

Supplemental Digital Content is available in the text
Keywords: health services administration, health facility environment, quality of health care, safety management, occupational health, patient safety, factor analysis
Abstract
Research shows an instability in the way workers in the healthcare field live, and a prevalence of an unhealthy lifestyle. Exhaustion, an overload of obligations and responsibilities and dissatisfaction are all factors that may result in both physical and mental disorders. The aim of our study is to analyze the association between individual and occupational aspects of hospital workers and their job satisfaction, burnout syndrome, and depressive symptoms, as well as the relationship between these 3 factors.
A transversal study was carried out from August to November 2016 in a teaching hospital that is a reference in healthcare to 13 cities in the State of São Paulo, Brazil. Workers with an employment relationship of a period of 3 months or longer were included in the study. Subjects for the study were recruited through random probability sampling. Data were collected using psychometric tools in order to analyze job satisfaction (Job Satisfaction Survey [JSS]), the presence of burnout syndrome (Maslach Burnout Inventory [MBI]) and depressive symptoms (Patient Health Questionnaire-9). Adjusted analyses were conducted and the prevalence ratio (PR) was calculated using Poisson regression. The partial least squares structural equation modeling (PLS-SEM) was used for the analyses.
The final sample of this study comprised 271 professionals. Administrative workers or technical support workers from the hospital showed to be more satisfied in their jobs compared to the healthcare professionals (P = .02). Time of professional activity was also associated with job satisfaction (P = .03). Men displayed burnout syndrome approximately twice as often as women (PR = 1.98; 95% CI: 1.03–3.79; P = .04). Workers who had a low household income presented a predominance twice as high of depressive symptoms (PR = 2.84; 95% CI: 1.24–6.51; P = .01). PLS-SEM confirmed the causal and inverse relationship between burnout syndrome and job satisfaction (P < .001). Depressive symptoms were considered predictors for professional exhaustion (P < .001).
Personal and occupational factors of hospital workers were associated with job satisfaction, burnout syndrome, and depressive symptoms. The absence of burnout was identified as a predictive aspect for job satisfaction, and depressive symptoms as a predictor for professional exhaustion.
1. Introduction
Healthcare professionals are exposed to a large emotional load derived from the suffering and pain of their patients and families. This is also associated with high work demands and their responsibilities.[1] In the long term, the exposure to these situations may affect the individual's personal fulfillment as well as their psychological aspects,[1,2] which may result in the use of medicines, alcohol, or even illegal drugs in order to alleviate the symptoms.[3,4]
The yearly estimate of 400 suicides committed by doctors, in the United States, has raised great concern.[5] Therefore, several organizations are gathering to make this scenario known, with the purpose of allowing interventions to be made.[5]
Physical and mental disorders are problems caused by the lack of well-being in an individual's daily life.[6] This lack of well-being can be a consequence of job dissatisfaction, resulting in a poor quality of life.[6]
Opportunities, institutional performance, a work team, benefits, rewards, and a humanistic supervision are some factors that establish professional satisfaction.[7,8] Healthcare professionals often experience a disparity regarding these aspects, resulting in job dissatisfaction.[9]
Burnout syndrome consists of a 3-dimensional process: emotional exhaustion, depersonalization, and decreased personal fulfillment.[10] Practitioners develop such symptoms due to psychological aspects and they express their feelings in relation to their patients in a negative way.[10] This is characterized as a social issue of great relevance, which generates high organizational costs.[10,11]
Depression is manifested through the following symptoms: depressive mood, lack of interest for everyday tasks, changes in appetite and weight, sleeping disorders, expressive agitation or slowness, fatigue, recurrent feelings of worthlessness and guilt, lack of concentration, and suicidal thoughts.[12] Work overload and the aspects that are caused by such instability are indicated as predictive factors for the development of disorders associated with depressive symptoms.[13,14]
The aim of our study is to analyze the association between individual and occupational aspects of hospital workers and their job satisfaction, burnout syndrome, and depressive symptoms, as well as the relationship between these 3 factors.
2. Methods
2.1. Study design
This is a cross-sectional study conducted in a teaching hospital between August and November of 2016.
2.2. Setting
We conducted the research in a teaching hospital, in the northwestern area of São Paulo State, in Brazil. The hospital contained a total of 174 beds, and 16 of them were in the intensive care unit. This hospital is a reference in healthcare for 13 cities, and it is a private and philanthropic institution, characterized by urgency and emergency aid. It also specializes in medical care to high-risk pregnancies and high-complexity care in nephrology, orthopedics, and traumatology.
In 2016, the institutional mortality rate was 5% and the hospital mortality rate 6%, with an average of 640 hospitalizations and 360 surgeries per month.
In July 2016, 7% of the hospital workers were away from their duties or on medical leave. The main cause for their leave was due to a depression diagnosis (29%).
2.3. Participants
Professionals with an employment relationship longer than or equal to 3 months and who consented to participate were included in the study. Individuals under notice, on medical leave, on vacation period or workers from third-party companies were not included.
Participants were selected through random sampling from the list of professionals obtained from the institution's human resources department and were invited to participate by the main researcher.
2.4. Variables
Sociodemographic, economic and occupational characteristics were analyzed. They were self-reported by the participants and included: gender (male or female), age (in years and categorized in the age range of 18–35, 36–50 or ≥ 51), socioeconomic class (A, B, C or D, E), level of education (higher education, complete secondary education or incomplete secondary education), profession or field of activity (health professionals or ones from the technical and administrative support), interaction or direct contact with the patient (yes or no), and time working in the area (in years, categorized in the time range of < 1, 1–2, 3–4, 5–10, 11–20 or ≥ 21).
Job satisfaction, burnout syndrome, and depression symptoms were measured as dependent variables.
2.5. Data sources and measurement
Data were collected through an electronic questionnaire filled out by the participant in a device (tablets), after signing the informed consent form.
