

Abstract
Objective
Social and mobile media are playing a significant role in the digitization of health sectors globally. New technology provides an opportunity for stakeholders (i.e., patients and healthcare professionals) to engage with each other in virtual environments to discuss health-related issues. This study examines the role of social and mobile media in digitizing the health sector in Pakistan through MARHAM, the platform which is the subject of this case study.
Method
A thematic content analysis of MARHAM’s social media (Facebook group, Facebook page, and Twitter account) and mobile media application (“app” and website) were chosen for sampling. Some 6083 group posts, 1724 tweets and 1123 Facebook posts populated our sample.
Results
Analysis results indicate that MARHAM’s Facebook group most often fields patient inquiries. The most discussed health issues were: women’s health issues (43.23%), children’s diseases (16.63%), psychological issues (15.45%), dental issues (9.50%), skin problems (5.93%), others (5.04%), and obesity (4.19%). MARHAM’s Facebook page and Twitter account were mainly used for health education and awareness. Their mobile application and website were used by healthcare professionals and for patient registration.
Conclusion
The study’s results suggest that MARHAM is playing a significant role in the health sector of Pakistan, addressing primarily women and children’s issues through their Facebook group. Like many who have an online presence, MARHAM faces certain challenges, including the public’s low literacy rates and scant Internet access.
Keywords: MARHAM, digital health, Pakistan, women’s health issues, obesity, psychological issues, children’s diseases, new technology, mobile application, social media
Introduction
The role of social and new media in the health sector has emerged as a fascinating area of research for health communication scholars. Currently, efforts are being made to digitize the health sector by governments and corporate sectors globally. Issues related to health digitization are being explored in various forms, including problems around smartphone use in public health,1 online patient engagement,2 measurement of alcohol intoxication through digital devices,3 and “online substance-use,” effectiveness, and harmfulness.4 However, these studies are focused on developed nations such as the Netherlands, Switzerland, the United Kingdom, Australia, Canada, and the US. This is due to developing nations lagging in new technology infrastructure and adoption that significantly revolutionizes and affects the health sector. As such, low- and middle-income nations5 such as Pakistan and India face many challenges in providing quality and affordable health services to their citizens.
In Pakistan, health problems increase daily and treatment is scarce due to poor financial, economic, and environmental conditions.6 Poverty is the paramount reason for poor health conditions. Past scholars have linked health with poverty and have substantially demonstrated the strong causal link.7 To counter various diseases and health problems, citizens need to be educated, enjoy a strong economic situation, have access to the latest equipment, and most importantly, a consistent and established relationship with healthcare professionals.8 In Pakistan, individuals avoid using state-provided medical facilities because of their “poor quality” and “unreliability.”9 A survey of Pakistani government hospitals10 suggested that the behavior of hospital administration, the irresponsible attitudes of healthcare professionals (HCPs), and the illiteracy as well as poverty of citizens deters the Pakistani people from using state and public hospitals for treatment.
There are many challenges to improving the healthcare system in Pakistan. Key challenges include health sector corruption, a growing national population, and continued low literacy rates. According to the 2017 Transparency International11 report, Pakistan ranked 117/180 countries and its corruption score was 32/100 (0 means most corrupt and 100 means highly clean). Another report by Transparency International12 claimed that the health sector continues to be the third most corrupt state department in Pakistan, a ranking it first achieved in 2009, rising from seventh position.12 According to the United Nations International Children's Emergency Fund (UNICEF),13 Pakistan has a 78.8 per 1000 children under 5 years of age mortality rate. Meanwhile, the country’s education sector speaks volumes about its corruption and administrative issues. Pakistan is second worst in the world for school dropout, 5.1 million in 2010 – two-thirds of which were girls. In 2010, the national education budget was 2.3% of Pakistan’s GNP.14 The most recent census indicates that Pakistan has reached a record high population of 207.7 million, which makes it the fifth largest country in the world. An alarming example that illustrates the birth-rate explosion is a Pakistani male who had sired 36 children from three different wives by the age of 57, and was urged to take a fourth wife.15
Pakistan’s younger generation has embarked on a few initiatives in different sectors, including health and new media technology, to bring about societal change. In a very short time they have generated a number of thriving startups in the country.16
MARHAM: digital health initiative in Pakistan
MARHAM (a health sector startup in Pakistan) was established in January 2016 as a private initiative to digitize and facilitate the health industry of Pakistan. As the startup’s website states:
Together we can share the burden of those fighting a disease.
A month after its founding, MARHAM created its Facebook group, Facebook page, and Twitter handle. Its venues provide users with the ability to book appointments online, locate nearby MARHAM-registered doctors, or post their queries online to get second opinions from HCPs. The startup was the first of its kind in Pakistan, and was also among the top seven startups initiated in Pakistan in recent years. The Express Tribune noted the app’s seminal functionality: “connecting doctors and patients with the tap of a finger”.17 As compared to the old, traditional methods of booking appointments with HCPs, the mobile app provides opportunities for patients and HCPs to connect with each other through technology. “Find doctors with mobile app ‘Marham’ in Pakistan”18 is how one news outlet referenced the startup’s technological capabilities. Ahmed and Sheikh9 argued that people do not go to governmental hospitals because of administrative problems and poor health quality The app’s aim is to make sure healthcare access becomes easier than it has ever been.16 Today, the country is living in the age of the Internet and social media, and MARHAM is partially responsible for that change. The new mobile app aims to revolutionize the healthcare system in Pakistan.19
From a scholarly standpoint, there is a lack of research exploring the role of digitization in public sectors, particularly health. From a Pakistani context, no significant scientific study has been conducted to investigate the role of new media technology in catering to the needs of the people in the health sector. Identifying a substantial gap in established literature, we analyzed the role of the newly developed MARHAM application to facilitate online health communication across Pakistan. We analyzed MARHAM’s Facebook group, Facebook page, and Twitter handle, as well as its mobile application and website through a thematic content analysis.
