

Supplemental Digital Content is available in the text
Keywords: high-intensity laser therapy, musculoskeletal disorder, pain, systematic review meta-analysis
Abstract
Background:
Although high-intensity laser therapy (HILT) has been used for the management of musculoskeletal disorders (MSD), studies examining the effectiveness of HILT have been limited. We investigated the effectiveness of HILT in MSD using a systematic review and meta-analysis.
Methods:
We searched the ovid MEDLINE, ovid Embase, Cochrane CENTRAL library, and Web of Science until January, 2018. Relevant studies concerning the effectiveness of HILT in patients with MSD were included. Both placebo and active controls were considered as comparators and only randomized controlled trial (RCT) design studies were included. Risk of bias (ROB) was used for the quality assessment of the RCT. For continuous variables, a meta-analysis was conducted using an inverse variance random effects model. The mean difference (MD) for visual analog scale pain and standardized mean difference (SMD) for disability were applied.
Results:
Twelve studies were selected for this systematic review. In 11 studies, comprising 736 patients, pain was significantly improved by HILT compared with a control group (MD: −1.01; 95% confidence interval [CI]: −1.28 to −0.74). From the analysis of 688 patients from 10 studies, the pooled standardized mean difference (SMD) of HILT showed a significant improvement in disability scores compared with those in the control group (SMD, −1.09; 95% CI −1.77, −0.41). In subgroup analysis by treatment regions, the mean difference (MD) in neck pain was the highest at −1.02 (95% CI: −1.45, −0.58) than in controls, followed by back pain (MD, −0.91; 95% CI: −1.24, −0.59).
Conclusions:
The results of this study show that HILT treatment for back and neck pain significantly improved pain and disability scores compared with controls. The ROB of the included studies was moderate; however, significant heterogeneity existed. Thus, additional well-designed studies involving larger samples with long-term follow-up are needed to further assess each laser application, treatment region, and comparator.
1. Introduction
Musculoskeletal disorders (MSD) comprise the most common conditions worldwide. One in 2 people have a MSD in the United States and the estimated number of individuals affected reached about 126.6 million in 2012.[1] In particular, individuals with back and neck pain total approximately 75.7 million.[2] The cost of MSD was estimated to be approximately $213 billion in 2011, which is 1.4% of the gross domestic product (GDP) in the United States.[2,3]
MSD derives from a soft-tissue injury or pain in the musculoskeletal system including muscles, nerves, tendons, joints, and cartilage in the upper and lower limb, neck, and lower back.[4,5] Various causes of MSD pain can be attributed to result from damage of muscle tissue, trauma, postural strain, repetitive movements, overuse, and prolonged immobilization.[6] The main purpose of MSD treatment is to improve pain and physical disabilities.[7] Treatment for MSD pain includes nonsteroidal anti-inflammatory drugs (NSAID), analgesics, corticosteroid injections, as well as acupuncture or acupressure. In addition, self-management and education, exercise, manual therapy, and psychosocial therapy have also been considered nonpharmacological treatments.[8] Recently, laser therapy including low-level laser therapy (LLLT) and high-intensity laser therapy (HILT) have been used for the management of MSD. Laser therapy is a noninvasive treatment having a low incidence of adverse effects.[9]
In a systematic review, LLLT applied for pain treatment in MSD showed significant differences compared to control groups.[10] HILT can stimulate joints more deeply and treat a wider area than LLLT,[11] thus, the application of HILT for MSD may improve pain and function when compared to LLLT. However, studies regarding the effectiveness for HILT have been limited. Thus, it is necessary to investigate the effectiveness of HILT in MSD patients. The aim of the present study was to perform a systematic review and meta-analysis regarding the effectiveness of HILT in treatment of MSD.
2. Methods
2.1. Literature search
We searched the core databases including ovid MEDLINE, ovid Embase, the Cochrane CENTRAL library, and Web of Science up to January 17, 2018. The MeSH terms and text words included in the search strategy are shown in Supplementary Table 1. To maximize the sensitivity of the included articles, an only intervention-related term was used for searching articles. The search terms included “high-intensity laser therapy” and “HILT.” In the Web of Science database, the term “pain” was also applied to the search strategy.
2.2. Study selection
We included studies conducted to examine the effectiveness of HILT in patients with MSD. Treatment regions for MSD included the back, neck, shoulder, arm, or hands. Placebo or active comparators such as ultrasound, brace, transcutaneous electrical nerve stimulation (TENS), transaction therapy, medical treatment bandage, or exercise were considered as comparators. The randomized controlled trial (RCT) design study was the only design included and studies written in both English and Korean were included. Two reviewers independently selected the studies based on the inclusion criteria. If disagreement occurred, a final decision for inclusion was confirmed by a third reviewer.
2.3. Quality assessment
The risk of bias (ROB) tool developed by Cochrane group was used for quality assessment.[12] We estimated 3 levels (low, unclear, and high) for 7 items including random sequence generation, allocation concealment, blinding of participants, blinding of outcome assessment, incomplete outcome data, selective reporting, and funding source. Two independent reviewers assessed the ROB and a consensus was reached with another reviewer in cases of inconsistency.
