

Abstract
Objective
While gender differences in hypertension and increased prevalence rates among women at midlife have been documented in multiple settings, the evidence on the Arab world has not been systematically examined. This review summarizes the evidence related to gender disparities in midlife hypertension in this region.
Methods
We searched MEDLINE and Social Sciences Citation Index (SSCI) databases for studies, published between January 2000 and August 2015, on hypertension in the 22 countries of the Arab region. We abstracted information on the prevalence of hypertension among women and men, in general populations during midlife.
Results
Nineteen studies provided data on the prevalence of hypertension by gender and age in the Arab world. Higher rates of hypertension were found among Arab women at midlife in most countries. In studies that included subjects younger than 35 years old, a decrease in sex ratios (M/F) at midlife was observed in all countries except Palestine. Higher female prevalence rates are observed in the 4th decade of life in most countries of the region, almost two decades earlier than in other parts of the world.
Conclusions
This review highlights the need for more systematic examinations of hypertension in the Arab region, its risk factors, and the reasons for the particular patterns of gender differences that are observed. Such research would have considerable implications for prevention, treatment, and improved well-being.
Keywords: Midlife, Women, Gender disparities, Sex ratio, Hypertension, High Blood Pressure, Arab World
Background
High blood pressure (HBP) is the leading risk factor for global disease burden, being responsible for almost 55% of cardiovascular deaths and 8.6% of disability-adjusted life years (DALYs) in 2015 [1–5]. Hypertension is often underestimated among women due to the common belief that cardiovascular disease is a “male” problem [6] — a misperception that still prevails, despite hypertension being the highest risk factor for global mortality among women, accounting for 20.4% of total deaths in 2015 [4]. Overall prevalence of hypertension is similar among women and men, but gender disparities in HBP have been shown to be age-dependent, with a remarkable increase at midlife in rates of hypertension among women as compared to men [7–11]. The National Health and Nutrition Examination Survey (NHANES) 2007–2012 showed that hypertension was higher among males until age 54, similar among males and females from 55 to 64 years of age, and higher among females from age 65 [12]. The mechanisms underlying these age-dependent disparities are not fully understood. Several factors have been invoked, including sex hormones, the renin–angiotensin system, oxidative stress, weight gain and sympathetic activation [6, 13, 14]. While the hormonal alterations observed in women during menopause have been the prevailing hypothesis, epidemiological studies have not been conclusive in this regard, with some studies suggesting that the rise in blood pressure after menopause is age-related, and others arguing that ovarian hormones contribute to an increased risk of hypertension, independently of age [9, 10, 15–18].
Hypertension is particularly high among adults in the Eastern Mediterranean region [1] and is the first risk factor for mortality and morbidity in the North Africa and Middle East region, accounting for 8% of DALYs in 2013, with a remarkable increase of 83% since 1990 [19]. The prevalence of hypertension among Arab middle-aged populations has not been analyzed by gender. This study aims at (1) summarizing available data on the prevalence of hypertension by gender and age, with special attention to the midlife in the Arab world; (2) examining gender disparities related to midlife hypertension in the Arab world; and (3) discussing key factors that could explain these gender disparities.
Methods
We searched MEDLINE and Social Sciences Citation Index (SSCI) databases for studies published between January 2000 and August 2015, on hypertension in countries of the Arab region. The selection of studies was done as a two-step process. First, studies were eligible for inclusion if they: (1) were conducted among residents of Arab countries (defined as the 22 countries of the Arab League); (2) reported on the prevalence of hypertension, and/or awareness, treatment or control of hypertension; (3) described the study design and methods; and (4) described how hypertension was assessed. Studies published in any language were included. Multi-country studies were included if they presented data on at least one Arab country. Studies conducted exclusively on clinical populations or on individuals suffering from particular diseases, and studies conducted on Arabs residing outside the Arab region were excluded. Additional quality considerations were taken into account: studies that did not report on sample size, age range of study population, methods to assess hypertension, cut-offs values, and studies that presented inconsistent numbers were excluded.
A further selection process was performed to retain only those studies reporting the prevalence of hypertension among general populations by gender during midlife. Midlife is typically defined starting at age 40 and extending to age 60, and studies differ as to how they define the exact beginning and end of midlife [20]. In this analysis, we used slightly wider cut-off points of 35 and 65, reflecting the age ranges of many of the surveys, in order to include the largest number of subjects in the analysis.
For each study, we calculated the sex ratios and present the significance of differences in the sex ratio; p-values are presented either as reported in the original publications, or as calculated based on chi-square tests. All statistical analyses were carried out using STATA version 13 (STATA Corporation, College Station, Texas, USA).
Results
Out of 251 articles, 19 fulfilled the eligibility criteria (Fig. 1). They covered 11 out of the 22 countries that are members of the Arab league: Algeria [21, 22], Egypt [23], Jordan[24, 25], Kingdom of Saudi Arabia (KSA) [26, 27], Kuwait [28], Lebanon [29, 30], Oman [31], Palestine [32], Syria [33], Tunisia [34–38], and UAE (United Arab Emirates) [39]. The 19 articles were based on surveys assessing the prevalence of chronic conditions, including HBP among general populations. Five of the studies were based on nationally representative samples; these were conducted in KSA [27], Lebanon [30], Oman [31], and Tunisia [34, 36]. Hypertension was assessed by actual blood pressure measurements in three studies [26, 27, 39]; by either blood pressure measurements or previous diagnosis as reported by respondents in 12 studies[21, 22, 24, 29, 31–38]; and by self-report of HBP in four studies [23, 25, 28, 30].
Fig. 1.
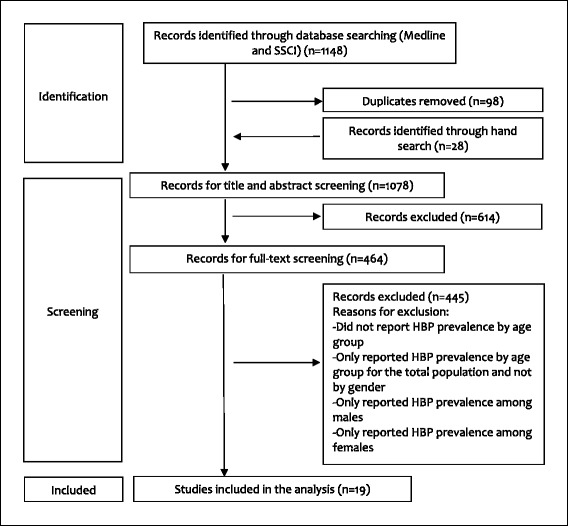
Study flow diagram
Table 1 shows the prevalence of hypertension in the Arab region by gender for 16 studies that provided the percent prevalence by gender and age. We present prevalence according to the specific age categories included in the studies, and prevalence during midlife (by selecting age groups from 35 to 65 years wherever possible); the total study sample size is also presented. For all but three studies that had missing data [25, 31, 35], the p-value for the gender difference in prevalence of hypertension is presented. The prevalence of hypertension during midlife could not be pooled across the different studies, due to the disparity in age group categorization and in ways of assessing hypertension.
