

Supplemental Digital Content is available in the text
Keywords: cancer, epidemiology, incidence rates, public health, systematic review, United Arab Emirates
Abstract
Objective:
We conducted a systematic review to explore the United Arab Emirates (UAE)'s cancer-specific epidemiological profiles.
Methods:
We followed the standardized methods for conducting and reporting systematic reviews. We employed a highly sensitive and extensive strategy to identify all studies on the prevalence and incidence of cancer in the UAE, searching electronic databases and the grey literature. We assessed the methodological quality of the studies, summarized them, and qualitatively analyzed their results.
Results:
We included 4 retrospective studies published between 2003 and 2011, reporting data gathered between 1982 and 2004. The majority of the data were collected from national cancer registries and addressed adult Emiratis and certain cancer types. All included studies employed validated procedures for diagnostic confirmation. The overall age-standardized cancer rates were 70.1 and 74.2 per 100,000 in males and females, respectively. Lung, gastric, and prostate cancer ranked as the top 3 types in Emirati males; while breast, cervical, and thyroid cancer were the top 3 types in Emirati females. Men exhibited higher rates of lung and stomach cancers compared with women. The majority of the studies were of acceptable methodological quality.
Conclusions:
Our findings highlight the need for high-quality future research and systematic cancer data collection and registration to provide reliable data on the current incidence of cancer. We hope that our findings guide the tailoring of interventions aimed at curbing cancer rates in the UAE.
1. Introduction
Generally, worldwide cancer rates have increased, resulting in over 8.7 million deaths by 2015, thus ranking cancer as the second cause following cardiovascular diseases in associated mortality rates.[1] These are mostly related to rapid population growth, increasing life expectancy, urbanization with progressively westernized lifestyles.[2] Similarly, the burden of cancer in the United Arab Emirates (UAE) was high and ranked the second leading cause of non-communicable diseases (NCD)-related mortality in the country.[3,4] In the GLOBOCAN 2012 reports, cancer incidence and mortality rates in UAE reached 92.5 and 58 per 100,000 people, respectively.[5] During the mid-twentieth century, the UAE rose to become one of the fastest growing economies globally,[6–8] with this growth leading to economic, sociodemographic, and lifestyle changes of its population, paralleled by an epidemiological increase in the rates of NCD. Subsequent national studies in the UAE associated this increase in cancer rates with an accentuated exposure to several risk factors including physical inactivity and sedentary lifestyles,[9–11] the overconsumption of high-caloric and poorly-nutritive meals,[11] an increase in obesity rates,[12] an increase in smoking prevalence,[13] and elevated air pollutant levels.[14]
In 2011, the United Nations recognized NCDs, including cancer, as global crises, highlighting the need for implementation research to guide action against NCDs at regional and global levels.[15,16] Moreover, WHO announced that “in order to combat the global epidemic of cancer and NCDs it is imperative to create a baseline for monitoring trends and to assess the progress of countries in addressing the epidemic”. Cancer control planning requires accurate data, including reliable cancer registries and monitoring and evaluation programs to ensure programs are appropriately prioritized and to assure quality.[17] Consequently, WHO urged governments to strengthen their health information systems with reliable and evidence-based research data.
In light of this global need for NCD research, in addition to the lack of recent national estimates on cancer epidemiology in the UAE, it is important to understand the present status of the cancer burden and related risk factors in UAE. We, therefore, aimed to systematically review the literature on the epidemiology of cancer in the UAE to compile, critically appraise the available evidence, highlight existing gaps worth addressing in future studies and inform the country's responsible bodies of cancer's current epidemiological profile for use in tailoring interventions aligned with the local and global health agendas.
2. Materials and methods
We followed the standardized methods outlined by the PRISMA group for conducting and reporting our systematic review,[18] the protocol of which was registered on the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42016035747). Ethical approval was not required for this systematic review as no primary data were collected.
2.1. Database search
We used both, a free keyword search and a controlled vocabulary search (i.e., Medical Subject Headings (MeSH terms), to broaden the sensitivity of our search strategy. We adapted each of the search vocabulary terms used according to the databases searched which included: MEDLINE, PubMed, EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Index Medicus for the Eastern Mediterranean Region (IMEMR), ProQuest Dissertations & Theses Database, Open Access Theses and Dissertations (OATD), and Web of Science. To ensure a high sensitivity for our search and to maximize our retrieval of potentially eligible references, we attempted to exhaust the search vocabulary we used. Examples of MeSH terms included: “Neoplasms” for cancers; “United Arab Emirates, Arabs” for the UAE; and “Incidence, Prevalence, Epidemiological monitoring, Epidemiologic studies, Epidemiology” for epidemiology. We did not use any search filter for the date of publication, that is, we did not restrict our search to a particular time frame. A detailed copy of the search strategy used for each database is made available in (Appendix 1). We ran our initial search on June 19, 2015, and then updated it on April 4, 2017 to ensure that our retrieved references are up-to-date.