2.4. Data extraction
Items for data extraction were prespecified by the authors. Patient characteristics such as diagnosis, mean age, and standard deviation (SD), and percentage of males in the included studies were extracted. Interventions and sample size, evaluation time, and country conducting the study were also summarized. Pain and disability were extracted as outcome measures. For HILT application methods, the type of laser, wavelength, output power, energy density, application time, number of total sessions and sessions per week, application site, and the process of application were listed.
2.5. Statistical analysis
For continuous variables, a meta-analysis was conducted using an inverse variance random effects model. The mean difference (MD) for VAS pain and standardized mean difference (SMD) for disability were applied. VAS pain was reported using the same unit; however, disability measures were reported using diverse units due to the different instruments used. For 3 arm studies, splitting of the shared group was applied according to the Cochrane group guidelines.[12] For example, in studies examining HILT versus Placebo versus active comparator, the HILT group was included in both the HILT versus Placebo and HILT versus active comparator groups. Thus, the number of individuals in the HILT was divided, but the same mean and SD were applied in both groups. This method was applied for continuous outcomes. For disability, a higher score presented higher disability except for one study. Thus, the mean of the study with an opposite value was multiplied by −1 in order to align the direction.
The pooled estimate of the subgroup according to treatment region was analyzed. The placebo comparator was used in subgroup analysis by treatment region or follow-up period, if the study included a 3-arm intervention. The subgroup analysis according to comparators (placebo or active controls) was also estimated. Heterogeneity was assessed using forest plot visually and Higgins I2 with P-value. In order to identify publication biases, contour funnel plots were used. The Review Manager 5.3 program was used for all analysis.
3. Results
3.1. Literature search
From the initial literature search, 626 articles were identified and 225 articles were included for title or abstract screening after removing duplicates (Fig. 1). Following the full text review of 107 articles, 94 were excluded because the studies did not focus on HILT, no patients with MSD were included, no outcomes of interest were reported, the study design was ineligible, or papers were not original articles. Ultimately, 12 studies were included in this systematic review.[13–24]
Figure 1.
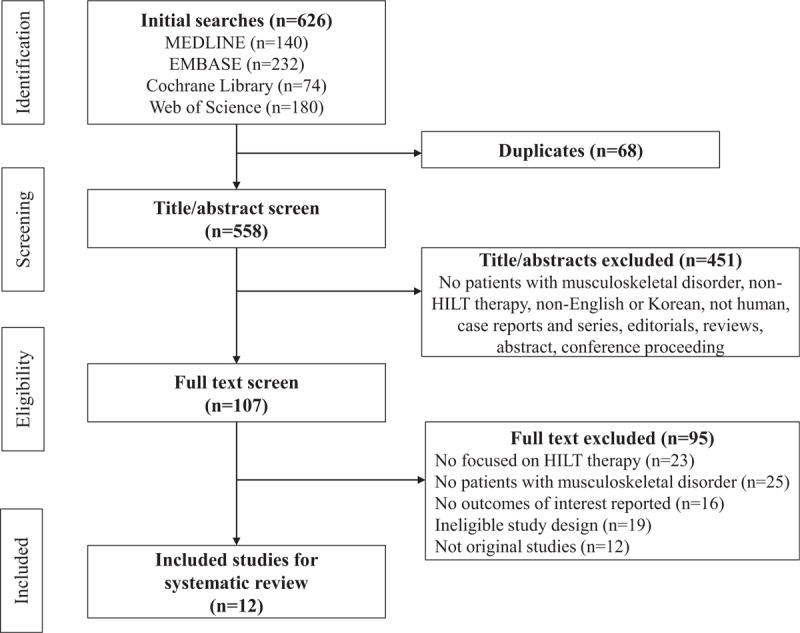
PRISMA flow diagram of study selections.
3.2. General characteristics of the included studies
The included studies consisted of patients having back, neck, shoulder, arm, and hand pain (Table 1 ). Comparators were varied and included placebo, exercise, ultrasound, transcutaneous electrical nerve stimulation (TENS), brace, transaction therapy, and bandages. The mean age of the subjects included in the studies ranged from 32 to 58 years old and the percentage of males ranged from 0% to 100%. Trials were conducted in Egypt, Saudi Arabia, Turkey, Italy, Poland, China, and South Korea.
Table 1.
Study characteristics of randomized controlled trials of high-intensity laser therapy in musculoskeletal disorders.
