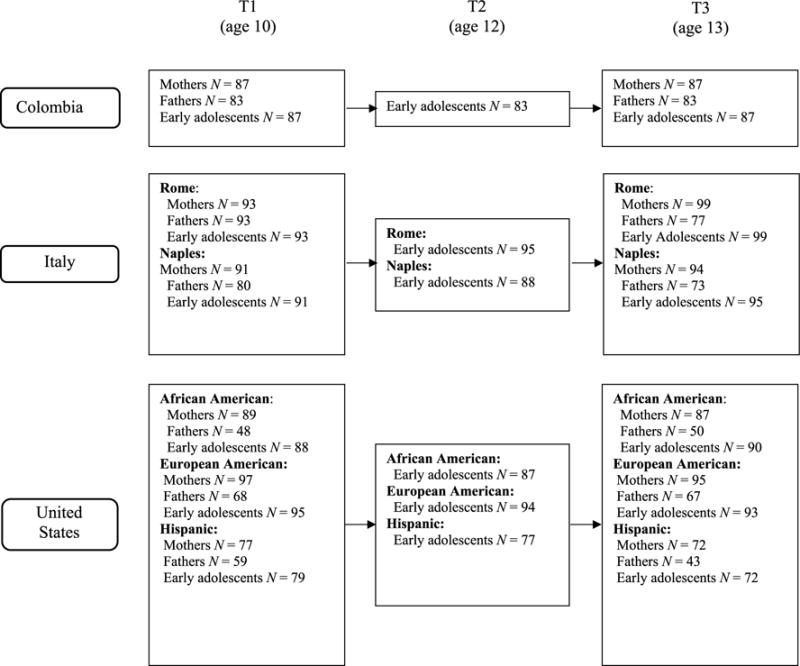
Sample sizes for each site separately for mothers, fathers, and early adolescents at each time-point.
2.2. Procedure
Letters describing the study were sent home with youths, and parents were asked to return a signed form if they were willing to be contacted further. Families were then enrolled in the study until the target sample size was reached in each country. To make each country’s sample as representative as possible of the city from which it was drawn, families of students from private and public schools were sampled in the approximate proportion to which they were represented in the population of the city. Furthermore, youths were sampled from schools serving high-, middle-, and low-income families in the approximate proportion to which these income groups were represented in the local population. These sampling procedures resulted in an economically diverse sample that ranged from low income to high income within each site. For example, in Colombia, there are six well-defined socioeconomic strata, so we sampled families such that their socioeconomic strata matched the socioeconomic distribution of the population of Medellin.
A procedure of forward- and back-translation was used to ensure the linguistic and conceptual equivalence of measures across languages (Maxwell, 1996). Substantial efforts were implemented to ensure that the measures would be valid in all sites by focusing on linguistic equivalence as well as the cultural meanings that would be imparted by the measures (Erkut, 2010). Measures were administered in the following languages: Spanish (Colombia and the United States), Italian (Italy), and English (the United States).
After obtaining approvals from institutional review boards, parental informed consent, and child assent, questionnaires were completed in the participant’s home or location of their choosing (e.g., school). Interviewers read each question to youths and recorded their answers. Rating scales were provided in the form of visual aids to help youths remember response options. Testing sessions lasted approximately one hour. Depending on the site, parents were given modest financial compensation for their participation or youths were given a small age-appropriate gift to thank them for their participation.
2.3. Measures
2.3.1. Mothers’ and fathers’ self-efficacy beliefs about anger regulation (T1 and T3)
Participants rated (1 = not well at all; 5 = very well) their ability to manage anger with two items (i.e., “How well can you manage negative feelings when reprimanded by significant others?” and “How well can you avoid flying off the handle when you get angry?”) of the Regulative Emotional Self-Efficacy Scale (RESE; Caprara et al., 2008; Caprara, Vecchione, et al., 2013). The items considered in the present study are two out of the three items from the original RESE scale that had the highest factor loadings in confirmatory factor analyses with young adults from Italy, US, and Bolivia (Caprara et al., 2008; Caprara, Vecchione, et al., 2013). Mean correlations between these two items across the six groups (i.e., Medellin, Colombia; Naples, Italy; Rome, Italy; European Americans, African Americans, and Hispanic Americans in Durham, North Carolina, USA) were significant for mothers at T1 (r = .50, p < .001) and T3 (rs = .42 and .50 ps < .001), as well as for fathers at T1 and T3 (rs = .45 and .84, ps < .001). Mean alphas for these two items across the six groups were .66 (T1) and .59 (T3) for mothers and .68 (T1) and .62 (T3) for fathers. Average item-total correlations were .46 (T1) and .35 (T3) for mothers and .51 (T1) and .44 (T3) for fathers.
2.3.2. Early adolescents’ self-efficacy beliefs about anger regulation (T2)
Early adolescents rated (1 = not well at all; 5 = very well) three item pertaining their perceived ability to deal with anger (i.e., “How well can you keep from getting angry when others unfairly treat you badly?”; “How well can you avoid getting angry when others keep giving you a hard time?”, and “How well can you avoid flying off the handle when you get angry?”; Caprara et al., 2008). Early adolescents also rated three items from the Self-efficacy beliefs about anger regulation subscale from the Anger Self-Regulation scale (Di Giunta et al., 2017), which is a vignette-based measure of emotion specific self-regulation. We examined youths’ answers about how well they could deal with their anger in the three out of six vignettes (1 = not at all well – 5 = very well) that had the highest factor loadings in a confirmatory factor analysis conducted with this same sample (Di Giunta et al., 2017). Across the six groups, the mean alpha for the items from the two measures combined (i.e., the questionnaire- and vignette-based measures) was .75.