Role of social and mobile media in health sector
While social media offer an opportunity for patients to obtain immediate and cost-effective advice from HCPs, it also poses many challenges to online health communication. Previous scholars have explored the relationship between patients and HCPs via social and mobile media. One study analyzed meta data about the use of social media to build relationships between HCPs and patients. They measured the effects of relationship-building on patients.8 Other scholars have suggested that the Government Digital Service model is being used in the transformation of the health sector by governments. Unfortunately the adopted method is not transparent.20 In addition, digital tools have become great sources for medical awareness and education for patients to share information about their health problems and connect with clinicians.21 As Roland suggested in her study, “the core benefit of social media in medicine, is always likely to remain an individual choice in the same way as you have a choice in how to write” (p.1).21 Mesko explored the importance of online searching for medical treatment content and time management tools.22 He claimed in his study that, back in 2008, it was time consuming to look at a blog related to medical education, but now social media has brought this capability to every cell phone and digital device.
Ventola investigated the use of purpose-built applications in the health field and their importance for HCPs.23 The study’s results argued that HCPs use mobile devices and software applications for five purposes: “administration, health record maintenance and access, communications and consulting, reference and information gathering, and medical education” (p.2). Ventola’s study was more focused on HCPs’ use of digital devices but it did not consider patients and HCPs as the target audience. Our study is audience-centered and identifies what users can receive from their use of digital devices in health communication. This study is audience-centered because social media users are the target audience of the MARHAM network and we analyzed audience health-related inquiries to examine the possible topics discussed in the MARHAM Facebook group. Mesko22 wanted to identify the latest trends in the field and interconnectivity through these digital devices. But the questions are: where are the audiences? What have HCPs done for patients through digital devices? Do HCPs try to share their expertise through their blog, Facebook pages, or Twitter handle? Are HCPs connected with patients through digital devices? These open questions have gone unanswered in many studies. Our study’s focus is the engagement of both sides: HCPs and patients. The interaction of both stakeholder groups through new media technology is significant and vital to explore. For example, Benetoli et al.24 conducted a focus group with 36 patients who used social media to access health-related information. Their study revealed that a patient’s use of social media was positively impacted by their relationship with HCPs: the HCPs’ interaction with patients through social media empowered the users.
Hawkins et al.25 argued that even though social media use is increasing, engagement with HCPs can be challenging for users. Since the inception of MARHAM’s accessibility to engage the community online with HCPs, their Facebook group has accumulated 112,479 people and 80,000 have “liked” their Facebook page. Their Twitter has very few followers because the users of this social platform are less trendy in Pakistan compared with Facebook. Individuals are not only sharing their problems on social media, they are also commenting and responding to those posts.26 For example, researchers conducted a survey in Italy about the sharing of antibiotic-related information on the Internet and social media. They conducted a cross-sectional study with a two-stage cluster sampling. The study concluded that the “Internet and social media are widely used for antibiotic-related information seeking in the Italian population” (p.7).26
Prasad27 noted that social media’s image is “the equivalent of a surgical scalpel—both are excellent tools but only if they are used appropriately and wisely” (p.4). He suggested the power of social media is important and different in raising one’s profile on the Internet. Scholars focused on regional studies for example26 conducted a survey on an Italian population; Benetoli et al.24 undertook their study with Australian participants; Saeed and Ibrahim10 discussed problems faced by people from government hospitals in Karachi; and Coathup et al.2 revealed online patient engagement in the UK.
An overview of Pakistan’s use of social and mobile media in health sector
The Punjab Information Technology Board (PITB) is the first and leading government institution working toward the digitalizing of Pakistan in terms of new media and technology. The institution
aims at not only modernizing the governance techniques through transparency induced methods but also at increasing the digital literacy of the citizens – among many other services. PITB is committed to effectively and efficiently provide [sic] IT services and infrastructure to the government and local and international businesses (p.1).28
According to the PITB website, several projects have been successfully completed and more continue, but there remains a long way to go. PITB renders its service to the health, law and order, education, agriculture, and transportation sectors. In the health sector, PITB is working on e-vaccinations, disease surveillance systems, a Dengue Activity Tracking System, a biometric attendance system for health facilities, monitoring systems for a polio campaign, a drug inspection and monitoring evaluation system, and a medicine procurement and drug testing laboratory automation program (p.2).28
The Dengue Activity Tracking System was successful in combating dengue fever across the province of Punjab during 2012–13. Rana29 stated that 252,935 cases of dengue fever were reported, 17,057 were confirmed by laboratory tests, and deaths totaled 219 in 2011. However, at the end of 2013 there were 9037 cases and only 2,164 confirmed by the laboratory with no reported deaths. This success story illustrates the effective use of new technology to control dengue fever in Pakistan.
Further, Pakistan’s telecommunication sector is growing daily. The Express Tribune described its technological changes in stating that Pakistan’s IT sector had gone through an historic move in the past few years and the country had taken the lead in adopting new technology.30 Another report by the Dawn illustrated the rise in social and mobile media usage in Pakistan, but noted that the Internet is still not common in the country.31
Hussain et al.32 investigated the impact of social and mobile media practices in Pakistan. They analyzed the issues faced by active Facebook users across Pakistan. Their survey was conducted in the four largest cities of Pakistan including Islamabad, Lahore, Quetta, and Peshawar. Questions were asked of the respondents about privacy, fake accounts requests, unwanted advertisements, and multimedia issues. A mixed-methods approach was applied to examine the problems faced by Facebook users. The results revealed that 30% to 55% of people complain, but 11% to 30% of users do not complain about the issues on Facebook.
