

Abstract
Background:
Chronic caregiving stress may accelerate biological aging; however, the ability to integrate the meaning of caregiving through self-awareness, adaptation, and growth can buffer the negative effects of stress. Narrative researchers have shown that people who coherently integrate difficult experiences into their life story tend to have better mental health, but no prior study has examined the prospective association between narrative identity and biological indicators, such as telomere length. We tested whether narrative identity might be prospectively associated with resilience to long-term parenting stress, depressive symptoms, and protection from telomere shortening, especially among caregivers.
Methods:
We conducted a semi-structured interview about parenting and quantified narrative themes by applying well-validated, standardized coding systems with high interrater reliability among 88 mothers: 32 “caregivers” (mothers with a child diagnosed with an autism spectrum disorder), and 56 “controls” (mothers with a neurotypical child). To assess longitudinal changes, we measured mental health (parenting stress [PS], depressive symptoms [DS]) and leukocyte telomere length [LTL], a biomarker of aging, at baseline and again 18 months later. We examined whether narrative identity themes were related to these outcomes and whether associations differed across caregivers versus controls.
Results:
Caregivers exhibited significantly higher basal levels of PS and DS relative to controls (all p’s<.05), but no significant difference in LTL (p>.05). Caregivers rated higher in the narrative theme of integration showed healthier future 18-month trajectories in PS [B=−0.832, 99% CI [−1.315, −0.155], p<.01) and LTL (B=1.193, 99% CI [0.526, 2.130], p<.01), but no differences in depressive symptoms (p>.05), adjusting for age and antidepressant use. Analyses examining affective themes in caregiver narratives did not demonstrate significant associations. Narrative themes did not predict outcomes in controls.
Conclusions:
The data suggest that narratives reflecting coherent integration, but not necessarily affect, prospectively relate to psychological and biological stress resilience. Maternal caregivers’ ability to tell an integrated story of their parenting experiences forecasts lower parenting stress and telomere shortening over time. This study suggests the possibility that helping individuals better integrate the meaning of stressful experiences, but not necessarily to affectively redeem them, may constitute a potential novel target for intervention among chronically stressed populations such as caregivers.
Keywords: Narrative identity, leukocyte telomere length, stress resilience, cellular aging, parenting stress
Introduction
Stress resilience can be defined as the ability to “bounce back” after exposure to a major stressor. Meta-analyses predicting symptoms of psychological distress have reported that most people mostly recover within a few years of an acute stressful event, and this recovery process has been defined as a ‘resilient trajectory’ (Galatzer-Levy, Huang, & Bonanno, 2018). However, we need to better identify and measure the psychological factors that best predict a resilient trajectory following exposure to chronic stress, such as continuous caring for a loved one with a disability or chronic disease. Although modifiable psychological factors such as coping strategies, self-efficacy, and social support each predict a small amount of variance in resilience trajectories, they do not tend to reliably predict the majority of psychological or biomarker health outcomes (Bonanno & Diminich, 2013). Better understanding of the modifiable psychological factors that predict more resilient mental and physiological trajectories would allow for the development of interventions targeting reductions in the adverse effects of chronic stress on health.
Narrative identity is the internalized, evolving story of the self that integrates the reconstructed past, perceived present, and imagined future (McAdams, 2001; McAdams & McLean, 2013; Singer, 2004). Scholars working in personality psychology have developed a set of tools for conceptualizing, operationalizing, and analyzing the how individuals psychologically construct the narrative of their life, termed narrative identity (Adler et al., 2017; Hammack, 2008; McAdams, 2001; McAdams & McLean, 2013; Singer, 2004). Narrative identity confers a sense of unity and purpose to the self (McAdams, 2001) and may provide the psychological foundation that shapes how one processes stressor exposures as they occur (Adler et al., 2015). When individuals process stressor exposures as threats or challenges to personal identity, this can impact many aspects of their lives and in so doing can exert “biographical disruption” (Bury, 1982). Individual differences in the construction of narrative identity are associated with different psychological well-being outcomes, both concurrently and prospectively (Adler, Lodi-Smith, Philippe, & Houle, 2016).
A robust literature demonstrates that narrative identity correlates with and predicts psychological health, above and beyond demographic and dispositional personality trait variables (Adler et al., 2016). For example, in a longitudinal study of parents of children with Down Syndrome, parents who constructed a coherent narrative identity, who tried to make sense of their situation, whose respective stories foreshadowed an unexpected turn, and who narrated a happy ending to their parental transition, reported better psychological well-being two years later (King, Scollon, Ramsey, & Williams, 2000). Individual differences in narrative identity have also demonstrated prospective positive associations with desistence from alcohol among alcoholics (Dunlop & Tracy, 2013), symptomatic improvement among psychotherapy clients (Adler, 2012), enhanced psychological well-being in the wake of a major physical illness diagnoses (Adler et al., 2015), and increased life satisfaction among mid-life adults following major life-changing decisions (Bauer, McAdams, & Sakaeda, 2005). However, no prior study has reported on associations between individual differences in narrative identity and biological health or aging factors.
Caregiving is a unique type of ongoing stressor which may require shifts in identity (Yu, Cheng, & Wang, 2018). In a review of resilient trajectories in the context of caregiving, the positive aspects of caregiving were multidimensional and included sense of personal growth and purpose in life (Yu et al., 2018). Examining narrative identities is conducive to assessing this type of meta-appraisal of the caregiving experience. Caregiving for a child with an autism spectrum disorder (ASD) is a chronic situation that can increase vulnerability to stressor exposures. For example, maternal caregiving is associated with more negative daily interactions with one’s child, shifts in bone marrow-derived immune cell populations with implications for inflammation and repair, and accelerated biological aging (Aschbacher et al., 2017; Epel et al., 2004). Indeed, caregiving for a child with an ASD is significantly more stressful than parenting a neurotypical child (Hayes & Watson, 2013). Similarly, exposure to the chronic stress of caregiving for an individual with dementia has been associated with shorter telomeres (Damjanovic et al., 2007), and in parental caregivers, greater perceived stress was associated with shorter telomeres (Epel et al., 2004).
