

ᅟ
Engineering of biologic skin substitutes has progressed over time from individual applications of skin cells, or biopolymer scaffolds, to combinations of cells and scaffolds for treatment, healing, and closure of acute and chronic skin wounds. Skin substitutes may be categorized into three groups: acellular scaffolds, temporary substitutes containing allogeneic skin cells, and permanent substitutes containing autologous skin cells. Combined use of acellular dermal substitutes with permanent skin substitutes containing autologous cells has been shown to provide definitive wound closure in burns involving greater than 90% of the total body surface area. These advances have contributed to reduced morbidity and mortality from both acute and chronic wounds but, to date, have failed to replace all of the structures and functions of the skin. Among the remaining deficiencies in cellular or biologic skin substitutes are hypopigmentation, absence of stable vascular and lymphatic networks, absence of hair follicles, sebaceous and sweat glands, and incomplete innervation. Correction of these deficiencies depends on regulation of biologic pathways of embryonic and fetal development to restore the full anatomy and physiology of uninjured skin. Elucidation and integration of developmental biology into future models of biologic skin substitutes promises to restore complete anatomy and physiology, and further reduce morbidity from skin wounds and scar. This article offers a review of recent advances in skin cell thrapies and discusses the future prospects in cutaneous regeneration.
Keywords: Burns, Cell therapy, Skin substitute, Tissue engineering, Wound closure, Scar, Regenerative medicine
Background
Advances in burn care during the recent past have included improvements in fluid resuscitation, early wound excision, respiratory support and management of inhalation injury, improved nutrition and modulation of the hypermetabolic response, infection control and enhanced immune function, incorporation of aerobic exercise during recovery, and development of anti-scarring strategies [1]. These advances have led to significant reductions in mortality, hospital stay, and long-term morbidity. In addition to these comprehensive innovations, skin cell therapies have become part of the treatment plan for extensive burns. This review will summarize several of the most significant advances since 1980 and discuss prospects for further progress in cutaneous regeneration in the future.
Review
Medical needs
Cutaneous burns can generate a continuum of injuries with increasing depth into the skin. Partial-thickness burns often do not require grafting and, if debrided and treated with antimicrobial dressings, will heal spontaneously from regrowth of epithelial appendages (hair follicles, sebaceous and sweat glands) to cover the wounds. However, deep partial-thickness burns which do not heal within ~ 3 weeks and full-thickness burns require replacement of the epidermal barrier by transplantation of autologous keratinocytes. Transplantation can be accomplished by either conventional split-thickness skin grafts (STSG), applications of keratinocyte suspensions or sheets, or dermal-epidermal skin substitutes [2–5]. Autologous keratinocytes may persist indefinitely and provide permanent wound closure, whereas allogeneic keratinocytes will remain on the wound for a few days to weeks [6–8], delivering growth factors and extracellular matrix components to wounds that promote more rapid wound closure by autologous cells [9]. Combinations of widely meshed and expanded (i.e., 1:6) autografts or micrografts applied to excised, full-thickness burns and covered with allograft [10, 11] have been reported, but are slow to heal, allow granulation tissue to form, and tend to scar. Conversely, unmeshed sheet grafts applied as early as possible to critical areas (i.e., face, hands, feet, perineum) have been shown to reduce granulation tissue, minimize scar, and produce optimal functional and cosmetic outcomes [2, 12, 13].
Biological requirements and current alternatives
Wound closure after full-thickness burns requires reestablishment of stable epidermis as a minimum requirement. Stability of the epidermis depends on reformation of the basement membrane and vascularized connective tissues to anchor the outer skin to the body. Split-thickness skin satisfies these requirements but does not replace the epidermal adnexa (hair follicles, sebaceous glands, sweat glands) or regenerate a full complement of sensory or motor nerves. Table 1 summarizes the anatomic features of uninjured skin compared to STSG, engineered skin substitutes (ESS), and healed skin after grafting. It is important to note that split-thickness skin at the first harvest does not regenerate hair follicles, sebaceous glands, or sweat glands but does contain pigmented melanocytes and vascular and neural networks which the engineered skin does not. At the second and subsequent harvests of autografts, pigmentation becomes irregular and scar is more pronounced. Compared with autografts, autologous-ESS containing cultured keratinocytes and fibroblasts may also contain “passenger melanocytes” which may colonize the wound and generate focal, but incomplete, pigmentation [14–16]. Of these deficiencies, perhaps the absence of sweat glands is most important to patients with large total body surface area (TBSA) burns because it impairs the ability to thermo-regulate properly.
Table 1.
Comparisons of cell types in native, engineered and grafted skin (adapted from [99])
| Tissue type | Cell type or structure | Uninjured skin | Split-thickness skin graft | Engineered skin substitutes | Healed skin after grafting |
|---|---|---|---|---|---|
| Epidermis | Keratinocytes | + | + | + | + |
| Hair follicle | + | − | − | − | |
| Sebocytes | + | − | − | − | |
| Sweat gland | + | − | − | − | |
| Melanocytes | + | ± | ± | ± | |
| Immune cells | + | + | − | + | |
| Nerve | + | + | − | ± | |
| Dermis | Fibroblasts | + | + | ± | + |
| Endothelial cells | + | + | − | + | |
| Extracellular matrix | + | ± | ± | ± | |
| Smooth muscle | + | + | − | ± | |
| Immune cells | + | + | − | + | |
| Nerve | + | + | − | ± |
Table 2 provides a partial list of acellular, temporary, and permanent skin substitutes that are either available commercially in the USA or in clinical trials. Acellular skin substitutes recruit fibro-vascular tissues from the wound bed and may consist of either biopolymers, such as collagen and chondroitin-sulfate or elastin (Integra® Dermal Regeneration Template [17]; MatriDerm®) [18], decellularized human dermis (AlloDerm™) [19], derivatized hyaluronic acid (Hyalomatrix®) [20], or polyurethane (BioTemporizing Matrix, “BTM”) [21, 22]. Each of these materials protects open wounds, promotes ingrowth of fibrovascular tissue, and may suppress granulation tissue and scar. However, the biologic materials (i.e., acellular dermis, collagen, hyaluronic acid) are prone to microbial contamination in the absence of antimicrobial agents due to their properties as biological ligands for bacteria and degradation by enzymatic activities [23, 24]. In comparison, synthetic polymers (i.e., polyurethane, poly-glycolic/poly-lactic acids) are often degraded by hydrolysis, have fewer microbial binding sites, and are less prone to microbial contamination. If used as dermal substitutes, the acellular materials may require 2 to 4 weeks to vascularize sufficiently to support a STSG. However, if used as a scaffold for cell transplantation, 2 weeks or longer for vascularization would negatively impact cell survival and reduce cellular engraftment and wound closure. Of the available acellular skin substitutes, Integra® currently has the broadest usage for extensive, life-threatening burns and burn scars in the USA [25] and has demonstrated very favorable outcomes [26, 27] since its introduction in 1996 [17]. Similar results have been described recently using the BTM material which currently remains in clinical trial [22].
Table 2.
Biologic skin substitutes, commercially available or in clinical trial (adapted from [100])
| Model [references] | Composition | Indications for use |
|---|---|---|
| Acellular skin substitutes | ||
| Integra Dermal Regeneration Template [17, 101] | Bovine collagen and chondroitin-sulfate coated with silicone | Burns, reconstructive surgery |
| AlloDerm [19, 102] | Decellularized human dermis | Repair or replacement of damaged or inadequate integumental tissue |
| MatriDerm [103, 104] | Bovine collagen and elastin | Burns, reconstructive surgery |
| Hyalomatrix [20, 105] | Derivatized hyaluronic acid | Partial- and full-thickness wounds |
| BioTemporizing Matrix [22, 106] | Bilaminate degradable polyurethane | Burns, reconstructive surgery |
| Temporary skin substitutes (dressings) | ||
| Cadaver allograft [29, 107] | Split-thickness skin from human donors, unfrozen or cryopreserved | Burns, reconstructive surgery |
| Porcine xenograft [31, 32] | Split-thickness porcine skin, cryopreserved or lyophilized | Burns, reconstructive surgery |
| Apligraf® [108, 109] | Allo hF in collagen gel plus stratified allo hK | Diabetic foot ulcers |
| StrataGraft® [33, 110] | Allo hF in collagen gel plus stratified allo hK | Partial-thickness burns |
| DermaGraft® [111, 112] | Allo hF on poly-galactin mesh | Diabetic foot ulcers |
| Permanent skin substitutes (grafts) | ||
| EpiCel® [34, 113] | Cultured auto hK multi-layer sheet | Full-thickness burns |
| ReCell® [3, 114] | Uncultured suspension of auto hK, delivered as a spray | Partial-thickness burns |
| Reconstructed skin [36, 115] | Auto hF on acellular scaffold of dermal extracelluar matrix, plus stratified auto hK | Full-thickness burns, venous and mixed ulcers |
| Autologous engineered skin substitute [39, 116] | Auto hF on a collagen-GAG scaffold, plus stratified auto hK | Full-thickness burns |
Cellular skin substitutes
Transplantation of cellular skin substitutes has had wide-ranging results for temporary or permanent wound coverage. Temporary cellular dressings include direct harvest of split-thickness skin, available as either fresh or cryopreserved human cadaver skin [28, 29], or porcine skin with storage by chemical fixation or lyophilization [30–32]. In addition, allogeneic human fibroblasts and/or keratinocytes have been combined with degradable scaffolds (i.e., partially denatured collagen (Apligraf™; StrataGraft™) [6, 33], poly-glycolic/poly-lactic acids (DermaGraft™)) which deliver growth factors and extracellular matrix to wounds to promote autologous healing but do not persist more than a few days to weeks. Autologous keratinocytes have been applied as cultured cell sheets (EpiCel™) [34], sprayed cell suspensions prepared during surgery (ReCell™) [35], with culture-expanded fibroblasts as the dermal component [36], or in combination with a polymeric dermal scaffold populated with autologous culture-expanded fibroblasts [37, 38]. Figure 1 shows the histologic organization of a dermal-epidermal skin substitute, surgical application, and results in a pediatric patient [39]. These approaches have helped to reduce mortality in large burns (> 40% TBSA), but they lack hair follicles and glands after transplantation. Limitations of keratinocyte sheets have included poor durability and ulceration [40, 41] and with sprayed keratinocyte suspensions a requirement for co-application with widely meshed skin autograft [42] which reduces the conservation of donor skin and increases scarring after wound closure.
