

Abstract
Background
Improved medical practice efficiency has been demonstrated by physicians using mobile device (mobile phones, tablets) electronic medical record (EMR) systems. However, the quantitative effects of these systems have not been adequately measured.
Objective
This study aimed to determine the effectiveness of near-field communication (NFC) integrated with a mobile EMR system regarding physician turnaround time in a hospital emergency department (ED).
Methods
A simulation study was performed in a hospital ED. Twenty-five physicians working in the ED participated in 2 scenarios, using either a mobile device or personal computer (PC). Scenario A involved randomly locating designated patients in the ED. Scenario B consisted of accessing laboratory results of an ED patient at the bedside. After completing the scenarios, participants responded to 10 questions that were scored using a system usability scale (SUS). The primary metric was the turnaround time for each scenario. The secondary metric was the usability of the system, graded by the study participants.
Results
Locating patients from the ED entrance took a mean of 93.0 seconds (SD 34.4) using the mobile scenario. In contrast, it only required a mean of 57.3 seconds (SD 10.5) using the PC scenario (P<.001). Searching for laboratory results of the patients at the bedside required a mean of only 25.2 seconds (SD 5.3) with the mobile scenario, and a mean of 61.5 seconds (SD 11.6) using the PC scenario (P<.001). Sensitivity analysis comparing only the time for login and accessing the relevant information also determined mobile devices to be significantly faster. The mean SUS score of NFC-mobile EMR was 71.90 points.
Conclusions
NFC integrated with mobile EMR provided for a more efficient physician practice with good usability.
Keywords: near-field communication, electronic medical records, emergency department, mobile health, mHealth
Introduction
Background
An emergency department (ED) is often characterized by chaos and inefficiency [1]. It is where the severity of a patient’s injury or distress varies and changes unpredictably. The location of patients also changes based on their clinical process or test results, which may become available at different times. Physicians need to check changed locations and laboratory results frequently by walking back and forth between personal computer (PC) stations and patients’ beds. In a fast-paced ED, such interruptions cause physicians to waste a substantial amount of time and ultimately result in patient dissatisfaction [2]. As the installation of PCs to all bedsides is costly and ineffective regarding space utilization, better alternatives must be considered.
Related Technologies
The ED providers strive to improve the efficiency of the workflow by exploiting advanced technologies. With the emergence of electronic medical records (EMR), mobile EMR systems are receiving increasing attention as mobile devices (ie, mobile phones, tablets), and mobile apps are becoming more common [3,4]. The portability and near ubiquity of mobile EMR allow health care providers to access patient records wherever they are needed [5].
Near-field communication (NFC) is widely used in various communication apps. In the field of health care, usage scenarios including patient identification [6], blood transfusion [7], drug administration [8], medical staff tracking [9], and medical record access [10] have already been proven. The wave of NFC technology in the health care field has been combined with the internet of things technologies [11]. Through a combination of mobile EMR systems, NFC technology can improve workflow using bedside technology [12].
Study Objectives
Numerous studies have investigated the qualitative and quantitative benefits of each technology separately [12-14]. However, the efficacy of the combined technologies for improved physician productivity in health care has not been investigated to date. More rigorous quantitative studies investigating usability estimates are required to develop and eventually adopt such systems in practice. Additionally, it is essential to determine a system’s effectiveness in clinical settings. This study aims to determine the effectiveness of an NFC-integrated mobile EMR system regarding physician turnaround time in an ED.
Methods
Study Setting
This simulation study took place in an academic ED in Seoul, South Korea. The study was reviewed and approved by the Samsung Medical Center Institutional Review Board (IRB no. SMC 2018-01-144-001).
The ED is part of a tertiary academic teaching hospital with approximately 9000 daily outpatients and 2000 inpatient beds [15]. The ED holds 69 treating beds. The number of annual visits is approximately 79,000. Although the ED is heavily equipped with PCs at each station (84 PCs total), there are no PCs at the bedsides. Most of the beds are not in private rooms but are open to stations except isolation beds.
The hospital developed the proposed mobile EMR system. It operates on the institution’s EMR system, which was also developed internally. The overall system had a significant update in July 2016. Figure 1 shows a schematic of the architecture of the EMR system.
Figure 1.