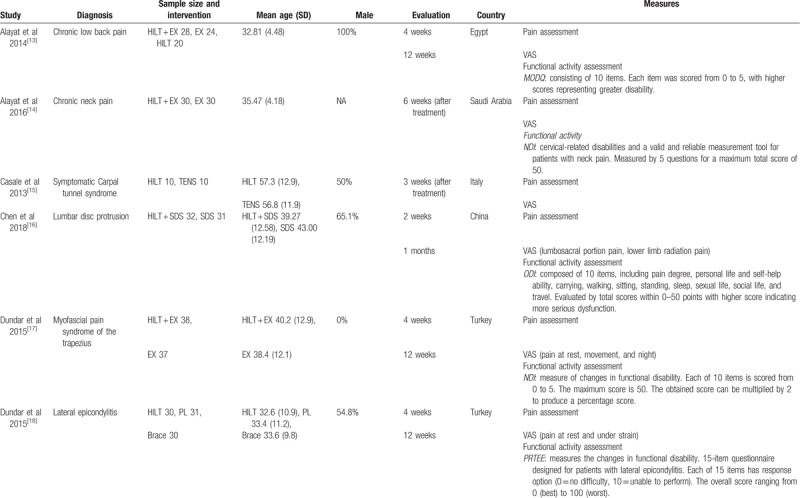
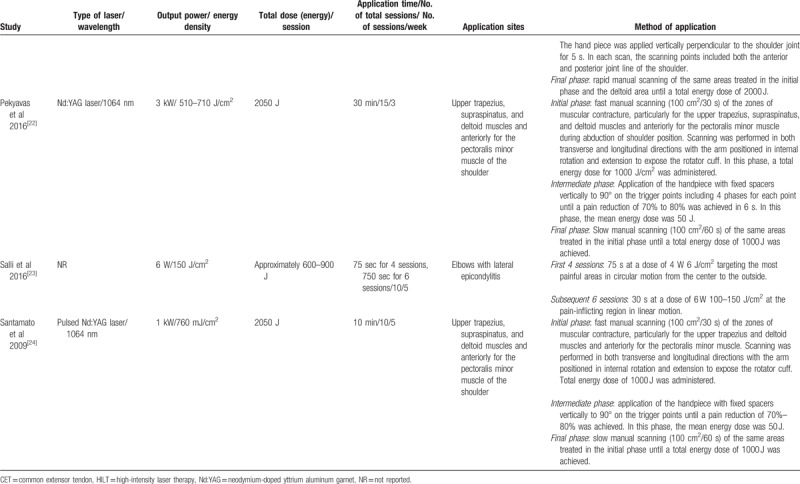
Pain was assessed using a visual analog scale (VAS). A 10-cm VAS was used to measure pain and possible scores ranged from 0 (no pain) to 10 (worst pain). Thus, higher VAS scores indicated higher pain. A functional activity assessment was used according to the treatment regions. For low-back pain, disability was measured as the Oswestry Disability Index (ODI) and the Neck Disability Index (NDI) was used for estimating neck disability. The Shoulder Pain and Disability Index (SPADI) and the Constant Murley Scale (CMS) for shoulder pain, and the Patient-related Tennis Elbow Evaluation (PRTEE), and the Disabilities of the Arm Shoulder and Hand questionnaire (DASH) for arm/hand pain were used as disability measures. The outcomes were evaluated after 2 weeks to 12 weeks of treatment. The characteristics used for HILT in the included studies are summarized in Table 2 .
Table 1 (Continued).
Study characteristics of randomized controlled trials of high-intensity laser therapy in musculoskeletal disorders.
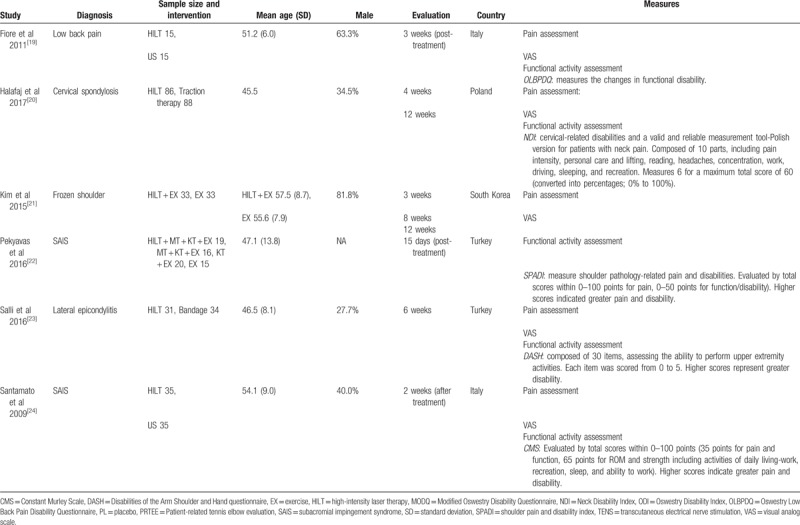
Table 2 (Continued).
Study protocols of randomized controlled trials for high-intensity laser therapy in musculoskeletal disorders.
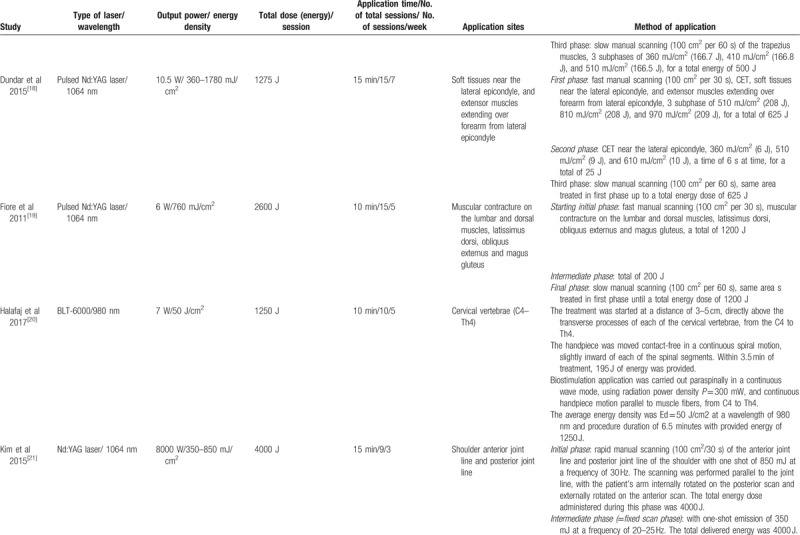
Table 2 (Continued).
