

Abstract
Background and Objectives:
People who are afraid of heights may have a perceptual bias, such that they see heights as higher than they truly are. The current study tested if there is a causal relationship between treatments for height fear and changes in perceptual bias.
Methods:
Specifically, the effects on perceptual bias following three height fear interventions (exposure, cognitive bias modification for interpretations, and a combination of exposure and cognitive bias modification) and a control condition were examined in individuals with an extreme fear of heights (N=107).
Results:
Results provided preliminary evidence that some height fear interventions reduce perceptual bias. Specifically, participants that completed exposure had a significant decrease in perceptual bias, and participants in the cognitive bias modification and combination conditions had decreases in perceptual bias at the level of non-significant trends, while no reduction occurred for the control condition.
Limitations:
Limitations of this study include that the hypothesis was largely informed by data from a parent study and that the effect sizes were small; thus, replicating these results is warranted.
Conclusions:
These findings suggest that there may be a causal relationship between height fear treatments and altered perception of heights.
Keywords: acrophobia, height fear, perceptual bias, exposure, cognitive bias modification
People with a fear of heights may see heights differently from non-fearful people. For instance, people high (vs. low) in height fear tend to overestimate heights when viewed from above (Teachman, Stefanucci, Clerkin, Cody, & Proffitt, 2008). Further, perceptual overestimation of heights is associated with both trait and state fear of heights (Stefanucci & Proffitt, 2009). However, these correlational findings leave critical questions unanswered about the causal relationship between height fear (acrophobia) treatments and visual perception. Bias in visual perception is distinct from constructs modulated by cognitive processes, such as reported fear or cognitive bias, and may thus represent automatic processes that develop and/or maintain anxiety disorders (Teachman et al., 2008). Despite the potential significance of bias in visual perception, no study to our knowledge has investigated the malleability of this bias. The current study uses an experimental design to test the malleability of perceptual bias by assessing perception of heights before and after height fear interventions. In contrast to other studies that have relied upon self-reported visual perception (Rachman & Cuk, 1992; Stefanucci, Proffitt, Clore, & Parekh, 2008), we used a visual matching task designed to capture what participants truly saw, distinct from their interpretations, beliefs, and other cognitive phenomena (Clerkin, Cody, Stefanucci, Proffitt, & Teachman, 2009; Teachman et al., 2008).
Acrophobia treatments challenge beliefs about the dangerousness of heights, and this change in perceived risks associated with heights may influence visual perception. This idea follows from theories of embodied perception, which suggest that visual perception is affected by individuals’ assessments of the opportunities and risks of action (Proffitt, 2006). Thus, manipulating the perceived risks of being on heights may exacerbate visual perceptual bias of heights, especially for height-fearful relative to non-fearful people (Clerkin et al., 2009).
Together, this prior work suggests that acrophobia treatments may influence perceptual bias via altering interpretations that heights are risky. Interventions that target exaggerated beliefs about the risks of being on heights, such as Cognitive Bias Modification for Interpretations (CBM-I), may thus affect height perception. CBM-I is a computerized intervention intended to shift people’s interpretations of ambiguous scenarios to be more benign and less threatening. CBM-I has increased adaptive interpretations across a range of anxiety problems (see Hallion & Ruscio, 2011). Similarly, exposure therapy, the gold-standard treatment for acrophobia, provides novel experiences that may reduce the evaluation of heights as risky. In exposure therapy, people confront feared stimuli and remain in those situations so that they learn they can tolerate their anxiety (Craske et al., 2008; Foa & Kozak, 1986). Exposure therapy has been shown to be consistently effective in reducing acrophobia (Baker et al., 2010; Emmelkamp & Felten, 1985).
