

Abstract
Background
Cancer is highly prevalent worldwide and can cause high levels of distress in patients, which is often neglected in medical care. Smartphone apps are readily available and therefore seem promising to deliver distress-reducing interventions such as mindfulness and relaxation programs.
Objective
This study aimed to evaluate the feasibility of a mindfulness and relaxation app for cancer patients. We looked at characteristics of participating patients in a mobile health (mHealth) study, including adherence to the app intervention, predictors for adherence, and patients’ feedback regarding the app.
Methods
In this prospective observational study with a mixed-methods approach, cancer patients received a mindfulness and relaxation self-care app. Cancer patients were recruited online and through hospitals in Switzerland. We assessed self-reported measures (eg, quality of life, anxiety, depressive symptoms, openness to experience, resistance to change) at baseline, and the app gathered data on patients’ practicing time. With 8 semistructured interviews, we obtained patients’ feedback about the app and recommendations for improvements. We looked at 3 dimensions of the Reach, Effectiveness, Adoption, Implementation, and Maintenance framework (reach, adoption, and maintenance) and analyzed data for adherence for the first 10 weeks of the app intervention. We report descriptive statistics for patient characteristics and app use. For the prediction of adherence, we used Kaplan-Meier analyses with log-rank tests and a Cox proportional hazards regression.
Results
Data from 100 cancer patients (74 female) showed that 54 patients were using the app exercises continuously until week 10. In continuous app users, the median number of exercises per week dropped from 4 (interquartile range, IQR 1-7) at week 1 to a median of 2 (IQR 1-4) at week 10. Our analyses revealed 4 significant predictors for better adherence: female gender, higher openness to experience, higher resistance to change, and more depressive symptoms. Interviews revealed that the patients generally were satisfied with the app but also made suggestions on how to improve it.
Conclusions
Our study indicates that a mindfulness and relaxation mHealth intervention for cancer patients is feasible with acceptable adherence and largely positive feedback from patients.
Trial Registration
German Clinical Trials Register DRKS00010481; https://www.drks.de/drks_web/navigate.do?navigation Id=trial.HTML&TRIAL_ID=DRKS00010481 (Archived by WebCite at http://www.webcitation.org/73xGE1B0P)
Keywords: mobile app, mindfulness, relaxation, cancer, patient compliance
Introduction
Background
Cancer is highly prevalent worldwide, with an estimated 14 million newly diagnosed patients per year [1]. According to the World Health Organization, cancer is the second leading cause of death, with an increasing economic impact over recent years [2]. For patients, the diagnosis of cancer and subsequent treatment (eg, radiation or chemotherapy) can cause high levels of distress [3,4]. About every second cancer patient has clinically relevant distress, with elevated levels of depression or anxiety [5]. However, psychological support of patients is often not implemented in standard medical care [6-8]. In addition, many patients neglect their distress and do not seek psychosocial support [9]. However, untreated distress can reduce quality of life as well as lower adherence with recommended medical care and, therefore, negatively affect patients’ recovery [8,10]. Thus, a variety of treatments such as counseling and Mind Body Medicine (MBM) interventions have been suggested to reduce cancer patients’ distress during initial care and rehabilitation [11-13].
MBM focuses on the interactions between psychological and biological processes and their impact on health [14,15] and has shown beneficial effects in reducing cancer patients’ distress [13,16]. MBM usually combines a variety of interventions, such as exercise, Qigong, relaxation, and mindfulness meditation [14]. Some of these interventions, for example, mindfulness and relaxation, are also commonly used on their own and have been studied extensively with promising effects in both healthy and patient populations [15,17-20]. In addition, an increasing number of cancer patients are interested in or use mindfulness or relaxation interventions [21].
Regular practice is crucial for the effect of mindfulness and relaxation-based interventions, which can be difficult to achieve due to lack of motivation, time constraints, as well as limited access to interventions [22]. Further restrictions for regular practice and access-limiting factors include geographical distance, financial constraints, lack of treatment providers or lack of knowledge thereof [8,9,23]. For cancer patients, regular practice might additionally be hindered due to restrictions caused by cancer (eg, fatigue and nausea) and its comprehensive treatments.
Mobile health (mHealth) interventions might overcome some of the restrictions of face-to-face interventions. The access to interventions can be easier due to a large and increasing number of smartphone owners [24]. In 2017, more than 32% of the world population and more than 60% of the population in Western Europe and North America owned a smartphone [25]. In addition, mHealth interventions have some specific advantages compared with face-to-face interventions. These advantages include easy and pervasive access to information (ie, psychoeducation), engaging audio and/or visual material, potential customization of the app according to client’s preferences and needs, provision of regular feedback, reminders, and reduced perceived stigmatization due to potentially less therapist contact [24,26]. mHealth interventions can also be a good support for patients’ self-care [26]. Such self-care interventions can have beneficial effects on cancer patients’ distress and quality of life [27] and can be implemented via an app using audio instructions.
To date, mHealth interventions using a mindfulness or relaxation intervention strategy have been under-researched, with the focus of studies primarily on Web-based electronic Health (eHealth) interventions [28]. For eHealth interventions, studies indicate that mindfulness- and relaxation-based interventions can have beneficial effects on health outcomes in various populations, including cancer patients [28-30]. Beneficial effects of eHealth were reported for stress, well-being, anxiety, depression, and mindfulness. The majority of available primary studies in these reviews focused on eHealth interventions, with a partial emphasis on Web-based patient-therapist interactions. However, less is known about the feasibility and effectiveness of mHealth interventions, and certain disadvantages (eg, technical problems, concerns about data security) are well known [26]. Eysenbach [31] coined the term “law of attrition,” which emphasizes that early and rapid attrition rates are an inherent problem in technology-delivered interventions. Especially in self-care interventions with regular exercises, good adherence itself often becomes an intervention goal. Although recent eHealth studies report acceptable rates of adherence (eg, 60% completed 4 or more out of 6 modules [32] and 71% practiced more than 50% of the days during 8 weeks [33]), little is known about the adherence to mindfulness and relaxation mHealth programs for cancer patients. Therefore, when setting up a self-care mHealth intervention, it is important to know which factors might influence the patient adherence.
Objective
The aim of this mHealth study, then, was to evaluate the feasibility of a mindfulness and relaxation app for cancer patients and its impact on health outcomes according to the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework [34]. In this analysis, we looked at the characteristics of patients who participated in this mHealth study, adherence and predictors for adherence, as well as patients’ feedback regarding the mHealth intervention from interviews.
Methods
Study Design
We performed a prospective observational study using a mixed-methods approach. Quantitative data consisted of 4 paper-and-pencil questionnaires sent to cancer patients at baseline, weeks 4, 10, and 20. Qualitative data consisted of semistructured interviews with 8 cancer patients. Corresponding to the principles of theoretical sampling [35], we recruited the interviewees based on the sample distributions of gender and intervention dropouts versus continuous app users. We conducted individual qualitative interviews over the telephone with these patients; selecting 4 of them who used the app on a regular basis and 4 who did not use the app regularly. We conducted qualitative interviews with these patients; 4 of them used the app on a regular basis and 4 did not use the app regularly. This study was guided by the RE-AIM evaluation framework [34], which consists of the following 5 dimensions: reach, effectiveness, adoption, implementation, and maintenance. For this analysis, we focused on 3 dimensions, namely reach, adoption, and maintenance during the first 10 weeks of the intervention. The dimensions effectiveness and implementation as well as results about the entire 20 weeks will be reported in an upcoming paper. The cantonal ethics committee granted ethical approval for the study (BASEC-Nr. 2016-00258) in April 2016, and the study was positively audited within the regular ICH-GCP audit of the University Hospital Zurich in August 2016. We registered the study in the German Clinical Trials Register (DRKS00010481).