Fig. 1.
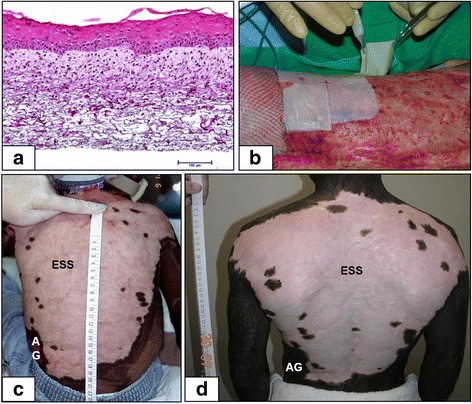
Clinical application of autologous engineered skin substitutes (ESS). a Histology of ESS shows a collagen-based polymer scaffold populated with cultured dermal fibroblasts and epidermal keratinocytes. Scale bar = 0.1 mm. b Surgical application of ESS on prepared wounds can be performed using forceps and secured with staples. c An African-American subject treated with ESS at 3 years of age shows predominant hypopigmentation. d The same subject at 14 years of age has persistent hypopigmentation but has required no reconstruction of the ESS site. Scales in centimeters
Preclinical investigations have reported more complex models that also include melanocytes [43–45], microvascular endothelial cells [46–48], mesenchymal stem cells [49–51], adipocyte stem cells [52], sensory nerve cells [53], hair follicle progenitor cells [54–56], or induced pluripotent stem cells (iPSCs) [57, 58]. Figure 2 shows restoration of natural skin color in human ESS with isogeneic melanocytes grafted to immunodeficient mice [59] and localization of melanocytes to their normal anatomic location at the basement membrane. These kinds of models promote activation of biological signaling pathways which may stimulate more rapid and complete healing, or drive expression of additional phenotypes to correct anatomic deficiencies. The prospective benefits of progenitor cells may include generation of additional populations of differentiated parenchymal cells (e.g., hair, sweat glands, nerve) in engineered skin grafts. Figure 3 shows the expression of hair in engineered skin containing neonatal murine skin cells [54]. As biologic complexity increases and phenotypes are restored, engineered tissues gain structures and functions that do not result from mechanisms of wound healing. These added properties may derive from embryonic or fetal mechanisms that regulate tissue morphogenesis, in addition to the mechanisms of wound healing. Together, the combination of developmental biology, wound healing, and biomedical engineering constitute the emerging field of regenerative medicine.
Fig. 2.
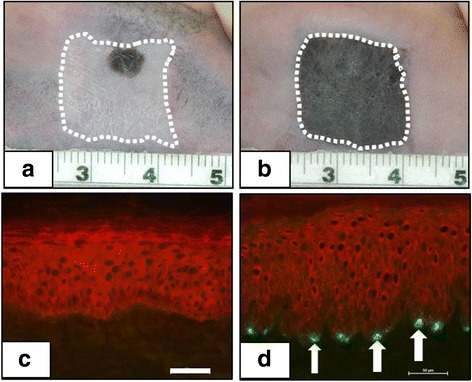
Correction of pigmentation with cultured autologous melanocytes in preclinical studies. a Human engineered skin substitutes (ESS) on immunodeficient mice showing hypopigmentation at 12 weeks after grafting. b Correction of hypopigmentation after 12 weeks by addition of isogeneic human melanocytes to ESS. Scales in centimeters. c Immunolabeling of epidermis with anti-cytokeratin (red) and the melanocyte-specific maker, tyrosinase-related protein-1 (TRP-1; negative). d Immunolabeling of ESS with added melanocytes shows epidermis (red), and TRP-1-positive melanocytes at the dermal-epidermal junction (white arrows) as in uninjured skin. Scale bars = 50 μm
Fig. 3.
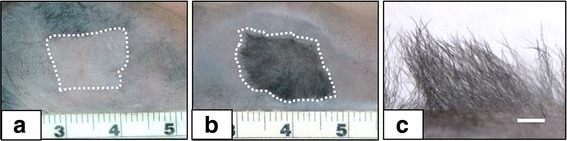
Induction of hair follicles in vivo from neonatal dermal cells grafted to immunodeficient mice. a Human dermal fibroblasts and human epidermal keratinocytes express no hair. b Neonatal murine fibroblasts and human neonatal keratinocytes express chimeric hair at 4 weeks after grafting. Scales in cm. c Higher magnification showing density of regenerated hair is similar to that on positive control mice. Scale = 1 mm
Contemporary research and regenerative medicine
Although great progress has been made in reductions of morbidity and mortality in management of burn wounds, some of the most exciting advances remain ahead. These prospective advances include, but are not limited to, (a) complete restoration of skin anatomy and physiology, (b) gene therapies for specific applications, (c) automated and robotic fabrication of engineered tissues to increase efficiencies and reduce costs, and (d) quantification of wounds with non-invasive biophysical instruments.
Table 3 summarizes the anatomic and physiologic properties that may be missing from split-thickness skin autograft, ESS, or healed wounds after grafting. Among these phenotypes are epidermal barrier, dermal-epidermal junction, hair folliculogenesis and cycling, sebaceous glands, pigmentation, sensory and motor innervation, cardiovascular systems, and subcutaneous fat. Each of these phenotypes results from specific gene expression pathways that regulate its formation. Examples of these pathways are listed and referenced in the table. It is noteworthy that some of the phenotypes share regulatory pathways, such as hair follicles and sweat glands being regulated by wingless integration site of murine mammary tumor virus (Wnt), β-catenin, ectodysplasin (EDA), and its receptor (EDAR) [60, 61]. Similarly, there are members of the Sry-regulated HMG box (Sox) family of transcription factors that are expressed in formation of hair (Sox-2, -21), sebaceous glands (Sox-9), pigmentation (Sox-10), innervation (Sox-2, -10), and cardiovascular development (Sox-7, -17, -18). Despite these similarities, each pathway is expressed in a context of its microenvironment (e.g., stem cells, extracellular matrix) which also contributes to the genesis and stability of the phenotype. Undoubtedly, as continuing studies in developmental biology elucidate these pathways, greater capabilities to guide the anatomy and physiology of biologic skin substitutes will be gained.
Table 3.
