

Abstract
Objective
This study aims to understand the basis of continued HIV-1 transmission in Zambian and Rwandan HIV-1 discordant couples in the context of ART.
Design
We identified 9 Zambian and 7 Rwandan acutely-infected, epidemiologically-linked couples from government CVCT clinics where transmitting partners reported being on ART near the time of transmission.
Methods
We quantified viral load (VL) and plasma antiretroviral (ARV) drug concentrations near the time of transmission and used these as surrogate measures for adherence. We also sequenced the polymerase gene from both donor and recipient partners to determine the presence of drug resistance mutations (DRM).
Results
In Zambia, all transmitting partners had detectable VL and 8/9 were not on therapeutic ARV regimens. In the remaining couple, despite being on a therapeutic regimen, DRM were present and transmitted. In Rwanda, although 6/7 transmitting partners had detectable VL, therapeutic levels of ARV were detected in 4/7, but were accompanied by DRM. In the remaining 3 couples, either no ARV or sub-therapeutic regimens were detected.
Conclusions
A reduction of ART effectiveness in non-trial settings was associated with lack of ARVs in plasma and detectable VL, as well as DR. In Zambia, where CVCT is not widely implemented, inconsistent adherence was high in couples unaware of their HIV discordance. In Rwanda, where CVCT is deployed country-wide, virologic failure was associated with DR and subsequent transmission. Together, these findings suggest that increasing ART availability in resource-limited settings without risk reduction strategies that promote adherence, may not be sufficient to control the HIV epidemic in the post-ART era.
Keywords: HIV-1 transmission, ART, CVCT, discordant couples, adherence, drug resistance, transmission pairs
INTRODUCTION
According to the World Health Organization (WHO), the rates of HIV-1 acquisition worldwide remain stable, with approximately 2 million new HIV infections per year [1], with over half acquired in marriage in sub-Saharan Africa [2–4]. Despite the effectiveness of ART in the treatment and prevention of HIV acquisition and transmission [5–10], in resource-limited settings, behavioral interventions, such as couples’ voluntary counseling and testing (CVCT), remain the most cost-effective ways to reduce transmission (by up to 75%) in co-habiting couples [11–15]. Moreover, both ART uptake and effectiveness for treatment and prevention are improved when couples are counseled together and made aware of their partner’s status [8, 16]. Although WHO guidelines support CVCT for HIV prevention [17], fewer than 10% of African couples have been jointly tested and counseled, highlighting the need for widespread implementation of CVCT [18].
The prevention clinical trial, HPTN 052, established that transmission could be reduced by up to 96% (approximately 2.5/100 PY in the delayed treatment control arm vs. <0.5/100 PY in the early ART arm) [8, 9] in HIV discordant couples who had already benefited from a substantial reduction in transmission following CVCT, when ART was added and VL in the positive partner was completely suppressed.
While ART can be effective in treating [5, 7, 10] and preventing HIV-1 transmission [10], it has become clear that suboptimal adherence, a determinant of ART failure, is a major obstacle to its continued success [19–21]. Indeed, it is estimated that less than half of the HIV-1 population on ART is virologically suppressed [1], likely due to suboptimal adherence, which is a major driver of DR [19]. In addition, as ART availability increases worldwide, so does the rate of primary drug resistance (PDR) [22–24]. The PASER-M study showed that rates of PDR were significantly higher in sites where there was early widespread access to ART [25]. The increasing risk of acquisition and transmission of DR viral variants suggest ART alone may not be sufficient to tackle this epidemic.
Despite the near 100% effectiveness of ART to prevent transmission in clinical trials, we observe ongoing transmission in HIV discordant couples reporting ART usage (Wall et al., submitted) in government clinics. Since, there is an increased risk for suboptimal adherence in low- to lower-middle income countries [19], we hypothesized that this may be the source of virologic failure and subsequent transmission. As transmission frequency can vary based on viral subtype [26], we sought to investigate whether this contributed to HIV-1 transmission in both heterosexual Zambian (subtype C) and Rwandan (subtype A) couples where the HIV positive partner reported ART usage. An analysis of transmission in these two countries allows a comparison in the context of the two most globally common subtypes (C and A) and different healthcare systems. We observed remarkable differences between the two countries. In epidemiologically linked Zambian pairs, we found that, despite the reported use of ART, a majority (7/9) of the transmitting partners had quantifiable VL and no ARV in plasma. In contrast, in 7 Rwandan transmission pairs analyzed in parallel, the majority showed quantifiable ARV levels in plasma. In more than half of the Rwandan couples we detected DRM, a majority of which were transmitted to their partners. Identifying the factors associated with HIV-1 transmission, in the context of reported use of ARV, will inform public health strategies to achieve effective prevention and treatment approaches in the post-ART era.
MATERIALS AND METHODS
SETTINGS AND STUDY POPULATIONS
Heterosexual couples were recruited for couples counseling and testing (CVCT) in urban government clinics in Zambia and Rwanda as described in Supplementary Methods. In Zambia, during the initial visit, couples were tested for HIV-1 and, based on their HIV-1 serostatus, counseled and referred to appropriate services. Serodiscordant couples were asked to return to clinic at 1 and 3 months after the initial visit for repeat HIV counseling and testing (of the negative partner) and reinforcement of risk reduction counseling messages. If seroconversion in the previously HIV negative partner was detected, linkage analysis of viruses from both partners was performed [27]. For the current study, we selected couples where the donor partner reported the prior use of ART during their initial counseling visit. The incidence of transmission prior to CVCT (i.e. where the seronegative partner seroconverted prior to their month 1 visit) in these couples was estimated as ~9% (Wall et al., submitted).
Rwandan couples who met the following criteria were chosen for the study: previously undergone CVCT and referral for ART, returning for their 3-month routine follow-up visit in government clinics in Kigali, and the seronegative partner had now seroconverted. This study protocol was approved by the following institutional review boards: University of Zambia Research Ethics Committee, Rwanda Ethics Committee, and IRB at Emory University; all subjects gave written informed consent for participation in the study.