Another example of adopting digital platforms regards the government of Khyber Pakhtunkhwa’s (KPK) health department actively using social media to inform and educate the provincial public. The KPK health department joined social media in 2016; currently, they have 19,400 Twitter followers, and their Facebook page has 62,538 likes and 63,050 followers. This effective social media use by the administration, shows that Pakistanis are adopting new technology in the health sector.33 The numbers are better than other provincial health departments who do not have a social media presence. The KPK health department website is user-friendly and colorful compared with other provincial health department websites.
Based on the presented research, we proposed the following research questions to address in this study:
RQ1: What are the most discussed health issues in MARHAM’s Facebook group?
RQ2: What are the key challenges and opportunities to the digital health process in Pakistan?
RQ3: How is MARHAM contributing to the digital health sector in Pakistan?
Method
Data collection, study design and sample
We answered the previous outlined questions with a mixed-methods approach. This exploratory study was the first ever conducted in Pakistan regarding the digitization of the health sector. First, we carried out a qualitative content analysis of social media posts of the MARHAM Facebook closed group, Facebook page, and Twitter tweets for possible categories. The unit of analysis was text posted on all social media platforms. We excluded photos and videos from the analysis to remain focused on our research questions. The unit of analysis is important for a study.34 Pakistan has 51% male, 48.76% female, and 0.24% transgender population.35 Men have higher literacy rates (69%) than women (45%) in Pakistan.36 According to the annual report of the Pakistan Telecommunication Authority,37 only 19% of people have access to the Internet in Pakistan. In the quantitative part, we used the descriptive statistics for the female and male sample. We then used statistical analysis to identify the percentages of the most discussed health issues in the MARHAM Facebook group.
We retrieved the data from social media (Facebook page posts and Twitter tweets). We used Python 2 to fetch Facebook posts and Tweepy library for Twitter tweets. For Facebook, we typed the user name of the page: @marham.pk. We used a Facebook token, which can be obtained from https://developers.facebook.com/tools/explorer. After applying this token, the system extracted the complete data from the Facebook page. The system extracted the data file into a CSV file. We converted the file into an Excel spreadsheet to analyze the frequencies of reactions, likes, shares, and comments. The total number of statuses was 1124 from February 2016 through February 2018. For Twitter, tweets were extracted through the Tweepy Application Programming Interface (API) with Python software to access the complete tweets data. The total number of tweets posted by the MARHAM Twitter handle from February 2016 until February 2018 was 1724. MARHAM’s Facebook group data was provided by the MARHAM organization. The Facebook group is a closed group and nobody can retrieve the posts without the organization’s authority. For the Facebook group data we used a six-month time frame to answer the research questions. We selected the six-month time frame to run from June–December 2017. The total number of posts during these six months was 6083. These 6083 posts in the MARHAM group were sufficient to answer the first research question and to give an overview of the most discussed health issues in the MARHAM Facebook group during this period.
We developed a comprehensive Excel spreadsheet to code the data. We analyzed the text manually through predefined categories. We used the categories for which MARHAM is providing a services to patients through its social and mobile media forums. We applied a deductive approach to analyzing the Facebook group text, the Facebook page, and Twitter tweets. MARHAM facilitates citizens in the following categories: gynecologist, Ear-Nose-Throat (ENT), gastroenterologist, orthopedic, neuro physician, general physician, cardiologist, psychiatrist, neurosurgeon, and pulmonologist.38 While keeping in mind these categories, we categorized the content of posts into seven broad types: 1) women’s health issues (pregnancy, periods, infertility, and breast feeding), 2) dental issues, 3) skin problems, 4) psychological problems (stress, depression, anxiety, looking for a psychologist, and tension), 5) obesity (weight loss/gain), 6) children’s diseases, and 7) others (cough, typhoid, diabetes, hair loss, diarrhea, malaria, HIV, fits, snoring, heart attack, cholera, hepatitis, dengue, stomach, kidney, ulcer, liver, blood pressure, and asthma). To develop these categories we used a qualitative approach; after identifying the main themes and topics we quantified the data and used the frequencies of the themes via the quantitative approach. Table 1 shows the derived categories from the text while looking at the specializations we used to answer our second research question.
Table 1.
Sample composition deducted from MARHAM’s Facebook group.
