

Abstract
AIM
To assess the association between liver fat content (LFC) and weight status in young adults using proton magnetic resonance spectroscopy (1H MRS) technique.
METHODS
Seventy-eight healthy young adults, between 19-30 years of age participated in this study. This group was then separated into a control of 39 subjects and an overweight/obese group (OW/OB group) consisting of 39 subjects. Blood biochemical quantity and 1H MRS was performed for LFC assessment.
RESULTS
LFC was found to be almost three times higher in OW/OB group when compared to the control group. A 48.7% incidence of non-alcoholic fatty liver disease in the OW/OB group was found. Blood biochemical measurements showed statistically higher low-density lipoproteins and triglyceride, lower high-density lipoproteins, and increased glycosylated hemoglobin and fasting glucose in the OW/OB group. Body mass index was a significant independent predictor for LFC after adjusting for age and sex (multiple linear regression; β = 0.459, P < 0.001).
CONCLUSION
Due to the prevalence of high LFC in the OW/OB group, it can be proposed that weight gain and obesity are sensitive indicators of high hepatic fat content.
Keywords: Young adults, Overweight, Obesity, Non-alcoholic fatty liver disease, Body mass index, Proton magnetic resonance spectroscopy, Cholesterol
Core tip: Non-alcoholic fatty liver disease (NAFLD) is one of the most common chronic liver diseases. The prevalence of NAFLD in young adults is a growing public health concern. Interestingly, the liver fat content (LFC) of an overweight/obese group was approximately three times higher than the control group. This result suggests that obesity can increase LFC and is a risk factor for higher NAFLD in overweight and obese young adults. This current study also demonstrated the importance of Body Mass Index as a tool for risk prevention and control of NAFLD and metabolic syndromes.
INTRODUCTION
Non-alcoholic fatty liver disease (NAFLD) is one of the most common chronic liver diseases and is increasing at an alarming rate. Previous studies have reported a positive correlation between BMI and lipid accumulation in the liver, which leads to a higher risk of NAFLD, cirrhosis[1,2], and dyslipidemia[3].
Due to modern lifestyles and diet, there has been a persistent increase in the number of NAFLD patients. This increase occurred at the same time that there were also increases in the number of people considered to be obese all over the world[4,5]. NAFLD in young adults is a topic that has received slight recognition, yet this age group is the most likely to gain weight and develop obesity from diet and lifestyle as they are transitioning into adulthood[6]. The prevalence of NAFLD in young adults has increased almost 2.5 times over 30 years with half of morbidly obese young adults having NAFLD[7]. However, despite the growing public health concern about obesity and NAFLD in young adults, necessary information addressing the effects of obesity and NAFLD pathogenesis in this age group is lacking, and there is an urgent need for better consideration of its effects and mechanisms[8,9]. Proton magnetic resonance spectroscopy (1H MRS) is a well-established non-invasive technique for liver metabolite assessment and is known for its high accuracy for determining liver fat quantification when compared to biopsy[10,11]. As far as we know, there’s no study to date that has investigated the effects of obesity on liver fat content (LFC) by 1H MRS in healthy young adults.
The aim of this present study is to assess the association between LFC by 1H MRS technique, blood serum biochemical measures of total cholesterol (Cho), low-density lipoproteins (LDL), high-density lipoproteins (HDL), fasting plasma glucose (FG), glycosylated hemoglobin (HbA1c), and being overweight/obese (OW/OB) as a young adult.
MATERIALS AND METHODS
Study population
The subjects of this current study were 78 healthy young adults between 19-30 years of age. Subjects were randomly chosen from a young adult population residing in Chiang Mai, Thailand through recruitment efforts using posters, or were personally invited to join the study. The control group was comprised of 39 subjects who had engaged in moderate physical activity, and who had a body mass index (BMI) in the normal range according to the World Health Organization (15.8-24.9 kg/m2)[12]. The OW/OB group was comprised of 39 subjects who had a BMI that was in the overweight and obese range (> 25 kg/m2)[12]. Exclusion criteria for both groups was diagnoses with a chronic disease or liver injury in any form, alcohol consumption of more than 150 g/wk, hyperglycemia (FBS > 140 mg/dL), hypertriglyceridemia (TG > 300 mg/dL), hepatotoxic medication usage, athletes, contraindication for magnetic resonance imaging (MRI), and poor 1H MRS resolution. Subjects were given a questionnaire about health and lifestyle in order to include or exclude subjects for the study. Eating and exercise habits, occupation, and personal and family medical history were also provided. The Ethics Committee of the Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai, Thailand (AMSEC-61EX-016) approved all procedures.