In the current study, we investigated the malleability of perceptual bias by testing if acrophobia interventions affect perception in individuals with extreme height fear. Perceptions of heights were measured before and after two height fear intervention sessions (i.e.,CBM-I, exposure therapy, a combination of CBM-I and exposure therapy (combined), or a sham CBM-I condition [control]). Prior research using the current dataset demonstrated that all active conditions (CBM-I, exposure, and combined) reduced height fear overall, compared with the control condition (Steinman & Teachman, 2014). Interestingly, the lack of a synergistic effect of the combined intervention is consistent with other research suggesting that combining effective treatments may not lead to better outcomes (Foa et al., 2005). In the present study, we extended this research by investigating whether height fear interventions shift perceptual bias. We hypothesized that all height fear intervention conditions, relative to the control, would reduce visual perceptual bias. Further, we hypothesized that the influence of condition on change in perceptual bias would be mediated by change in interpretation bias.
Method
Participants
To be eligible, participants needed to have Acrophobia Questionnaire-Anxiety subscale scores of at least 45.45 (AQ-Anxiety; Cohen, 1972, 1977), and to score in the subthreshold or threshold range on the Specific Phobia section of the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders (4th ed., SCID; First, Spitzer, Gibbon, & Williams, 1994). See Steinman and Teachman (2014) for a CONSORT diagram for the parent study. Following treatment assignment (N=114), four participants were excluded (due to experimenter error, n=3, or false reporting, n=1). Three of the 110 participants whose data were analyzed in the parent study did not complete the perceptual bias measures, and were thus excluded from analyses in the present study. This resulted in a final sample of 107 participants (76.6% female), with 28 participants in the control condition, 26 in the exposure condition, 27 in the CBM condition, and 26 in the combined condition. Mean age of the sample was 23.58 years (SD=11.46, range=18–67). Reported race was White (68.2%), Asian (17.8%), Black/African American (7.5%), bi-or multi-racial (4.7%), and other (1.9%).
Materials1
Height fear.
Participants completed the AQ-Anxiety (Cohen, 1977), a 20-item questionnaire measuring fear of various heights (e.g., “Riding a Ferris wheel”). Cronbach’s alpha was .72 at pre-intervention and .89 at post-intervention.
Interpretation bias.
Participants’ interpretation of risks associated with heights was evaluated with the Heights Interpretation Questionnaire (HIQ; Steinman & Teachman, 2011). Participants were asked to read and imagine themselves in two height-relevant scenarios (e.g., climbing a ladder) and rate the likelihood of eight interpretations related to each scenario (e.g., “You will fall”) on a 5-point scale. Cronbach’s alp ha was .89 at pre-intervention and .93 at post-intervention.
Visual perceptual bias.
To assess visual perception of heights, participants completed a visual matching task designed to minimize the influence of explicit cognitive processes (e.g., Clerkin et al., 2009; Teachman et al., 2008). Prior to the task, participants completed a guided imagery exercise in which they imagined themselves falling off the 26-foot high balcony (modified from Clerkin et al., 2009). Next, participants looked over the balcony at a disc on the ground below the balcony and positioned the experimenter to be as far away from them horizontally along the balcony as the participant was from the disc on the ground below the balcony (i.e., vertically). Participants were encouraged to look back at the disc on the ground frequently while positioning the experimenter. A ratio was computed comparing the estimated distance with the actual distance.
Height fear interventions (two sessions each).
CBM-I.
Participants in the CBM-I and combined conditions completed modifications of Interpretation Modification Program (IMP; modified from Beard & Amir, 2008) and Scenario Training (modified from Mathews & Mackintosh, 2000). In IMP, participants were trained to associate positive words (and reject negative words) with 76 ambiguous, height-relevant sentences. In each trial, participants were presented with a positive or negative word on the computer screen, followed by an ambiguous, height-relevant sentence. Participants were asked to indicate whether or not the positive or negative word and the height-relevant sentence were related, and were given positive feedback (e.g., “You are correct”) if they responded that positive words were related to the sentences or that negative words were not related to the sentences. Otherwise, they received negative feedback (e.g., “ You are incorrect”). During Scenario Training, participants read and imagined themselves in a series of 64 height-relevant ambiguous scenarios that ended with a positive, anxiety-incongruent word. Participants were instructed to read the height-relevant scenarios and complete a word fragment (which had only one solution) that resolved the ambiguity of the scenario in a positive manner. Then participants were asked to answer a comprehension question that reinforced the positive interpretation of the scenario. See Steinman and Teachman (2014) for further detail. Training examples are included in the appendix of this paper.