The present study
In the present analyses, we examined longitudinal associations between narrative identity themes and a measure of biological aging among mothers of children with an ASD (“caregivers”) and mothers of neurotypical children (“controls”). Specifically, we aimed to identify narrative identity themes that might promote resilient trajectories in terms of leukocyte telomere length and mental health over an 18-month timeframe. We indexed biological health as leukocyte telomere length. We indexed mental health using measures of perceived parenting stress and depressive symptoms. We assessed narrative identity themes in transcripts of structured interviews with mothers (caregivers and controls) focused on their parenting experiences and the application of well-validated coding processes (Adler et al., 2017). We explicitly designed these interviews to elicit examples of both rewarding and challenging experiences associated with parenting in order to obtain a full range of affective experiences as well as reflections on the processes of integration and meaning-making.
We examined two larger dimensions of narrative identity as potential pathways towards resilient trajectories. The first was an affective journey of one’s life experiences. Such journeys often tend to follow one of two dominant thematic trajectories; the negative experience is either seen as the seed for later positive changes (theme of redemption sequences), or the negative experience is construed as contaminating and ruining an otherwise positive episode (theme of contamination sequences’, McAdams, Reynolds, Lewis, Patten, & Bowman, 2001). All lives have positive and negative elements, so the narration of redemption or contamination sequences is a matter of where one draws connections and parses the chapter breaks in one’s story (McAdams et al., 2001). These affective themes have been widely examined in the literature on narrative identity and its association with psychological health (Adler et al., 2016; McAdams & McLean, 2013). The second dimension was a growth journey, which measures the coherent integration of challenging experiences into one’s broader identity (theme of integration) and the general effort to make meaning from one’s situation that would inform future choices (theme of meaning-making). The search for coherence and meaning is a fundamental human process (e.g., Frankl, 1985; Park, 2010), yet not always pleasant (Frazier et al., 2009). Hence, the extent to which people choose to emphasize it in their life stories represents a narrative individual difference, one that has also received extensive empirical attention (e.g., Adler et al., 2016).
Prior work demonstrates the heightened relevance of narrative identity for psychological wellbeing in the context of new life challenges (Adler et al., 2015). Thus, we hypothesized that narrative identity themes would more strongly predict mental health outcomes among caregivers than controls, and also explored whether narrative identity themes would better predict telomere shortening, as a marker of biological aging, more so among caregivers than controls. Although no prior work has examined the associations between narrative identity and biomarkers, the literature to date examining narrative identity and psychological health suggests that greater redemption, integration, and meaning-making may be associated with better outcomes (here, lesser parenting stress and depressive symptoms, and slower biological aging), whereas greater contamination may be associated with worse outcomes (here, greater parenting stress and depressive symptoms, and faster telomere shortening).
Method
Participants
Data were collected as part of a larger study on maternal caregiver stress and cellular aging (Aschbacher et al., 2017; Prather et al., 2015). Participants were 88 mothers (32 caregiving mothers with a child diagnosed with an autism spectrum disorder (ASD) and 56 controls, mothers with a neurotypical child) living in the San Francisco Bay area who were recruited through parenting publications, mailings, social media, local schools, child development centers, and (for caregivers) the University of California, San Francisco, Sensory Neurodevelopment and Autism Program. Eligible mothers were non-smokers between 20 and 50 years of age and who had at least one child between the ages of 2 and 16 years old. Inclusion criteria for mothers in the caregiver group included caring for a child diagnosed with an ASD (e.g., autism, Asperger syndrome, or a pervasive developmental disorder not otherwise specified). We excluded caregivers if their scores on the Perceived Stress Scale (PSS; S. Cohen, Kamarck, & Mermelstein, 1983) were below 13 during the eligibility phone screen, to ensure a high-stress caregiver group. Inclusion criteria for mothers in the control group included caring for a neurotypical child without any chronic disease. We excluded control mothers if their PSS scores were 19 or higher during the eligibility phone screen, to ensure a low-stress control group. The mean PSS score for women in nationally representative samples is roughly 16 (S. Cohen & Janicki-Deverts, 2012), and we permitted an overlap in PSS scores for the two groups to reduce longitudinal statistical regression to the mean (see Aschbacher et al., 2017 for details).
Additional exclusion criteria for all potential participants included major chronic diseases (e.g., diabetes, cardiovascular, autoimmune, history of stroke, brain injury, cancer, endocrine disorders), regular use of steroid prescription medications, or meeting criteria for current posttraumatic stress, bipolar, or eating disorders. At baseline, we did not exclude caregivers for antidepressant use, whereas we excluded control mothers for antidepressant use as this would suggest that their non-medicated levels of psychological distress could be higher than the permitted cutoff. Six caregiver and two control mothers began taking antidepressants after enrollment, and we elected to statistically control for this factor rather than exclude them from analyses. The Committee for Human Research at the University of California, San Francisco, approved of this research. We obtained written consent from all participants and compensated participants for their time.
Procedures
Participants completed self-report measures, blood draws, and weight assessments (using a digital scale) at baseline and 18 months later during in-person laboratory visits. Participants completed daily diary self-reports assessing physical activity for 7 days at each timepoint, baseline and 18 months later. At the baseline laboratory visit participants also completed a height measurement (using a wall-mounted Stadiometer) and an interview about their experience as parents. These interviews were recorded, transcribed, and coded by trained narrative coders.
Parenting interview.
Participants completed an in-person interview about their experience as parents at their baseline visit. We asked participants, “Can you take a few minutes and talk about some examples of particularly positive or rewarding experience you had parenting your child?” and “Can you describe some of the most stressful or challenging experiences you’ve had being a parent to your child?” For caregivers, we also asked about their experience when learning of their child’s ASD diagnosis, and how the condition has impacted their life (see Appendix A for complete interview questions). Participants had up to three minutes to answer each question. We recorded and subsequently transcribed all interview responses, verbatim.
Measures
Chronic stress, perceived global stress, and parenting stress.