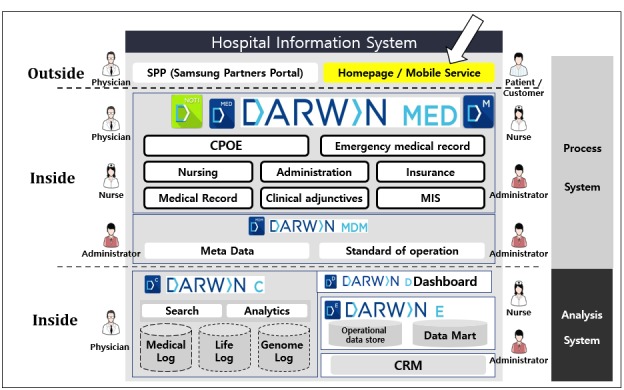
Overall schematic description of the hospital information system architecture relationship at the Samsung Medical Center. DARWIN: data analytics and research window for integrated knowledge; CPOE: computerized physician order entry; MIS: management information system; MDM: master data management; CRM: customer relationship management.
The mobile EMR uses an Android app that gives physicians access to inpatient, outpatient, and emergency department information. Users can log into the system with their fingerprint and search for locations, clinical notes, vital signs, laboratory results, and medical images. The NFC function was implemented in April 2017. When a physician links the EMR mobile device to an NFC tag which contains information about its location, the mobile app is automatically initiated. Using fingerprint authentication, physicians can log in and view the EMR of patients at the location that corresponds with their NFC location. When tagging NFC tags at the entrance of a specific zone, the list of patients at the tagged NFC zone who are in charge of mobile device users is popped up. Figure 2 shows the access process.
Figure 2.
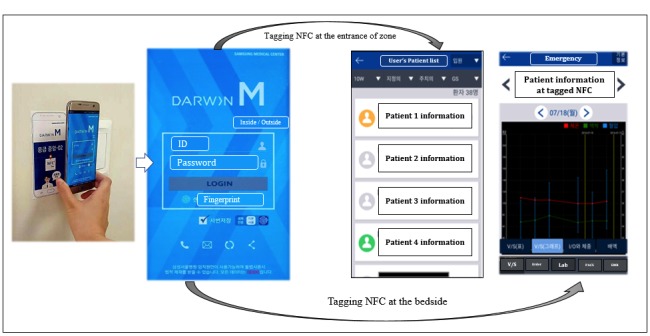
Usage scene when the mobile electronic medical records (EMR) communicate with the near-field communication (NFC) system and the display of the mobile EMR progression after tagging NFC. V/S: vital sign.
Study Participants
Physicians who worked in the ED during the study were asked to participate. Physician participants were recruited between April 1 to April 20, 2018. Among the 35 ED physicians, 25 (71%) agreed to participate in this study.
Study Scenarios and Sensitivity Analysis
After a brief introduction, the physicians went through 2 sequential scenarios. The first scenario (scenario A) involved locating patients in the ED from the ED gate. Physicians were given the name of a patient and were required to locate them using either a PC EMR at the nearest site in the ED gate or mobile EMR. After locating the patient, the participant was guided to reach their bedside. The second scenario (scenario B) involved looking up a laboratory result from the bedside. Physicians were brought to a patient’s bedside and were required to determine a specific laboratory result using either a mobile device or PC interface. As there were no PCs at the bedside, physicians had to perform a few steps to identify available PCs and return with a report. The steps in each scenario are shown in Figure 3, and the flow of each scenario is shown in Figure 4.
Figure 3.
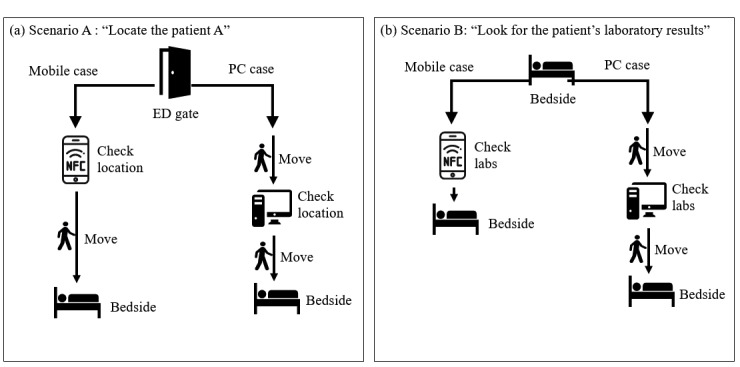
Schematic view of simulation scenarios. (a) Locating the patient. (b) Looking up laboratory results for the patient. ED: emergency department; PC: personal computer.