VIRAL LOAD (VL) TESTING
HIV-1 VL determination (in copies/mL) was performed on plasma using the Abbott Real-Time HIV-1 VL assay (Abbott Molecular; Abbott Park, IL). For more details, see Supplemental Methods.
LIQUID CHROMATOGRAPHY TANDEM MASS SPECTROSCOPY (LC-MS/MS) FOR DETECTION OF ANTIRETROVIRAL AGENTS
To detect and quantify ARV levels in patient plasma, a high-performance liquid chromatography-tandem mass spectrometry (LC-MS/MS) approach was used similar to previously described methods (see Supplemental Methods) [28].
ARV levels were recorded in ng/mL. Effective concentrations, where 50 or 90% (EC50 or EC90) of the drug’s maximal effect was observed, were calculated for each ARV (Supplemental Table 1).
VIRAL RNA EXTRACTION, PCR AMPLIFICATION, AND POPULATION SEQUENCING OF HIV-1 pol
Viral RNA was extracted from plasma samples and reverse transcribed as previously described [29]. Alternatively, genomic DNA was used as a template for low VL samples. Nested PCR amplification was performed for 5’-half HIV-1 genomes (~4.5kb) with the Q5® High-Fidelty enzyme (New England BioLabs Inc., Ipswich, MA). Primers listed in Supplemental Table 2.
Positive PCR amplicons were pooled and purified. Pooled populations were sequenced using either Sanger (GenScript; Piscataway, NJ) or SMRT technology platform (Pacific Biosciences; Menlo Park, CA) based on sample availability. More details are available in Supplemental Methods.
MULTIPLEX RNA PCR ASSAY FOR LACK OF VL SUPPRESSION IN NON-TRANSMITTING POSITIVE PARTNERS (NT)
Viral RNA was extracted from plasma samples for 50 NT using E.Z.N.A Viral RNA extraction kit (Omega Bio-tech, Norcross, GA). As described (Basu et al., manuscript in preparation), RNA was subjected to a multiplexed one-step RT-PCR first round PCR reaction using SuperScript III One-Step RT-PCR System (Invitrogen, Waltham, MA). Three small regions were multiplexed: gp41 (460 bp), gag (560 bp), and pol (218 bp). Second round amplification for each region was then performed independently.
PAC-BIO LIBRARY PREPARATION, SEQUENCING, AND ANALYSIS OF HIV-1 POL
A SMRTbell library containing barcoded and non-barcoded 5’-half genomes was generated, per manufacturer’s protocol (Pacific Biosciences Inc., CA). Sequencing was performed as previously described [30]. Exported data files were processed using the MDPSeq software pipeline [30] and output sequences aligned in Geneious (Biomatters Ltd., Auckland, NZ).
DRUG RESISTANCE MUTATION (DRM) ANALYSIS
Pol sequences for both donor and recipient partners (where available) were submitted for DRM analysis (HIVdb, HIV Drug Resistance database) [31]. Each DRM identified was assigned a drug penalty score and these scores were added to determine the level of drug resistance to eight ARV; scores ≥60 were considered high-level resistance.
RESULTS
HIV-1 Transmission in Zambian couples reporting ART use
To understand the factor(s) associated with ongoing HIV-1 transmission in Zambian serodiscordant couples in the context of ART, we identified and recruited nine epidemiologically linked pairs from government clinics where the donor self-reported being on ART. Of the nine couples, all donors had detectable VL (Figure 1A) ranging from 7,852 to 444,440 copies/mL (median: 47,600 copies/mL). These VL were more similar to those of chronically infected ART-naïve individuals from our larger heterosexual transmission (HT) cohort [32], RZHRG, where for 1,652 individuals, the median VL was 70,000 copies/mL. In contrast the median VL for 77 ART-treated individuals in the same cohort was significantly lower (160 copies/mL; p<0.0001) [11].
Figure 1. Plasma viral loads (VL) and ARV concentrations in Zambian donors reportedly on ART.
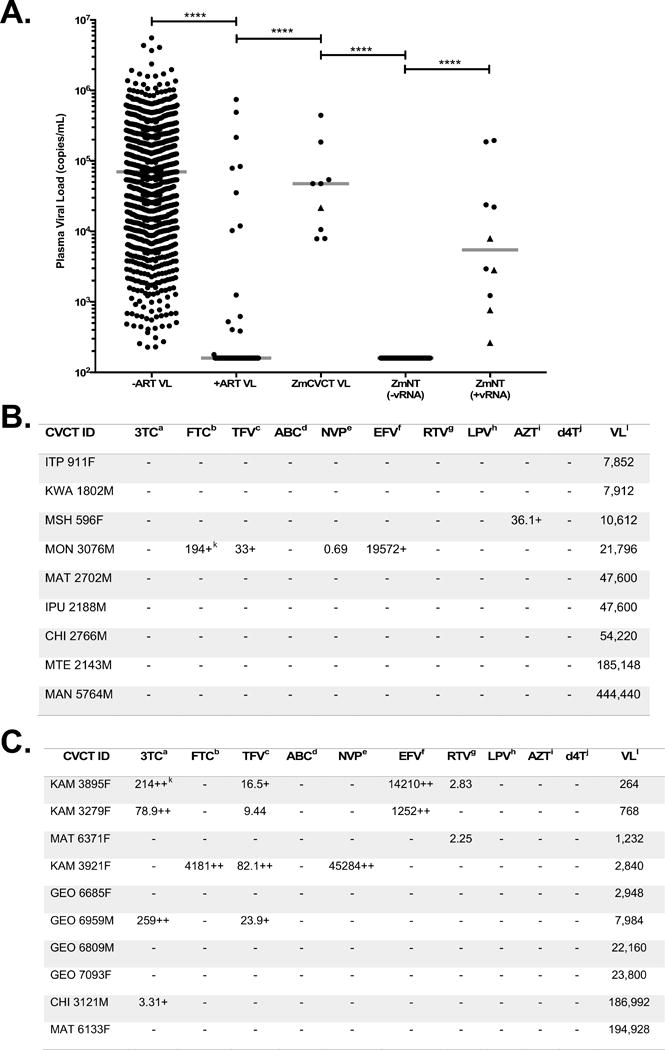
(A) Plasma VL (copies/mL) were quantified using a quantitative RT-PCR assay (see Methods). VL from Zambian ART-naïve (-ART VL) and ART-treated (+ART VL) individuals from the Rwanda-Zambia HIV Research Group (RZHRG) database were compared to those from Zambian (Zm) transmitting partners from nine linked transmission pairs (ZmCVCT) and 50 Zm Non-Transmitting (ZmNT) donors (vRNA- or vRNA+). Median VL represented by gray lines. Triangles indicate individuals with at least two detectable ARV in their plasma. (B) Plasma concentration of 10 different ARV and corresponding VL from ZmCVCT transmitting partners. (C) Plasma concentration of 10 different ARV and corresponding VL from vRNA+ ZmNT partners. Generic drug names (superscripts a-j), EC50 and EC90 for these ARVs are provided in Supplemental Table 1. Drug concentrations are in nM; + = >EC50; ++ = >EC90. Plasma VL - copies/mL.
