

Abstract
Socioeconomic status (SES) has a measurable and significant effect on cardiovascular health. Biologic, behavioral, and psychosocial risk factors prevalent in disadvantaged individuals accentuate the link between SES and cardiovascular disease (CVD). Four measures have been consistently associated with CVD in high-income countries: income level, educational attainment, employment status, and neighborhood socioeconomic factors. Additionally, disparities based on gender have been shown in several studies. Interventions targeting patients with low SES have predominantly focused on modification of traditional CVD risk factors. Promising approaches are emerging that can be implemented on an individual, community, or population basis to reduce disparities in outcomes. Structured physical activity has demonstrated effectiveness in low-SES populations, and geo-mapping may be used to identify targets for large-scale programs. Task shifting, the redistribution of healthcare management from physician to non-physician providers in an effort to improve access to healthcare, may have a role in select areas. Integration of SES into traditional CVD risk prediction models may allow improved management of high-risk individuals, but cultural and regional differences in SES make generalized implementation challenging. Future research is required to better understand the underlying mechanisms of CVD risk that affect individuals of low SES and to determine effective interventions for high-risk patients. We review the current state of knowledge on the impact of SES on the incidence, treatment, and outcomes of CVD in high-income societies and suggest future research directions aimed at the elimination of these adverse factors as well as the integration of measures of SES into the customization of cardiovascular treatment.
Keywords: Cardiovascular disease, socioeconomic status, social determinants of health, task shifting
Introduction
Cardiovascular diseases (CVD) remain the leading cause of death from chronic disease in the U.S. and worldwide despite remarkable advances made in the last century. CVD accounts for nearly 1 in 3 deaths in the U.S. despite a 25.3% decrease in age-standardized deaths attributed to CVD from 2004 to 2014.1 Traditional CVD risk factors have been identified, including hypertension, dyslipidemia, diabetes, family history of premature coronary heart disease (CHD), and smoking, however, the contribution of social determinants of health, as best represented by socioeconomic status (SES), to CVD risk is poorly understood. Low SES has been linked to the development of CVD and may confer a cardiovascular risk that is equivalent to traditional risk factors.2, 3 The increased burden of CVD in people with low SES is due to a constellation of biologic, behavioral, and psychosocial risk factors that are more prevalent in disadvantaged individuals.4, 5
Established interventions exist for addressing SES-related determinants of health and health inequities.6 Several interventions have been evaluated to improve health disparities due to social inequity, but results are inconsistent.7 Better understanding of SES and risk stratification are critical first steps in identifying and tailoring interventions to improve CVD risk in the population. We review the current state of knowledge on the impact of SES on the incidence, treatment, and outcomes of CVD in high-income societies and suggest future research directions aimed at the elimination of these adverse factors as well as the integration of measures of SES into the customization of cardiovascular treatment.
Overview of Socioeconomic Factors
The factors that comprise an individual’s SES vary between location and culture.8-10 Four markers for SES have demonstrated an association with CVD in high-income countries (HIC): income level, educational attainment, employment status, and environmental factors (see Figure 1).11-17 Although many factors have been used as surrogates for SES, these particular markers are advantageous due to their ease of collection by questionnaire in addition to the substantial existing literature characterizing their association with clinical CVD outcomes. Additionally, it is unlikely that a single marker of SES is adequate in predicting CVD risk due to the interactions between SES factors, regional variations in SES associations with CVD, and the dynamic changes between SES markers and CVD outcomes throughout an individual’s life course.8, 11, 18
Figure 1.
Markers of socioeconomic status.
Low- and middle-income countries (LMIC) carry approximately 80% of the global burden of CVD.19 However, studies evaluating the association between SES and cardiovascular health in LMIC are limited and often contain conflicting findings.10, 20 Furthermore, the association of SES and CVD in LMIC cannot be extrapolated from studies in HIC; obesity is an epidemic among the impoverished in HIC but is a disease of the rich in low-income countries due to increased access to a Western diet.21 Characterization of the impact of SES in LMIC will require additional high-quality prospective studies and is beyond the scope of this review.
Income Level
Income level has been consistently associated with CVD risk.11, 12 A large study in the United States and Finland found an increased risk of non-fatal MI and sudden cardiac death in the low-income cohorts that persisted after adjusting for smoking and alcohol consumption.12 The results may be applicable at both an individual and neighborhood level.22 Gerber et al. found that each $10,000 increase in median income of a neighborhood reduced mortality risk in the group by 10%.22
A study of more than 15,000 patients admitted for acute myocardial infarction (AMI) or CHD in the Netherlands found that individuals in the lower quintiles of income had significantly higher rates of 28-day and 1-year mortality.23 Increased mortality was also shown for the lowest income quartile compared to the highest income quartile in a cohort presenting with ST-elevation myocardial infarction (STEMI) (HR 1.17, 95% CI 1.11-1.25).24 Residents in low-income areas were less likely to receive a left heart catheterization within 24 hours of a STEMI or within 48 hours of a non-ST elevation myocardial infarction compared with patients from high-income areas.24 The authors of this study posited that the difference may be due to the perception that low-income individuals would be less likely to comply with critical post-percutaneous coronary intervention (PCI) medications (e.g. antiplatelet agents) or that low-income patients were less likely to be offered more expensive procedures (e.g. drug-eluting stents).24 The mortality difference between income groups in the study was attenuated after adjustment for time to left heart catheterization.24 Increased mortality rates were also present in patients from low-income areas in Taiwan, a HIC with universal healthcare, who were hospitalized with AMI.25
Mortality differences in low-income patients may be partially driven by disparities in standards of care. Low-income patients in the Netherlands were less likely to undergo interventions, including PCI, when presenting with AMI.23 Cardiac rehabilitation (CR), a proven therapy to reduce mortality and hospital readmissions after AMI,26, 27 is less likely to be attended or completed by individuals from low-income areas after hospitalization for CHD, PCI, or coronary artery bypass graft (CABG) surgery.28 Studies have also demonstrated that statin medications were less likely to be initiated after AMI in low-income individuals.29, 30 Men with low incomes were less likely to receive other guideline-recommended medications, including beta-blockers and angiotensin-converting enzyme inhibitors, but the association was attenuated in women.30
The substandard care may be partially explained by decreased access to quality care in the socially disadvantaged.31-33 Lack of access to quality care has been shown to increase heart failure and post-AMI hospital readmission rates in the United States,33 and patients with financial barriers to health care had fewer yearly medical checkups, were less likely to use aspirin, and were at higher risk of future CVD events.32
Low-income individuals in Taiwan undergoing CABG received lower quality care and experienced higher mortality than the high-income cohort.31 France, like Taiwan, has a national health system but still faces inequalities in access to primary care and coronary revascularizations in low-income areas.34 These studies highlight the difficulty in providing equal care to a patient population regardless of income. Inequalities in access to care, interventions, and prescribing practices will need to be addressed before care becomes equivalent between social groups.
Educational Attainment
The inverse relationship between educational attainment and CVD in HIC has been known for decades, and new population-based studies continue to provide insight into the strength of the association and its underlying mechanisms.13, 35 A large study by Woodward et al. analyzed nearly 90,000 individuals in Australia and New Zealand and found that those with a primary education had an increased risk of CVD, cardiovascular mortality, and all-cause mortality compared with individuals with a tertiary education.35 Higher education was associated with increased alcohol consumption and inversely related to smoking, blood pressure, cholesterol levels, and diabetes.35
Several studies have also demonstrated a higher risk of AMI in individuals with lower educational level.36-38 Lower educational attainment also predicts worse short term (30 day) and long term (≥1 year) outcomes after AMI.22, 39-41 Of the several socioeconomic factors examined in a cohort of patients from South Korea, only low education (≤6 years of schooling) was associated with increased risk of cardiac events or all-cause mortality.41 Patients with low SES tend to have an increased number of comorbidities but receive fewer interventions.40, 42 Despite their increased comorbidities, individuals with lower education level were less likely to be referred to tertiary prevention programs, including CR, than those who had higher education level.42
Educational attainment may affect health in several ways. Individuals with less education tend to have an increased number of CVD risk factors.5 An analysis in the Netherlands by Kershaw et al. demonstrated that a majority (56.6%) of CHD risk in individuals with low education was due to behavioral and biological risk factors.43 The most significant contributors were smoking (27.3%), obesity (10.2%), physical inactivity (6.3%), and hypertension (5.3%).43 Hu et al. determined that approximately half of the increased risk of incident AMI in low education groups was explained by traditional risk factors.36 Even with these estimates, the mechanisms underlying the remainder of the increased risk associated with low educational attainment remains to be determined.
A potential contributor to CVD risk is the strong correlation between education and health literacy.44, 45 Individuals with poor health literacy are more likely to be noncompliant with their medications46 and experience increased all-cause mortality.47 The association between health literacy and outcomes may be partially mediated by poor reading comprehension, which has an indirect effect on CHD risk.48 The absolute effect of health literacy and reading comprehension on CVD risk requires further characterization, but may be an area for intervention in individuals with low education attainment. It is also important to note that although studies looking at the impact of SES on outcomes adjust for variables such as traditional risk factors, there is potential for residual confounding that may be contributing to adverse health that is not accounted for in the models.