Study protocols of randomized controlled trials for high-intensity laser therapy in musculoskeletal disorders.
3.3. Quality assessment
The results of quality assessment are presented in Fig. 2. In random sequence generation, selective reporting, and funding source, the percentage of low-quality studies was over 75% and also more than 50% indicated blinding of participants of outcome assessment, as well as incomplete outcome data. The percentage of low risk for allocation concealment was below 50% as for most of the included studies it was neither conducted nor reported.
Figure 2.
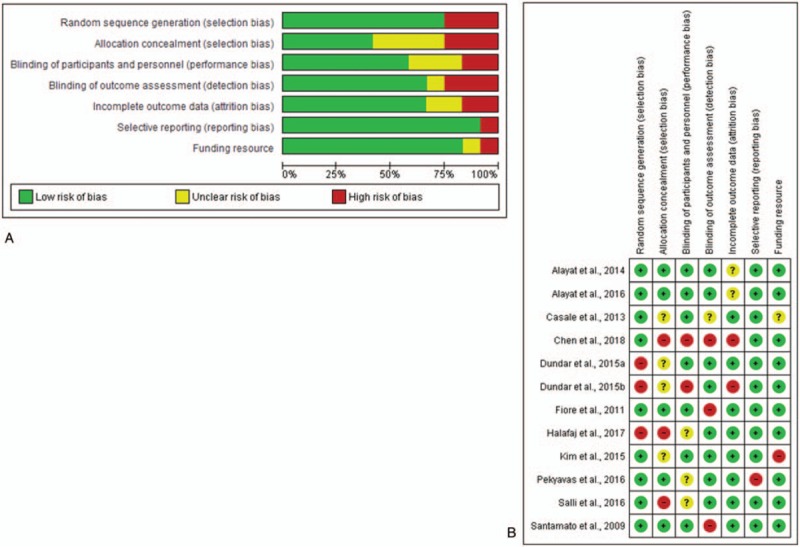
Quality assessment of included studies using risk of bias assessment (A) ROB graph and (B) ROB summary. +: low ROB; −: high ROB; ?: unclear ROB. ROB = risk of bias.
3.4. Pain
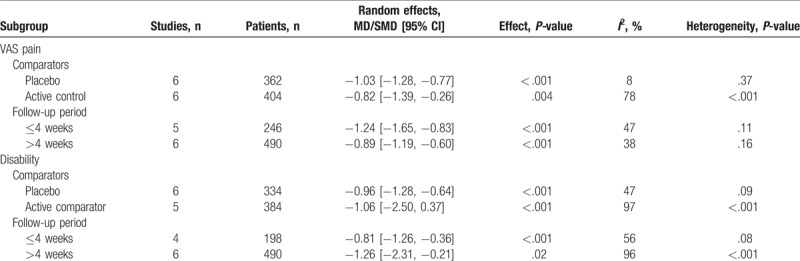
In 11 studies including 736 patients, HILT significantly improved pain compared to the control group (MD: −1.01; 95% CI: −1.28, −0.74) (Fig. 3). There was no apparent systematic bias in the contour funnel plot. Although an asymmetry was detected, the missing values were both in significant and non-significant areas (Fig. 4A). In subgroup analysis by treatment regions, the MDs for the neck were the highest at −1.02 (95% CI: −1.45, −0.58) compared to the control group, followed by the back (MD: −0.91; 95% CI −1.24, −0.59) and the arms/hands subgroups (MD: −0.82; 95% CI: −1.43, −0.21). There was no significant difference for the shoulder pain subgroup between the HILT and control groups. The heterogeneity in the neck and shoulder pain subgroups was significant (I2=73%; P = .02 for the neck and I2 = 88%, P = .004 in the shoulder subgroups); however, there was no significant heterogeneity in the back pain subgroup (I2 = 0%; P = .88) or the arm/hand subgroup (I2 = 0%; P = .42). In particular, the MD of HILT for pain was −1.03 (95% CI: −1.28, −0.77) and −0.82 (−1.39, −0.26) for the placebo and active control groups, respectively (Table 3). Heterogeneity was not significant compared to placebo (I2 = 8%; P = .37), while there was significant heterogeneity compared to the active control group (I2 = 78%; P < .001). According to the follow-up periods, the pooled pain effect did not show any significant differences.
Figure 3.