Figure 4.
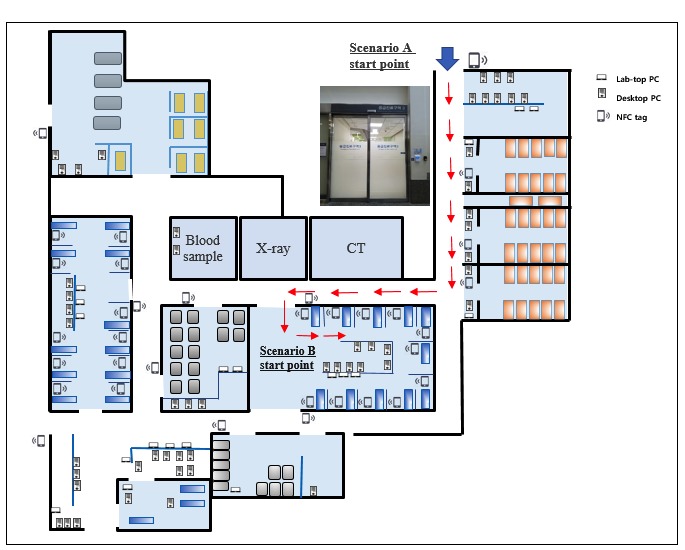
The flow of locating the patient and the scenario place in the emergency department. CT: computed tomography; NFC: near-field communication; PC: personal computer.
Physicians were randomly assigned to follow either scenario A or B using either a mobile device (mobile case) or a PC (PC case) as described in Multimedia Appendix 1. An independent observer recorded the activities with a camera and completed a case report form with time stamps during the process. Patients were not simulated. Real patients were accessed in the emergency department. However, since we used only partial patient data such as name, location, and laboratory data which was already available, the clinical condition did not influence the study’s outcome.
We performed a sensitivity analysis using the data without considering movement intervals. This test was performed to determine whether or not there was a consistent outcome if the condition allowed for more available PCs, which are at the gate and the bedside.
Survey
After completing all scenarios, physician participants responded to 10 questions using the system usability scale (SUS). The SUS is composed of a 5-point Likert scale rated from 1 (strongly disagree) to 5 (strongly agree) that investigates the usability of the NFC-integrated mobile EMR system [16]. The SUS score calculation formula is as follows:

Measurement and Outcome
The primary metric was the length of turnaround time for each scenario. The secondary metric was the usability of the system, as graded by the study physician participants. We collected demographic data from each participant and recorded the time intervals of each step of the process for both scenarios. We also analyzed time intervals among groups sorted by age, gender, and occupation. Afterward, the SUS questionnaires were collected and analyzed.
Statistical Analysis
Continuous variables are expressed in terms of mean and standard deviations (SD), whereas categorical variables are expressed in frequencies and percentages. The time mean difference was examined using a paired t-test. A value of P<.05 was considered to be statistically significant. As descriptive statistics could not confirm a normal distribution of participants between the 2 dependent groups divided by age, gender, and occupation, the Mann-Whitney U test was applied for time interval difference analysis.
Results
Main Outcome
Among 25 physician participants, 14 (56%) were male, and 11 (44%) were female. The general characteristics of the participants are shown in Table 1.
Table 1.
Characteristics of the physician participants.
| Participant characteristic | Value | ||
| Age (years), mean (SD) | 30.6 (4.9) | ||
| Age groups (years), n (%) | |||
| ≥30 | 12 (48) | ||
| <30 | 13 (52) | ||
| Gender, n (%) | |||
| Male | 14 (56) | ||
| Female | 11 (44) | ||
| Occupation, n (%) | |||
| Intern | 4 (16) | ||
| Resident | 15 (60) | ||
| Specialist | 6 (24) | ||
| Time worked at hospital (years), mean (SD) | 4.6 (4.0) | ||
It required a mean of 93.0 seconds (SD 34.4) to locate the patient from the entrance of the ED in the PC case but only a mean of 57.3 seconds (SD 10.5) in the mobile case, which was significantly faster (P<.001). Accessing laboratory results at the patient’s bedside required a mean of only 25.2 seconds (SD 5.3) in the mobile case compared to a mean of 61.5 seconds (SD 11.6) in the PC case. These data were statistically significant (P<.001). A schematic comparison is shown in Figure 5.
Figure 5.