Control.
Participants in the control condition completed a sham variation of CBM-I. In this variation, none of the trials were emotionally ambiguous or related to height fear, although approximately 25% of the trials included height content, in order to control for effects related to reading about heights (e.g., potential arousal) and to make this condition more credible. However, the height-related items did not reference fear and did not involve resolution of emotional ambiguity. The control tasks were designed to match the CBM-I paradigms for task demands (e.g., attention, time, format) so the training looked quite similar to the active CBM condition but removed the posited active ingredients.
Exposure therapy.
Participants in the exposure and the combined conditions completed an exposure therapy treatment protocol modified from Antony, Craske, and Barlow’s (2006) fears and phobia treatment manual. Exposure therapy was comprised of: 1) psychoeducation about height fear, 2) socialization to treatment, which involved an explanation of habituation and the goals of exposure exercises, and 3) imaginal and in vivo exposures, which took place on various heights throughout the university’s campus. Participants completed exposures in a graded manner based on their individualized height fear hierarchies. During each exposure, the participant was invited to enter the feared situation and encouraged to remain in that situation while their fear decreased and the person had an opportunity to note that their feared consequences did not occur.
Procedure
Potential participants completed the AQ-Anxiety and Specific Phobia section of the SCID. Participants were told that the purpose of the study was to investigate an experimental height fear intervention. Participants were sequentially assigned to the CBM-I, exposure, combined, or the control condition.2 Following consent, participants completed a baseline session, two 90-minute intervention sessions (one week apart), and a post-intervention session. This study received approval from the university’s Institutional Review Board.
Analytic Plan
First, bivariate correlations were calculated. Second, unstandardized residual change scores were computed to capture change in the dependent variable (perceptual bias) and mediator (interpretation bias; see Hummel-Rossi & Weinberg, 1975). Third, a planned weighted contrasts Analysis of Variance (ANOVA) was conducted with condition (coded as control = +3; CBM = −1; exposure = −1; combined = −1) as the independent variable and change in perceptual bias as the dependent variable. Fourth, follow-up paired-samples t-tests were conducted to compare pre- vs. post-treatment perceptual bias scores within each condition.
Finally, the hypothesis that change in interpretation bias would mediate the relation between condition and change in perceptual bias was tested using the PROCESS macro (Hayes, 2013). The data for the three active conditions were collapsed (coded as 1) and compared to the control condition (coded as 0) to compute the indirect effect of condition (active vs. control) on change in perceptual bias through the proposed mediator (change in interpretation bias). Ten-thousand bootstrap samples were used, and statistical significance was determined by 95% bootstrap confidence intervals that did not overlap with zero. To calculate the magnitude of the indirect effect, a PM effect size was calculated, which corresponds to the ratio of the indirect effect to the total effect (Preacher & Kelley, 2011). Two participants did not complete the HIQ post-intervention; to account for these participants, pairwise deletion was used in the bivariate correlation analyses, and listwise deletion was used in the mediation analysis.
Results3
Bivariate Relations
To characterize the relations between pre- and post-intervention interpretation bias, height perception, and height fear, bivariate correlations were calculated (see Table 1). As expected, perceptual bias and interpretation bias were significantly correlated at both pre- and post-intervention assessments. Surprisingly, although height fear and perceptual bias were significantly correlated at the post-intervention assessment, they were not correlated at pre-intervention.
Table 1.
