

Endoscopic tattooing directly into large dysplastic lesions is often performed for lesion identification before EMR or endoscopic submucosal dissection (ESD). Several case reports have demonstrated the difficulty of attempting endoscopic resection of previously tattooed lesions, primarily because of tattoo-induced submucosal fibrosis, inadequate lifting of the lesion, and obscuring of the dissection planes.1, 2, 3
Recently, the U.S. Food and Drug Administration approved a tissue retractor system (ORISE TRS; Boston Scientific Corp, Marlborough, Mass, USA) to be used in situations in which tissue manipulation is required independently of the endoscope (Fig. 1). It consists of an expandable nitinol-based retractor cage at its most distal end attached to an overtube that allows for insertion and removal of the endoscope without losing position in the colon. Two flexible channels run through the overtube and allow insertion of tissue graspers. Manipulation of these graspers can provide tension and improves visualization of the dissection plane. We describe the case of a patient who underwent successful ESD of a previously tattooed large fibrotic rectal lesion with the assistance of the novel tissue retractor system (Video 1, available online at www.VideoGIE.org).
Figure 1.
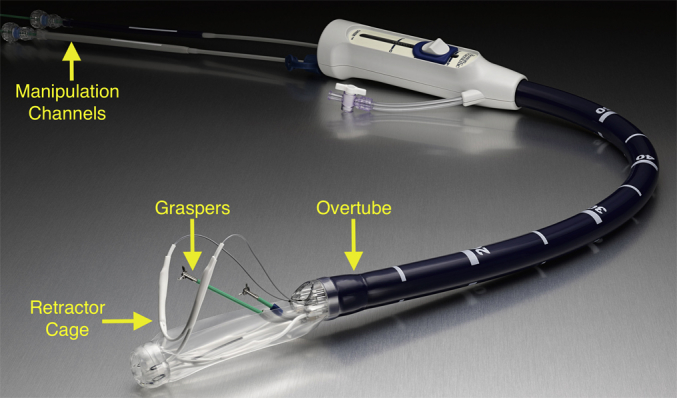
The tissue retractor system consists of a retractable cage attached to an overtube that allows for insertion and removal of the endoscope without losing position within the colon. There are 2 manipulation channels that run through the overtube and can allow insertion of graspers. When retracted, the cage provides stabilization within the colon, and graspers allow for the maximal tensile force needed to visualize the dissection plane.
A 50-year-old man who presented with rectal bleeding was found to have a 7-cm Laterally spreading lesion-granular type rectal mass during colonoscopy (Figs. 2 and 3). The lesion was tattooed directly with SPOT (GI Supply, Camp Hill, Pa, USA), and the patient was referred to our colorectal surgeons for possible surgical resection. Subsequent EUS demonstrated the lesion to be confined to the mucosa. Although prior biopsy specimens had shown tubulovillous adenoma, the presence of large nodules and depressed areas within the laterally spreading tumor brought up concerns that a covert invasive component might be present. Furthermore, the presence of tattoo within the lesion raised concerns that submucosal fibrosis was present and EMR would not be technically feasible. Therefore, a decision was made to pursue en bloc resection by ESD.
Figure 2.
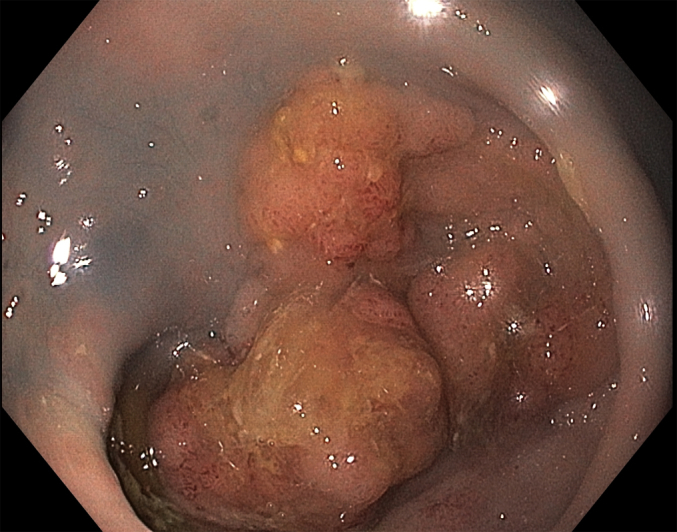
Bulky 7-cm laterally spreading rectal tumor with slightly irregular vessel pattern and nodularity with evidence of previous tattoo into and around the lesion.