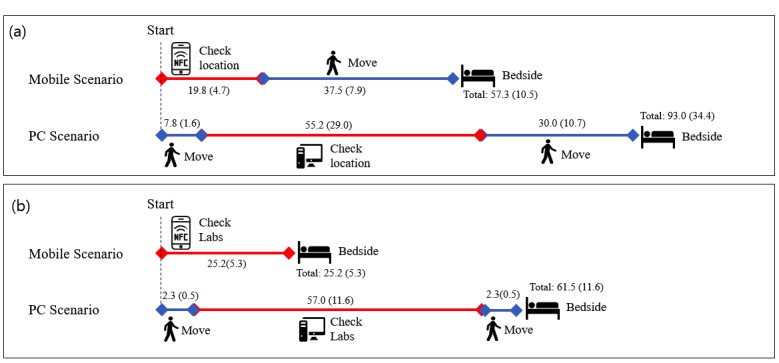
Graphical view of main results. (a) Locating the patient. (b) Looking up laboratory results for the patient. NFC: near-field communication; PC: personal computer.
Sensitivity Analysis
We compared the time required for login with the time for finding relevant information. Login using the mobile device EMR required a mean of 13.1 seconds (SD 2.9) for scenario A and a mean of 12.5 seconds (SD 2.1) for scenario B. Login by PC took longer with a mean of 36.2 seconds (SD 15.2) for scenario A and a mean of 30.5 seconds (SD 7.7) for scenario B. The differences in time were statistically significant (P<.001). Finding the location of patients after login required a mean of only 6.8 seconds (SD 3.6) using the mobile device, whereas it took a mean of 18.9 seconds (SD 16.9) using a PC. Accessing a specific laboratory test result required a mean of 12.8 seconds (SD 5.3) using the mobile device and a mean of 26.5 seconds (SD 8.0) using a PC. These data were statistically significant (P<.001). The results are shown in Table 2.
Table 2.
A comparison between the 2 scenarios of time spent on specific tasks.
| Task | Time (seconds), mean (SD) | P value | ||||
| Mobile case | Personal computer case | |||||
| Scenario A | ||||||
| Login | 13.1 (2.9) | 36.2 (15.2) | <.001 | |||
| Accessing relevant information | 6.8 (3.6) | 18.9 (16.9) | <.001 | |||
| Total | 19.8 (4.7) | 55.2 (29.0) | <.001 | |||
| Scenario B | ||||||
| Login | 12.5 (2.1) | 30.5 (7.7) | <.001 | |||
| Accessing relevant information | 12.8 (5.3) | 26.5 (8.0) | <.001 | |||
| Total | 25.2 (5.3) | 57.0 (11.6) | <.001 | |||
Survey
The mean SUS score of NFC-mobile EMR was 71.90 points. The results are shown in Table 3.
Table 3.
Score results (n=25) from the system usability scale (SUS) to assess the near-field communication mobile emergency medical record (NFC-mobile EMR).
| Question | Mean (SD) |
| 1. I think that I would like to use this NFC-mobile EMR frequently. | 3.92 (0.95) |
| 2. I found the NFC-mobile EMR unnecessarily complex. | 1.76 (0.83) |
| 3. I thought the NFC-mobile EMR was easy to use. | 4.40 (0.50) |
| 4. I think that I would need the support of a technical person to be able to use the NFC-mobile EMR. | 2.72 (1.10) |
| 5. I found that the various functions in the NFC-mobile EMR were well-integrated. | 4.24 (0.72) |
| 6. I thought there was too much inconsistency in the NFC-mobile EMR. | 4.20 (0.64) |
| 7. I would imagine that most people would learn to use the NFC-mobile EMR very quickly. | 4.48 (0.59) |
| 8. I found the NFC-mobile EMR very cumbersome to use. | 1.56 (0.51) |
| 9. I felt very confident using the NFC-mobile EMR. | 3.88 (0.78) |
| 10. I needed to learn a lot of things before I could get going with the NFC-mobile EMR. | 1.92 (0.57) |
| Total score | 71.90 (7.61) |
Discussion
Principal Findings
This study aimed to improve physician efficiency by reducing the time spent walking to check patient information with the aid of the technological integration between NFC and mobile device EMR. To the best of our knowledge, this is the first study to examine the efficiency of this system and comparing it with the PC EMR. The mobile total turnaround time for performing tasks was significantly reduced in both scenarios. Sensitivity analysis showed that mobile device EMR incorporated with NFC was significantly faster than PC-integrated EMR regarding login time and accessing laboratory results.