Bivariate Correlations for Pre- and Post-Intervention Interpretation Bias, Perceptual Bias, and Height Fear.
| 1. | 2. | 3. | 4. | 5. | 6. | |
|---|---|---|---|---|---|---|
| 1. Interpretation Bias Pre | - | |||||
| 2. Interpretation Bias Post | .51** | - | ||||
| 3. Height Perception Pre | .20* | 26** | - | |||
| 4. Height Perception Post | .09 | .22* | .63** | - | ||
| 5. Height Fear Pre | .37** | .24* | -.05 | .01 | - | |
| 6. Height Fear Post | .43** | .75** | .14 | .23* | .28** | - |
p<.05,
p<.01; Interpretation Bias was measured with the Heights Interpretation Questionnaire (HIQ; Steinman & Teachman, 2011); Height Perception was measured with a visual matching task (Clerkin et al., 2009; Teachman et al., 2008), and Height Fear was measured with the AQ-Anxiety (Cohen, 1977).
Differences in Perceptual Bias Across and within Conditions
Directionally consistent with hypotheses but not statistically significant at p<.05, results of the one-way ANOVA contrast showed a trend for participants in the active (vs. control) conditions to show greater reductions in perceptual bias, t(103)=1.82, p=.07, d=.36. Consistent with hypotheses, paired samples t-tests indicated that participants in the control condition did not experience significant decreases in perceptual bias (t(27)=1.36, p=.19, d=.21), while participants in the exposure condition showed statistically significant decreases in perceptual bias pre- to post-treatment (t(25)=2.87, p=.01, d=.51). Participants in the CBM- I (t(26)=2.02, p=.054, d=.39) and combined (t(25)=1.88, p =.07, d=.30) conditions showed reductions in perceptual bias at the level of a nonsignificant trend.
Change in Interpretation Bias as Mediator between Condition and Change in Perceptual Bias
As expected, there was a significant effect of condition (active vs. control) on the change in interpretation bias (b=−9.22, p<.0001; see Figure 1). However, contrary to expectations, change in interpretation bias was not associated with change in perceptual bias (b=.002, p=.62). Further, contrary to our hypotheses, the indirect effect of condition on change in perceptual bias was not statistically significant (indirect effect=−.01, SE=.03, 95% CI [−.08, .05], PM=.12). Similarly, when subscales of the HIQ were tested as mediators between condition and change in perceptual bias, no significant indirect effects emerged.
Figure 1.
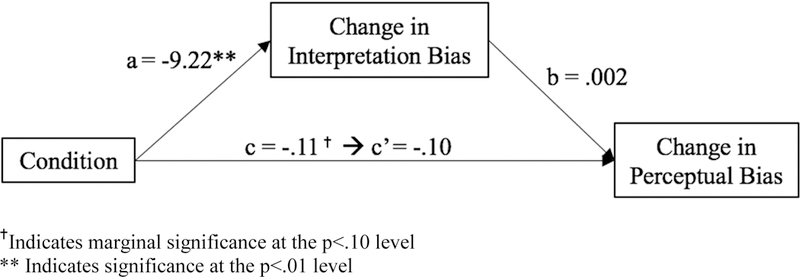
Indirect effect of condition (dummy coded) on perceptual bias.
Discussion
The present study provided evidence that treatments for height fear may sometimes alter perceptual bias of heights. Results showed preliminary support, at the level of a nonsignificant trend, that participants in the active (CBM-I, exposure, and combined) vs. control condition experienced greater reductions in perceptual bias. Further, in follow-up t-tests, participants in the exposure condition demonstrated a statistically significant decrease in perceptual bias, and participants in the other two active conditions demonstrated reductions in perceptual bias that approached statistical significance, with effect sizes ranging from small to moderate.
These findings extend initial correlational data (Teachman et al., 2008) and provide tentative support for theories of embodied perception (i.e., that evaluation of risk affects perception; see Proffitt, 2006). Specifically, our findings suggest perception of heights may be directly influenced by interventions that reduce evaluations of risk on heights. Notwithstanding, because the effect sizes were relatively small, and in some cases findings did not reach statistical significance, it will be important to replicate these results to determine their robustness. Further, determining how to strengthen the magnitude of the effects is needed. For example, additional intervention sessions may strengthen the interventions’ effects on perceptual bias. This seems especially likely given that individuals were still experiencing elevated levels of height fear at the post-intervention assessment, on average (see Steinman & Teachman, 2014).