We operationalized chronic stress using the objective criterion of caregiving for a child with ASD versus parenting a neurotypical child (caregiver versus control, respectively), as caregiving for a child with ASD is generally significantly more stressful than caring for a neurotypical child (Hayes & Watson, 2013). We coded group status as control (0) and caregiver (1).
For eligibility purposes (see participants) we quantified perceived global stress using the Perceived Stress Scale (PSS; S. Cohen et al., 1983), a standard 10-item questionnaire that assesses subjective perceptions of average stress levels over the previous month. PSS items reflect the perception that one’s life is uncontrollable, unpredictable and overwhelm one’s capacity to cope. Response options form a 5-point Likert scale ranging from 0 (never) to 4 (very often), and higher scores indicate greater perceived stress (Cronbach’s alpha for this sample at baseline: .87).
We quantified parenting stress using the 18-item Parental Stress Scale (Berry & Jones, 1995), in which all items are answered on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 {strongly agree). We reverse-coded all positive items before summing them such that higher scores indicate greater parenting stress (Cronbach’s alpha for this sample at baseline: .85).
Depressive symptoms.
We assessed depressive symptoms using the 30-item Inventory for Depressive Symptomatology (IDS), in which all equally weighted items are answered on a Likert scale from 0 to 3, with higher scores indicating more pathology (Cronbach’s alpha for this sample at baseline: .79; Rush, Gullion, Basco, Jarrett, & Trivedi, 1996).
Leukocyte Telomere length (LTL).
We quantified leukocyte telomere length (LTL) in whole blood cells at the UCSF Blackburn Laboratory. DNA was purified in batches using the QIAamp® DNA Mini Kit (QIAGEN, Hilden, Germany, Cat. Number 51104). The telomere length assay methodology uses PCR (polymerase chain reaction) and T/S (telomere/single copy gene) ratio units, as described in detail elsewhere (Lin, Epel, & Blackburn, 2012; Lin et al., 2010).
Narrative themes.
Two trained coders assessed each parenting interview prompt independently and achieved high inter-rater reliability (see reliability statistics for each theme, below). We averaged codes across the full interview for all themes described below.
Redemption.
Redemption sequences are recorded when participants include an affective shift in their story from negative to positive (McAdams et al., 2001). In redemption sequences, narratives that begin with emotions such as sadness, anger, or anxiety are transformed into emotions such as happiness or joy. For example, one participant said, “I have to say, I used to cry a lot and say, ‘why, why does this happen to us?’And one day, my daughter was writing a speech she was going to give at an autism conference and it said, ‘when my mom always asks ‘why does this happen to us’ I just want to tell my mom, ‘Why not? Because we are the perfect family for him [my brother]. ‘ And I think she’s right. I have to say it’s a gift.” In this excerpt, the participant describes an emotional shift from sadness to gratitude. Redemption sequences were scored as 0 (absence) and 1 (presence) in the response to each narrative prompt (McAdams et al., 2001). Two trained coders achieved high interrater reliability for redemption sequences (kappa = 0.75, percent agreement = 99%).
Contamination.
Contamination sequences are recorded when participants include an affective shift in their story from positive to negative (McAdams et al., 2001). In contamination sequences, narratives that begin with demonstrably positive emotions are overwhelmed, undermined, or ruined by negative ones. For example, one participant said, “Before you have children, you know, there’s this whole unexpected feeling of ‘what’s going to happen, what will I have, how many will I have,’ it’s like you’re looking to the future. But now it’s sad and I know I’m not having any more. So I guess in a way, you sort of see life not as a wide open space.” In this excerpt, the participant describes an emotional shift from hopeful anticipation to sad resignation. Contamination sequences were scored as 0 (absence) and 1 (presence) in the response to each narrative prompt (McAdams et al., 2001). Two trained coders achieved high inter-rater reliability for contamination sequences (kappa = 0.84, percent agreement = 95%).
Integration.
The theme of integration reflects the extent to which participants describe the specific ways in which a given story relates to their broader sense of self. In highly integrated stories, the narrator expresses the meaning of the recounted experiences within the context of their larger life story or as it fits into their identity. This theme is one component of a coding system used for assessing the psychological coherence of personal narratives (Baerger & McAdams, 1999). We selected this theme because it targets the participant’s effort to make sense of their experiences (the other components of this coding system tap participants’ orienting of the listener, their success in coherently structuring the chronological flow of the narrative, and their use of affective language to underscore the importance of the narrative). Integration was scored on a 4-point scale, with the lowest score representing the complete absence of integrative themes and the highest score representing elaborated and specific connections between the episode being narrated and the narrator’s sense of self (Adler, 2012). In this specific sample, examples of integration tended to include a better understanding of one’s identify in relation to their child. For example, one participant said, “I think parenting is the ultimate life test. And it’s a journey, and I mean I think we are evolving all the time. Cause no matter how many books you read, your kids will teach you more about yourself than you know. So I think the biggest thing that I’ve learned is: [parenting is] really a reflection of who you are in terms of how you are reacting to a child and whenever moment, whether it’s happy or sad, and really having to do a lot of work on understanding how I was raised and how that impacts how I’m raising our child.” In this excerpt, the participant extrapolates from the specific parenting experience she has just described (watching her preschooler improvise a song with completely different lyrics) to her broader sense of self. She notes how any given moment provides her an opportunity to reflect on how her own experiences from childhood impact the way she behaves as a parent and how this process is always evolving. Two trained coders achieved high inter-rater reliability for integration (ICC Case 2, Type 1 = 0.80).
Meaning-making.
The theme of meaning-making reflects the extent to which participants describe arriving at a sense of understanding about a specific experience. This sense of meaning may take various forms, and is scored along a continuum from specific lessons (low meaning), to vague meaning making, to specific insights that transcend the particulars of the experience (high meaning; McLean & Pratt, 2006). Unlike the theme of integration, the theme of meaning-making does not require participants to coherently weave a specific experience into their broader sense of self to receive the highest scores. High meaning-making must convey insights that extend beyond the immediate episode being narrated, but these insights may be about any topic. For example, one participant said, “I had to learn to separate a little bit, because you don’t want your kids to ever feel pain but what dreadful people would they become if they never had some emotional difficulty.” In this example, the narrator shifts from her story about a specific challenge her daughter experienced to a broader insight about the importance of emotional difficulty in raising flexible and empathic children. Meaning-making was scored on a 4-point scale, with the lowest score representing no meaning made and the highest score representing an explicit insight that transcends the particular episode (McLean & Pratt, 2006). Two trained coders achieved high inter-rater reliability for meaning-making (ICC Case 2, Type 1 = 0.81).