As the familiarity of mobile device use could be different among the demographic groups, we compared the total time interval difference between PC and mobile cases. Multimedia Appendix 2 shows that the mobile case was consistently faster for all groups. However, there were significant differences in the time interval between age and occupation during scenario B. These findings are contrary to the general belief that the younger generation is more familiar with newer technology [17]. A further study on mobile device familiarity is needed because the simulation was done with a small sample size.
We also evaluated usability with the SUS questionnaire. The SUS was used after the physician participant had an opportunity to use the system being evaluated. A score over 70 on the questionnaire (range 0-100) indicated that the NFC-integrated mobile device EMR was “acceptable,” and the adjective rating was “good” [18]. There was no significant statistical difference among groups based on age, gender, and occupation.
Advantages and Disadvantages
Various measures have been implemented to address ED inadequacies. Improving the ED work efficiency is one crucial in-hospital factor. Ideal physical structures for work have already been demonstrated [19]. Several studies have shown the positive effect of developing clinical guidelines and protocols for effective evaluation of efficiency [20,21]. Newer technologies such as radio frequency identification-integrated point-of-care testing [22], triage kiosks [23], and dashboards [24] have been well studied. Ubiquitous near patient access to EMR via NFC is determined to be useful in this regard. Compared to installing new structures in an already heavily equipped ED, implementing an NFC tag system is a relatively easy way to improve workflow regarding cost and space utilization.
As most mobile EMR functions are more readily accessible with PCs, our study paid attention to superiority only available in mobile EMR. Mobile device systems outperform PC systems concerning mobility and personalization (at the provider level, and patient level). We have measured the turnaround time as the primary outcome of these merits. Thus, we have shown that physicians can gain access to information without physically moving the location of their patients.
Portability of mobile EMR could be improved by incorporating accessibility through NFC. Our study revealed a statistically significant difference in login time which was more effective by mobile EMR than by PC EMR (Table 2). A previous study by Holden [25] demonstrated that the issue of accessibility to EMR such as system login and system response time could negatively impact the usability of mobile EMR. NFC integrated response and fingerprint login at the location of interest using a mobile device could be beneficial because the process is simplified and less time-consuming. This system also appears to reduce security concerns from failed logouts or departure without logging out, by using the individual’s mobile device.
An increase in the length of time physicians spend at the bedside is likely to increase patient satisfaction [26]. With this bedside technology, the physician can show radiologic results or laboratory results to patients who cannot ambulate.
Inconsistent loading time due to varying network coverage could be a disadvantage for this technology. For example, mobile devices without NFC function cannot be used. Physicians might routinely tend to use PC EMR because PC EMR covers mobile EMR. A previous study by Duhm et al [14] demonstrated that a physician usually underestimates actual time savings during their professional capacity. The results of this study make a compelling argument and provide preliminary evidence in support of adequately addressing this tendency, particularly concerning reduced workflow using mobile EMR with NFC functionality.
However, to enhance emergency physician performance, a multidimensional approach is required, rather than a single tool. ED processes are complicated, with multiple steps from various providers often originating from outside the ED.
Limitations
First among the limitations of this study is that this investigation was conducted at a single center. Additional studies conducted at multiple centers or EDs are needed to improve the generalizability of our conclusions.
Secondly, participants had different levels of familiarity with mobile devices and NFC tags. Only some participants were familiar with NFC because the system was built over a year ago, which might cause bias.
Thirdly, each participant encountered various encumbrances because this study was conducted in an actual emergency room. For example, when attempting to locate a patient in the middle of a scenario, the nearest PC may have been occupied by another staff member, which led to the physician being forced to use a PC that was further away. Also, while moving to a patient’s bedside, there was an occasion when a participant was forced to stop because a moving stretcher cart or medical staff member blocked the aisle. In addition, some of the PCs used were comparatively slow. As mentioned above, unpredictable circumstances might influence the overall time measured for each scenario. As shown in Multimedia Appendix 3, the variability of turnaround time fluctuated. However important, these events could not be systemically quantified.
Finally, the usability assessment for NFC-mobile EMR via SUS could be overrated because responses were filled out immediately after performing scenarios, which in most cases, resulted in the superiority of NFC-mobile EMR. Further studies could investigate usability over a more extended period of the physician’s working practice.