Surprisingly, change in interpretation bias did not mediate the relation between condition and change in perceptual bias, despite evidence that change in interpretation bias mediated the relation between CBM and height fear in the parent study (Steinman & Teachman, 2014). Future studies could explore alternative mechanisms of perceptual bias reduction, such as changes in subjective distress level, attentional biases, or behavioural avoidance. Additionally, future research could explore ways to directly alter perceptual bias, to evaluate whether manipulation of perception affects fear of heights.
Although speculative, an alternative possible mechanism between acrophobia interventions and change in perceptual bias may be inhibitory learning. According to the inhibitory learning model of fear reduction (Craske et al., 2008; Craske, Treanor, Conway, Zbozinek, & Vervliet, 2014), exposure therapy acts in part by violating expectancies (e.g., bringing an acrophobic individual safely up a ladder and violating the expectancy that they will fall), which disrupts the connection between a conditioned, objectively-neutral stimulus (e.g., a ladder) and an unconditioned, adverse stimulus (e.g., a fall). Mechanisms similar to exposure-based inhibitory learning may be operating in CBM-I (e.g., training participants to inhibit associations of ambiguity and dangerous outcomes, and increase associations of ambiguity and safety; see Beadel, Mathews, & Teachman, 2016); Beadel, Smyth, & Teachman, 2014). There are limitations to consider in interpreting these results. First, the design did not test whether change in interpretation bias temporally preceded change in perceptual bias. Second, our hypothesis that all active conditions would equivalently reduce perceptual bias was largely informed by data from the parent study, and effects were small. Thus, replicating findings with an external data set will be critical. Related, it is interesting that participants in the exposure condition experienced the most reliable effect of treatment on perceptual bias. This finding should be explored in future research, with emphasis on determining the mechanisms driving change in perceptual bias. Finally, it was surprising that pre-intervention perceptual bias was not correlated with pre-intervention height fear (although these variables were correlated when measured post-intervention). This is not the first study conducted by our lab group that failed to find a connection between height fear and perception (e.g., Twedt, Steinman, Clerkin, Zadra, Proffitt, & Teachman, 2008), suggesting that this effect may only appear under specific conditions that are not yet fully understood. In sum, although open questions remain about the causal relationship between changes in perception and fear, our findings suggest tentative support for theories of embodied perception, and provide preliminary evidence that existing treatments, especially exposure therapy, act to reduce perceptual bias in acrophobia.
Highlights.
Tested effects of height fear treatments on changes in perceptual bias of heights.
Height-fearful participants who underwent exposure had reductions in perceptual bias.
Other active treatments showed marginally significant perceptual bias decreases.
Participants in the control condition had no significant changes in perceptual bias.
Acknowledgements
This work was supported in part by NIH grants RO1MH075781 and R01MH113752 to Bethany A. Teachman and an Association for Behavioral and Cognitive Therapies Dissertation Award to Shari A. Steinman. We thank Jessica Beadel, Joanna Chango, Meghan Cody, David Fask, Jennifer Green, Erin Miga, and Meg Reuland for their assistance as therapists in this study. We also thank Katherine Bian, Celia Cressy, Alexander Cutler, Lauren Faulkner, Victoria Gravett, Barrett Jacobson, Elizabeth Manzella, and Alexandra Werntz for their research assistance. Finally, thanks to members of the Teachman, Clerkin, and Steinman Labs for their helpful feedback and suggestions.
APPENDIX
CBM-I Only and Combined conditions: Scenario Training Examples
Scenario: You are standing on the edge of a balcony of a ten-story building. You realize the railings are shorter than they are on most balconies. The chances of you falling are mini_al.
Comprehension Question: Are you likely to fall off the balcony?
Scenario: You are on a flight to Chicago. Looking out of your window, you begin to feel slightly dizzy from looking at the land so far below. You know that having this sensation is nor_al.
Comprehension Question: Is your dizziness a sign of danger?