2.2. Searching other sources
In addition to searching online databases for relevant studies, we searched the grey literature, namely the websites of The International Diabetes Federation (IDF) and the World Bank. Moreover, we contacted expert scholars and public health researchers in the field to check for any ongoing relevant studies, and we searched the reference lists of the included studies for relevant research that we may have missed in our earlier search.
Our original search was intended to capture studies addressing the epidemiology and/or costs of each of cancer and cardiometabolic disorders in the UAE, 2 of the 4 NCDs of key importance to the country's public health professionals and policy-makers.[19] However, because cancer and cardiometabolic disorders likely differ regarding their underlying risk factors and patient profiles, we opted to report the data for each of them separately in a different review. Given the overlap in the search employed and the outcomes of interest, the 2 reviews share the same above-mentioned protocol (CRD42016035747).
2.3. Inclusion and exclusion criteria
All studies had to meet the following pre-set criteria for inclusion:
Original studies (e.g., editorials, case reports, case series, and reviews were excluded)
Observational design: cohort or cross-sectional designs for epidemiological studies (prevalence and incidence studies), economic models, cross-sectional, or longitudinal analyses for cost data
Addressing cancer (of any type)
Addressing data in the UAE
Addressing UAE population irrespective of age and nationality
Studies published in English or Arabic, with no limits on their year of publication.
2.4. Study selection
Independently and in pairs, 3 reviewers (RB, RR, and HR) searched for potentially eligible studies by screening subsets of the titles and abstracts of the retrieved references, using Endnote© as their reference manager. The authors then paired themselves into 2 teams (RB and RR; HR and HH); individually and as a pair, each team screened the retrieved full texts of the studies deemed potentially eligible earlier during the title and abstract screening stage. For the full-text screening stage, the authors used a screening tool that they had designed and pre-tested via a calibration exercise prior to this stage. When the members of a team disagreed on a particular study, they consulted a third reviewer for resolution.
2.5. Data extraction and analysis
After the completion of the stages above, the 2 members in each team –independently and in pairs- extracted relevant data from the included studies, consulting a third reviewer whenever they disagreed. As pre-set in our protocol, we performed a qualitative synthesis (i.e., narrative summary) of the data extracted from the included studies, since quantitative analysis (i.e., meta-analysis) was not feasible due to the considerable differences in the estimates used in the different studies. For epidemiological data, we sought to report age-standardized incidence rates (ASR) whenever available.
2.6. Risk of bias assessment
For risk of bias assessment, we used the tool employed by Kox et al[20] which is a modified version of the original tool employed by Shamliyan et al.[21] The original tool addresses the internal validity of a study, defined as the extent to which the results of a study are precise for its subjects, and the external validity of a study, the extent to which those results are generalizable to the target population.[21] The initial development of the checklist by Shamliyan et al[21] was based on a systematic literature review, and the checklist was then refined after pilot trials of validity and reliability were conducted by expert reviewers. We followed the scoring proposed by Kox et al,[20] whereby a score of 1 was granted when the criterion was sufficiently met; and a score of 0 when the criterion was unclear or insufficiently met.
Two authors (HR and RR) conducted the risk of bias assessment independently and as a pair, reaching consensus via discussion among each other in cases of disagreement.
3. Results
Our initial search addressing cancer and cardiometabolic diseases retrieved 6789 records, of which only 4 were eventually included. The subsequent updated search retrieved no new hits (Fig. 1). Table 1 summarizes the characteristics and results of the included studies.
Figure 1.