Candidate covariates.
Participants self-reported their age, educational attainment, race/ethnicity, household income, NSAID use, and antidepressant use. Household income was coded into two categories (above and below $150,000/year) as this was roughly a median point for this sample. At baseline, participants answered questions about their daily physical activity over the course of 7 days. We multiplied each activity’s Metabolic Equivalent of Task scores (METs1) by the number of minutes participants reported engaging in that activity that day to obtain total daily METs, which were then averaged across the week (see Aschbacher et al., 2017).
Analytic Plan
Data preparation, descriptive information, and correlations.
The narrative themes (redemption, contamination, integration, and meaning-making) exhibited right-skewed distributions, which were not improved by log-transformation; hence, we reported group medians and Mann U Whitney tests in Table 1 and conducted Spearman correlations to calculate the associations between narrative themes and other study variables (Table 2).
Table 1.
Descriptive information for caregivers and controls at baseline
| Caregivers | Controls | |
|---|---|---|
| Demographic Characteristics | (n=32) | (n=56) |
| Age, Yearsa | 44.58 (0.88) | 42.07 (0.62)* |
| Non-Hispanic Caucasianb | 24 (75%) | 42 (75%) |
| Educationb | 12 (38%) | 29 (53%) |
| Incomeb | 12 (38%) | 27 (48%) |
| Psychological Factors | ||
| Parental Stress Scalea | 46.51 (1.70) | 36.27 (1.05)** |
| Depressive Symptomsa | 21.29 (1.33) | 11.67 (0.80)** |
| Health & Medical Factors | ||
| NSAIDsb | 2 (6%) | 0 (0%) |
| Antidepressant Useb | 6 (19%) | 1 (2%)** |
| Physical Activity, METsa | 1048.48 (180.60) | 1152.07 (96.31) |
| Body Mass Indexa | 24.65 (0.73) | 24.89 (0.59) |
| Leukocyte Telomere Lengtha | 1.06 (0.03) | 1.07 (0.02) |
| Narrative Factors | ||
| Integrationc | 0.20 (0.40) | 0.00 (0.33) |
| Meaning-Makingc | 0.40 (0.20) | 0.33 (0.67) |
| Contaminationc | 0.00 (0.00) | 0.00 (0.00) |
| Redemptionc | 0.00 (0.20) | 0.00 (0.00)** |
Note.
p ≤.01;
p ≤.05;
N=88;
=M(SEM), p-values from independent t-test;
= n(%) p-values from chi-squared tests or Fisher’s Exact Test where n<5;
=Median (IQR), p-values derived from a Mann Whitney U-test; Non-Hispanic Caucasian (1), all other races and Hispanics of any race (0); Education coded as Bachelor’s or less (0) or more than a Bachelor’s (1), education was missing for one participant; Income coded as <$150k (0) or >=$150k (1); Physical activity computed as Metabolic Equivalent of Task scores (METs) based on the average over 7 days of self-reported activity.
Table 2.
Spearman’s correlations among narrative themes and psychological factors for caregivers and controls
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| Caregivers | ||||||
| 1. Integration | .514** | −.303† | −.051 | −.156 | −.279 | |
| 2. Meaning Making | .741** | −.273 | .211 | −.149 | −.245 | |
| 3. Contamination | .057 | .022 | .305† | −.047 | .016 | |
| 4. Redemption | .020 | .076 | .2.77* | −.202 | .011 | |
| 5. Depressive symptoms | −.172 | −.180 | .170 | −.012 | .343† | |
| 6. Parenting Stress | −.055 | .006 | .295* | .074 | .337* | |
| Controls | ||||||
Note.
p ≤.01;
p ≤.05;
p <.10;
N= 88; caregivers (n=32), controls (n=56); Depression=Inventory of Depressive Symptomology; Spearman rank order (non-parametric) correlations among caregivers (top right of diagonal, shaded) and controls (bottom left of diagonal, non-shaded).
Longitudinal regression analyses.
To test the associations between narrative themes at baseline and change in our primary outcomes over the subsequent 18 months, we calculated standardized residualized change scores for each outcome (i.e., parenting stress, depressive symptoms, and LTL over 18 months), such that change was uncorrelated with baseline levels (J. Cohen, Cohen, West, & Aiken, 2003). In robust regression analyses (Huber, 1973), we report median bootstrapped coefficients with 90% resampling and 100 iterations to minimize the impact of skewed distributions. We used a rigorous 99% confidence interval (critical alpha=.01) to determine whether the bootstrapped robust regression coefficients were statistically significant. We report both unadjusted results and results that covary for age and antidepressant use, as these two factors significantly differed between the two groups. We found that only two control mothers were scored above a 0 on contamination (see Table 1); hence, we did not test contamination in the final regression models, because the sample size was too small to yield interpretable results for the interaction effects. We entered each narrative theme sequentially into the regression models as independent predictors, along with group status (caregiver vs. control), and the group status*narrative theme interaction term and (in adjusted models) covariates. We deemed results of these bootstrapped regression models interpretable only if they met two conditions: 1) the group*narrative theme interaction term was statistically significant, and 2) one of the groups exhibited a statistically significant simple effect. We conducted these statistical analyses in Python 2.7 using the statsmodels and sklearn libraries.
Descriptive information and correlations.
As shown in Table 1, caregivers tended to be slightly older than controls (p=.020) and were more likely to use antidepressants (p=.009). Caregivers endorsed higher levels of parenting stress and depressive symptoms relative to controls (p’s≤.01) but did not differ in leukocyte telomere length (LTL) (p>.05). Caregivers also evidenced significantly higher levels of redemption than non-caregivers (p=.008). As shown in Table 2, with the exception of integration and meaning-making, narrative themes were not very highly correlated with one another, which supports their analysis as separate constructs. Narrative themes were not statistically significantly associated with depressive symptoms or parenting stress among caregivers or controls, likely due to the small sample, though their associations mostly followed the expected directions.