Table 1.
Hypertension prevalence by gender and age group in the Arab World (> = 18 years), 2000-2015
| Country | First Author (Year of publication) |
Sample size a | Age group (years) b | Prevalence of Hypertension (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| By age group | Midlife c | Total sample | |||||||||||||
| Male | Female | Ratio M/F | 95% CI | Male | Female | Ratio M/F | 95% CI | Male | Female | Ratio M/F | 95% CI | ||||
| Self-reported hypertension | |||||||||||||||
| Egypt | Abolfotouh, M.A. (2008) [23] | 1800 | 18–24 | 0.7 | 2.1 | 0.33 | [0.04-2.59] | 16.6 | 31.6 | 0.53*** | [0.36-0.78] | 7.3 | 10.5 | 0.70 * | [0.51-0.94] |
| 25–44 | 4.2 | 7.6 | 0.55 * | [0.32-0.97] | |||||||||||
| 45–64 | 16.6 | 31.6 | 0.53*** | [0.36-0.78] | |||||||||||
| > = 65 | 20.0 | 43.8 | 0.46 | [0.19-1.09] | |||||||||||
| Jordan | Kulwicki, A. D. (2001) [25] | 209 | 17-34 | 2.3 | 1.6 | 1.44 e | e | 11.1 | 11.4 | 0.97 e | e | 7.1 | 9.6 | 0.74 | [0.29-1.91] |
| 35-54 | 11.1 | 11.4 | 0.97 e | ||||||||||||
| 55-93 | 14.3 | 35.3 | 0.41 e | ||||||||||||
| Kuwait | Shah, N.M. (2010) [28] | 2487 | 50-59 | 30.7 | 32.0 | 0.96 | [0.77-1.20] | 30.7 | 32.0 | 0.96 | [0.77-1.20] | 52.3 | 49.5 | 1.06 | [0.98-1.14] |
| 60-69 | 50.8 | 55.1 | 0.92 | [0.81-1.05] | |||||||||||
| > = 70 | 67.0 | 69.3 | 0.97 | [0.88-1.06] | |||||||||||
| Lebanon | Tohme, R. A. (2005) [30] | 2010a | 30-40 | 5.7 | 5.8 | 0.98 | [0.52-1.86] | 22.0 | 23.1 | 0.95 | [0.75-1.21] | 22.1 | 24.4 | 0.91 | [0.78-1.09] |
| 41-50 | 13.7 | 15.5 | 0.88 | [0.58-1.34] | |||||||||||
| 51-60 | 31.3 | 32.6 | 0.96 | [0.73-1.26] | |||||||||||
| 61-70 | 41.0 | 60.6 | 0.68 ** | [0.53-0.87] | |||||||||||
| >70 | 53.4 | 64.6 | 0.83 | [0.63-1.09] | |||||||||||
| Diagnosed hypertension based on BP measurements d | |||||||||||||||
| Algeria | Hamida, F. (2013) [21] | 722 | 40-49 | 21.1 | 20.6 | 1.02 | [0.59-1.77] | 29.2 | 33.3 | 0.88 | [0.63-1.21] | 51.3 | 49.7 | 1.03 | [0.90-1.21] |
| 50-59 | 40.8 | 48.1 | 0.85 | [0.58-1.24] | |||||||||||
| 60-69 | 71.4 | 67.6 | 1.06 | [0.85-1.32] | |||||||||||
| > = 70 | 75.7 | 80.6 | 0.94 | [0.80-1.11] | |||||||||||
| Jordan | Khader, Y. (2007) [24] | 1121 | 25-44 | 33.0 | 32.2 | 1.02 | [0.79-1.32] | g | 49.5 | 52.0 | 0.95 | [0.84-1.08] | |||
| 45-85 | 63.7 | 73.2 | 0.87 * | [0.77-0.98] | |||||||||||
| KSA | Al-Daghri, N.M. (2011) [26] | 9149 | 18 - 45 | 16.8 | 12.2 | 1.38 *** | [1.18-1.61] | 41.6 | 39.9 | 1.04 | [0.93-1.17] | 31.5 | 23.8 | 1.32 *** | [1.21-1.42] |
| 46 - 60 | 41.6 | 39.9 | 1.04 | [0.93-1.17] | |||||||||||
| 61 - 80 | 57.2 | 61.1 | 0.94 | [0.84-1.04] | |||||||||||
| Al-Nozha, M. M. (2007) [27] | 17230a | 30-39 | 14.1 | 10.4 | 1.36 *** | [1.18-1.57] | 28.6 | 29.6 | 0.97 | [0.90-1.03] | 28.6 | 23.9 | 1.20 *** | [ 1.14-1.26] | |
| 40-49 | 23.0 | 24.1 | 0.95 | [0.86-1.06] | |||||||||||
| 50-59 | 34.9 | 39.5 | 0.88 ** | [0.81-0.96] | |||||||||||
| 60-70 | 44.6 | 50.4 | 0.88 ** | [0.82-0.96] | |||||||||||
| Lebanon | Matar, D. (2015) [29] | 1697 | 21-34 | 20.0 | 9.0 | 2.22*** | [1.43-3.39] | 49.9 | 37.4 | 1.33 *** | [1.14-1.56] | 42.7 | 29.5 | 1.45**f | [1.28-1.68] |
| 35-49 | 42.0 | 24.0 | 1.75 *** | [1.33-2.28] | |||||||||||
| 50-64 | 60.0 | 54.0 | 1.11 | [0.94-1.32] | |||||||||||
| > = 65 | 76.0 | 68.0 | 1.12 | [0.92-1.37] | |||||||||||
| Oman | Al-Riyami A. (2002) [31] | 6414a | 20-39 | 23.9 | 16.8 | 1.42 e | e | 46.5 | 50.7 | 0.92 | e | 35.3 | 31.3 | 1.13***f | [1.06-1.22] |
| 40-59 | 46.5 | 50.7 | 0.92 e | ||||||||||||
| > = 60 | 60.9 | 68.1 | 0.89 e | ||||||||||||
| Palestine | Khdour, M. R. (2013) [32] | 2077 | 25-44 | 17.0 | 16.7 | 1.02 | [0.75-1.38] | 34.3 | 27.6 | 1.24 * | [1.03-1.51] | 29.2 | 26.4 | 1.11** | [0.96-1.27] |
| 45-64 | 34.3 | 27.6 | 1.24 * | [1.03-1.51] | |||||||||||
| > = 65 | 52.3 | 48.3 | 1.08 | [0.86-1.37] | |||||||||||
| Tunisia | Ben Romdhane, H. (2012) [34] | 8007a | 35-44 | 16.0 | 14.5 | 1.10 | [0.94-1.30] | 24.3 | 29.4 | 0.83*** | [0.76-0.89] | 27.3 | 33.1 | 0.82f | [0.77-0.88] |
| 45-54 | 26.3 | 33.6 | 0.78*** | [0.69-0.89] | |||||||||||
| 55-64 | 40.3 | 53.5 | 0.75*** | [0.67-0.85] | |||||||||||
| 65-74 | 51.1 | 66.0 | 0.77*** | [0.69-0.87] | |||||||||||
| Ben Romdhane, H. (2005) [35] | 1837 | 40-49 | 21.4 | 30.4 | 0.70 e | e | g | 38.7 | 48.2 | 0.80*** | [0.72-0.90] | ||||
| 50-59 | 40.5 | 54.4 | 0.74 e | ||||||||||||
| 60-69 | 56.0 | 73.0 | 0.77 e | ||||||||||||
| Bouguerra, R. (2006) [36] | 3857a | 20-29 | 31.3 | 22.2 | 1.41 ** | [1.10-1.82] | 41.3 | 52.6 | 0.79*** | [0.69-0.89] | 45.2 | 44.0 | 1.03 | [0.96-1.11] | |
| 30-39 | 28.9 | 29.5 | 0.98 | [0.78-1.22] | |||||||||||
| 40-49 | 34.4 | 45.5 | 0.76 ** | [0.62-0.91] | |||||||||||
| 50-59 | 52.4 | 63.1 | 0.83 * | [0.71-0.98] | |||||||||||
| 60-69 | 65.6 | 75.3 | 0.87 * | [0.78-0.97] | |||||||||||
| > = 70 | 76.1 | 82.5 | 0.92 | [0.82-1.03] | |||||||||||
| Elasmi, M. (2009) [37] | 2483 | 35-44 | 9.0 | 17.0 | 0.53*** | [0.39-0.75] | 22.9 | 33.0 | 0.69*** | [0.61-0.79] | 25.0 | 36.0 | 0.69*** | [0.62-0.78] | |