2.3.3. Early adolescent internalizing and externalizing behavior (T1 and T3)
Parents and early adolescents, respectively, completed the Child Behavior Checklist (CBCL) and Youth Self-Report (YSR; Achenbach, 1991). We examined two subscales: Internalizing problems (31 items in CBCL and 29 items in YSR) and Externalizing problems (33 items in CBCL and 30 items in YSR). Respondents indicated whether each behavior was not true (coded as 0), somewhat or sometimes true (coded as 1), or very true or often true (coded as 2). Achenbach measures have been used in at least 60 cultural groups (Achenbach, 2004). Several researchers have demonstrated cross-cultural and cross-language equivalence of the measures across cultural groups (e.g., Weisz, Suwanlert, Chaiyasit, & Walter, 1987). Total scores were created separately by respondent by averaging across all items within each scale. Averaging across years and across sites, alphas were .88 for early adolescent, .86 for mother-, and .86 for father-reported internalizing problems. Alphas averaging across years and across sites were .89 for early adolescent-, .86 for mother-, and .85 for father-reported externalizing problems. Mothers’ and fathers’ reports, averaged across items and then years and sites were moderately correlated for both internalizing (r = .38) and externalizing (r = .53) problems. Given these significant relations, we created a multi-informant composite score (separately for internalizing problems and externalizing problems) that aggregated mothers’ and fathers’ reports (labeled parent-report in subsequent analyses). Parents’ and early adolescents’ reports were not as highly correlated for internalizing (r = .22) and externalizing problems (r = .32). We therefore examined early adolescents’ reports of internalizing and externalizing symptoms separately from parent-reported symptoms.
2.4. Analytic plan
We fit two developmental path models with relations from mothers’ and fathers’ self-efficacy about anger regulation (when their children were 10 years old) to early adolescents’ self-efficacy about anger regulation (12) and from early adolescents’ self-efficacy about anger regulation (at age 12) to early adolescent adjustment (internalizing and externalizing at age 13), controlling for stability in both parents’ self-efficacy and early adolescents’ adjustment from ages 10 to 13. In the first path analysis, parent reports of early adolescent adjustment were considered; in the second path analysis, self-reports of early adolescent adjustment were considered. In both path analyses, we also included relations from (a) internalizing symptoms at age 10 to externalizing symptoms at age 13 and from externalizing symptoms at age 10 to internalizing symptoms at age 13; (b) from parents’ self-efficacy about anger regulation at age 10 to early adolescents’ adjustment at age 13 and from early adolescents’ adjustment at age 10 to parents’ self-efficacy at age 13; (c) from early adolescents’ self-efficacy at age 12 to early adolescents’ adjustment at age 13 and from early adolescents’ adjustment at age 10 to early adolescents’ self-efficacy at age 12. We allowed all measures to covary within waves, and each measure was predicted by parental education, early adolescents’ age, and gender.
In all models, full information maximum likelihood (FIML; Arbuckle, 1996) within Mplus 7 (Muthén & Muthén, 1998–2012) was used to account for missing data (due to 1% attrition over time for both mothers and children, and 12% attrition for fathers). Given that obtaining a significant χ2 becomes increasingly likely with large sample sizes (Kline, 1998), evaluation of the goodness of fit was based on the other indices that are less sensitive to sample size. A model was considered to have good fit if the CFI and TLI ≥ .95, the RMSEA ≤ .06, and the SRMR ≤ .08 (Hu & Bentler, 1999). An a priori developmental model was tested for fit. Multiple-group models were then tested across the six cultural groups and across the different informants used to examine youths’ adjustment. A configural invariance model in which no parameter estimates were constrained to be equal was compared with a model in which all structural paths were constrained to be equal across groups. Following Cheung and Rensvold (2002), if the differences in χ2 values for the two models were nonsignificant, we could be reasonably certain that the model fit well across groups. As in the a priori model, if the difference in fit between the constrained and unconstrained multiple group models did not meet the criteria above, we examined model modification indices and iteratively released paths. This procedure identifies paths that are community-specific rather than universal.
Mediated effects were calculated using the procedures outlined by MacKinnon, Lockwood, Hoffman, West, and Sheets (2002). Furthermore, we used the asymmetric confidence interval method recommended by MacKinnon et al. (2002) to formally test mediation. The critical values for the upper and lower confidence limits for indirect effects were calculated using the program PRODCLIN2 (MacKinnon, Fritz, Williams, & Lockwood, 2007).
3. Results
3.1. Descriptive statistics and correlations
Table 1 displays descriptive statistics for the overall sample, separately for mothers, fathers, and adolescents. Univariate normality of variables was examined, and none of the variables was found to have univariate skewness > 2.0 or kurtosis > 7.0 (Curran, West, & Finch, 1996). Correlations among the examined variables for the overall sample are reported in Table 2. T1 and T3 Descriptive statistics and correlations separately by cultural group are in Supplementary Tables S2-S8.
Table 2.
Correlations among the examined variables in the total sample.
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) | (14) | (15) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Early adolescents’ gender | (1) | 1 | ||||||||||||||
| Early adolescents’ age; T1 | (2) | .01 | 1 | |||||||||||||
| Parental education; T1 | (3) | −.03 | .05 | 1 | ||||||||||||
| Mothers’ self-efficacy beliefs about their own anger regulation | ||||||||||||||||
| Mother report; T1 | (4) | −.01 | −.01 | .08 | 1 | |||||||||||
| Mother report; T3 | (5) | −.02 | .03 | .06 | .53** | 1 | ||||||||||
| Fathers’ self-efficacy beliefs about their own anger regulation | ||||||||||||||||
| Father report; T1 | (6) | .02 | −.01 | .01 | .04 | .04 | 1 | |||||||||
| Father report; T3 | (7) | .05 | .05 | .04 | .15** | .18** | .26** | 1 | ||||||||
| Early adolescents’ self-efficacy beliefs about their own anger regulation | ||||||||||||||||
| Self report; T2 | (8) | .01 | .02 | .01 | .10* | .14** | −.01 | .09 | 1 | |||||||
| Early adolescent internalizing problems | ||||||||||||||||
| Parent report; T1 | (9) | .05 | −.05 | −.21** | −.24** | −.22** | −.02 | −.23** | −.04 | 1 | ||||||
| Parent report; T3 | (10) | .16** | −.04 | −.18** | −.27** | −.26** | −.06 | −.26** | −.11* | .66** | 1 | |||||
| Self report; T1 | (11) | .09* | −.07 | −.01 | −.03 | −.01 | −.01 | −.10 | −.22** | .20** | .20** | 1 | ||||
| Self report; T3 | (12) | .26** | .04 | .04 | −.07 | −.11** | −.01 | −.02 | −.22** | .23** | .46** | .34** | 1 | |||
| Early adolescent externalizing problems | ||||||||||||||||
| Parent report; T1 | (13) | −.03 | −.07 | −.18** | −.11* | −.14** | −.03 | −.16** | −.08 | .63** | .09* | .37** | .11* | 1 | ||
| Parent report; T3 | (14) | −.01 | −.08 | −.24** | −.15** | −.25** | −.04 | −.21** | −.15** | .44** | .10* | .55** | .17** | .67** | 1 | |
| Self report; T1 | (15) | −.03 | −.08 | −.19** | −.15** | −.20** | −.01 | −.10 | −.07 | .59** | .08 | .36** | .10* | .92** | .65** | 1 |
| Self report; T3 | (16) | .11* | .03 | .08 | −.01 | −.09* | .02 | .01 | −.33** | .14** | .34** | .18** | .59** | .29** | .26** | .37** |
Note.
p ≤ 0.05;
p ≤ 0.01.