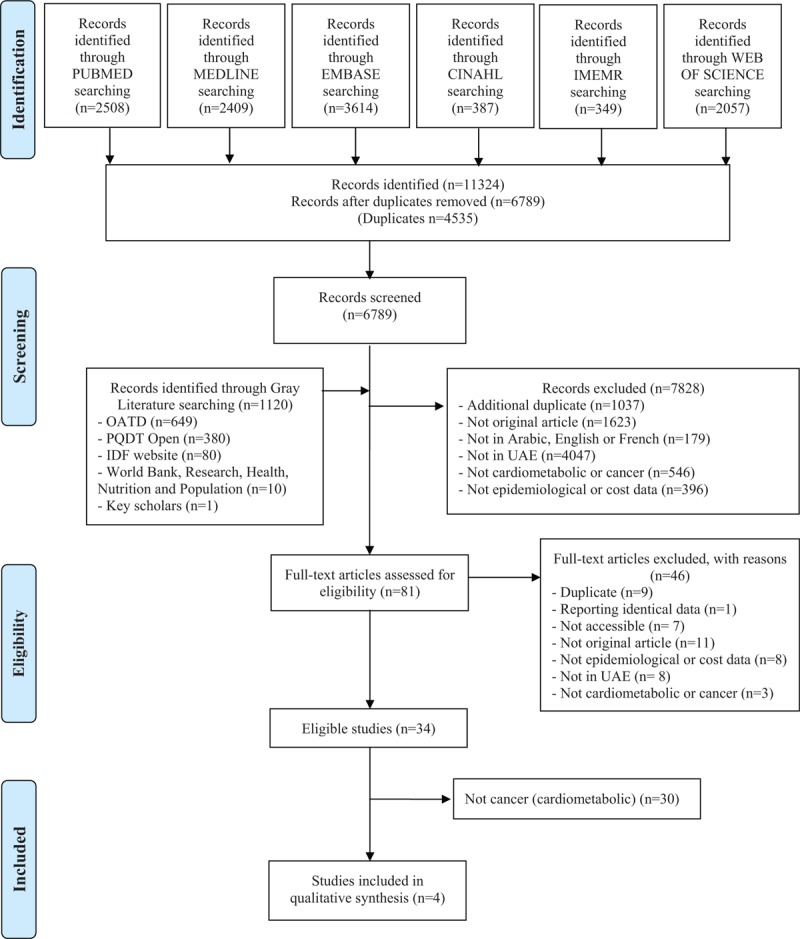
Flow diagram of reference screening and selection.
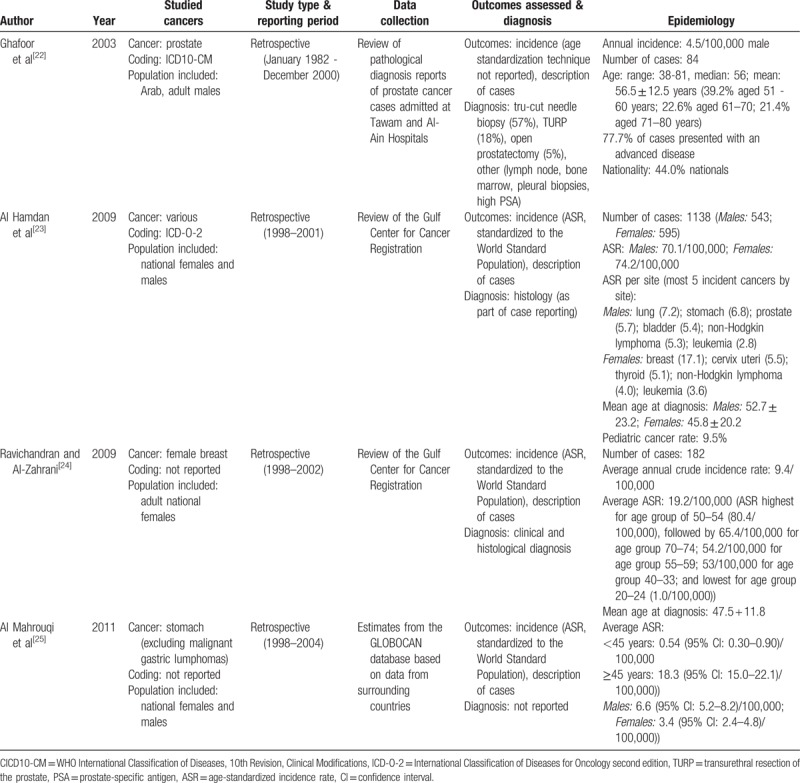
Table 1.
Characteristics and results of the included studies.
3.1. Characteristics of included studies
All included studies were published between 2003 and 2011,[22–25] reporting data gathered over different time intervals within an overall 22-year timeframe. The oldest time-point of data collection was 1982,[22] while the most recent one was 2004,[25] which clearly indicates a 13-year-gap in research from the latest time-point to present.
All 4 included studies collected their data retrospectively, with 1 of them reporting data collected over a period longer than a decade.[22] Our search did not retrieve any eligible cross-sectional or prospective studies, thus rendering us unable to trend cancer rates or determine its prevalence.
Only 1 study addressed cancer in general without focusing on a particular type,[23] while the rest focused on specific types/categories of cancer: prostate cancer,[22] female breast cancer,[24] and stomach cancer.[25]
Only Ghafoor et al[22] reported data retrieved from the medical records of all cancer cases admitted into local UAE hospitals, with Tawam Hospital in Al Ain region being the primary source of that data due to its predominance as a major oncology referral center in the UAE. The other studies were more likely to report accurate national estimates of cancer incidence, retrieving their data either from the Gulf Center for Cancer Registration which collects data from all over the UAE[23,24] or from the GLOBOCAN database which retrieves its data from neighboring countries.[25] To confirm their cancer diagnosis, all studies employed clinical, histological, and laboratory investigations, wherever applicable, with the exception of Al Mahrouqi et al[25] who did not report their diagnostic means.