| Category | Example |
|---|---|
| Women’s Health Issues (pregnancy, periods, infertility, and breast feeding) | I am 33 weeks pregnant its my second pregnancy. From last few days, whenever I have any meal my heartbeat increases and I feel so dizzy that I cant stand. I took my blood sugar test after 1 and half hour of taking meal the value was 156 and at other event it was 133. My doctor suggested me few tests (fasting, 2hrP.P and HbA1C) and results came out normal (report attached in comments) so she asked me to stop taking all vitamins and calcium and take Nexum and Motilium for a week. Can anyone suggest good gynecologist for infertility purpose?? Along with hospital name n details??? |
| Dental Issues | Need dental expertise … Plz guide about clear path invisible aligners.. 1) R they really better than braces? 2) How does it cost to go for such aligners? 3) how much time does the whole procedure take? Thanku |
| Skin Problems | Need help Facing skin problem from more then 5 year,my skin is so sensitive that even i cant apply any moisturizer, having pimples breakouts dark spots, scars, uneven skin, visited many dermatologist but koi faida nae hota, plz suggest any dermatologist that u have experienced personally … |
| Psychological Problems (stress, depression, anxiety, looking for psychologist, and tension) | sir i have a problem related to depresiion i fell very guilt all the time dimenished ability to think or concentarte or indeviceness nearly every day and also recurrent thought of death i think that i shoolud do suside and also feeling of worthlessness Is there any way, to either completely or to some extent, reduce the tendency of anxiety and stress …?? |
| Obesity (weight loss/gain) | My sister is so much underweight and skinny. Have tried heavy diets, shakes everything..but weight bilkul nai barhta (not gaining weight). |
| Children’s Diseases | Salaam please post my query. My son has a genetic disorder called achondroplasia. A form of dwarfism. He gets his complete polio vaccinations accordingly from the hospital. But they keep coming home and insist. How can we stop them. My baby girl is 7 month old … her pee smells alot … dnt know what to do … Plz help me out Child of age of 2 and half years … He only urinate three times a day.. Like once in 6 hours. Is it ok or less?? |
| Others (cough, typhoid, diabetes, hair loss, diarrhea, malaria, HIV, fits, snoring, heart attack, cholera, hepatitis dengue, stomach, kidney, ulcer, liver, blood pressure, and asthma) | my sister has ulcers in mouth for the past three weeks. its realy painful, she is having difficulty in eating and even talking.she uses somogel, daktorin, kenalog and nistora drops but haven't been able to get rid of them kindly suggest something effective.need expert advice. thanks in advance! I am facing extreme hairfall … what could be the reason?… please suggest me something … Attaching picture in comments. Thank you. |
For the qualitative part of the analysis we used intercoder reliability according to the Holsti39 formula for nominal data. For example, reliability = 2M/N1 + N2; N1 represents one coder, N2 represents the second coder, while M represents the decisions made by both coders. The 86% intercoder reliability level was achieved, which was sufficient to investigate the coded data. Descriptive analysis was used to analyze the demographics of users. We used a quantitative approach to answer RQ1. For RQ2 we applied a deductive qualitative content analysis approach. According to the Elo and Kyngas40 the “deductive approach is useful if the general aim was to test a previous theory in a different situation” (p.107). To answer RQ3 we used an interpretive analysis of the patients’ inquiries and analyzed the available features of the mobile application.
MARHAM used two platforms, social and mobile media, to facilitate the patients and HCPs in Pakistan. Social media included their Facebook page, Facebook group, and Twitter account, while mobile media included a mobile application and website. Social and mobile media were divided into three main categories to make it easier for analysis, for example, 1) Facebook page and Twitter account, 2) mobile application and website, and 3) Facebook group. We did not include the Facebook group in Category 1 because the Facebook closed group is only used for queries, while the Facebook page and Twitter handle are used for health awareness and education. We categorized on the basis of their purpose. The website and application were being used for one main purpose, to register patients and HCPs or for appointments. The Facebook page and Twitter account were being used for health awareness and education, for example, how you can avoid developing a cough. The Facebook group was mainly used for patient inquiries and healthcare professional guidelines for them.
Results
Most discussed health issues in MARHAM Facebook in the group group
The 6083 group posts were analyzed to answer our first research question. We found that, as per our predefined disease categories, the most discussed health issues in the MARHAM Facebook closed group were women’s health issues (pregnancy, periods, infertility, and breast feeding; n = 2630, 43.23%), children’s diseases (n = 1012, 16.63%), psychological problems (stress, depression, anxiety, looking for psychologist, and tension; n = 940, 15.45%), dental issues (n = 578, 9.50%), skin problems (n = 361, 5.93%), others (cough, typhoid, diabetes, hair loss, diarrhea, malaria, HIV, fits, snoring, heart attack, cholera, hepatitis dengue, stomach, kidney, ulcer, liver, blood pressure, and asthma) (n = 307, 5.04%), and obesity (weight loss/gain) (n = 255, 4.19%). It is pertinent to mention that we considered children’s diseases under the age of 5 years. While posting questions people mentioned children’s ages so we coded those diseases under this category.
The most discussed health-related issues in the MARHAM Facebook group included women’s health issues, which constituted 43.23% of all issues discussed. Most of the queries were related to pregnancy, periods, infertility, and breast feeding. The second most discussed health problem was related to children’s diseases (63%). For example, untimely sleep patterns, baby’s crying, baby’s diet, and fever, etc. The least discussed health issues were skin problems (5.93%) and others, including cough, temperature, hepatitis, and snoring, etc. (5.04%). Figure 1 indicates the MARHAM Facebook group users’ gender. As Figure 1 depicts, the number of female users in the group is higher than male users. Most users fall under the 25–34 age category. The second highest number of users falls under the 18–24 age category. More than 60% of Pakistan’s population is considered to be youth.41
Figure 1.

MARHAM Facebook group users as per age and gender.
MARHAM has more than 1.5 million users across Pakistan and abroad on both social and mobile media. So far, 375,416 people have booked online appointments in 17 cities in Pakistan since January 2016. As per MARHAM’s Facebook group, they provide services to five patients per minute in Pakistan’s 17 cities. MARHAM has users in many countries. Figure 2 represents the top 10 countries where MARHAM has most users. Pakistan (n = 90,084), Kingdom of Saudi Arabia (n = 3899), India (n = 3272), United Arab Emirates (n = 2928), United Sates of America (n = 1667), United Kingdom (n = 1482), Australia (n = 833), Canada (n = 799), Bangladesh (n = 708), and Uganda (n = 563). These countries have the highest number of MARHAM online users. According to The Express Tribune the current statistics show that Saudi Arabia is the favorite destination of Pakistanis to find employment. Saudi Arabia has 2.6 million Pakistani workers, United Kingdom has 1.7 million Pakistanis, and United Arab Emirates holds the fourth place having most Pakistanis with 1.6 million and United States is fifth with 900,350 Pakistani job holders.42
Figure 2.