Eligibility Criteria
We included female and male cancer patients (18 years or older) with any cancer diagnosis at any stage of cancer, who owned either an iOS- or Android-based smartphone with at least a weekly connection to the internet. We excluded patients if they had suicidal ideation or insufficient German language skills. Furthermore, patients who intended to move to another country and patients with insufficient knowledge on how to use a smartphone were excluded.
Recruitment
We recruited cancer patients in 2 different settings: (1) cancer patients who participated in a supportive MBM treatment (either as individual session or as a 10-week group treatment) or (2) cancer patients without an MBM treatment.
For setting 1, cancer patients were recruited at the Institute for Complementary and Integrative Medicine, University Hospital Zurich (ICI). All available cancer patients in an MBM group treatment (between June 2016 and December 2017; 12 groups with a total of 81 patients) were invited at the third session of the course to participate in the study. Therefore, enrolled patients from setting 1 were using the app partially in parallel to the MBM group treatment. In addition, we asked the health professionals of the ICI to distribute leaflets during individual MBM consultations with cancer patients.
For setting 2, patients were recruited through the University Hospital Zurich (ICI, cancer center, Department of Radiotherapy, and University Hospital Facebook page), University Hospital Basel, and the Cantonal Hospital Aarau. Cancer patients were informed of the study using leaflets in the waiting areas or during consultations. In addition, we informed cancer patients through the Swiss Cancer League via leaflets and their Facebook page, as well as through the Cancer League of Zurich.
Interested patients initially contacted a researcher at the ICI by phone or email and made an appointment for a 10-min telephone screening interview. During the screening interview, the researcher explained the study and assessed the eligibility of the patient. In addition, the researcher recommended that the patient carry out 1 of the 3 exercises of the app at least once a day on 5 different days per week during the 20-week intervention. However, the researcher also stated that patients were free to choose when, where, and how often they practiced. After the researcher provided all information and if the patient met the eligibility criteria, the researcher asked for contact details of the patient. Subsequently, the patient received the written study information with the informed consent form, as well as the first questionnaire by mail. We sent an email to every included patient with a code to activate the app. Thereafter, patients were able to use the app free of charge. The date of the code distribution was considered as the start of the intervention for each patient. No other verbal contact between the researcher and the patients took place after inclusion of patients.
Intervention
The mindfulness and relaxation app comprised 2 main features: (1) mindfulness and relaxation exercises guided by audio instructions and (2) a notification feature. The first feature of the app contained 3 exercises and was the main component of the app. The exercises were mindfulness meditation, guided imagery, and progressive muscle relaxation audio files with a duration of about 15 min each. Every exercise was guided by a narrator with either a male or female voice.
The second feature of the app was a notification feature, which reminded the patient to practice daily. The patient could set the time of notification according to individual preferences. The reminder to practice popped up as a push notification on the mobile device every day at the time set by the patient. The concept of the app built on previously developed relaxation study apps of an affiliated group [36], which were designed for patients with chronic low back pain (Relaxback) and chronic neck pain (Relaxneck).The app was developed by the software company Smart Mobile Factory GmbH (Berlin, Germany). After thorough testing, the app was released in June 2016 on the Apple iTunes Store and on the Google Play Store for Android devices. After the release, the content of the app was not changed. Screenshots of the app are available in Multimedia Appendices 1 and 2.
Outcomes
Reach
For the dimension reach, we looked into which and how many cancer patients participated in the study. We present baseline characteristics to describe participating patients: type of cancer, status of cancer treatment, sociodemographic data (gender, age, and highest education), distress (Distress-Thermometer [37,38]), quality of life (FACT-G, Functional Assessment of Cancer Therapy-General [39]), and anxiety and depression (HADS, Hospital Anxiety Depression Scale [40]).
The Distress-Thermometer consists of 1 item with a scale from 0 to 10 and assesses experienced distress in the past week. A score between 5 or higher is considered as clinically relevant distress [41]. The FACT-G consists of 27 items, which assess the 4 subscales: physical well-being (Cronbach alpha=.851), social well-being (Cronbach alpha=.760), emotional well-being (Cronbach alpha=.702), and functional well-being (Cronbach alpha=.794). Each item is rated on a 5-point scale (0-4), resulting in a score range of 0 to 108, with a higher score indicating a better quality of life. The HADS consists of 14 items, with 7 items for each subscale, that is, anxiety (Cronbach alpha=.787) and depression (Cronbach alpha=.667). Each item is rated on a 4-point scale (0-3), leading to a maximum score of 21 for each subscale. A score between 0 and 7 is considered normal, whereas a score between 8 and 11 is considered as borderline, and a score above 11 as caseness.
Adoption
For the dimension adoption, we looked at indicators of patients’ adoption of the app intervention into their regular life, adherence, and information about barriers and facilitators for regular use. For this purpose, we analyzed the use of the app during the first 10 weeks. We derived app use data from tracking the practicing time with the audios (start and end time and type of exercise used). This information was visible only for the research team (as an XML log file through the backend) and was not displayed to users. In addition, we analyzed results from interviews with patients regarding their adoption of the app intervention.
As a first indicator for app intervention adoption, we report the number of completed app exercises per week. We considered an exercise as completed if the patient used the exercise for at least 10 min (out of 15 min). As a second indicator, we report the number of intervention dropouts versus number of continuous app users per week. Intervention dropouts were defined as enrolled patients who never completed an exercise or did not complete an exercise during 4 consecutive weeks after initial practice. A patient counted as an intervention dropout in the first of the 4 weeks, in which he or she did not complete any exercise. According to our definition, a patient who never completed an exercise is an intervention dropout at week 1. Patients not classified as intervention dropouts were defined as continuous app users. Consequently, continuous app use was defined as at least weekly use of 1 or more app exercises. We also report results from 8 semistructured patient interviews, in which we inquired about patients’ general impression regarding the app, app usage, and suggestions for improvements (for interview guideline, see Multimedia Appendix 3).
Maintenance
For the dimension maintenance, we looked into predictors for continuous app use. First, we assumed that patients with higher openness to experience are more often continuous app users. Second, we assumed that patients with higher resistance to change are less often continuous app users. In addition, we tested in explorative analyses if quality of life (FACT-G), anxiety (HADS anxiety), depression (HADS depression) at baseline and sociodemographic data (gender and age), as well as setting are associated with continuous app use. During the interviews, we also explored possible reasons for continuous app use and intervention dropout.
We measured openness to experience with the respective subscale of the NEO 5-Factor Inventory (NEO-FFI [42]) using the 5-item short version (Cronbach alpha=.755). Each item is rated on a 4-point scale (0-4), leading to a score with a range from 0 to 20. A higher score indicates greater openness to experience. We also used the Resistance to Change (RTC) Scale [43], which consists of 17 items (Cronbach alpha=.839). Each item is rated on a 6-point scale (1-6), resulting in a score with a range from 17 to 102. A higher score indicates greater resistance to change.
Sample Size
In this feasibility study, the sample size is an outcome in itself (ie, dimension reach in the evaluation framework). Therefore, we did not perform an a priori sample size calculation, but the aim was to recruit about 100 patients to conduct explorative analyses about the feasibility of the app with sufficient precision.
Data Analysis
Quantitative Data
Trained researchers entered data from printed case report forms using REDCap electronic data capture tools [44] hosted at the University Hospital Zurich. Analyses were conducted using SPSS version 25.0 (IBM Corp, Armonk, NY, USA) [45].