Moreover, only 1 of the included studies reported data for patients of all nationalities,[22] while the rest reported data specific to Emiratis only.[23,24] Finally, only 2 studies reported ASRs for cancer incidence.[23,24]
As part of our gray literature search, we received 5 reports from the cancer registry at Tawam Hospital. The records did not report incidence or prevalence estimates, except for 1 reporting data from 1998 to 2001, which was later disseminated as an article by Al Hamdan et al;[23] and was included in our review.
3.2. Results of included studies
Among the included studies, Al Hamdan et al's study[23] provides the most exhaustive data on ASRs of all cancer types among Emiratis during the period 1998 to 2001. Thus, we decided to use it as the comparator for data reported by the other studies.
According to that study, the overall ASRs of cancer were 70.1 and 74.2 per 100,000 in males and females respectively, with pediatric cancers constituting around 9.5% of all newly diagnosed cases during that period.[23] According to that study, the 3 most incident cancers among Emirati males were lung (ASR:7.2), gastric (ASR:6.8), and prostate (ASR:5.7) cancers, in contrast to breast (ASR:17.1), cervical (ASR:5.5), and thyroid (ASR:5.1) cancers as the top 3 cancers among Emirati females.[23] Another study published in the same year collected its data over a comparable period of time (1998–2002) and validated breast cancer's top rank among female cancers, reporting a similar ASR of 19.2 for breast cancer among Emirati females.[24] Likewise, the UAE-specific estimate reported by Al Mahrouqi et al[25] for male gastric cancer overlapped with that of Al Hamdan et al[23] (ASRs of 6.6 and 6.8 respectively), confirming gastric cancer's remarkable incidence in males. The incidence of stomach cancers among Emirati women was found to be almost half of that of their male counterparts (ASR:3.4) according to the same study.[25] Al Hamdan et al[23] also highlighted the staggering difference in lung cancer incidence rates in Emirati females compared with males (ASRs of 2.9 vs 7.2 respectively). Finally, none of the included studies mentioned the histological type (s) of breast, stomach, or lung cancers most commonly encountered.
Regarding prostate cancer, Ghafoor et al[22] reported an incidence of 4.5 per 100,000 among Emirati males, an estimate that is slightly less than that reported more recently by Al Hamdan et al (ASR:5.7).[23] However, because the type of estimate reported by Ghafoor et al was unspecified (age-standardized or otherwise),[22] it is difficult to precisely compare the 2 estimates or to trend prostate cancer rates over time. Nonetheless, the former study[22] still reported an identical listing of the 3 most incident male cancers in the UAE (from most to least incident: lung, gastric, and prostate cancers)[22] as in Al Hamdan et al[23].
Finally, only 2 studies correlated part of their reported cancer incidences with established corresponding risk factors[23,24]: female breast cancer in association with reproductive factors,[24] and various types of cancer correlated with smoking practice (s) and/or reproductive factors.[23] However, none of those studies reported statistically appropriate association measures for the addressed risk factors and their corresponding cancer (s).
3.3. Quality of evidence in the included studies
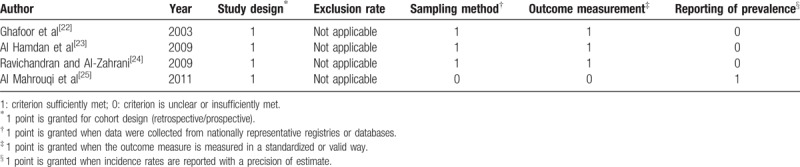
All included studies were minimally flawed with regards to their design as they employed a retrospective data collection approach.[22–25] Additionally, almost all of the included studies,[22–24] except for 1,[25] seem to have used adequate sampling methods through obtaining exhaustive samples from registry databases. Likewise, the same studies[22–24] appear to have employed standardized and validated diagnostic tools for cancer confirmation leading to minimally flawed outcome measurement, with the exception of the same study.[25] Conversely, however, only the latter study of Al Mahrouqi et al[25] provided ASR estimates with their confidence intervals as part of its reporting of cancer incidence (Table 2).
Table 2.
Risk of bias assessment of the included studies.
4. Discussion
To our best knowledge, this is the first systematic review addressing cancer epidemiology in UAE and highlighting existent gaps in the literature, that is, the lack of high-quality epidemiological studies, as well as detailed cancer registries within UAE.