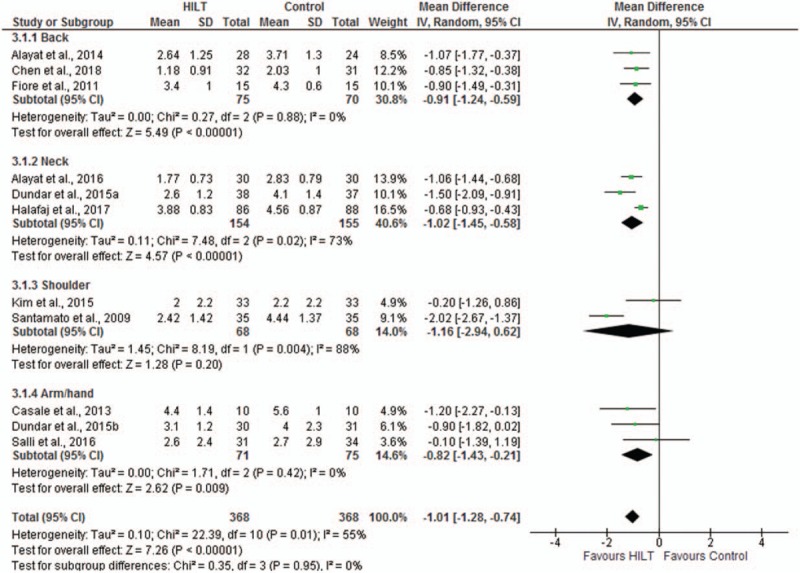
Mean difference in visual analog scale pain between high-intensity laser therapy and comparator.
Figure 4.

Contour funnel plot of included studies (A) pain (B) disability.
Table 2.
Study protocols of randomized controlled trials for high-intensity laser therapy in musculoskeletal disorders.
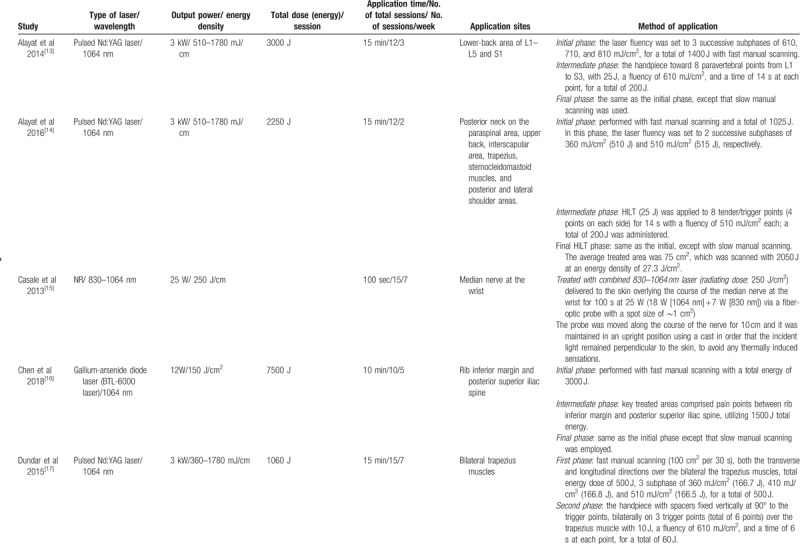
Table 3.
Subgroup analysis in pain and disability of high-intensity laser therapy versus control for musculoskeletal disorder.
3.5. Disabilities
A total of 688 patients from 10 studies indicated that the pooled SMD of HILT significantly improved disability compared with the control group (SMD: −1.09; 95% CI: −1.77, −0.41) (Fig. 5). We could not detect any obvious publication bias by the contour funnel plot despite asymmetry (Fig. 4B). Both significant and nonsignificant data were missing. In the subgroup analysis for each treatment region, a similar trend in SMD was observed in both the disability scores and pain scores; however, the SMD in the shoulder pain subgroup significantly improved and there was no significant difference in the arm/hand subgroup. The disability following HILT significantly improved compared to the placebo group (SMD: −0.96; 95% CI: −1.28, −0.64), however, there was no significant improvement between the HILT and the active control groups (SMD: −1.06; 95% CI: −2.50, 0.37) (Table 3). In comparison with the control group, there was no significant heterogeneity (I2 = 47%; P = .09), while a significant heterogeneity was observed in comparison with the active control group (I2 = 97%; P < .001). The SMD for disability stratified according to the follow-up period showed improvement with a longer follow-up period, however, the CIs overlapped.
Figure 5.