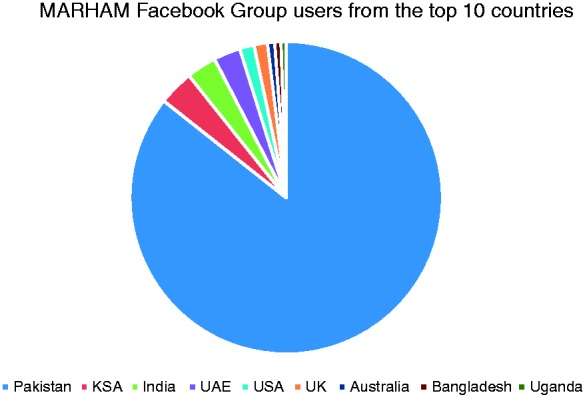
MARHAM online users in top 10 countries in the world.
Figure 3 illustrates the major cities: Lahore (n = 28,672), Karachi (n = 28,378), Islamabad (n = 6280), Multan (n = 1727), Faisalabad (n = 2293), Rawalpindi (n = 2730), Peshawar (n = 1858), and Jhelum (n = 2927) in Pakistan. There are five types of services MARHAM provides to its users, including a health forum, free medical advice, a second opinion about issues, a weight loss program, and blog through the MARHAM application. By 31st of December 2017, MARHAM had uploaded their video, which showed that 12,000 doctors had already registered through their online application. More than 20,000 authentic online cases were dealt with and consultations were provided, with more than 2900 reviews for guidance to others. This video was liked by 254 people and had 39 comments.
Figure 3.

MARHAM users in top eight cities of Pakistan.
Facebook page and Twitter account
Table 2 presents the total number of Facebook page posts: 1123 including four events, 559 photos, 23 statuses, and 111 videos. The 1724 Twitter tweets were examined to answer our first research question. MARHAM joined Twitter in February 2016. So far, the MARHAM Twitter account has not been very active. We measured the activeness of Twitter and Facebook with five tweets and posts per day. The Facebook page of the MARHAM has more than 79,000 likes and 80,000 followers. MARHAM is addressing health issues via social media networks. Within two years, MARHAM got immediate response through its online presence, but the interactivity with its followers is very low. The average share per post is only 2.70 and 2.74 comments, which illustrates that their Facebook page is not source of discussion for the patients or HCPs. The Facebook page and Twitter account are mainly being used for awareness-raising purposes. The health blog posts are shared on these platforms.
Table 2.
MARHAM Facebook page statistics and users’ interaction with posts.
| Total number of “Likes” | 79,452 |
| Followers | 80,154 |
| Posts | 1124 |
| Average reactions per post | 76.7 |
| Average “Likes” per posts | 74.5 |
| Average shares per post | 2.70 |
| Average comments per post | 2.74 |
| Mission of the Facebook page | MARHAM aims to be the primary digital healthcare solution for the people of Pakistan. It has been created with an idea to address the medical and health issues posed to patients and doctors. You can post health-related questions on MARHAM’s forum and get instant help about cures and the right doctors. |
| Administrators and moderators of the page | 16 (3 administrators, 13 moderator: 8 female, 8 male) |
| Total photos with posts | 558 (49.7%) |
| Total links with posts | 111 (9.8%) |
| Total videos with Posts | 453 (40.3%) |
MARHAM has more followers than the provincial health departments of Pakistan, but reactions showed low interactivity online. There could be many factors underlying this, however, despite having more than 80,000 followers, there was not even 1% of interactivity found from stakeholders (patients and HCPs). There was no difference with their Twitter handle; Twitter even had a lower rate of reactions and interactivity, for example, an average of 2.47 tweets per day and no replies, likes, or retweets. With 457 followers on Twitter, there was a reaction average of zero. The Internet World Stats43 showed that there were 32 million Facebook users in Pakistan. On the other hand, Twitter has 3.1 million users in Pakistan.44
We analyzed the Facebook posts and Twitter tweets through correlation analysis and found there was 99% similarity in the Facebook posts’ and Twitter tweets’ content.
Table 3 illustrates that the MARHAM Twitter is being used for health-related awareness and education through tweets. They only shared blog posts on their Twitter account to raise awareness among patients about health issues on Twitter. For example, one post boasts the headline, “3 Grim Outcomes of Excessive Eating”. Therefore they are not only providing services but also educating through social networks. Most of the tweets and Facebook page posts are shared from the website with click button to engage readers through social networking sites. As we show in tables 2 and 3, there is not much user engagement on either social networks, but the Facebook group is very active in answering users’ questions.
Table 3.
MARHAM Twitter account statistics and user engagement.
| No. of Tweets | User name | Followers | Following | Tweets average per day | Joining date |
|---|---|---|---|---|---|
| 1724 | @marhampk | 457 | 279 | 2.4 | February 2016 |
MARHAM mobile application and official website
MARHAM’s mobile app and website are used for appointment bookings, and patient and healthcare professional registration. According to the latest statistics, more than 12,000 HCPs have registered with MARHAM. However, 1215 HCPs are available through their extended profiles, while others do not have complete profiles on the MARHAM mobile app and website. Male HCPs number 827 (68%) and female HCPs total 388 (32%). This ratio is only for those who have extended profiles on MARHAM’s website and mobile app. Table 4 illustrates healthcare professional’s specializations across 10 health areas. Apart from the role of gynecologist, there are fewer female HCPs in every field compared with male, which strongly associates with the low literacy rates found among women in Pakistan. According to the latest data provided by MARHAM, most of the HCPs prefer to register with MARHAM via their website rather than through the mobile app. Similarly, patients feel more comfortable using the website compared with the mobile app.
Table 4.