Developmental pathways and regulatory factors for cutaneous phenotypes (adapted from [100])
| Cutaneous structures and phenotypes | Regulatory pathways and factors |
|---|---|
| Epidermal barrier | Ca2+ [117, 118] Transglutaminase, loricrin [119, 120] Essential fatty acids, stratum corneum lipids [121, 122] |
| Dermal-epidermal junction | Integrins [123, 124] FAK-Ras-MapK [60, 124] PKB/Akt-ERK1/2 [125] |
| Hair follicle genesis and cycling | Wnt/β-catenin/DKK4/BMPs [60, 61] EDA/EDAR [126, 127] Sox-2, -21 [128, 129] |
| Sebaceous glands | Rac1-Sox9-Lrig1 [61, 130] Wnt; Blimp1; IHH; c-myc [131] TGFβ-1 [132] |
| Sweat glands | Wnt/β-catenin [133] EDA/EDAR/NF-κB [134] DKK4, SHH [135] |
| Pigmentation | c-kit/SCF; [136] ET-3/EDNRB2 [137] Sox-10/Mitf; Eph/EphR; [138] |
| Sensory and motor innervation | c-jun [139] Sox-2,-10 [55] Oct-6; Krox-20; Pax 3 [140] |
| Cardiovascular system | Sox-7, -17, -18 [141] Mef2c/β-catenin [142] VEGF; HOXA9, VEZF1 [143] |
| Subcutaneous fat | PPARγ [144] Pref-1; Fabp4 [145] Myf5; Ebf2; Prdm16; Pgc-1α [146] |
EDA ectodysplasin, EDAR ectodysplasin receptor, TGFβ-1 transforming growth factor β-1, VEGF, vascular endothelial growth factor
Gene therapies for the skin have been studied extensively over the years and have met with limited success [62–64]. Risks from use of retrovirus-based expression systems suggest that lentiviral-mediated genetic modifications may have greater safety and efficacy in prospective studies [65, 66]. However, at least two examples of gene therapy in skin substitutes are currently active in the areas of innate antimicrobial peptides (e.g., cathelicidins, β-defensins) [67, 68] in allogeneic engineered skin to promote healing of chronic wounds and collagen VII for recessive dystrophic epidermolysis bullosa (RDEB) [69, 70]. These approaches to gene therapies require careful considerations for safety and efficacy in clinical applications. Constitutive overexpression of human beta defensin-3 with a non-viral plasmid DNA in an allogeneic model of a skin substitute has been evaluated for microbial management of contaminated wounds and was not tumorigenic [71]. These kinds of approaches provide novel examples for wound management and correction of congenital skin diseases and open countless opportunities for future reductions of morbidity and mortality from skin wounds. The CRISPR/Cas9 system for gene editing [72] offers an alternative for genetic modification of cells without the associated risks of viral vectors [73, 74].
In addition to unique compositions of cells, gene expression, and scaffolds to construct analogs of skin, a critical and limiting factor to greater availability of skin substitutes is manual fabrication of these complex materials. To address this limitation, numerous methods for robotic fabrication of skin and other tissue substitutes have been described [75]. Many of these approaches are highly precise and involve extrusion of cell-populated matrices into specific shapes for transplantation. For skin models, techniques include multi-layering of multiple cell types [76], “ink-jet printing” [77], or transfer of cell-matrix droplets onto a culture substrate by actuation of a laser pulse [78]. Although these robotic systems accomplish physical transfers with relatively high efficiency, they may injure cells by transient exposures to high pressure, temperature, or chemical toxicities. Importantly, cells suspended in viscous scaffolds may be deprived of cellular attachments to cell surface receptors (e.g., integrins, cadherins), resulting in irreversible proliferative arrest and apoptosis [79]. Avoidance of these kinds of growth inhibitions will be essential to the eventual success of robotic systems. It is important to recognize that these kinds of attachment and signaling deprivations do not occur during fetal morphogenesis or wound healing. Therefore, providing tissue-specific ligands for cell surface receptors, or maintaining signaling pathways that regulate proliferation, will likely be required to optimize the mitotic rates of cells in engineered tissues. One approach to satisfying this requirement is formation of cellular organoids [75] which provide cell-cell attachments to preserve cell cycle signaling without attachment of cells to scaffolds or plastic vessels.
Assessments of skin wounds have progressed from subjective examinations by clinicians to more objective measures with non-invasive instruments for both diagnostic and prognostic evaluations. For diagnostic purposes, scanning laser Doppler flowmetry has been shown to provide accurate assessments of burn depth and color with simultaneous image capture [80–82]. Accuracy in determining the TBSA of burns has also been improved with computer software for digital mapping of skin injuries to better calculate critical interventions such as fluid resuscitation. Three-dimensional photography and laser surface scanning [83, 84] provide topographic data that may be coupled with body mapping to generate virtual representations of patients that can be revised during the hospital course to construct a timeline of clinical progress. Non-invasive instruments for assessments of color, shape, surface texture, visco-elastic properties, blood flow, temperature, pH, surface hydration, and water vapor transmission have been adapted from applications in dermatology for more objective determinations of scars [85]. Although these kinds of instruments have high accuracy, they often provide assessments of individual points within fields of wounds or scars which must be considered in sampling plans for data interpretation. Because point measures typically do not represent heterogeneous wounds, data collection at multiple sites is needed to compensate for the subjective selection of individual points to measure within the treatment field. With these kinds of considerations, application of non-invasive instruments for wound assessments has been shown to correct for inter-rater variability in ordinal or observational evaluations of wounds and scars.
Regulatory environments and requirements
Safety and efficacy of skin substitutes are regulated in the USA by the US Food and Drug Administration (FDA). Biologic skin substitutes have increased in complexity from models that replace either dermis or epidermis, to dermal-epidermal models, to those that deliver combinations of biopolymer scaffolds, multiple cell types, or multiple cell sources, to those that express gene products for prospective improvements in wound healing. This spectrum of unprecedented materials presented questions regarding the regulatory framework within which each model would be evaluated for consideration of permission to market. Traditionally, the FDA has consisted of three centers for evaluation of human therapeutics: the Center for Devices and Radiologic Health (CDRH), the Center for Biologics Evaluation and Research (CBER), and the Center for Drug Evaluation and Research (CDER). Availability of cadaveric allograft has been provided under regulations for tissue banking, which are administered by CBER. As the spectrum of research models of skin substitutes broadened during the 1980s and 1990s, several investigative therapies had components that required consideration by multiple centers at FDA. The agency responded proactively with two initiatives that have contributed to greater clarity of the regulatory process and with Guidance for Industry [86, 87] on how to propose a path to market.
An early initiative was FDA’s participation in establishment of definitions and standards for tissue-engineered medical products (TEMPs) through formation of a Division IV of Committee F04 for medical devices through the American Society for Testing and Materials (ASTM) [88]. Beginning in 1997, this organization has had members from academics, government, and industry participating in a consensus process for composing definitions of materials and provision of methods for calibration and testing of the materials. With regard to skin substitutes, the ASTM process has resulted in a Standard Guide for Classification of Therapeutic Skin Substitutes [89], providing consensus definitions and nomenclature. The second initiative was FDA’s establishment in 2002 of the Office of Combination Products, by which investigative therapies are reviewed initially for their primary mode of action [90]. This office confers with the Centers for Human Therapeutics to designate new therapies at a lead center at FDA with participation from other centers as appropriate. Together, these initiatives have added clarity to the assignment of novel therapeutics to a designated regulatory path [91]. In addition to providing a framework for innovative investigative therapies, FDA provides “expanded access” or “compassionate use” permissions for treatment of selected conditions that present high risks of mortality or morbidity to patients [92, 93].
More recently, the 21st Century Cures Act (Cures Act) was signed into law in the USA in December, 2016. As the name implies, this law is intended to facilitate and expedite the availability of novel therapies to patients with serious, or potentially life-threatening, conditions. The Cures Act provides for expedited therapeutic development programs including the Regenerative Medicine Advanced Therapy (RMAT) designation for eligible biologics products, and the Breakthrough Devices program which is designed to facilitate the review of certain innovative medical devices [94]. These new designations by FDA are in addition to previous expedited regulatory pathways of Fast Track development [95], Breakthrough Therapy designation [96], Accelerated Approval [97], and Priority Review designation for drugs [98]. Together, these alternative pathways to provisional or full marketing are likely to increase access to the most advanced therapies by patient populations with the greatest medical needs.
Conclusions
Future prospects for biologic skin substitutes are extensive and diverse. Advances in use and regulation of stem cells in the skin are highly likely to lead to autologous skin substitutes with greater homology to uninjured skin by providing restoration of skin pigmentation, epidermal appendages (hair, sebaceous and sweat glands), a vascular plexus, and subcutaneous tissues. Genetic modification of autologous cells opens tremendous opportunities for regulation of wound closure, reductions in scar formation, and correction of congenital diseases. As these advances in biologic skin substitutes translate into clinical care, it can be predicted with confidence that reductions in morbidity from acquired and congenital skin diseases will also be realized.
Acknowledgements
The authors gratefully acknowledge the expert technical assistance of Christopher Lloyd and Mark Kleiner for the performance of the preclinical studies, Mary Rolfes for the histology, Laura James for the statistical support, and Laura Fowler, RN, and Judy Nelson, RN, for the performance of the clinical research studies.
Funding
Funding of the authors’ studies has been provided by the National Institutes of Health (grant no. 1R21AR064341-01A1), the US Department of Defense (contract no. W81XWH-13-2-0052), and the Shriners Hospitals for Children (grant nos. 85200 and 84050).
Availability of data and materials
Data and materials in this manuscript are referenced from previous publications and may be available from commercial suppliers or upon request from the reference laboratories.
Abbreviations
- ASTM
American Society for Testing and Materials
- BTM
BioTemporizing Matrix
- CBER
Center for Biologics Evaluation and Research
- CDER
Center for Drug Evaluation and Research
- CDRH
Center for Devices and Radiologic Health
- CRISPR
Clustered Regularly Interspaced Short Palindromic Repeats
- Cures Act
The 21st Century Cures Act
- FDA
Food and Drug Administration
- RMAT
Regenerative Medicine Advanced Therapy
- STSG
Split-thickness skin graft
- TEMPs
Tissue-engineered medical products
- RDEB
recessive dystrophic epidermolysis bullosa
Authors’ contributions
Both authors contributed to the content of this manuscript and provided consent for publication. Both authors read and approved the final manuscript.