For the reach analyses, we used descriptive statistics (frequencies and percentages for categorical and dichotomous variables, mean and SD for continuous variables) for baseline data on sociodemographic characteristics (gender, age, and education), health status (type of cancer, status of cancer treatment, FACT-G, HADS, and Distress-Thermometer), and the setting of the enrolled patients. For the adoption analyses, we used boxplots to report median and interquartile range (IQR) of the number of completed exercises per week (week 1 to 10) for all enrolled patients, as well as for continuous app users during the 10-week intervention. In addition, we used a Kaplan-Meier plot to visualize the number of dropouts per week. For the maintenance analyses, we used Kaplan-Meier analyses with a log-rank test to compare continuous app users (ie, reversed rate of attrition) according to different baseline variables. As predictors, we used the following categorical variables: gender, setting, age groups (18-40, 41-55, 56+), high versus low well-being (FACT-G median split at 76.83), high versus low openness to experience (NEO-FFI-O median split at 17.00), high versus low resistance to change (RTC median split at 51.00), normal versus suggestive or higher anxiety or depression (HADS anxiety or depression scores of 0-7 vs 8 or higher). Subsequently, we performed a Cox proportional hazards regression with all significant predictors in the log-rank test in the Kaplan-Meier analyses.
For missing data, we used multiple imputation to conduct the Cox proportional hazards regression with a full dataset. We carried out imputations for the sum scores of FACT-G, as missing single items are already considered in the calculation of FACT-G sum scores (FACT-G sum scores are not calculated if there are more than 50% items missing in a subscale). For HADS, NEO-FFI-O, and RTC, we imputed all items with 1 or more missing values. For all other analyses (ie, descriptive analyses for the dimensions reach and adoption, Kaplan-Meier analyses for the dimension maintenance), we used complete datasets.
Qualitative Data
For the interview analyses about the adoption and maintenance of the intervention, we transcribed the recorded interviews verbatim and used thematic coding for structuring the interviews using MAXQDA 11 (VERBI Software, Berlin, Germany). Thereafter, we used content analysis according to Mayring [46].
Results
Reach
During the recruitment phase between June 2016 and December 2017, a total of 118 patients expressed interest in participating in the study and were screened for eligibility. All of the 118 patients fulfilled the eligibility criteria and received the informed consent form. By the end of December 2017, 100 patients signed and returned the informed consent form and were enrolled in the study (see Figure 1).
Figure 1.

Patient flowchart. FMI: Freiburg Mindfulness Inventory; PROMIS 29: Patient Reported Outcomes Measurement Information System 29; NEO-FFI-O: NEO Five-Factor Inventory - openness to experience; FACT-G: Functional Assessment of Cancer Therapy-General; RTC: Resistance to Change; FoP-Q-SF: Fear of Progression Questionnaire - Short Form; HADS: Hospital Anxiety Depression Scale.
Baseline characteristics of all enrolled patients (N=100), as well as of continuous app users (54/100, 54%) and intervention dropouts (46/100, 46%) are presented in Table 1. The majority of patients (83/100, 83%) were recruited independent of the MBM treatment (setting 2). Patients were 74% (74/100) female, and the mean age of all patients was 53.24 (SD 11.55) with a range of 23 to 84 years. The most common diagnosis was breast cancer (39/100, 39%). The majority of participants had completed higher education, whereas 41% (41/100) had completed secondary education and 33% (33/100) had obtained a university degree. The Distress-Thermometer indicated that the enrolled patients reported, on average, elevated and clinically relevant distress levels. The HADS scores indicated that the enrolled patients had, on average, normal scores of anxiety and depressive symptoms. Continuous app users and intervention dropouts differed in their gender, with 85% (46/85) female continuous app users versus 61% (28/61) female intervention dropouts.
Table 1.
Baseline characteristics of all enrolled patients, continuous app users, and intervention dropouts.
| Baseline characteristics | Total (N=100) | Continuous app users (n=54) | Intervention dropouts (n=46) | |
| Gender, n (%) | ||||
|
|
Female | 74 (74) | 46 (85) | 28 (61) |
|
|
Male | 26 (26) | 8 (15) | 18 (39) |
| Age (years), mean (SD) | 53.24 (11.55) | 54.77 (11.27) | 51.45 (11.74) | |
| Type of cancer, n (%) | ||||
|
|
Breast cancer | 39 (39) | 26 (48) | 13 (28) |
|
|
Colon cancer | 9 (9) | 4 (7) | 5 (11) |
|
|
Ovarian or cervical cancer | 6 (6) | 6 (11) | 0 (0) |
|
|
Lung cancer | 6 (6) | 5 (9) | 1 (2) |
|
|
Others | 40 (40) | 13 (24.) | 27 (59) |
| Status of cancer treatment, n (%) | ||||
|
|
Total removal | 46 (46) | 26 (48) | 20 (44) |
|
|
Recurrence or incomplete removal | 25 (25) | 12 (22) | 13 (28) |
|
|
Uncertain | 3 (3) | 2 (4) | 1 (2) |
|
|
Others | 26 (26) | 14 (26) | 12 (26) |
| Highest education, n (%) | ||||
|
|
Primary school | 3 (3) | 2 (4) | 1 (2) |
|
|
Apprenticeship | 22 (22) | 10 (19) | 12 (26) |
|
|
Secondary education | 41 (41) | 24 (44) | 17 (37) |
|
|
University degree | 33 (33) | 17 (32) | 16 (35) |
|
|
Unknown | 1 (1) | 0 (0) | 0 (0) |
| Setting, n (%) | ||||
|
|
Setting 1a | 17 (17) | 9 (17) | 8 (17) |
|
|
Setting 2b | 83 (83) | 45 (83) | 38 (83) |
| Distress-Thermometer, mean (SD) | 5.29 (2.31) | 5.36 (2.47) | 5.22 (2.14) | |
| FACT-Gc Quality of life, mean (SD) | 75.54 (13.85) | 76.56 (14.08) | 74.33 (13.63) | |
| HADSd anxiety, mean (SD) | 6.88 (3.50) | 7.17 (3.60) | 6.53 (3.38) | |
| HADS depression, mean (SD) | 4.96 (2.78) | 5.37 (3.05) | 4.48 (2.37) | |
aSetting 1: cancer patients with a supportive Mind Body Medicine treatment.
bSetting 2: cancer patients without a supportive Mind Body Medicine treatment.
cFACT-G: Functional Assessment of Cancer Therapy-General.
dHADS: Hospital Anxiety Depression Scale.
Adoption
The number of app exercises completed within the first 10 weeks of the intervention across all patients is presented in Figure 2. During the first week, the median of completed exercises was at 2 with an IQR of 0 to 6, that is, 50% of patients completed 2 or more exercises per week. Over the course of 10 weeks, the median dropped to 0 with an IQR of 0 to 2.5.
Figure 2.
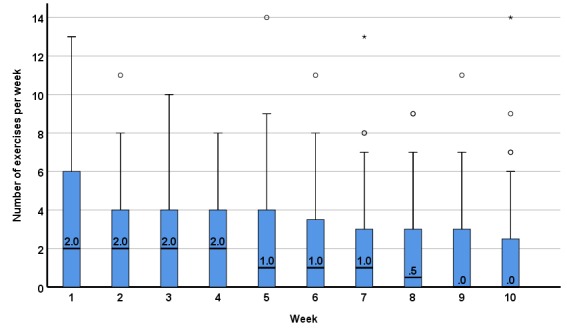
Completed app exercises by all patients who were enrolled in the study (N=100) per week (median, interquartile range).
The median of app exercises completed across the first 10 weeks of the intervention for continuous app users is presented in Figure 3. During the first week, the median of completed exercises was 4 (IQR 1-7) and dropped down to a median of 2 (IQR 1-4) in week 10.
Figure 3.
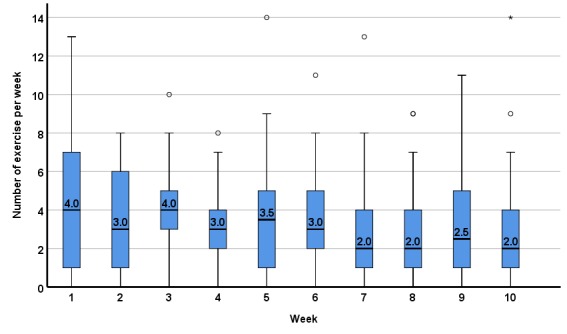
Completed app exercises by continuous app users within a 10-week app intervention (n=54) per week (median, interquartile range).