Healthcare professional’s specializations and gender distribution registered through MARHAM’s website and mobile application.
| No. | Healthcare professionals’ specializations | Male | Female | Total |
|---|---|---|---|---|
| 1 | ENT | 36 | 2 | 38 |
| 2 | Gynecologists | 4 | 74 | 78 |
| 3 | Gastroenterologists | 36 | 2 | 38 |
| 4 | Orthopedics | 41 | 5 | 46 |
| 5 | Neuro physicians | 11 | 1 | 12 |
| 6 | General physicians | 125 | 46 | 171 |
| 7 | Cardiologists | 24 | 4 | 28 |
| 8 | Psychiatrists | 29 | 7 | 36 |
| 9 | Neurosurgeons | 11 | 1 | 12 |
| 10 | Pulmonologists | 29 | 7 | 36 |
| Total | 346 | 149 | 495 |
Table 4 denotes the HCPs (n = 495) who are dealing with selected categories and MARHAM’s main services related to these diseases. There are fewer females in these categories compared with male HCPs (male: n = 346, 70%; female: n = 149, 30%). The large number of general physicians are registered under the selected categories (n = 125, 25%) male and (n = 46, 09%) female. The least number are registered as neuro physicians/neuro surgeons: male (n = 11), female (n = 1). The organization launched a mobile app supported by android and IOS systems in January 2016. The mobile offers a diversity of features to patients and HCPs, including the options to post a question, book online healthcare professional appointments, and read about health issues. Table 5 shows the statistics of the mobile app and its ranking and features.
Table 5.
MARHAM Google Play Store update on 15 March 2018.
| Official name | Supports | Installs | Reviews | Features | Ranking |
|---|---|---|---|---|---|
| MARHAM | Android/IOS | 10,00+ | 492 | Find a doctor, Find a hospital, Health forum (post your problem), Book online appointments, Free service (Get free medical services), Get second opinion (Get second opinion of a doctor), Weight loss program and Health blog (read health blog) | 4.6/5 |
MARHAM: prospects and challenges
MARHAM has played a significant role in the online health communication process in Pakistan since January 2016. The startup is enabling deprived Pakistani communities to ask their questions directly to HCPs through the MARHAM Facebook group and mobile app. They are providing opportunities for the people of Pakistan who cannot afford expensive healthcare to access a range of professionals 24/7. However, as Pakistan is a developing country, MARHAM faces several challenges in persuading individuals to adopt a digital culture of health-related issues. Pakistani citizens do not tend to be “tech-savvy” due to the low literacy rate and because one-third of the population lives below the poverty line. Almost 60 million people live below the poverty line in Pakistan: they earn less than US $30.00 per month.45 The main challenge for many Pakistanis is with HCPs who charge thousands of Pakistani rupee in fees for a checkup. Certainly in this way they are being treated well and provided with quality healthcare, but the majority of them cannot afford it. Meanwhile, MARHAM is represents an opening for the Pakistani community to consult professionals about their problems through social and mobile media.
Currently, MARHAM is expanding into the small cities of Pakistan, but there is long way to go. For example, there were no users from Kashmir region, Gilgit-Baltistan and tribal belt, and most parts of Baluchistan, KPK, and Sindh province, which are less progressive regions than Punjab province. The second challenge is that more than 60% of the population of Pakistan lives in rural areas. The less than 40% of people living in urban areas can book appointments, ask questions online, and consult about their health problems anytime, but what about the 60% who lives in rural areas, people who do not have access to the Internet? What about people who do not have HCPs in their local areas? Simply focusing on urban areas and particular audiences does not seem to be practical for keeping in view the large number of people living in rural areas of the country.
Another challenge relates to dealing with fake doctors. Yes, MARHAM has a mechanism to deal with this, but this problem necessitates a comprehensive plan and strategy at governmental and corporate level to address this phenomenon. They do have a verification system via the Pakistan Medical Association, however, this mechanism is ineffective for the ongoing debate about fake doctors. There is a need to address not only fake clinicians and HCPs but also bogus clinics. For example: fake HCPs have worked in government and well-reputed hospitals for many months: Dawn reported, “Fake neurosurgeon worked at Lahore's Services Hospital for eight months”.46 The problem of fake degrees that occurs in every discipline including the medical fields also represents a challenge at state and corporate levels. The Punjab Healthcare Commission has closed almost 6000 bogus treatment centers since 2015. The closed establishments included hospitals, laboratories, and homeopathic clinics that were involved in malpractices across the Punjab province.47 Furthermore, the ratio of people to doctors in Pakistan also fails to meet international healthcare standards.
Discussion
The journey into digital health processes does not have a long history in Pakistan. The MARHAM initiative began two years ago and subsequently launched as a facilitator of an online health sector. The impact of the initiative has proved tremendous in terms of cases dealt with, the number of online bookings, and registration of the 12,000 HCPs through the web and mobile app. The organization has increased the number of followers on social media and group members able to discuss their health-related problems with the tap of finger. MARHAM’s social media statistics will change in future studies because numbers are continuously growing. Facebook’s response to patient inquiries is very immediate and they have 16 group moderators and administrators to respond rapidly.
On the other hand, the following limitations must be considered when interpreting the findings presented. First, the sample for this study did not turn out to be ideal for answering the research questions. The selected MARHAM’s Facebook group has a huge number of postings whereas its Facebook page and Twitter account has less activity. From the Facebook page and Twitter account the whole data were used as sample; for the Facebook group we used only time frames (six months). The Facebook page had 1123 posts, the Facebook group had 6083 posts and Twitter had 1724 tweets in two years. As a result, the sample for this study was not sufficiently balanced – too many MARHAM Facebook group posts and fewer Facebook page postings and Twitter tweets – and contained insufficient interaction on Twitter and the Facebook page. Twitter is less popular in developing countries because of its features. Twitter is considered a network for professionals, therefore MARHAM does not have real engagement with the general population though Twitter. The low interaction of users on Twitter indicates that people are frequent users of mobile application and Facebook group. Twitter does not provide feature like groups, as on Facebook, this is one of the reasons why there is low interactivity among users and HCPs from the MARHAM network.