Ethics approval and consent to participate
All human subject research was performed with approval of the University of Cincinnati Institutional Review Board with regulatory oversight by the US Food and Drug Administration. All animal subject research was performed with approval of the University of Cincinnati Institutional Animal Care and Use Committee and the Animal Care and Use Research Office of the US Army Medical Research and Materiel Command.
Consent for publication
An informed consent to publish de-identified data was obtained from the subjects.
Competing interests
The authors declare that they have no competing interests.
Contributor Information
Steven T. Boyce, Phone: +1-513-872-6080, Email: steven.boyce@uc.edu
Andrea L. Lalley, Email: alalley@shrinent.org
References
- 1.Finnerty CC, Capek K, Voigt C, Hundeshagen G, Cambiaso-Daniel J, Porter C, Sousse LE, El Ayadi A, Zapata-Sirvent R, Guillory A, et al. The P50 research center in perioperative sciences: how the investment by the National Institute of General Medical Sciences in Team Science has reduced post-burn mortality. J Trauma Acute Care Surg. 2017;83(3):532–542. doi: 10.1097/TA.0000000000001644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Warden GD, Saffle JR, Kravitz M. A two-stage technique for excision and grafting of burn wounds. J Trauma. 1982;22(2):98–103. doi: 10.1097/00005373-198202000-00004. [DOI] [PubMed] [Google Scholar]
- 3.Wood FM, Giles N, Stevenson A, Rea S, Fear M. Characterisation of the cell suspension harvested from the dermal epidermal junction using a ReCell(R) kit. Burns. 2012;38(1):44–51. doi: 10.1016/j.burns.2011.03.001. [DOI] [PubMed] [Google Scholar]
- 4.Green H, Kehinde O, Thomas J. Growth of human epidermal cells into multiple epithelia suitable for grafting. Proc Natl Acad Sci U S A. 1979;76:5665–5668. doi: 10.1073/pnas.76.11.5665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Boyce ST, Hansbrough JF. Biologic attachment, growth, and differentiation of cultured human epidermal keratinocytes on a graftable collagen and chondroitin-6-sulfate substrate. Surgery. 1988;103:421–431. [PubMed] [Google Scholar]
- 6.Falanga V, Sabolinski M. A bilayered living skin construct (APLIGRAF) accelerates complete closure of hard-to-heal venous ulcers. Wound Repair Regen. 1999;7(4):201–207. doi: 10.1046/j.1524-475X.1999.00201.x. [DOI] [PubMed] [Google Scholar]
- 7.Griffiths M, Ojeh N, Livingstone R, Price R, Navsaria H. Survival of Apligraf in acute human wounds. Tissue Eng. 2004;10(7-8):1180–1195. doi: 10.1089/ten.2004.10.1180. [DOI] [PubMed] [Google Scholar]
- 8.Centanni JM, Straseski JA, Wicks A, Hank JA, Rasmussen CA, Lokuta MA, Schurr MJ, Foster KN, Faucher LD, Caruso DM, et al. StrataGraft skin substitute is well-tolerated and is not acutely immunogenic in patients with traumatic wounds: results from a prospective, randomized, controlled dose escalation trial. Ann Surg. 2011;253(4):672–683. doi: 10.1097/SLA.0b013e318210f3bd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Parenteau NL, Sabolinski M, Prosky S, Nolte C, Oleson M, Kriwet K, Bilbo P. Biological and physical factors influencing the successful engraftment of a cultured human skin substitute. Biotechnol Bioeng. 1996;523:3–14. doi: 10.1002/(SICI)1097-0290(19961005)52:1<3::AID-BIT1>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- 10.Alexander JW, MacMillan BG, Law E, Kittur DS. Treatment of severe burns with widely meshed skin autograft, and meshed skin allograft overlay. J Trauma. 1981;21(6):433–438. [PubMed] [Google Scholar]
- 11.Medina A, Riegel T, Nystad D, Tredget EE. Modified meek micrografting technique for wound coverage in extensive burn injuries. J Burn Care Res. 2016;37(5):305–313. doi: 10.1097/BCR.0000000000000244. [DOI] [PubMed] [Google Scholar]
- 12.Gallico Iii GG, O'Connor NE, Compton CC, Remensynder JP, Kehinde O, Green H. Cultured epithelial autografts for giant congenital nevi. Plast Reconstr Surg. 1989;84:1–9. doi: 10.1097/00006534-198907000-00001. [DOI] [PubMed] [Google Scholar]
- 13.Nikkhah D, Booth S, Tay S, Gilbert P, Dheansa B. Comparing outcomes of sheet grafting with 1:1 mesh grafting in patients with thermal burns: a randomized trial. Burns. 2015;41(2):257–264. doi: 10.1016/j.burns.2014.07.023. [DOI] [PubMed] [Google Scholar]
- 14.Compton CC, Warland G, Kratz G. Melanocytes in cultured epithelial grafts are depleted with serial subcultivation and cryopreservation: implications for clinical outcome. J Burn Care Rehabil. 1998;19(4):330–336. doi: 10.1097/00004630-199807000-00011. [DOI] [PubMed] [Google Scholar]
- 15.Harriger MD, Warden GD, Greenhalgh DG, Kagan RJ, Boyce ST. Pigmentation and microanatomy of skin regenerated from composite grafts of cultured cells and biopolymers applied to full-thickness burn wounds. Transplantation. 1995;59(5):702–707. doi: 10.1097/00007890-199503150-00011. [DOI] [PubMed] [Google Scholar]
- 16.Greenhalgh DG. A primer on pigmentation. J Burn Care Res. 2015;36(2):247–257. doi: 10.1097/BCR.0000000000000224. [DOI] [PubMed] [Google Scholar]
- 17.Heimbach D, Luterman A, Burke J, Cram A, Herndon D, Hunt J, Jordan M, McManus W, Solem L, Warden G, Zawacki B. Artificial dermis for major burns: a multi-center randomized clinical trial. Ann Surg. 1988;208(3):313–9. [DOI] [PMC free article] [PubMed]
- 18.Atherton DD, Tang R, Jones I, Jawad M. Early excision and application of matriderm with simultaneous autologous skin grafting in facial burns. Plast Reconstr Surg. 2010;125(2):60e–61e. doi: 10.1097/PRS.0b013e3181c725e5. [DOI] [PubMed] [Google Scholar]
- 19.Jansen LA, De CP, Guay NA, Lineaweaver WC, Shokrollahi K. The evidence base for the acellular dermal matrix AlloDerm: a systematic review. Ann Plast Surg. 2013;70(5):587–594. doi: 10.1097/SAP.0b013e31827a2d23. [DOI] [PubMed] [Google Scholar]
- 20.Gravante G, Delogu D, Giordan N, Morano G, Montone A, Esposito G. The use of Hyalomatrix PA in the treatment of deep partial-thickness burns. J Burn Care Res. 2007;28(2):269–274. doi: 10.1097/BCR.0B013E318031A236. [DOI] [PubMed] [Google Scholar]
- 21.Greenwood JE, Dearman BL. Split skin graft application over an integrating, biodegradable temporizing polymer matrix: immediate and delayed. J Burn Care Res. 2012;33(1):7–19. doi: 10.1097/BCR.0b013e3182372be9. [DOI] [PubMed] [Google Scholar]
- 22.Greenwood JE, Wagstaff MJ, Rooke M, Caplash Y. Reconstruction of extensive calvarial exposure after major burn injury in 2 stages using a biodegradable polyurethane matrix. Eplasty. 2016;16:e17. [PMC free article] [PubMed] [Google Scholar]
- 23.Muangman P, Deubner H, Honari S, Heimbach DM, Engrav LH, Klein MB, Gibran NS. Correlation of clinical outcome of integra application with microbiologic and pathological biopsies. J Trauma. 2006;61(5):1212–1217. doi: 10.1097/01.ta.0000195982.71400.84. [DOI] [PubMed] [Google Scholar]
- 24.Heimbach DM, Warden GD, Luterman A, Jordan MH, Ozobia N, Ryan CM, Voigt DW, Hickerson WL, Saffle JR, DeClement FA, et al. Multicenter postapproval clinical trial of Integra dermal regeneration template for burn treatment. J Burn Care Rehabil. 2003;24(1):42–48. doi: 10.1097/00004630-200301000-00009. [DOI] [PubMed] [Google Scholar]
- 25.Branski LK, Herndon DN, Pereira C, Mlcak RP, Celis MM, Lee JO, Sanford AP, Norbury WB, Zhang XJ, Jeschke MG. Longitudinal assessment of Integra in primary burn management: a randomized pediatric clinical trial. Crit Care Med. 2007;35(11):2615–2623. doi: 10.1097/01.CCM.0000285991.36698.E2. [DOI] [PubMed] [Google Scholar]
- 26.Kopp J, Magnus NE, Rubben A, Merk HF, Pallua N. Radical resection of giant congenital melanocyte nevus and reconstruction with meek-graft covered integra dermal template. Dermatol Surg. 2003;29(6):653–657. doi: 10.1046/j.1524-4725.2003.29157.x. [DOI] [PubMed] [Google Scholar]
- 27.Moiemen NS, Vlachou E, Staiano JJ, Thawy Y, Frame JD. Reconstructive surgery with Integra dermal regeneration template: histologic study, clinical evaluation, and current practice. Plast Reconstr Surg. 2006;117(7 Suppl):160S–174S. doi: 10.1097/01.prs.0000222609.40461.68. [DOI] [PubMed] [Google Scholar]