| 45-54 | 30.0 | 43.0 | 0.70*** | [0.59-0.84] | |||||||||||
| 55-64 | 37.0 | 63.0 | 0.59*** | [0.49-0.71] | |||||||||||
| 65-69 | 51.0 | 78.0 | 0.65*** | [0.51-0.81] | |||||||||||
| UAE | Baynouna, L. M. (2008) [39] | 817 | 20-29 | 5.1 | 1.7 | 3.00 | [0.32-28.01] | 26.2 | 29.4 | 0.89 | [0.65-1.22] | 21.8 | 19.8 | 1.10 | [0.84-1.44] |
| 30-39 | 11.1 | 7.0 | 1.59 | [0.65-4.00] | |||||||||||
| 40-49 | 17.0 | 23.0 | 0.74 | [0.42-1.30] | |||||||||||
| 50-59 | 33.6 | 38.8 | 0.87 | [0.59-1.26] | |||||||||||
| > = 60 | 36.8 | 36.7 | 1.00 | [0.57-1.76] | |||||||||||
BP blood pressure, CI Confidence interval, F Female, M Male, SBP systolic blood pressure, DBP diastolic blood pressure
*p <0.05 ** p ≤ 0.01; *** p ≤ 0.001: significant difference between genders. For the age groups and the midlife age categories, p-values were calculated based on chi-square tests assessing the significance of differences in sample proportion. For the total sample, p-values were presented either as reported in the original publications [21, 24, 26–32, 34–37], or calculated based on chi-square tests [23, 25, 39]
aNationally representative studies
bThe age groups that were selected for each study in order to generate midlife prevalence of hypertension are highlighted in bold.
cPrevalence of midlife hypertension by gender was compiled by selecting the age groups falling between 35 to 65 years in the original publications
dHypertension was assessed by actual BP measurements [26, 27, 39], or by either BP measurements or self-report of previous diagnosis [21, 24, 29, 31, 32, 34–37]. For BP measurements, hypertension was identified when SBP > =140 and/or DBP > =90 mmHg for all studies except for Khader et al., 2007 [24] and Bouguerra et al., 2006 [36], where the cut-offs used were SBP > =130 and/or DBP > =85 mmHg
eSignificance between genders and 95% confidence intervals could not be calculated due to insufficient data [25, 31, 35]
fThe significant difference between genders for the total sample, reported from the original publications, was adjusted in three studies [29, 31, 34]
gPrevalence of midlife hypertension could not be determined due to overlapping age ranges [24], or insufficient data to generate pooled prevalence [35]
Among middle-aged subjects (35–65 years old), sex ratios (M/F) for the prevalence of hypertension were generally lower than one (Table 1). However in three studies conducted in Lebanon [29], Palestine [32] and KSA [26], the reverse was true, with hypertension higher in males than females, and the difference statistically significant in the first two studies (p <0.001 and p = 0.027, respectively) [29, 32]. Patterns of age-gender disparities in hypertension varied across countries. In one group of studies (one conducted in Egypt, two in Jordan and three in Tunisia), hypertension was higher in females than males in the total sample size and at midlife [23–25, 34, 35, 37]. In other countries of the region (Algeria, KSA, Kuwait, Oman, and the UAE), overall prevalence rates of hypertension were higher among males, but prevalence was higher among women at midlife [21, 27, 28, 31, 39] with the three exceptions noted above [26, 29, 32].
Similar results were observed in three studies that provided only graphic representations of HBP prevalence among women and men: prevalence rates at midlife were higher among women than men in Algeria, Syria and Tunisia [22, 33, 38]. In Algeria, the sex ratio (M/F) was lower than one across all age categories including midlife [22]. In Syria [33], while M/F ratio was higher than one before midlife, the reverse was observed later on. In Tunisia, HBP was almost 1.5 times higher among females than males from 35 to 64 years of age [38].
Figure 2 provides a graphic illustration of gender disparities and shows M/F ratios for the prevalence of hypertension by age group. The dotted horizontal line corresponds to a M/F ratio of one; solid lines above represent higher prevalence among males and solid lines below represent higher prevalence among females. Most studies showed ratios <1 for years corresponding to midlife. In studies that included subjects younger than 35 years old [23–27, 29–32, 36, 39], M/F ratios decreased at midlife, except in Palestine [32], where the sex ratio increased during midlife, with a significant difference between genders (p = 0.027). In Jordan [24, 25], KSA [27], Oman [31], Tunisia [36] and the UAE [39], M/F ratios were initially higher than one at younger ages, but this pattern was reversed at midlife when M/F ratios decreased to less than one. On the other hand, in one study conducted in Lebanon [29], the M/F ratio decreased during midlife but remained >1; and in one study conducted in KSA [26], the sex ratio decreased, remaining >1 among middle-aged subjects, and decreasing to <1 among the elderly.