Employment Status
Employment is a commonly used marker of SES, and unemployment has been associated with increased risk of CVD.11, 14, 49 Analysis by Mejean et al. demonstrated a 20% increase in risk of CHD events in an unemployed, French population without preexisting heart disease (HR 1.20, CI 1.04-1.39) after adjustment for age, gender, diet, and lifestyle.49 A large proportion (46%) of the CHD risk is explained by dietary and lifestyle mediators, most notably alcohol consumption (17%) and smoking (13%).49
A recent study of individuals with high SES relative to the general population also demonstrated an increased risk of cardiovascular events in the unemployed despite extensive adjustment for covariates, including age, gender, biological characteristics, behavioral variables, and socioeconomic factors.14 The outcomes of the unemployed population in the study were worse than the retired cohort, which suggests that the detrimental effect of unemployment may be driven by the job loss itself.14 An alternative explanation is that those with poor health may be more likely to become unemployed. Nonetheless, it is important to note that unemployment is associated with increased CVD burden in the socially advantaged as well as those with low SES at baseline.
Dupre et al. performed a comprehensive study on the relationship between employment status and risk for AMI in the U.S.50 Unemployment was associated with a 35% increased risk for AMI (HR 1.35, CI 1.10-1.66) within the first year, after which time the risk disappeared.50 Cumulative number of job losses was associated with an incremental increase in AMI risk, and cumulative time spent unemployed was also significantly associated with increased risk for AMI.50 The risks remained significant after adjustment for socioeconomic, behavioral, and clinical variables.50 The mechanisms underlying poorer outcomes with unemployment are not clear. In this study, time of entry into the workforce, which could suggest educational differences or health difficulties, was not significantly associated with outcomes.50 A possible explanation is that of cumulative stress, since worse outcomes were seen with additional episodes of job loss and increased time spent unemployed. One limitation of the study was an older cohort (median age 62 years) that may not be representative of the overall workforce.50
Environmental Factors
Neighborhood socioeconomic characteristics, in addition to individual SES, have been associated with CVD risk factors, adverse events and mortality.15-17 A population analysis of the Atherosclerosis Risk in Community study showed that living in disadvantaged areas is linked to higher incidence of CHD after controlling for individual income, education and employment status.17 The findings were supported by a recent analysis of data from the Jackson Heart Study, which found an association between neighborhood disadvantage and cumulative biological risk, a score derived from biomarkers representing cardiovascular, metabolic, inflammatory, and neuroendocrine health.51 The environmental impact of health status and outcomes is driven by both physical and social attributes.16, 52 Physical features of neighborhoods include presence of sidewalks or recreational spaces, access to transportation, and availability and cost of healthy foods, while social attributes include safety, deprivation, social support, and lack of community cohesion.16 Socioeconomic differences in neighborhood characteristics can impact availability of resources and influence promotion or maintenance of a healthy lifestyle. Favorable neighborhoods are associated with reduced cardiovascular risk factors, as long-term exposure to environments with greater access to physical activity and healthy food was associated with lower incidence of diabetes and lower prevalence of overweight or obesity.53, 54 Other social characteristics, including neighborhood crime, also contribute to cardiovascular risk. In a multi-ethnic populations, high individual- and neighborhood-level safety were associated with decreasing body mass index over time.55 In contrast, poorly-rated physical environments based on walking environment, availability of healthy food, safety, aesthetics, and social coherence were associated with elevated depressive symptoms and greater increase in waist circumference in individuals living in those neighborhoods.56
Poor dietary options and the increased cost of healthy food may also contribute to the increased CVD risk of disadvantaged neighborhoods. Low income areas have fewer food outlets and supermarkets which results in limited access to fresh fruits and vegetables.57, 58 The cost of healthy food is also higher in poor areas with limited access, due in part to the lower prevalence of supermarkets which typically offer lower prices and a variety of brand options.59, 60 Low income areas lacking access to healthy, affordable foods are known as “food deserts” which are associated with diet-related chronic diseases and obesity.61 There are also racial disparities in food availability as neighborhoods with a high prevalence of African Americans tend to have more fast food restaurants59, fewer supermarkets60, and fewer healthy options.62
Neighborhood characteristics can change with time and provide additional insight into the relationship between environmental factors and cardiovascular health. Recent results from a longitudinal study with a 12-year follow-up period showed that increasing density of neighborhood healthy food resources was associated with lower coronary artery calcium over time. However, changes in other neighborhood characteristics, including walking and social environment, were not associated with changes in coronary artery calcium.63 Further longitudinal studies have demonstrated that neighborhoods with favorable physical activity increased individual activities and improved cardiovascular risk factors.64, 65 However, previous studies also showed that individuals often move into neighborhoods with similar SES across their life course, which impairs attempts to establish a causal relationship between environment and CVD.66, 67 Unfortunately, a recent update by the USDA showed relatively small changes in low-income and low-access neighborhoods between 2010 and 2015 data.68 Disadvantaged communities must be a priority in order to effectively reduce CVD disparities in individuals with low SES.
Psychosocial Factors and CVD Outcomes
Psychosocial factors, including stress and depression, are strongly associated with adverse CVD outcomes, and growing evidence suggests they may disparately affect individuals of low SES.69, 70 In analysis of the REGARDS study, a prospective observational cohort in the United States, individuals earning <$35,000 annually who reported both stress and depressive symptoms had a 48% higher risk of developing CVD and a 33% increased risk of all-cause mortality after adjustment for socioeconomic, clinical, and behavioral factors.69 The association was not present in subjects earning ≥$35,000 per year.69 Likewise, a study of psychological distress (depression, anxiety, and stress) demonstrated that the risk of CHD mortality was increased in those with low (HR 1.31, p=0.001), but not high, SES (p=0.107).70 The disparity in risk may related to inadequate social or material resources to cope with stressful events and higher rates of adverse health behaviors, including smoking and physical inactivity, that are associated with stress and depression.71, 72 The contribution of poor health behaviors in psychosocial distress is supported by a study from Ye et al. that found the increased risk of MI or death in depressed individuals was attenuated after adjustment for behavioral mechanisms, in particular smoking and physical inactivity.73 In addition to identification and treatment of the components of psychosocial stress, these findings suggest a role for aggressive targeting of smoking cessation and physical activity in these individuals.
SES and CVD Outcomes based on Sex
Women are overrepresented amongst those living in poverty; thus, are disproportionately affected by the disparities in the distribution of wealth, income and access to resources which ultimately can affect overall health and quality of life. In the Women’s Ischemic Syndrome Evaluation (WISE) study, women with ischemic heart disease in the lowest SES (household income <$20,000/year) were more likely to be uninsured or have public insurance, yet had much higher drug costs and higher 5-year re-hospitalization rates when compared with higher-income women.74 Income had far greater impact than any other SES measure, including race, education, marital status or employment status.74 In a universal healthcare system (Southern Alberta, Canada), neighborhood SES was associated with the use of cardiac catheterization and 30-day mortality after ACS in women, but this same association was not seen in men.75
Interventions to Improve Health Behaviors and Risk Factors
Programs aimed at improving health in the socially disadvantaged must first focus on aggressively targeting traditional risk factors that have strong associations with low SES.7 Behavioral counseling to reduce CVD risk factors including cholesterol levels, blood pressure, and diabetes incidence has been proven effective in the general population and is recommended by the U.S. Preventive Services Task Force.76, 77 Counseling of the family members of a patient with CVD, who are also at higher risk of vascular events, may improve dietary intake and physical activity, but further research into the applicability of these results to low-SES individuals is required. Studies have shown moderate success with smoking cessation programs aimed at patients of low SES.78 Brown et al. utilized an internet-based smoking cessation program to evaluate the success rate between socioeconomic groups and demonstrated a significant improvement in the low-SES cohort that was not realized in the high-SES population.78
However, other studies have suggested more limited efficacy in individuals with low SES.79, 80 Siren et al. found that behavioral counseling improved smoking cessation only in a high-education cohort and had no effect in a low-education group.79 In a study evaluating lifestyle interventions in low-income American Indians and Native Alaskans the low-income groups had less improvement in BMI, unhealthy food consumption, and physical activity when compared with the high-income group.80 The study did find an indirect relationship between the number of trained staff at each location and the success of risk faster modification.80 Health-counseling has been shown to improve diet in low-SES individuals, and interventions focused on the lack of convenient and affordable access to the components of a healthy diet may also be necessary to improve dietary habits in low-SES areas.79
Regular physical activity is associated with a decreased risk of CVD and its comorbidities.81, 82 Likewise, physical inactivity is an independent risk factor for poor CVD outcomes.83 However, despite the known impact of physical activity and inactivity on CVD modulation, fewer than half of U.S. adults met the recommended levels of physical activity in 2011.84 The burden of inadequate leisure-time physical activity is especially pronounced in individuals of low SES, which may be due to increased occupational responsibilities or reduced access to safe facilities for exercise.85, 86 Programs aimed at increasing physical activity have demonstrated promising results in individuals with low SES.79, 87 The “Walk Your Heart to Health” program successfully improved physical activity in a low- to middle-income group consisting primarily of ethnic minorities in Detroit, Michigan.87 The intervention group met three times weekly at community sites and walked for an increasing amount of time (45-90 minutes). Physical activity of the group was increased at 8 weeks, and improvements were noted in the cohort’s systolic blood pressure, fasting blood glucose, total cholesterol, waist circumference, and BMI at 8 weeks that were maintained at 32 weeks.87 Physical activity appears to be an important target in low-SES communities due to its widespread benefits and inherently inexpensive nature, however, physical insecurity (violence, crime) or lack of infrastructure (sidewalks, bicycle paths) in the neighborhood social environment may severely impact an individual’s ability to create a sustainable physical activity regimen.88 Thus, policy intervention to address such factors in low socioeconomic populations must be addressed in conjunction with efforts to change individual behavior.89
A substantial barrier to the primary prevention of CVD, especially in low-SES groups, is a lack of access to healthcare providers. Given the increasing demands on physicians, strategies have been developed to better appropriate available resources. One effective community based strategy using this paradigm is “task shifting,” an idea conceived by the World Health Organization as early as 1980 and defined as redistributing primary care responsibilities from physician to non-physician providers.90 Although a dearth of evidence exists for the use of task shifting in HIC, the Adeyemo trial in Nigeria, a LMIC, demonstrated a reduction in systolic blood pressure from a pre-intervention mean of 168/92 to a goal of less <140/90 in 66.7% of patients utilizing nurse-driven task shifting compared with 65.4% of patients receiving usual medical care.91 Task-shifting can be further extended to include health workers without formal healthcare training, known as community health workers (CHW). CHW play a valuable role in cost-effective screening for CVD in low-resource countries and communities.92, 93 Given the constraints of modern medical practice, task shifting may have utility for CVD screening and risk factor improvement in areas with reduced resources.