- 28.Herndon DN. Total burn care. 4. Phildelphia: W.B. Saunders; 2012. [Google Scholar]
- 29.Kagan RJ, Robb EC, Plessinger RT. Human skin banking. Clin Lab Med. 2005;25(3):587–605. doi: 10.1016/j.cll.2005.06.008. [DOI] [PubMed] [Google Scholar]
- 30.Harris RP, Compton JB, Abstan S. Comparison of fresh, frozen, and lyophilized porcine skin as xenografts on burned patients. Burns. 1976;2:71–75. doi: 10.1016/S0305-4179(76)80001-0. [DOI] [Google Scholar]
- 31.Burkey B, Davis W, 3rd, Glat PM. Porcine xenograft treatment of superficial partial-thickness burns in paediatric patients. J Wound Care. 2016;25(2):S10–S15. doi: 10.12968/jowc.2016.25.Sup2.S10. [DOI] [PubMed] [Google Scholar]
- 32.Hermans MH. Porcine xenografts vs. (cryopreserved) allografts in the management of partial thickness burns: is there a clinical difference? Burns. 2014;40(3):408–415. doi: 10.1016/j.burns.2013.08.020. [DOI] [PubMed] [Google Scholar]
- 33.Schurr MJ, Foster KN, Lokuta MA, Rasmussen CA, Thomas-Virnig CL, Faucher LD, Caruso DM, len-Hoffmann BL. Clinical evaluation of NIKS-based bioengineered skin substitute tissue in complex skin defects: phase I/IIa clinical trial results. Adv Wound Care (New Rochelle) 2012;1(2):95–103. doi: 10.1089/wound.2011.0343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sood R, Roggy D, Zieger M, Balledux J, Chaudhari S, Koumanis DJ, Mir HS, Cohen A, Knipe C, Gabehart K, et al. Cultured epithelial autografts for coverage of large burn wounds in eighty-eight patients: the Indiana University experience. J Burn Care Res. 2010;31(4):559–568. doi: 10.1097/BCR.0b013e3181e4ca29. [DOI] [PubMed] [Google Scholar]
- 35.Gravante G, Di Fede MC, Araco A, Grimaldi M, De AB, Arpino A, Cervelli V, Montone A. A randomized trial comparing ReCell system of epidermal cells delivery versus classic skin grafts for the treatment of deep partial thickness burns. Burns. 2007;33(8):966–972. doi: 10.1016/j.burns.2007.04.011. [DOI] [PubMed] [Google Scholar]
- 36.Duranceau L, Genest H, Bortoluzzi P, Moulin V, Auger FA, Germain L. Successful grafting of a novel autologous tissue-engineered skin substitutes (dermis and epidermis) on twelve burn patients. J Burn Care Res. 2014;35(3):S121. [Google Scholar]
- 37.Boyce ST, Warden GD. Principles and practices for treatment of cutaneous wounds with cultured skin substitutes. Am J Surg. 2002;183(4):445–456. doi: 10.1016/S0002-9610(02)00813-9. [DOI] [PubMed] [Google Scholar]
- 38.Hansbrough JF, Boyce ST, Cooper ML, Foreman TJ. Burn wound closure with cultured autologous keratinocytes and fibroblasts attached to a collagen-glycosaminoglycan substrate. JAMA. 1989;262(15):2125–2130. doi: 10.1001/jama.1989.03430150093032. [DOI] [PubMed] [Google Scholar]
- 39.Boyce ST, Simpson PS, Rieman MT, Warner PM, Yakuboff KP, Kevin BJ, Nelson JK, Fowler LA, Kagan RJ. Randomized, paired-site comparison of autologous engineered skin substitutes and split-thickness skin graft for closure of extensive, full-thickness burns. J Burn Care Res. 2017;38(2):61–70. doi: 10.1097/BCR.0000000000000401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Desai MH, Mlakar JM, McCauley RL, Abdullah KM, Rutan RL, Waymack JP, Robson MC, Herndon DN. Lack of long term durability of cultured keratinocyte burn wound coverage: a case report. J Burn Care Rehabil. 1991;12:540–545. doi: 10.1097/00004630-199111000-00009. [DOI] [PubMed] [Google Scholar]
- 41.Wood FM, Kolybaba ML, Allen P. The use of cultured epithelial autograft in the treatment of major burn injuries: a critical review of the literature. Burns. 2006;32(4):395–401. doi: 10.1016/j.burns.2006.01.008. [DOI] [PubMed] [Google Scholar]
- 42.Sood R, Roggy DE, Zieger MJ, Nazim M, Hartman BC, Gibbs JT. A comparative study of spray keratinocytes and autologous meshed split-thickness skin graft in the treatment of acute burn injuries. Wounds. 2015;27(2):31–40. [PubMed] [Google Scholar]
- 43.Boyce ST, Medrano EE, Abdel-Malek ZA, Supp AP, Dodick JM, Nordlund JJ, Warden GD. Pigmentation and inhibition of wound contraction by cultured skin substitutes with adult melanocytes after transplantation to athymic mice. J Invest Dermat. 1993;100(4):360–365. doi: 10.1111/1523-1747.ep12471822. [DOI] [PubMed] [Google Scholar]
- 44.Bottcher-Haberzeth S, Klar AS, Biedermann T, Schiestl C, Meuli-Simmen C, Reichmann E, Meuli M. “Trooping the color”: restoring the original donor skin color by addition of melanocytes to bioengineered skin analogs. Pediatr Surg Intl. 2013;29(3):239–247. doi: 10.1007/s00383-012-3217-0. [DOI] [PubMed] [Google Scholar]
- 45.Duval C, Chagnoleau C, Pouradier F, Sextius P, Condom E, Bernerd F. Human skin model containing melanocytes: essential role of keratinocyte growth factor for constitutive pigmentation-functional response to alpha-melanocyte stimulating hormone and forskolin. Tissue Eng Part C Methods. 2012;18(12):947–957. doi: 10.1089/ten.tec.2011.0676. [DOI] [PubMed] [Google Scholar]
- 46.Supp DM, Wilson-Landy K, Boyce ST. Human dermal microvascular endothelial cells form vascular analogs in cultured skin substitutes after grafting to athymic mice. FASEB J. 2002;16(8):797–804. doi: 10.1096/fj.01-0868com. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Black AF, Berthod F, L'Heureux N, Germain L, Auger FA. In vitro reconstruction of a human capillary-like network in a tissue-engineered skin equivalent. FASEB J. 1998;12(13):1331–1340. doi: 10.1096/fasebj.12.13.1331. [DOI] [PubMed] [Google Scholar]
- 48.Tremblay PL, Hudon V, Berthod F, Germain L, Auger FA. Inosculation of tissue-engineered capillaries with the host’s vasculature in a reconstructed skin transplanted on mice. Am J Transplant. 2005;5(5):1002–1010. doi: 10.1111/j.1600-6143.2005.00790.x. [DOI] [PubMed] [Google Scholar]
- 49.Bhowmick S, Scharnweber D, Koul V. Co-cultivation of keratinocyte-human mesenchymal stem cell (hMSC) on sericin loaded electrospun nanofibrous composite scaffold (cationic gelatin/hyaluronan/chondroitin sulfate) stimulates epithelial differentiation in hMSCs: in vitro study. Biomaterials. 2016;88:83–96. doi: 10.1016/j.biomaterials.2016.02.034. [DOI] [PubMed] [Google Scholar]
- 50.Klar AS, Biedermann T, Michalak K, Michalczyk T, Meuli-Simmen C, Scherberich A, Meuli M, Reichmann E. Human adipose mesenchymal cells inhibit melanocyte differentiation and the pigmentation of human skin via increased expression of TGF-beta1. J Invest Dermatol. 2017;137(12):2560–2569. doi: 10.1016/j.jid.2017.06.027. [DOI] [PubMed] [Google Scholar]
- 51.Huang S, Lu G, Wu Y, Jirigala E, Xu Y, Ma K, Fu X. Mesenchymal stem cells delivered in a microsphere-based engineered skin contribute to cutaneous wound healing and sweat gland repair. J Dermatol Sci. 2012;66(1):29–36. doi: 10.1016/j.jdermsci.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 52.Morissette Martin P, Maux A, Laterreur V, Mayrand D, V LG, Moulin VJ, Fradette J. Enhancing repair of full-thickness excisional wounds in a murine model: impact of tissue-engineered biological dressings featuring human differentiated adipocytes. Acta Biomaterialia. 2015;22:39–49. [DOI] [PubMed]
- 53.Blais M, Parenteau-Bareil R, Cadau S, Berthod F. Concise review: tissue-engineered skin and nerve regeneration in burn treatment. Stem Cells Transl Med. 2013;2(7):545–551. doi: 10.5966/sctm.2012-0181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Sriwiriyanont P, Lynch KA, McFarland KL, Supp DM, Boyce ST. Characterization of hair follicle development in engineered skin substitutes. PLoS One. 2013;8(6):e65664. doi: 10.1371/journal.pone.0065664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gagnon V, Larouche D, Parenteau-Bareil R, Gingras M, Germain L, Berthod F. Hair follicles guide nerve migration in vitro and in vivo in tissue-engineered skin. J Invest Dermatol. 2011;131(6):1375–1378. doi: 10.1038/jid.2011.34. [DOI] [PubMed] [Google Scholar]
