

Abstract
Aim:
Limited data regarding stroke subtypes exist from South Asian countries. The aim of the study was to determine the pattern of ischemic stroke subtypes and their associated risk factors, in a 10-year long hospital-based registry in the South Indian city of Hyderabad.
Materials and Methods:
The Hyderabad stroke registry systematically collected clinical, radiological, and laboratory data of fully investigated consecutive stroke patients and studied pattern of ischemic stroke subtypes and their risk factor association.
Results:
The cohort comprised of 2642 patients: 2072 (78.4%) were ischemic and 570 (21.6%) were hemorrhagic strokes. In the ischemic stroke cohort, the mean age was 54.1 years and 1622 (78.3%) were men. The most common ischemic stroke subtype was large artery atherosclerosis (LAA) comprising 37.6% (n = 779), followed by small vessel occlusion comprising 19.9% (n = 413) and cardioembolism 11% (n = 228). Stroke of other determined etiologies constituted 4.2% (n = 86) and stroke of undetermined etiology was observed in 27.3%. Among patients with LAA, 610 (78.3%) patients had intracranial and 169 (21.7%) had extracranial disease as the underlying mechanism. Risk factor profile demonstrated that hyperlipidemia was significantly associated with LAA and ischemic heart disease with cardioembolic strokes.
Conclusions:
The study reveals a distinct pattern of ischemic stroke subtypes in the Indian context that has overlapping features of registries from West and East Asian countries. Both large artery and small vessel diseases are substantially represented with a predominance of intracranial atherosclerosis. The study results have significant implications for developing preventive and management strategies for stroke care and research in India.
Keywords: India, intracranial atherosclerosis, South Asia, stroke subtypes
INTRODUCTION
Ischemic stroke is quite heterogeneous in its pathophysiological mechanisms, and this forms the basis of stroke subtyping. The importance of subtyping is highlighted by the fact that current guidelines for stroke prevention and treatment are subtype specific.[1,2] Recently, genetic mechanisms underlying stroke have also been found to be subtype specific.[3] Interestingly, data from stroke registries have demonstrated regional variability in the pattern of stroke subtypes and their risk factor profiles.[4,5,6,7,8,9,10] However, majority of these studies have been conducted in North America, Europe, the UK, and Australia. Stroke studies from Asia report patterns mainly from East Asia, and limited data exist regarding stroke subtypes from countries in South Asia.[11] Knowledge about the regional pattern of stroke subtype will help to develop population-specific screening tools for instituting appropriate preventive and therapeutic measures. The present study has been conducted in a university hospital in the South Indian city of Hyderabad, over a period of 10 years and is aimed to investigate the pattern of ischemic stroke subtypes and their associated risk factors.
Aim of the study
The study aimed to investigate the pattern of ischemic stroke subtypes and their associated risk factors in a stroke registry based in the South Indian city of Hyderabad, over a period of 10 years.
MATERIALS AND METHODS
Consecutive stroke patients evaluated in the stroke Registry of Nizam's Institute of Medical Sciences, a university hospital in Hyderabad, India, during the period 2001–2011 were prospectively included in this study. The Hyderabad stroke registry was designed to comprehensively evaluate and record clinical, radiological, and laboratory data of consecutive acute stroke patients with a structured protocol.[12] Patients were uniformly investigated to determine the underlying mechanism of stroke with computed tomography scan or magnetic resonance imaging (MRI) with angiogram, carotid duplex examination, electrocardiography, two-dimensional (2D)-transthoracic echocardiography, and basic laboratory investigations. Of the 2072 ischemic stroke patients, 85.8% (n = 1779) underwent MRI, 73% (n = 1512) were evaluated with a neck vessel Doppler, and 79.8% (n = 1654) underwent a 2D echocardiogram. Among patients in whom the underlying mechanism was not identified, one or more of additional investigations including 24 h electrocardiography (Holter) monitoring, transesophageal echocardiography, digital subtraction cerebral angiography, and hematological investigations for systemic disorders were done.