The economic classification was performed through the Brazilian Criteria,[15] an instrument composed of 15 items that analyze ownership of assets, housing conditions, the head of the household's level of education and access to public services. The household monthly income in Brazilian real (BRL) was estimated for each stratum, which was converted to United States dollars (USD) based on the currency of the Central Bank of Brazil on July 1, 2016 (1 USD = 3.2292 BRL): Class A 20,888 BRL, 6468 USD; Class B 4852–9254 BRL, 1503–2866 USD; Class C 1625–2705 BRL, 503–838 USD and Class D and E 768 BRL, 238 USD.[15]
Job satisfaction was measured by the Job Satisfaction Survey (JSS) in its translated and validated version for Brazil.[16] This survey is best applied in heterogeneous populations, since it provides a wide and comprehensive investigation and contemplates different situations of employment contentment.[16–18] The JSS consists of 36 items distributed in 9 dimensions: payment, promotion, supervision, benefits, contingent rewards, operating procedures, coworkers, nature of work, and communication. The answers are given by a 6-point Likert scale.[19] The analyzed total score may correspond to: dissatisfaction (score of 36–108), does not represent dissatisfaction or satisfaction (score of 109–143), and satisfaction (score of 144–216).[17]
We used the Maslach Burnout Inventory–Human Services Survey (MBI–HSS)[20,21] considered a gold-standard in the measurement of professional exhaustion,[22] in order to identify burnout syndrome. This tool consists of 3 subscales, with a total of 22 items that assess the characteristics of the burnout syndrome: emotional exhaustion (EE), depersonalization (DE), and low personal accomplishment (lPA).[20] A Likert scale[19] was used to clarify our results. We adopted a scoring system ranging from 1 to 5, which was already used in other researches conducted in Brazil.[23] The results are displayed in 3 different scores as each subscale was analyzed separately.[20] In our study, we considered burnout syndrome as the simultaneous occurrence of relevant problems (moderate or severe), including EE (≥ 16), DE (≥ 7), and lPA (≤ 38), in the MBI–HSS.
Screening of depressive symptoms was performed through the Patient Health Questionnaire-9 (PHQ-9).[24] The questionnaire consisted of 9 items based on the Statistical Diagnosis of Mental Disorders criteria,[12] which show the presence of depressive mood, anhedonia, sleeping disorders, fatigue, lack of energy, changes in appetite and weight, feelings of guilt or worthlessness, difficulty concentrating, slowness or agitation, and suicidal thoughts in the last 14 days. The 9 items of this tool correspond to a Likert scale[19] and the total score ranges from 0 to 27.[24] Evidence has shown that a cutoff point of ≥ 9 was considered to have the highest sensibility (77.5%) and specificity (86.7%) in Brazil.[25] Therefore, we adopted this method to categorize individuals who displayed relevant episodes of depressive symptoms.
2.6. Bias
In order to minimize the risk of information bias and distortions that could force positive or negative answers, the research was presented to the management group and to the leaders of the hospital, in order to emphasize its importance and to disseminate the aim of the study among all the work teams. This procedure had the intention to provide autonomy and prevent any discomfort so that the professionals could express their true perceptions, without fear of retaliation, especially in the questions that assessed superiors or the institution.
Furthermore, the researcher responsible for the data collection was trained in order to comprehend the method and application of the instruments. The researcher went to the work sectors, where the collection also occurred, in the most opportune moment for the recruited employee. After signing the informed consent form, the tablet was handed to the participant, while the researcher was available to clarify any doubts. This measure sought to ensure the confidentiality and comfort of the participants.
2.7. Study size
We calculated the number of participants (246, 95% CI) from the total number of workers in the hospital (n = 677), considering confidence limits of 5%, and design effect of 1 (random population sample).[26] We reached a total number of 270 participants after 10% was added to our previous amount of individuals. We first prepared a list of 270 workers randomly selected and another list containing the same amount of people in order to replace participants who presented objections or other reasons not to participate in the study.
2.8. Statistical methods
Firstly, descriptive statistics of the variables measured in our study was performed. Subsequently, we calculated the frequency for the categorical variables, and the mean and standard deviation (SD) for the continuous variables.
Adjusted analyses (multivariate) were performed according to analytical conjecture. We then calculated prevalence ratio (PR) through Poisson regression in order to estimate the association between the participants’ characteristics and the dependent variables.
Partial least squares structural equation modeling (PLS-SEM)[27] was used to estimate dependency relationships, as well as to determine how the primary outcomes are linked in our study. This process was carried out in 2 steps: validation and reliability of the measurements; analysis of the structural model.[27]
To complete the first step, we determined job satisfaction according to the results obtained through the JSS, burnout according to the MBI results, and depressive symptoms according to the PHQ-9.
We verified convergent validity considering the values obtained through average variance extracted (AVE), and these values are recommended to be >0.5.[27,28] For discriminant validity, we adopted comparison criteria, in which the square roots of the AVE must be higher than the correlation values among the 3 constructs.[27,28] The Cronbach's alpha coefficient (α) and the composite reliability (CR) were used for reliability assessment. Values > 0.6 were considered acceptable.[27] The factorial loads of the instruments’ domains were also described, with acceptable values ≥0.5.[27]
For the second step, we analyzed Pearson's correlation coefficient (R2) as follows: small effect = R2 ≥ 2%; medium effect = R2 ≥ 13%; and large effect = R2 ≥ 26%.[29] Predictive relevance (Q2) was assessed by a redundancy coefficient and was considered appropriate when Q2 > 0.[27] Coefficient of community determined the effect size (f2) as small (f2 ≥ 0.02), medium (f2 ≥ 0.15), and large (f2 ≥ 0.35).[27] The goodness-of-fit index (GoF) was considered acceptable when its value was > 0.36.[30]
At last, we established the significance and relationship between the 3 aspects we analyzed and path coefficient, which is expressed by values ranging from −1 to 1.[27] Regarding the path coefficient, values close to 1 (or to −1 for negative associations) show a strong correlation.[27]
Path diagrams were used to illustrate the relationship between the constructs. Straight arrows represent causal relationships. The arrows are pointed from the predictive variable (or construct) to the dependent variable.[27] Curved arrows correspond to the correlations between the constructs; however, no causality was involved.[27]
We used the statistics software Stata (version 13.1) for all analyses. The confidence interval and the significance level were standardized in 95% (95% CI) and 5%, respectively.