- 56.Agabalyan NA, Rosin NL, Rahmani W, Biernaskie J. Hair follicle dermal stem cells and skin-derived precursor cells: exciting tools for endogenous and exogenous therapies. Exp Dermatol. 2017;26(6):505–509. doi: 10.1111/exd.13359. [DOI] [PubMed] [Google Scholar]
- 57.Gledhill K, Guo Z, Umegaki-Arao N, Higgins CA, Itoh M, Christiano AM. Melanin transfer in human 3D skin equivalents generated exclusively from induced pluripotent stem cells. PLoS One. 2015;10(8):e0136713. doi: 10.1371/journal.pone.0136713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Itoh M, Umegaki-Arao N, Guo Z, Liu L, Higgins CA, Christiano AM. Generation of 3D skin equivalents fully reconstituted from human induced pluripotent stem cells (iPSCs) PLoS One. 2013;8(10):e77673. doi: 10.1371/journal.pone.0077673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Boyce ST, Lloyd CM, Kleiner MC, Swope VB, Abdel-Malek Z, Supp DM. Restoration of cutaneous pigmentation by transplantation to mice of isogeneic human melanocytes in dermal-epidermal engineered skin substitutes. Pigment Cell Melanoma Res. 2017;30(6):531–540. doi: 10.1111/pcmr.12609. [DOI] [PubMed] [Google Scholar]
- 60.Zhang Y, Tomann P, Andl T, Gallant NM, Huelsken J, Jerchow B, Birchmeier W, Paus R, Piccolo S, Mikkola ML, et al. Reciprocal requirements for EDA/EDAR/NF-kappaB and Wnt/beta-catenin signaling pathways in hair follicle induction. Dev Cell. 2009;17(1):49–61. doi: 10.1016/j.devcel.2009.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Morgan BA. The dermal papilla: an instructive niche for epithelial stem and progenitor cells in development and regeneration of the hair follicle. Cold Spring Harb Perspect Med. 2014;4(7):a015180. doi: 10.1101/cshperspect.a015180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Morgan JR, Barrandon Y, Green H, Mulligan RC. Expression of an exogenous growth hormone gene in transplantable human epidermal cells. Science. 1987;237:1476–1479. doi: 10.1126/science.3629250. [DOI] [PubMed] [Google Scholar]
- 63.Wilson JM, Birinyi LK, Salomon RN, Libby P, Callow AD, Mulligan RC. Genetically modified endothelial cells in the treatment of human diseases. Trans Assoc Am Physicians. 1989;102:139–147. [PubMed] [Google Scholar]
- 64.Selden RF, Skoskiewicz MJ, Howie KB, Russell PS, Goodman HM. Implantation of genetically engineered fibroblasts into mice: implications for gene therapy. Science. 1987;236(4802):714–718. doi: 10.1126/science.3472348. [DOI] [PubMed] [Google Scholar]
- 65.Clement F, Grockowiak E, Zylbersztejn F, Fossard G, Gobert S, Maguer-Satta V. Stem cell manipulation, gene therapy and the risk of cancer stem cell emergence. Stem Cell Investig. 2017;4:67. doi: 10.21037/sci.2017.07.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.White M, Whittaker R, Gandara C, Stoll EA. A guide to approaching regulatory considerations for lentiviral-mediated gene therapies. Hum Gene Ther Methods. 2017;28(4):163–176. doi: 10.1089/hgtb.2017.096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Bals R, Weiner DJ, Moscioni AD, Meegalla RL, Wilson JM. Augmentation of innate host defense by expression of a cathelicidin antimicrobial peptide. Infect Immun. 1999;67(11):6084–6089. doi: 10.1128/iai.67.11.6084-6089.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Comer AR, Rasmussen CA, Thomas-Virnig CL, Lokuta MA, Shaughnessy LM, Schlosser SJ, Johnston CE, Bauer RL, Cleven TD, Wieczorek NC, et al. Preclinical development and planned clinical evaluation of a human skin substitute engineered to secrete elevated levels of a host defense peptide. Proceedings of the Innovations in Wound Healing Conference. 2014; (abstract).
- 69.Siprashvili Z, Nguyen NT, Bezchinsky MY, Marinkovich MP, Lane AT, Khavari PA. Long-term type VII collagen restoration to human epidermolysis bullosa skin tissue. Hum Gene Ther. 2010;21(10):1299–1310. doi: 10.1089/hum.2010.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Ortiz-Urda S, Lin Q, Green CL, Keene DR, Marinkovich MP, Khavari PA. Injection of genetically engineered fibroblasts corrects regenerated human epidermolysis bullosa skin tissue. J Clin Invest. 2003;111(2):251–255. doi: 10.1172/JCI200317193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Gibson AL, Thomas-Virnig CL, Centanni JM, Schlosser SJ, Johnston CE, Van Winkle KF, Szilagyi A, He LK, Shankar R, Allen-Hoffmann BL. Nonviral human beta defensin-3 expression in a bioengineered human skin tissue: a therapeutic alternative for infected wounds. Wound Repair Regen. 2012;20(3):414–424. doi: 10.1111/j.1524-475X.2012.00786.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Komor AC, Badran AH, Liu DR. CRISPR-based technologies for the manipulation of eukaryotic genomes. Cell. 2017;168(1-2):20–36. doi: 10.1016/j.cell.2016.10.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Go DE, Stottmann RW. The impact of CRISPR/Cas9-based genomic engineering on biomedical research and medicine. Curr Mol Med. 2016;16(4):343–352. doi: 10.2174/1566524016666160316150847. [DOI] [PubMed] [Google Scholar]
- 74.Peng R, Lin G, Li J. Potential pitfalls of CRISPR/Cas9-mediated genome editing. FEBS J. 2016;283(7):1218–1231. doi: 10.1111/febs.13586. [DOI] [PubMed] [Google Scholar]
- 75.Patra S, Young V. A review of 3D printing techniques and the future in biofabrication of bioprinted tissue. Cell Biochem Biophys. 2016;74(2):93–98. doi: 10.1007/s12013-016-0730-0. [DOI] [PubMed] [Google Scholar]
- 76.Lee V, Singh G, Trasatti JP, Bjornsson C, Xu X, Tran TN, Yoo SS, Dai G, Karande P. Design and fabrication of human skin by three-dimensional bioprinting. Tissue Engineering Part C Methods. 2014;20(6):473–484. doi: 10.1089/ten.tec.2013.0335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Cui X, Boland T. Human microvasculature fabrication using thermal inkjet printing technology. Biomaterials. 2009;30(31):6221–6227. doi: 10.1016/j.biomaterials.2009.07.056. [DOI] [PubMed] [Google Scholar]
- 78.Koch L, Deiwick A, Schlie S, Michael S, Gruene M, Coger V, Zychlinski D, Schambach A, Reimers K, Vogt PM, et al. Skin tissue generation by laser cell printing. Biotechnol Bioeng. 2012;109(7):1855–1863. doi: 10.1002/bit.24455. [DOI] [PubMed] [Google Scholar]
- 79.Cho HJ, Youn SW, Cheon SI, Kim TY, Hur J, Zhang SY, Lee SP, Park KW, Lee MM, Choi YS, et al. Regulation of endothelial cell and endothelial progenitor cell survival and vasculogenesis by integrin-linked kinase. Arterioscler Thromb Vasc Biol. 2005;25(6):1154–1160. doi: 10.1161/01.ATV.0000164312.20008.93. [DOI] [PubMed] [Google Scholar]
- 80.Burke-Smith A, Collier J, Jones I. A comparison of non-invasive imaging modalities: Infrared thermography, spectrophotometric intracutaneous analysis and laser Doppler imaging for the assessment of adult burns. Burns. 2015;41(8):1695–1707. doi: 10.1016/j.burns.2015.06.023. [DOI] [PubMed] [Google Scholar]
- 81.Jaskille AD, Ramella-Roman JC, Shupp JW, Jordan MH, Jeng JC. Critical review of burn depth assessment techniques: part II. Review of laser doppler technology. J Burn Care Res. 2010;31(1):151–157. doi: 10.1097/BCR.0b013e3181c7ed60. [DOI] [PubMed] [Google Scholar]
- 82.Ida T, Iwazaki H, Kawaguchi Y, Kawauchi S, Ohkura T, Iwaya K, Tsuda H, Saitoh D, Sato S, Iwai T. Burn depth assessments by photoacoustic imaging and laser Doppler imaging. Wound Repair Regen. 2016;24(2):349–355. doi: 10.1111/wrr.12374. [DOI] [PubMed] [Google Scholar]
- 83.Farrar E, Pujji O, Jeffery S. Three-dimensional wound mapping software compared to expert opinion in determining wound area. Burns. 2017;43(8):1736–1741. doi: 10.1016/j.burns.2017.05.015. [DOI] [PubMed] [Google Scholar]
- 84.Bailey JK, Burkes SA, Visscher MO, Whitestone J, Kagan RJ, Yakuboff KP, Warner P, Randall Wickett R. Multimodal quantitative analysis of early pulsed-dye laser treatment of scars at a pediatric burn hospital. Dermatol Surg. 2012;38(9):1490–1496. doi: 10.1111/j.1524-4725.2012.02451.x. [DOI] [PubMed] [Google Scholar]
- 85.Serup J, Jemed GBE, Grove GL. Handbook of non-invasive methods and the skin, 2nd edn. CRC Press, Inc.: Boca Raton; 2006.