Numerous studies have evaluated the role of community interventions on major adverse cardiovascular events and risk factors. Mass media negatively portraying tobacco reduces smoking prevalence by approximately 2%.94 Tobacco cessation rates can be further impacted by increasing prices of tobacco products and state programs to provide nicotine replacement therapy.94 Task-shifting the role of smoking cessation management to a community pharmacist increased the “quit rate” from 2.7% to 14.3% in study participants.94 Similar effects are seen with mass media advocacy for salt restriction and dietary modification.94 Subsidization of healthy foods is another community-level intervention that has demonstrated benefit in low income individuals. Reducing the cost of healthy foods has been shown to improve diets and reduce the barriers to a healthy diet in food deserts.95 Similarly, taxation of unhealthy foods decreases their consumption.95 A combined strategy can be used to improve diets in at-risk communities. Environmental engineering, including construction of new supermarkets to increase access to healthy foods, still lacks adequate data to support its use.95
Heart disease exhibits regional clustering in the United States (see Figure 2).96 Geomapping, the identification of geographic “hot spots” of individuals at high risk for CVD, may be utilized in the future to target communities that would benefit from aggressive community-based interventions.97 Geomapping has demonstrated promising early results in Sweden for identification of at-risk populations for diabetes and could be adapted to provide increased screening and treatment services for low-SES communities with a high prevalence of CVD risk.98
Figure 2.
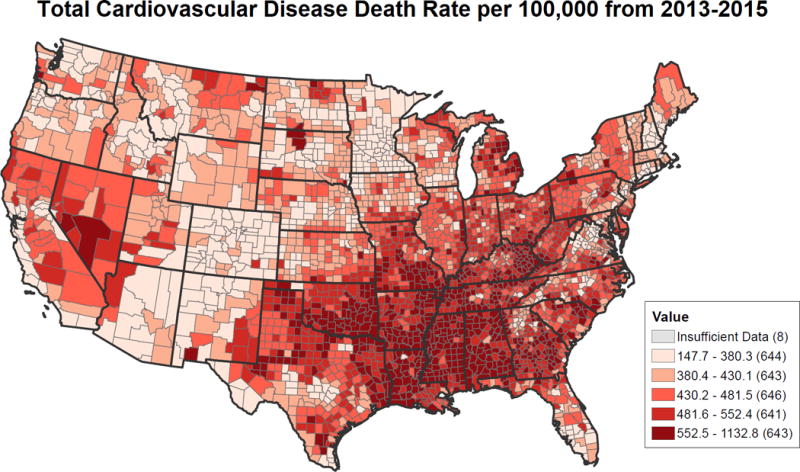
Cardiovascular disease death rates in individuals aged ≥35, by county between 2013-2015. Rates are spatially smoothed to enhance the stability of rates in counties with small populations. Data sources are the National Vital Statistics System and National Center for Health Statistics. This map was created using the Interactive Atlas of Heart Disease and Stroke, a website developed by the Centers for Disease Control and Prevention, Division for Heart Disease and Stroke Prevention.96
Strategies for identifying and improving health disparities in the United States were addressed in a Think Tank meeting organized by The National Heart, Lung, and Blood Institute.99 The panel recommendations focus on the conversion of evidence to implementation through an increased breadth of research themes and transdisciplinary training programs to expand research capacities.99 The panel further emphasized the role of platforms to optimize research and the development of collaborator and stakeholder networks to create benchmark studies.99 See the Figure 3 for a summary of potential interventions in individuals with low SES.
Figure 3.
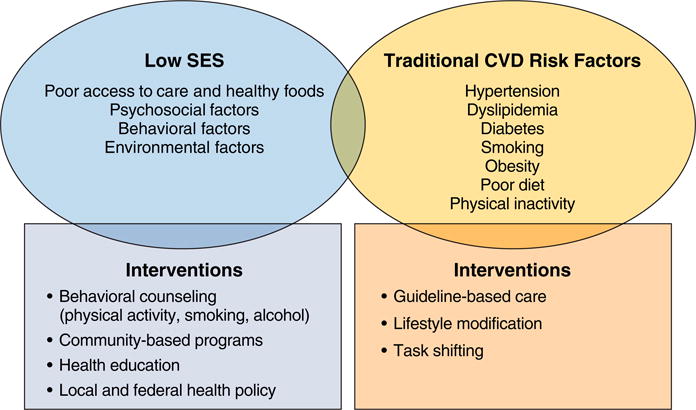
Association between low socioeconomic status, cardiovascular risk factors, cardiovascular disease, and interventions. CVD, cardiovascular disease; SES, socioeconomic status.
Targeting lower socioeconomic populations certainly must involve multi-level behavioral interventions at the individual and community level that incorporate a comprehensive understanding of social determinants of health and a concerted effort to engage the community.89 Specific efforts to reform the socioecological environment for primordial and primary prevention, as outlined by the AHA Guide for Improving Cardiovascular Health at the Community level, include an emphasis to direct resources to support legislation encouraging smoking cessation, promote sodium restriction in processed foods, and support modifications in the environment to encourage physical activity.89 Through utilization of existing, cohesive networks such as healthcare facilities, schools, religious organizations, worksites, social networks, media networks, and virtual communities, physicians, policy makers, and activists can develop a more effective platform to engage and intervene in communities at a grass-roots level.89 Unfortunately, data addressing improvement in CVD in lower SES populations through targeted intervention are limited, and further studies should be performed to investigate the potential impact of such interventions.88 Additionally, while community interventions play an essential role in changing individual behavior, macro-level factors may significantly impede the capacity to change individual behavior and should also be addressed.
Future Trends and Directions
A study in England determined that CHD mortality was decreasing in individuals of all SES, but the rate of decline was steepest in the most affluent group compared to those with lower SES.100 Lotufo et al. noted similar findings in a comparison of high- and low-income groups in Brazil, a high-middle income country.101 Several countries have also seen flattening of the reductions in CHD mortality in younger individuals of low SES.102, 103 In the United States and Scotland, the trend may be linked to increasing inequalities in smoking in low socioeconomic groups.102, 103 The United States has also experienced an increase in diabetes among the socially deprived.102, 104 These trends are concerning and suggest that while overall cardiovascular care is improving, the advances are preferentially helping the socially advantaged and widening the gap of health inequality.
Properly risk-stratifying patients will be a critical aspect of identifying low-SES patients with an increased risk of CVD that would not be conveyed by traditional risk factors alone. The ASSIGN score and QRISK algorithm in the United Kingdom are alternative risk stratification tools that integrate postal code income with traditional CVD risk factors.105, 106 The ASSIGN score provided a statistically significant, but marginal, improvement in risk prediction when compared to the Framingham Risk Score (FRS).105 The QRISK algorithm also improved prediction of CVD events in individuals whose risk was under-predicted by the FRS.106 While QRISK and ASSIGN are meant to serve as alternative approaches to the FRS, Franks et al. incorporated SES markers directly into the existing FRS framework.107 The integration of educational attainment and income as additional markers to predict risk into the FRS removed the SES bias seen in low-SES individuals.107 Accurate prediction is important to identify appropriate candidates for aggressive primary prevention, which includes statin therapy in individuals at borderline risk for CVD or additional resources dedicated to counseling in patients with multiple markers for low SES. Models incorporating SES for risk prediction are challenging due to the regional and cultural differences in SES markers. It remains to be seen if a single risk stratification system will be adequate or if regional variants will be required, particularly with the use of the American College of Cardiology and American Heart Association atherosclerotic CVD risk assessment tool in the U.S. population.
Several organizations have created initiatives to reduce health disparities in the United States and worldwide. In 2011, the World Health Organization (WHO) set a goal to reduce premature deaths from non-communicable diseases, including CVD, by 25% by 2025 (25by25).108 The WHO action plan targets modifiable CVD risk factors: tobacco use, alcohol intake, sodium intake, physical inactivity, diabetes mellitus/obesity, and hypertension.109 The World Heart Federation expanded that goal to include a 25% reduction in CVD mortality by the year 2025 through nine strategies, including reduction in tobacco use, detection and treatment of hypertension, improved access to proven CVD medications, implementation of community-based interventions, creation of large studies to characterize lifestyle habits of regional populations, and the development of partnerships between high- and low-resource countries to facilitate transfer of knowledge and funding.110, 111
Reducing disparities in health will require a multi-level, collaborative approach. The overarching principles include a focus on identifying individuals and communities at greatest risk and putting more resources towards these groups, improving access to quality health care, increasing cultural competence, and revamping medical education. Government (federal and local), businesses/employers, health care systems, schools, community organizations and individuals/families all have an integral role in elimination of health disparities (Figure 4). Furthermore, since the foundation of SES and health in adulthood are influenced by conditions in childhood, targeted preschool and early childhood interventions have important implications for reducing disparities.112
Figure 4.