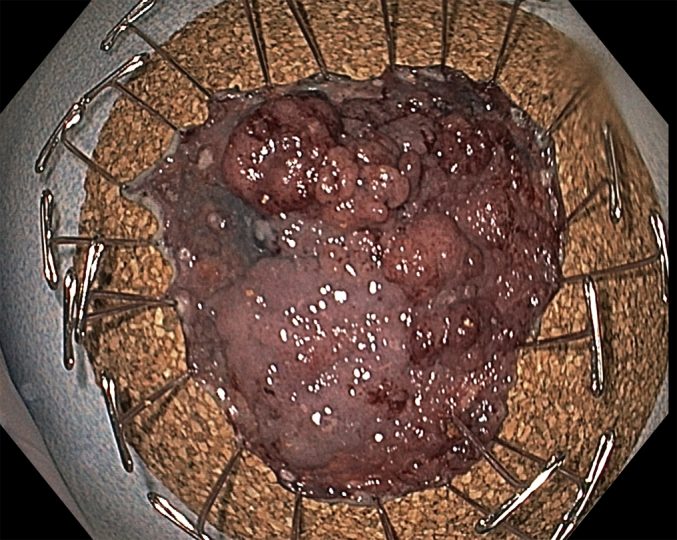
Figure 3.
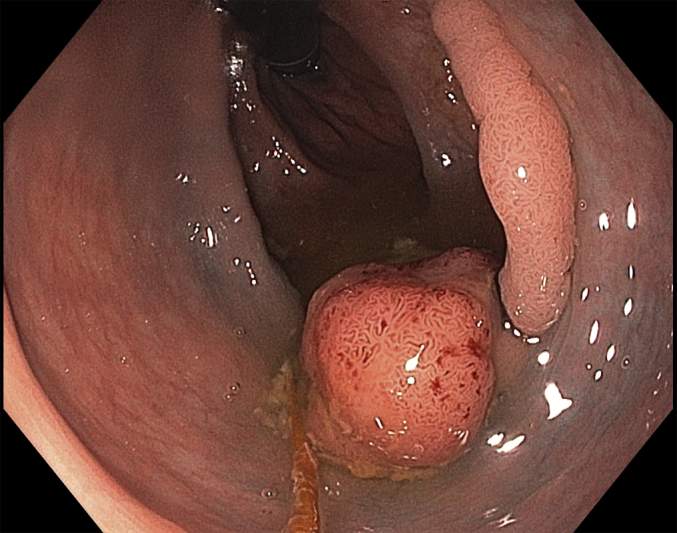
Lesion seen in the retroflexed view.
Thermocautery marks were placed around the lesion edge (Fig. 4). A full circumferential incision around the lesion was made with the Hybrid I type knife (ERBE USA, Marietta, Ga, USA) with alternating injections of normal saline solution/methylene blue mixture into the submucosa and mucosal cutting with the use of Endo Cut Q, effect 3, duration 1, interval 1. The ORISE TRS was positioned over the lesion. The lesion edge was then grasped with the dedicated grasper to provide traction (Fig. 5), and submucosal dissection was begun. Most of the dissection was performed with the Endo Cut Q setting. In areas where no fibrosis was present and adequate submucosal lift was achieved, dissection was carried out with the use of forced coagulation, effect 2, 50 Watts. Hemostasis was accomplished with the Coag grasper (Olympus America, Center Valley, Pa, USA) and the use of soft coagulating current 80 W, effect 5. During submucosal dissection, a very densely fibrotic area was encountered. The tissue layers were obliterated, and visualization was very difficult because of the jet-black discoloration from the prior tattoo (Fig. 6). Triangulation from the ORISE device (Fig. 7) and repeated submucosal injections of normal saline solution/methylene blue facilitated dissection through the area in a safe and efficient manner. The mass was successfully resected en bloc (Figs. 8 and 9), and the patient was discharged home. At the 30-day follow-up visit, no adverse events had occurred. Histopathologic analysis revealed tubulovillous adenoma with high-grade dysplasia and negative lateral and deep margins.