- 86.US Food and Drug Administration Guidance for industry: guidance for human somatic cell therapy and gene therapy. Federal Register. 1998;63:36413. [Google Scholar]
- 87.US Food and Drug Administration Guidance for industry: chronic cutaneous ulcer and burn wounds - developing products for treatment. Federal Register. 2006;65(125):39912. [Google Scholar]
- 88.American Society for Testing and Materials . Standard guide for preservation of tissue engineered medical products. In., Report No.: F 2386-04. West Conshohocken: ASTM International; 2007. [Google Scholar]
- 89.American Society for Testing and Materials . Standard guide for classification of therapeutic skin substitutes. In., Report No.: F 2311-08. West Conshohocken: ASTM International; 2009. [Google Scholar]
- 90.US Food and Drug Administration . Guidance for industry: how to write a request for designation. 2011. [Google Scholar]
- 91.Witten CM, McFarland RD, Simek SL. Concise review: the U.S. Food and Drug Administration and Regenerative Medicine. Stem Cells Transl Med. 2015;4(12):1495–1499. doi: 10.5966/sctm.2015-0098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.US Food and Drug Administration . Expanded access for medical devices: compassionate use. 2014. [Google Scholar]
- 93.US Food and Drug Administration . Expanded access (Compassionate use) 2017. [Google Scholar]
- 94.US Food and Drug Administration . 21st century cures act. 2017. [Google Scholar]
- 95.US Food and Drug Administration . Fast track. 2017. [Google Scholar]
- 96.US Food and Drug Administration . Breakthrough therapy. 2017. [Google Scholar]
- 97.US Food and Drug Administration . Accelerated approval. 2017. [Google Scholar]
- 98.US Food and Drug Administration . Priority review. 2017. [Google Scholar]
- 99.Boyce ST. Design principles for composition and performance of cultured skin substitutes. Burns. 2001;27(5):523–533. doi: 10.1016/S0305-4179(01)00019-5. [DOI] [PubMed] [Google Scholar]
- 100.Boyce ST, Supp DM. Biologic skin substitutes. In: Albanna MZ, Holmes JH, editors. Skin tissue engineering and regenerative medicine. New York: Academic Press/Elsevier; 2016. pp. 211–238. [Google Scholar]
- 101.Lohana P, Hassan S, Watson SB. Integra in burns reconstruction: our experience and report of an unusual immunological reaction. Ann Burns Fire Disasters. 2014;27(1):17–21. [PMC free article] [PubMed] [Google Scholar]
- 102.Ellis CV, Kulber DA. Acellular dermal matrices in hand reconstruction. Plast Reconstr Surg. 2012;130(5 Suppl 2):256S–269S. doi: 10.1097/PRS.0b013e318265a5cf. [DOI] [PubMed] [Google Scholar]
- 103.Halim AS, Khoo TL, Mohd Yussof SJ. Biologic and synthetic skin substitutes: an overview. Indian J Plast Surg. 2010;43(Suppl):S23–S28. doi: 10.4103/0970-0358.70712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.DeVries HJC, Mekkes JR, Middelkoop E, Hinrichs WLJ, Wildevuur CHR. Dermal substitutes for full-thickness wounds in one-stage grafting model. Wound Repair Regen. 1993;1:244–252. doi: 10.1046/j.1524-475X.1993.10410.x. [DOI] [PubMed] [Google Scholar]
- 105.Myers SR, Partha VN, Soranzo C, Price RD, Navsaria HA. Hyalomatrix: a temporary epidermal barrier, hyaluronan delivery, and neodermis induction system for keratinocyte stem cell therapy. Tissue Eng. 2007;13(11):2733–2741. doi: 10.1089/ten.2007.0109. [DOI] [PubMed] [Google Scholar]
- 106.Greenwood JE, Dearman BL. Comparison of a sealed, polymer foam biodegradable temporizing matrix against Integra(R) dermal regeneration template in a porcine wound model. J Burn Care Res. 2012;33(1):163–173. doi: 10.1097/BCR.0b013e318233fac1. [DOI] [PubMed] [Google Scholar]
- 107.May SR, DeClement F. Skin banking. Part I. Procurement of transplantable cadaveric allograft skin for burn wound coverage. J Burn Care Rehabil. 1981;2:7–23. doi: 10.1097/00004630-198101000-00003. [DOI] [Google Scholar]
- 108.Griffiths CEM, Nickoloff BJ. Keratinocyte intercellular adhesion molecule-1 (ICAM-1) expression precedes dermal T lymphocyte infiltration in allergic contact dermatitis (Rhus dermatitis) Am J Pathol. 1989;135:1045–1053. [PMC free article] [PubMed] [Google Scholar]
- 109.Carlson M, Faria K, Shamis Y, Leman J, Ronfard V, Garlick J. Epidermal stem cells are preserved during commercial-scale manufacture of a bilayered, living cellular construct (Apligraf(R)) Tissue Eng Part A. 2011;17(3-4):487–493. doi: 10.1089/ten.tea.2010.0268. [DOI] [PubMed] [Google Scholar]
- 110.Schurr MJ, Foster KN, Centanni JM, Comer AR, Wicks A, Gibson AL, Thomas-Virnig CL, Schlosser SJ, Faucher LD, Lokuta MA, et al. Phase I/II clinical evaluation of StrataGraft: a consistent, pathogen-free human skin substitute. J Trauma. 2009;66(3):866–873. doi: 10.1097/TA.0b013e31819849d6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Frykberg RG, Marston WA, Cardinal M. The incidence of lower-extremity amputation and bone resection in diabetic foot ulcer patients treated with a human fibroblast-derived dermal substitute. Adv Skin Wound Care. 2015;28(1):17–20. doi: 10.1097/01.ASW.0000456630.12766.e9. [DOI] [PubMed] [Google Scholar]
- 112.Harding K, Sumner M, Cardinal M. A prospective, multicentre, randomised controlled study of human fibroblast-derived dermal substitute (Dermagraft) in patients with venous leg ulcers. Intnl Wound J. 2013;10(2):132–137. doi: 10.1111/iwj.12053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Gallico Iii GG, O'Connor NE, Compton CC, Kehinde O, Green H. Permanent coverage of large burn wounds with autologous cultured human epithelium. N Engl J Med. 1984;311:448–451. doi: 10.1056/NEJM198408163110706. [DOI] [PubMed] [Google Scholar]
- 114.Campanella SD, Rapley P, Ramelet AS. A randomised controlled pilot study comparing Mepitel ® and SurfaSoft ® on paediatric donor sites treated with Recell ®. Burns. 2011;37(8):1334–1342. doi: 10.1016/j.burns.2011.04.019. [DOI] [PubMed] [Google Scholar]
- 115.Boa O, Cloutier CB, Genest H, Labbe R, Rodrigue B, Soucy J, Roy M, Arsenault F, Ospina CE, Dube N, et al. Prospective study on the treatment of lower-extremity chronic venous and mixed ulcers using tissue-engineered skin substitute made by the self-assembly approach. Adv Skin Wound Care. 2013;26(9):400–409. doi: 10.1097/01.ASW.0000433102.48268.2a. [DOI] [PubMed] [Google Scholar]
- 116.Boyce ST, Kagan RJ, Greenhalgh DG, Warner P, Yakuboff KP, Palmieri T, Warden GD. Cultured skin substitutes reduce requirements for harvesting of skin autograft for closure of excised, full-thickness burns. J Trauma. 2006;60(4):821–829. doi: 10.1097/01.ta.0000196802.91829.cc. [DOI] [PubMed] [Google Scholar]
- 117.Elsholz F, Harteneck C, Muller W, Friedland K. Calcium--a central regulator of keratinocyte differentiation in health and disease. Eur J Dermatol. 2014;24(6):650–661. doi: 10.1684/ejd.2014.2452. [DOI] [PubMed] [Google Scholar]
- 118.Boyce ST, Ham RG. Calcium-regulated differentiation of normal human epidermal keratinocytes in chemically defined clonal culture and serum-free serial culture. J Invest Dermatol. 1983;81(1 Suppl):33s–40s. doi: 10.1111/1523-1747.ep12540422. [DOI] [PubMed] [Google Scholar]