The Kaplan-Meier survival curve of continuous app users is presented in Figure 4. During the first week, 14/100 (14%) patients never started or stopped using the app exercises on a regular basis and were categorized at week 1 as intervention dropouts. At the end of the intervention, 54/100 (54%) patients were using the app exercises on a regular basis, and between week 1 and week 10, the decline can be regarded as continuous without any specific sensitive weeks to drop out.
Figure 4.
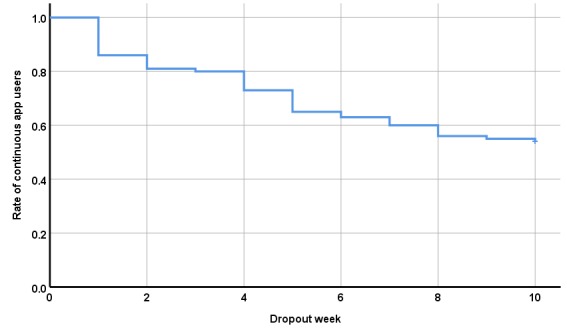
Kaplan-Meier survival curve of all enrolled patients (N=100) over 10 weeks.
Maintenance
The Kaplan-Meier plots for intervention dropouts by gender, setting, age groups, and well-being are presented in Figure 5. The Kaplan-Meier plots for intervention dropouts by openness to experience, resistance to change, anxiety, and depression are presented in Figure 6. Log-rank tests indicated 4 significant predictors for continuous app users, namely gender, openness to experience, resistance to change, and depression.
Figure 5.
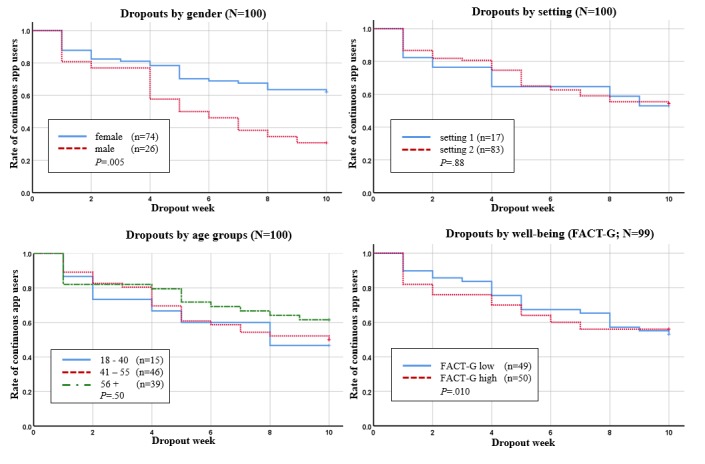
Kaplan-Meier survival curves for continuous app users by gender, setting, age groups and well-being. FACT-G: Functional Assessment of Cancer Therapy-General.
Figure 6.
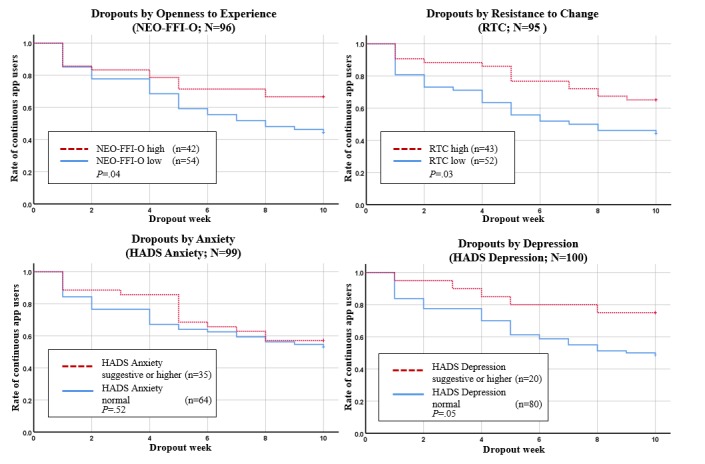
Kaplan-Meier survival curves for continuous app users by openness to experience, resistance to change, anxiety and depression. NEO-FFI-O: NEO Five-Factor Inventory - openness to experience; RTC: Resistance to Change; HADS: Hospital Anxiety Depression Scale.
At week 10, 62% (46/74) of the female patients were still using the app continuously, whereas only 31% (8/26) of the male patients were using the app continuously. Therefore, females had a better adherence to use the app continuously over time than men (P=.005). In the high openness to experience group (NEO-FFI-O), 67% (28/42) of patients still used the app continuously through week 10. In the NEO-FFI-O low openness group, 44% (24/54) used the app continuously through week 10. Thus, patients with high openness to experience had a better adherence than patients with low openness to experience over time (P=.044). In patients with normal HADS depression values, only 49% (39/80) used the app exercises continuously compared with 75% (15/20) in the HADS suggestive or higher depression group (P=.046). In patients with high RTC, 65% (28/43) used the app exercises continuously, but in the low RTC group, only 44% (23/52)of patients used the app exercises continuously through week 10. Therefore, patients in the high RTC group had a better adherence in continuous app use (P=.03). For the factors setting, age groups, well-being (FACT-G), anxiety (HADS anxiety), log-rank tests did not result in significant group differences.
The 4 significant factors of the univariate log-rank test (gender, NEO-FFI-O, RTC, HADS depression) for the prediction of continuous app users went into the multivariate Cox proportional hazards regression. The multivariate analysis indicated solely gender as an independent factor for continuous app use, with an odds ratio (OR) of 2.16 (95% CI 1.09 to 4.27), with a higher chance for attrition in male cancer patients (P=.01). The 3 other factors (NEO-FFI-O, RTC, and HADS depression) did not contribute significantly in this analysis after controlling for gender: high openness to experience was associated with lower odds for attrition (OR 0.96; 95% CI 0.89 to 1.04; P=.30); high RTC with lower odds for attrition (OR 0.98, 95% CI 0.95 to 1.01; P=.17); more depressive symptoms with lower odds for attrition (OR 0.92, 95% CI: 0.80 to 1.03; P=.13).
Qualitative Results
We invited 8 patients (2 from setting 1, 7 female, mean age 50.70 years (SD 15.06), 3 with breast cancer) to an interview, and all agreed to take part. Interviews were conducted between October 2016 and April 2017 and lasted on average 23 min. The qualitative analysis of the interviews yielded 4 themes which were as follows: (1) general feedback regarding the app, (2) suggestions for improvement, (3) personal preferences, and (4) reasons for app use and nonuse.
General feedback about the app was predominantly positive. The interviewed patients appreciated the simplicity of the app and the easy-to-use interface. One patient stated the following regarding the design:
It was great. It was very simple, very self-explanatory. You didn’t need to look around a lot and it also looked good. Yes, in any case, well designed.
Female, 35 years old
Two patients who attended an MBM course evaluated the app as a good addition to the face-to-face MBM course. The feedback about the number of exercises was mixed: Some patients regarded the implemented 3 exercises as sufficient, whereas others would welcome a larger selection of exercises. Most patients interviewed used and appreciated the reminder in the app. Some patients mentioned that they would have been less compliant without the reminders and, therefore, perceived the reminder as helpful for a continuous app use. For instance, 1 patient stated the following:
Yes, [the reminder function] was very good. A couple of times this was very good. I would have forgotten it a couple of times, if I wouldn’t have had this reminder.