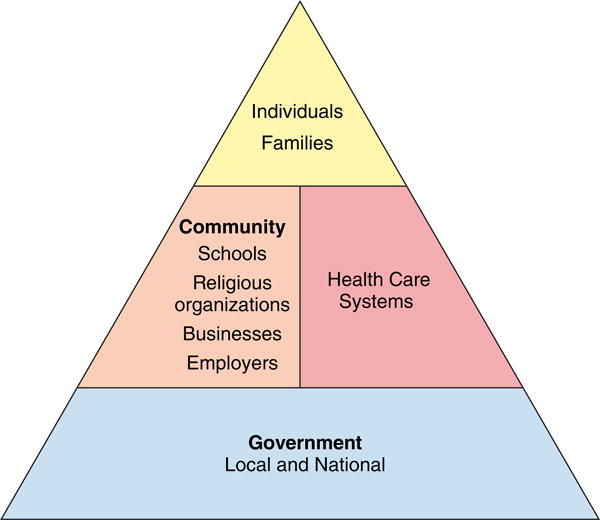
Interventions at the community, government, healthcare systems and individual level should be targeted equally in efforts to reduce disparities in heath.
The focus of future studies should be on implementation research evaluating strategies to reduce health disparities. These studies should be designed to identify effective policy changes and program interventions to reduce disparities. Furthermore, the costs and benefits of individual and community-level interventions to identify the most cost-effective strategies and interventions should be studied.113
Conclusion
SES has a measurable and significant impact on cardiovascular health. Individuals of low SES carry a substantial burden of CVD and are more likely to experience increased event rates and poorer outcomes. Current models do not adequately account for the risk conveyed by low SES. We now have compelling evidence showing that the independent association between SES and mortality is comparable in strength and consistency to that of the traditional major risk factors.3 As Tobias concluded, the strength of that evidence “is now impossible to ignore”.114 The time has come for increased focus on effective and sustainable interventions informed by clinical and population science insights from SES research. Additionally, further research is required to better understand the underlying mechanisms of CVD risk that disproportionately affect individuals of low SES. Once the causes of the discrepancies in health equity are better understood, targeted interventions can be pursued to better address disparities in populations at risk.
Acknowledgments
Sources of Funding
PS is supported by the Abraham J. & Phyllis Katz Foundation (Atlanta, GA).
AAQ is supported by 1R61HL138657-01, 5P01HL101398-02, 1P20HL113451-01, 1P30DK111024-01, AHA 0000031288, 1RF1AG051633-01, R01 NS064162-01, R01 HL89650-01, HL095479-01, 1U10HL110302-01, 1DP3DK094346-01, 2P01HL086773-06A1.
Footnotes
Disclosures
The authors have no financial conflicts of interest to disclose.
References
- 1.Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Statistics C and Stroke Statistics S Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation. 2017;135:e146–e603. doi: 10.1161/CIR.0000000000000485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Franks P, Winters PC, Tancredi DJ, Fiscella KA. Do changes in traditional coronary heart disease risk factors over time explain the association between socio-economic status and coronary heart disease? BMC Cardiovasc Disord. 2011;11:28. doi: 10.1186/1471-2261-11-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Stringhini S, Carmeli C, Jokela M, Avendaño M, Muennig P, Guida F, Ricceri F, d’Errico A, Barros H, Bochud M, Chadeau-Hyam M, Clavel-Chapelon F, Costa G, Delpierre C, Fraga S, Goldberg M, Giles GG, Krogh V, Kelly-Irving M, Layte R, Lasserre AM, Marmot MG, Preisig M, Shipley MJ, Vollenweider P, Zins M, Kawachi I, Steptoe A, Mackenbach JP, Vineis P, Kivimäki M, Alenius H, Avendano M, Barros H, Bochud M, Carmeli C, Carra L, Castagné R, Chadeau-Hyam M, Clavel-Chapelon F, Costa G, Courtin E, Delpierre C, D’Errico A, Dugué P-A, Elliott P, Fraga S, Gares V, Giles G, Goldberg M, Greco D, Hodge A, Irving MK, Karisola P, Kivimäki M, Krogh V, Lang T, Layte R, Lepage B, Mackenbach J, Marmot M, McCrory C, Milne R, Muennig P, Nusselder W, Panico S, Petrovic D, Polidoro S, Preisig M, Raitakari O, Ribeiro AI, Ribeiro AI, Ricceri F, Robinson O, Valverde JR, Sacerdote C, Satolli R, Severi G, Shipley MJ, Stringhini S, Tumino R, Vineis P, Vollenweider P, Zins M. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet. 2017;389:1229–1237. doi: 10.1016/S0140-6736(16)32380-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lynch JW, Kaplan GA, Cohen RD, Tuomilehto J, Salonen JT. Do Cardiovascular Risk Factors Explain the Relation between Socioeconomic Status, Risk of All-Cause Mortality, Cardiovascular Mortality, and Acute Myocardial Infarction? Am J Epidemiol. 1996;144:934–942. doi: 10.1093/oxfordjournals.aje.a008863. [DOI] [PubMed] [Google Scholar]
- 5.Winkleby MA, Jatulis DE, Frank E, Fortmann SP. Socioeconomic status and health: how education, income, and occupation contribute to risk factors for cardiovascular disease. Am J Public Health. 1992;82:816–820. doi: 10.2105/ajph.82.6.816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Adler NE, Glymour MM, Fielding J. Addressing Social Determinants of Health and Health Inequalities. JAMA. 2016;316:1641–1642. doi: 10.1001/jama.2016.14058. [DOI] [PubMed] [Google Scholar]
- 7.Davis AM, Vinci LM, Okwuosa TM, Chase AR, Huang ES. Cardiovascular health disparities: a systematic review of health care interventions. Med Care Res Rev. 2007;64:29S–100S. doi: 10.1177/1077558707305416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mackenbach JP, Cavelaars AE, Kunst AE, Groenhof F. Socioeconomic inequalities in cardiovascular disease mortality; an international study. Eur Heart J. 2000;21:1141–1151. doi: 10.1053/euhj.1999.1990. [DOI] [PubMed] [Google Scholar]
- 9.Gebreab SY, Diez Roux AV, Brenner AB, Hickson DA, Sims M, Subramanyam M, Griswold ME, Wyatt SB, James SA. The impact of lifecourse socioeconomic position on cardiovascular disease events in African Americans: the Jackson Heart Study. J Am Heart Assoc. 2015;4:e001553. doi: 10.1161/JAHA.114.001553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jankovic J, Eric M, Stojisavljevic D, Marinkovic J, Jankovic S. Socio-Economic Differences in Cardiovascular Health: Findings from a Cross-Sectional Study in a Middle-Income Country. PLoS One. 2015;10:e0141731. doi: 10.1371/journal.pone.0141731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mosquera PA, San Sebastian M, Waenerlund AK, Ivarsson A, Weinehall L, Gustafsson PE. Income-related inequalities in cardiovascular disease from mid-life to old age in a Northern Swedish cohort: A decomposition analysis. Soc Sci Med. 2016;149:135–144. doi: 10.1016/j.socscimed.2015.12.017. [DOI] [PubMed] [Google Scholar]
- 12.Kucharska-Newton AM, Harald K, Rosamond WD, Rose KM, Rea TD, Salomaa V. Socioeconomic indicators and the risk of acute coronary heart disease events: comparison of population-based data from the United States and Finland. Ann Epidemiol. 2011;21:572–579. doi: 10.1016/j.annepidem.2011.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Liu K, Cedres LB, Stamler J, Dyer A, Stamler R, Nanas S, Berkson DM, Paul O, Lepper M, Lindberg HA, Marquardt J, Stevens E, Schoenberger JA, Shekelle RB, Collette P, Shekelle S, Garside D. Relationship of education to major risk factors and death from coronary heart disease, cardiovascular diseases and all causes, Findings of three Chicago epidemiologic studies. Circulation. 1982;66:1308–1314. doi: 10.1161/01.cir.65.1.146. [DOI] [PubMed] [Google Scholar]
- 14.Meneton P, Kesse-Guyot E, Mejean C, Fezeu L, Galan P, Hercberg S, Menard J. Unemployment is associated with high cardiovascular event rate and increased all-cause mortality in middle-aged socially privileged individuals. Int Arch Occup Environ Health. 2015;88:707–716. doi: 10.1007/s00420-014-0997-7. [DOI] [PubMed] [Google Scholar]
- 15.Clark CR, Ommerborn MJ, Hickson DA, Grooms KN, Sims M, Taylor HA, Albert MA. Neighborhood disadvantage, neighborhood safety and cardiometabolic risk factors in African Americans: biosocial associations in the Jackson Heart study. PLoS One. 2013;8:e63254. doi: 10.1371/journal.pone.0063254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Diez Roux AV. Residential environments and cardiovascular risk. Jurban health. 2003;80:569–589. doi: 10.1093/jurban/jtg065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Diez Roux AV, Merkin SS, Arnett D, Chambless L, Massing M, Nieto FJ, Sorlie P, Szklo M, Tyroler HA, Watson RL. Neighborhood of residence and incidence of coronary heart disease. New Eng j med. 2001;345:99–106. doi: 10.1056/NEJM200107123450205. [DOI] [PubMed] [Google Scholar]