2.9. Ethical aspects
The research was approved by the Research Ethics Committee of the State University of São Paulo, School of Pharmaceutical Sciences of Araraquara, Brazil (Protocol no. 1.644.886/2016). An authorization was obtained from the institution in which the research was conducted and all participants provided a written informed consent form.
3. Results
3.1. Participants
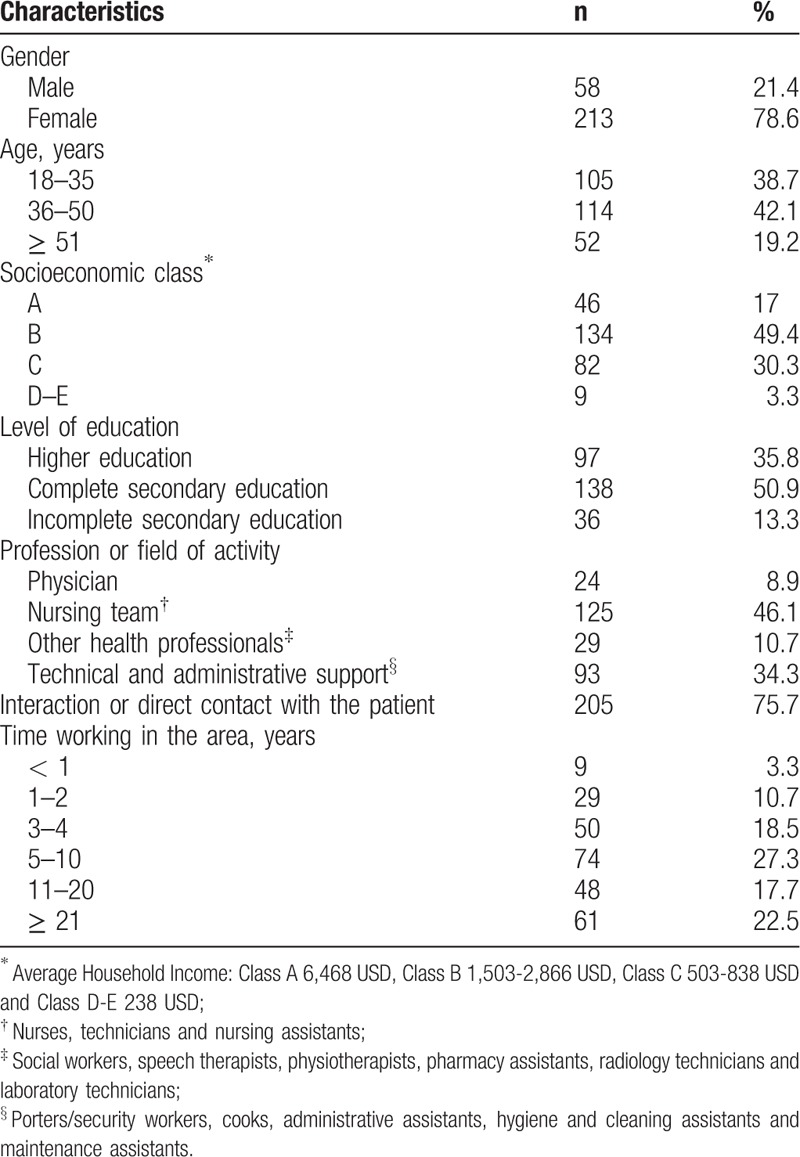
Around 271 professionals were included in our study (response rate = 88.9%; Fig. 1). The predominant characteristics were the following: women (n = 213; 78.6%), aged 36–50 years old (n = 114; 42.1%), from the nursing staff (n = 125; 46.1%) with 5–10 years of experience in this field (n = 74; 27.3%) (Table 1).
Figure 1.

Composition of the study sample.
Table 1.
Sociodemographic and labor characteristics of study professionals, n = 271.
3.2. Job satisfaction
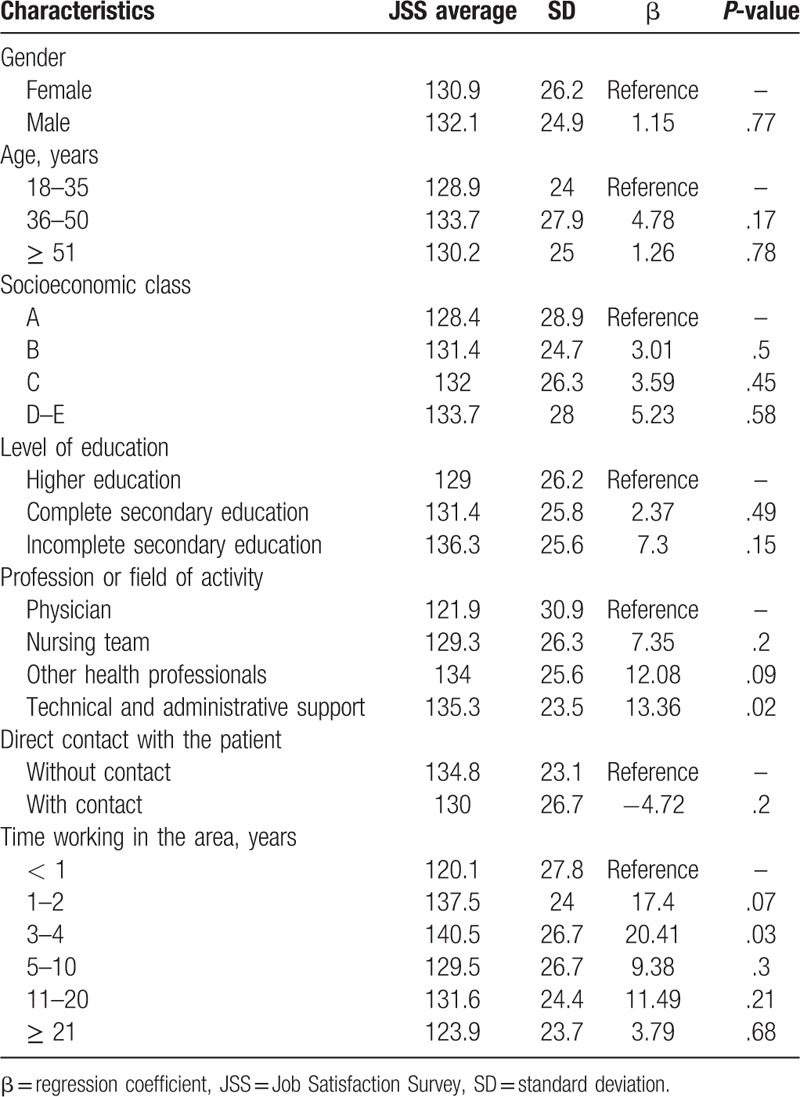
The type of job and time of professional activity were significantly associated with job satisfaction (Table 2). This relationship demonstrated that administrative or technical support workers expressed more satisfaction in their jobs compared to physicians (P = .02). Additionally, workers with 3–4 years of experience presented higher job satisfaction levels compared to those who had less than a year of professional activity (P = .03).