LFC assessment by 1H MRS
Liver metabolite spectra were obtained by 1H MRS technique on MRI 1.5 T (Achieva, Philips Medical Systems, Best, The Netherlands) using sense cardiac coil. T2-weighted turbo spin echo (TSE) transverse (TR/TE = 871/80 ms) and coronal T2-weighted (TR/TE = 829/80 ms) images were applied for localization. PRESS sequence with TR = 2000 ms, TE = 43 ms, number of signal averages = 96. Voxel size of 10 × 10 × 10 mm3 was carefully placed in right lobe of the liver (Couinaud lobe segment V-VIII), carefully avoiding any large vessels and bile duct. The liver metabolite signals without water suppression were obtained and analyzed for metabolized quantification by AMARES algorithm available on jMRUI software[13-15]. Spectrum fitting and quantification was done for water peak (4.72 ppm), and major lipid spectrum peaks (CH3 = 0.9 ppm, CH2 = 1.3 ppm, 2.1 ppm) with prior knowledge and Gaussian line shape was then applied[16]. Signal intensity correction was done for T2 relaxation using linear least-square equation with previous determination for T2 of water and fat. LFC was calculated by a validated method described elsewhere[17,18]. NAFLD was determined as LFC > 5.56%[18].
Blood examination
Blood collection of subjects was done by The Associated Medical Science Clinical Service Center, Chiang Mai University. Ten milliliters of intravenous blood was drawn from antecubital veins and was biochemically analyzed using a fully automated analyzer (Architect ci8200, Abbott Diagnostic). The test focused on Cho, HDL, VLDL, TG, FG, and HbA1c. Subjects were told to fast for 10-12 h prior to blood examination. Later, LDL concentration was calculated from novel adjustable LDL estimation equations[19,20].
Dyslipidemia was described as an abnormality of Cho levels in plasma including increased Tri and LDL, and decreased HDL. The National Cholesterol Education Project (NCEP) Adult Treatment Panel (ATP) III has defined dyslipidemia as Cho ≥ 200 mg/dL, Tri ≥ 150 mg/dL, LDL ≥ 130 mg/dL, and HDL ≤ 40 mg/dL[21]. Normal FG ranges should be between 70-100 mg/dL, and FG between 100-125 mg/dL is considered prediabetes. Normal HbA1c levels should be less than 6%[22].
Anthropometry
The same examiner measured every subject. Subjects wore only an examination cloth. Height and bodyweight were measured to the nearest 0.5 cm and 0.1 kg respectively. Waist circumference (WC) and hip circumference (HC) was acquired while instructed to breathe out mildly. Both measurements were done using non-elastic tape. WC was measured at the midpoint of the lower margin of the rib and the top of the iliac crest. HC was measured at the widest section of the buttocks. Waist-to-hip ratio (W/H ratio) was calculated from WC divided by HC.
Statistical analysis
Statistical analysis was performed using SPSS statistical software version 17.0. Normal distribution results are expressed as mean ± SD. The Kolmogorov-Smirnov test and the Shapiro-Wilk test were performed to determine data normality. Comparison of LFC and blood biochemical examination between groups was then further compared with an unpaired samples t-test. Relationship between groups was done with Pearson correlation. Multiple stepwise linear regression analysis was used to verify the relationships between LFC and independent of significant corelate variables. Results with P value < 0.05 were considered statistically significant.
RESULTS
A total of 78 healthy subjects in the young adult age group (19-30 years old) participated in this study. The control group of 39 subjects and the OW/OB group of 39 subjects had an average BMI of 20.9 ± 0.3 and 31.3 ± 0.5 kg/m2, respectively. The characteristics of LFC, anthropometric, and biochemical data of all subjects are shown in Table 1.
Table 1.