CBM-I Only and Combined conditions: Interpretation Modification Paradigm (IMP) Examples
Words that may be displayed: Alarming or Normal
Sentence: You feel short of breath as you are climbing up a fire escape to a 4th story landing.
Words that may be displayed: Alright or Threatening
Sentence: As you are cleaning leaves from your gutter, the ladder you are on makes a creaking sound.
Control Condition: Scenario Training Examples
Non-height-relevant:
Scenario: You go to the grocery store. While you are there, you buy eggs, bread, and juice. You forget to purchase m_lk.
Comprehension Question: Did you remember to buy milk?
Height-relevant:
Scenario: You are on a date. You are eating dinner at a restaurant on a rooftop terrace. You look at your date as the food is served and feel h_ngry.
Comprehension Question: Are you eating at a restaurant?
Control Condition: Interpretation Modification Paradigm (IMP) Examples
Non-height-relevant:
Words that may be displayed: Big or Small
Sentence: You watch a tiny ant crawl across the floor.
Height-relevant:
Words that may be displayed: Cold or Hot
Sentence: While on a balcony, you feel the warm sun on your face.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Only measures relevant to current hypotheses are included here. For a complete list of measures, please see Steinman and Teachman (2014).
There were occasional cases when a scheduling difficulty necessitated assignment to a given condition based on availability of a therapist or research assistant.
Although six out of seven experimenters in the present study rounded distance estimates to the nearest inch, one experimenter rounded estimates to the nearest six inches. Thus, analyses were run twice, once including and once excluding this experimenter. When analyses were run without the experimenter, the only meaningful difference was that change in perceptual bias for the Combined condition no longer trended toward significance (t(14) = .90, p =.38, d = .15).
The authors declare no conflict of interest.
References
- Antony MM, Craske MG, & Barlow DH (2006). Mastering your fears and phobias:Workbook (2nd ed.). Oxford: University Press. [Google Scholar]
- Baker A, Mystkowski J, Culver N, Yi R, Mortazavi A, & Craske MG (2010). Does habituation matter? Emotional processing theory and exposure therapy for acrophobia. Behaviour Research and Therapy, 48(11), 1139–1143. 10.1016/j.brat.2010.07.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beard C & Amir N (2008). A multi-session interpretation modification program: Changes in interpretation and social anxiety symptoms. Behaviour Research and Therapy 46, 1135–1141. 10.1016/j.brat.2008.05.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beadel JR, Mathews A, & Teachman BA (2016). Cognitive bias modification to enhance resilience to a panic challenge. Cognitive Therapy and Research, 40(6), 799–812. 10.1007/s10608-016-9791-z [Google Scholar]
- Beadel JR, Smyth FL, & Teachman BA (2014). Change processes during cognitive bias modification for obsessive compulsive beliefs. Cognitive Therapy and Research, 38(2), 103–119. 10.1007/s10608-013-9576-6 [Google Scholar]
- Clerkin EC, Cody MW, Steffanucci JK, Proffitt DR, & Teachman BA (2009). Imagery and fear influence height perception. Journal of Anxiety Disorders, 23, 381–386. 10.1016/j.janxdis.2008.12.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen DC (1972). Personality predictors and the outcome of varieties of desensitization Unpublished doctoral dissertation, Harvard University, Cambridge, MA. [Google Scholar]
- Cohen DC (1977). Comparison of self-report and behavioral procedures for assessing acrophobia. Behavior Therapy, 8, 17–23. 10.1016/S0005-7894(77)80116-0 [Google Scholar]
- Craske MG, Kircanski K, Zelikowsky M, Mystkowski J, Chowdhury N, & Baker A (2008). Optimizing inhibitory learning during exposure therapy. Behaviour Research and Therapy, 46(1), 5–27. 10.1016/j.brat.2007.10.003 [DOI] [PubMed] [Google Scholar]