Conclusion
NFC-integrated mobile EMR is effective for reducing the turnaround time of physicians when practicing in the field and has excellent usability.
Acknowledgments
The authors would like to acknowledge the support provided by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (grant number 2018R1C1B6002877).
Abbreviations
- ED
emergency department
- EMR
emergency medical record
- NFC
near-field communication
- PC
personal computer
- SUS
system usability scale
Randomly allocated scenario quest for each participant. PC: personal computer.
Comparison of time spent among age, gender, and occupation for each scenario.
Graphical comparison between mobile and personal computer scenario time of all participants.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Berger E. Breaking point: Report calls for Congressional rescue of hospital emergency departments. Ann Emerg Med. 2006 Aug;48(2):140–2. doi: 10.1016/j.annemergmed.2006.06.022. [DOI] [PubMed] [Google Scholar]
- 2.Weigl M, Beck J, Wehler M, Schneider A. Workflow interruptions and stress atwork: a mixed-methods study among physicians and nurses of a multidisciplinary emergency department. BMJ Open. 2017 Dec 22;7(12):e019074. doi: 10.1136/bmjopen-2017-019074. http://bmjopen.bmj.com/cgi/pmidlookup?view=long&pmid=29275350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kim J, Lee Y, Lim S, Lee J. How Are Doctors Using Mobile Electronic Medical Records? An In-Depth Analysis of the Usage Pattern. Stud Health Technol Inform. 2017;245:1231. [PubMed] [Google Scholar]
- 4.Yeo K, Lee K, Kim J, Kim T, Choi Y, Jeong W, Hwang H, Baek RM, Yoo S. Pitfalls and Security Measures for the Mobile EMR System in Medical Facilities. Healthc Inform Res. 2012 Jun;18(2):125–35. doi: 10.4258/hir.2012.18.2.125. https://www.e-hir.org/DOIx.php?id=10.4258/hir.2012.18.2.125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Burdette SD, Herchline TE, Oehler R. Surfing the web: practicing medicine in a technological age: using smartphones in clinical practice. Clin Infect Dis. 2008 Jul 01;47(1):117–22. doi: 10.1086/588788. [DOI] [PubMed] [Google Scholar]
- 6.Aguilar A, van der Putten W, Kirrane F. Positive patient identification using RFID and wireless networks. 11th Annual Conference and Scientific Symposium (HISI); November 2006; Dublin, Ireland. 2006. Nov, [Google Scholar]
- 7.Gutierrez A, Levitt J, Reifert D, Raife T, Diol B, Davis R, Veeramani R. Tracking blood products in hospitals using radio frequency identification: Lessons from a pilot implementation. VOXS. 2013 May 31;8(1):65–69. doi: 10.1111/voxs.12015. [DOI] [Google Scholar]
- 8.Houliston B. Integrating RFID technology into a drug administration system. Journal of Applied Computing and Information; HIC 2005 and HINZ 2005: Proceedings; 2005; Brunswick East, Vic.: Health Informatics Society of Australia. 2005. pp. 453–461. [Google Scholar]
- 9.Halamka J. Early experiences with positive patient identification. J Healthc Inf Manag. 2006;20(1):25–7. [PubMed] [Google Scholar]
- 10.Ajami S, Rajabzadeh A. Radio Frequency Identification (RFID) technology and patient safety. J Res Med Sci. 2013 Sep;18(9):809–13. http://europepmc.org/abstract/MED/24381626. [PMC free article] [PubMed] [Google Scholar]
- 11.Lee BM, Ouyang J. Intelligent Healthcare Service by using Collaborations between IoT Personal Health Devices. IJBSBT. 2014 Feb 28;6(1):155–164. doi: 10.14257/ijbsbt.2014.6.1.17. [DOI] [Google Scholar]
- 12.Köstinger H, Gobber M, Grechenig T, Tappeiner B, Schramm W. Developing an NFC based patient identification and ward round system for mobile devices using the android platform. Point-of-Care; 2013 IEEE Point-of-Care Healthcare Technologies (PHT); 16-18 Jan. 2013; Bangalore, India. 2013. Jan 16, p. 2013. [Google Scholar]