Fig. 2.
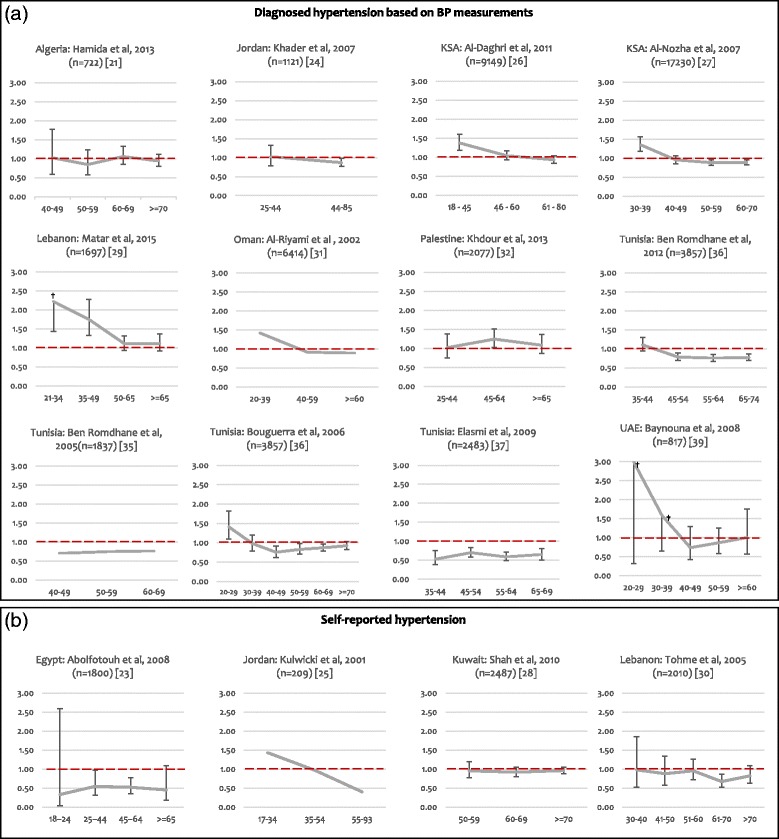
Sex Ratios (M/F) for the prevalence of hypertension by age category in the Arab world. Legend: BP: Blood pressure; F: Female; M: Male. a Hypertension was assessed by actual BP measurements [26, 27, 39], or by either BP measurements or self-report of previous diagnosis [21, 24, 29, 31, 32, 34–37]; b Hypertension was self-reported. The solid line corresponds to the M/F ratio by age group for each study. The dotted horizontal line corresponds to a M/F ratio of 1; solid lines above represent higher prevalence among males and solid lines below represent higher prevalence among females. The sample size for each study is shown in parenthesis. The error bars presented in the graphs correspond to the 95% CI of the sex ratios. The 95% CI in three studies [25], [31], and [35], could not be calculated due to insufficient data. † The upper limits of the 95% CI of the sex ratios were: 3.39 for the age group of 21–34 in Matar et al., 2015 [29], 28.01 and 4.00 for the age groups of 20–29 and 30–39, respectively, in Baynouna et al., 2008 [39].These values are not shown on the graphs, as we fixed the upper limit of the y-axis to 3, in order to keep the same scale for all graphs and allow comparisons
Discussion
This is the first review to analyze gender disparities in hypertension among middle-aged Arabs. We were able to retrieve 19 articles reporting on the prevalence of hypertension in the Arab region, by gender and age category, including the age range of 35 to 65 years. The paucity of research is remarkable, given that hypertension is the leading risk factor for morbidity and mortality in the region [3, 19].
A large body of evidence shows that gender disparities in HBP are age-dependent, with women witnessing a steeper increase in hypertension during midlife, as compared to men [7–11]. Cross-sectional studies such as the NHANES 2007–2012 [40, 41], the Community Hypertension Evaluation Clinic Program [42], and the Hypertension Detection and Follow-up Program Cooperative Group [43] indicate that blood pressure rises more steeply among middle-aged women than men, and that HBP rates in women surpass those of men around the fifth and sixth decades of life [15]. The Framingham Heart study also showed that blood pressure rates increased in middle-aged women, although they did not exceed those of men at any age between 30 and 60 years of age [44].
In this review, and consistent with the evidence in most settings, we found that sex ratios (M/F) in the prevalence of HBP decreased at midlife in most Arab countries, indicating that blood pressure increases at midlife among Arab women. We also found that the overall prevalence of hypertension was higher among middle-aged women as compared to men. Importantly, the prevalence of HBP among women surpassed that of men starting in the 4th decade of life, which is consistent with previous studies conducted in the Middle East [7], but different from studies conducted in the United States [12], Europe [45, 46], and China [47, 48], where rates of hypertension in women exceeded those of men only starting the 6th decade of life.
The only Arab population where the M/F ratio increases during midlife is in Palestine. This finding is puzzling, not only because it is an exception compared to the rest of the countries of the region, but also because other evidence indicates that overweight and obesity, which are associated with higher blood pressure, are higher among middle-aged Palestinian women than men [49]. One can conjecture that in the context of continuing political and military conflict, men may be more exposed to stress and economic hardship than women, and hence more vulnerable to blood pressure increases. This would be in line with literature showing that stress is associated with increased blood pressure, probably via mechanisms involving excessive sympathetic nervous system activation and transient endothelial dysfunction which can lead to vasoconstriction [50].
The higher prevalence of HBP among women has been attributed to a number of biological and environmental factors [26]. Estrogen has been shown to have vasodilation properties and progesterone to induce vascular relaxation through various mechanisms [51–56]. In line with this evidence, menopause is frequently pinpointed as a risk factor for HBP in midlife women, since the protective effects of ovarian hormones on blood pressure gradually disappear with the onset of menopause. Several cross-sectional studies have reported significantly higher blood pressure in postmenopausal than premenopausal women [57, 58]. Nevertheless, the association of menopause with HBP is complex due to confounding factors such as age and body weight [9, 10, 15–18]. Evidence from few prospective studies [59–61] suggests that menopause per se is not associated with increases in BP. In the Arab world, menopause was significantly and positively associated with HBP in several cross-sectionals studies conducted in Lebanon [62], Bahrain [63], and North African countries [64–66].