All patients with ischemic stroke were subtyped according to the Trial of ORG 10172 in acute stroke treatment (TOAST) classification system.[13] Large artery atherosclerosis (LAA) (intracranial or extracranial LAA), cardioembolism (CE), small vessel occlusion (SVO) or lacunar stroke, stroke of other determined etiologies, and stroke of undetermined etiology. Strokes of undetermined etiology were diagnosed in participants with more than one underlying mechanism, in patients without identifiable cause despite extensive evaluation, and in those with incomplete evaluation. Patients were classified into stroke subtypes based on the review of clinical records and investigations by neurologists trained to apply the TOAST classification system. At least two neurologists reviewed data of an individual patient to arrive at the mechanism of stroke subtype. The study was approved by the Institutional Ethical Committee of Nizam's Institute of Medical Sciences.
Statistical analysis
Descriptive statistics for categorical variables were performed by computing the frequencies in each category. For quantitative variables, approximate normality of the distribution was assessed. Variables following normal distribution were summarized by mean and standard deviation. The association between stroke subtypes and the risk factors was determined by analysis of variance test. Multinomial logistic regression was performed to identify demographic and clinical risk factors associated with LAA (Extracranial LAA and Intracranial LAA), SVO, and CE. All tests were two tailed; P <0.05 was considered statistically significant. Statistical analysis was carried out using IBM SPSS, Version 20 (IBM SPSS Statistics, Somers NY, USA).
RESULTS
During the study period, 2642 consecutive patients with stroke were enrolled in the stroke registry, and among them, 2072 (78.4%) were ischemic and 570 (21.6%) were hemorrhagic strokes. The ischemic cohort consisted of 1622 men (78.3%) and the mean age was 54.1 years. The most common ischemic stroke subtype was LAA (37.6% [n = 779]), followed by SVO (19.9% [n = 413]) and CE (11% [n = 228]). Stroke of other determined etiologies constituted 4.2% (n = 86) of ischemic strokes, and stroke of undetermined etiology was observed in 27.3% (n = 566). Among the 779 patients in whom stroke was attributable to LAA, 610 (78.3%) had intracranial LAA and 169 (21.7%) had extracranial LAA. The most commonly detected causes of stroke in the group of patients with other determined etiologies were moyamoya disease (7%), vasculitis (7%), protein C, S and antithrombin-III deficiency (7.2%), antiphospholipid antibody syndrome (5.8%), HIV infection (2.3%), and others (5.6%).
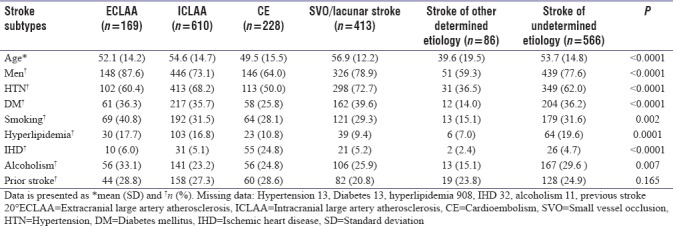
Table 1 shows patient characteristics and prevalence of risk factors across subtypes of ischemic stroke. Significant differences noted on post hoc analysis were older age of patients with SVO, stronger association of hypertension (HTN) with SVO compared to other subtypes, higher prevalence of diabetes mellitus (DM) with SVO and LAA, higher prevalence of hyperlipidemia with LAA, and more frequent association of ischemic heart disease (IHD) with cardioembolic stroke, compared to other subtypes. Male gender, smoking, and chronic alcoholism were more common with extracranial LAA. Prior stroke was more frequently encountered with CE and LAA compared to SVO. Strokes of other determined etiologies were less commonly associated with all of these risk factors.
Table 1.