Although the recommended ART regimens for Zambia are TDF-XTC-EFV/NVP, because some individuals may receive other therapies, we quantitated the concentration of a total of 10 ARVs in patient plasma using HPLC-MS/MS (Figure 1B). Only two donors (MON 3076M and MSH 596F) had detectable ARV in plasma. MON 3076M had three drugs (FTC, TFV, EFV) above the effective concentration 50 (EC50) and one drug (NVP) below the EC50, which is consistent with first-line ART prescribed in Zambia. For MSH 596F, only AZT was detectable.
Although an interruption in ART likely contributed to the majority of transmission events in the nine Zambian couples, to determine if DRM contributed to transmission, we amplified and sequenced the pol gene from both donor and recipient in each couple. In one couple, MON 3076, we detected six DRM that together conferred high-level resistance to six ARV in the donor partner (Figure 2A), including the four (FTC, TFV, EFV, NVP) detected in donor plasma (Figure 1B). All but one DRM (V106M) was detected in the recipient (Figure 2B). Although both partners exceeded the threshold for high-level resistance to EFV and NVP (cumulative penalty scores of 60 and above), the donor’s level of resistance was higher (140 for EFV and NVP) than the recipient (85 for EFV and 135 for NVP).
Figure 2. DRMs lead to drug resistance/susceptibility in one linked transmission pair.
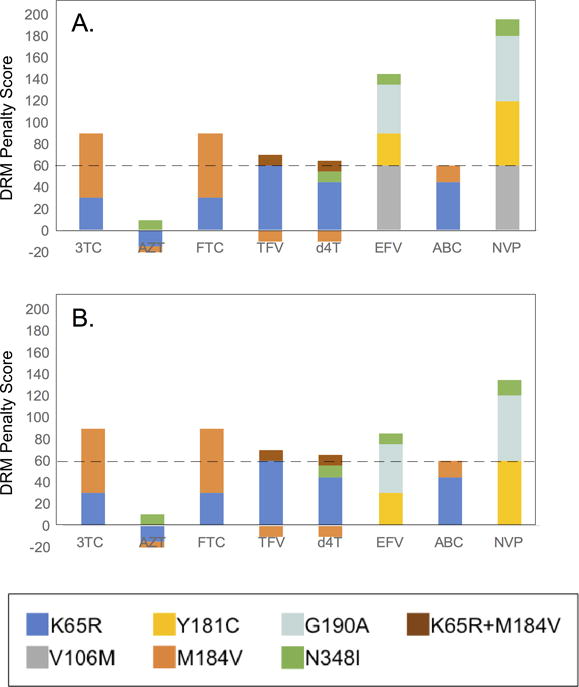
Transmitted drug resistance in one couple (MON 3076). Major drug resistance mutations (DRM) in transmitting/donor partner (A) and the seroconverter/recipient (B) partner at the time of transmission. Each DRM contributes to ARV resistance positively (values greater than 0) or negatively (values less than 0). The contribution of each DRM is estimated by penalty scores (generated by the Stanford HIV drug resistance database). The cumulative penalty score determines the level of drug resistance (between 0-9: susceptible; 10-14: potential low level resistance; 15-29, low level resistance; 30-59, intermediate resistance; ≥60, high level resistance).
VL AND ARV DETECTION IN NON-TRANSMITTING ZAMBIAN PARTNERS REPORTING ART
To confirm that a majority of individuals in Zambian government clinics who reported ARV use understood their ART status and correctly answered the question, we randomly selected 50 Zambian serodiscordant couples from the same clinics and where the HIV positive partner (25M, 25F) self-reported ARV use. These individuals had not transmitted (NT) to their partners. Forty out of the fifty NTs (80%) had no trace of viral RNA in plasma samples in an in-house multiplex qualitative RNA PCR assay (Basu et al., manuscript in preparation) in which we amplified three genomic regions of HIV-1 (gag, pol, gp41). We were able to detect viral RNA (for at least one genomic region) in the remaining ten individuals. The VLs in these individuals ranged from 264-194,928 copies/mL, with a median VL of 5,466 copies/mL (Figure 1A). As a control, we quantified the VL of eight randomly selected individuals from the 40 that were undetectable to confirm the absence of viral RNA/viral replication. Consistent with the qualitative results, all VL were undetectable (Figure 1A).
Of the ten viral RNA positive individuals (Figure 1C), four had no drug present in their plasma, five had at least one drug above its EC50, and one had only one drug (below the EC50) detected. Plasma from the eight RNA negative control individuals all contained three drugs with plasma concentrations near or above the EC50. Thus, for those positive partners reporting ARV use in government clinics, ART was consistent with their response to the questionnaire, and overall adherence in the population was high.