Obesity is a major cause of elevated blood pressure [6] and is remarkably higher among Arab women than men at midlife [49]. Obesity and overweight are associated with higher risk of hypertension and mortality among women than men of the same age [67]. The mechanism behind this association is still a matter of debate, and research has considered a variety of biological and hormonal factors [6, 68]. Lack of physical activity can also contribute to HBP, and global comparisons show that physical inactivity in the Arab world is particularly high [69, 70]. A closer examination of possible differences in environmental or behavioral factors among Arab middle-aged women and men, such as exposure to stress or salt consumption, could provide further insights into the reasons behind these gender differences.
The fact that the reversal in the sex ratios occurs earlier in the Arab world than elsewhere (the 4th, compared to the 6th decade of life) deserves further investigation. Some studies have documented that mean age at menopause is earlier in Arab countries than in countries of the North [71–73]. Earlier menopause may be a contributing factor, but is unlikely to fully account for this earlier onset of hypertension. In addition the prevalence rates of obesity, diabetes, and physical inactivity in women from the Middle East and North Africa (MENA) region are among the highest worldwide [49, 69, 74–76]. Other studies have shown that obesity prevalence rates are higher among women than men globally, and that the lowest M/F sex ratios are observed in the MENA region including at midlife [49, 77]. Clustering of elevated blood pressure, abdominal obesity, type 2 diabetes, and dyslipidemia has been well documented in the literature [78], and involves several complex mechanisms including insulin resistance, inflammation, oxidative stress, endothelial dysfunction, activation of the sympathetic nervous system and the renin-angiotensin-aldosterone system [79]. It may be that the higher rates of obesity, diabetes, and physical inactivity observed among Arab Women as compared to global figures, contribute to explaining the earlier onset of hypertension and reversal of sex ratios observed in the Arab region. Further investigations that consider hypertension, together with other genetic and social determinants would throw light on other possible reasons.
The findings of this review should be considered in light of the following limitations. First, the review is based on a relatively small number of studies, and although the results appear to be consistent across studies, they cannot be taken to be representative of the region. Secondly, the prevalence of hypertension was not available for the same age categories across all the studies, hence comparative statistics have to be taken with caution. Thirdly, the statistical significance of gender differences was calculated based on information provided in the articles and we did not have access to the data themselves. Fourthly, it is possible that in those four studies where hypertension was based on self-reports, the higher prevalence among women could be attributed to women’s tendency to self-report their medical conditions to a greater extent than men [8]; this would not, however, explain why the same gender differences are also found in studies that relied on measured hypertension. Fifth, studies that met the inclusion criteria were all cross-sectional, and thus comparing the prevalence of hypertension in men and women across the life span is likely to be confounded by the changes in representation of the surviving population. This highlights the need for longitudinal studies that would allow comparing the same study population over time [15].
Conclusions
This review has analyzed the available evidence on hypertension by gender during midlife, among Arab populations. The relatively small number of articles that met inclusion criteria highlights an important research gap, particularly in view of the risk factor that HBP represents in the Arab world. M/F ratios decrease at midlife in most Arab countries, and underscore the importance of refuting the misconception that hypertension is a “man’s disease.” The increase in prevalence of hypertension among women occurs earlier than in other regions; this pattern deserves further investigation. Studies that consider biological factors, behaviors, and the socio-cultural context of the Arab region are needed in order to understand the reasons behind such gender differences and identify those factors that could be modified in order to formulate programs designed to improve well-being among women and men.
Acknowledgements
We would like to thank Eman Sharara for helping with data extraction.
Funding
This work was funded in part by a grant (106981–001) from the International Development Research Centre (IDRC) in Canada. The funder had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Availability of data or materials
The datasets used and/or analysed during the current study are available from the corresponding author.
Authors’ contributions
CA (Akl) drafted the paper and conducted data screening, extraction, analysis and interpretation; CA (Akik) conducted the search; CA (Akik) and HG supervised the work and contributed to data analysis, interpretation and writing. CMO designed the analysis, supervised the work and critically reviewed the paper. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- DALYs
Disability-adjusted life years
- DBP
Diastolic blood pressure
- F
Female
- HBP
High blood pressure
- KSA
Kingdom of Saudi Arabia
- M
Male
- MENA
Middle East and North Africa
- NHANES
National Health and Nutrition Examination Survey
- SBP
Systolic blood pressure
- SSCI
Social Sciences Citation Index
- UAE
United Arab Emirates
Contributor Information
Christelle Akl, Email: cga17@aub.edu.lb.
Chaza Akik, Email: ca36@aub.edu.lb.
Hala Ghattas, Email: hg15@aub.edu.lb.
Carla Makhlouf Obermeyer, Phone: +961-1-350000, Email: cm39@aub.edu.lb.
References
- 1.WHO . A global brief on Hypertension. Switzerland: World Health Organization; 2013. Why hypertension is a major public health issue. [Google Scholar]
- 2.GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 2015. 2013;385(9963):117–71. [DOI] [PMC free article] [PubMed]
- 3.Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Amann M, Anderson HR, Andrews KG, Aryee M, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study. Lancet (London, England) 2012. 2010;380(9859):2224–2260. doi: 10.1016/S0140-6736(12)61766-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.IHME. GBD Compare Data Visualization. Seattle, WA: IHME, University of Washington: Institute for Health Metrics and Evaluation; 2016.[http://vizhub.healthdata.org/gbd-compare]; (Accessed on 11 Jan 2016).