It should be noted that the last national study conducted in the UAE on the topic was between 1998 and 2001,[23] listing lung, gastric, and prostate cancers as the 3 most incident cancers in men compared with breast, cervical, and thyroid cancers in women. Similarly, worldwide, Bray et al[26] reported that the most prevalent cancers are the breast, colorectal, prostate, lung, and stomach, while among women the most prevalent cancers are breast, cervical, and thyroid. The radical difference and lack of overlap in any of the most incident cancer types among the 2 sexes suggest considerably different underlying risk profiles among them. This warrants further investigation aimed at identifying those sex-specific determinants that may be targeted with future screening and treatment programs. Particularly, the more than 2-fold higher rate of lung cancer in men compared with women (ASR: 7.2 vs 2.9) is worth highlighting. Clearly, this may be due to lower rates of smoking among women compared with men in the UAE[27,28] (8.6% vs 37.4% respectively)[29] and should serve as a reminder of the importance of adequate tobacco control policies that would reduce the corresponding male lung cancer rates. The lung cancer ASR results in the UAE were similar to the results reported in Yemen (6.4 per 100,000), and Oman (6.7 per 100,000).[30] While in Lebanon, lung cancer was the most common cancer in 2003 with 31.6 cases per 100,000 people. This high ASR was due to high prevalence of smoking among Lebanese males.[31]
As for gastric cancer, Charafeddine et al[31] found that H. Pylori often establishes an asymptomatic chronic inflammatory process within the gastric mucosa following infection, and this process is strongly correlated with gastric cancers. Therefore, the high incidence rates of stomach cancer among UAE men could simply be the result of the high H. pylori-carrier rates among middle-easterners in general[32,33] and those with low socio-economic status in particular.[34] Just like the case of lung cancer, remarkably lower rates of gastric cancer were found in women compared with men in the UAE (ASR 3.4 vs 6.8 respectively).[23] However, this may be due to a lack of adequate or any control in the study of smoking status, which has been identified as a confounder in several studies associating H. pylori infection with gastric cancer, as highlighted by Peleteiro et al.[35] This study[35] demonstrated a specifically much stronger direct correlation between positive H. pylori carrier status in addition to concomitant smoking and developing gastric cancer, compared with a positive H. pylori carrier status alone.
Breast cancer is the most common cancer among women in Arab countries.[36] Breast cancer incidence among women in this review was strikingly much higher than that of any other cancer in either sex.[23] In fact, the Health Authority of Abu Dhabi (HAAD) reported that the prevalence of breast cancer among all cancers diagnosed in Abu Dhabi reached 20.3% in 2014, with an associated mortality rate of 12.2%, thus making breast cancer the most incident in that Emirate.[37] Similarly, another study conducted in 2013 at Tawam Hospital also reported breast cancer as the most common female cancer, constituting 22.8% of all female cancers.[38] However, the remarkably lower ASR of breast cancer among Arab compared with western women[39] is paradoxically met by an earlier onset of cancer (by up to a decade) in the former group.[40,41] Similar breast cancer ASR was reported in Kuwait[42] while it was higher in Jordan[43] and Lebanon.[44] Thus, it is also worthwhile to investigate the reasons behind those differences in order to possibly identify the risk factors unique to each.[39] Moreover, a small-scale study conducted at Tawam Hospital in 2012 showed that women aged less than 40 in the UAE possess a much higher incidence of HER2-positive breast cancer compared with their older counterparts (54.3% vs 34.2% respectively; P = .007).[45] Thus, in addition to its worse prognosis compared with other breast cancer subtypes, higher proportion in younger compared with older Emirati women, and the earlier age of onset of breast cancer in general in Emirati women compared with their western counterparts,[46,47] lands breast cancer its second rank among the most common causes of death in UAE women as per the Ministry of Health (MOH).[48]
The results from this review are comparable with incidence estimates provided by GLOBOCAN, except for the incidence of female breast cancer which was reported to be 17.1 cases per 100.000 women in this analysis, compared with 39.2 cases per 100.000 women in GLOBOCAN.[5] The discrepancy between the GLOBOCAN's reported incidence rate and the one reported in this study could be due to the inadequate documentation of breast screening and early detection programs, as well as under-reporting and incompleteness of the cancer registry in the UAE.
It should be noted that the age-standardized rates for the incidence and mortality from the most common types of cancer (breast, lung, colorectal) in the UAE are lower compared with Western countries.[5] This is likely to be due to the younger age of the population, less exposure to some risk factors, lower levels of screening compared with Western countries, and possibly incomplete registration. However, these rates are projected to double by the year 2020, since life expectancy of the population in the UAE is increasing, the exposure time to lifestyle risk factors will increase[4] and maintaining health and allocating resources in old age will become increasingly challenging.[49]
Our exhaustive and highly sensitive search strategy used to retrieve relevant studies and our adherence to standardized and validated methods of systematic review conduction[18] contribute to the rigor of our review. Moreover, our transparency in reporting the search employed and our use of a validated quality assessment tool also enhance our review's credibility further.