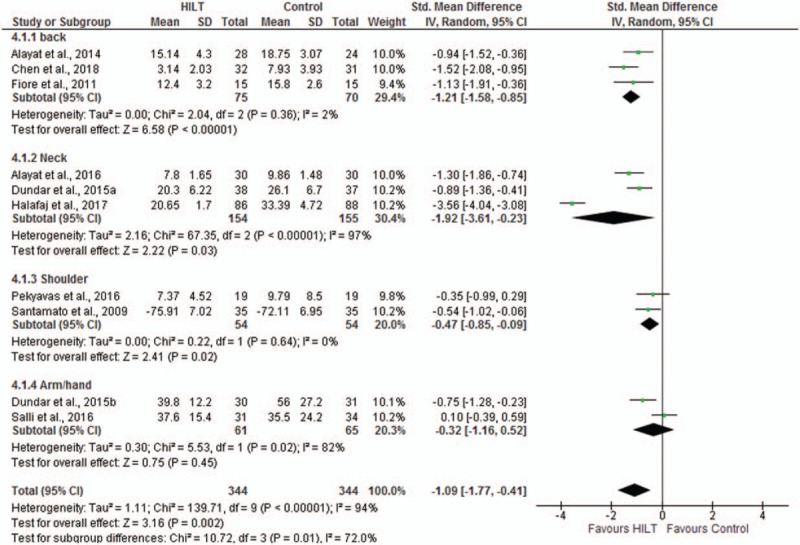
Standardized mean difference in disability measurement between high-intensity laser therapy and control.
4. Discussion
Application of HILT for pain and functional ability of MSD showed significant improvement compared to controls. The studies included in this meta-analysis generally had moderate ROB.
We were unable to find any previous reviews evaluating the effectiveness of HILT for the management of MSD, but a systematic review for LLLT in pain was available. The systematic review included 1462 patients with MSD from 8 studies.[10] The pain in the LLLT group significantly decreased compared to the control group following treatment (MD: −0.85; 95% CI: −1.22, −0.48), a result, which was similar to our study showing that pain in the HILT-exposed group significantly decreased compared to controls (MD: −1.01; 95% CI: −1.28, −0.74).
Huang et al[25] conducted a systematic review for LLLT application in chronic back pain. The weighted mean difference (WMD) of LLLT in pain was −13.57 (95% CI: −17.42, −9.72) compared to placebo and there was no significant difference in the disability score using the ODI (SMD: −0.38; 95% CI: −1.14, 0.39). In our study, exposure to HILT in patients with back pain resulted in a significant improvement in both pain and disability scores compared to the control groups (MD: −0.91; 95% CI: −1.24, −0.59 for pain and SMD: −1.21; 95% CI: −1.58, −0.85).
In the study by Chow et al., LLLT applied to patients with neck pain significantly improved pain and disability scores compared to placebo (WMD: 19.86; 95% CI: 10.04–29.68 for pain and SMD: 1.38; 95% CI: 0.39–2.37 for the disability score).[26] These results were similar to the results of our study. The pain and disability scores in the HILT group significantly improved compared to the control group (MD: −1.02; 95% CI: −1.45, −0.58 for pain and SMD: −1.92; 95% CI: −3.61, −0.23).
HILT has been known to reduce heat accumulation in tissues and to have photothermal and photochemical effects in deep tissues for limited periods.[11] These properties favor treatment of deep tissues and structures by increasing cell metabolism, vascular permeability, and blood flow.[13,24,27] The pain control effect achieved by HILT might be attributed to multiple mechanisms. In the central nervous system, the secretion of endogenous opioids such as β-endorphins is increased by laser therapy and these could centrally inhibit pain sensations.[28] In the peripheral nervous system, substance P sensitizes pain-transmitting neurons and leads to hyperalgesia; however, laser therapy has been reported to decrease the secretion of substance P by peripheral receptors.[14,29] Laser therapy might increase the latency and decrease the conduction velocity of sensory nerves by inhibiting Ae- and C-fiber transmission; these in turn may decrease the transmission of pain signals.[30] In tissues, laser therapy may also reduce the release of histamine and bradykinin in injured tissues and increase the pain threshold.[31,32] These multiple actions of laser therapy may represent the underlying mechanisms involved in the control the pain in MSD. In addition, a decrease in pain sensation has a significant effect on the increase of range of motion and the quality of life of the patient.[22] Thus, functional ability in patients with MSD could also be also improved.
The present study has several strengths. First, to the best of our knowledge, this study is the first systematic review examining the effectiveness of HILT for MSD. Thus, our results present the best available evidence for pain and disability recovery following HILT in patients with MSD including back, neck, shoulder, arm, and hand pain. Second, the ROB of the included studies was not high on quality assessment. Therefore, the results of this systematic review may be considered reliable because of the moderate quality of the included studies. Third, the effectiveness of HILT was present not only for MSD overall but also for different treatment regions, thus allowing a comprehensive evaluation of the effects of HILT
The study has some limitations that should be considered while interpreting the results. First, some heterogeneity identified in the pain and disability scores, thus we performed the meta-analysis using a random effects model. Subgroup analyses were conducted, which allowed a decrease in the heterogeneity of some subgroups as in case of comparing placebo with treatment of the back pain. Second, there may be a possibility of a publication bias. The results from the contoured funnel plot produced an asymmetry. However, the contoured funnel plot showed the missing data in both significant and not significant regions and the asymmetry of the contoured funnel plot could not completely explain the publication bias. Third, the detailed information relative to the application of the laser could not be presented because of the diversity of lasers, such as type of laser or application method, used in the included studies. Finally, all of the included studies were RCTs with short-term follow-up to elucidate the clinical effectiveness of HILT for pain management. However, the present study is meaningful as it presents the effectiveness of HILT for treatment of MSD.