Demographic and risk factors profile of various ischemic stroke subtypes
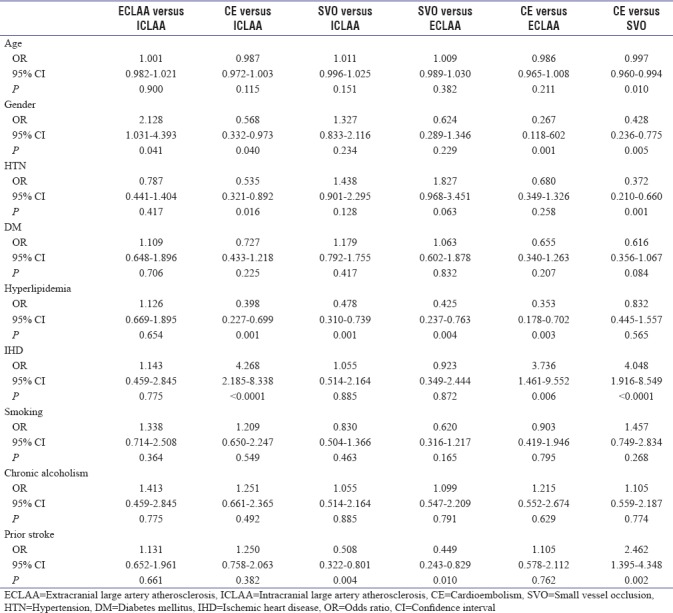
In multivariate model analysis of risk factor differences between LAA, SVO, and CE, significant findings were demonstrated [Table 2]. Hyperlipidemia was strongly associated with intracranial and extracranial LAA compared to SVO and CE, and IHD was most frequently associated with CE compared to LAA and SVO. Prior stroke was associated more often with LAA and CE compared to SVO.
Table 2.
Risk factors associated with ischemic stroke subtypes: Multinomial logistic regression
DISCUSSION
Subtyping ischemic stroke is crucial for planning proper treatment and prevention strategies. Stroke recurrence and mortality differ among subtypes, and importantly, treatment strategies are specific to underlying mechanisms.[1,2] Furthermore, epidemiological and genetic studies in stroke require accurate phenotyping and indicate genetic associations specific to subtype.[3] There are, however, significant racial and ethnic differences in patterns of ischemic stroke subtypes. While patterns of stroke mechanisms are fairly well established in Western and East Asian countries, evidence from developing South Asian countries like India is still limited. The present 10-year long study from India is the largest single-center prospective study so far of comprehensively evaluated acute ischemic stroke patients from South Asia. The characteristic feature was that the most common stroke subtype was intracranial LAA, accounting for 29.4% of ischemic strokes. Risk factor profile demonstrated different patterns of associations with subtypes: hyperlipidemia was strongly associated with LAA and IHD with cardioembolic strokes.
We compared patterns of ischemic stroke subtypes in India with the West and East Asia [Table 3].[4,6,7,11,12,14,15,16,17,18] A recent study from India reported ischemic stroke subtypes in a hospital population across different centers, and while the proportion of LAA was the highest similar to our study, the proportion of extracranial and intracranial large artery disease was not reported.[11] Extracranial LAA dominated composition of LAA in Western countries,[19,20,21] but intracranial LAA accounted for nearly 80% of LAA in the Hyderabad registry, consistent with reports from other East and South Asian countries,[7,22,23] thereby confirming that intracranial LAA is the prominent subtype of LAA across Asia. In contrast, SVO or lacunar stroke contributed to 19.9% of all ischemic strokes, and this proportion is less than reported from China (42.2%),[15] Taiwan (32.7%),[16] Korea (25.4%),[7] and Japan (34.2%)[17] while more comparable to data from the West (range: 15%–23%).[4,6,9,10,24,25]
Table 3.