- 119.Rice RH, Durbin-Johnson BP, Ishitsuka Y, Salemi M, Phinney BS, Rocke DM, Roop DR. Proteomic analysis of loricrin knockout mouse epidermis. J Proteome Res. 2016;15(8):2560–2566. doi: 10.1021/acs.jproteome.6b00108. [DOI] [PubMed] [Google Scholar]
- 120.Wikramanayake TC, Stojadinovic O, Tomic-Canic M. Epidermal Differentiation in Barrier Maintenance and Wound Healing. Adv Wound Care (New Rochelle) 2014;3(3):272–280. doi: 10.1089/wound.2013.0503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Feingold KR, Elias PM. Role of lipids in the formation and maintenance of the cutaneous permeability barrier. Biochim Biophys Acta. 2014;1841(3):280–294. doi: 10.1016/j.bbalip.2013.11.007. [DOI] [PubMed] [Google Scholar]
- 122.Ponec M, Weerheim A, Kempenaar J, Mulder A, Gooris GS, Bouwstra J, Mommaas AM. The formation of competent barrier lipids in reconstructed human epidermis requires the presence of vitamin C. J Invest Dermatol. 1997;109(3):348–355. doi: 10.1111/1523-1747.ep12336024. [DOI] [PubMed] [Google Scholar]
- 123.Haass NK, Smalley KS, Li L, Herlyn M. Adhesion, migration and communication in melanocytes and melanoma. Pigment Cell Res. 2005;18(3):150–159. doi: 10.1111/j.1600-0749.2005.00235.x. [DOI] [PubMed] [Google Scholar]
- 124.Kramer IJ. Integrins, cell survival, and cell proliferation. In: Kramer IJ, editor. Cell Signalling. 3. New York: Academic Press; 2016. pp. 681–693. [Google Scholar]
- 125.Kippenberger S, Hofmann M, Zoller N, Thaci D, Muller J, Kaufmann R, Bernd A. Ligation of beta4 integrins activates PKB/Akt and ERK1/2 by distinct pathways-relevance of the keratin filament. Biochim Biophys Acta. 2010;1803(8):940–950. doi: 10.1016/j.bbamcr.2010.03.009. [DOI] [PubMed] [Google Scholar]
- 126.Ohyama M, Zheng Y, Paus R, Stenn KS. The mesenchymal component of hair follicle neogenesis: background, methods and molecular characterization. Exp Dermatol. 2009;19(2):89–99. doi: 10.1111/j.1600-0625.2009.00935.x. [DOI] [PubMed] [Google Scholar]
- 127.Chueh SC, Lin SJ, Chen CC, Lei M, Wang LM, Widelitz R, Hughes MW, Jiang TX, Chuong CM. Therapeutic strategy for hair regeneration: hair cycle activation, niche environment modulation, wound-induced follicle neogenesis, and stem cell engineering. Expert Opin Biol Ther. 2013;13(3):377–391. doi: 10.1517/14712598.2013.739601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Kiso M, Tanaka S, Saba R, Matsuda S, Shimizu A, Ohyama M, Okano HJ, Shiroishi T, Okano H, Saga Y. The disruption of Sox21-mediated hair shaft cuticle differentiation causes cyclic alopecia in mice. Proc Natl Acad Sci USA. 2009;106(23):9292–9297. doi: 10.1073/pnas.0808324106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Driskell RR, Clavel C, Rendl M, Watt FM. Hair follicle dermal papilla cells at a glance. J Cell Sci. 2011;124(Pt 8):1179–1182. doi: 10.1242/jcs.082446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Xu M, Horrell J, Snitow M, Cui J, Gochnauer H, Syrett CM, Kallish S, Seykora JT, Liu F, Gaillard D, et al. WNT10A mutation causes ectodermal dysplasia by impairing progenitor cell proliferation and KLF4-mediated differentiation. Nat Commun. 2017;8:15397. doi: 10.1038/ncomms15397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Niemann C, Horsley V. Development and homeostasis of the sebaceous gland. Semin Cell Dev Biol. 2012;23(8):928–936. doi: 10.1016/j.semcdb.2012.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.McNairn AJ, Doucet Y, Demaude J, Brusadelli M, Gordon CB, Uribe-Rivera A, Lambert PF, Bouez C, Breton L, Guasch G. TGFbeta signaling regulates lipogenesis in human sebaceous glands cells. BMC Dermatol. 2013;13:2. doi: 10.1186/1471-5945-13-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Lu C, Fuchs E. Sweat gland progenitors in development, homeostasis, and wound repair. Cold Spring Harb Perspect Med. 2014;4(2):a015222. doi: 10.1101/cshperspect.a015222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Zeng B, Xiao X, Li S, Lu H, Lu J, Zhu L, Yu D, Zhao W: Eight mutations of three genes (EDA, EDAR, and WNT10A) identified in seven hypohidrotic ectodermal dysplasia patients. Genes. 2016 7(9); epub. doi: 10.3390/genes7090065. PMID: 27657131. [DOI] [PMC free article] [PubMed]
- 135.Cui CY, Kunisada M, Esibizione D, Douglass EG, Schlessinger D. Analysis of the temporal requirement for eda in hair and sweat gland development. J Invest Dermatol. 2009;129(4):984–993. doi: 10.1038/jid.2008.318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Adameyko I, Lallemend F, Aquino JB, Pereira JA, Topilko P, Muller T, Fritz N, Beljajeva A, Mochii M, Liste I, et al. Schwann cell precursors from nerve innervation are a cellular origin of melanocytes in skin. Cell. 2009;139(2):366–379. doi: 10.1016/j.cell.2009.07.049. [DOI] [PubMed] [Google Scholar]
- 137.Cichorek M, Wachulska M, Stasiewicz A, Tyminska A. Skin melanocytes: biology and development. Postepy Dermatol Alergol. 2013;30(1):30–41. doi: 10.5114/pdia.2013.33376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Aoki Y, Saint-Germain N, Gyda M, Magner-Fink E, Lee YH, Credidio C, Saint-Jeannet JP. Sox10 regulates the development of neural crest-derived melanocytes in Xenopus. Dev Biol. 2003;259(1):19–33. doi: 10.1016/S0012-1606(03)00161-1. [DOI] [PubMed] [Google Scholar]
- 139.Kaucka M, Adameyko I. Non-canonical functions of the peripheral nerve. Exp Cell Res. 2014;321(1):17–24. doi: 10.1016/j.yexcr.2013.10.004. [DOI] [PubMed] [Google Scholar]
- 140.Biedermann T, Klar AS, Bottcher-Haberzeth S, Schiestl C, Reichmann E, Meuli M. Tissue-engineered dermo-epidermal skin analogs exhibit de novo formation of a near natural neurovascular link 10 weeks after transplantation. Pediatr Surg Int. 2014;30(2):165–172. doi: 10.1007/s00383-013-3446-x. [DOI] [PubMed] [Google Scholar]
- 141.Francois M, Koopman P, Beltrame M. SoxF genes: key players in the development of the cardio-vascular system. Int J Biochem Cell Biol. 2010;42(3):445–448. doi: 10.1016/j.biocel.2009.08.017. [DOI] [PubMed] [Google Scholar]
- 142.Wat JJ, Wat MJ. Sox7 in vascular development: review, insights and potential mechanisms. Int J Dev Biol. 2014;58(1):1–8. doi: 10.1387/ijdb.130323mw. [DOI] [PubMed] [Google Scholar]
- 143.Bruderer M, Alini M, Stoddart MJ. Role of HOXA9 and VEZF1 in endothelial biology. J Vasc Res. 2013;50(4):265–278. doi: 10.1159/000353287. [DOI] [PubMed] [Google Scholar]
- 144.Janani C, Ranjitha Kumari BD. PPAR gamma gene - A review. Diabetes Metab Syndr. 2015;9(1):46–50. doi: 10.1016/j.dsx.2014.09.015. [DOI] [PubMed] [Google Scholar]
- 145.Kang S, Kong X, Rosen ED. Adipocyte-specific transgenic and knockout models. Methods Enzymol. 2014;537:1–16. doi: 10.1016/B978-0-12-411619-1.00001-X. [DOI] [PubMed] [Google Scholar]
- 146.Harms M, Seale P. Brown and beige fat: development, function and therapeutic potential. Nat Med. 2013;19(10):1252–1263. doi: 10.1038/nm.3361. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data and materials in this manuscript are referenced from previous publications and may be available from commercial suppliers or upon request from the reference laboratories.