HIV-1 Transmission in Rwandan couples reporting ART use
Rwanda differs from Zambia in that CVCT is deployed country-wide and a majority of couples know each partner’s HIV status. We hypothesized that consistent adherence, therefore, would be better than in Zambia. We identified seven acute transmission pairs from Rwandan government clinics, where the donor partner reported ARV usage, and determined VL and ARV levels for these couples. The plasma VL in the donors at the time of sampling ranged from undetectable (<160 copies/mL) to 914,000 copies/mL with a median of 3,658 copies/mL (Figure 3A). Although this value was lower than the median VL for a set of untreated Rwandans for whom VL were available (median: 17,244 copies/ml), it was not significantly different (p=0.085). In contrast, a set of ART-treated individuals from the RZHRG-Projet San Francisco transmission cohort had a median VL of 160, which was significantly lower (p<0.0001).
Figure 3. Plasma VL in Rwandan donors trend lower than Zambian donors.
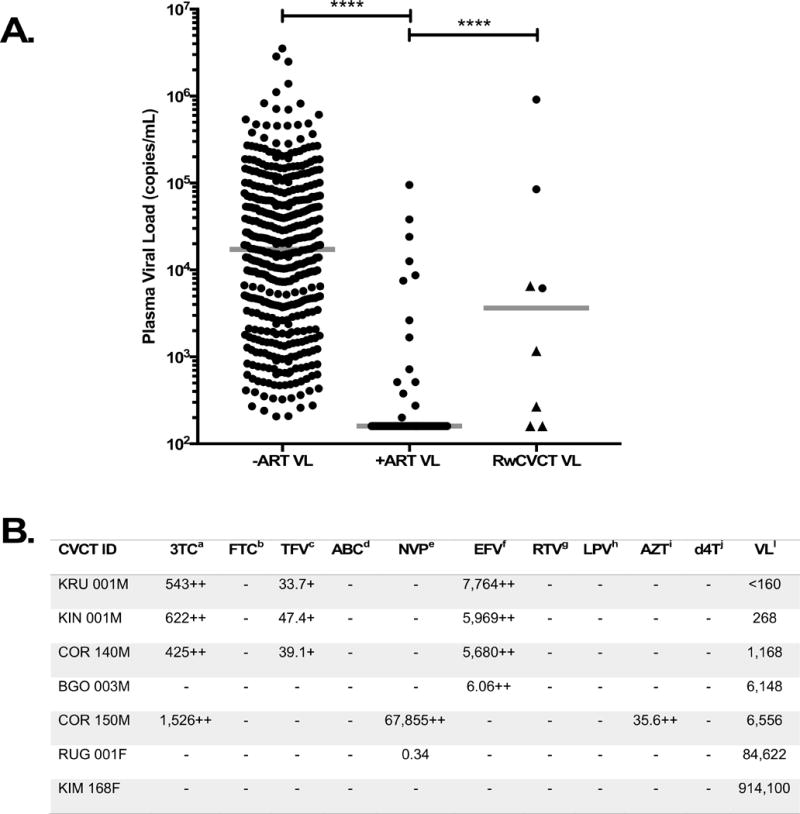
(A) Plasma VL (copies/mL) were quantified using a quantitative RT-PCR assay (see Methods). VL from Rwandan (Rw) ART-naïve (-ART VL) and ART-treated (+ART VL) individuals from the RZHRG database were compared to those from the transmitting partners of seven epidemiologically linked transmission pairs (RwCVCT VL). Median VL represented by gray lines. Triangles indicate individuals with at least two detectable ARV in plasma. (B) Plasma concentration of 10 different ARV and corresponding VL from RwCVCT transmitting partners. Generic drug names (superscripts a-j), EC50 and EC90 for these ARVs are provided in Supplemental Table 1. Drug concentrations are in nM; + = >EC50; ++ = >EC90. Plasma VL - copies/mL.
To confirm ART status, we screened plasma samples for the presence of 10 ARV (Supplementary Table 1; Figure 3B). In contrast to what we observed in Zambia, a total of four of seven ART-reporting donors (57%) had at least three ARV with concentrations above the EC50, while two of seven (29%) had only one ARV present. The remaining individual (14%) had no detectable ARV. The triple therapies detected were again consistent with WHO-recommended first-line regimens (TDF/3TC/EFV). Due to the detection of ARV in 85.7% of these donors, we hypothesized that DR rather than an interruption in ART may contribute to transmission in this subset. Indeed, we were able to determine or infer the presence of DRM in four of the seven couples; of these couples, there was evidence for transmitted DR in three pairs (75%). In the BGO 003 pair, we detected one NNRTI DRM, V106M, in the donor, rendering the virus highly-resistant (penalty score: 60) to NVP and EFV treatment (Figure 4A; left); however, this DRM was not detected in the partner (Figure 4A; right), although reversion between transmission and sampling is possible.
Figure 4. DRM result in treatment failure and subsequent transmission in Rwandan pairs.