- 5.Ezzati M, Riboli E. Behavioral and dietary risk factors for noncommunicable diseases. N Engl J Med. 2013;369(10):954–964. doi: 10.1056/NEJMra1203528. [DOI] [PubMed] [Google Scholar]
- 6.Gudmundsdottir H, Hoieggen A, Stenehjem A, Waldum B, Os I. Hypertension in women: latest findings and clinical implications. Therapeutic advances in chronic disease. 2012;3(3):137–146. doi: 10.1177/2040622312438935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. The Lancet. 2005;365(9455):217–223. doi: 10.1016/S0140-6736(05)70151-3. [DOI] [PubMed] [Google Scholar]
- 8.Doumas M, Papademetriou V, Faselis C, Kokkinos P. Gender differences in hypertension: myths and reality. Curr Hypertens Rep. 2013;15(4):321–330. doi: 10.1007/s11906-013-0359-y. [DOI] [PubMed] [Google Scholar]
- 9.Oparil S, Miller AP. Gender and blood pressure. J Clin Hypertens (Greenwich) 2005;7(5):300–309. doi: 10.1111/j.1524-6175.2005.04087.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Igho Pemu P, Ofili E. Hypertension in women: part I. J Clin Hypertens (Greenwich) 2008;10(5):406–410. doi: 10.1111/j.1751-7176.2008.06552.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pimenta E. Hypertension in women. Hypertension research : official journal of the Japanese Society of Hypertension. 2012;35(2):148–152. doi: 10.1038/hr.2011.190. [DOI] [PubMed] [Google Scholar]
- 12.Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, et al. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–e322. doi: 10.1161/CIR.0000000000000152. [DOI] [PubMed] [Google Scholar]
- 13.Reckelhoff JF. Gender differences in the regulation of blood pressure. Hypertension. 2001;37(5):1199–1208. doi: 10.1161/01.HYP.37.5.1199. [DOI] [PubMed] [Google Scholar]
- 14.Nuzzo A, Rossi R, Modena MG. Hypertension alone or related to the metabolic syndrome in postmenopausal women. Expert Rev Cardiovasc Ther. 2010;8(11):1541–1548. doi: 10.1586/erc.10.147. [DOI] [PubMed] [Google Scholar]
- 15.Sandberg K, Ji H. Sex differences in primary hypertension. Biology of sex differences. 2012;3(1):7. doi: 10.1186/2042-6410-3-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Coylewright M, Reckelhoff JF, Ouyang P. Menopause and hypertension: an age-old debate. Hypertension. 2008;51(4):952–959. doi: 10.1161/HYPERTENSIONAHA.107.105742. [DOI] [PubMed] [Google Scholar]
- 17.Casiglia E, Tikhonoff V, Caffi S, Bascelli A, Schiavon L, Guidotti F, Saugo M, Giacomazzo M, Martini B, Mazza A, et al. Menopause does not affect blood pressure and risk profile, and menopausal women do not become similar to men. J Hypertens. 2008;26(10):1983–1992. doi: 10.1097/HJH.0b013e32830bfdd9. [DOI] [PubMed] [Google Scholar]
- 18.Cifkova R, Pitha J, Lejskova M, Lanska V, Zecova S. Blood pressure around the menopause: a population study. J Hypertens. 2008;26(10):1976–1982. doi: 10.1097/HJH.0b013e32830b895c. [DOI] [PubMed] [Google Scholar]
- 19.Mokdad AH, Forouzanfar MH, Daoud F, El Bcheraoui C, Moradi-Lakeh M, Khalil I, Afshin A, Tuffaha M, Charara R, Barber RM, et al. Health in times of uncertainty in the eastern Mediterranean region, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet Global health. 2016;4(10):e704–713. [DOI] [PMC free article] [PubMed]
- 20.Lachman ME, Teshale S, Agrigoroaei S. Midlife as a pivotal period in the life course: balancing growth and decline at the crossroads of youth and Old Age. International journal of behavioral development. 2015;39(1):20–31. doi: 10.1177/0165025414533223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hamida F, Atif ML, Temmar M, Chibane A, Bezzaoucha A, Bouafia MT. [Prevalence of hypertension in El-Menia oasis, Algeria, and metabolic characteristics in population] Ann Cardiol Angeiol. 2013;62(3):172–178. doi: 10.1016/j.ancard.2013.04.008. [DOI] [PubMed] [Google Scholar]
- 22.Latifa BH, Kaouel M. [Cardiovascular risk factors in Tlemcen (Algeria)] Sante. 2007;17(3):153–158. doi: 10.1684/san.2007.0079. [DOI] [PubMed] [Google Scholar]
- 23.Abolfotouh MA, Soliman LA, Mansour E, Farghaly M, El-Dawaiaty AA. Central obesity among adults in Egypt: prevalence and associated morbidity. East Mediterr Health J. 2008;14(1):57–68. [PubMed] [Google Scholar]
- 24.Khader Y, Bateiha A, El-Khateeb M, Al-Shaikh A, Ajlouni K. High prevalence of the metabolic syndrome among Northern Jordanians. J Diabetes Complications. 2007;21(4):214–219. doi: 10.1016/j.jdiacomp.2005.11.003. [DOI] [PubMed] [Google Scholar]
- 25.Kulwicki AD, Kepler C. Assessment of cardiovascular risk factors among residents of a city in Jordan. J Cult Divers. 2001;8(2):34–40. [PubMed] [Google Scholar]
- 26.Al-Daghri NM, Al-Attas OS, Alokail MS, Alkharfy KM, Yousef M, Sabico SL, Chrousos GP. Diabetes mellitus type 2 and other chronic non-communicable diseases in the central region, Saudi Arabia (Riyadh cohort 2): a decade of an epidemic. BMC Med. 2011;9:76. doi: 10.1186/1741-7015-9-76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Al-Nozha MM, Abdullah M, Arafah MR, Khalil MZ, Khan NB, Al-Mazrou YY, Al-Maatouq MA, Al-Marzouki K, Al-Khadra A, Nouh MS, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28(1):77–84. [PubMed] [Google Scholar]
- 28.Shah NM, Behbehani J, Shah MA. Prevalence and correlates of major chronic illnesses among older Kuwaiti nationals in two governorates. Medical principles and practice : international journal of the Kuwait University, Health Science Centre. 2010;19(2):105–112. doi: 10.1159/000273069. [DOI] [PubMed] [Google Scholar]