Characteristic and biochemical analysis of 78 subjects in the control and overweight/obese groups
| Control group | OW/OB group | P-value |
Correlation with LFC |
||
| r | P value | ||||
| n | 39 | 39 | - | - | - |
| Gender (male/female) | 12/27 | 24/15 | - | - | - |
| LFC (%) | 2.7 ± 0.2 | 8.1 ± 1.0 | < 0.001b | - | - |
| Age | 22.3 ± 1.6 | 22.1 ± 0.3 | 0.662 | -0.058 | 0.611 |
| BMI (kg/m2) | 20.9 ± 0.3 | 31.3 ± 0.5 | < 0.001b | 0.531 | < 0.001b |
| WC (cm) | 74.6 ± 1.4 | 112.6 ± 7.4 | < 0.001b | 0.259 | 0.022a |
| HC (cm) | 90.7 ± 1.3 | 122.5 ± 7.5 | < 0.001b | 0.212 | 0.062 |
| W/H ratio | 0.8 ± 0.0 | 0.9 ± 0.0 | < 0.001b | 0.388 | < 0.001b |
| FG (mg/dL) | 83.1 ± 1.1 | 89.9 ± 1.1 | < 0.001b | 0.144 | 0.21 |
| Cho (mg/dL) | 187.3 ± 6.8 | 200.7 ± 6.1 | 0.147 | 0.093 | 0.419 |
| Tri (mg/dL) | 77.8 ± 5.2 | 117.1 ± 8.8 | < 0.001b | 0.223 | 0.05 |
| HDL (mg/dL) | 59.3 ± 2.5 | 47.7 ± 1.4 | < 0.001b | -0.185 | 0.105 |
| LDL (mg/dL) | 111.1 ± 5.6 | 130.1 ± 5.1 | 0.014a | 0.133 | 0.246 |
| HbA1c (%) | 5.1 ± 0.1 | 5.5 ± 0.1 | < 0.001b | 0.345 | 0.002a |
Data expressed as mean ± SD.
P < 0.05;
P < 0.001. OW/OB: Overweight/obese; LFC: Liver fat content; BMI: Body mass index; WC: Waist circumference; HC: Hip circumference; W/H ratio: Waist-to-hip ratio; FG: Fasting plasma glucose; Cho: Cholesterol; Tri: Triglyceride; HDL: High-density lipoproteins; LDL: Low-density lipoproteins; HbA1c: Glycosylated hemoglobin.
Seventy-eight spectra were obtained and were analyzed for LFC. The corrected value of liver fat by weight was calculated by a method validated by Longo et al[17] and Szczepaniak et al[18]. Representative spectrum from the right lobe of the liver was shown in Figure 1.
Figure 1.

Proton magnetic resonance spectroscopy technique was used for liver fat assessment. Water peak was shown occurring at 4.72 ppm, peaks in fat for CH3 occurred at 0.9 ppm, and CH2 peaked at 1.3 ppm and 2.1 ppm. A: Magnetic resonance imaging axial image of abdomen show voxel localization in right lobe liver for liver fat content quantification. B: Representative fitted proton magnetic resonance spectroscopy spectrum of right lobe liver.
As expected, LFC, anthropometric, and biochemical results were significantly different between the two groups with the exception of age and Cho. The OW/OB group reported statistically higher BMI, LFC, WC, HC, FG, Tri, LDL, HbA1c, and statistically lower HDL. Cho also was found to be increased in the OW/OB group, but this tendency was not statistically significant. The prevalence of dyslipidemia in the OW/OB group (69.2%) was higher than in the control group (48.7%). There were no subjects in the control group who exceeded the normal FG and HbA1c ranges.
Interestingly, the LFC of the OW/OB group was approximately three times higher than the control group. Additionally, 19 subjects (48.7%) in the OW/OB group had LFC > 5.56%, which is considered to be a cut off point for NAFLD according to a previous large cohort 1H MRS LFC study[18]. Furthermore, dyslipidemia was present in 47.4% of participants in the OW/OB group, and abnormal HbA1c was found in 10.5% of OW/OB subjects.
The data in this study was normally distributed. Pearson correlation analysis was conducted as preliminary analysis for possible predictor variable for LFC and is presented in Table 1. Various statistically significant correlations of LFC and variables were found, with moderate correlation occurring with BMI and mild correlation with W/H ratio, HbA1c, and waist circumference. Among the blood biochemical results, HbA1c showed the highest correlation with LFC followed by Tri. The Pearson correlations and data distribution by sex in both groups is shown in Figure 2. This indicates that the overall data between male and woman in each group is distributed in the same way.
Figure 2.

Pearson correlation coefficient (r) and data distribution by sex in each group between body mass index, waist-to-hip ratio, glycosylated hemoglobin, and liver fat content as measured by proton magnetic resonance spectroscopy. BMI: Body mass index; HbA1c: Glycosylated hemoglobin; LFC: Liver fat content; W/H ratio: Waist-to-hip ratio.
The correlation was then compared between HbA1c and FG to determine the indicator for diabetes. Even if a low positive correlation was found in FG, it is not statistically significant, while the HbA1c showed a statistically significant positive correlation with LFC. The correlation of diabetes (HbA1c and FG) markers is compared in Figure 3.