- 18.Lewis MW, Khodneva Y, Redmond N, Durant RW, Judd SE, Wilkinson LL, Howard VJ, Safford MM. The impact of the combination of income and education on the incidence of coronary heart disease in the prospective Reasons for Geographic and Racial Differences in Stroke (REGARDS) cohort study. BMC Public Health. 2015;15:1312. doi: 10.1186/s12889-015-2630-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basanez MG, Baxter A, Bell ML, Benjamin EJ, Bennett D, Bernabe E, Bhalla K, Bhandari B, Bikbov B, Bin Abdulhak A, Birbeck G, Black JA, Blencowe H, Blore JD, Blyth F, Bolliger I, Bonaventure A, Boufous S, Bourne R, Boussinesq M, Braithwaite T, Brayne C, Bridgett L, Brooker S, Brooks P, Brugha TS, Bryan-Hancock C, Bucello C, Buchbinder R, Buckle G, Budke CM, Burch M, Burney P, Burstein R, Calabria B, Campbell B, Canter CE, Carabin H, Carapetis J, Carmona L, Cella C, Charlson F, Chen H, Cheng AT, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahiya M, Dahodwala N, Damsere-Derry J, Danaei G, Davis A, De Leo D, Degenhardt L, Dellavalle R, Delossantos A, Denenberg J, Derrett S, Des Jarlais DC, Dharmaratne SD, Dherani M, Diaz-Torne C, Dolk H, Dorsey ER, Driscoll T, Duber H, Ebel B, Edmond K, Elbaz A, Ali SE, Erskine H, Erwin PJ, Espindola P, Ewoigbokhan SE, Farzadfar F, Feigin V, Felson DT, Ferrari A, Ferri CP, Fevre EM, Finucane MM, Flaxman S, Flood L, Foreman K, Forouzanfar MH, Fowkes FG, Fransen M, Freeman MK, Gabbe BJ, Gabriel SE, Gakidou E, Ganatra HA, Garcia B, Gaspari F, Gillum RF, Gmel G, Gonzalez-Medina D, Gosselin R, Grainger R, Grant B, Groeger J, Guillemin F, Gunnell D, Gupta R, Haagsma J, Hagan H, Halasa YA, Hall W, Haring D, Haro JM, Harrison JE, Havmoeller R, Hay RJ, Higashi H, Hill C, Hoen B, Hoffman H, Hotez PJ, Hoy D, Huang JJ, Ibeanusi SE, Jacobsen KH, James SL, Jarvis D, Jasrasaria R, Jayaraman S, Johns N, Jonas JB, Karthikeyan G, Kassebaum N, Kawakami N, Keren A, Khoo JP, King CH, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Laden F, Lalloo R, Laslett LL, Lathlean T, Leasher JL, Lee YY, Leigh J, Levinson D, Lim SS, Limb E, Lin JK, Lipnick M, Lipshultz SE, Liu W, Loane M, Ohno SL, Lyons R, Mabweijano J, MacIntyre MF, Malekzadeh R, Mallinger L, Manivannan S, Marcenes W, March L, Margolis DJ, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGill N, McGrath J, Medina-Mora ME, Meltzer M, Mensah GA, Merriman TR, Meyer AC, Miglioli V, Miller M, Miller TR, Mitchell PB, Mock C, Mocumbi AO, Moffitt TE, Mokdad AA, Monasta L, Montico M, Moradi-Lakeh M, Moran A, Morawska L, Mori R, Murdoch ME, Mwaniki MK, Naidoo K, Nair MN, Naldi L, Narayan KM, Nelson PK, Nelson RG, Nevitt MC, Newton CR, Nolte S, Norman P, Norman R, O’Donnell M, O’Hanlon S, Olives C, Omer SB, Ortblad K, Osborne R, Ozgediz D, Page A, Pahari B, Pandian JD, Rivero AP, Patten SB, Pearce N, Padilla RP, Perez-Ruiz F, Perico N, Pesudovs K, Phillips D, Phillips MR, Pierce K, Pion S, Polanczyk GV, Polinder S, Pope CA, 3rd, Popova S, Porrini E, Pourmalek F, Prince M, Pullan RL, Ramaiah KD, Ranganathan D, Razavi H, Regan M, Rehm JT, Rein DB, Remuzzi G, Richardson K, Rivara FP, Roberts T, Robinson C, De Leon FR, Ronfani L, Room R, Rosenfeld LC, Rushton L, Sacco RL, Saha S, Sampson U, Sanchez-Riera L, Sanman E, Schwebel DC, Scott JG, Segui-Gomez M, Shahraz S, Shepard DS, Shin H, Shivakoti R, Singh D, Singh GM, Singh JA, Singleton J, Sleet DA, Sliwa K, Smith E, Smith JL, Stapelberg NJ, Steer A, Steiner T, Stolk WA, Stovner LJ, Sudfeld C, Syed S, Tamburlini G, Tavakkoli M, Taylor HR, Taylor JA, Taylor WJ, Thomas B, Thomson WM, Thurston GD, Tleyjeh IM, Tonelli M, Towbin JA, Truelsen T, Tsilimbaris MK, Ubeda C, Undurraga EA, van der Werf MJ, van Os J, Vavilala MS, Venketasubramanian N, Wang M, Wang W, Watt K, Weatherall DJ, Weinstock MA, Weintraub R, Weisskopf MG, Weissman MM, White RA, Whiteford H, Wiebe N, Wiersma ST, Wilkinson JD, Williams HC, Williams SR, Witt E, Wolfe F, Woolf AD, Wulf S, Yeh PH, Zaidi AK, Zheng ZJ, Zonies D, Lopez AD, AlMazroa MA, Memish ZA. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet (London, England) 2012;380:2197–2223. doi: 10.1016/S0140-6736(12)61689-4. [DOI] [PubMed] [Google Scholar]
- 20.Goyal A, Bhatt DL, Steg PG, Gersh BJ, Alberts MJ, Ohman EM, Corbalan R, Eagle KA, Gaxiola E, Gao R, Goto S, D’Agostino RB, Califf RM, Smith SC, Jr, Wilson PW, Reduction of Atherothrombosis for Continued Health Registry I Attained educational level and incident atherothrombotic events in low- and middle-income compared with high-income countries. Circulation. 2010;122:1167–1175. doi: 10.1161/CIRCULATIONAHA.109.919274. [DOI] [PubMed] [Google Scholar]
- 21.Dinsa GD, Goryakin Y, Fumagalli E, Suhrcke M. Obesity and socioeconomic status in developing countries: a systematic review. Obesity Reviews. 2012;13:1067–1079. doi: 10.1111/j.1467-789X.2012.01017.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gerber Y, Weston SA, Killian JM, Therneau TM, Jacobsen SJ, Roger VL. Neighborhood income and individual education: effect on survival after myocardial infarction. Mayo Clin proc. 2008;83:663–669. doi: 10.4065/83.6.663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stirbu I, Looman C, Nijhof GJ, Reulings PG, Mackenbach JP. Income inequalities in case death of ischaemic heart disease in the Netherlands: a national record-linked study. J Epidemiol Community Health. 2012;66:1159–1166. doi: 10.1136/jech-2011-200924. [DOI] [PubMed] [Google Scholar]
- 24.Yong CM, Abnousi F, Asch SM, Heidenreich PA. Socioeconomic inequalities in quality of care and outcomes among patients with acute coronary syndrome in the modern era of drug eluting stents. J Am Heart Assoc. 2014;3:e001029. doi: 10.1161/JAHA.114.001029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wang JY, Wang CY, Juang SY, Huang KY, Chou P, Chen CW, Lee CC. Low socioeconomic status increases short-term mortality of acute myocardial infarction despite universal health coverage. Int J Cardiol. 2014;172:82–87. doi: 10.1016/j.ijcard.2013.12.082. [DOI] [PubMed] [Google Scholar]
- 26.Dunlay SM, Pack QR, Thomas RJ, Killian JM, Roger VL. Participation in cardiac rehabilitation, readmissions, and death after acute myocardial infarction. Am J Med. 2014;127:538–46. doi: 10.1016/j.amjmed.2014.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Doll JA, Hellkamp A, Thomas L, Ho PM, Kontos MC, Whooley MA, Boyden TF, Peterson ED, Wang TY. Effectiveness of cardiac rehabilitation among older patients after acute myocardial infarction. Am Heart J. 2015;170:855–864. doi: 10.1016/j.ahj.2015.08.001. [DOI] [PubMed] [Google Scholar]
- 28.Lemstra ME, Alsabbagh W, Rajakumar RJ, Rogers MR, Blackburn D. Neighbourhood income and cardiac rehabilitation access as determinants of nonattendance and noncompletion. Can J Cardiol. 2013;29:1599–1603. doi: 10.1016/j.cjca.2013.08.011. [DOI] [PubMed] [Google Scholar]
- 29.Rasmussen JN, Gislason GH, Rasmussen S, Abildstrom SZ, Schramm TK, Kober L, Diderichsen F, Osler M, Torp-Pedersen C, Madsen M. Use of statins and beta-blockers after acute myocardial infarction according to income and education. J Epidemiol Community Health. 2007;61:1091–1097. doi: 10.1136/jech.2006.055525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hanley GE, Morgan S, Reid RJ. Income-related inequity in initiation of evidence-based therapies among patients with acute myocardial infarction. J Gen Intern Med. 2011;26:1329–35. doi: 10.1007/s11606-011-1799-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yu TH, Hou YC, Chung KP. Do low-income coronary artery bypass surgery patients have equal opportunity to access excellent quality of care and enjoy good outcome in Taiwan? Int J Equity Health. 2014;13:64. doi: 10.1186/s12939-014-0064-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Parikh PB, Yang J, Leigh S, Dorjee K, Parikh R, Sakellarios N, Meng H, Brown DL. The impact of financial barriers on access to care, quality of care and vascular morbidity among patients with diabetes and coronary heart disease. J Gen Intern Med. 2014;29:76–81. doi: 10.1007/s11606-013-2635-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675–681. doi: 10.1001/jama.2011.123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gusmano MK, Weisz D, Rodwin VG, Lang J, Qian M, Bocquier A, Moysan V, Verger P. Disparities in access to health care in three French regions. Health Policy. 2014;114:31–40. doi: 10.1016/j.healthpol.2013.07.011. [DOI] [PubMed] [Google Scholar]