Female, 63 years old
Patients offered various suggestions for improvement. Several patients mentioned that they would like exercises with background music. One patient explained it as follows:
I think it is also precisely the high art of meditation or relaxation that you can relax as much as possible while not falling asleep. Some need chimes, while others need absolute silence to be able to do this. And I realize that when it is absolutely silent, either I fall asleep or I start to contemplate. When I have some music or chimes, it works better for me personally.
Female, 42 years old
As stated above, some patients also would welcome a larger variety of exercises (eg, autogenic training) or variations in the duration of exercises. Another patient stated also that the recordings of the exercises were too clean (ie, no noises from breathing), as the exercises were recorded in a studio. This led to the patient being startled when the narrator continued with the instruction after a moment of silence. One patient mentioned she did not set up the reminder during the first time she used the app and later forgot about the reminder function. Therefore, this patient suggested that the reminder function could be placed more prominently in the app instead of the options menu. The interviewer also inquired if the patients would appreciate a feedback system in the form of exercise statistics. The majority of interviewed patients had the opinion that such a feature would not be helpful. Some patients stated that statistics might even be stressful, as it might lead to a guilty conscience if the patient is not using the exercises as often as planned. One patient suggested that statistics might be added to the app as an optional feature. Only 2 patients thought that such a feature might be helpful.
The third topic that emerged from the qualitative analysis was personal preferences. Most interviewed patients mentioned that they developed some form of preference regarding the app use (eg, preference for a specific exercise, gender of narrator, time of day when using the exercises) during the intervention while they were trying out what suits them best. One patient stated the following:
Right at the beginning I tried [to do the exercises] before I went to bed. But I’m not a fan of having my cellphone, when I fall asleep, next to my head for the entire night. For this reason I changed it to lunchtime.
Female, 31 years old
The fourth topic that emerged from the qualitative analysis involved reasons for app use and nonuse. As a reason for using the app, patients mentioned that the exercises were beneficial and helped them to relax. One patient stated the following:
[The app exercises] have been good for me. I will continue to do my exercises. […] I believe I benefit [from the exercises]. It also makes you happy.
Female, 63 years old
As reasons for nonuse, 3 patients mentioned that they had previous experience with meditation or relaxation exercises. Therefore, these patients were already used to exercise routines, which differed from the instructions or the manner in general of the app exercises. One of these patients mentioned that she had learned and was used to silent meditation, and therefore the guided exercises in the app were more distracting than helpful to her. Another patient mentioned that she had experience in guided meditation and relaxation exercises, which differed linguistically and in form of conduct compared with the app exercises. This patient mentioned that she was unable to get used to these new exercises and was repeatedly comparing the app exercises with the already known exercises. Therefore, this patient could not relax as intended during the app exercises. A third patient mentioned that she was used to exercises with more guidance and described her experience with the app as follows:
Maybe because [the instructions in the app exercises] were different from what I was used to do by myself, where [the exercise] was guided the entire time. […] I did consider it more bothersome that…[…] your thoughts drift away because you get the feeling that [the exercise] should continue.
Female, 49 years old
As a further reason for nonuse, 1 patient mentioned that she was distracted by the choice of words and expressions in the app exercises. This patient mentioned that she had studied linguistics and had learned to closely scrutinize language. This caused her to be distracted during the app exercises, which is why she stopped using the app. Another patient mentioned that she suffered from cancer-related fatigue and that she was not able to complete an exercise when she was unduly fatigued. Furthermore, 1 patient stated he had technical problems with his smartphone and therefore was not able to use the app during the entire 10 weeks.
Discussion
Summary of Findings
mHealth interventions with the aim of reducing distress in cancer patients seem promising due to easy access and potential positive effects for patients. To our knowledge, this is one of the first studies looking in detail at characteristics of users, adherence rates, and possible predictors for adherence in a mindfulness and relaxation mHealth study for cancer patients. This feasibility study showed that adherence to the mHealth intervention during the first 10 weeks was acceptable, with 54% of patients still using the app regularly in week 10 with a median of completed exercises ranging from 2 to 4 per week. Therefore, our study does not confirm the concern that adherence in mHealth interventions is in general poor, which would limit treatment implementation. The adherence of our patients is also comparable with recent research on adherence to e- and mHealth interventions for cancer patients [32,33]. A study by Beatty el al [32] reported that 60% of cancer patients completed 4 or more modules of an eHealth intervention with 6 modules, which aimed at reducing distress in cancer patients. A mindfulness app study for cancer patients and caregivers [33] reported that 71% of the participants practiced with the app on more than half of the days throughout 8 weeks.
The uptake of our intervention was good, with 117 screened and eligible patients, of whom 100 patients returned the informed consent form. In addition, 74%, mainly female, patients enrolled in this study, which is consistent with characteristics of mHealth users in other studies with 84% female patients [47] and 54% female patients [48]. The mean age of participating patients was 53 years; this is comparable with other face-to-face mindfulness and relaxation interventions [49] or Web-based interventions for cancer patients [32]. The interviews showed that the patients were satisfied with the app in general. However, several and sometimes contradictory suggestions were made for improving the app, such as less versus more guidance in the exercises and larger variety in exercises versus the notion that 3 exercises are sufficient.
Predictors for Adherence
Of a total of 8 investigated predictors for continuous app use, 4 turned out to be statistically significant. The strongest predictor was gender, with higher adherence in female cancer patients. Beyond the higher interest of female cancer patients to participate in this mindfulness and relaxation mHealth study, they were also more adherent after starting with the exercises. This result is in line with a study by Ruland et al [50], in which an analysis of use patterns in an eHealth intervention to support cancer patients’ illness management revealed that female patients used the system almost twice as often as male patients. However, a study by Duman-Lubberding et al [51] investigated the feasibility of a Web-based self-management app and did not find a gender difference in adherence. Therefore, it seems likely that the type of intervention (eg, relaxation and mindfulness meditation) might be relevant for gender differences in adherence, which is also in line with studies about the use of complementary and alternative medicine, where users tend to be more often female [52,53].
A second predictor for continuous app use was the personality trait openness to experience, whereby higher openness to experience predicted more continuous app use. This result fits with previous research, which has shown that openness to experience predicts the use of complementary and alternative medicine, including mindfulness and relaxation [54,55]. Our study confirms that higher openness to experience still predicts the adherence to a mindfulness and relaxation intervention, even if the intervention is delivered through an app.
A third predictor for continuous app use was a higher score in resistance to change. This finding is contrary to our hypothesis, as we assumed that higher resistance to change would be associated with less adherence as the intervention promotes a new health behavior. However, our results indicate the opposite. When a patient has decided to follow a new exercise routine (ie, mindfulness and relaxation mHealth intervention), a higher resistance to change actually promotes continuous app use. To our knowledge, the Resistance to Change Scale had not previously been used to predict adherence to mHealth interventions for cancer patients. However, a study conducted in China by Deng et al [56] showed that resistance to change is negatively related to the intention to use mHealth services. Another study showed that resistance to change is negatively related to perceived usefulness of mHealth in elderly people in China [57]. Therefore, on the one hand, resistance to change might be a barrier for the uptake of an mHealth intervention, but on the other, it might be supportive in adhering to a new commitment, such as the regular use of a mindfulness and relaxation app.
A fourth predictor for continuous app use was higher depressive symptoms. This finding is surprising, as depressive symptoms are associated with decreased motivation and reduced activity [58]. In line with these corollaries, a study investigating a mindfulness-based cancer recovery program [49] reported a negative correlation of depressive symptoms and practicing time of yoga at home. Another study [59] reported that moderate to severe depressive symptoms predicted lower adherence to adjuvant cancer therapies. However, a study by Børøsund et al [60] found that high levels of depression were associated with high use of components of a Web-based illness management program in breast cancer patients. As depressed patients are oftentimes troubled with motivational deficits and face difficulties to stay active, the development of effective interventions with a good adherence in depressed patients is highly relevant. Our study indicates that mindfulness and relaxation mHealth interventions seem a feasible tool as supportive interventions for cancer patients with elevated depressive symptoms. This finding might also indicate that some patients adhere better to mindfulness and relaxation (ie, patients with higher depressive symptoms), whereas other patient groups with lower levels of distress are not in need of such interventions or might prefer other intervention types.