However, our review also faces major limitations that should be taken into consideration in interpreting the results. First of all, we were limited by the fact that the studies included did not report the estimate precision for each of their point estimates, with the exception of only 1 study, that by Al Mahrouqi et al[25]. Moreover, almost all the data reported in our review were derived from the Gulf Center for Cancer Registration, posing a major limitation on our reported data and coupled with the lack of adequate and up-to-date centralized registries to keep track of all new incident cases and trend cancer incidence over time limited our confidence in the generated data. Ideally and whenever possible, the effect estimates reported by each study included in a systematic review should be pooled together to provide a generalized pooled estimate for the outcome of interest. However, in systematic reviews of epidemiological studies such as our review, qualitative (i.e., narrative) synthesis of the extracted data is preferred given that in many instances the estimates reported differ remarkably among the studies with regards to their type (percentages, proportions, patient-years etc.) and the years they span, making their pooling an actual error rather than a need. Thus, we were limited to perform a qualitative synthesis of the data in our review to avoid non-coherent and heterogeneous pooling errors. Moreover, we could not find any study assessing pediatric cancers in the UAE; this is particularly worth highlighting given the UAE's large youth proportion that makes up about 34% of the nation.[50] Finally, we were unable to identify the population's specific risk factors of cancer, which otherwise could have been targeted by national interventional efforts.
5. Conclusions
Generally, this study attempted to provide compiled incidence data of cancer rates in UAE, identify gaps, and inform healthcare specialists on the problems arising from lack of up to date detailed cancer incidence registration in UAE. We hope that the findings of our review provide a comprehensive and preliminary evidence for future relevant studies to build upon since awareness of status and trends in the incidence rate of cancer in the country can be useful for better planning and prevention.
We highlight the need for high-quality future research in this area to provide reliable data on the current incidence of cancer in the UAE to investigate the population's specific cancer determinants, and to identify the reasons behind the existent differences in cancer rates across the sexes and nationalities within the country. We hope our findings provide some evidence on the need for more detailed cancer data collation and registration that should be regularly updated to reflect the true burden of cancer in UAE since the cancer burden is expected to increase due to population growth and increasing life expectancies in UAE.
Acknowledgments
We would like to thank Dr Maria Amer who is the Cancer Registry Manager in Tawam Hospital—Al Ain—UAE for her valuable assistance.
Author contributions
Conceptualization: Hadia Radwan, Rami A. Ballout, Rana Rizk.
Formal analysis: Hadia Radwan, Hayder Hasan, Rami A. Ballout, Rana Rizk.
Methodology: Hadia Radwan.
Supervision: Rana Rizk.
Writing – original draft: Hadia Radwan, Rami A. Ballout, Rana Rizk.
Writing – review & editing: Hadia Radwan, Hayder Hasan, Rami A. Ballout, Rana Rizk.
Rana Rizk orcid: 0000-0002-8850-6502.
Supplementary Material
Footnotes
Abbreviations: ASR = age-standardized incidence rates, MeSH terms = Medical Subject Headings, NCD = non-communicable diseases, UAE = United Arab Emirates.