Comparison in ischemic stroke subtypes between registries from different countries
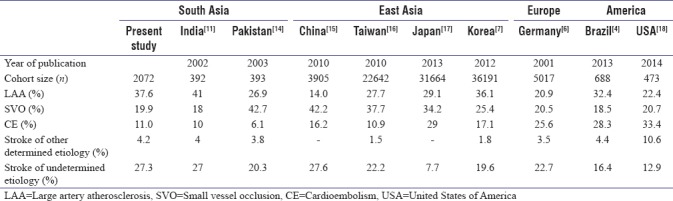
Cardioembolic strokes accounted for 11% of ischemic strokes in our registry. While this is similar to majority of hospital-based studies from Asia,[8,14,16] registries from North America, the UK, and Europe report a much higher frequency, and in fact, CE is considered to be one of the most common causes of stroke in the West.[6,18,9,24] It is, however, possible that some cases of CE may have remained undetected in our cohort, explaining the larger proportion of cardioembolic strokes reported in a recent study from India.[11] Stroke of undetermined etiology was observed in 27.3%, consistent with earlier studies.[4,6,7,8] It is now recognized that a significant proportion of strokes of undetermined etiology are cardioembolic in origin and the source may be detected by more extensive investigations including long-term electrocardiogram monitoring and transesophageal echocardiography.[26]
We observed that HTN, DM, and hyperlipidemia were the common risk factors across all ischemic stroke subtypes. On univariate analysis, the strongest association of HTN was with SVO, and DM correlated with both SVO and LAA consistent with prevailing reports.[4,5,6,8,9] Similarly, smoking and chronic alcoholism were more often associated with extracranial LAA.[5,6] On multivariate analysis, significant findings that emerged were the association of hyperlipidemia with LAA and IHD with CE.[27] Patients with LAA and CE also had a higher frequency of a prior stroke compared to SVO. This finding is supported by previous studies[28] and emphasizes the need to accurately identify these two-stroke mechanisms, to prevent recurrence in high-risk patients.
The strengths of the study are that, to the best of our knowledge, this is the largest single-center prospective study of comprehensively evaluated patients with acute ischemic stroke from South Asia. Data were derived over a period of 10 years and the remarkable similarity in results first reported in a smaller cohort more than a decade earlier,[12] provides strong supportive evidence for the ischemic stroke subtype pattern described. Stroke diagnosis was made systematically by trained stroke neurologists, based on relevant investigations required for TOAST classification of subtypes. An important limitation is that it was a hospital-based study and therefore likely to underestimate very mild and fatal strokes. However, extensive investigations to determine stroke subtypes are difficult to perform in community studies, and most stroke registries that have contributed to understanding pathophysiological mechanisms in stroke have been conducted worldwide in large hospital cohorts.
CONCLUSIONS
This study from a hospital-based registry in India reveals a distinct pattern of ischemic stroke subtypes, characterized by the significant overlap between Western and East Asian stroke patterns. High frequency of intracranial LAA while consistent with patterns in East Asian countries is lower than in the West. The lower frequency of SVO is unlike seen in East Asia while consistent with the West. Lower frequency of CE was observed in relation to the West but was comparable to other Asian countries. The reasons underlying this pattern of stroke subtypes in a South Asian registry are not clearly understood at present and may be potentially related to genetic, environmental, and vascular risk factors, requiring the need for further research in this direction. Awareness of stroke subtypes and their risk factors will be crucial in developing prevention strategies, proper management, and organization of health-care services in India.