Table 2.
Analysis of the association of sociodemographic and labor variables with job satisfaction.
3.3. Burnout syndrome
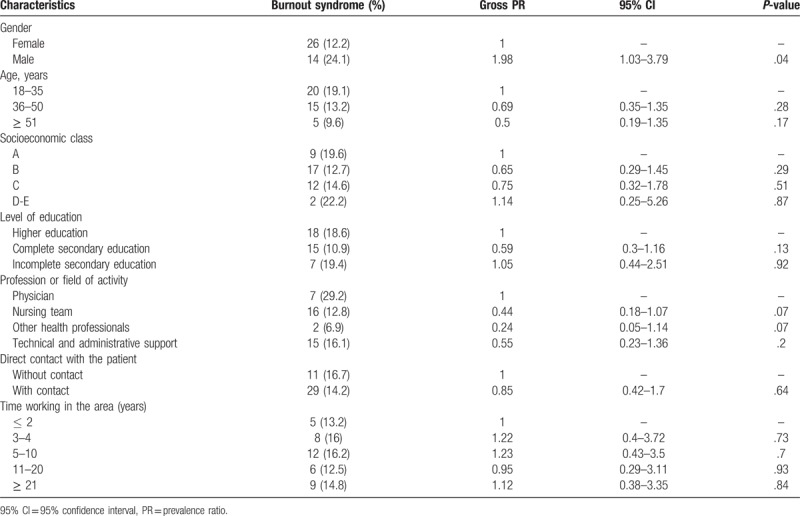
Correlation of sociodemographic and employment data with manifestation of burnout syndrome is shown in detail in Table 3. Men expressed exhaustion about twice as often as women (PR = 1.98; 95% CI: 1.03–3.79; P = .04).
Table 3.
Analysis of the association of sociodemographic and occupational variables with burnout syndrome.
3.4. Depressive symptoms
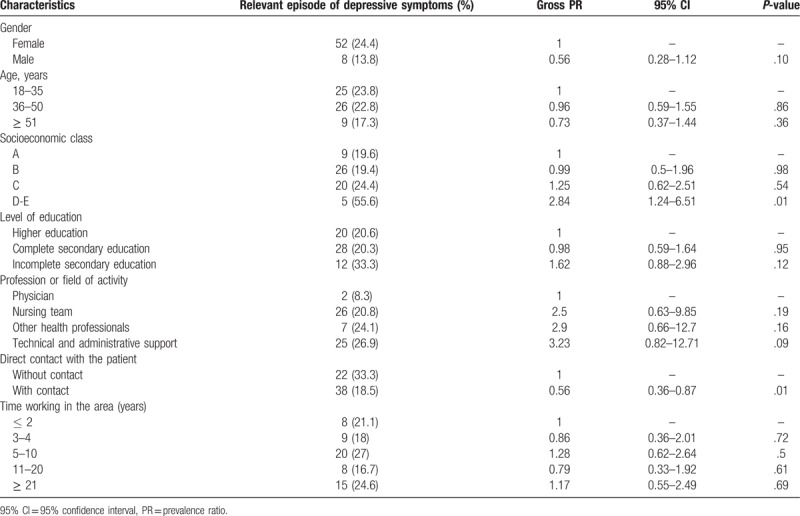
Table 4 shows the prevalence of relevant episodes of depressive symptoms divided by the individuals’ characteristics. Workers who belong to a lower socioeconomic class presented twice as many relevant episodes of depressive symptoms compared to those in upper socioeconomic classes (PR = 2.84; 95% CI: 1.24–6.51; P = .01). Contact with hospital patients was a protective factor against relevant episodes of depressive symptoms (PR = 0.56; 95% CI: 0.36–0.87; P = .01).
Table 4.
Analysis of the association of sociodemographic and labor variables with relevant episodes of depressive symptoms.
3.5. PLS-SEM (first step): validation and reliability of measurements
We verified convergent validity in the constructs in the first step of the PLS-SEM. AVE was lower than the value specified for the job satisfaction aspect (AVE = 0.41); yet, its reliability was certified (CR = 0.86, α = 0.82). The construct concerning depressive symptoms showed similar results (AVE = 0.45, CR = 0.88, α = 0.84). The burnout construct confirmed a convergent validity (AVE = 0.62) as well as reliability (CR = 0.63, α = 0.69).
Square roots of the AVE of constructs (job satisfaction = 0.64; burnout = 0.79; depressive symptoms = 0.67) were higher than correlation values between constructs (job satisfaction > burnout = 0.38; job satisfaction > depressive symptoms = 0.18; burnout > depressive symptoms = 0.38), and they also confirmed the discriminant validity of the measurements.
The factorial loads of the domains of instruments that composed the constructs varied between 0.48 (operating procedures) and 0.78 (contingent rewards) for job satisfaction, −0.66 (personal accomplishment) and 0.89 (emotional exhaustion) for burnout, and 0.36 (item 9 of the PHQ) and 0.8 (item 2 of the PHQ) for depressive symptoms (Addendum Table 5).