- 35.Woodward M, Peters SA, Batty GD, Ueshima H, Woo J, Giles GG, Barzi F, Ho SC, Huxley RR, Arima H, Fang X, Dobson A, Lam TH, Vathesatogkit P, Asia Pacific Cohort Studies C Socioeconomic status in relation to cardiovascular disease and cause-specific mortality: a comparison of Asian and Australasian populations in a pooled analysis. BMJ Open. 2015;5:e006408. doi: 10.1136/bmjopen-2014-006408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hu B, Li W, Wang X, Liu L, Teo K, Yusuf S, Investigators I-H Marital status, education, and risk of acute myocardial infarction in Mainland China: the INTER-HEART study. J epidemiol. 2012;22:123–129. doi: 10.2188/jea.JE20100175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kelly MJ, Weitzen S. The association of lifetime education with the prevalence of myocardial infarction: an analysis of the 2006 Behavioral Risk Factor Surveillance System. J commun health. 2010;35:76–80. doi: 10.1007/s10900-009-9189-x. [DOI] [PubMed] [Google Scholar]
- 38.Rosengren A, Subramanian SV, Islam S, Chow CK, Avezum A, Kazmi K, Sliwa K, Zubaid M, Rangarajan S, Yusuf S, Investigators I Education and risk for acute myocardial infarction in 52 high, middle and low-income countries: INTERHEART case-control study. Heart. 2009;95:2014–2022. doi: 10.1136/hrt.2009.182436. [DOI] [PubMed] [Google Scholar]
- 39.Mehta RH, O’Shea JC, Stebbins AL, Granger CB, Armstrong PW, White HD, Topol EJ, Califf RM, Ohman EM. Association of mortality with years of education in patients with ST-segment elevation myocardial infarction treated with fibrinolysis. J Am Coll Cardiol. 2011;57:138–146. doi: 10.1016/j.jacc.2010.09.021. [DOI] [PubMed] [Google Scholar]
- 40.Gerber Y, Goldbourt U, Drory Y, Israel Study Group on First Acute Myocardial I Interaction between income and education in predicting long-term survival after acute myocardial infarction. European journal of cardiovascular prevention and rehabilitation: official journal of the European Society of Cardiology, Working Groups on Epidemiology & Prevention and Cardiac Rehabilitation and Exercise Physiology. 2008;15:526–532. doi: 10.1097/HJR.0b013e328304feac. [DOI] [PubMed] [Google Scholar]
- 41.Kim JH, Jeong MH, Park IH, Choi JS, Rhee JA, Lee DH, Park SH, Kim IS, Jeong HC, Cho JY, Jang SY, Lee KH, Park KH, Sim DS, Kim KH, Hong YJ, Park HW, Kim JH, Ahn Y, Cho JG, Park JC. The association of socioeconomic status with three-year clinical outcomes in patients with acute myocardial infarction who underwent percutaneous coronary intervention. J Korean med sci. 2014;29:536–543. doi: 10.3346/jkms.2014.29.4.536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Alter DA, Iron K, Austin PC, Naylor CD, Group SS Socioeconomic status, service patterns, and perceptions of care among survivors of acute myocardial infarction in Canada. JAMA. 2004;291:1100–1107. doi: 10.1001/jama.291.9.1100. [DOI] [PubMed] [Google Scholar]
- 43.Kershaw KN, Droomers M, Robinson WR, Carnethon MR, Daviglus ML, Monique Verschuren WM. Quantifying the contributions of behavioral and biological risk factors to socioeconomic disparities in coronary heart disease incidence: the MORGEN study. Eur J Epidemiol. 2013;28:807–14. doi: 10.1007/s10654-013-9847-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Luepker RV, Rosamond WD, Murphy R, Sprafka JM, Folsom AR, McGovern PG, Blackburn H. Socioeconomic status and coronary heart disease risk factor trends. The Minnesota Heart Survey. Circulation. 1993;88:2172–2179. doi: 10.1161/01.cir.88.5.2172. [DOI] [PubMed] [Google Scholar]
- 45.Cajita MI, Cajita TR, Han HR. Health Literacy and Heart Failure: A Systematic Review. J Cardiovasc Nurs. 2016;31:121–130. doi: 10.1097/JCN.0000000000000229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Zhang NJ, Terry A, McHorney CA. Impact of health literacy on medication adherence: a systematic review and meta-analysis. Ann Pharmacother. 2014;48:741–751. doi: 10.1177/1060028014526562. [DOI] [PubMed] [Google Scholar]
- 47.Bostock S, Steptoe A. Association between low functional health literacy and mortality in older adults: longitudinal cohort study. BMJ. 2012;344:e1602. doi: 10.1136/bmj.e1602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Loucks EB, Gilman SE, Howe CJ, Kawachi I, Kubzansky LD, Rudd RE, Martin LT, Nandi A, Wilhelm A, Buka SL. Education and coronary heart disease risk: potential mechanisms such as literacy, perceived constraints, and depressive symptoms. Health Educ Behav. 2015;42:370–379. doi: 10.1177/1090198114560020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mejean C, Droomers M, van der Schouw YT, Sluijs I, Czernichow S, Grobbee DE, Bueno-de-Mesquita HB, Beulens JW. The contribution of diet and lifestyle to socioeconomic inequalities in cardiovascular morbidity and mortality. Int J Cardiol. 2013;168:5190–5195. doi: 10.1016/j.ijcard.2013.07.188. [DOI] [PubMed] [Google Scholar]
- 50.Dupre ME, George LK, Liu G, Peterson ED. The cumulative effect of unemployment on risks for acute myocardial infarction. Arch Intern Med. 2012;172:1731–1737. doi: 10.1001/2013.jamainternmed.447. [DOI] [PubMed] [Google Scholar]
- 51.Barber S, Hickson DA, Kawachi I, Subramanian SV, Earls F. Neighborhood Disadvantage and Cumulative Biological Risk Among a Socioeconomically Diverse Sample of African American Adults: An Examination in the Jackson Heart Study. J racial ethn health disparities. 2016;3:444–456. doi: 10.1007/s40615-015-0157-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Diez-Roux AV, Nieto FJ, Muntaner C, Tyroler HA, Comstock GW, Shahar E, Cooper LS, Watson RL, Szklo M. Neighborhood environments and coronary heart disease: a multilevel analysis. Am J Epidemiol. 1997;146:48–63. doi: 10.1093/oxfordjournals.aje.a009191. [DOI] [PubMed] [Google Scholar]
- 53.Christine PJ, Auchincloss AH, Bertoni AG, Carnethon MR, Sánchez BN, Moore K, Adar SD, Horwich TB, Watson KE, Roux AVD. Longitudinal associations between neighborhood physical and social environments and incident type 2 diabetes mellitus: the Multi-Ethnic Study of Atherosclerosis (MESA) JAMA intern med. 2015;175:1311–1320. doi: 10.1001/jamainternmed.2015.2691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Creatore MI, Glazier RH, Moineddin R, Fazli GS, Johns A, Gozdyra P, Matheson FI, Kaufman-Shriqui V, Rosella LC, Manuel DG, Booth GL. Association of Neighborhood Walkability With Change in Overweight, Obesity, and Diabetes. JAMA. 2016;315:2211–2220. doi: 10.1001/jama.2016.5898. [DOI] [PubMed] [Google Scholar]
- 55.Powell-Wiley TM, Moore K, Allen N, Block R, Evenson KR, Mujahid M, Diez Roux AV. Associations of Neighborhood Crime and Safety and With Changes in Body Mass Index and Waist Circumference: The Multi-Ethnic Study of Atherosclerosis. Am J Epidemiol. 2017;186:280–288. doi: 10.1093/aje/kwx082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Remigio-Baker RA, Roux AVD, Szklo M, Crum RM, Leoutsakos J-M, Franco M, Schreiner PJ, Carnethon MR, Nettleton JA, Mujahid MS. Physical environment may modify the association between depressive symptoms and change in waist circumference: the Multi-Ethnic Study of Atherosclerosis. Psychosomatics. 2014;55:144–154. doi: 10.1016/j.psym.2013.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Alwitt LF, Donley TD. Retail stores in poor urban neighborhoods. J Consum Aff. 1997:139–164. [Google Scholar]
- 58.Giang T, Karpyn A, Laurison HB, Hillier A, Perry RD. Closing the grocery gap in underserved communities: the creation of the Pennsylvania Fresh Food Financing Initiative. J Public Health Manag Pract. 2008;14:272–279. doi: 10.1097/01.PHH.0000316486.57512.bf. [DOI] [PubMed] [Google Scholar]
- 59.Block JP, Scribner RA, DeSalvo KB. Fast food, race/ethnicity, and income: a geographic analysis. Am J Prev Med. 2004;27:211–217. doi: 10.1016/j.amepre.2004.06.007. [DOI] [PubMed] [Google Scholar]
- 60.Block D, Kouba J. A comparison of the availability and affordability of a market basket in two communities in the Chicago area. Public Health Nutr. 2006;9:837–845. doi: 10.1017/phn2005924. [DOI] [PubMed] [Google Scholar]