Financial support and sponsorship
This study was funded by Indian Council of Medical Research, Govt of India.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Jauch EC, Saver JL, Adams HP, Jr, Bruno A, Connors JJ, Demaerschalk BM, et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44:870–947. doi: 10.1161/STR.0b013e318284056a. [DOI] [PubMed] [Google Scholar]
- 2.Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:2160–236. doi: 10.1161/STR.0000000000000024. [DOI] [PubMed] [Google Scholar]
- 3.NINDS Stroke Genetics Network (SiGN), International Stroke Genetics Consortium (ISGC). Loci associated with ischaemic stroke and its subtypes (SiGN): A genome-wide association study. Lancet Neurol. 2016;15:174–84. doi: 10.1016/S1474-4422(15)00338-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Porcello Marrone LC, Diogo LP, de Oliveira FM, Trentin S, Scalco RS, de Almeida AG, et al. Risk factors among stroke subtypes in Brazil. J Stroke Cerebrovasc Dis. 2013;22:32–5. doi: 10.1016/j.jstrokecerebrovasdis.2011.05.022. [DOI] [PubMed] [Google Scholar]
- 5.Liu X, Xu G, Wu W, Zhang R, Yin Q, Zhu W, et al. Subtypes and one-year survival of first-ever stroke in Chinese patients: The Nanjing stroke registry. Cerebrovasc Dis. 2006;22:130–6. doi: 10.1159/000093241. [DOI] [PubMed] [Google Scholar]
- 6.Grau AJ, Weimar C, Buggle F, Heinrich A, Goertler M, Neumaier S, et al. Risk factors, outcome, and treatment in subtypes of ischemic stroke: The German stroke data bank. Stroke. 2001;32:2559–66. doi: 10.1161/hs1101.098524. [DOI] [PubMed] [Google Scholar]
- 7.Jung KH, Lee SH, Kim BJ, Yu KH, Hong KS, Lee BC, et al. Secular trends in ischemic stroke characteristics in a rapidly developed country: Results from the Korean stroke registry study (secular trends in Korean stroke) Circ Cardiovasc Qual Outcomes. 2012;5:327–34. doi: 10.1161/CIRCOUTCOMES.111.963736. [DOI] [PubMed] [Google Scholar]
- 8.Aquil N, Begum I, Ahmed A, Vohra EA, Soomro BA. Risk factors in various subtypes of ischemic stroke according to TOAST criteria. J Coll Physicians Surg Pak. 2011;21:280–3. [PubMed] [Google Scholar]
- 9.Hajat C, Heuschmann PU, Coshall C, Padayachee S, Chambers J, Rudd AG, et al. Incidence of aetiological subtypes of stroke in a multi-ethnic population based study: The South London stroke register. J Neurol Neurosurg Psychiatry. 2011;82:527–33. doi: 10.1136/jnnp.2010.222919. [DOI] [PubMed] [Google Scholar]
- 10.Gezmu T, Schneider D, Demissie K, Lin Y, Gizzi MS. Risk factors for acute stroke among South Asians compared to other racial/ethnic groups. PLoS One. 2014;9:e108901. doi: 10.1371/journal.pone.0108901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sylaja PN, Pandian JD, Kaul S, Srivastava MV, Khurana D, Schwamm LH, et al. Ischemic stroke profile, risk factors, and outcomes in India: The indo-US collaborative stroke project. Stroke. 2018;49:219–22. doi: 10.1161/STROKEAHA.117.018700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kaul S, Sunitha P, Suvarna A, Meena AK, Uma M, Reddy JM. Subtypes of ischemic stroke in a metropolitan city of south India (one year data from a hospital based stroke registry) Neurol India. 2002;50:S8–14. [Google Scholar]
- 13.Adams HP, Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of org 10172 in acute stroke treatment. Stroke. 1993;24:35–41. doi: 10.1161/01.str.24.1.35. [DOI] [PubMed] [Google Scholar]
- 14.Syed NA, Khealani BA, Ali S, Hasan A, Akhtar N, Brohi H, et al. Ischemic stroke subtypes in Pakistan: The Aga Khan University Stroke Data Bank. J Pak Med Assoc. 2003;53:584–8. [PubMed] [Google Scholar]