3.2. Mothers’, fathers’, and early adolescents’ self-efficacy about anger regulation and early adolescents’ adjustment
In the first path analysis (i.e., with parents’ reports of early adolescents’ adjustment at age 13 as an outcome), the a priori model (Fig. 1) fit the data, χ2(4) = 9.98, p = .05, CFI = 1.00, RMSEA = .05, 90% CI = .01–.09, SRMR = .02. In this model, all measures were highly stable across time. Stronger mothers’ self-efficacy beliefs about anger regulation (when youths were 10) were associated with stronger early adolescents’ self-efficacy beliefs about anger regulation at age 12, which was in turn inversely associated with early adolescents’ internalizing and externalizing symptoms at age 13. We tested whether the relation of mothers’ self-efficacy beliefs to internalizing and externalizing symptoms was mediated through early adolescents’ self-efficacy beliefs. Considering both internalizing and externalizing symptoms as outcomes, the unstandardized indirect effects were not significant (b = .0021, SE = 0.001; 95% CI = −0.006, 0 and b = .0021, SE = 0.001; 95% CI = −0.005, 0, respectively).
In the second path analysis (i.e., with early adolescents’ self-reported adjustment as the outcome), the a priori model fit the data, χ2(4) = 12.99, p = .02, CFI = .99, RMSEA = .06, 90%CI = .03–.10, SRMR = .02. As found in the previous path analysis, stronger mothers’ self-efficacy beliefs about anger regulation when their children were 10 were associated with stronger early adolescents’ self-efficacy beliefs about anger regulation at age 12, which were in turn associated with lower levels of early adolescents’ internalizing and externalizing symptoms at age 13. For both internalizing and externalizing symptoms as outcomes, the unstandardized indirect effect was significant (b = −.005, SE = .003; 95% CI = −.011, −.001 and b = −.005, SE = .002; 95% CI = −.01, −.001, respectively).
3.3. Multiple-group model: results for cross-cultural comparisons
By testing multiple-groups models, we examined whether the effects were broadly generalizable or circumscribed to a subset of groups. Multiple-group models were tested across the six cultural groups (one from Colombia, two from Italy [from the cities of Rome and Naples], and three ethnic groups from the US [African Americans, European Americans, and Hispanics]) to determine whether the model fit for each group. A configural invariance model with no constraints had good fit for both the model with parents’ reports of early adolescent adjustment as the outcome (i.e., Model 1; χ2(24) = 30.76, p = .16, CFI = 1.00, RMSEA = .07, 90%CI = .03–.10, SRMR = .05) and the model with self-reports of early adolescent adjustment as the outcome (i.e., Model 2; χ2(24) = 34.07, p = .08, CFI = .99, RMSEA = .06, 90%CI = .00–.12, SRMR = .03). These unconstrained models were compared to models with equality constraints across the six cultural groups (within-wave covariances and the impact of the covariates on the examined variables also were constrained to be invariant across cultures). The differences in model fit, Model 1: Δχ2(295) = 399.72, p < .001 and Model 2: Δχ2(295) = 405.52, p < .001, indicated that all paths were not invariant across the six cultural groups.
To achieve an acceptable difference in model fit, we incrementally released nine paths in the model with parent-reported youth adjustment and nine paths in the model with adolescent self-reported adjustment. Change in model fit for the revised models was—Model 1: Δχ2(286) = 321.09, p = .08 and Model 2: Δχ2(286) = 325.26, p = .05. To put these modifications in context, there were 59 paths across the six groups (i.e., 354 paths total) that could have been released, but only 9 (2.5%) had to be released in both models to achieve a nonsignificant difference in model fit. Thus, except for very few structural paths in the model, the final model fit for families across the six cultural groups.
Looking across multiple-group models, several paths were consistently invariant. In both models, for parent- and self-reports of early adolescent adjustment (Figs. 3 and 4, respectively), the following paths were invariant and significant: the stability of externalizing symptoms from T1 to T3; the bidirectional negative association between early adolescents’ self-efficacy about anger regulation and early adolescents’ externalizing problems; and the negative association between early adolescents’ self-efficacy about anger regulation at T2 and early adolescents’ internalizing symptoms at T3. In addition, in the model examining parent-reported early adolescent adjustment, the following paths were invariant and significant: the stability of both fathers’ self-efficacy beliefs and early adolescents’ internalizing symptoms from T1 to T3; the negative association between mothers’ self-efficacy about anger regulation at T1 and early adolescents’ internalizing and externalizing symptoms at T3; and the negative association between early adolescents’ internalizing symptoms at T1 and fathers’ self-efficacy beliefs at T3. In the model examining self-reports of early adolescents’ adjustment, the following path was invariant and significant: the negative association between early adolescents’ internalizing symptoms at T1 and early adolescents’ self-efficacy beliefs at T2. Considering the structural paths from the conceptual model, the only path that was different cross-culturally was the association from mothers’ self-efficacy about anger regulation at T1 to early adolescents’ self-efficacy about anger regulation at T2. This path was nonsignificant only for African Americans in both models with parent- and self -reports of early adolescents’ adjustment. Moreover, two cross-cultural differences emerged when examining self-reports of early adolescents’ internalizing problems: (a) stronger father self-efficacy about anger regulation at T1 was associated (unexpectedly) with more internalizing symptoms at T3 only among Colombians; and (b) more internalizing problems at T1 were associated with weaker maternal self-efficacy beliefs about anger regulation at T3 only among European Americans from the United States. See Supplementary Information for details regarding models (see Supplementary Tables S9 and S10).