- 29.Matar D, Frangieh AH, Abouassi S, Bteich F, Saleh A, Salame E, Kassab R, Azar RR. Prevalence, awareness, treatment, and control of hypertension in Lebanon. J Clin Hypertens (Greenwich) 2015;17(5):381–388. doi: 10.1111/jch.12485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Tohme RA, Jurjus AR, Estephan A. The prevalence of hypertension and its association with other cardiovascular disease risk factors in a representative sample of the Lebanese population. J Hum Hypertens. 2005;19(11):861–868. doi: 10.1038/sj.jhh.1001909. [DOI] [PubMed] [Google Scholar]
- 31.Al-Riyami AA, Afifi MM. Hypertension in Oman: distribution and correlates. Journal of the Egyptian Public Health Association. 2002;77(3–4):383–407. [PubMed] [Google Scholar]
- 32.Khdour MR, Hallak HO, Shaeen M, Jarab AS, Al-Shahed QN. Prevalence, awareness, treatment and control of hypertension in the Palestinian population. J Hum Hypertens. 2013;27(10):623–628. doi: 10.1038/jhh.2013.26. [DOI] [PubMed] [Google Scholar]
- 33.Al Ali R, Rastam S, Fouad FM, Mzayek F, Maziak W. Modifiable cardiovascular risk factors among adults in Aleppo. Syria Int J Public Health. 2011;56(6):653–662. doi: 10.1007/s00038-011-0278-0. [DOI] [PubMed] [Google Scholar]
- 34.Ben Romdhane H, Ben Ali S, Skhiri H, Traissac P, Bougatef S, Maire B, Delpeuch F, Achour N. Hypertension among Tunisian adults: results of the TAHINA project. Hypertension research : official journal of the Japanese Society of Hypertension. 2012;35(3):341–347. doi: 10.1038/hr.2011.198. [DOI] [PubMed] [Google Scholar]
- 35.Ben Romdhane H, Skhiri H, Bougatef S, Ennigrou S, Gharbi D, Chahed MK, Achour N. [Hypertension prevalence, awareness, treatment and control: results from a community based survey] Tunisie Medicale. 2005;83(Suppl 5):41–46. [PubMed] [Google Scholar]
- 36.Bouguerra R, Ben Salem L, Alberti H, Ben Rayana C, El Atti J, Blouza S, Gaigi S, Achour A, Ben Slama C, Zouari B. Prevalence of metabolic abnormalities in the Tunisian adults: a population based study. Diabetes Metab. 2006;32(3):215–221. doi: 10.1016/S1262-3636(07)70271-9. [DOI] [PubMed] [Google Scholar]
- 37.Elasmi M, Feki M, Sanhaji H, Jemaa R, Haj Taeib S, Omar S, Mebazaa A, El Ati J, Hsairi M, Kaabachi N. [Prevalence of conventional cardiovascular risk factors in the Great Tunis population] Rev Epidemiol Sante Publique. 2009;57(2):87–92. doi: 10.1016/j.respe.2008.12.010. [DOI] [PubMed] [Google Scholar]
- 38.Allal-Elasmi M, Feki M, Zayani Y, Hsairi M, Haj Taieb S, Jemaa R, Sanhaji H, Omar S, Mebazaa A, Kaabachi N. Prehypertension among adults in Great Tunis region (Tunisia): A population-based study. Pathol Biol (Paris) 2012;60(3):174–179. doi: 10.1016/j.patbio.2011.03.007. [DOI] [PubMed] [Google Scholar]
- 39.Baynouna LM, Revel AD, Nagelkerke NJ, Jaber TM, Omar AO, Ahmed NM, Naziruldeen MK, Al-Sayed MF, Nour FA. High prevalence of the cardiovascular risk factors in Al-Ain, United Arab Emirates. An emerging health care priority. Saudi Med J. 2008;29(8):1173–1178. [PubMed] [Google Scholar]
- 40.Burt VL, Whelton P, Roccella EJ, Brown C, Cutler JA, Higgins M, Horan MJ, Labarthe D. Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988–1991. Hypertension 1995. 1995;25(3):305–313. doi: 10.1161/01.hyp.25.3.305. [DOI] [PubMed] [Google Scholar]
- 41.Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, et al. Heart disease and stroke statistics--2011 update: a report from the American Heart Association. Circulation. 2011;123(4):e18–e209. doi: 10.1161/CIR.0b013e3182009701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Stamler J, Stamler R, Riedlinger WF, Algera G, Roberts RH. Hypertension screening of 1 million Americans. Community Hypertension Evaluation Clinic (CHEC) program, 1973 through. Jama 1976. 1975;235(21):2299–2306. doi: 10.1001/jama.235.21.2299. [DOI] [PubMed] [Google Scholar]
- 43.Cornoni-Huntley J, LaCroix AZ, Havlik RJ. Race and sex differentials in the impact of hypertension in the United States. The National Health and Nutrition Examination Survey I Epidemiologic Follow-up Study. Arch Intern Med. 1989;149(4):780–788. doi: 10.1001/archinte.1989.00390040022005. [DOI] [PubMed] [Google Scholar]
- 44.Vokonas PS, Kannel WB, Cupples LA. Epidemiology and risk of hypertension in the elderly: the Framingham Study. J Hypertens Suppl. 1988;6(1):S3–S9. [PubMed] [Google Scholar]
- 45.Falaschetti E, Mindell J, Knott C, Poulter N. Hypertension management in England: a serial cross-sectional study from 1994 to 2011. The Lancet. 2014;383(9932):1912–1919. doi: 10.1016/S0140-6736(14)60688-7. [DOI] [PubMed] [Google Scholar]
- 46.Lacruz ME, Kluttig A, Hartwig S, Loer M, Tiller D, Greiser KH, Werdan K, Haerting J. Prevalence and Incidence of Hypertension in the General Adult Population: Results of the CARLA-Cohort Study. Medicine. 2015;94(22):e952. doi: 10.1097/MD.0000000000000952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wang Y, Peng X, Nie X, Chen L, Weldon R, Zhang W, Xiao D, Cai J. Burden of hypertension in China over the past decades: systematic analysis of prevalence, treatment and control of hypertension. Eur J Prev Cardiol. 2016;23(8):792–800. doi: 10.1177/2047487315617105. [DOI] [PubMed] [Google Scholar]
- 48.Gao Y, Chen G, Tian H, Lin L, Lu J, Weng J, Jia W, Ji L, Xiao J, Zhou Z, et al. Prevalence of hypertension in china: a cross-sectional study. PLoS One. 2013;8(6):e65938. doi: 10.1371/journal.pone.0065938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.IHME. Overweight and Obesity Viz. Seattle, WA: IHME, University of Washington: Institute for Health Metrics and Evaluation; 2014. [Available from http://vizhub.healthdata.org/obesity]; (Accessed on 11 Jan 2016).