Figure 3.
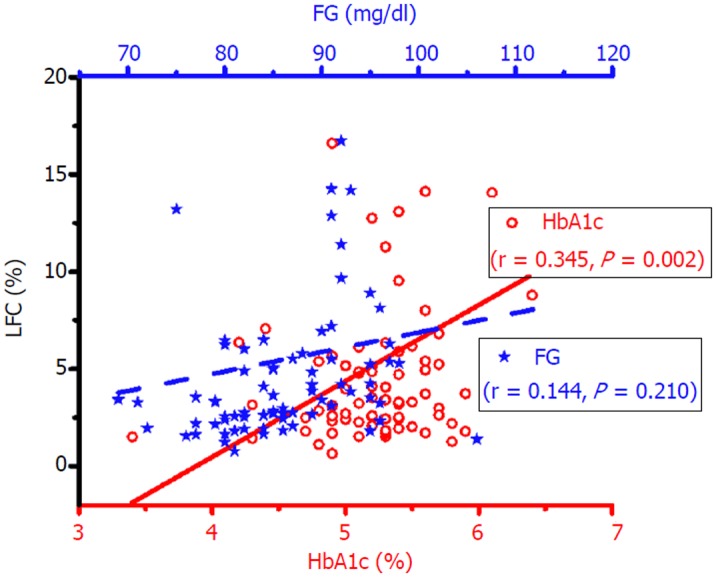
Pearson correlation between glycosylated hemoglobin (circle in red, lower x axis), fasting plasma glucose (star in blue, upper X axis), and liver fat content as measured by proton magnetic resonance spectroscopy. BMI: Body mass index; FG: Fasting plasma glucose; HbA1c: Glycosylated hemoglobin; LFC: Liver fat content.
A multiple linear regression was used to predict the LFC from significantly correlated blood biochemical marker (HbA1c, Tri) and anthropography marker (BMI, W/H ratio). Standardized coefficient and correlations are presented in Table 2. BMI and HbA1c were found to be significant positive independent predictor for LFC after adjusting for age and sex. However, only BMI remained statistically significant as an independent predictor for LFC after HbA1C adjusting for age, sex, and BMI.
Table 2.
Multiple linear regression analysis showing relationship of blood biochemical marker and anthropometry marker with LFC as the dependent variable
|
Model 1 |
Model 2 |
Model 3 |
|||||||
| R2 | β(SE) | P | R2 | β(SE) | P | R2 | β(SE) | P | |
| HbA1c | 0.135 | 0.306 | 0.002 | 0.174 | 0.339 | 0.004 | 0.298 | 0.120 | 0.327 |
| (1.273) | (1.283) | (1.379) | |||||||
| Tri | 0.131 | 0.247 | 0.065 | 0.590 | -0.029 | 0.590 | |||
| (0.012) | (0.013) | (0.012) | |||||||
| BMI | 0.295 | 0.463 | < 0.001a | 0.299 | 0.459 | < 0.001a | |||
| (0.109) | (0.111) | ||||||||
| WC | -0.026 | 0.824 | -0.034 | 0.774 | |||||
| (0.016) | (0.017) | ||||||||
| W/H ratio | 0.145 | 0.247 | 0.136 | 0.288 | |||||
| (8.768) | (9.018) | ||||||||
Model 1 is unadjusted model. Model 2 is Model 1 adjusted for sex and age. Model 3 is Model 2 adjust for body mass index. Statistical significance:
P < 0.001. β: Standardized coefficient; SE: Estimated error; R2: Correction coefficient; LFC: Liver fat content; HbA1c: Glycosylated hemoglobin; Tri: Triglyceride; BMI: Body mass index; WC: Waist circumference; W/H ratio: Waist-to-hip ratio.
DISCUSSION
In recent years, the prevalence of NAFLD in young adults has been increasing at an alarming rate that parallels with the global epidemic of weight gain and obesity. The prevalence of obesity in young adult is double that of younger ages[8]. Various studies have stated the close relationships between obesity, dyslipidemia, insulin resistance, and NAFLD[23,24]. MRI has proven to be a powerful imaging tool for liver cirrhosis diagnosis[25], and is known for its ability to non-invasively and accurately quantify liver fat using the 1H MRS technique, which is suitable for longitudinal follow-ups when compared to liver biopsy. Liver biopsies are the gold standard, but are an invasive method.
The results of this study confirmed once again the association between BMI and LFC, the higher risk of dyslipidemia, the probability of insulin resistance, and the prospect of metabolic disease in young adults.