The authors have no conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
References
- [1].Fitzmaurice C, Allen C, Barber RM, et al. Global Burden of Disease Cancer Collaboration Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the Global Burden of Disease Study. JAMA Oncol 2017;3:524–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Belahsen R. Nutrition transition and food sustainability. Proc Nutr Soc 2014;73:385–8. [DOI] [PubMed] [Google Scholar]
- [3].World Health Organization. Regional Office for the Eastern Mediterranean. United Arab Emirates. Noncommunicable Diseases (NCD) Country Profiles. 2014. Available at: http://www.who.int/nmh/countries/are_en.pdf?ua=1 Accessed April 22, 2018. [Google Scholar]
- [4].Loney T, Aw TC, Handysides DG, et al. An analysis of the health status of the United Arab Emirates: the “Big 4” public health issues. Glob Health Action 2013;6:20100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN. Int J Cancer 2015;5:E359–386. [DOI] [PubMed] [Google Scholar]
- [6].Government.ae. The Official Portal of UAE Government. 2016. Available at: https://government.ae/en/about-the-uae Accessed August 16, 2016. [Google Scholar]
- [7].Shihab M. Abed IA, Hellyer P. Economic Development in the UAE. United Arab Emirates: a new perspective. London: Trident Press Ltd; 2001. 249–60. [Google Scholar]
- [8].United Arab Emirates National Bureau of Statistics. Population Estimates 2006–2010. nd. Available at: http://www.fcsa.gov.ae/ReportPDF/Population%20Estimates%202006%20-%202010.pdf Accessed August 5, 2016. [Google Scholar]
- [9].Henry CJK, Lightowler HJ, Al-Hourani HM. Physical activity and levels of inactivity in adolescent females ages 11-16 years in the United Arab Emirates. Am J Hum Biol 2004;16:346–53. [DOI] [PubMed] [Google Scholar]
- [10].World Health Organization. Regional Office for the Eastern Mediterranean. Country cooperation strategy for WHO and United Arab Emirates: 2012–2017. 2012 [cited 2017 Sep 29]; Available at: http://apps.who.int/iris/bitstream/10665/113226/1/CCS_UAE_2012_EN_14947.pdf. [Google Scholar]
- [11].Ng SW, Zaghloul S, Ali H, et al. Nutrition transition in the United Arab Emirates. Eur J Clin Nutr 2011;65:1328–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study. Lancet 2014;384:766–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Maziak W, Taleb ZB, Bahelah R, et al. The global epidemiology of waterpipe smoking. Tob Control 2015;24suppl 1:i3–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Brauer M, Freedman G, Frostad J, et al. Ambient air pollution exposure estimation for the Global Burden of Disease. Environ Sci Technol 2016;50:79–88. [DOI] [PubMed] [Google Scholar]
- [15].United Nations General Assembly. Political declaration of the high-level meeting of the general assembly on the prevention and control of noncommunicable diseases. 2011; United Nations. Imprint [New York]: UN, 16 Sept. 2011. [Google Scholar]
- [16].Beaglehole R, Bonita R, Alleyne G, et al. UN high-level meeting on non-communicable diseases: addressing four questions. Lancet 2011;378:449–55. [DOI] [PubMed] [Google Scholar]
- [17].World Health Organization. National Cancer Control Programmes (NCCP). 2018. Available at: http://www.who.int/cancer/nccp/en/ Accessed May 05, 2018. [Google Scholar]
- [18].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].World-Class Healthcare UAE Vision 2021. 2017. Available at: https://www.vision2021.ae/en/national-priority-areas/world-class-healthcare Accessed May 10, 2017. [Google Scholar]
- [20].Kox LS, Kuijer PPF, Kerkhoffs GM, et al. Prevalence, incidence and risk factors for overuse injuries of the wrist in young athletes: a systematic review. Br J Sports Med 2015;49:11898–21196. [DOI] [PubMed] [Google Scholar]
- [21].Shamliyan TA, Kane RL, Ansari MT, et al. Development quality criteria to evaluate nontherapeutic studies of incidence, prevalence, or risk factors of chronic diseases: pilot study of new checklists. J Clin Epidemiol 2011;64:637–57. [DOI] [PubMed] [Google Scholar]
- [22].Ghafoor M, Schuyten R, Bener A. Epidemiology of prostate cancer in United Arab Emirates. Med J Malaysia 2003;58:712–6. [PubMed] [Google Scholar]
- [23].Al Hamdan N, Ravichandran K, Al Sayyad J, et al. Incidence of cancer in Gulf Cooperation Council countries, 1998-2001. East Mediterr Health J 2009;15:600–11. [PubMed] [Google Scholar]
- [24].Ravichandran K, Al Zahrani AS. Association of reproductive factors with the incidence of breast cancer in Gulf Cooperation Council countries. East Mediterr Health J 2009;15:612–21. [PubMed] [Google Scholar]
- [25].Al-Mahrouqi H, Parkin L, Sharples K. Incidence of stomach cancer in Oman and the other Gulf Cooperation Council countries. Oman Med J 2011;26:258–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Bray F, Ren JS, Masuyer E, et al. Global estimates of cancer prevalence for 27 sites in the adult population in. Int J Cancer 2013;132:1133–45. [DOI] [PubMed] [Google Scholar]