3.6. PLS-SEM (second step): analysis of structural model
Structural model analysis of the relationship between the aspects job satisfaction and burnout was confirmed by the following tests: coefficient of determination of large effect (R2 = 0.38), adequate predictive relevance (Q2 = 0.15), large effect size (f2 = 0.46), and acceptable quality of adjustment (GoF = 0.42). On the relationship between the job satisfaction constructs and depressive symptoms, an medium effect determination coefficient (R2 = 0.19), a considerable predictive significance (Q2 = 0.08), a large effect size (f2 = 0.43) and inadequate quality of fit (GoF = 0.29) were found. To relate burnout constructs and depressive symptoms, a large effect coefficient (R2 = 0.38), a plausible predictive relevance (Q2 = 0.23), a large effect size (f2 = 0.5) and a suitable quality of fit (GoF = 0.43) were found.
The graphical representation of the complete set of this association, illustrated by the path diagram in Figure 2, determined a causal relationship in which the absence of burnout was a predictor of job satisfaction (path coefficient = −0.57; P <.001), as well as depressive symptoms were a predictor for burnout (path coefficient = 0.61; P <.001). The association between the constructs depressive symptoms and job satisfaction was not statistically significant (path coefficient = −0.08; P = .18).
Figure 2.
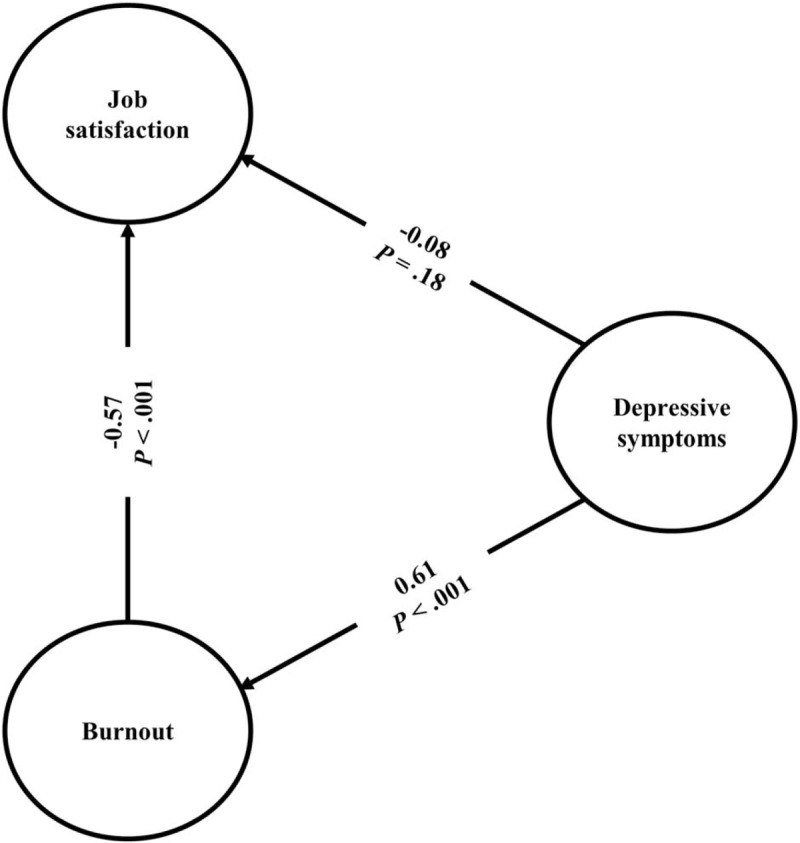
Pathways diagram of the relationship between job satisfaction, burnout, and depressive symptoms.
4. Discussion
4.1. Key results and implications for the practice
Our data indicate that job satisfaction was higher in administrative professionals or technical support workers and in those with 3 to 4 years of experience in the position. Men presented more exhaustion than women did. Workers with a lower income reported more depressive symptoms than ones with a higher income, and having contact with patients was a protective factor for the manifestation of these episodes.
The PLS-SEM made it possible to understand the behavior of the association between work satisfaction, burnout and depressive symptoms. A causal relationship was established and the absence of burnout revealed itself as a predictive factor for job satisfaction. In addition, depressive symptoms proved to be a predictor for the development of burnout.
Among the studies conducted in Latin America about the consequences of the psychosocial work environment and regarding burnout, the context of health care systems or the professionals of this field are the population that receive more focus in studies and one of the most researched areas.[31] A systematic review that evaluated the burnout syndrome in Latin American countries found that of the 89 studies reviewed (from 2000 to 2010), 15 (18%) were conducted in Brazil.[31] It is important to conduct researches that not only aim at addressing the measurement instruments of professional exhaustion, in addition to the adaptation or validation of these tools, but also aim at analyzing the actual impact of this clinical condition in the quality of life of the individual affected and the particularities associated with it.[31] A study conducted in Spain and in Latin America with health professionals (n = 11,530) showed that emotional exhaustion and satisfaction levels of participants at work are associated with the thought of quitting the profession.[32]
Currently, according to the assessment carried out by the World Health Organization (WHO),[33] there is a shortage of 7.2 million skilled professionals in health care and projections show that this global deficit can reach the total of 12.9 million in 2035. On the other hand, the demand for medical care and the emerging public health challenges are factors that are intensifying, the estimates indicate an increase of 1.9 billion people that will seek health care services until 2035.[33] Despite the fact that some countries obtain advanced resources, others still do not address this situation as a priority and the WHO stresses the need for the creation of policies regarding improvement of the work environment and the quality of the health workforce, as well as the influence of these factors on patient care.[33] Therefore, our study presents data to assist health care managers and the decision-making process, especially in Brazil.
4.2. Association with previous studies: connection between sociodemographic and occupational variables with job satisfaction, burnout, and depression
An investigation carried out with healthcare workers demonstrated the opposite relationship between the time of activity and satisfaction at work.[34] Therefore, it is proposed that the longer the time of work, the lower the satisfaction with professional activities.[34] Similar results were found in the present study and, although workers with <1 year of activity had a low satisfaction score, those with 5 or more years of work reported a decrease of well-being in the profession compared to professionals with 3 and 4 years of experience.