Among all participants, changes in parenting stress were associated with changes in depressive symptoms (r=.278, p=.010) but were not significantly associated with changes in T/S ratio (r=−.031, p=.778), and changes in depressive symptoms were not significantly associated with changes in T/S ratio (r=−.093, p=.397). Among caregivers, changes in parenting stress were not significantly associated with changes in depressive symptoms (r=.244, p=.203) or changes in T/S ratio (r=−.262, p=.169), and changes in depressive symptoms were not significantly associated with changes in T/S ratio (r=−. 154, p=.417). Among controls, changes in parenting stress were significantly associated with changes in depressive symptoms (r=.289, p=.031), however, changes in T/S ratio were not significantly associated with changes in parenting stress (r=.076, p=.580) or changes in depressive symptoms (r=−.085, p=.535).
Results
Participants
Participant characteristics appear in Table 1.
Longitudinal Regression Analyses
Correlations among study variables appear in Table 2. We report bootstrapped regression coefficients and their 99% confidence intervals (CIs) for interaction terms in Table 3.
Table 3.
Interaction tests of group by narrative factors predicting future 18-month changes in outcomes3.
| Unadjusted Models | Adjusted Models (age, antidepressants) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | Integration | Meaning Making | Redemption | Integration | Meaning Making | Redemption | ||||||
| Outcome | B | 99% CI | B | 99% CI | B | 99% CI | B | 99% CI | B | 99% CI | B | 99% CI |
| Parenting Stress (PS) | −0.83 | −1.32 −0.16 |
0.43 | −0.01 0.97 |
−0.57 | −2.14 0.95 |
−0.80 | −1.29 −0.14 |
0.44 | −0.10 1.02 |
−0.66 | −2.14 1.19 |
| Depressive Symptoms (DS) | −0.50 | −1.23 −0.07 |
−0.15 | −0.59 0.39 |
−0.38 | −1.77 1.05 |
−0.37 | −1.13 0.07 |
−0.07 | −0.56 0.53 |
−0.41 | −1.87 1.03 |
| Leukocyte Telomere Length (LTL) | 1.19 | 0.53 2.13 |
−0.08 | −0.64 0.50 |
−0.59 | −3.66 3.52 |
1.05 | 0.48 1.84 |
−0.21 | −0.72 0.35 |
−0.77 | −2.86 2.32 |
Note.
p<.01;
Outcome=Standardized residualized change in PS, DS, or LTL from baseline to 18 months; negative coefficients indicate that individuals with higher levels of the given narrative factor at baseline experienced a greater decrease (or lesser increase) in the outcome variable over the subsequent 18 months. Model specifications: A sample of n=88 provided complete data for analyses (caregivers n=32; controls n=56; however, three caregivers were missing data for change in PS and 2 for change in IDS). Adjusted models account for age and antidepressant use. All models are based on bootstrapped robust regression coefficients, where the estimates represent the median coefficient of the bootstrapped distribution and the CI represents the 99% confidence interval (lower bound, upper bound).
Leukocyte Telomere Length (LTL).
Average LTL did not significantly differ in the whole sample from baseline (M±SEM: 1.064±0.016) to 18 months (M±SEM: 1.064±0.016; ns). Nonetheless, as shown in Table 3, there was a significant group*integration interaction predicting change in LTL in both unadjusted and adjusted models. Deconstruction of the unadjusted interaction term revealed significant simple effects for each group, caregivers (B= 1.437, 99% CI: [0.973, 2.487]) and controls (B=0.305, 99% CI: [0.02, 0.589]). However, after adjusting for age and antidepressant use, the simple effect for caregivers (B=1.245, 99% CI: [0.832, 2.329]) remained significant, whereas the simple effect was for controls was no longer significant (B=0.153, 99% CI: [−0.013, 0.383]). This indicates that greater integration was prospectively associated with significantly greater LTL lengthening over 18 months among caregivers. Other narrative themes (meaning-making, redemption) did not interact with group to statistically significantly predict LTL.
Parenting stress (PS).
Overall, PS did not change from baseline (M±SEM: 39.775±1.044) to 18 months (M±SEM: 39.902±1.090) in this sample (ns). As shown in Table 3, there was a significant group*integration interaction predicting change in PS in both unadjusted and adjusted models. However, deconstruction of this interaction did not reveal significant simple effects of integration on change in PS with this conservative critical alpha of .01 among caregivers (B=−0.548; 99% CI: [−1.361, 0.168]) or controls (B=0.175, 99% CI: [−0.357, 0.369]). Together, these findings suggest that although the slopes of change in caregivers and controls were significantly different from each other, in split group analyses (with lower statistical power), each group’s slope did not statistically significantly differ from zero. The direction of results, however, does show that caregivers who showed greater narrative integration experienced decreases in PS over time, which is numerically consistent with the pattern of effects with LTL. Other narrative themes (meaning-making, redemption) did not interact with group to predict PS.
Depressive symptoms [DS].
Overall, DS decreased significantly from baseline (M±SEM: 15.160±0.875) to 18 months (M±SEM: 13.090±0.876; p=.003). As shown in Table 3, there was a significant group*integration interaction predicting change in DS in an unadjusted model, but this finding did not hold after adjusting for age and antidepressant use (adjusted model). Deconstruction of the unadjusted interaction term did not reveal significant simple effects of integration on change in DS among caregivers (B=−0.262, 99% CI: [−1.022, 0.003]) or controls (B=0.188, 99% CI: [−0.048, 0.364]), although the direction of the numerical pattern was consistent again with findings from LTL and PS. Other narrative themes (meaning-making, redemption) did not interact with group to predict DS2.