Fig. 3.
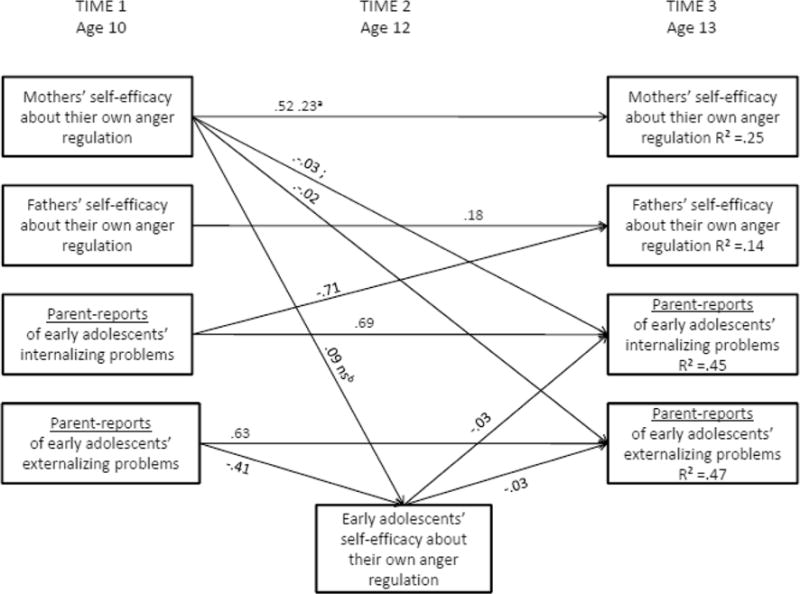
Partially constrained model of relations among mothers’ and fathers’ self-efficacy about anger regulation, early adolescents’ self-efficacy about anger regulation, and parents’reports of early adolescents’ internalizing and externalizing problems across six ethnic/cultural groups, controlling for parental education, early adolescents’ sex and age (not shown), and within-wave relations (not shown). Note. Only significant paths (p < .01) for at least one out of six cultural groups are reported. Unstandardized coefficients are presented. The numbers without a superscript refer to those paths for which the six cultural groups were constrained to be equal. Superscripts a and b indicate the paths for which the equality constraint was lifted in one cultural group in comparison to the other ones. The equality constraint was lifted from the following paths: a in Naples; b in U.S. African Americans. For ease of interpretation, within-wave covariances and paths from parental education, child sex, and age are not depicted in the Figure (see Supplementary Tables S9 and S10; in addition, the standardized coefficients separately by group are reported in Tables S11–S16).
Fig. 4.
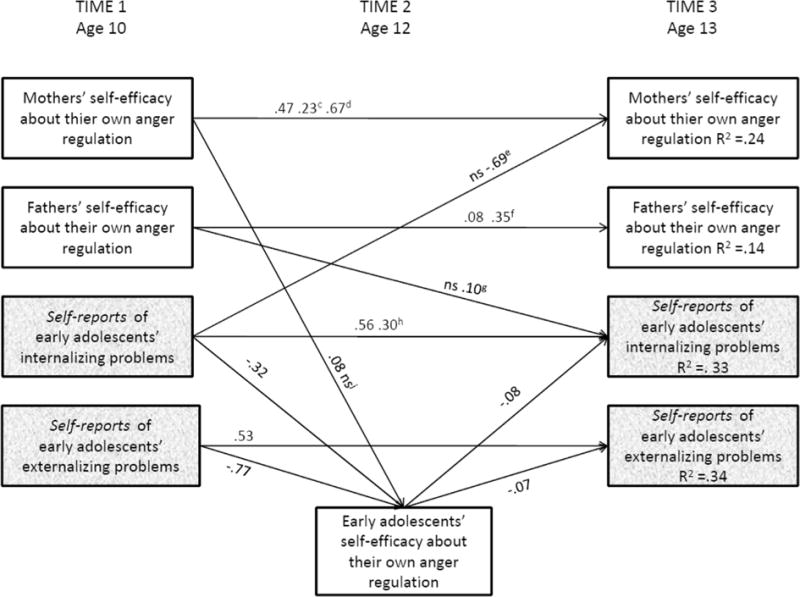
Partially constrained model of relations among mothers’ and fathers’ self-efficacy about anger regulation, early adolescents’ self-efficacy about anger regulation, and self-reports of early adolescents’ internalizing and externalizing problems across six ethnic/cultural groups, controlling for parental education, early adolescents’ sex and age (not shown), and within-wave relations (not shown). Note. Only significant paths (p < .01) for at least one out of six cultural groups are reported. Unstandardized coefficients are presented. The numbers without a superscript refer to those paths for which the six cultural groups were constrained to be equal. Superscripts c to i indicate the path for which the equality constraint was lifted in one cultural group in comparison to the others. The equality constraint was lifted from the following paths: c in Naples; d in U.S. European Americans; e in U.S. European Americans; f in Rome; g in Colombia; h in U.S. Hispanics; i in U.S. African Americans. For ease of interpretation, within-wave covariances and paths from parental education, child sex and age are not depicted in the Figure (see Supplementary Tables S9 and S10; in addition, the standardized coefficients separately by group are reported in Tables S11–S16).
4. Discussion
Mental health problems often have their origins in adolescence and are associated with a wide range of adverse outcomes in adulthood (e.g., Costello et al., 2011). Understanding the determinants of adolescents’ mental health problems can contribute to improving future generations’ well-being. Previous studies suggest that adolescents’ emotional and behavioral problems might vary across cultures and have changed over time (e.g., Achenbach et al., 2003; Collishaw et al., 2010; Tick et al., 2007). One cannot assume that factors predicting maladjustment today are the same as those from decades ago. Therefore, it is important to examine determinants of adolescents’ internalizing and externalizing problems within current cultural contexts and across cultural contexts.