- 50.Rozanski A, Blumenthal JA, Kaplan J. Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy. Circulation. 1999;99(16):2192–2217. doi: 10.1161/01.CIR.99.16.2192. [DOI] [PubMed] [Google Scholar]
- 51.Dubey RK, Oparil S, Imthurn B, Jackson EK. Sex hormones and hypertension. Cardiovasc Res. 2002;53(3):688–708. doi: 10.1016/S0008-6363(01)00527-2. [DOI] [PubMed] [Google Scholar]
- 52.Duerrschmidt N, Wippich N, Goettsch W, Broemme HJ, Morawietz H. Endothelin-1 induces NAD(P)H oxidase in human endothelial cells. Biochem Biophys Res Commun. 2000;269(3):713–717. doi: 10.1006/bbrc.2000.2354. [DOI] [PubMed] [Google Scholar]
- 53.Fischer M, Baessler A, Schunkert H. Renin angiotensin system and gender differences in the cardiovascular system. Cardiovasc Res. 2002;53(3):672–677. doi: 10.1016/S0008-6363(01)00479-5. [DOI] [PubMed] [Google Scholar]
- 54.Fortepiani LA, Zhang H, Racusen L, Roberts LJ, 2nd, Reckelhoff JF. Characterization of an animal model of postmenopausal hypertension in spontaneously hypertensive rats. Hypertension. 2003;41(3 Pt 2):640–645. doi: 10.1161/01.HYP.0000046924.94886.EF. [DOI] [PubMed] [Google Scholar]
- 55.Mortensen LH, Pawloski CM, Kanagy NL, Fink GD. Chronic hypertension produced by infusion of endothelin in rats. Hypertension. 1990;15(6 Pt 2):729–733. doi: 10.1161/01.HYP.15.6.729. [DOI] [PubMed] [Google Scholar]
- 56.Yang XP, Reckelhoff JF. Estrogen, hormonal replacement therapy and cardiovascular disease. Curr Opin Nephrol Hypertens. 2011;20(2):133–138. doi: 10.1097/MNH.0b013e3283431921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Staessen J, Bulpitt CJ, Fagard R, Lijnen P, Amery A. The influence of menopause on blood pressure. J Hum Hypertens. 1989;3(6):427–433. [PubMed] [Google Scholar]
- 58.Staessen JA, Ginocchio G, Thijs L, Fagard R. Conventional and ambulatory blood pressure and menopause in a prospective population study. J Hum Hypertens. 1997;11(8):507–514. doi: 10.1038/sj.jhh.1000476. [DOI] [PubMed] [Google Scholar]
- 59.Do KA, Green A, Guthrie JR, Dudley EC, Burger HG, Dennerstein L. Longitudinal study of risk factors for coronary heart disease across the menopausal transition. Am J Epidemiol. 2000;151(6):584–593. doi: 10.1093/oxfordjournals.aje.a010246. [DOI] [PubMed] [Google Scholar]
- 60.Matthews KA, Crawford SL, Chae CU, Everson-Rose SA, Sowers MF, Sternfeld B, Sutton-Tyrrell K. Are changes in cardiovascular disease risk factors in midlife women due to chronological aging or to the menopausal transition? J Am Coll Cardiol. 2009;54(25):2366–2373. doi: 10.1016/j.jacc.2009.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Torng PL, Su TC, Sung FC, Chien KL, Huang SC, Chow SN, Lee YT. Effects of menopause on intraindividual changes in serum lipids, blood pressure, and body weight--the Chin-Shan Community Cardiovascular Cohort study. Atherosclerosis. 2002;161(2):409–415. doi: 10.1016/S0021-9150(01)00644-X. [DOI] [PubMed] [Google Scholar]
- 62.Arevian M, Adra M, Kubeissi L. Risk factors for coronary artery disease (CAD) in Lebanese-Armenian women. Health Care Women Int. 2004;25(10):933–949. doi: 10.1080/07399330490508631. [DOI] [PubMed] [Google Scholar]
- 63.Al-Mahroos F, Al-Roomi K, McKeigue PM. Relation of high blood pressure to glucose intolerance, plasma lipids and educational status in an Arabian Gulf population. Int J Epidemiol. 2000;29(1):71–76. doi: 10.1093/ije/29.1.71. [DOI] [PubMed] [Google Scholar]
- 64.Nejjari C, Arharbi M, Chentir MT, Boujnah R, Kemmou O, Megdiche H, Boulahrouf F, Messoussi K, Nazek L, Bulatov V. Epidemiological Trial of Hypertension in North Africa (ETHNA): an international multicentre study in Algeria, Morocco and Tunisia. J Hypertens. 2013;31(1):49–62. doi: 10.1097/HJH.0b013e32835a6611. [DOI] [PubMed] [Google Scholar]
- 65.Belfki H, Ben Ali S, Aounallah-Skhiri H, Traissac P, Bougatef S, Maire B, Delpeuch F, Achour N, Ben Romdhane H. Prevalence and determinants of the metabolic syndrome among Tunisian adults: results of the Transition and Health Impact in North Africa (TAHINA) project. Public Health Nutr. 2013;16(4):582–590. doi: 10.1017/S1368980012003291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Ben Ali S, Belfki-Benali H, Aounallah-Skhiri H, Traissac P, Maire B, Delpeuch F, Achour N, Ben Romdhane H. Menopause and metabolic syndrome in tunisian women. Biomed Res Int. 2014;2014:457131. doi: 10.1155/2014/457131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Wilson PW, D’Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med. 2002;162(16):1867–1872. doi: 10.1001/archinte.162.16.1867. [DOI] [PubMed] [Google Scholar]
- 68.Jarvie JL, Foody JM. Recognizing and improving health care disparities in the prevention of cardiovascular disease in women. Curr Cardiol Rep. 2010;12(6):488–496. doi: 10.1007/s11886-010-0135-4. [DOI] [PubMed] [Google Scholar]
- 69.Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. The Lancet. 2012;380(9838):247–257. doi: 10.1016/S0140-6736(12)60646-1. [DOI] [PubMed] [Google Scholar]
- 70.Sallis JF, Bull F, Guthold R, Heath GW, Inoue S, Kelly P, Oyeyemi AL, Perez LG, Richards J, Hallal PC. Progress in physical activity over the Olympic quadrennium. The Lancet. 2016;388(10051):1325–1336. doi: 10.1016/S0140-6736(16)30581-5. [DOI] [PubMed] [Google Scholar]
- 71.Reynolds RF, Obermeyer CM. Age at natural menopause in Beirut, Lebanon: the role of reproductive and lifestyle factors. Ann Hum Biol. 2001;28(1):21–29. doi: 10.1080/03014460150201850. [DOI] [PubMed] [Google Scholar]
- 72.Reynolds RF, Obermeyer CM. Age at natural menopause in Spain and the United States: results from the DAMES project. Am J Hum Biol. 2005;17(3):331–340. doi: 10.1002/ajhb.20121. [DOI] [PubMed] [Google Scholar]
- 73.Reynolds RF, Obermeyer CM. Correlates of the age at natural menopause in Morocco. Ann Hum Biol. 2009;30(1):97–108. doi: 10.1080/03014460210165908. [DOI] [PubMed] [Google Scholar]
- 74.NCD Risk Factor Collaboration. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet (London, England). 2016;387(10027):1513–30. [DOI] [PMC free article] [PubMed]
- 75.Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet. 2014;384(9945):766–781. doi: 10.1016/S0140-6736(14)60460-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Dumith SC, Hallal PC, Reis RS, Kohl HW., 3rd Worldwide prevalence of physical inactivity and its association with human development index in 76 countries. Prev Med. 2011;53(1–2):24–28. doi: 10.1016/j.ypmed.2011.02.017. [DOI] [PubMed] [Google Scholar]
- 77.Kanter R, Caballero B. Global gender disparities in obesity: a review. Advances in nutrition. 2012;3(4):491–498. doi: 10.3945/an.112.002063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Grundy SM. Diagnosis and management of the metabolic syndrome: an American heart association/national heart, lung, and blood institute scientific statement. Circulation. 2005;112(17):2735–2752. doi: 10.1161/CIRCULATIONAHA.105.169404. [DOI] [PubMed] [Google Scholar]
- 79.Cheung BM, Li C. Diabetes and hypertension: is there a common metabolic pathway? Curr Atheroscler Rep. 2012;14(2):160–166. doi: 10.1007/s11883-012-0227-2. [DOI] [PMC free article] [PubMed] [Google Scholar]