Limitations
This study has some limitations. First, the number of potentially interested patients for this intervention could not be assessed. Therefore, we were not able to calculate the rate of the total number of eligible cancer patients compared with the number of cancer patients with interest in a mindfulness and relaxation mHealth intervention. Second, for our definition of continuous app, we had no empirical data because the necessary dose for clinically significant improvements is still unclear for this kind of mHealth intervention. Instead, we opted for a clinical and rational justification, in which the term “continuous” use was operationalized as an at least weekly use of 1 or more app exercises. Third, the use of generated categories for age and the median split for other variables as predictors can be challenged. For age, we chose 3 age categories that represent patients of younger (18-40), middle (41-55), and older (56 plus) age. The use of median split variables has been critically discussed in the literature (see eg, Iacobucci et al [61]), with a major critique being the loss of information. In our case, the loss of information can be justified with the illustrative capacity of Kaplan-Meier survival curves and the following use of a multivariate Cox proportional hazards regression. Fourth, as the sample size was an outcome in itself, we did not perform an a priori sample size calculation. With a sample size (N) of 100, we had a power of 0.63 in the Cox proportional hazards regression for the main effect (OR 2.16) of gender as a predictor. For a power of 0.8, a sample size (N) of 150 would be necessary.
Conclusions and Future Research
The acceptable adherence to the intervention and the generally positive feedback by patients indicate that this app intervention is feasible. Suggestions for improvement by patients indicate that patients’ needs are heterogeneous, which should be taken into account when developing other mHealth interventions. Due to the acceptable adherence and positive feedback by cancer patients, mindfulness and relaxation mHealth interventions might be promising supportive interventions, also for cancer patients with elevated depressive symptoms.
To further prove the importance of mindfulness and relaxation mHealth interventions for cancer patients, future research needs to investigate their effectiveness. As the dose potentially influences the effectiveness of mindfulness and relaxation interventions, future research should also look into dose-response relationships between the time spent exercising with the app and health outcomes. Knowledge of such a dose-response relationship could be of use to guide subsequent studies regarding intervention duration and practice recommendation for patients. This study suggests that variability across patients in weekly app use is large. About half of the patients used the app exercises continuously over 10 weeks and therefore adhered to the intervention. These interindividual differences in the use of app exercises underline the importance to take adherence into account when analyzing effectiveness data. Furthermore, these interindividual differences on adherence bring up the question if mindfulness- and relaxation-based mHealth interventions are better suited for specific patient groups (eg females, patients with higher depressive symptoms). In turn, male patients or patients with less distress might not be in need of such interventions or might require additional motivational interventions.
Acknowledgments
This study was funded by the Swiss Cancer League (KLS-3564-02-2015). The authors acknowledge and thank the contribution of Isabelle Werninger, who supported the project in both administration and data entry.
Abbreviations
- CRF
case report form
- FACT-G
Functional Assessment of Cancer Therapy-General
- FMI
Freiburg Mindfulness Inventory
- FoP-Q-SF
Fear of Progression Questionnaire - Short Form
- HADS
Hospital Anxiety Depression Scale
- ICI
Institute for Complementary and Integrative Medicine, University Hospital Zurich
- IQR
interquartile range
- MBM
Mind Body Medicine
- mHealth
mobile health
- NEO-FFI-O
NEO Five-Factor Inventory - openness to experience
- OR
odds ratio
- PROMIS 29
Patient Reported Outcomes Measurement Information System 29
- RTC
Resistance to Change
Screenshots of the CanRelax App exercises.
{kind=link}
Screenshots of the CanRelax App notification feature.
{kind=link}
Interview guideline.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015 Mar 01;136(5):E359–86. doi: 10.1002/ijc.29210. doi: 10.1002/ijc.29210. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization Cancer. [2018-05-15]. 2018 http://www.who.int/en/news-room/fact-sheets/detail/cancer .
- 3.Mehnert A, Brähler E, Faller H, Härter M, Keller M, Schulz H, Wegscheider K, Weis J, Boehncke A, Hund B, Reuter K, Richard M, Sehner S, Sommerfeldt S, Szalai C, Wittchen H, Koch U. Four-week prevalence of mental disorders in patients with cancer across major tumor entities. J Clin Oncol. 2014 Nov 01;32(31):3540–6. doi: 10.1200/JCO.2014.56.0086.JCO.2014.56.0086 [DOI] [PubMed] [Google Scholar]
- 4.Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. The prevalence of psychological distress by cancer site. Psychooncology. 2001;10(1):19–28. doi: 10.1002/1099-1611(200101/02)10:1<19::aid-pon501>3.0.co;2-6.10.1002/1099-1611(200101/02)10:1<19::AID-PON501>3.0.CO;2-6 [DOI] [PubMed] [Google Scholar]
- 5.Carlson LE. Distress Management Through Mind-Body Therapies in Oncology. J Natl Cancer Inst Monogr. 2017 Nov 01;2017(52) doi: 10.1093/jncimonographs/lgx009.4617824 [DOI] [PubMed] [Google Scholar]
- 6.Faller H, Koch U, Brähler Elmar, Härter Martin, Keller M, Schulz H, Wegscheider K, Weis J, Boehncke A, Hund B, Reuter K, Richard M, Sehner S, Szalai C, Wittchen H, Mehnert A. Satisfaction with information and unmet information needs in men and women with cancer. J Cancer Surviv. 2016 Feb;10(1):62–70. doi: 10.1007/s11764-015-0451-1.10.1007/s11764-015-0451-1 [DOI] [PubMed] [Google Scholar]
- 7.Burg MA, Adorno G, Lopez EDS, Loerzel V, Stein K, Wallace C, Sharma DKB. Current unmet needs of cancer survivors: analysis of open-ended responses to the American Cancer Society Study of Cancer Survivors II. Cancer. 2015 Feb 15;121(4):623–30. doi: 10.1002/cncr.28951. doi: 10.1002/cncr.28951. [DOI] [PubMed] [Google Scholar]
- 8.Carlson LE, Angen M, Cullum J, Goodey E, Koopmans J, Lamont L, MacRae JH, Martin M, Pelletier G, Robinson J, Simpson JSA, Speca M, Tillotson L, Bultz BD. High levels of untreated distress and fatigue in cancer patients. Br J Cancer. 2004 Jun 14;90(12):2297–304. doi: 10.1038/sj.bjc.6601887. doi: 10.1038/sj.bjc.6601887.6601887 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Waller A, Williams A, Groff SL, Bultz BD, Carlson LE. Screening for distress, the sixth vital sign: examining self-referral in people with cancer over a one-year period. Psychooncology. 2013 Feb;22(2):388–95. doi: 10.1002/pon.2102. [DOI] [PubMed] [Google Scholar]