The highlight of this study is that LFC in the OW/OB group is higher when compared to the control group, even if both groups were revealed to be healthy. This prevalent rate is consistent with earlier findings where 57.4% of NAFLD subjects in young adults also had high BMI[7,26]. This tendency should also be considered with a higher prevalence of dyslipidemia, prediabetes, and hyperglycemia among subjects with LFC > 5.56%. In accordance with the present results, previous studies have demonstrated that the risk for dyslipidemia starts to increase progressively with a BMI over 21 kg/m2 and LDL and Tri levels are used to evaluate the risk for coronary artery disease[27].
A new important finding is that the biochemical and anthropographic markers associated with LFC are significantly different between the OW/OB group and the control group. Among the blood lipid markers, Tri and LDL were found to be statistically higher, and HDL was found to be statistically lower when compared to the control group. However, no significant differences were found for Cho, even though the Cho in the OW/OB subjects had increased slightly with almost half of the control group having dyslipidemia. This could be explained by the fact that the two characteristics of the subjects in this age group were that they were exposed to high caloric, low fiber “ready-to-eat” foods, consumed sugary beverages, and had low physical activity. It can be expected that these effects can change the Cho levels in blood[6,28].
The Pearson correlation analysis showed moderate correlation of BMI and LFC and mild correlation with W/H ratio and WC. The association of BMI and LFC was additionally confirmed by multilinearity regression analysis as a significant independent variable after being adjusted for age, sex, and other anthropometric variables. This outcome is dissimilar with previous studies that proposed that W/H ratio can be used as a tool to predict the risks of liver cirrhosis and NAFLD in place of BMI[29,30]. A possible explanation is the difference in fat accumulation mechanisms and that weight gain is the main pathogenic mechanism of liver fat accumulation in this age group as was previously proposed by Van Wagner et al[31].
HbA1c and FG are also found to be statistically different between the two groups with a slightly positive correlation with LFC. However, only HbA1c is a statistically significant independent variable for LFC after adjusting for age and sex. This result may suggest that HbA1c is a better tool for reflecting the NAFLD effects on insulin resistance than the FG. This assumption is reflected in other research done on the association between HbA1c and NALFD in non-diabetic subjects[32] and on the association of prediabetes characteristics independent of total body fat in obese adolescents with high liver fat assessment by MRI[23]. Elevated HbA1c further confirms the high risk of cardiovascular disease and insulin resistance in overweight and obese young adults.
This study has a few limitations such as the high prevalence of dyslipidemia in the control group that may be caused by the sample characteristics. This group being mostly comprised of young adults engaged in academic studies and whose exercise levels were determined by a questionnaire. There may have been a potential for over reporting by the subjects. A second limitation is that LDL was calculated by an adjustable ratio equation and was not measured directly by biochemical assessment.
To our knowledge, this is the first study on the topic of non-invasive assessment of LFC by 1H MRS technique in healthy young adults without any complications or earlier diagnoses of chronic disease. The high prevalence of NAFLD (LFC > 5.56%) contributed to the impact of silent chronic disease in young adults that had become obese. Although the current study is based on a small sample of subjects, the findings have drawn together various interesting subjects on the effects of BMI, how it contributes to LFC, and how it is a high risk factor of metabolic syndrome in young adults. Previous studies on young adults after a 39 year follow-up has shown that an obese young adult who remained obese throughout their adult life increased their risk of developing severe liver disease[26]. This study suggested a role of BMI in increasing LFC and as a factor in higher NAFLD risk for overweight and obese young adults. The importance of weight control as the primary risk prevention and control of NAFLD and many metabolic syndromes has been proposed. However, this study may reveal the importance in raising awareness for early prevention before NAFLD transitions into chronic liver disease later in adulthood. Future studies on this topic are therefore recommended as young adults are at a high risk for developing severe liver disease. Further, implications of these findings may be forthcoming in future research using longitudinal studies with larger groups of subjects.
In conclusion, it is proposed that the prevalence of high LFC in the OW/OB group can be the result of weight gain and obesity, and may be a leading pathogenic mechanism of liver fat accumulation in young adults. This current study demonstrated the importance of BMI as a tool for the prevention and control of NAFLD and metabolic syndrome in young adults.
ARTICLE HIGHLIGHTS
Research background
In recent years, the prevalence of non-alcoholic fatty liver disease (NAFLD) in young adults has been increasing at an alarming rate that parallels the global epidemic of weight gain and obesity. NAFLD in young adults is a topic that has received little recognition, yet this age group is the most likely to gain weight and develop obesity from their diet and lifestyle as they are transitioning into adulthood. However, despite the growing public health concern about obesity and NAFLD in young adults, necessary information addressing the effects of obesity and NAFLD pathogenesis in this age group is lacking.