We examined with multiple cultural groups the prediction by self-efficacy beliefs about anger regulation of early adolescents’ internalizing and externalizing problems (e.g., Bandura et al., 2003; Caprara et al., 2010). We found that stronger maternal self-efficacy beliefs about anger regulation were associated with stronger early adolescent self-efficacy beliefs about anger regulation. This finding is consistent with previous theoretical models positing that observational learning that occurs within the family context (Eisenberg et al., 1998; Morris et al., 2007) affects youths’ personality. Overall, this path was supported in all countries and ethnic groups examined with one exception–African Americans in the US. We are hesitant to interpret this group difference because it constituted such a small percentage of the overall number of paths tested (i.e., in our model, only 2.5% had to be released). Overall, it appears that across cultural and ethnic groups mothers’ beliefs about how well they can regulate their anger in stressful situations is associated with their children’s beliefs about how well they can regulate their own ager in similar situations.
We did not find support for the relation between fathers’ and children’s self-efficacy beliefs. One possible explanation for this result is that there may be fewer opportunities for early adolescents to observe fathers’ self-efficacy beliefs about anger regulation. For example, mothers spend more time with their children in direct physical and nonphysical care (e.g., food preparation and nurturing) whereas fathers spend more time with their children in play activities (Bonney, Kelley, & Levant, 1999). Thus, in comparison to fathers, mothers might be more likely to experience stressful situations that provide modeling of self-efficacy beliefs of anger regulation to their children.
Consistent with prior theory (Eisenberg et al., 1998; Morris et al., 2007), we found that parents’ self-efficacy beliefs predicted not only early adolescents’ self-efficacy, but also early adolescents’ adjustment. Across the six groups, mothers’ stronger self-efficacy beliefs about anger regulation were invariantly associated with early adolescents’ greater internalizing and externalizing symptoms three years later across the six groups. These findings were specific to parents’ reports of early adolescents’ adjustment, whereas paths to early adolescents’ self-reported adjustment were invariant and not significant. Thus, a partial source of this significant longitudinal association might be due to shared method variance. However, we found the opposite path to be significant as well from (a) parents’ reports of early adolescent internalizing problems at T1 to lower fathers’ self-efficacy beliefs about anger regulation at T3 (this path was invariant across the six cultural groups) and from (b) early adolescents’ self-reported internalizing problems at T1 to lower mothers’ self-efficacy beliefs about anger regulation at T3. The latter path was significant only for European Americans from the USA so it is not a robust finding. Moreover, unexpectedly, we found that only among Colombians, fathers with stronger self-efficacy beliefs about anger regulation had children who reported more internalizing problems. Although this finding is limited and preliminary, one possible explanation for it might be empathic self-efficacy (i.e., the ability to sense another person’s feelings and need for emotional support; Bandura et al., 2003). Previous research suggests that early adolescent girls with more empathic self-efficacy are more vulnerable to internalizing symptoms (Bandura et al., 2003). Furthermore, mothers who are emotionally competent (e.g., high in empathy, high in positive emotional communication) tend to have adolescent children who are high in empathy-related functioning (e.g., high in perspective taking and sympathy; Eisenberg & McNally, 1993; Eisenberg, VanSchyndel, & Hofer, 2015). Thus, it might be that Colombian fathers, whose involvement in parenting in the last decade has increased (Gómez, 2006; Ripoll-Núñez & Alvarez, 2008), and who are also emotionally competent (i.e., high in self-efficacy beliefs about anger regulation), might have adolescent children who are high in empathic self-efficacy, and who are in turn also high in internalizing symptoms. Those are speculations that will need further verification.
Consistent with previous findings that there are negative relations between adolescents’ self-efficacy beliefs about emotion regulation and mental health symptoms (e.g., Bandura et al., 2003; Caprara et al., 2010; Valois et al., 2015; Zullig et al., 2014), we found that early adolescents’ self-efficacy beliefs about anger regulation were associated with both externalizing and internalizing symptoms, and both of these paths were invariant across cultures. We also found that early adolescents’ self-efficacy about anger regulation mediated the relation between mothers’ self-efficacy beliefs about anger regulation and. early adolescents’ self-reported adjustment (even after controlling for several important factors). In other words, after witnessing their mothers’ low self-efficacy beliefs about anger regulation, early adolescents may come to believe that they are incapable of dealing with their own anger and act in ways consistent with such beliefs, resulting in poorer adjustment during adolescence (e.g., Bandura et al., 2003; Caprara et al., 2008).
Fewer internalizing and externalizing symptoms at T1 were associated with early adolescents’ stronger self-efficacy beliefs about anger regulation at T2. This result is in line with Bandura’s (1997) view that mastery experiences are an important source of information about self-efficacy. Early adolescents who experience more internalizing and externalizing symptoms presumably have fewer mastery experiences regarding emotion regulation which in turn might predict their beliefs about how well they can handle difficult emotional situations.
4.1. Strengths, limitations and conclusions
Our multi-reporter work contributes conceptually to the literature by demonstrating that self-efficacy beliefs about anger regulation are cognitive mechanisms shared by family members. In addition, our longitudinal design allowed us to examine reciprocal relations among some variables (i.e., parents’ self-efficacy and early adolescents’ behavioral problems) which, as argued by Cole and Maxwell (2003) provides a more stringent test of mediation than does the use of cross-sectional data.
One limitation of this study is the low to moderate stability of paternal self-efficacy beliefs about anger regulation. This might have been due to the attrition rate of 12% of missing fathers from T1 to T3 or because of the small number of items used in this study. In addition, we found only limited support for our mediational hypotheses—only two (out of 8) were supported. One reason might be that our model did not consider another important link between parents’ and early adolescents’ self-efficacy beliefs, namely parenting quality. For example, parents who believe they are less capable of handling anger might be more likely to use corporal punishment or psychological aggression, which does not provide good modeling to their children and could influence their children’s self-efficacy beliefs about anger regulation. Future studies should investigate the mediating role of parenting behaviors on the relations between parents’ and adolescents’ self-efficacy beliefs about emotion regulation. A better understanding of early adolescents’ self-efficacy beliefs about anger regulation and their antecedents (e.g., parents’ self-efficacy about anger regulation) could advance scientists’ and practitioners’ abilities to identify, prevent, and ameliorate the antecedents and negative consequences of poor psychological adjustment in adolescence. Self-efficacy beliefs about emotion regulation are closely aligned with techniques already used in interventions for adolescents (Caprara et al., 2014; 2015). Explicating the influence of parents’ and early adolescents’ self-efficacy beliefs about emotion regulation could have clear translatable implications for enhancing existing empirically-based intervention methods. Our results highlight the utility of focusing on parents’ and early adolescents’ self-efficacy about anger regulation, as a promising cross-cultural deterrent of adolescent mental health problems. Improving mothers’ self-efficacy beliefs about their ability to manage anger can indirectly reduce the risk of mental health problems for their children by affecting their children’s self-efficacy beliefs about anger regulation. If replicated and verified with additional experimental and longitudinal research, these findings can be translated into interventions designed to improve emotion regulation skills to decrease early adolescent health risk behaviors (e.g., Houck et al., 2016).