Efforts from healthcare system managers are necessary to provide improvements in the work environment, as well as to address the demands that emerge over time. Therefore, it will be possible to determine an appropriate career management that will prevent healthcare professionals from becoming unsatisfied and ultimately leave their profession or from maintaining an unnecessary and constant change of jobs.[35]
Health professionals experience exhaustive workflows and negative factors ranging from low wages to lack of institutional support.[1,8,9,36] This situation raises the immorality of the exhaustion of these individuals.[1,8,9,36]
Regarding the sociodemographic characteristics associated with burnout, other studies relate the condition mainly to gender, age, marital status, and educational level.[11] A systematic review that evaluated 47 different articles, conducted with the objective of determining the main factors correlated with exhausted medical workers, identified the female gender as a predictive aspect of burnout.[37]
On the other hand, a multi-center study in Switzerland related an attenuated burnout risk in a work group with a higher proportion of female nurses and showed that men, nursing assistants and those under 40 years old were more likely to develop the syndrome.[38] This result resembles what we found in this study, and both stand out, as they show a different risk profile of the event than most of the research published, as well as bring new perspectives. Thus, it is essential to implement prevention strategies in the population that presents the key conditions.[37]
Among the characteristics of people who presented depression symptoms, an investigation done in Brazil with doctors, nurses, nursing assistants, and community healthcare workers, found that of the 469 participants with major depression, the majority (n = 286; 61% ) had low monthly income, when compared to other workers.[39] Data that reinforces the current research, which identified more chances to manifest depressive symptoms in individuals with lower average household incomes.
Meta-analysis that examined 26 studies conducted in several countries (mostly in the USA, n = 15) elaborated on the significant relationship between income inequality and the risk of depression.[40] The same situation relates to the relevance of programs that support equitable income distribution in order to protect the mental health of the population.[40]
According to a research that analyzed the characteristics of suicides in Australia (2001–2012), the rate of female healthcare workers affected was higher than those who worked in other jobs (P <.001).[41] It is necessary for policy makers to examine this data and to organize strategies for this population to be assisted, as well as to promote the viability of these services.[39]
4.3. Correlation between job satisfaction, burnout syndrome, and depression
An investigation carried out in 2 Brazilian pediatric hospitals with a nursing team (n = 267) evaluated the correlation of the results obtained between the emotional exhaustion domain of MBI and work satisfaction.[42] The study indicated significant relations and established that the lower the level of emotional exhaustion, the higher the job satisfaction.[42] In Norway, a study with nurses and physicians working in intensive care units (ICUs) also showed the relation of emotional exhaustion to job satisfaction (r = −0.4; P < .001).[43] These results are similar to those presented in the current study and our research contributes with more evidence, since it determines the correlation of burnout syndrome (EE junction, DE, lPA) to job satisfaction.
An evaluation conducted with Chinese emergency physicians, with the objective of measuring psychological, burnout, and job satisfaction levels among these workers, also presented similar data to our study.[44] In the analysis of correlation, the research shows a possible weak relation between depression and job satisfaction, although not statistically significant as the relation between job satisfaction with the dimensions of emotional exhaustion and depersonalization of burnout syndrome (P < .05).[44]
In the literature, there is a discussion about the relationship between depression and burnout, which considers whether they are distinct adverse states or if they are symptoms of continuity of the same clinical picture.[45–47] The present study expands the analysis of these hypotheses and suggests depressive symptoms as a predictive factor for the development of burnout syndrome.
An investigation with medical professionals has determined that insomnia and depression are aspects that influence burnout.[48] Another research, carried out with ICU nurses, showed that the higher the level of emotional exhaustion and depersonalization, and the lower the personal achievement, the greater the manifestation of depressive symptomatology.[49]
4.4. Limitations and strength of the study
This study used a cross-sectional method, which does not detect incidences since it does not perform a follow-up period. Therefore, the evaluation of the exposure and outcome occurs in a single moment, which makes it difficult to determine a temporal relationship between them. Nevertheless, this method is important for its usefulness in measuring predominances and in the planning of healthcare policies. The results of this study also represent a local and singular analysis. In addition, we based this research on answers reported from the perspective of the participants, although they may vary according to individual criteria, it represents the understanding of the real scenario and perception of the professionals, in contrast with an external analysis.
One distinguishing scientific evidence of this study is the detail and focus on the different areas and professional categories present in a hospital. It encompassed a multidisciplinary team, since we understand that all of these workers contribute directly or indirectly to the provision of healthcare. We achieved a high participation rate in the survey, as shown by the high overall response rate to the instruments (88.9%). We believe that the method of data collection adopted, along with the instruments in the electronic device and the presence of the researcher to clarify any questions, was able to provide convenience and autonomy for the participants. In other studies using the same instruments, participation ranged from 50% to 81%.[43,50–54]
Our study supports the WHO line of research regarding human factors, organizational aspects, and individual particularities that affect work performance.[55] We suggest that the results of this research contribute to raise the attention of managers over current alarming problems, which affect the workers, in these institutions.
We also recommend the development of new studies that evaluate other aspects (personal and organizational) that could affect the quality of life of healthcare workers, as well as the resulting outcomes in patient care, in order to avoid an epidemic of work-related diseases and, consequently, adverse events in patients.
5. Conclusion
It is possible to relate the type of profession and the time in the position, to job satisfaction of hospital workers. The gender of the participants is associated with burnout. Average household income and patient contact are associated with depressive symptoms.
Furthermore, the absence of burnout syndrome was a predictive aspect for the development of job satisfaction, according to the correlation analysis between the 3 aforementioned factors. Depressive symptoms proved to be a predictor of professional exhaustion.
These results are important notions for policy makers and raise pertinent hypotheses for future studies. Investments made to support programs for the management of psychosocial demands, associated with this population, can avoid an epidemic of work-related diseases.
Acknowledgments
We thank the hospital workers, participants of the research, who voluntarily consented and contributed to the conception of this scientific research. We would also like to thank the Academic Publishing Advisory Center (Centro de Assessoria de Publicação Acadêmica, CAPA—www.capa.ufpr.br) of the Federal University of Paraná for assistance with English language editing.
Author contributions
Conceptualization: Alan Maicon de Oliveira, Marcus Tolentino Silva, Taís Freire Galvão.
Data curation: Alan Maicon de Oliveira, Marcus Tolentino Silva, Luciane Lopes.
Formal analysis: Alan Maicon de Oliveira, Marcus Tolentino Silva.
Funding acquisition: Alan Maicon de Oliveira.
Investigation: Alan Maicon de Oliveira.
Methodology: Taís Freire Galvão, Luciane Cruz Lopes.