Research motivation
NAFLD is a chronic liver disease that is one of the most common health problems among young adults. We aim to identify the effects of obesity on liver fat content (LFC) and health in this age group. This information is crucial for primary prevention and a better understanding of NAFLD pathogenesis in young adults.
Research objectives
The aim of this present study is to assess the association between LFC by proton magnetic resonance spectroscopy (1H MRS) technique. Using biochemical tests, the total cholesterol (Cho), low-density lipoproteins (LDL), high-density lipoproteins (HDL), fasting plasma glucose (FG), glycosylated hemoglobin (HbA1c), and being overweight/obese (OW/OB) will be determined.
Research methods
A total of 78 healthy subjects in the young adult age group (19-30 years old) participated in this study. A control group was made up of 39 healthy subjects, and the experimental group was made up of 39 overweight or obese (OW/OB) subjects. We performed the liver fat assessment by 1H MRS technique on MRI 1.5 T that was calculated into LFC. Intravenous blood was drawn for biochemical analysis. The test focused on Cho, HDL, VLDL, TG, FG, and HbA1c. The waist circumference (WC) and hip circumference (HC) of each subject was measured, and the waist-to-hip ratio (W/H ratio) was calculated.
Research results
LFC from the OW/OB group (8.1% ± 1.0%) was found to be statistically higher when compared to the control group (2.7% ± 0.2%) (P < 0.001). Additionally, 48.7% of subjects in the OW/OB group had LFC > 5.56%, which is considered to be a cut off point for NAFLD. The OW/OB group reported statistically higher BMI, LFC, WC, HC, FG, Tri, LDL, HbA1c, and statistically lower HDL. Cho was increased in the OW/OB group compared to the control group, but was not statistically significant. The association of BMI and LFC was additionally confirmed by multilinearity regression analysis as a significant independent variable after being adjusted for age and sex (P < 0.001). These findings indicated that BMI is a sensitive marker for LFC in young adults.
Research conclusions
It is proposed that the prevalence of high LFC in the OW/OB group can be the result of weight gain and obesity, and may be a leading pathogenic mechanism of liver fat accumulation in young adults. Moreover, high BMI is a risk factor for metabolic syndrome in young adults. This current study demonstrated the importance of weight control as a tool for the prevention and control of NAFLD and metabolic syndrome in young adults.
Research perspectives
Further study on this topic may require larger groups of subjects, and should also investigate the alteration of LFC and BMI throughout the adult years as a longitudinal study.
Footnotes
Institutional review board statement: Approved by the Ethics Committee of the Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai, Thailand (AMSEC-61EX-016).
Informed consent statement: All study participants provided informed written consent prior to study enrollment.
Conflict-of-interest statement: The authors declare no conflicts of interest.
Manuscript source: Unsolicited manuscript
Peer-review started: June 11, 2018
First decision: July 11, 2018
Article in press: August 21, 2018
Specialty type: Gastroenterology and hepatology
Country of origin: Thailand
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): 0
Grade C (Good): C, C
Grade D (Fair): 0
Grade E (Poor): 0
P- Reviewer: Metin U, Pallav K S- Editor: Cui LJ L- Editor: Filipodia E- Editor: Tan WW
Contributor Information
Duanghathai Pasanta, Department of Radiologic Technology, Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai 50200, Thailand.
Montree Tungjai, Department of Radiologic Technology, Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai 50200, Thailand.
Sirirat Chancharunee, Department of Chemistry, Faculty of Science, Chiang Mai University, Chiang Mai 50200, Thailand.
Warayuth Sajomsang, National Nanotechnology Center, National Science and Technology Development Agency, Thailand Science Park, Pathum Thani 12120, Thailand.
Suchart Kothan, Department of Radiologic Technology, Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai 50200, Thailand. suchart.kothan@cmu.ac.th.