- 10.Ryan H, Schofield P, Cockburn J, Butow P, Tattersall M, Turner J, Girgis A, Bandaranayake D, Bowman D. How to recognize and manage psychological distress in cancer patients. Eur J Cancer Care (Engl) 2005 Mar;14(1):7–15. doi: 10.1111/j.1365-2354.2005.00482.x.ECC482 [DOI] [PubMed] [Google Scholar]
- 11.Faller H, Schuler M, Richard M, Heckl U, Weis J, Küffner R. Effects of psycho-oncologic interventions on emotional distress and quality of life in adult patients with cancer: systematic review and meta-analysis. J Clin Oncol. 2013 Feb 20;31(6):782–93. doi: 10.1200/JCO.2011.40.8922.JCO.2011.40.8922 [DOI] [PubMed] [Google Scholar]
- 12.Sheard T, Maguire P. The effect of psychological interventions on anxiety and depression in cancer patients: results of two meta-analyses. Br J Cancer. 1999 Aug;80(11):1770–80. doi: 10.1038/sj.bjc.6690596. http://europepmc.org/abstract/MED/10468295 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Carlson LE, Zelinski E, Toivonen K, Flynn M, Qureshi M, Piedalue K, Grant R. Mind-Body Therapies in Cancer: What Is the Latest Evidence? Curr Oncol Rep. 2017 Aug 18;19(10):67. doi: 10.1007/s11912-017-0626-1.10.1007/s11912-017-0626-1 [DOI] [PubMed] [Google Scholar]
- 14.Monti DA, Sufian M, Peterson C. Potential role of mind-body therapies in cancer survivorship. Cancer. 2008 Jun 01;112(11 Suppl):2607–16. doi: 10.1002/cncr.23443. doi: 10.1002/cncr.23443. [DOI] [PubMed] [Google Scholar]
- 15.Astin JA, Shapiro SL, Eisenberg DM, Forys KL. Mind-Body Medicine: State of the Science, Implications for Practice. The Journal of the American Board of Family Medicine. 2003 Mar 01;16(2):131–147. doi: 10.3122/jabfm.16.2.131. [DOI] [PubMed] [Google Scholar]
- 16.Greenlee H, DuPont-Reyes MJ, Balneaves LG, Carlson LE, Cohen MR, Deng G, Johnson JA, Mumber M, Seely D, Zick SM, Boyce LM, Tripathy D. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin. 2017 May 06;67(3):194–232. doi: 10.3322/caac.21397. doi: 10.3322/caac.21397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Huang H, He M, Wang H, Zhou M. A meta-analysis of the benefits of mindfulness-based stress reduction (MBSR) on psychological function among breast cancer (BC) survivors. Breast Cancer. 2016 Jul;23(4):568–76. doi: 10.1007/s12282-015-0604-0.10.1007/s12282-015-0604-0 [DOI] [PubMed] [Google Scholar]
- 18.Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits. Journal of Psychosomatic Research. 2004 Jul;57(1):35–43. doi: 10.1016/s0022-3999(03)00573-7. [DOI] [PubMed] [Google Scholar]
- 19.Dimidjian S, Arch JJ, Schneider RL, Desormeau P, Felder JN, Segal ZV. Considering Meta-Analysis, Meaning, and Metaphor: A Systematic Review and Critical Examination of “Third Wave” Cognitive and Behavioral Therapies. Behav Ther. 2016 Dec;47(6):886–905. doi: 10.1016/j.beth.2016.07.002.S0005-7894(16)30048-X [DOI] [PubMed] [Google Scholar]
- 20.Blanck P, Perleth S, Heidenreich T, Kröger P, Ditzen B, Bents H, Mander J. Effects of mindfulness exercises as stand-alone intervention on symptoms of anxiety and depression: Systematic review and meta-analysis. Behav Res Ther. 2018 Mar;102:25–35. doi: 10.1016/j.brat.2017.12.002.S0005-7967(17)30244-9 [DOI] [PubMed] [Google Scholar]
- 21.King N, Balneaves LG, Levin GT, Nguyen T, Nation JG, Card C, Truant T, Carlson LE. Surveys of Cancer Patients and Cancer Health Care Providers Regarding Complementary Therapy Use, Communication, and Information Needs. Integr Cancer Ther. 2015 Nov;14(6):515–24. doi: 10.1177/1534735415589984.1534735415589984 [DOI] [PubMed] [Google Scholar]
- 22.Carmody J, Baer RA. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J Behav Med. 2008 Feb;31(1):23–33. doi: 10.1007/s10865-007-9130-7. [DOI] [PubMed] [Google Scholar]
- 23.Beatty L, Lambert S. A systematic review of internet-based self-help therapeutic interventions to improve distress and disease-control among adults with chronic health conditions. Clin Psychol Rev. 2013 Jun;33(4):609–22. doi: 10.1016/j.cpr.2013.03.004.S0272-7358(13)00044-5 [DOI] [PubMed] [Google Scholar]
- 24.Luxton D, McCann R, Bush N, Mishkind M, Reger G. mHealth for mental health: Integrating smartphone technology in behavioral healthcare. Prof Psychol Res Pr. 2011;42(6):505–512. doi: 10.1037/a0024485. [DOI] [Google Scholar]
- 25.Statista Smartphone user penetration as percentage of total global population from to 2021. 2014. [2018-05-22]. 2018 https://www.statista.com/statistics/203734/global-smartphone-penetration-per-capita-since-2005/
- 26.Price M, Yuen EK, Goetter EM, Herbert JD, Forman EM, Acierno R, Ruggiero KJ. mHealth: a mechanism to deliver more accessible, more effective mental health care. Clin Psychol Psychother. 2014 Aug;21(5):427–36. doi: 10.1002/cpp.1855. http://europepmc.org/abstract/MED/23918764 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McCorkle R, Ercolano E, Lazenby M, Schulman-Green D, Schilling LS, Lorig K, Wagner EH. Self-management: Enabling and empowering patients living with cancer as a chronic illness. CA Cancer J Clin. 2011 Jan;61(1):50–62. doi: 10.3322/caac.20093. doi: 10.3322/caac.20093.caac.20093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mikolasek M, Berg J, Witt CM, Barth J. Effectiveness of Mindfulness- and Relaxation-Based eHealth Interventions for Patients with Medical Conditions: a Systematic Review and Synthesis. Int J Behav Med. 2017 Jul 27; doi: 10.1007/s12529-017-9679-7.10.1007/s12529-017-9679-7 [DOI] [PubMed] [Google Scholar]
- 29.Fish J, Brimson J, Lynch S. Mindfulness Interventions Delivered by Technology Without Facilitator Involvement: What Research Exists and What Are the Clinical Outcomes? Mindfulness (N Y) 2016 Jun;7(5):1011–1023. doi: 10.1007/s12671-016-0548-2. http://europepmc.org/abstract/MED/27642370 .548 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Spijkerman MPJ, Pots WTM, Bohlmeijer ET. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin Psychol Rev. 2016 Apr;45:102–14. doi: 10.1016/j.cpr.2016.03.009. https://linkinghub.elsevier.com/retrieve/pii/S0272-7358(15)30062-3 .S0272-7358(15)30062-3 [DOI] [PubMed] [Google Scholar]
- 31.Eysenbach G. The law of attrition. J Med Internet Res. 2005 Mar;7(1):e11. doi: 10.2196/jmir.7.1.e11. http://www.jmir.org/2005/1/e11/ v7e11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Beatty L, Kemp E, Binnion C, Turner J, Milne D, Butow P, Lambert S, Yates P, Yip D, Koczwara B. Uptake and adherence to an online intervention for cancer-related distress: older age is not a barrier to adherence but may be a barrier to uptake. Support Care Cancer. 2017 Dec;25(6):1905–1914. doi: 10.1007/s00520-017-3591-1.10.1007/s00520-017-3591-1 [DOI] [PubMed] [Google Scholar]
- 33.Kubo A, Altschuler A, Kurtovich E, Hendlish S, Laurent C, Kolevska T, Li Y, Avins A. A Pilot Mobile-Based Mindfulness Intervention for Cancer Patients and Their Informal Caregivers. Mindfulness. 2018:2018–10. doi: 10.1007/s12671-018-0931-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999 Sep;89(9):1322–1327. doi: 10.2105/ajph.89.9.1322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Glaser B, Strauss A. Discovery of grounded theory: Strategies for qualitative review. Chicago, IL: Aldine De Gruyter; 1967. [Google Scholar]