Project administration: Marcus Tolentino Silva, Luciane Cruz Lopes.
Resources: Alan Maicon de Oliveira, Marcus Tolentino Silva.
Software: Marcus Tolentino Silva.
Supervision: Marcus Tolentino Silva, Luciane Cruz Lopes.
Validation: Alan Maicon de Oliveira.
Visualization: Alan Maicon de Oliveira.
Writing – original draft: Alan Maicon de Oliveira.
Writing – review & editing: Marcus Tolentino Silva, Taís Freire Galvão, Luciane Cruz Lopes.
Alan Maicon de Oliveira: 0000-0002-3880-0287.
Alan Maicon de Oliveira orcid: 0000-0002-3880-0287.
Supplementary Material
Footnotes
Abbreviations: 95% CI = 95% confidence interval, AVE = average variance extracted, BRL = Brazilian real, CR = composite reliability, DE = depersonalization, EE = emotional exhaustion, GoF = goodness-of-fit, ICU = intensive care unit, JSS = Job Satisfaction Survey, lPA = low personal accomplishment, MBI–HSS = Maslach Burnout Inventory–Human Services Survey, PHQ-9 = Patient Health Questionnaire-9, PLS-SEM = partial least squares structural equation modeling, PR = prevalence ratio, SD = standard deviation, USA = United States of America, USD = United States dollars, WHO = World Health Organization.
The authors would like to thank the financial support (scholarship) of the National Council for Scientific and Technological Development of Brazil (process number: 130828/2016-5).
The authors have no conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
The authors of this work have nothing to disclose.
References
- [1].van Mol MMC, Kompanje EJO, Benoit DD, et al. The prevalence of compassion fatigue and burnout among healthcare professionals in intensive care units: a systematic review. PLoS One 2015;10:e0136955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ 2008;336:488–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Ullström S, Andreen Sachs M, Hansson J, et al. Suffering in silence: a qualitative study of second victims of adverse events. BMJ Qual Saf 2014;23:325–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Gazoni FM, Amato PE, Malik ZM, et al. The impact of perioperative catastrophes on anesthesiologists: results of a National Survey. Anesth Analg 2012;114:596–603. [DOI] [PubMed] [Google Scholar]
- [5].Editorial Suicide among health-care workers: time to act. Lancet 2017;389:2. [DOI] [PubMed] [Google Scholar]
- [6].Spiliopoulos K, Gansera L, Weiland HC, et al. Chronic stress and coping among cardiac surgeons: a single center study. Rev Bras Cir Cardiovasc 2014;29:308–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Currie EJ, Carr Hill RA. What are the reasons for high turnover in nursing? A discussion of presumed causal factors and remedies. Int J Nurs Stud 2012;49:1180–9. [DOI] [PubMed] [Google Scholar]
- [8].de Oliveira Vasconcelos Filho P, de Souza MR, Elias PEM, et al. Physicians’ job satisfaction and motivation in a public academic hospital. Hum Resour Health 2016;14:75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Teles MAB, Barbosa MR, Vargas AMD, et al. Psychosocial work conditions and quality of life among primary health care employees: a cross sectional study. Health Qual Life Outcomes 2014;12:72–172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry 2016;15:103–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Chuang CH, Tseng PC, Lin CY, et al. Burnout in the intensive care unit professionals: a systematic review. Medicine 2016;95:e5629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders DSM-5. Arlington: American Psychiatric Publishing; 2013. [Google Scholar]
- [13].Bonde JPE. Psychosocial factors at work and risk of depression: a systematic review of the epidemiological evidence. Occup Environ Med 2008;65:438–45. [DOI] [PubMed] [Google Scholar]
- [14].Nieuwenhuijsen K, Bruinvels D, Frings-Dresen M. Psychosocial work environment and stress-related disorders, a systematic review. Occup Med 2010;60:277–86. [DOI] [PubMed] [Google Scholar]
- [15].Brazilian Market Research Association. Brazilian Criteria 2015 and social class distribution update for 2016. ABEP; 2016: Available at: http://www.abep.org/Servicos/Download.aspx?id=13 Accessed July, 2016. [Google Scholar]
- [16].Souza ACD, Milani D, Alexandre NMC. Adaptação cultural de um instrumento para avaliar a satisfação no trabalho. Rev Bras Saúde Ocup 2015;40:219–27. [Google Scholar]
- [17].Spector PE. Measurement of human service staff satisfaction: Development of the Job Satisfaction Survey. Am J Community Psychol 1985;13:693–713. [DOI] [PubMed] [Google Scholar]
- [18].van Saane N, Sluiter JK, Verbeek JHAM, et al. Reliability and validity of instruments measuring job satisfaction—a systematic review. Occup Med 2003;53:191–200. [DOI] [PubMed] [Google Scholar]
- [19].Likert R. A technique for the measurement of attitudes. Arch Psychol 1932;140:1–55. [Google Scholar]
- [20].Maslach C, Jackson SE. The measurement of experienced burnout. J Organ Behav 1981;2:99–113. [Google Scholar]
- [21].Benevides-Pereira AMT. MBI-Maslach Burnout Inventory e suas adaptações para o Brasil. Anais XXXII Reunião Anual Psicol 2001;1:84–5. [Google Scholar]
- [22].Schaufeli WB, Leiter MP, Maslach C. Burnout: 35 years of research and practice. Career Devel Int 2009;14:204–20. [Google Scholar]
- [23].Carlotto MS, Câmara SG. Propriedades psicométricas do Maslach Burnout Inventory em uma amostra multifuncional. Estudos Psicol 2007;24:325–32. [Google Scholar]
- [24].Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Int Med 2001;16:606–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Santos IS, Tavares BF, Munhoz TN, et al. Sensibilidade e especificidade do Patient Health Questionnaire-9 (PHQ-9) entre adultos da população geral. Cadernos Saúde Pública 2013;29:1533–43. [DOI] [PubMed] [Google Scholar]
- [26].Dean AG, Sullivan KM, Soe MM. OpenEpi: Open Source Epidemiologic Statistics for Public Health. OpenEpi; 2013: Available at: http://www.openepi.com Accessed: May 2016. [Google Scholar]