Supplementary Material
Acknowledgments
We thank the families who participated in this research and the many research assistants who helped gather data.
Funding
This research was funded by the Jacobs Foundation, the Josiah Charles Trent Memorial Foundation, the Transdisciplinary Prevention Research Center at Duke University, the Eunice Kennedy Shriver National Institute of Child Health and Human Development [grant RO1-HD054805], and the Fogarty International Center [grant RO3-TW008141].
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.adolescence.2018.01.009.
Footnotes
This article is part of a Special Issue entitled Adolescent Psychopathology in Times of Change.
Conflicts of interest
The authors declare no conflicts of interest.
References
- Achenbach TM. Integrative guide for the 1991 CBCL/4-18, YSR, and TRF profiles. Burlington, VT: University of Vermont, Department of Psychiatry; 1991. [Google Scholar]
- Achenbach TM. Cross-cultural perspectives on developmental psychopathology. In: Gielen UP, Roopnarine J, editors. Childhood and adolescence: Cross-cultural perspectives and applications. Westport, CT: Praeger; 2004. pp. 411–429. [Google Scholar]
- Achenbach TM, Dumenci L, Rescorla LA. Are American children’s problems still getting worse? A 23-year comparison. Journal of Abnormal Child Psychology. 2003;31:1–11. doi: 10.1023/a:1021700430364. http://dx.doi.org/10.1023/A:1021700430364. [DOI] [PubMed] [Google Scholar]
- Arbuckle JL. Full information estimation in the presence of incomplete data. In: Marcoulides GA, Schumacker RE, editors. Advanced structural equation modeling. Mahwah, NJ: Erlbaum; 1996. pp. 243–277. [Google Scholar]
- Bandura A. Social foundations of thought and action: A social cognitive. Englewood Cliffs, NJ: Prentice Hall; 1986. [Google Scholar]
- Bandura A. Self-efficacy: The exercise of control. New York: Freeman; 1997. [Google Scholar]
- Bandura A. Social cognitive theory in cultural context. Journal of Applied Psychology: An International Review. 2002;51:269–290. [Google Scholar]
- Bandura A, Caprara GV, Barbaranelli C, Gerbino M, Pastorelli C. Role of affective self-regulatory efficacy on diverse spheres of psychosocial functioning. Child Development. 2003;74:769–782. doi: 10.1111/1467-8624.00567. http://dx.doi.org/10.1111/1467-8624.00567. [DOI] [PubMed] [Google Scholar]
- Bonney JF, Kelley ML, Levant RF. A model of fathers’ behavioral involvement in child care in dual-earner families. Journal of Family Psychology. 1999;13:401–415. http://dx.doi.org/10.1037/0893-3200.13.3.401. [Google Scholar]
- Bridgett DJ, Burt NM, Edwards ES, Deater-Deckard K. Intergenerational transmission of self-regulation: A multidisciplinary review and integrative conceptual framework. Psychological Bulletin. 2015;141(3):602. doi: 10.1037/a0038662. http://dx.doi.org/10.1037/a0038662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brotman MA, Kircanski K, Leibenluft E. Irritability in children and adolescents. Annual Review of Clinical Psychology. 2017;13:317–341. doi: 10.1146/annurev-clinpsy-032816-044941. http://dx.doi.org/10.1146/annurev-clinpsy-032816–044941. [DOI] [PubMed] [Google Scholar]
- Caprara GV, Di Giunta L, Eisenberg N, Gerbino M, Pastorelli C, Tramontano C. Assessing regulatory emotional self-efficacy: A cross cultural study. Psychological Assessment. 2008;20:227–237. doi: 10.1037/1040-3590.20.3.227. http://dx.doi.org/10.1037/1040-3590.20.3.227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caprara GV, Di Giunta L, Pastorelli C, Eisenberg N. Mastery of negative affect: A hierarchical model of emotional self-efficacy beliefs. Psychological Assessment. 2013a;25:105–116. doi: 10.1037/a0029136. http://dx.doi.org/10.1037/a0029136. [DOI] [PubMed] [Google Scholar]
- Caprara GV, Gerbino M, Paciello M, Di Giunta L, Pastorelli C. Counteracting depression and delinquency in late adolescence: The role of regulatory emotional and interpersonal self-efficacy beliefs. European Psychologist. 2010;15:34–48. http://dx.doi.org/10.1027/1016-9040/a000004. [Google Scholar]
- Caprara GV, Kanacri BPL, Gerbino M, Zuffianò A, Alessandri G, Vecchio G, Bridglall B. Positive effects of promoting prosocial behavior in early adolescence: Evidence from a school-based intervention. International Journal of Behavioral Development. 2014;38:386–396. http://dx.doi.org/10.1177/0165025414531464. [Google Scholar]
- Caprara GV, Kanacri BPL, Zuffianò A, Gerbino M, Pastorelli C. Why and how to promote adolescents’ prosocial behaviors: Direct, mediated and moderated effects of the CEPIDEA school-based program. Journal of Youth and Adolescence. 2015;44:2211–2229. doi: 10.1007/s10964-015-0293-1. http://dx.doi.org/10.1007/s10964-015-0293-1. [DOI] [PubMed] [Google Scholar]
- Caprara G, Vecchione M, Barbaranelli C, Alessandri G. Emotional stability and affective self-regulatory efficacy beliefs: Proofs of integration between trait theory and social cognitive theory. European Journal of Personality. 2013b;27:145–154. http://dx.doi.org/10.1002/per.1847. [Google Scholar]
- Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling. 2002;9:233–255. http://dx.doi.org/10.1207/S15328007SEM0902_5. [Google Scholar]
- Cole DA, Maxwell SE. Testing mediational models with longitudinal data: Questions and tips in the use of structural equation modeling. Journal of Abnormal Psychology. 2003;112:558–577. doi: 10.1037/0021-843X.112.4.558. http://dx.doi.org/10.1037/0021-843X.112.4.558. [DOI] [PubMed] [Google Scholar]