- 61.Dubowitz T, Zenk SN, Ghosh-Dastidar B, Cohen DA, Beckman R, Hunter G, Steiner ED, Collins RL. Healthy food access for urban food desert residents: examination of the food environment, food purchasing practices, diet and BMI. Public Health Nutr. 2015;18:2220–2230. doi: 10.1017/S1368980014002742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Lewis LB, Sloane DC, Nascimento LM, Diamant AL, Guinyard JJ, Yancey AK, Flynn G, for the Reach Coalition of the African Americans Building A Legacy Of Health Project African Americans’ Access to Healthy Food Options in South Los Angeles Restaurants. Am J Pub Health. 2005;95:668–673. doi: 10.2105/AJPH.2004.050260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Wing JJ, August E, Adar SD, Dannenberg AL, Hajat A, Sanchez BN, Stein JH, Tattersall MC, Diez Roux AV. Change in Neighborhood Characteristics and Change in Coronary Artery Calcium: A Longitudinal Investigation in the MESA (Multi-Ethnic Study of Atherosclerosis) Cohort. Circulation. 2016;134:504–513. doi: 10.1161/CIRCULATIONAHA.115.020534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Muller-Riemenschneider F, Pereira G, Villanueva K, Christian H, Knuiman M, Giles-Corti B, Bull FC. Neighborhood walkability and cardiometabolic risk factors in Australian adults: an observational study. BMC Public Health. 2013;13:755. doi: 10.1186/1471-2458-13-755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Van Dyck D, Cerin E, Cardon G, Deforche B, Sallis JF, Owen N, De Bourdeaudhuij I. Physical activity as a mediator of the associations between neighborhood walkability and adiposity in Belgian adults. Health & place. 2010;16:952–960. doi: 10.1016/j.healthplace.2010.05.011. [DOI] [PubMed] [Google Scholar]
- 66.Sampson RJ, Sharkey P. Neighborhood selection and the social reproduction of concentrated racial inequality. Demography. 2008;45:1–29. doi: 10.1353/dem.2008.0012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Glass TA, Bilal U. Are neighborhoods causal? Complications arising from the ‘stickiness’ of ZNA. Social Science & Medicine. 2016;166:244–253. doi: 10.1016/j.socscimed.2016.01.001. [DOI] [PubMed] [Google Scholar]
- 68.Rhone A, Ploeg MV, Dicken C, Williams R, Breneman V. Low-Income and Low-Supermarket-Access Census Tracts, 2010-2015. U.S. Department of Agriculture, Economic Research Service; Jan, 2017. (EIB-165). [Google Scholar]
- 69.Sumner JA, Khodneva Y, Muntner P, Redmond N, Lewis MW, Davidson KW, Edmondson D, Richman J, Safford MM. Effects of Concurrent Depressive Symptoms and Perceived Stress on Cardiovascular Risk in Low- and High-Income Participants: Findings From the Reasons for Geographical and Racial Differences in Stroke (REGARDS) Study. J Am Heart Assoc. 2016;5:1–14. doi: 10.1161/JAHA.116.003930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Lazzarino AI, Hamer M, Stamatakis E, Steptoe A. Low socioeconomic status and psychological distress as synergistic predictors of mortality from stroke and coronary heart disease. Psychosomatic medicine. 2013;75:311–316. doi: 10.1097/PSY.0b013e3182898e6d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Heslop P, Smith GD, Carroll D, Macleod J, Hyland F, Hart C. Perceived stress and coronary heart disease risk factors: the contribution of socio-economic position. Brit j health psychol. 2001;6:167–178. doi: 10.1348/135910701169133. [DOI] [PubMed] [Google Scholar]
- 72.Ng DM, Jeffery RW. Relationships between perceived stress and health behaviors in a sample of working adults. Health psychology. 2003;22:638–642. doi: 10.1037/0278-6133.22.6.638. [DOI] [PubMed] [Google Scholar]
- 73.Ye S, Muntner P, Shimbo D, Judd SE, Richman J, Davidson KW, Safford MM. Behavioral mechanisms, elevated depressive symptoms, and the risk for myocardial infarction or death in individuals with coronary heart disease: the REGARDS (Reason for Geographic and Racial Differences in Stroke) study. J Am Coll Cardiol. 2013;61:622–630. doi: 10.1016/j.jacc.2012.09.058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Shaw LJ, Merz CN, Bittner V, Kip K, Johnson BD, Reis SE, Kelsey SF, Olson M, Mankad S, Sharaf BL, Rogers WJ, Pohost GM, Sopko G, Pepine CJ. Importance of socioeconomic status as a predictor of cardiovascular outcome and costs of care in women with suspected myocardial ischemia. Results from the National Institutes of Health, National Heart, Lung and Blood Institute-sponsored Women’s Ischemia Syndrome Evaluation (WISE) J women’s health (2002) 2008;17:1081–1092. doi: 10.1089/jwh.2007.0596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Fabreau GE, Leung AA, Southern DA, Knudtson ML, McWilliams JM, Ayanian JZ, Ghali WA. Sex, socioeconomic status, access to cardiac catheterization, and outcomes for acute coronary syndromes in the context of universal healthcare coverage. Circ Cardiovasc Qual Outcomes. 2014;7:540–549. doi: 10.1161/CIRCOUTCOMES.114.001021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.LeFevre ML. Behavioral counseling to promote a healthful diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2014;161:587–593. doi: 10.7326/M14-1796. [DOI] [PubMed] [Google Scholar]
- 77.Lin JS, O’Connor E, Evans CV, Senger CA, Rowland MG, Groom HC. Behavioral counseling to promote a healthy lifestyle in persons with cardiovascular risk factors: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2014;161:568–578. doi: 10.7326/M14-0130. [DOI] [PubMed] [Google Scholar]
- 78.Brown J, Michie S, Geraghty AW, Yardley L, Gardner B, Shahab L, Stapleton JA, West R. Internet-based intervention for smoking cessation (StopAdvisor) in people with low and high socioeconomic status: a randomised controlled trial. Lancet Respir med. 2014;2:997–1006. doi: 10.1016/S2213-2600(14)70195-X. [DOI] [PubMed] [Google Scholar]
- 79.Siren R, Eriksson JG, Peltonen M, Vanhanen H. Impact of health counselling on cardiovascular disease risk in middle aged men: influence of socioeconomic status. PLoS One. 2014;9:e88959. doi: 10.1371/journal.pone.0088959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Jiang L, Huang H, Johnson A, Dill EJ, Beals J, Manson SM, Roubideaux Y. Socioeconomic Disparities in Weight and Behavioral Outcomes Among American Indian and Alaska Native Participants of a Translational Lifestyle Intervention Project. Diabetes care. 2015;38:2090–2099. doi: 10.2337/dc15-0394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Blair SN, Kampert JB, Kohl HW, 3rd, Barlow CE, Macera CA, Paffenbarger RS, Jr, Gibbons LW. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA. 1996;276:205–210. [PubMed] [Google Scholar]
- 82.Sesso HD, Paffenbarger RS, Jr, Lee IM. Physical activity and coronary heart disease in men: The Harvard Alumni Health Study. Circulation. 2000;102:975–980. doi: 10.1161/01.cir.102.9.975. [DOI] [PubMed] [Google Scholar]
- 83.Borrell LN. The effects of smoking and physical inactivity on advancing mortality in U.S. adults. Ann Epidemiol. 2014;24:484–487. doi: 10.1016/j.annepidem.2014.02.016. [DOI] [PubMed] [Google Scholar]
- 84.Schiller JS, Lucas JW, Ward BW, Peregoy JA. Summary health statistics for U.S. adults: National Health Interview Survey, 2010. Vital and health statistics Series 10, Data from the National Health Survey. 2012:1–207. [PubMed] [Google Scholar]
- 85.Andrade AC, Peixoto SV, Friche AA, Goston JL, Cesar CC, Xavier CC, Proietti FA, Diez Roux AV, Caiaffa WT. Social context of neighborhood and socioeconomic status on leisure-time physical activity in a Brazilian urban center: The BH Health Study. Cadernos de saude publica. 2015;31(Suppl 1):136–147. doi: 10.1590/0102-311X00069514. [DOI] [PubMed] [Google Scholar]
- 86.Gidlow C, Johnston LH, Crone D, Ellis N, James D. A systematic review of the relationship between socio-economic position and physical activity. Health Ed J. 2006;65:338–367. [Google Scholar]
- 87.Schulz AJ, Israel BA, Mentz GB, Bernal C, Caver D, DeMajo R, Diaz G, Gamboa C, Gaines C, Hoston B, Opperman A, Reyes AG, Rowe Z, Sand SL, Woods S. Effectiveness of a walking group intervention to promote physical activity and cardiovascular health in predominantly non-Hispanic black and Hispanic urban neighborhoods: findings from the walk your heart to health intervention. Health Educ Behav. 2015;42:380–392. doi: 10.1177/1090198114560015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Havranek EP, Mujahid MS, Barr DA, Blair IV, Cohen MS, Cruz-Flores S, Davey-Smith G, Dennison-Himmelfarb CR, Lauer MS, Lockwood DW, Rosal M, Yancy CW, American Heart Association Council on Quality of C, Outcomes Research CoE, Prevention CoC, Stroke Nursing CoL, Cardiometabolic H and Stroke C Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2015;132:873–898. doi: 10.1161/CIR.0000000000000228. [DOI] [PubMed] [Google Scholar]
- 89.Pearson TA, Palaniappan LP, Artinian NT, Carnethon MR, Criqui MH, Daniels SR, Fonarow GC, Fortmann SP, Franklin BA, Galloway JM, Goff DC, Jr, Heath GW, Frank AT, Kris-Etherton PM, Labarthe DR, Murabito JM, Sacco RL, Sasson C, Turner MB, American Heart Association Council on E and Prevention American Heart Association Guide for Improving Cardiovascular Health at the Community Level, 2013 update: a scientific statement for public health practitioners, healthcare providers, and health policy makers. Circulation. 2013;127:1730–1753. doi: 10.1161/CIR.0b013e31828f8a94. [DOI] [PubMed] [Google Scholar]