5. Conclusions
The results of this study showed that HILT treatment for back and neck pain significantly improved pain and functional disability compared to controls. The ROB of the included studies was moderate; however, significant heterogeneity existed. Thus, in the future, larger, well-designed studies are warranted to assess different laser applications, treatment regions, and comparators.
Author contributions
Contributions: Conception and design: Hyun-Ju Seo and Hyun Jin Song; Literature search: Hyun-Ju Seo, Hyun Jin Song, Youngjin Lee, and Sung Kyu Kim; Quality assessment: Hyun-Ju Seo, Hyun Jin Song, Youngjin Lee, and Sung Kyu Kim; Data extraction: Hyun-Ju Seo, Hyun Jin Song, Youngjin Lee, and Sung Kyu Kim; Analysis and interpretation of data: Hyun-Ju Seo and Hyun Jin Song; Drafting of article: Hyun Jin Song; Obtaining of funding; Hyun-Ju Seo.
Hyun-Ju Seo orcid: 0000-0001-9019-1135.
Supplementary Material
Footnotes
Abbreviations: CI = confidence interval, CMS = Constant Murley Scale, DASH = Disabilities of the Arm Shoulder and Hand questionnaire, GDP = gross domestic product, HILT = high-intensity laser therapy, HILT = high-intensity laser therapy, LLLT = low-level laser therapy, MD = mean difference, MSD = musculoskeletal disorders, NDI = Neck Disability Index, NSAIDs = nonsteroidal anti-inflammatory drugs, ODI = Oswestry Disability Index, PRTEE = Patient-related Tennis Elbow Evaluation, RCT = randomized controlled trial, ROB = risk of bias, SD = standard deviation, SMD = standardized mean difference, SPADI = Shoulder Pain and Disability Index, TENS = transcutaneous electrical nerve stimulation, VAS = visual analog scale, WMD = weighted mean difference.
Ethics approval and consent to participate: Ethical approval was not needed for this study.
Competing interest: The authors declare that they have no competing interests.
All authors critically revised the manuscript and gave final approval of the article for submission.
This study was supported by a grant from Chosun University, Gwangju, Republic of Korea.
The authors have no conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
References
- [1].National Center for Health Statistics (NCHS). National Health Interview Survey (NHIS). Adult sample. Centers for Disease Control and Prevention (CDC). Available at: www.cdc.gov/nchs/nhis/nhis_2012_data_release.htm Accessed June 1, 2018. [Google Scholar]
- [2].Bone and Joint Initiative. The impact of musculoskeletal disorders on Americans – Opportunities for action. 2016. Available at: http://www.boneandjointburden.org/docs/BMUSExecutiveSummary2016.pdf Accessed June 1, 2018. [Google Scholar]
- [3].Medical Expenditures Panel Survey (MEPS). Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services, 1996–2011. Agency for Healthcare Research and Quality (AHRQ). Available at: https://www.meps.ahrq.gov/mepsweb/ Accessed June 1, 2018. [Google Scholar]
- [4].World Health Organization (WHO). Musculoskeletal conditions. Available at: http://www.who.int/mediacentre/factsheets/musculoskeletal/en/ Accessed June 1, 2018. [Google Scholar]
- [5].The National Institute for Occupational Safety and Health (NIOSH). Musculoskeletal Health Program. Centers for Disease Control and Prevention (CDC). Available at: https://www.cdc.gov/niosh/programs/msd/ Accessed June 1, 2018. [Google Scholar]
- [6].The National Institute for Occupational Safety and Health (NIOSH). Musculoskeletal disorders and workplace factors - A critical review of epidemiologic evidence for work-related musculoskeletal disorders of the neck, upper extremity, and low back. Centers for Disease Control and Prevention (CDC). Available at: https://www.cdc.gov/niosh/docs/97-141/ Accessed June 1, 2018. [Google Scholar]
- [7].Woolf AD, Akesson K. Understanding the burden of musculoskeletal conditions. The burden is huge and not reflected in national health priorities. BMJ 2001;322:1079–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Babatunde OO, Jordan JL, Van der Windt DA, et al. Effective treatment options for musculoskeletal pain in primary care: a systematic overview of current evidence. PLoS One 2017;12:e0178621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Braddon RLCL. Physical Medicine and Rehabilitation. Philadelphia: Saunders. Elsevier; 2011. [Google Scholar]
- [10].Clijsen R, Brunner A, Barbero M, et al. Effects of low-level laser therapy on pain in patients with musculoskeletal disorders: a systematic review and meta-analysis. Eur J Phys Rehabil Med 2017;53:603–10. [DOI] [PubMed] [Google Scholar]
- [11].Zati A, Valent A. Physical therapy: new technologies in rehabilitation medicine. Edizioni Minerva Medica 2006. 162–85. [Google Scholar]
- [12].Higgins JPT, Green S. (eds). Cochrane handbook for systematic reviews of interventions: The Cochrane Collaboration, version 5.1.0. 2011. Available at: http://handbook.cochrane.org/v5.0.2/ Accessed February 18, 2018. [Google Scholar]