- Collishaw S, Maughan B, Natarajan L, Pickles A. Trends in adolescent emotional problems in England: A comparison of two national cohorts twenty years apart. Journal of Child Psychology and Psychiatry. 2010;51:885–894. doi: 10.1111/j.1469-7610.2010.02252.x. http://dx.doi.org/10.1111/j.1469-7610.2010.02252.x. [DOI] [PubMed] [Google Scholar]
- Copeland WE, Shanahan L, Egger H, Angold A, Costello EJ. Adult diagnostic and functional outcomes of DSM-5 disruptive mood dysregulation disorder. American Journal of Psychiatry. 2014;171:668–674. doi: 10.1176/appi.ajp.2014.13091213. http://dx.doi.org/10.1176/appi.ajp.2014.13091213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costello EJ, Copeland W, Angold A. Trends in psychopathology across the adolescent years: What changes when children become adolescents, and when adolescents become adults? Journal of Child Psychology and Psychiatry. 2011;52:1015–1025. doi: 10.1111/j.1469-7610.2011.02446.x. http://dx.doi.org/10.1111/j.1469-7610.2011.02446.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curran PJ, West SG, Finch JF. The robustness of test statistics to non-normality and specification error in confirmatory factor analysis. Psychological Methods. 1996;1:16–29. http://dx.doi.org/10.1037/1082-989X.1.1.16. [Google Scholar]
- Denham SA, Mitchell-Copeland J, Strandberg K, Auerbach S, Blair K. Parental contributions to preschoolers’ emotional competence: Direct and indirect effects. Motivation and Emotion. 1997;21:65–86. http://dx.doi.org/10.1023/A:1024426431247. [Google Scholar]
- Di Giunta L, Iselin AM, Eisenberg N, Pastorelli C, Gerbino M, Lansford JE, Thartori E. Measurement invariance and convergent validity of anger and sadness self-regulation scales among youth from six cultural groups. Assessment. 2017;24:484–502. doi: 10.1177/1073191115615214. http://dx.doi.org/10.1177/1073191115615214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, Cumberland A, Spinrad TL. Parental socialization of emotion. Psychological Inquiry. 1998;9:241–273. doi: 10.1207/s15327965pli0904_1. http://dx.doi.org/10.1207/s15327965pli0904_1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, McNally S. Socialization and mothers’ and adolescents’ empathy-related characteristics. Journal of Research on Adolescence. 1993;3:171–191. http://dx.doi.org/10.1207/s15327795jra0302_4. [Google Scholar]
- Eisenberg N, Spinrad TL. Emotion-related regulation: Sharpening the definition. Child Development. 2004;75:334–339. doi: 10.1111/j.1467-8624.2004.00674.x. http://dx.doi.org/10.1111/j.1467-8624.2004.00674.x. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, VanSchyndel SK, Hofer C. The association of maternal socialization in childhood and adolescence with adult offsprings’ sympathy/caring. Developmental Psychology. 2015;51:7–16. doi: 10.1037/a0038137. http://dx.doi.org/10.1037/a0038137. [DOI] [PubMed] [Google Scholar]
- Erkut S. Developing multiple language versions of instruments for intercultural research. Child Development Perspectives. 2010;4:19–24. doi: 10.1111/j.1750-8606.2009.00111.x. http://dx.doi.org/10.1111/j.1750-8606.2009.00111.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fichter MM, Xepapadakos F, Quadflieg N, Georgopoulou E, Fthenakis WE. A comparative study of psychopathology in Greek adolescents in Germany and in Greece in 1980 and 1998 -18 years apart. European Archives of Psychiatry and Clinical Neuroscience. 2004;254:27–35. doi: 10.1007/s00406-004-0450-0. http://dx.doi.org/10.1007/s00406-004-0450-0. [DOI] [PubMed] [Google Scholar]
- Gómez V. Quality of family and work roles and its relationship with health indicators in men and women. Sex Roles. 2006;55:787–799. http://dx.doi.org/10.1007/s11199-006-9132-x. [Google Scholar]
- Houck CD, Hadley W, Barker D, Brown LK, Hancock E, Almy B. An emotion regulation intervention to reduce risk behaviors among at-risk early adolescents. Prevention Science. 2016;17:71–82. doi: 10.1007/s11121-015-0597-0. http://dx.doi.org/10.1007/s11121-015-0597-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. http://dx.doi.org/10.1080/10705519909540118. [Google Scholar]
- Kessler RC, Angermeyer M, Anthony JC, De Graff R, Demyttenaere K, Gasquet I, Üstün TB. Lifetime prevalence and age-of-onset distributions of mental disorders in the world health Organization’s world mental health survey initiative. World Psychiatry. 2007;6:168–176. [PMC free article] [PubMed] [Google Scholar]
- Kim-Cohen J, Caspi A, Moffitt TE, Harrington H, Milne BJ, Poulton R. Prior juvenile diagnoses in adults with mental disorder: Developmental follow-back of a prospective-longitudinal cohort. Archives of General Psychiatry. 2003;60:709–717. doi: 10.1001/archpsyc.60.7.709. http://dx.doi.org/10.1001/archpsyc.60.7.709. [DOI] [PubMed] [Google Scholar]
- Kitayama S, Markus H, Kurokawa M. Culture, emotion, and well-being: Good feelings in Japan and the United States. Cognition and Emotion. 2000;14:93–124. http://dx.doi.org/10.1080/026999300379003. [Google Scholar]
- Kline RB. Principles and practices of structural equation modeling. New York: Guilford; 1998. [Google Scholar]
- Kosidou K, Magnusson C, Mittendorfer-Rutz E, Hallqvist J, HellnerGumpert C, Idrizbegovic S, Dalman C. Recent time trends in levels of self-reported anxiety, mental health service use and suicidal behaviour in Stockholm. Acta Psychiatrica Scandinavica. 2010;122:47–55. doi: 10.1111/j.1600-0447.2009.01487.x. http://dx.doi.org/10.1111/j.1600-0447.2009.01487.x. [DOI] [PubMed] [Google Scholar]