- Craske MG, Treanor M, Conway CC, Zbozinek T, & Vervliet B (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23. 10.1016/j.brat.2014.04.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emmelkamp PM, & Felten M (1985). The process of exposure in vivo: Cognitive and physiological changes during treatment of acrophobia. Behaviour Research and Therapy, 23(2), 219–223. 10.1016/0005-7967(85)90034-8 [DOI] [PubMed] [Google Scholar]
- Foa EB, & Kozak MJ (1986). Emotional processing of fear: Exposure to corrective information. Psychological Bulletin, 99(1), 20–35. doi: 0.1037/0033-2909.99.1.20 [PubMed] [Google Scholar]
- Foa EB, Hembree EA, Cahill SP, Rauch SAM, Riggs DS,Feeny NC, & Yadin E (2005). Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: Outcome at academic and community clinics. Journal of Consulting and Clinical Psychology, 73, 953–964. 10.1037/0022-006X.73.5.953 [DOI] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, & Williams JBW (1994). Structured Clinical Interview for Axis I DSM-IV Disorders New York: Biometric Research Department, New York State Psychiatric Institute. [Google Scholar]
- Hallion LS, & Ruscio AM (2011). A meta-analysis of the effect of cognitive bias modification on anxiety and depression. Psychological Bulletin, 137(6), 940–958. 10.1037/a0024355 [DOI] [PubMed] [Google Scholar]
- Hayes AF (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach Guilford Press. [Google Scholar]
- Hummel-Rossi B, & Weinberg SL (1975). Practical guidelines in applying current theories to the measurement of change, Parts I and II Greenwich, CT: Johnson Associates. [Google Scholar]
- Jones EB, & Sharpe L (2017). Cognitive bias modification: A review of meta- analyses. Journal of affective disorders, 223, 175–183. 10.1016/j.jad.2017.07.034 [DOI] [PubMed] [Google Scholar]
- Mathews A, & Mackintosh B (2000). Induced emotional interpretation bias and anxiety. Journal of Abnormal Psychology, 109(4), 602–615. 10.1037/0021-843X.109.4.602 [PubMed] [Google Scholar]
- Preacher KJ, & Kelley K (2011). Effect size measures for mediation models: quantitative strategies for communicating indirect effects. Psychological methods, 16(2), 93–115. 10.1037/a0022658 [DOI] [PubMed] [Google Scholar]
- Proffitt DR (2006). Embodied perception and the economy of action. Perspectives on Psychological Science, 1(2), 110–122. 10.1111/j.1745-6916.2006.00008.x [DOI] [PubMed] [Google Scholar]
- Rachman S, & Cuk M (1992). Fearful distortions. Behaviour Research and Therapy, 30(6), 583–589. 10.1016/0005-7967(92)90003-Y [DOI] [PubMed] [Google Scholar]
- Stefanucci JK, & Proffitt DR (2009). The roles of altitude and fear in the perception of height. Journal of Experimental Psychology: Human Perception and Performance, 35(2), 424–438. 10.1037/a0013894 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stefanucci JK, Proffitt DR, Clore GL, & Parekh N (2008). Skating down a steeper slope: Fear influences the perception of geographical slant. Perception, 37(2), 321–323. 10.1068/p5796 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinman SA, & Teachman BA (2011). Cognitive processing and acrophobia: Validating the Heights Interpretation Questionnaire. Journal of Anxiety Disorders, 25, 896–902. 10.1016/j.janxdis.2011.05.001 Corrigendum published 2012, Journal of Anxiety Disorders, 26, 258–259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinman SA, & Teachman BA (2014). Reaching new heights: Comparing interpretation bias modification to exposure therapy for extreme height fear. Journal of Consulting and Clinical Psychology, 82(3), 404–417. 10.1037/a0036023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teachman BA, Stefanucci JK, Clerkin EM, Cody MW, & Proffitt DR (2008). A new mode of fear expression: Perceptual bias in height fear. Emotion, 8, 296–301. 10.1037/1528-3542.8.2.296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Twedt EL, Steinman SA, Clerkin EM, Zadra J, Proffitt DR, & Teachman BA (2008). Crossover effects: The relationship between fear and perception for individuals with height fear and spider fear Unpublished dataset. [Google Scholar]