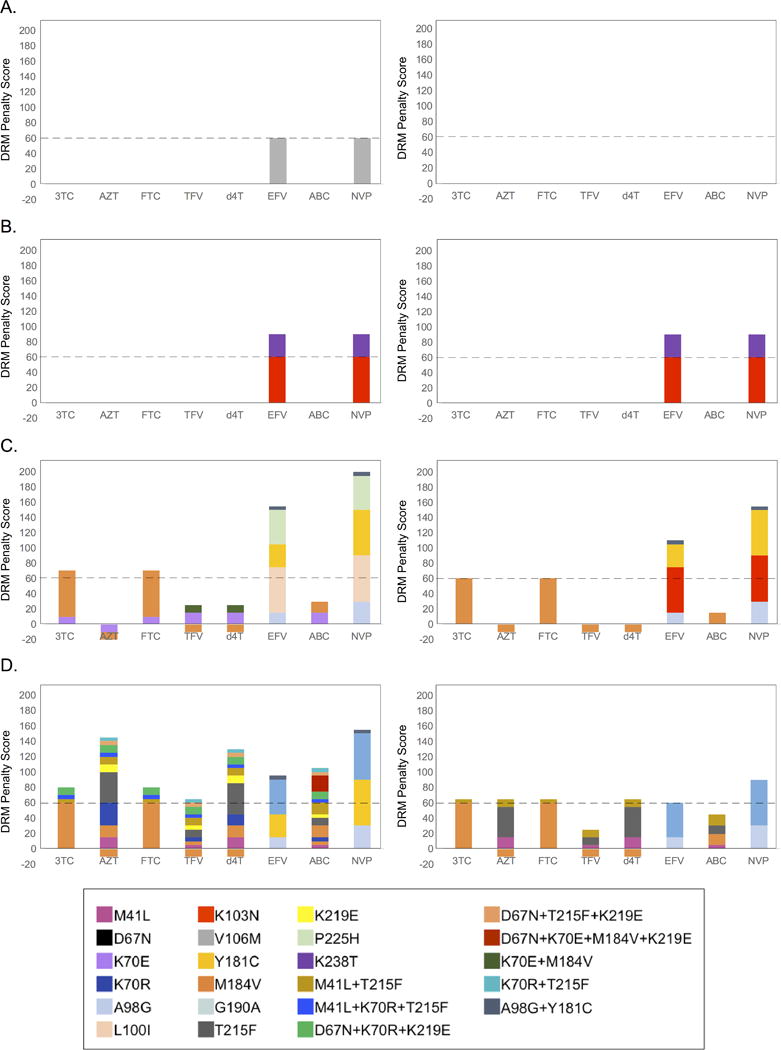
Pol sequences for donor and recipient partners were submitted to the Stanford HIV Drug Resistance database for the identification of potential DRM. Major DRM were detected in (A) BGO 003M (donor), (B) RUG 001F (donor) and RUG 001M (recipient), (C) COR 140F (recipient), and (D) COR 150M (donor) and COR 150F (recipient). The contribution of each DRM is estimated by penalty scores (a Stanford HIV drug resistance database measure). The cumulative penalty score determines the level of drug resistance (between 0-9: susceptible; 10-14: potential low level resistance; 15-29, low level resistance; 30-59, intermediate resistance; ≥60, high level resistance.
In the RUG 001 pair, we identified two NNRTI DRM in the donor virus (Figure 4B; left), K103N and K238T, which contributed to high-level resistance and were detected in the partner (Figure 4B; right). Although we were unable to directly sequence the COR 140 donor, we detected two distinct DR viral populations in the recipient’s plasma, suggesting multi-variant transmission. Viral variant 1 contained three NNRTI and one NRTI DRM, which confer high-level resistance to both classes of drug (Figure 4C; left). Viral variant 2 contained six DRM, three of which were present in variant 1 (Figure 4C; right). This variant encoded two additional NNRTI and one additional NRTI DRM (Figure 4C). In the COR 150 pair, we detected nine DRM in the donor virus (Figure 4D; left). Three mutations contributed to high-level NNRTI resistance, while two rendered the virus highly-resistant to several NRTI. Only five DRM were detected in the partner (Figure 4D; right). Finally, viral sequences obtained from the KIN 001 and KIM 168 couples showed no evidence of DRM.
These data show that, in contrast with Zambia, at least half of the ART-reporting transmitting couples had evidence of DRM, indicating DR was strongly associated with HIV-1 transmission in these Rwandan heterosexual transmission pairs.
DISCUSSION
In HIV discordant couples, CVCT followed by ART remains the only effective intervention to prevent HIV-1 transmission [8, 9]. Moreover, in developing countries where the current infrastructure may prohibit the successful deployment of resources necessary to achieve full virologic suppression [33, 34], CVCT remains a key component of prevention efforts. The goal of this study was to understand the basis of ongoing HIV-1 transmission in the context of ART in discordant African couples, where the disease burden is the greatest.
HIV-1 Transmission in Heterosexual Zambian Couples
Many factors, including socioeconomic status, availability, adherence, duration of treatment, and acquired or transmitted DR, can affect the efficacy of ART regimens [19, 22, 23, 25, 35]. Of these factors, virologic suppression is largely dependent on strict adherence [19]. Previous work assessing ART adherence in sub-Saharan Africa has focused mainly on identifying barriers to adherence and the consequences of non- or suboptimal adherence on the individual [19, 36]. However, limited data is available on how lack of adherence and DR impact HIV-1 transmission in couples in African settings [37].
To address this, we analyzed 9 cases of acute transmission identified in couples attending CVCT in government clinics where transmitting partners reported ART use prior to the time of transmission. We measured VL and screened for ARVs in plasma samples of the transmitting partners as these measures help gauge adherence and ART efficacy. In Zambia, all nine transmitting partners had detectable VL with a median similar to that of ART-naïve Zambians from a larger cohort, demonstrating that none of these individuals were on HIV-1 suppressive therapy. Indeed, a majority (7/9) of donors had no detectable ARV in their plasma, providing unambiguous evidence for why these individuals had quantifiable VL. However, despite measurable levels of ARV in two donors, both had plasma VL >10,000 copies/mL. These data suggested that treatment failure may have allowed for transmission in these two couples. We detected six DRM in one donor that contributed to high-level DR to several ARV including those present in donor plasma. As the likelihood of developing DR in ART-treated individuals is relatively low when adherence is high [22, 23, 36, 38, 39], the presence of DRM in the donor suggests suboptimal adherence at some point in time. Although our study was limited by sample size and lacked longitudinal follow-up, these data suggest that HIV-1 transmission in this group was largely associated non-adherence; however, a larger prospective study with longitudinal sampling is required to establish a causal relationship.
The lack of adherence at the time of sampling observed in these transmitting couples, was not simply due to a lack of understanding of the question during CVCT, since in a group of 50 non-transmitting HIV positive partners tested in the same government clinics in Lusaka and Ndola, a majority (40 of 50) had undetectable VL indicating that adherence in the overall population was high.
HIV-1 Heterosexual Transmission in Rwandan couples
Naturally occurring polymorphisms that differentiate viral subtypes have been shown to alter the structure of drug targets resulting in differential responses to ARV [40, 41]. Thus factor(s) contributing to HIV-1 transmission in the face of reported ARV use could be different in Zambia (subtype C) versus Rwanda (mainly subtype A). Moreover, because CVCT is deployed nationally in Rwanda and both partners know their partner’s HIV status, we predicted that adherence may be better than in Zambia. Indeed, in a similar analysis of seven Rwandan heterosexual transmission pairs, where the transmitting partner reported being on ART, we detected ARV in 6/7 donors (although only four were on fully therapeutic regimens of a triple therapy). Over half of the transmitting partners (4/7) had DRM that yielded intermediate to high-level DR. In addition, of these four couples, three transmitted DRM to their acutely infected partner. The frequency with which DRM were detected in the seroconverting partner may be an underestimate, since sampling at three months could allow reversion to wild-type, and may explain why fewer DRM were identified in the seroconvertor. These data indicate that a majority of transmissions in this limited number of Rwandan pairs was associated with DRM.