References
- 1.Fabbrini E, Sullivan S, Klein S. Obesity and nonalcoholic fatty liver disease: biochemical, metabolic, and clinical implications. Hepatology. 2010;51:679–689. doi: 10.1002/hep.23280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Loomis AK, Kabadi S, Preiss D, Hyde C, Bonato V, St Louis M, Desai J, Gill JM, Welsh P, Waterworth D, et al. Body Mass Index and Risk of Nonalcoholic Fatty Liver Disease: Two Electronic Health Record Prospective Studies. J Clin Endocrinol Metab. 2016;101:945–952. doi: 10.1210/jc.2015-3444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rao W, Su Y, Yang G, Ma Y, Liu R, Zhang S, Wang S, Fu Y, Kou C, Yu Y, et al. Cross-Sectional Associations between Body Mass Index and Hyperlipidemia among Adults in Northeastern China. Int J Environ Res Public Health. 2016;13 doi: 10.3390/ijerph13050516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lonardo A, Ballestri S, Guaraldi G, Nascimbeni F, Romagnoli D, Zona S, Targher G. Fatty liver is associated with an increased risk of diabetes and cardiovascular disease - Evidence from three different disease models: NAFLD, HCV and HIV. World J Gastroenterol. 2016;22:9674–9693. doi: 10.3748/wjg.v22.i44.9674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. doi: 10.1002/hep.28431. [DOI] [PubMed] [Google Scholar]
- 6.Poobalan A, Aucott L. Obesity Among Young Adults in Developing Countries: A Systematic Overview. Curr Obes Rep. 2016;5:2–13. doi: 10.1007/s13679-016-0187-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mrad RA, Merjaneh N, Mubarak G, Lopez R, Zein NN, Alkhouri N. The increasing burden of nonalcoholic fatty liver disease among young adults in the United States: A growing epidemic. Hepatology. 2016;64:1386–1387. doi: 10.1002/hep.28555. [DOI] [PubMed] [Google Scholar]
- 8.Dietz WH. Obesity and Excessive Weight Gain in Young Adults: New Targets for Prevention. JAMA. 2017;318:241–242. doi: 10.1001/jama.2017.6119. [DOI] [PubMed] [Google Scholar]
- 9.Doycheva I, Watt KD, Alkhouri N. Nonalcoholic fatty liver disease in adolescents and young adults: The next frontier in the epidemic. Hepatology. 2017;65:2100–2109. doi: 10.1002/hep.29068. [DOI] [PubMed] [Google Scholar]
- 10.Reeder SB, Cruite I, Hamilton G, Sirlin CB. Quantitative Assessment of Liver Fat with Magnetic Resonance Imaging and Spectroscopy. J Magn Reson Imaging. 2011;34:spcone. doi: 10.1002/jmri.22580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Graffy PM, Pickhardt PJ. Quantification of hepatic and visceral fat by CT and MR imaging: relevance to the obesity epidemic, metabolic syndrome and NAFLD. Br J Radiol. 2016;89:20151024. doi: 10.1259/bjr.20151024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452. [PubMed] [Google Scholar]
- 13.Naressi A, Couturier C, Devos JM, Janssen M, Mangeat C, de Beer R, Graveron-Demilly D. Java-based graphical user interface for the MRUI quantitation package. MAGMA. 2001;12:141–152. doi: 10.1007/BF02668096. [DOI] [PubMed] [Google Scholar]
- 14.Stefan D, Cesare FD, Andrasescu A, Popa E, Lazariev A, Vescovo E, Strbak O, Williams S, Starcuk Z, Cabanas M, et al. Quantitation of magnetic resonance spectroscopy signals: the jMRUI software package. Meas Sci Technol. 2009;20:104035. [Google Scholar]
- 15.Vanhamme L, van den Boogaart A, Van Huffel S. Improved method for accurate and efficient quantification of MRS data with use of prior knowledge. J Magn Reson. 1997;129:35–43. doi: 10.1006/jmre.1997.1244. [DOI] [PubMed] [Google Scholar]
- 16.Hamilton G, Yokoo T, Bydder M, Cruite I, Schroeder ME, Sirlin CB, Middleton MS. In vivo characterization of the liver fat ¹H MR spectrum. NMR Biomed. 2011;24:784–790. doi: 10.1002/nbm.1622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Longo R, Pollesello P, Ricci C, Masutti F, Kvam BJ, Bercich L, Crocè LS, Grigolato P, Paoletti S, de Bernard B. Proton MR spectroscopy in quantitative in vivo determination of fat content in human liver steatosis. J Magn Reson Imaging. 1995;5:281–285. doi: 10.1002/jmri.1880050311. [DOI] [PubMed] [Google Scholar]