Discussion
Challenging life situations like caregiving for a family member with a chronic condition require tremendous adaptation. The way we integrate these experiences into our narrative identity – the way we make sense our lives by telling stories about our experiences – may reveal how we cope with major stressful life events, such as being a parent of a child with autism spectrum disorder. Our results demonstrate for the first time that individual differences in integration, a growth-related theme in participants’ narrative identity, are prospectively associated with different trajectories of leukocyte telomere length (LTL) over the following 18 months. Caregiving mothers, whose narratives were characterized by high levels of psychological integration, had slower LTL shortening over time, relative to control mothers. In addition, we did not find significant associations between the affective theme of redemption and subsequent LTL change, suggesting growth processes may be more important than affective processes for this biomarker in the context of chronic stress. If replicated, these analyses add narrative integration as a new predictor of resilient trajectories during chronic stress, which has heretofore never been examined in the context of biomarkers of aging.
Most research linking chronic stress to health has focused on symptoms of distress or coping strategies. This is the first study we are aware of to use narrative approaches to assess stress resilience in the context of chronic stress exposures (caregiving) in relation to physical health and aging. How parents tell the story of their parenting stresses and joys reveals their implicit models of how their parenting role has been appraised and integrated into their life story and thus could shape levels of parenting stress over time. This method can assess aspects of one’s identity in the context of an ongoing, important, and often challenging social role like parenting, reflecting in a holistic way the way parents serve as the actor, agent, and author of their life (McAdams, 2013). Further, by influencing how the common parenting stressors are experienced and understood, these different narrative styles could potentially have an impact on chronic stress arousal and restorative capacities and indices of health. For LTL, it is likely that the interaction of buffering factors (e.g., “multisystem resiliency”) and stress exposure indices (e.g., in this study, being a caregiver or a control mother) will predict outcomes better than the individual effects of buffers or stress exposures alone (Puterman & Epel, 2012).
We examined two broad categories of narrative styles in this study, one focused on an affective journey (i.e., redemption and contamination) and another focused on a growth journey (i.e., integration and meaning-making). Our results indicate that the integration component of growth narratives during stressful experiences is one pathway towards better psychological and physical health. Among caregivers, the theme of integration emerged as the strongest predictor of positive outcomes in this sample: Greater integration predicted less parenting stress and less LTL shortening more strongly among caregivers than in controls. This finding aligns with another study focused on this same sample of caregivers, in which greater acceptance of child’s diagnosis (based on a new self-report scale) was related to lower levels of depression over the ensuing year (Paz, Siegel, Coccia, & Epel, 2018). In contrast, affective themes in participants’ narratives did not demonstrate similar associations. It is worth noting, however, that because few narratives included contamination, we could not analyze the interaction effects of this affective theme, and we only ultimately analyzed redemption. Nonetheless, these results suggest the possibility that caregivers may find narrative strategies aimed at integrating their challenging experiences and their new life-defining situation into their broader sense of self more beneficial than those aimed at alleviating negative emotions. It may be helpful for parental caregivers of children with chronic conditions, who often have altered life trajectories, to coherently integrate this “biographical disruption” (Bury, 1982) into their overall identity. Large cognitive shifts may often be necessary for healthy adaptation to a life of caregiving. For example, disengagement from unattainable goals in dementia caregivers predicts better mental health (Wrosch, Amir, & Miller, 2011).
Although there are psychometrically valid measures of trait-like stress resilience, these measures may be of less value in predicting an individual’s actual adaptation over time, as they have not robustly predicted mental health or biological outcomes longitudinally (Bonanno & Diminich, 2013). Such measures capture how effectively one believes that he or she is rising above challenging situations in general, and these measures tend to lack explanatory power beyond the idea that certain types of people “don’t sweat the small stuff.” A fundamental problem with such measures is that resiliency is not a general characteristic of a person, but a response to a situation; hence, our model reflects this inherent interaction of a stressful exposure by a coping strategy. We believe the study of resilient trajectories in the context of chronic stress would benefit from an increased focus on narrative identity: specifically, the ways in which people craft stories about their experiences in order to provide their sense of self with unity and purpose. This perspective offers a theoretical framework, a methodological operationalization, and an analytical strategy for assessing the unique meaning each individual derives from their experience (Adler et al., 2017). Rather than focusing solely on a self-report questionnaire-based assessment of adaptation to stress, which inevitably taps beliefs, a narrative identity approach encourages participants to simply share their stories in an authentic way, enacting and demonstrating their narrative identity, and only subsequently applies empirically-derived categories for distilling the relevant thematic variables. Narrative identity therefore offers stress researchers both a theoretical foundation and an unobtrusive set of tools for examining individuals’ phenomenological experience of their stress, one which the present study has demonstrated to be associated with different trajectories of resilience.
Future studies might strive to identify the cognitive-affective network that underlies the narrative theme of “integration” during adaptation to a major chronic stressor. Integration involves the coherent synthesizing of new experiences into one’s current self-story. One can also view integration from a neuroscientific perspective, which may help future researchers deconstruct or identify the mechanisms by which a somewhat abstract concept like integration might influence a cellular level marker like telomere length. Specifically, the dorsal anterior cingulate cortex (dACC) has been implicated in the ability to engage in behavioral flexibility or persistence (Kolling et al., 2016; Rose Addis & Tippett, 2008). The dACC is also involved in the resolution of conflicting pieces of information, including inputs from reward and threat centers, in order to mobilize goal-oriented behavior. Hence, the dACC and cognitive tests that depend heavily on the dACC may be of interest in relation to integration. Moreover, autobiographical reasoning is a key aspect of integration, which is hypothesized to influence encoding of memories with respect to the Eriksonian identity goals of the self (Kolling et al., 2016). Effectively, autobiographical memories serve to record self-defining experiences of success or failure that mark major shifts in expectations and therefore guide behavior going forward. As an individual contemplates decisions in the present, they relate these to salient autobiographical memories of these self-defining success or failure experiences, and thereby guide future decision making (e.g., McLean, Pasupathi, & Pals, 2007; Pasupathi, 2001). Narrative themes of integration effectively capture this process. Parental caregivers have more challenges in the pursuit of developing positive evaluations of their parenting and their other roles in life. This may explain why integration of views of parenting amongst caregivers, but not controls, predicts healthier trajectories in parenting stress. It is not clear why integration did not predict changes in depressive symptoms; however, in contrast to parenting stress, depressive symptom measures encompass different and more heterogeneous domains (e.g., sleep, appetite). Also, the fact that caregivers were more likely to take antidepressants, and we covarying for antidepressant use in the adjusted analyses, may have meant that statistical analyses could not sufficiently disentangle caregiver status from antidepressant use in relation to trajectories of depressive symptoms. Finally, integration may have served as a buffer to the chronic stress arousal that can leading to telomere shortening amongst caregivers.