Differences between Zambian and Rwandan couples
Although, subtype could offer a biological basis for some of the observed differences between the two groups, these disparities are more likely linked to differences in infrastructure including national CVCT and treatment of the HIV+ partner in Rwanda.
As a part of routine government CVCT visits, HIV+ individuals are asked whether or not they are on ART. The transmission pairs included in this study were selected based on reported ART use prior to counseling by the chronically infected transmitting partner, yet the majority of Zambians (8/9) and a little over 40% of the Rwandans were not taking therapeutic levels ARVs at the time of sampling, consistent with a previous report that self-report is not the most reliable measure of adherence [42].
Several studies have reported that the risk of HIV-1 transmission varies based on plasma VL of the HIV positive partner with transmission being negligible for individuals with VL <1,500 copies/mL [43, 44]. While in Zambia, all the transmitting partners had VL >8,000 copies/mL; almost half of the Rwandan transmitting partners had VL <1,500 copies/mL. Although these Rwandan couples were selected because the transmitting partner reported ART use prior to transmission, we cannot rule out a brief period of non-adherence where VL increased sufficiently to allow transmission. While there is evidence to suggest a correlation between blood and genital fluid VL, ART can lead to differences in these compartments due to differential penetration of tissues [45]. Thus, it is also possible that insufficient penetration of ARV in the genital tract could explain how these donors with extremely low plasma VL (<500 copies/mL) still transmitted to their partners. Evaluation of VL in the genital compartments may be required to firmly establish the cause of transmission in couples with such low VL.
In conclusion, although CVCT is effective at preventing HIV-1 infection and ART in discordant couples is additive in its preventive impact [6], it is unlikely that ART alone will end the AIDS epidemic. In this study, our data suggest that non-adherence and DR are both associated with ongoing transmission in the context of more widely available ART in Zambia and Rwanda respectively, and that these factors differentially impacted both cohorts. We noted that the development of DR not only led to treatment failure in the donor, but also subsequent transmission of DRM to the recipient partners, compromising future treatment options for that individual. Because VL testing is either limited or not available in Rwanda and Zambia respectively, early detection of problems with adherence or DR is not occurring. Together, these data suggest that public health interventions, such as early partner involvement through CVCT, which reinforce the importance of adherence, as well as the development and widespread deployment of cost-effective VL and DR testing are essential to achieving the maximal benefit from ART.
Supplementary Material
Acknowledgments
The investigators thank all the volunteers in Zambia who participated in this study and all the staff at the Zambia Emory HIV Research Project in Lusaka who made this study possible. The investigators would like to thank Jon Allen, Sheng Luo, and Paul Farmer for technical assistance, sample management, and database management. This study was funded by R01 MH095503-05 (SA), R37 AI51231 and R01 AI64060 (E.H.). This work was also supported, in part, by the Virology Core at the Emory Center for AIDS Research by performing viral load determinations (grant P30 AI050409); the Yerkes National Primate Research Center base grant through the Office of Research Infrastructure Programs/OD P51OD11132. This study is supported in part by IAVI (SA), whose work is made possible by generous support from many donors including: the Bill & Melinda Gates Foundation; the Ministry of Foreign Affairs of Denmark; Irish Aid; the Ministry of Finance of Japan; the Ministry of Foreign Affairs of the Netherlands; the Norwegian Agency for Development Cooperation (NORAD); the United Kingdom Department for International Development (DFID), and the United States Agency for International Development (USAID). The full list of IAVI donors is available www.iavi.org. The contents are the responsibility of the study authors and do not necessarily reflect the views of USAID or the United States Government. DB was in receipt of post-doctoral training support from NIH Training Grant R25 TW009337. E.H. is a Georgia Eminent Scholar.
Footnotes
None of the authors have a commercial or other association that might pose a conflict of interest with regard to this manuscript.
A preliminary report of these studies was presented as a poster at the 2016 HIV Research for Prevention Conference, October 2016, Chicago, IL.
Author Roles:
Evonne Woodson, Alec Goldberg, Clive Michelo, Debby Basu, Sijia Tao and Yong Jiang performed the experiments. Evonne Woodson, William Kilembe, and Eric Hunter wrote the manuscript. William Kilembe, Etienne Karita, Susan Allen directed the fieldwork and sample collection. Susan Allen, Debby Basu, Evonne Woodson and Eric Hunter conceived the study. All authors reviewed and edited the manuscript.