- [27].Trading Economics. Smoking prevalence - males (% of adults) in the United Arab Emirates. 2017. Available at: https://tradingeconomics.com/united-arab-emirates/smoking-prevalence-males-percent-of-adultswb-data.html Accessed September 29, 2017. [Google Scholar]
- [28].Awofeso N, Hamidi S, Rammohan A, et al. Correlates of tobacco use and physical activity among Emirati citizens and non-citizens residents in Dubai, UAE. Glob J Med Public Health 2014;3: [Google Scholar]
- [29].Khattab A, Javaid A, Iraqi G, et al. Smoking habits in the Middle East and North Africa: Results of the BREATHE study. Respir Med 2012;106suppl 2:S16–24. [DOI] [PubMed] [Google Scholar]
- [30].Pakzad R, Mohammadian-Hafshejani A, Ghoncheh M, et al. The incidence and mortality of lung cancer and their relationship to development in Asia. Transl Lung Cancer Res 2015;4:763–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Charafeddine MA, Olson SH, Mukherji D, et al. Proportion of cancer in a Middle Eastern country attributable to established risk factors. BMC Cancer 2017;17:337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Khedmat H, Karbasi-Afshar R, Agah S, et al. Helicobacter pylori infection in the general population: a Middle Eastern perspective. Casp J Intern Med 2013;4:745–53. [PMC free article] [PubMed] [Google Scholar]
- [33].Bener A, Adeyemi EO, Almehdi AM, et al. Helicobacter pylori profile in asymptomatic farmers and non-farmers. Int J Environ Health Res 2006;16:449–54. [DOI] [PubMed] [Google Scholar]
- [34].Bener A, Uduman SA, Ameen A, et al. Prevalence of Helicobacter pylori infection among low socio-economic workers. J Commun Dis 2002;34:179–84. [PubMed] [Google Scholar]
- [35].Peleteiro B, Bastos J, Barros H, et al. Systematic review of the prevalence of gastric intestinal metaplasia and its area-level association with smoking. Gac Sanit 2008;22:236–46. [DOI] [PubMed] [Google Scholar]
- [36].El Saghir NS, Khalil MK, Eid T, et al. Trends in epidemiology and management of breast cancer in developing Arab countries: a literature and registry analysis. Int J Surg 2007;5:225–33. [DOI] [PubMed] [Google Scholar]
- [37].Health Authority-Abu Dhabi, Department of Health. Cancer Facts & Statistics. 2017. Available at: https://www.haad.ae/simplycheck/tabid/140/Default.aspx Accessed September 29, 2017. [Google Scholar]
- [38].Al-Sharbatti SS, Shaikh RB, Mathew E, et al. Assessment of breast cancer awareness among female university students in Ajman, United Arab Emirates. Sultan Qaboos Univ Med J 2014;14:e522–529. [PMC free article] [PubMed] [Google Scholar]
- [39].Breast Cancer Around the World - TIME [Internet]. [cited 2017 Sep 29]. Available at: http://webcache.googleusercontent.com/search?q=cache:ic9IEu7f2Y8J:content.time.com/time/interactive/0,31813,1668275,00.html&num=1&hl=en&gl=lb&strip=1&vwsrc=0. [Google Scholar]
- [40].Najjar H, Easson A. Age at diagnosis of breast cancer in Arab nations. Int J Surg 2010;8:448–52. [DOI] [PubMed] [Google Scholar]
- [41].Anders CK, Hsu DS, Broadwater G, et al. Young age at diagnosis correlates with worse prognosis and defines a subset of breast cancers with shared patterns of gene expression. J Clin Oncol 2008;26:3324–30. [DOI] [PubMed] [Google Scholar]
- [42].Elbasmi A1, Al-Asfour A, Al-Nesf Y, et al. Cancer in Kuwait: magnitude of the problem. AGulf J Oncol 2010;8:7–14. [PubMed] [Google Scholar]
- [43].Al-Tarawneh M, Khatib S, Arqub K. Cancer incidence in Jordan. East Mediterr Health J 2010;16:837–45. [PubMed] [Google Scholar]
- [44].Shamseddine A, Saleh A, Charafeddine M, et al. Cancer trends in Lebanon: a review of incidence rates for the period of 2003–2008 and projections until. Popul Health Metr 2014;12:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Bashir MA, Ali NA, Shaban S, et al. Young women in the UAE have higher incidence of HER2 positive breast cancer. Breast J 2012;18:637–8. [DOI] [PubMed] [Google Scholar]
- [46].Sorlie T, Perou CM, Tibshirani R, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci 2001;98:10869–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Sorlie T, Tibshirani R, Parker J, et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc Natl Acad Sci U S A 2003;100:8418–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].The National. Women in UAE need to be aware of cardiovascular disease. 2013. Available at: https://www.thenational.ae/uae/health/women-in-uae-need-to-be-aware-of-cardiovascular-disease-1.313491 Accessed September 29, 2017. [Google Scholar]
- [49].Hajjar RR, Atli T, Al-Mandhari Z, et al. Prevalence of aging population in the Middle East and its implications on cancer incidence and care. Ann Oncol 2013;24suppl 7:vii11–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].The World Factbook—Central Intelligence Agency [Internet]. [cited 2017 Sep 29]. Available at: https://www.cia.gov/library/publications/the-world-factbook/geos/ae.html14947.pdf. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.