Limitations
One major limitation in the present study was the small sample size, which may have particularly impacted the simple effects analyses in caregivers and non-caregivers separately, particularly given that there were fewer caregivers than controls. We note the absence of an a priori sample size calculation, as we conducted these secondary analyses on a subsample of participants in a larger study. Thus, some analyses may not have been sufficiently statistically powerful enough to detect effects4. The longitudinal and labor-intensive study design placed pragmatic constraints on this study but presented an opportunity for a series of initial exploratory analyses seeking to break new empirical ground.
Another limitation is that to optimally study resilient trajectories, we would need baseline assessments of the outcomes before one group of participants becomes caregivers. This is typically not possible in studies of caregivers, although it could be possible in a national prospective cohort study. Although narrative measures are not typically included in large studies, they could be included as part of burst study designs (Sliwinski, 2008).
The structure of the interview necessarily differed for caregivers than for con t rols, as it was important to include some interview prompts specifically about the experience of having a child with an autism spectrum disorder for caregivers. To leave this fact unacknowledged during these intimate interviews would have been ethically inappropriate. Nevertheless, it is possible that the presence of these additional prompts may have influenced caregiver group differences in narrative responses, leading to more opportunity for expression and the higher scores observed on some narrative themes. We statistically accounted for group differences in number of codes assigned to the narratives by averaging across all prompts to generate scores for each narrative theme for each participant.
Although we analyzed several narrative themes in the final regression results, we used a conservative critical alpha of .01 in the final regression models, which is quite conservative. We elected not to analyze contamination due to the low sample size of controls rated as having contamination present in their narrative (only two participants). While we found a significant interaction for depressive symptoms, because this did not hold when adjusting for antidepressant use and age, and because it did not hold in simple effects analyses in each separate group (caregiver versus control), we did not interpret this finding, though the general direction was consistent with the broader pattern of results.
Though the associations of baseline narrative themes with longitudinal change in outcomes is consistent with possible causal effects, we cannot conclude that the results are causal. It remains possible that a common underlying cause drove the observed associations. Research to date has not shown narrative factors to correlate with SES (Adler et al., 2016). Future studies might assess autonomic nervous system (ANS) reactivity while participants provide their narratives, and examine associations between narrative themes and ANS reactivity (as in Pasupathi, Wainryb, Mansfield, & Bourne, 2017) in order to better understand potential transducers of the effects reported here.
Lastly, these findings may be of limited generalizability. We observed these results among women; therefore, we cannot say whether they generalize to men. Affect expression and the identity associated with being “a mother” has strong gender norms in many cultures, may vary across different dominant cultural narratives about parenting (McLean & Syed, 2015) and may therefore not have the same effects on mental health or biological outcomes across genders. Additionally, the parent study design inclusion criteria did not afford the opportunity to examine caregivers with very low levels of perceived stress, who might be considered especially resilient. Future research on meaning-based coping and resilience should endeavor to include these individuals. These results may not generalize to individuals with a cancer diagnosis, whom we excluded from this study. Although much evidence associates short LTL with cancer (Ma et al., 2011; Wentzensen, Mirabello, Pfeiffer, & Savage, 2011; Willeit et al., 2010), there is also some evidence that longer LTL may increase risk for certain cancers (Codd et al., 2013). Importantly, these associations vary by type of cancer, with cancers with higher fatality rates show this association more strongly, and cancers with favorable prognoses showing modest or absent associations (Willeit et al., 2010). We note that there are no population-based norms for “short” or “long” telomere length, hence, we do not categorize people in terms of having “short” or “long” telomeres. Thus far, there is no evidence that the changes (e.g., slowing of shortening, or lengthening) in LTL length observed in the context of health behavior interventions would increase cancer risk.
Conclusion
In sum, integration – or the ability to weave challenging experiences into an overall coherent story of one’s identity – was associated with a pattern of maintaining or improving perceived stress levels and telomere maintenance. This opens the door for new treatment targets among chronically stressed caregivers. Narrative methods provide the opportunity to assess more complex psychological-cognitive constructs, such as meaning and integration, which are rarely explored in basic science research settings, but play a prominent role in clinical therapeutic ones. Counter to popular belief, coping strategies that focus on transforming negative experiences into positive ones are not always the most effective approach for life defining stressors such as maternal caregiving. Caring for an autistic child is a stressor that cannot objectively be “changed,” rather it must be transcended through enhanced psychological adaptation, one focused on integrating the new parental role into one’s broader narrative identity. This is a psychological process which many individuals undertake intuitively, but one which might be specifically targeted and enhanced by empirically-informed psychosocial intervention strategies. We hope this preliminary investigation will stimulate more research both replicating and extending findings focused on the potential impacts of narrative processes, and especially integrative themes on both psychological and physical health.
Figure 1.