- [27].Hair JF, Hult GTM, Ringle CM, et al. A Primer on Partial Least Squares Structural Equation Modelling (PLS-SEM). Los Angeles, CA: SAGE Publications; 2014. [Google Scholar]
- [28].Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Marketing Res 1981;18:39–50. [Google Scholar]
- [29].Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York, NY: Psychology Press; 1988. [Google Scholar]
- [30].Wetzels M, Odekerken-Schröder G, Van Oppen C. Using PLS path modeling for assessing hierarchical construct models: Guidelines and empirical illustration. MIS Quart 2009;33:177–95. [Google Scholar]
- [31].Bambula FD, Gómez IC. Research on burnout from 2000 to 2010 in Latin America. Psicol Desde Caribe 2016;33:113–31. [Google Scholar]
- [32].Suñer-Soler R, Grau-Martín A, Flichtentrei D, et al. The consequences of burnout syndrome among healthcare professionals in Spain and Spanish speaking Latin American countries. Burnout Res 2014;1:82–9. [Google Scholar]
- [33].Campbell J, Dussault G, Buchan J, et al. A Universal Truth: No Health without a Workforce. Forum Report, Third Global Forum on Human Resources for Health, Recife, Brazil. Geneva: Global Health Workforce Alliance and World Health Organization; 2013. [Google Scholar]
- [34].Shahnazi H, Daniali SS, Sharifirad G. Job satisfaction survey among health centers staff. J Educ Health Promot 2014;3:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Jackson TN, Pearcy CP, Khorgami Z, et al. The physician attrition crisis: a cross-sectional survey of the risk factors for reduced job satisfaction among US surgeons. World J Surg 2018;42:1285–92. [DOI] [PubMed] [Google Scholar]
- [36].Lu H, Barriball KL, Zhang X, et al. Job satisfaction among hospital nurses revisited: a systematic review. Int J Nurs Stud 2012;49:1017–38. [DOI] [PubMed] [Google Scholar]
- [37].Amoafo E, Hanbali N, Patel A, et al. What are the significant factors associated with burnout in doctors? Occup Med 2015;65:117–21. [DOI] [PubMed] [Google Scholar]
- [38].Merlani P, Verdon M, Businger A, et al. Burnout in ICU caregivers: a multicenter study of factors associated to centers. Am J Respir Crit Care Med 2011;184:1140–6. [DOI] [PubMed] [Google Scholar]
- [39].da Silva ATC, Peres MFT, Lopes CdS, et al. Violence at work and depressive symptoms in primary health care teams: a cross-sectional study in Brazil. Soc Psychiatry Psychiatr Epidemiol 2015;50:1347–55. [DOI] [PubMed] [Google Scholar]
- [40].Patel V, Burns JK, Dhingra M, et al. Income inequality and depression: a systematic review and meta-analysis of the association and a scoping review of mechanisms. World Psychiatry 2018;17:76–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Milner AJ, Maheen H, Bismark MM, et al. Suicide by health professionals: a retrospective mortality study in Australia, 2001–2012. Med J Aust 2016;205:260–5. [DOI] [PubMed] [Google Scholar]
- [42].Alves DFS, Guirardello EB. Safety climate, emotional exhaustion and job satisfaction among Brazilian paediatric professional nurses. Int Nurs Rev 2016;63:328–35. [DOI] [PubMed] [Google Scholar]
- [43].Myhren H, Ekeberg Ø, Stokland O. Job satisfaction and burnout among intensive care unit nurses and physicians. Crit Care Res Pract 2013;2013:786176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Xiao Y, Wang J, Chen S, et al. Psychological distress, burnout level and job satisfaction in emergency medicine: A cross-sectional study of physicians in China. Emerg Med Australas 2014;26:538–42. [DOI] [PubMed] [Google Scholar]
- [45].Schonfeld IS, Bianchi R. Burnout and depression: two entities or one? J Clin Psychol 2016;72:22–37. [DOI] [PubMed] [Google Scholar]
- [46].Bianchi R, Schonfeld IS, Laurent E. Is burnout separable from depression in cluster analysis? A longitudinal study. Soc Psychiatry Psychiatr Epidemiol 2015;50:1005–11. [DOI] [PubMed] [Google Scholar]
- [47].Bianchi R, Boffy C, Hingray C, et al. Comparative symptomatology of burnout and depression. J Health Psychol 2013;18:782–7. [DOI] [PubMed] [Google Scholar]
- [48].Iorga M, Socolov V, Muraru D, et al. Factors influencing burnout syndrome in obstetrics and gynecology physicians. BioMed Res Int 2017;2017:9318534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [49].Vasconcelos EMd, Martino MMFD, França SPdS. Burnout and depressive symptoms in intensive care nurses: relationship analysis. Rev Bras Enferm 2018;71:135–41. [DOI] [PubMed] [Google Scholar]
- [50].Pereira I, Veloso A, Silva IS, et al. Compromisso organizacional e satisfação laboral: um estudo exploratório em unidades de saúde familiar portuguesas. Cadernos Saúde Pública 2017;33: e00153914. [DOI] [PubMed] [Google Scholar]
- [51].Ai-Hong C, Saidah Nafisah J, Abdul Rahim MN. Comparison of job satisfaction among eight health care professions in private (non-government) settings. Malays J Med Sci 2012;19:19–26. [PMC free article] [PubMed] [Google Scholar]
- [52].Mijakoski D, Karadzinska-Bislimovska J, Basarovska V, et al. Burnout and work demands predict reduced job satisfaction in health professionals working in a surgery clinic. Open Access Maced J Med Sci 2015;3:166–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [53].Chou Y-C, Kröger T, Lee Y-C. Predictors of job satisfaction among staff in residential settings for persons with intellectual disabilities: a comparison between three residential models. J Appl Res Intellect Disab 2010;23:279–89. [Google Scholar]
- [54].Teixeira C, Ribeiro O, Fonseca AM, et al. Burnout in intensive care units—a consideration of the possible prevalence and frequency of new risk factors: a descriptive correlational multicentre study. BMC Anesthesiol 2013;13:38–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Group of WHO Patient Safety, World Health Organization Human Factors in Patient Safety: Review of Topics and Tools. 2009. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.