References
- 1.UNAIDS. global AIDS Update 2016. 2016:1–16. [Google Scholar]
- 2.Chomba E, Allen S, Kanweka W, Tichacek A, Cox G, Shutes E, et al. Evolution of couples’ voluntary counseling and testing for HIV in Lusaka, Zambia. J Acquir Immune Defic Syndr. 2008;47(1):108–115. doi: 10.1097/QAI.0b013e31815b2d67. [DOI] [PubMed] [Google Scholar]
- 3.Dunkle KL, Stephenson R, Karita E, Chomba E, Kayitenkore K, Vwalika C, et al. New heterosexually transmitted HIV infections in married or cohabiting couples in urban Zambia and Rwanda: an analysis of survey and clinical data. Lancet. 2008;371(9631):2183–2191. doi: 10.1016/S0140-6736(08)60953-8. [DOI] [PubMed] [Google Scholar]
- 4.Lambdin BH, Kanweka W, Inambao M, Mwananyanda L, Shah HD, Linton S, et al. Local residents trained as ‘influence agents’ most effective in persuading African couples on HIV counseling and testing. Health affairs. 2011;30(8):1488–1497. doi: 10.1377/hlthaff.2009.0994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Arts EJ, Hazuda DJ. HIV-1 antiretroviral drug therapy. Cold Spring Harb Perspect Med. 2012;2(4):a007161. doi: 10.1101/cshperspect.a007161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Baeten J, Celum C. Systemic and topical drugs for the prevention of HIV infection: antiretroviral pre-exposure prophylaxis. Annu Rev Med. 2013;64:219–232. doi: 10.1146/annurev-med-050911-163701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Celum C, Baeten JM. Antiretroviral-based HIV-1 prevention: antiretroviral treatment and pre-exposure prophylaxis. Antivir Ther. 2012;17(8):1483–1493. doi: 10.3851/IMP2492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505. doi: 10.1056/NEJMoa1105243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Loutfy MR, Wu W, Letchumanan M, Bondy L, Antoniou T, Margolese S, et al. Systematic review of HIV transmission between heterosexual serodiscordant couples where the HIV-positive partner is fully suppressed on antiretroviral therapy. PLoS One. 2013;8(2):e55747. doi: 10.1371/journal.pone.0055747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yoshimura K. Current status of HIV/AIDS in the ART era. J Infect Chemother. 2017;23(1):12–16. doi: 10.1016/j.jiac.2016.10.002. [DOI] [PubMed] [Google Scholar]
- 11.Allen S, Meinzen-Derr J, Kautzman M, Zulu I, Trask S, Fideli U, et al. Sexual behavior of HIV discordant couples after HIV counseling and testing. AIDS. 2003;17(5):733–740. doi: 10.1097/00002030-200303280-00012. [DOI] [PubMed] [Google Scholar]
- 12.Inambao M, Kilembe W, Canary LA, Czaicki NL, Kakungu-Simpungwe M, Chavuma R, et al. Transitioning couple’s voluntary HIV counseling and testing (CVCT) from stand-alone weekend services into routine antenatal and VCT services in government clinics in Zambia’s two largest cities. PLoS One. 2017;12(10):e0185142. doi: 10.1371/journal.pone.0185142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Karita E, Nsanzimana S, Ndagije F, Wall KM, Mukamuyango J, Mugwaneza P, et al. Implementation and Operational Research: Evolution of Couples’ Voluntary Counseling and Testing for HIV in Rwanda: From Research to Public Health Practice. J Acquir Immune Defic Syndr. 2016;73(3):e51–e58. doi: 10.1097/QAI.0000000000001138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kelley AL, Hagaman AK, Wall KM, Karita E, Kilembe W, Bayingana R, et al. Promotion of couples’ voluntary HIV counseling and testing: a comparison of influence networks in Rwanda and Zambia. BMC Public Health. 2016;16:744. doi: 10.1186/s12889-016-3424-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wall KM, Kilembe W, Nizam A, Vwalika C, Kautzman M, Chomba E, et al. Promotion of couples’ voluntary HIV counselling and testing in Lusaka, Zambia by influence network leaders and agents. BMJ Open. 2012;2(5) doi: 10.1136/bmjopen-2012-001171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Baeten JM, Donnell D, Ndase P, Mugo NR, Campbell JD, Wangisi J, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med. 2012;367(5):399–410. doi: 10.1056/NEJMoa1108524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Organization WH. Guidance on Couples HIV Testing and Counselling Including Antiretroviral Therapy for Treatment and Prevention in Serodiscordant Couples. 2012:1–79. [PubMed] [Google Scholar]
- 18.Czaicki NL, Davitte J, Siangonya B, Kastner R, Ahmed N, Khu NH, et al. Predictors of first follow-up HIV testing for couples’ voluntary HIV counseling and testing in Ndola, Zambia. J Acquir Immune Defic Syndr. 2014;66(1):e1–7. doi: 10.1097/QAI.0000000000000076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bijker R, Jiamsakul A, Kityo C, Kiertiburanakul S, Siwale M, Phanuphak P, et al. Adherence to antiretroviral therapy for HIV in sub-Saharan Africa and Asia: a comparative analysis of two regional cohorts. J Int AIDS Soc. 2017;20(1):1–10. doi: 10.7448/IAS.20.1.21218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chi BH, Cantrell RA, Zulu I, Mulenga LB, Levy JW, Tambatamba BC, et al. Adherence to first-line antiretroviral therapy affects non-virologic outcomes among patients on treatment for more than 12 months in Lusaka, Zambia. Int J Epidemiol. 2009;38(3):746–756. doi: 10.1093/ije/dyp004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shubber Z, Mills EJ, Nachega JB, Vreeman R, Freitas M, Bock P, et al. Patient-Reported Barriers to Adherence to Antiretroviral Therapy: A Systematic Review and Meta-Analysis. PLoS Med. 2016;13(11):e1002183. doi: 10.1371/journal.pmed.1002183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hamers RL, Sigaloff KC, Kityo C, Mugyenyi P, de Wit TF. Emerging HIV-1 drug resistance after roll-out of antiretroviral therapy in sub-Saharan Africa. Curr Opin HIV AIDS. 2013;8(1):19–26. doi: 10.1097/COH.0b013e32835b7f94. [DOI] [PubMed] [Google Scholar]
- 23.Hamers RL, Wallis CL, Kityo C, Siwale M, Mandaliya K, Conradie F, et al. HIV-1 drug resistance in antiretroviral-naive individuals in sub-Saharan Africa after rollout of antiretroviral therapy: a multicentre observational study. Lancet Infect Dis. 2011;11(10):750–759. doi: 10.1016/S1473-3099(11)70149-9. [DOI] [PubMed] [Google Scholar]