- [13].Alayat MS, Atya AM, Ali MM, et al. Long-term effect of high-intensity laser therapy in the treatment of patients with chronic low back pain: a randomized blinded placebo-controlled trial. Lasers Med Sci 2014;29:1065–73. [DOI] [PubMed] [Google Scholar]
- [14].Alayat MS, Mohamed AA, Helal OF, et al. Efficacy of high-intensity laser therapy in the treatment of chronic neck pain: a randomized double-blind placebo-control trial. Lasers Med Sci 2016;31:687–94. [DOI] [PubMed] [Google Scholar]
- [15].Casale R, Damiani C, Maestri R, et al. Pain and electrophysiological parameters are improved by combined 830-1064 high-intensity LASER in symptomatic carpal tunnel syndrome versus Transcutaneous Electrical Nerve Stimulation. A randomized controlled study. Eur J Phys Rehabil Med 2013;49:205–11. [PubMed] [Google Scholar]
- [16].Chen L, Liu D, Zou L, et al. Efficacy of high intensity laser therapy in treatment of patients with lumbar disc protrusion: a randomized controlled trial. J Back Musculoskelet Rehabil 2018;31:191–6. [DOI] [PubMed] [Google Scholar]
- [17].Dundar U, Turkmen U, Toktas H, et al. Effect of high-intensity laser therapy in the management of myofascial pain syndrome of the trapezius: a double-blind, placebo-controlled study. Lasers Med Sci 2015;30:325–32. [DOI] [PubMed] [Google Scholar]
- [18].Dundar U, Turkmen U, Toktas H, et al. Effectiveness of high-intensity laser therapy and splinting in lateral epicondylitis; a prospective, randomized, controlled study. Lasers Med Sci 2015;30:1097–107. [DOI] [PubMed] [Google Scholar]
- [19].Fiore P, Panza F, Cassatella G, et al. Short-term effects of high-intensity laser therapy versus ultrasound therapy in the treatment of low back pain: a randomized controlled trial. Eur J Phys Rehabil Med 2011;47:367–73. [PubMed] [Google Scholar]
- [20].Haładaj R, Pingot M, Topol M. The effectiveness of cervical spondylosis therapy with Saunders traction device and high-intensity laser therapy: a randomized controlled trial. Med Sci Monit 2017;23:335–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Kim SH, Kim YH, Lee HR, et al. Short-term effects of high-intensity laser therapy on frozen shoulder: a prospective randomized control study. Man Ther 2015;20:751–7. [DOI] [PubMed] [Google Scholar]
- [22].Pekyavas NO, Baltaci G. Short-term effects of high-intensity laser therapy, manual therapy, and Kinesio taping in patients with subacromial impingement syndrome. Lasers Med Sci 2016;31:1133–41. [DOI] [PubMed] [Google Scholar]
- [23].Salli A, Akkurt E, İzkі AA, et al. Comparison of high intensity laser and epicondylitis bandage in the treatment of lateral epicondylitis. Arch Rheumatol 2016;31:234–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Santamato A, Solfrizzi V, Panza F, et al. Short-term effects of high-intensity laser therapy versus ultrasound therapy in the treatment of people with subacromial impingement syndrome: a randomized clinical trial. Phys Ther 2009;89:643–52. [DOI] [PubMed] [Google Scholar]
- [25].Huang Z, Ma J, Chen J, et al. The effectiveness of low-level laser therapy for nonspecific chronic low back pain: a systematic review and meta-analysis. Arthritis Res Ther 2015;17:360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Chow RT, Johnson MI, Lopes-Martins RA, et al. Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis of randomised placebo or active-treatment controlled trials. Lancet 2009;374:1897–908. [DOI] [PubMed] [Google Scholar]
- [27].Kujawa J, Zavodnik L, Zavodnik I, et al. Effect of low-intensity (3.75-25 J/cm2) near-infrared (810 nm) laser radiation on red blood cell ATPase activities and membrane structure. J Clin Laser Med Surg 2004;22:111–7. [DOI] [PubMed] [Google Scholar]
- [28].Hagiwara S, Iwasaka H, Hasegawa A, et al. Pre-Irradiation of blood by gallium aluminum arsenide (830 nm) low level laser enhances peripheral endogenous opioid analgesia in rats. Anesth Analg 2008;107:1058–63. [DOI] [PubMed] [Google Scholar]
- [29].Hsieh YL, Hong CZ, Chou LW, et al. Fluence-dependent effects of low-level laser therapy in myofascial trigger spots on modulation of biochemicals associated with pain in a rabbit model. Lasers Med Sci 2015;30:209–16. [DOI] [PubMed] [Google Scholar]
- [30].Chow R, Armati P, Laakso EL, et al. Inhibitory effects of laser irradiation on peripheral mammalian nerves and relevance to analgesic effects: a systematic review. Photomed Laser Surg 2001;29:365–81. [DOI] [PubMed] [Google Scholar]
- [31].Maeda T. Morphological demonstration of low reactive laser therapeutic pain attenuation effect of the gallium aluminum arsenide diode laser. Laser Ther 1989;1:23–6. [Google Scholar]
- [32].King CE, Clelland JA, Knowles CJ, et al. Effect of helium-neon laser auriculotherapy on experimental pain threshold. Phys Ther 1990;70:24–30. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.