Figure 4.
Circumferential marking before incision is begun.
Figure 5.
Use of the grasping device through the tissue retractor system allows for tissue manipulation and adequate traction.
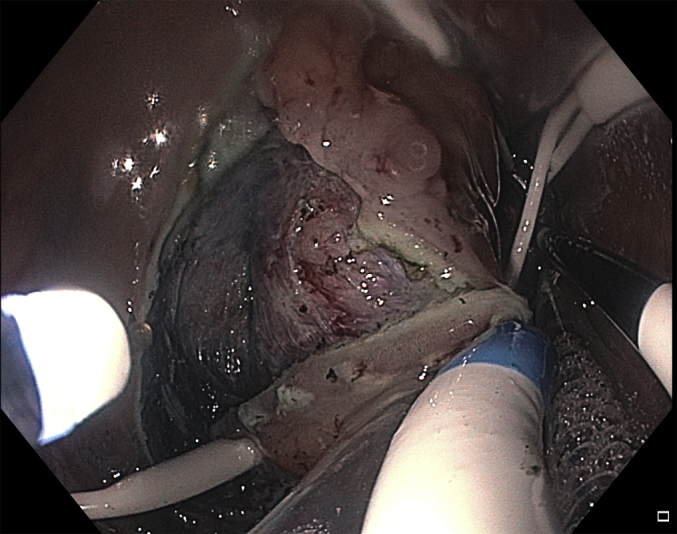
Figure 6.
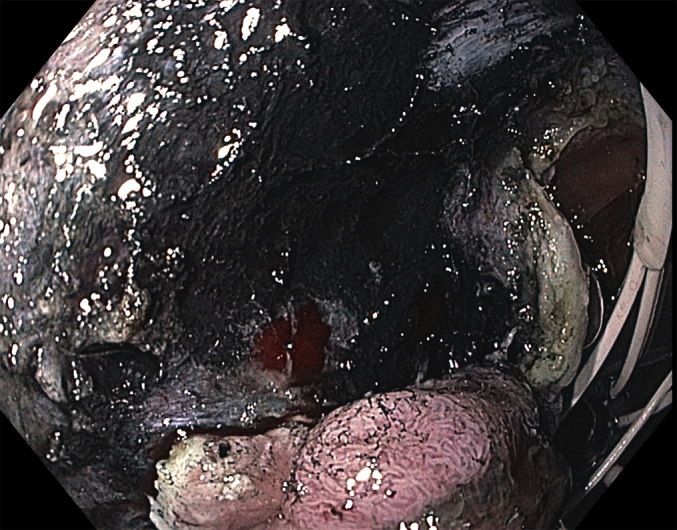
Significant tattoo material with corresponding fibrosis, limiting visibility of dissection field.
Figure 7.