- 18.Szczepaniak LS, Nurenberg P, Leonard D, Browning JD, Reingold JS, Grundy S, Hobbs HH, Dobbins RL. Magnetic resonance spectroscopy to measure hepatic triglyceride content: prevalence of hepatic steatosis in the general population. Am J Physiol Endocrinol Metab. 2005;288:E462–E468. doi: 10.1152/ajpendo.00064.2004. [DOI] [PubMed] [Google Scholar]
- 19.Martin SS, Blaha MJ, Elshazly MB, Toth PP, Kwiterovich PO, Blumenthal RS, Jones SR. Comparison of a novel method vs the Friedewald equation for estimating low-density lipoprotein cholesterol levels from the standard lipid profile. JAMA. 2013;310:2061–2068. doi: 10.1001/jama.2013.280532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sathiyakumar V, Park J, Golozar A, Lazo M, Quispe R, Guallar E, Blumenthal RS, Jones SR, Martin SS. Fasting Versus Nonfasting and Low-Density Lipoprotein Cholesterol Accuracy. Circulation. 2018;137:10–19. doi: 10.1161/CIRCULATIONAHA.117.030677. [DOI] [PubMed] [Google Scholar]
- 21.Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III) JAMA. 2001;285:2486–2497. doi: 10.1001/jama.285.19.2486. [DOI] [PubMed] [Google Scholar]
- 22.Introduction: Standards of Medical Care in Diabetes-2018. Diabetes Care. 2018;41:S1–S2. doi: 10.2337/dc18-Sint01. [DOI] [PubMed] [Google Scholar]
- 23.Cali AM, De Oliveira AM, Kim H, Chen S, Reyes-Mugica M, Escalera S, Dziura J, Taksali SE, Kursawe R, Shaw M, et al. Glucose dysregulation and hepatic steatosis in obese adolescents: is there a link? Hepatology. 2009;49:1896–1903. doi: 10.1002/hep.22858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Corbin KD, Zeisel SH. Choline metabolism provides novel insights into nonalcoholic fatty liver disease and its progression. Curr Opin Gastroenterol. 2012;28:159–165. doi: 10.1097/MOG.0b013e32834e7b4b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Numminen K, Tervahartiala P, Halavaara J, Isoniemi H, Höckerstedt K. Non-invasive diagnosis of liver cirrhosis: magnetic resonance imaging presents special features. Scand J Gastroenterol. 2005;40:76–82. doi: 10.1080/00365520410009384. [DOI] [PubMed] [Google Scholar]
- 26.Hagström H, Stål P, Hultcrantz R, Hemmingsson T, Andreasson A. Overweight in late adolescence predicts development of severe liver disease later in life: A 39years follow-up study. J Hepatol. 2016;65:363–368. doi: 10.1016/j.jhep.2016.03.019. [DOI] [PubMed] [Google Scholar]
- 27.Kopelman P. Health risks associated with overweight and obesity. Obes Rev. 2007;8 Suppl 1:13–17. doi: 10.1111/j.1467-789X.2007.00311.x. [DOI] [PubMed] [Google Scholar]
- 28.Zelber-Sagi S, Godos J, Salomone F. Lifestyle changes for the treatment of nonalcoholic fatty liver disease: a review of observational studies and intervention trials. Therap Adv Gastroenterol. 2016;9:392–407. doi: 10.1177/1756283X16638830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Schult A, Mehlig K, Björkelund C, Wallerstedt S, Kaczynski J. Waist-to-hip ratio but not body mass index predicts liver cirrhosis in women. Scand J Gastroenterol. 2018;53:212–217. doi: 10.1080/00365521.2017.1420219. [DOI] [PubMed] [Google Scholar]
- 30.Zheng RD, Chen ZR, Chen JN, Lu YH, Chen J. Role of Body Mass Index, Waist-to-Height and Waist-to-Hip Ratio in Prediction of Nonalcoholic Fatty Liver Disease. Gastroenterol Res Pract. 2012;2012:362147. doi: 10.1155/2012/362147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.VanWagner LB, Khan SS, Ning H, Siddique J, Lewis CE, Carr JJ, Vos MB, Speliotes E, Terrault NA, Rinella ME, et al. Body mass index trajectories in young adulthood predict non-alcoholic fatty liver disease in middle age: The CARDIA cohort study. Liver Int. 2018;38:706–714. doi: 10.1111/liv.13603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Bae JC, Cho YK, Lee WY, Seo HI, Rhee EJ, Park SE, Park CY, Oh KW, Sung KC, Kim BI. Impact of nonalcoholic fatty liver disease on insulin resistance in relation to HbA1c levels in nondiabetic subjects. Am J Gastroenterol. 2010;105:2389–2395. doi: 10.1038/ajg.2010.275. [DOI] [PubMed] [Google Scholar]