MARHAM users not only reside in Pakistan but in the Gulf States, and western countries including the United States, the UK, and Australia, where millions of Pakistani have lived for several decades. The use of MARHAM social and mobile media suggest that the Pakistani diaspora is also connected though new technology. The borderless technology is linking people from a local to a global level. Appadurai48 suggests that the “technoscape” has played a significant role in connecting communities across the world. There are millions of Pakistanis living abroad and the new media and technology has shrunk the distances making communication easier than before.
Due to limited resources, only a specific time frame of the MARHAM Facebook group posts was considered for analysis. We are generalizing our six-month results over other missing 1.5 years regarding the most discussed topics. Our study was regionally focused and has practical implications for the government of Pakistan to pay attention to over the emerging trends in digital health. For instance, provincial health departments should use social and mobile media to facilitate online health communication. State and province websites should be updated and user-friendly. Furthermore, the MARHAM initiative should be encouraged and the government should take steps to provide quality healthcare facilities for its citizens. The Express Tribune revealed that the government of Pakistan was spending US $9.3 per person, far less than the international standard, which is $60.00. The report claimed that 8–9 million pepole were affected by Hepatitus-C, 0.6 million people had tuberculosis, and almost 410,000 people were affected every year. The annual detected cases of malaria number 500,000.49
The existing literature in digital health suggests that new media and technology are playing an important role in informing and educating people regarding health issues. Similarly, this study’s findings argue that the Pakistani community has an opportinuty to adopt the new technology in the health sector. MARHAM is the first startup in Pakistan’s health sector, facilitating the process of online bookings, enabling people to find nearby HCPs and hospitals in all major cities of Paksitan. Online health communication between patients and HCPs is not common in Pakistan. It is worth mentioning here that Pakistani society is a conservative society where women have many problems in terms of education especially, and adult education, which is related to their health problems, however, the MARHAM platform provides a facility for all people regardless of gender, race, or ethinicty to ask questions in Facebook group or through the mobile application. Although digital health and health communication literature claims that it is normal practice in developed countries to communicate with HCPs, this is not always the case in developing and conservative societies such as Pakistan.
Conclusion
Although this study has its limitations, it nonetheless contributes insight to the growing field of the digitization of the health sector. This study focused on the role of social and mobile media in health communication in Pakistan. The present study’s data revealed possible effects related to topics posted by the Facebook group and the number of discussed health-related issues based on healthcare engagement and user questions. The study’s results concluded that MARHAM is playing an important role in digitizing the health sector. There is a long way to go to make this kind of projects and initiatives successful and adoptable for citizens. Until now, MARHAM’s focus has only been on urban areas because there is less Internet usage in rural areas compared with urban. Secondly, HCPs prefer to stay in urban areas and rural populations have to visit nearby cities for regular and emergency medical checkups. New technology should be a mechanism to facilitate the rural population’s access to healthcare.
The results suggest that the occurrence of online health communication effects also depends on how different HCPs and patients using social and mobile media engage with each other. Finally, future studies might employ mixed-methods approaches to not only analyze published content, but also interview HCPs and conduct surveys with social media users and MARHAM users to gain insight into the impact of the MARHAM initiative on HCPs and patients. MARHAM is the first initiative in Pakistan to facilitate online health communication through new technology. There is need for such initiatives at governmental level to digitize the health sector ensuring it becomes accessible to its citizens on mass. Overall, MARHAM is an opportunity for a deprived Pakistani community to adopt a new technology within the health sector.
Acknowledgements
The authors would like to thank the MARHAM administration for providing the data used in this study.
Contributorship
MI undertook the planning, execution, and data analysis of this study. MI prepared the first draft of the manuscript. AI read and approved the final version submitted. AI added the final touches to the manuscript.
Conflict of interests
MI and AI certify that they have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
Ethical approval
No ethics approval is required for this study as it did not involve clinical trials on humans or animals and it follows the principles of the Declaration of ICMJE.
Funding
This research study was not funded by any organization, entity or individual and was conducted in Germany and Russia through online resources in Pakistan.
Guarantor
MI
Peer review
This manuscript was reviewed by two individuals who have chosen to remain anonymous.
References
- 1.Velthoven MHV, Powell J, Powell G. Problematic smartphone use: digital approaches to an emerging public health problem. Digit Health 2018; 4: 2055207618759167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Coathup V, Finlay T, Teare HJ, et al. Making the most of the waiting room: electronic patient engagement, a mixed methods study. Digit Health 2018; 4: 2055207617751304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Riordan BC, Scarf D, Moradi S, et al. The accuracy and promise of personal breathalysers for research: steps toward a cost-effective reliable measure of alcohol intoxication? Digit Health 2017; 3: 2055207617746752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Milward J, Drummond C, Fincham-Campbell S, et al. What makes online substance-use interventions engaging? A systematic review and narrative synthesis. Digit Health 2018; 4: 2055207617743354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lewis T, Synowiec C, Lagomarsino G, et al. E-health in low- and middle-income countries: findings from the Center for Health Market Innovations. Bull World Health Org 2012; 90: 332–340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Amir M. Health issues. Pakistan Today, 26 April 2017.