- 36.Blödt S, Pach D, Roll S, Witt CM. Effectiveness of app-based relaxation for patients with chronic low back pain (Relaxback) and chronic neck pain (Relaxneck): study protocol for two randomized pragmatic trials. Trials. 2014 Dec 15;15:490. doi: 10.1186/1745-6215-15-490. https://trialsjournal.biomedcentral.com/articles/10.1186/1745-6215-15-490 .1745-6215-15-490 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.National Comprehensive Cancer Network Distress Management Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2003 Jul 01;1(3):344–344. doi: 10.6004/jnccn.2003.0031. [DOI] [PubMed] [Google Scholar]
- 38.Mehnert A, Müller D, Lehmann C, Koch U. Die deutsche Version des NCCN Distress-Thermometers. Zeitschrift für Psychiatrie, Psychologie und Psychotherapie. 2006 Jan;54(3):213–223. doi: 10.1024/1661-4747.54.3.213. [DOI] [Google Scholar]
- 39.Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, Silberman M, Yellen SB, Winicour P, Brannon J. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol. 1993 Mar;11(3):570–9. doi: 10.1200/JCO.1993.11.3.570. [DOI] [PubMed] [Google Scholar]
- 40.Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983 Jun;67(6):361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 41.Jacobsen PB, Donovan KA, Trask PC, Fleishman SB, Zabora J, Baker F, Holland JC. Screening for psychologic distress in ambulatory cancer patients. Cancer. 2005 Apr 01;103(7):1494–502. doi: 10.1002/cncr.20940. doi: 10.1002/cncr.20940. [DOI] [PubMed] [Google Scholar]
- 42.Costa P, McCrae R. Neo PI/FFI manual supplement for use with the NEO Personality Inventory and the NEO Five-Factor Inventory. Odessa, FL: Psychological Assessment Resources; 1989. [Google Scholar]
- 43.Oreg S. Resistance to change: Developing an individual differences measure. Journal of Applied Psychology. 2003;88(4):680–693. doi: 10.1037/0021-9010.88.4.680. [DOI] [PubMed] [Google Scholar]
- 44.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009 Apr;42(2):377–81. doi: 10.1016/j.jbi.2008.08.010. https://linkinghub.elsevier.com/retrieve/pii/S1532-0464(08)00122-6 .S1532-0464(08)00122-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp; 2017. [Google Scholar]
- 46.Mayring P. Qualitative Inhaltsanalyse: Grundlagen und Techniken. 11th edition. Basel: Beltz Pädagogik; 2010. [Google Scholar]
- 47.Elavsky S, Smahel D, Machackova H. Who are mobile app users from healthy lifestyle websites? Analysis of patterns of app use and user characteristics. Transl Behav Med. 2017 Dec;7(4):891–901. doi: 10.1007/s13142-017-0525-x. http://europepmc.org/abstract/MED/28929368 .10.1007/s13142-017-0525-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Wang BR, Park J, Chung K, Choi IY. Influential Factors of Smart Health Users according to Usage Experience and Intention to Use. Wireless Pers Commun. 2014 Apr 24;79(4):2671–2683. doi: 10.1007/s11277-014-1769-0. [DOI] [Google Scholar]
- 49.Tamagawa R, Speca M, Stephen J, Pickering B, Lawlor-Savage L, Carlson LE. Predictors and Effects of Class Attendance and Home Practice of Yoga and Meditation Among Breast Cancer Survivors in a Mindfulness-Based Cancer Recovery (MBCR) Program. Mindfulness. 2015 Jan 9;6(5):1201–1210. doi: 10.1007/s12671-014-0381-4. [DOI] [Google Scholar]
- 50.Ruland CM, Maffei RM, Børøsund E, Krahn A, Andersen T, Grimsbø GH. Evaluation of different features of an eHealth application for personalized illness management support: cancer patients' use and appraisal of usefulness. Int J Med Inform. 2013 Jul;82(7):593–603. doi: 10.1016/j.ijmedinf.2013.02.007.S1386-5056(13)00041-5 [DOI] [PubMed] [Google Scholar]
- 51.Duman-Lubberding S, van Uden-Kraan C F, Jansen F, Witte BI, van der Velden L A, Lacko M, Cuijpers P, Leemans CR, Verdonck-de Leeuw I M. Feasibility of an eHealth application "OncoKompas" to improve personalized survivorship cancer care. Support Care Cancer. 2016 May;24(5):2163–2171. doi: 10.1007/s00520-015-3004-2. http://europepmc.org/abstract/MED/26563178 .10.1007/s00520-015-3004-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Bishop FL, Lewith GT. Who Uses CAM? A Narrative Review of Demographic Characteristics and Health Factors Associated with CAM Use. Evid Based Complement Alternat Med. 2010 Mar;7(1):11–28. doi: 10.1093/ecam/nen023. doi: 10.1093/ecam/nen023.nen023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Reid R, Steel A, Wardle J, Trubody A, Adams J. Complementary medicine use by the Australian population: a critical mixed studies systematic review of utilisation, perceptions and factors associated with use. BMC Complement Altern Med. 2016 Jun 11;16:176. doi: 10.1186/s12906-016-1143-8. https://bmccomplementalternmed.biomedcentral.com/articles/10.1186/s12906-016-1143-8 .10.1186/s12906-016-1143-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Thomson P, Jones J, Browne M, Leslie SJ. Psychosocial factors that predict why people use complementary and alternative medicine and continue with its use: a population based study. Complement Ther Clin Pract. 2014 Nov;20(4):302–10. doi: 10.1016/j.ctcp.2014.09.004.S1744-3881(14)00065-6 [DOI] [PubMed] [Google Scholar]
- 55.Honda K, Jacobson JS. Use of complementary and alternative medicine among United States adults: the influences of personality, coping strategies, and social support. Prev Med. 2005 Jan;40(1):46–53. doi: 10.1016/j.ypmed.2004.05.001.S0091743504002695 [DOI] [PubMed] [Google Scholar]
- 56.Deng Z, Mo X, Liu S. Comparison of the middle-aged and older users' adoption of mobile health services in China. Int J Med Inform. 2014 Mar;83(3):210–24. doi: 10.1016/j.ijmedinf.2013.12.002.S1386-5056(13)00249-9 [DOI] [PubMed] [Google Scholar]
- 57.Guo X, Sun Y, Wang N, Peng Z, Yan Z. The dark side of elderly acceptance of preventive mobile health services in China. Electron Markets. 2012 Dec 11;23(1):49–61. doi: 10.1007/s12525-012-0112-4. [DOI] [Google Scholar]
- 58.Psychiatric Association . Diagnostic and statistical manual of mental disorders (DSM-5). 5th edition. Washington, DC: American Psychiatric Association; 2016. [Google Scholar]
- 59.Barber B, Dergousoff J, Nesbitt M, Mitchell N, Harris J, O'Connell D, Côté D, Biron V, Seikaly H. Depression as a predictor of postoperative functional performance status (PFPS) and treatment adherence in head and neck cancer patients: a prospective study. J Otolaryngol Head Neck Surg. 2015 Sep 18;44:38. doi: 10.1186/s40463-015-0092-4. https://journalotohns.biomedcentral.com/articles/10.1186/s40463-015-0092-4 .10.1186/s40463-015-0092-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Børøsund E, Cvancarova M, Ekstedt M, Moore SM, Ruland CM. How user characteristics affect use patterns in web-based illness management support for patients with breast and prostate cancer. J Med Internet Res. 2013 Mar 01;15(3):e34. doi: 10.2196/jmir.2285. http://www.jmir.org/2013/3/e34/ v15i3e34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Iacobucci D, Posavac SS, Kardes FR, Schneider MJ, Popovich DL. The median split: Robust, refined, and revived. Journal of Consumer Psychology. 2015 Oct;25(4):690–704. doi: 10.1016/j.jcps.2015.06.014. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Screenshots of the CanRelax App exercises.
Screenshots of the CanRelax App notification feature.
Interview guideline.