- 24.Stadeli KM, Richman DD. Rates of emergence of HIV drug resistance in resource-limited settings: a systematic review. Antivir Ther. 2013;18(1):115–123. doi: 10.3851/IMP2437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hamers RL, Schuurman R, Sigaloff KC, Wallis CL, Kityo C, Siwale M, et al. Effect of pretreatment HIV-1 drug resistance on immunological, virological, and drug-resistance outcomes of first-line antiretroviral treatment in sub-Saharan Africa: a multicentre cohort study. Lancet Infect Dis. 2012;12(4):307–317. doi: 10.1016/S1473-3099(11)70255-9. [DOI] [PubMed] [Google Scholar]
- 26.Kiwanuka N, Laeyendecker O, Quinn TC, Wawer MJ, Shepherd J, Robb M, et al. HIV-1 subtypes and differences in heterosexual HIV transmission among HIV-discordant couples in Rakai, Uganda. AIDS. 2009;23(18):2479–2484. doi: 10.1097/QAD.0b013e328330cc08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Trask SA, Derdeyn CA, Fideli U, Chen Y, Meleth S, Kasolo F, et al. Molecular epidemiology of human immunodeficiency virus type 1 transmission in a heterosexual cohort of discordant couples in Zambia. J Virol. 2002;76(1):397–405. doi: 10.1128/JVI.76.1.397-405.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rimawi BH, Johnson E, Rajakumar A, Tao S, Jiang Y, Gillespie S, et al. Pharmacokinetics and Placental Transfer of Elvitegravir, Dolutegravir, and Other Antiretrovirals during Pregnancy. Antimicrob Agents Chemother. 2017;61(6) doi: 10.1128/AAC.02213-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kraft CS, Basu D, Hawkins PA, Hraber PT, Chomba E, Mulenga J, et al. Timing and source of subtype-C HIV-1 superinfection in the newly infected partner of Zambian couples with disparate viruses. Retrovirology. 2012;9:22. doi: 10.1186/1742-4690-9-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dilernia DA, Chien JT, Monaco DC, Brown MP, Ende Z, Deymier MJ, et al. Multiplexed highly-accurate DNA sequencing of closely-related HIV-1 variants using continuous long reads from single molecule, real-time sequencing. Nucleic Acids Res. 2015;43(20):e129. doi: 10.1093/nar/gkv630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rhee SY, Gonzales MJ, Kantor R, Betts BJ, Ravela J, Shafer RW. Human immunodeficiency virus reverse transcriptase and protease sequence database. Nucleic Acids Res. 2003;31(1):298–303. doi: 10.1093/nar/gkg100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wall KM, Kilembe W, Vwalika B, Haddad LB, Lakhi S, Onwubiko U, et al. Sustained effect of couples’ HIV counselling and testing on risk reduction among Zambian HIV serodiscordant couples. Sexually transmitted infections. 2017 doi: 10.1136/sextrans-2016-052743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lahuerta M, Ue F, Hoffman S, Elul B, Kulkarni SG, Wu Y, et al. The problem of late ART initiation in Sub-Saharan Africa: a transient aspect of scale-up or a long-term phenomenon? J Health Care Poor Underserved. 2013;24(1):359–383. doi: 10.1353/hpu.2013.0014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rosen S, Fox MP. Retention in HIV care between testing and treatment in sub-Saharan Africa: a systematic review. PLoS Med. 2011;8(7):e1001056. doi: 10.1371/journal.pmed.1001056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Broder S. The development of antiretroviral therapy and its impact on the HIV-1/AIDS pandemic. Antiviral Res. 2010;85(1):1–18. doi: 10.1016/j.antiviral.2009.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ndahimana J, Riedel DJ, Mwumvaneza M, Sebuhoro D, Uwimbabazi JC, Kubwimana M, et al. Drug resistance mutations after the first 12 months on antiretroviral therapy and determinants of virological failure in Rwanda. Trop Med Int Health. 2016;21(7):928–935. doi: 10.1111/tmi.12717. [DOI] [PubMed] [Google Scholar]
- 37.Cori A, Ayles H, Beyers N, Schaap A, Floyd S, Sabapathy K, et al. HPTN 071 (PopART): a cluster-randomized trial of the population impact of an HIV combination prevention intervention including universal testing and treatment: mathematical model. PLoS One. 2014;9(1):e84511. doi: 10.1371/journal.pone.0084511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Huang A, Hogan JW, Luo X, DeLong A, Saravanan S, Wu Y, et al. Global Comparison of Drug Resistance Mutations After First-Line Antiretroviral Therapy Across Human Immunodeficiency Virus-1 Subtypes. Open Forum Infect Dis. 2016;3(2):ofv158. doi: 10.1093/ofid/ofv158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Liuzzi G. Genotypic resistance tests for the management of the patient failing highly active antiretroviral therapy: the resistance pattern in different biological compartments. Scand J Infect Dis Suppl. 2003;106:90–93. [PubMed] [Google Scholar]
- 40.Santoro MM, Perno CF. HIV-1 Genetic Variability and Clinical Implications. ISRN Microbiol. 2013;2013:481314. doi: 10.1155/2013/481314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wainberg MA, Brenner BG. The Impact of HIV Genetic Polymorphisms and Subtype Differences on the Occurrence of Resistance to Antiretroviral Drugs. Mol Biol Int. 2012;2012:256982. doi: 10.1155/2012/256982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Orrell C, Cohen K, Leisegang R, Bangsberg DR, Wood R, Maartens G. Comparison of six methods to estimate adherence in an ART-naive cohort in a resource-poor setting: which best predicts virological and resistance outcomes? AIDS Res Ther. 2017;14(1):20. doi: 10.1186/s12981-017-0138-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Quinn TC. Viral load, circumcision and heterosexual transmission. Hopkins HIV Rep. 2000;12(3):1, 5, 11. [PubMed] [Google Scholar]
- 44.Wawer MJ, Gray RH, Sewankambo NK, Serwadda D, Li X, Laeyendecker O, et al. Rates of HIV-1 transmission per coital act, by stage of HIV-1 infection, in Rakai, Uganda. J Infect Dis. 2005;191(9):1403–1409. doi: 10.1086/429411. [DOI] [PubMed] [Google Scholar]
- 45.Lorello G, la Porte C, Pilon R, Zhang G, Karnauchow T, MacPherson P. Discordance in HIV-1 viral loads and antiretroviral drug concentrations comparing semen and blood plasma. HIV Med. 2009;10(9):548–554. doi: 10.1111/j.1468-1293.2009.00725.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.