- 15.Wu B, Lin S, Hao Z, Yang J, Xu Y, Wu L, et al. Proportion, risk factors and outcome of lacunar infarction: A hospital-based study in a Chinese population. Cerebrovasc Dis. 2010;29:181–7. doi: 10.1159/000267277. [DOI] [PubMed] [Google Scholar]
- 16.Hsieh FI, Lien LM, Chen ST, Bai CH, Sun MC, Tseng HP, et al. Get with the guidelines-stroke performance indicators: Surveillance of stroke care in the Taiwan stroke registry: Get with the guidelines-stroke in Taiwan. Circulation. 2010;122:1116–23. doi: 10.1161/CIRCULATIONAHA.110.936526. [DOI] [PubMed] [Google Scholar]
- 17.Takizawa S, Shibata T, Takagi S, Kobayashi S. Japan Standard Stroke Registry Study Group. Seasonal variation of stroke incidence in Japan for 35631 stroke patients in the Japanese standard stroke registry, 1998-2007. J Stroke Cerebrovasc Dis. 2013;22:36–41. doi: 10.1016/j.jstrokecerebrovasdis.2011.06.005. [DOI] [PubMed] [Google Scholar]
- 18.Gutierrez J, Koch S, Dong C, Casanova T, Modir R, Katsnelson M, et al. Racial and ethnic disparities in stroke subtypes: A multiethnic sample of patients with stroke. Neurol Sci. 2014;35:577–82. doi: 10.1007/s10072-013-1561-z. [DOI] [PubMed] [Google Scholar]
- 19.Bogousslavsky J, Barnett HJ, Fox AJ, Hachinski VC, Taylor W. Atherosclerotic disease of the middle cerebral artery. Stroke. 1986;17:1112–20. doi: 10.1161/01.str.17.6.1112. [DOI] [PubMed] [Google Scholar]
- 20.Wityk RJ, Lehman D, Klag M, Coresh J, Ahn H, Litt B, et al. Race and sex differences in the distribution of cerebral atherosclerosis. Stroke. 1996;27:1974–80. doi: 10.1161/01.str.27.11.1974. [DOI] [PubMed] [Google Scholar]
- 21.Bang OY, Saver JL, Liebeskind DS, Pineda S, Yun SW, Ovbiagele B, et al. Impact of metabolic syndrome on distribution of cervicocephalic atherosclerosis: Data from a diverse race-ethnic group. J Neurol Sci. 2009;284:40–5. doi: 10.1016/j.jns.2009.03.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Padma MV, Gaikwad S, Jain S, Maheshwari MC, Misra NK. Distribution of vascular lesions in ischaemic stroke: A magnetic resonance angiographic study. Natl Med J India. 1997;10:217–20. [PubMed] [Google Scholar]
- 23.Dalal PM, Shah PM, Aiyar RR, Kikani BJ. Cerebrovascular diseases in west central India. A report on angiographic findings from a prospective study. Br Med J. 1968;3:769–74. doi: 10.1136/bmj.3.5621.769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Petty GW, Brown RD, Jr, Whisnant JP, Sicks JD, O'Fallon WM, Wiebers DO, et al. Ischemic stroke subtypes: A population-based study of incidence and risk factors. Stroke. 1999;30:2513–6. doi: 10.1161/01.str.30.12.2513. [DOI] [PubMed] [Google Scholar]
- 25.Schneider AT, Kissela B, Woo D, Kleindorfer D, Alwell K, Miller R, et al. Ischemic stroke subtypes: A population-based study of incidence rates among blacks and whites. Stroke. 2004;35:1552–6. doi: 10.1161/01.STR.0000129335.28301.f5. [DOI] [PubMed] [Google Scholar]
- 26.Katsanos AH, Bhole R, Frogoudaki A, Giannopoulos S, Goyal N, Vrettou AR, et al. The value of transesophageal echocardiography for embolic strokes of undetermined source. Neurology. 2016;87:988–95. doi: 10.1212/WNL.0000000000003063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schulz UG, Rothwell PM. Differences in vascular risk factors between etiological subtypes of ischemic stroke: Importance of population-based studies. Stroke. 2003;34:2050–9. doi: 10.1161/01.STR.0000079818.08343.8C. [DOI] [PubMed] [Google Scholar]
- 28.Lovett JK, Coull AJ, Rothwell PM. Early risk of recurrence by subtype of ischemic stroke in population-based incidence studies. Neurology. 2004;62:569–73. doi: 10.1212/01.wnl.0000110311.09970.83. [DOI] [PubMed] [Google Scholar]