- Lansford JE, Sharma C, Malone PS, Woodlief D, Dodge KA, Oburu P, & Tirado LMU. Corporal punishment, maternal warmth, and child adjustment: A longitudinal study in eight countries. Journal of Clinical Child & Adolescent Psychology. 2014;43:670–685. doi: 10.1080/15374416.2014.893518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Fritz MS, Williams J, Lockwood CM. Distribution of the product confidence limits for the indirect effect: Program PRODLIN. Behavior Research Methods. 2007;39:384–389. doi: 10.3758/bf03193007. http://dx.doi.org/10.3758/BF03193007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7:83–104. doi: 10.1037/1082-989x.7.1.83. http://dx.doi.org/10.1037/1082-989X.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markus HR, Kitayama S. Culture and the self: Implications for cognition, emotion, and motivation. Psychological Review. 1991;98:224–253. http://dx.doi.org/10.1037/0033-295X.98.2.224. [Google Scholar]
- Matsumoto D, Yoo SH, Fontaine J. Mapping expressive differences around the world: The relationship between emotional display rules and individualism versus collectivism. Journal of Cross-Cultural Psychology. 2008;39:55–74. http://dx.doi.org/10.1177/0022022107311854. [Google Scholar]
- Maxwell B. Translation and cultural adaptation of the survey instruments. In: Martin MO, Kelly DL, editors. Third international mathematics and science study (TIMSS) technical report, volume I: Design and development. Chestnut Hill, MA: Boston College; 1996. [Google Scholar]
- Mesquita B. Emotions in collectivist and individualist contexts. Journal of Personality and Social Psychology. 2001;80:68–74. doi: 10.1037//0022-3514.80.1.68. http://dx.doi.org/10.1037/0022-3514.80.1.68. [DOI] [PubMed] [Google Scholar]
- Morris AS, Silk JS, Steinberg L, Myers SS, Robinson LR. The role of the family context in the development of emotion regulation. Social Development. 2007;16:361–388. doi: 10.1111/j.1467-9507.2007.00389.x. http://dx.doi.org/10.1111/j.1467-9507.2007.00389.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. 7th. Los Angeles, CA: Muthén&Muthén; 1998–2012. [Google Scholar]
- Nock MK, Kazdin AE, Hiripi E, Kessler RC. Lifetime prevalence, correlates, and persistence of oppositional defiant disorder: Results from the National Comorbidity Survey Replication. Journal of Child Psychology and Psychiatry. 2007;48:703–713. doi: 10.1111/j.1469-7610.2007.01733.x. http://dx.doi.org/10.1111/j.1469-7610.2007.01733.x. [DOI] [PubMed] [Google Scholar]
- Pickles A, Aglan A, Collishaw S, Messer J, Rutter M, Maughan B. Predictors of suicidality across the life span: The Isle of Wight study. Psychological Medicine. 2010;40:1453–1466. doi: 10.1017/S0033291709991905. http://dx.doi.org/10.1017/S0033291709991905. [DOI] [PubMed] [Google Scholar]
- Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry. 2015;56:345–365. doi: 10.1111/jcpp.12381. http://dx.doi.org/10.1111/jcpp.12381. [DOI] [PubMed] [Google Scholar]
- Potthoff S, Garnefski N, Miklósi M, Ubbiali A, Domínguez-Sánchez FJ, Martins EC, Kraaij V. Cognitive emotion regulation and psychopathology across cultures: A comparison between six European countries. Personality and Individual Differences. 2016;98:218–224. http://dx.doi.org/10.1016/j.paid.2016.04.022. [Google Scholar]
- Ripoll-Núñez K, Alvarez C. Perceived intimate partner acceptance, remembered parental acceptance, and psychological adjustment among Colombian and Puerto Rican youths and adults. Cross-Cultural Research: The Journal of Comparative Social Science. 2008;42(1):23–34. http://dx.doi.org/10.1177/1069397107309859. [Google Scholar]
- Stringaris A, Cohen P, Pine DS, Leibenluft E. Adult outcomes of youth irritability: A 20-year prospective community-based study. American Journal of Psychiatry. 2009;166:1048–1054. doi: 10.1176/appi.ajp.2009.08121849. http://dx.doi.org/10.1176/appi.ajp.2009.08121849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tick NT, Van Der Ende J, Verhulst FC. Twenty-year trends in emotional and behavioral problems in Dutch children in a changing society. Acta Psychiatrica Scandinavica. 2007;116:473–482. doi: 10.1111/j.1600-0447.2007.01068.x. http://dx.doi.org/10.1111/j.1600-0447.2007.01068.x. [DOI] [PubMed] [Google Scholar]
- UNDP (United Nations Development Programme) Human development reports. 2012 Retrieved April 22, 2017 from http://hdr.undp.org/en/content/human-development-index-hdi.
- Valois RF, Zullig KJ, Hunter AA. Association between adolescent suicide ideation, suicide attempts and emotional self-efficacy. Journal of Child and Family Studies. 2015;24:237–248. http://dx.doi.org/10.1007/s10826-013-9829-8. [Google Scholar]
- Weisz JR, Suwanlert S, Chaiyasit W, Walter BR. Over- and undercontrolled referral problems among children and adolescents from Thailand and the United States: The wat and wai of cultural differences. Journal of Consulting and Clinical Psychology. 1987;55:719–726. doi: 10.1037//0022-006x.55.5.719. 10.1037=0022-006X.55.5.719. [DOI] [PubMed] [Google Scholar]
- Wong KYM. (Report submitted to Department of Applied Social Studies in Partial fulfillment of the Requirements for the Bachelor for Social Sciences in Psychology).A cultural comparison of cognitive emotion regulation strategies: Moderation of cultural values on psychological well-being. 2009 Retrieved April 22, 2017 from http://lbms03.cityu.edu.hk/oaps/ss2009-4708-wky771.pdf.
- Zullig KJ, Teoli DA, Valois RF. Emotional self-efficacy and alcohol and tobacco use in adolescents. Journal of Drug Education. 2014;44:51–66. doi: 10.1177/0047237915573526. http://dx.doi.org/10.1177/0047237915573526. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.