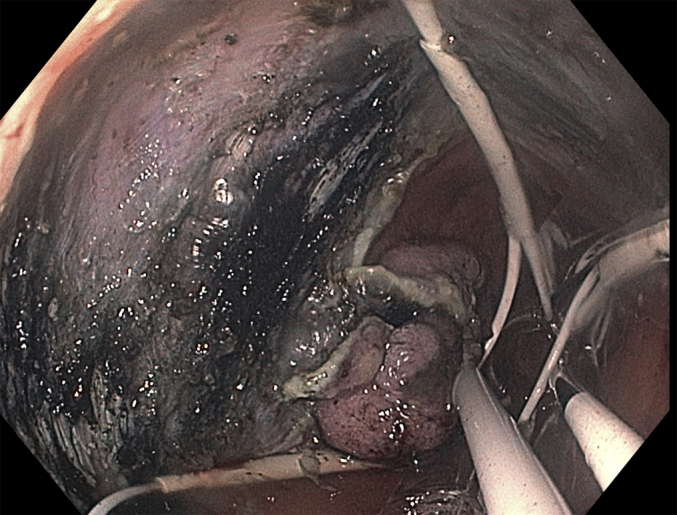
Triangulation of tissue retraction device with associated tissue grasper to allow for maximal tension and safe dissection through fibrotic tissue.
Figure 8.
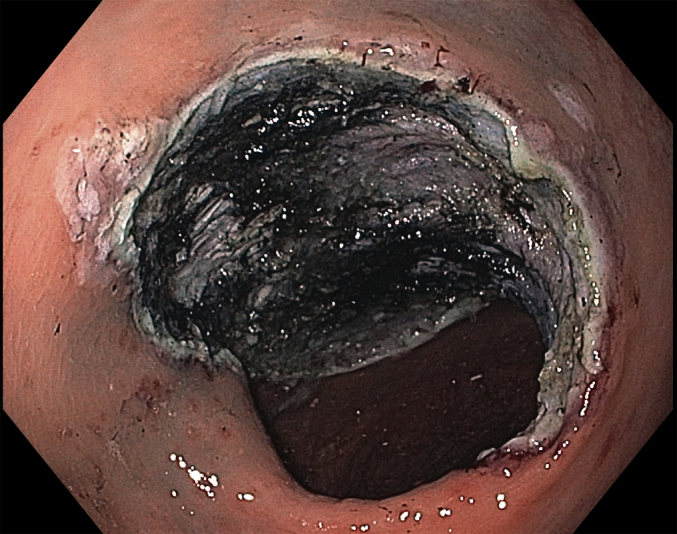
Endoscopic image after complete endoscopic submucosal dissection.
Figure 9.
Final en bloc resection specimen; histopathologic analysis revealed tubulovillous adenoma with high-grade dysplasia and negative deep and lateral margins.
This case illustrates the technical challenges that an endoscopist can encounter when attempting to perform ESD of a previously tattooed lesion. If tattoo marking is to be performed, it should be done just proximal or distal to the lesion but never directly into the lesion itself.4 The ORISE device can facilitate ESD in these scenarios by supplying constant tension and allowing for effective visualization of the dissection field.
Disclosure
Dr Yang and Dr Draganov are consultants for Boston Scientific. The other author disclosed no financial relationships relevant to this publication.
Supplementary data
Tissue retractor system-assisted endoscopic submucosal dissection of a rectal tumor with tattoo-induced fibrosis.
References
- 1.Chiba H., Tachikawa J., Kurihara D. Successful endoscopic submucosal dissection of colon cancer with severe fibrosis after tattooing. Clin J Gastroenterol. 2017;10:426. doi: 10.1007/s12328-017-0770-z. [DOI] [PubMed] [Google Scholar]
- 2.Ono S., Fujishiro M., Goto O. Endoscopic submucosal dissection for colonic laterally spreading tumors is difficult after target tattooing. Gastrointest Endosc. 2009;69:763–766. doi: 10.1016/j.gie.2008.08.024. [DOI] [PubMed] [Google Scholar]
- 3.Lane K.L., Vallera R., Washington K. Endoscopic tattoo agents in the colon: tissue responses and clinical implications. Am J Surg Pathol. 1996;20:1266–1270. doi: 10.1097/00000478-199610000-00013. [DOI] [PubMed] [Google Scholar]
- 4.Rex D.K. The appropriate use and techniques of tattooing in the colon. Gastroenterol Hepatol. 2018;14:314–317. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Tissue retractor system-assisted endoscopic submucosal dissection of a rectal tumor with tattoo-induced fibrosis.