- 13.Free C, Phillips G, Felix L, Galli L, Patel V, Edwards P. The effectiveness of M-health technologies for improving health and health services: a systematic review protocol. BMC Res Notes. 2010 Oct 06;3:250. doi: 10.1186/1756-0500-3-250. https://bmcresnotes.biomedcentral.com/articles/10.1186/1756-0500-3-250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Duhm J, Fleischmann R, Schmidt S, Hupperts H, Brandt SA. Mobile Electronic Medical Records Promote Workflow: Physicians' Perspective From a Survey. JMIR Mhealth Uhealth. 2016 Jun 06;4(2):e70. doi: 10.2196/mhealth.5464. http://mhealth.jmir.org/2016/2/e70/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cha WC, Ahn KO, Shin SD, Park JH, Cho JS. Emergency Department Crowding Disparity: a Nationwide Cross-Sectional Study. J Korean Med Sci. 2016 Aug;31(8):1331–6. doi: 10.3346/jkms.2016.31.8.1331. https://jkms.org/DOIx.php?id=10.3346/jkms.2016.31.8.1331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jordan Pw, Thomas B, Weerdmeester Ba, McClelland I. Usability Evaluation in Industry. Bristol, PA, USA: Florence, Kentucky, U.S.A.: Taylor & Francis; 1996. SUS-A quick and dirty usability scale; pp. 189–194. [Google Scholar]
- 17.McAlearney AS, Schweikhart SB, Medow MA. Doctors' experience with handheld computers in clinical practice: qualitative study. BMJ. 2004 May 15;328(7449):1162. doi: 10.1136/bmj.328.7449.1162. http://europepmc.org/abstract/MED/15142920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bangor A, Kortum P, Miller J. Determining what individual SUS scores mean: adding an adjective rating scale. J Usability Studies. 2009 May;4(3):114–123. [Google Scholar]
- 19.Zusman E. Form facilitates function: innovations in architecture and design drive quality and efficiency in healthcare. Neurosurgery. 2010 Jun;66(6):N24. doi: 10.1227/01.neu.0000375281.91778.45. [DOI] [PubMed] [Google Scholar]
- 20.Butti L, Bierti O, Lanfrit R, Bertolini R, Chittaro S, Delli CS, Del RD, Mancusi RL, Pertoldi F. Evaluation of the effectiveness and efficiency of the triage emergency department nursing protocol for the management of pain. J Pain Res. 2017;10:2479–2488. doi: 10.2147/JPR.S138850. doi: 10.2147/JPR.S138850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wright S, Trott A, Lindsell C, Smith C, Gibler W. Evidence-based emergency medicine. Creating a system to facilitate translation of evidence into standardized clinical practice: a preliminary report. Ann Emerg Med. 2008 Jan;51(1):80–6, 86.e1. doi: 10.1016/j.annemergmed.2007.04.009. [DOI] [PubMed] [Google Scholar]
- 22.Rao A, Dighe A. Radiofrequency Identification and Point-of-Care Testing. Point of Care: The Journal of Near-Patient Testing & Technology. 2004;3(3):130–134. doi: 10.1097/01.poc.0000138646.56228.65. [DOI] [Google Scholar]
- 23.Ackerman S, Tebb K, Stein J, Frazee B, Hendey G, Schmidt L, Gonzales R. Benefit or burden? A sociotechnical analysis of diagnostic computer kiosks in four California hospital emergency departments. Soc Sci Med. 2012 Dec;75(12):2378–85. doi: 10.1016/j.socscimed.2012.09.013. [DOI] [PubMed] [Google Scholar]
- 24.Swartz J, Cimino J, Fred M, Green Robert A, Vawdrey David K. Designing a clinical dashboard to fill information gaps in the emergency department. AMIA Annu Symp Proc. 2014;2014:1098–104. http://europepmc.org/abstract/MED/25954420. [PMC free article] [PubMed] [Google Scholar]
- 25.Holden RJ. Physicians' beliefs about using EMR and CPOE: in pursuit of a contextualized understanding of health IT use behavior. Int J Med Inform. 2010 Feb;79(2):71–80. doi: 10.1016/j.ijmedinf.2009.12.003. http://europepmc.org/abstract/MED/20071219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lin CT, Albertson GA, Schilling LM, Cyran EM, Anderson SN, Ware L, Anderson RJ. Is patients' perception of time spent with the physician a determinant of ambulatory patient satisfaction? Arch Intern Med. 2001 Jun 11;161(11):1437–42. doi: 10.1001/archinte.161.11.1437. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Randomly allocated scenario quest for each participant. PC: personal computer.
Comparison of time spent among age, gender, and occupation for each scenario.
Graphical comparison between mobile and personal computer scenario time of all participants.