- 90.Jeemon P, Narayanan G, Kondal D, Kahol K, Bharadwaj A, Purty A, Negi P, Ladhani S, Sanghvi J, Singh K, Kapoor D, Sobti N, Lall D, Manimunda S, Dwivedi S, Toteja G, Prabhakaran D, Investigators DS Task shifting of frontline community health workers for cardiovascular risk reduction: design and rationale of a cluster randomised controlled trial (DISHA study) in India. BMC Public Health. 2016;16:264. doi: 10.1186/s12889-016-2891-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Adeyemo A, Tayo BO, Luke A, Ogedegbe O, Durazo-Arvizu R, Cooper RS. The Nigerian antihypertensive adherence trial: a community-based randomized trial. J hypertens. 2013;31:201–207. doi: 10.1097/HJH.0b013e32835b0842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Gaziano T, Abrahams-Gessel S, Surka S, Sy S, Pandya A, Denman CA, Mendoza C, Puoane T, Levitt NS. Cardiovascular Disease Screening By Community Health Workers Can Be Cost-Effective In Low-Resource Countries. Health Aff (Millwood) 2015;34:1538–1545. doi: 10.1377/hlthaff.2015.0349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Gaziano TA, Abrahams-Gessel S, Denman CA, Montano CM, Khanam M, Puoane T, Levitt NS. An assessment of community health workers’ ability to screen for cardiovascular disease risk with a simple, non-invasive risk assessment instrument in Bangladesh, Guatemala, Mexico, and South Africa: an observational study. Lancet Global health. 2015;3:e556–e563. doi: 10.1016/S2214-109X(15)00143-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Shroufi A, Chowdhury R, Anchala R, Stevens S, Blanco P, Han T, Niessen L, Franco OH. Cost effective interventions for the prevention of cardiovascular disease in low and middle income countries: a systematic review. BMC Public Health. 2013;13:285. doi: 10.1186/1471-2458-13-285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Afshin A, Penalvo J, Del Gobbo L, Kashaf M, Micha R, Morrish K, Pearson-Stuttard J, Rehm C, Shangguan S, Smith JD, Mozaffarian D. CVD Prevention Through Policy: a Review of Mass Media, Food/Menu Labeling, Taxation/Subsidies, Built Environment, School Procurement, Worksite Wellness, and Marketing Standards to Improve Diet. Curr cardiol rep. 2015;17:98. doi: 10.1007/s11886-015-0658-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Map was created using the Interactive Atlas of Heart Disease and Stroke, a website developed by the Centers for Disease Control and Prevention, Division for Heart Disease and Stroke Prevention. http://www.cdc.gov/dhdsp/maps/atlas.
- 97.Bagheri N, Gilmour B, McRae I, Konings P, Dawda P, Del Fante P, van Weel C. Community cardiovascular disease risk from cross-sectional general practice clinical data: a spatial analysis. Prev Chronic Dis. 2015;12:E26. doi: 10.5888/pcd12.140379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Engdahl J, Holmen A, Rosenqvist M, Stromberg U. Uptake of atrial fibrillation screening aiming at stroke prevention: geo-mapping of target population and non-participation. BMC Public Health. 2013;13:715. doi: 10.1186/1471-2458-13-715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Sampson UK, Kaplan RM, Cooper RS, Diez Roux AV, Marks JS, Engelgau MM, Peprah E, Mishoe H, Boulware LE, Felix KL, Califf RM, Flack JM, Cooper LA, Gracia JN, Henderson JA, Davidson KW, Krishnan JA, Lewis TT, Sanchez E, Luban NL, Vaccarino V, Wong WF, Wright JT, Jr, Meyers D, Ogedegbe OG, Presley-Cantrell L, Chambers DA, Belis D, Bennett GC, Boyington JE, Creazzo TL, de Jesus JM, Krishnamurti C, Lowden MR, Punturieri A, Shero ST, Young NS, Zou S, Mensah GA. Reducing Health Inequities in the U.S.: Recommendations From the NHLBI’s Health Inequities Think Tank Meeting. J Am Coll Cardiol. 2016;68:517–254. doi: 10.1016/j.jacc.2016.04.059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Bajekal M, Scholes S, O’Flaherty M, Raine R, Norman P, Capewell S. Unequal trends in coronary heart disease mortality by socioeconomic circumstances, England 1982-2006: an analytical study. PLoS One. 2013;8:e59608. doi: 10.1371/journal.pone.0059608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Lotufo PA, Fernandes TG, Bando DH, Alencar AP, Bensenor IM. Income and heart disease mortality trends in Sao Paulo, Brazil, 1996 to 2010. Int J Cardiol. 2013;167:2820–2823. doi: 10.1016/j.ijcard.2012.07.006. [DOI] [PubMed] [Google Scholar]
- 102.Kanjilal S, Gregg EW, Cheng YJ, Zhang P, Nelson DE, Mensah G, Beckles GL. Socioeconomic status and trends in disparities in 4 major risk factors for cardiovascular disease among US adults, 1971-2002. Arch Intern Med. 2006;166:2348–2355. doi: 10.1001/archinte.166.21.2348. [DOI] [PubMed] [Google Scholar]
- 103.O’Flaherty M, Bishop J, Redpath A, McLaughlin T, Murphy D, Chalmers J, Capewell S. Coronary heart disease mortality among young adults in Scotland in relation to social inequalities: time trend study. BMJ. 2009;339:b2613. doi: 10.1136/bmj.b2613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Sims M, Diez Roux AV, Boykin S, Sarpong D, Gebreab SY, Wyatt SB, Hickson D, Payton M, Ekunwe L, Taylor HA. The socioeconomic gradient of diabetes prevalence, awareness, treatment, and control among African Americans in the Jackson Heart Study. Ann Epidemiol. 2011;21:892–898. doi: 10.1016/j.annepidem.2011.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Woodward M, Brindle P, Tunstall-Pedoe H. Adding social deprivation and family history to cardiovascular risk assessment: the ASSIGN score from the Scottish Heart Health Extended Cohort (SHHEC) Heart. 2007;93:172–176. doi: 10.1136/hrt.2006.108167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Hippisley-Cox J, Coupland C, Vinogradova Y, Robson J, Minhas R, Sheikh A, Brindle P. Predicting cardiovascular risk in England and Wales: prospective derivation and validation of QRISK2. BMJ. 2008;336:1475–1482. doi: 10.1136/bmj.39609.449676.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Franks P, Tancredi DJ, Winters P, Fiscella K. Including socioeconomic status in coronary heart disease risk estimation. Ann fam med. 2010;8:447–453. doi: 10.1370/afm.1167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Chao TF, Liu CJ, Wang KL, Lin YJ, Chang SL, Lo LW, Hu YF, Tuan TC, Chen TJ, Lip GY, Chen SA. Using the CHA2DS2-VASc score for refining stroke risk stratification in ‘low-risk’ Asian patients with atrial fibrillation. J Am Coll Cardiol. 2014;64:1658–1665. doi: 10.1016/j.jacc.2014.06.1203. [DOI] [PubMed] [Google Scholar]
- 109.Chao TF, Liu CJ, Wang KL, Lin YJ, Chang SL, Lo LW, Hu YF, Tuan TC, Chen TJ, Lip GY, Chen SA. Should atrial fibrillation patients with 1 additional risk factor of the CHA2DS2-VASc score (beyond sex) receive oral anticoagulation? J Am Coll Cardiol. 2015;65:635–642. doi: 10.1016/j.jacc.2014.11.046. [DOI] [PubMed] [Google Scholar]
- 110.Yusuf S, Wood D, Ralston J, Reddy KS. The World Heart Federation’s vision for worldwide cardiovascular disease prevention. Lancet. 2015;386:399–402. doi: 10.1016/S0140-6736(15)60265-3. [DOI] [PubMed] [Google Scholar]
- 111.Smith SC, Jr, Chen D, Collins A, Harold JG, Jessup M, Josephson S, Logstrup S, Jur C, Sacco RL, Vardas PE, Wood DA, Zoghbi WA. Moving from political declaration to action on reducing the global burden of cardiovascular diseases: a statement from the global cardiovascular disease taskforce. Circulation. 2013;128:2546–2548. doi: 10.1161/CIR.0b013e3182a93504. [DOI] [PubMed] [Google Scholar]
- 112.Vanassche T, Connolly SJ, Eikelboom JW, Healey JS, Lauw MN, Masiero S, Wang J, Yusuf S. Abstract 18936: Can Biomarkers Improve Risk Stratification of Atrial Fibrillation Patients? Analysis of 3578 Aspirin-treated Patients in ACTIVE and AVERROES. Circulation. 2014;130:A18936. [Google Scholar]
- 113.Williams DR, Purdie-Vaughns V. Social and Behavioral Interventions to Improve Health and Reduce Disparities in Health [Internet] 2015 [cited 2018 Jan 30]; available from https://www.ahrq.gov/professionals/education/curriculum-tools/population-health/williams.html.
- 114.Tobias M. Social rank: a risk factor whose time has come? Lancet (London, England) 2017;389:1172–1174. doi: 10.1016/S0140-6736(17)30191-5. [DOI] [PubMed] [Google Scholar]