- 7.Hafeez M. Poverty and poor health in Pakistan: exploring the effects of privatizing healthcare. Harvard Int Rev 2014; 35: 4. [Google Scholar]
- 8.Smailhodzic E, Hooijsma W, Boonstra A, et al. Social media use in healthcare: a systematic review of effects on patients and on their relationship with healthcare professionals. BMC Health Serv Res 2016; 16: 442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ahmed J, Shaikh BT. An all time low budget for healthcare in Pakistan. J Coll Physicians Surg Pak 2008; 18: 388–391. [PubMed] [Google Scholar]
- 10.Saeed A, Ibrahim H. Reasons for the problems faced by patients in government hospitals: results of a survey in a government hospital in Karachi, Pakistan. J Pak Med Assoc 2005; 55: 45–47. [PubMed] [Google Scholar]
- 11.Transparency International. Corruption Perceptions Index 2017, Berlin: Transparency International, 2017. [Google Scholar]
- 12.Transparency International. National Corruption Perception Survey TI Pakistan 2009, Karachi: Transparency International, 2009. [Google Scholar]
- 13.United Nations International Children’s Emergency Fund. Pakistan, New York City: United Nations International Children's Emergency Fund, 2015. [Google Scholar]
- 14.The United Nations Educational, Scientific and Cultural Organization. Education for All Global Monitoring Report, fact sheet; education in Pakistan, New York City: United Nations Educational, Scientific and Cultural Organization, 2012. [Google Scholar]
- 15.Constable P. Pakistan birth rate a ‘disaster in the making’ as population passes 207 million. The Independent, 10 September 2017.
- 16.Khalid H. 7 lesser-known Pakistani start-ups that can make your life so much more convenient. Dawn, 9 June 2017.
- 17.Kazi M. Marham – connecting doctors and patients with the tap of a finger. The Express Tribune, 5 June 2017.
- 18.Monitoring Report. Find doctors with mobile app ‘Marham’ in Pakistan. The News, 3 October 2016.
- 19.Jan Z. New app aims to revolutionise healthcare, finding a doctor online. The Nation, 18 June 2016.
- 20.Benjamin K, Potts HW. Digital transformation in government: lessons for digital health? Digit Health 2018; 4: 2055207618759168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Roland D. Social media and the digital health arena. Future Hosp J 2017; 4: 184–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mesko B. Online medical content curation and personal time management with Web 2.0: an exciting era. Cell Ther Transplant 2011; 2: 1–4. [Google Scholar]
- 23.Ventola CL. Mobile devices and apps for health care professionals: uses and benefits. Pharm Ther 2014; 39: 356–364. [PMC free article] [PubMed] [Google Scholar]
- 24.Benetoli A, Chen TF, Aslani P. How patients’ use of social media impacts their interactions with healthcare professionals. Patient Educ Couns 2018; 101: 439–444. [DOI] [PubMed] [Google Scholar]
- 25.Hawkins CM, Delao AJ, Hung C. Social media and the patient experience. J Am Coll Radiol 2016; 13: 1615–1621. [DOI] [PubMed] [Google Scholar]
- 26.Zucco R, Lvano F, Anfosso R, et al. Internet and social media use for antibiotic-related information seeking: findings from a survey among adult population in Italy. Int J of Med Info 2018; 111: 131–139. [DOI] [PubMed] [Google Scholar]
- 27.Prasad B. Social media, health care, and social networking. Gastrointest Endosc 2013; 77: 492–495. [DOI] [PubMed] [Google Scholar]
- 28.Punjab Information Technology Board. https://www.pitb.gov.pk/about (2018, accessed March 10 2018).
- 29.Rana S. Dengue fever: surveillance, forecasting and response in Pakistan. In: APAN 37th conference on dengue fever; let’s stop it. APAN, Bandung, Indonesia.
- 30.Zaheer F. Pakistan takes lead in adopting technology. The Express Tribune. 24 October 2010. [Google Scholar]
- 31.Web Desk. The rise of mobile and social media use in Pakistan. Dawn. 10 April 2015. [Google Scholar]
- 32.Hussain Z, Bhutto ZA, Rai G, et al. Statistical analysis of network based issues and their impact on social computing practices in Pakistan. J Comput Commun 2016; 4: 23. [Google Scholar]
- 33.KPK Health Department. Online referencing, http://www.healthkp.gov.pk/ (2018, accessed 10 March 2018).
- 34.Elo S, Kääriäinen M, Kanste O, et al. Qualitative content analysis: a focus on trustworthiness. S Open 2014. Feb 5; 4: 2158244014522633. [Google Scholar]
- 35.Pakistan Bureau of Statistics. Province wise provisional results of census – 2017, Islamabad: Pakistan Bureau of Statistics, 2017. [Google Scholar]
- 36.Zaman F. Female literacy rate. The Nation, 5 August 2016.
- 37.Pakistan Telecommunication Authority. Online referencing,https://pta.gov.pk/ (2017, accessed 5 March 2018).
- 38.MARHAM official website. Online refrencing,https://www.marham.pk/ (2018, accessed 2 March 2018).
- 39.Holsti OR. Content analysis for the social sciences and humanities, Reading, MA: Addison-Wesley, 1969. [Google Scholar]
- 40.Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs 2008; 62: 107–115. [DOI] [PubMed] [Google Scholar]
- 41.Rizvi O. The youth in Pakistan. Daily Times, 23 January 2017.
- 42.Tanoli Q. 2.43 million Pakistanis working in Europe. The Express Tribune, 24 April 2017.
- 43.Internet World Stats. Asia internet use, population data and Facebook statistics, https://www.internetworldstats.com/stats3.htm (2017, accessed 11 March 2018).
- 44.Ibrahim S. Pakistan social media users crossed 44 million in 2016–2017. Phone World, 14 February 2017.
- 45.Khan ZM. New poverty line makes a third of Pakistanis poor. Dawn, 8 April 2016.
- 46.Mahmood A. Fake neurosurgeon worked at Lahore's Services Hospital for eight months. Dawn, 15 April 2016.
- 47.Staff Report. PHC closed down 6,000 quack clinics since July 2015. The Express Tribune, 9 November 2017.
- 48.Appadurai A. Disjuncture and difference in the global cultural economy. Theo, Cult & Soc 1990; 7: 295–310. [Google Scholar]
- 49.Wasif S. Unhealthy revelations: Pakistan plagued by dismal healthcare system. The Express Tribune. 18 May 2013.