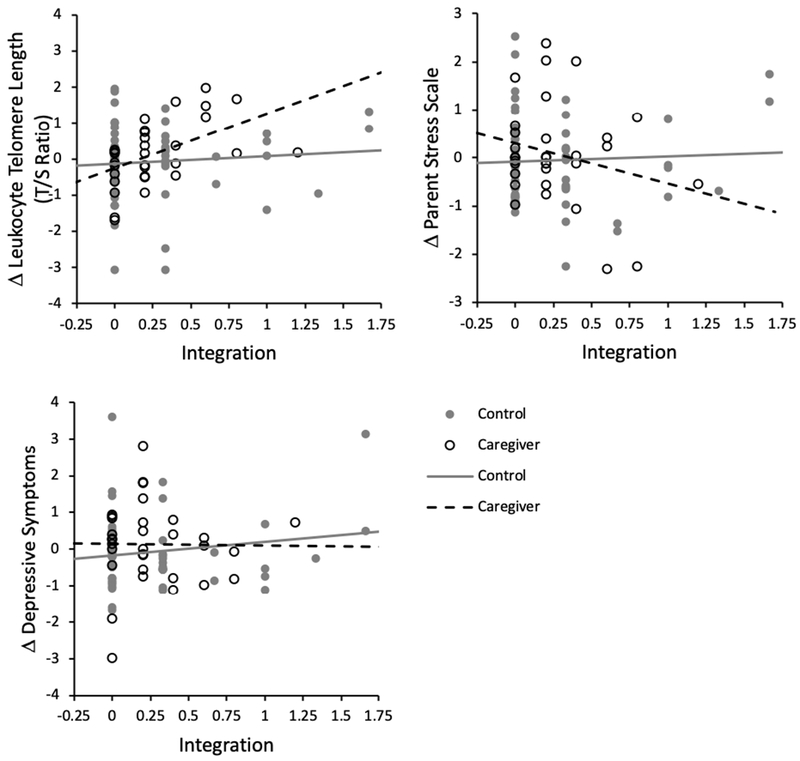
Differences in the longitudinal associations between narrative integration and outcomes among caregivers and controls.
Note. Plots depict the longitudinal associations of integration at baseline with residualized change in each outcome over the subsequent 18 months.
Highlights.
Caregiving for a child with an autism spectrum disorder (ASD) is a chronic stressor
How caregivers integrate stressful experiences is correlated with mental and psychobiological health outcomes
Caregivers with more integrated narratives had slower telomere shortening over 18 months
Narrative integration, not affective themes, correlated with positive biological indicators
Integrating what caregiving means for self-identity may be a source of stress resilience
Acknowledgments
Funding: The research was supported by a 1440 Award from the Mind and Life Institute (MRI-2014-1440-Mason) to Ashley E. Mason. This research was also supported by awards from the National Institutes of Health (NIH) to Elissa S. Epel (NIA; R01AG030424-01A2), Ashley E. Mason (NHLBI; K23HL133442), and Kirstin Aschbacher (NHLBI; K23HL112955). Additional support was provided to Kirstin Aschbacher from The Institute for Integrative Health (TIIH). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclosure: The authors declare no conflict of interest.
Available at: https://community.plu.edu/~chasega/met.html
After excluding participants using antidepressant medications (n=7), there was still no statistically significant interaction between group (caregiver vs. control) and integration in the prediction of depressive symptoms before (B=−0.256, 95% CI: −1.205, 0.459, ns) and after adjusting for age (B=−0.236, 95% CI: −1.223, 0.462, ns).
In this sample, income demonstrated bimodality such that a median split provided a reasonable metric of the data without skewing statistics. Regressions treating income and education as continuous variables yielded the same patterns of results and statistical significance as models in which we treated them dichotomously.
We conducted a crude power analysis with G*Power software using the correlation value between Integration and T/S ratio change among caregivers (r=.506) as an effect size estimate, with a critical alpha of .05 and power of .80, and we observed that a total sample size of n=25 would be needed to detect statistical significance in these analyses. For parenting stress, with a correlation among caregivers of r=−.248 (and the same critical alpha and power levels), a sample size of n=122 would be required to detect statistical significance in these analyses. Hence, we conclude that in this study, based on post hoc power calculations, our analysis appears sufficiently powered to detect the T/S ratio changes but may not have been sufficiently powered to detect changes in parenting stress.
References
- Adler JM (2012). Living into the story: Agency and coherence in a longitudinal study of narrative identity development and mental health over the course of psychotherapy. Journal of Personality and Social Psychology, 102(2), 367. [DOI] [PubMed] [Google Scholar]
- Adler JM, Dunlop WL, Fivush R, Lilgendahl JP, Lodi-Smith J, McAdams DP, … Syed M (2017). Research methods for studying narrative identity: A primer. Social Psychological and Personality Science, 8(5), 519–527. [Google Scholar]
- Adler JM, Lodi-Smith J, Philippe FL, & Houle I (2016). The incremental validity of narrative identity in predicting well-being: A review of the field and recommendations for the future. Personality and Social Psychology Review, 20(2), 142–175. [DOI] [PubMed] [Google Scholar]
- Adler JM, Turner AF, Brookshier KM, Monahan C, Walder-Biesanz I, Harmeling LH, … Oltmanns TF (2015). Variation in narrative identity is associated with trajectories of mental health over several years. Journal of Personality and Social Psychology, 108(3), 476–496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aschbacher K, Milush JM, Gilbert A, Almeida C, Sinclair E, Epling L, … Epel E (2017). Chronic stress is associated with reduced circulating hematopoietic progenitor cell number: A maternal caregiving model. Brain, Behavior, and Immunity, 59, 245–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baerger DR, & McAdams DP (1999). Life story coherence and its relation to psychological wellbeing. Narrative Inquiry, 9(1), 69–96. [Google Scholar]
- Bauer JJ, McAdams DP, & Sakaeda AR (2005). Interpreting the good life: growth memories in the lives of mature, happy people. Journal of Personality and Social Psychology, 88(1), 203–17. [DOI] [PubMed] [Google Scholar]
- Berry JO, & Jones WH (1995). The Parental Stress Scale: Initial Psychometric Evidence. Journal of Social and Personal Relationships, 12(3), 463–472. [Google Scholar]
- Bonanno GA, & Diminich ED (2013). Annual Research Review: Positive adjustment to adversity-trajectories of minimal-impact resilience and emergent resilience. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 54(4), 378–401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bury M (1982). Chronic illness as biographical disruption. Sociology of Health & Illness, 4(2), 167–182. [DOI] [PubMed] [Google Scholar]
- Codd V, Nelson CP, Albrecht E, Mangino M, Deelen J, Buxton JL, … Samani NJ (2013). Identification of seven loci affecting mean telomere length and their association with disease. Nature Genetics, 45(4), 422–427, 427e1–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen J, Cohen P, West SG, & Aiken LS (2003). Applied multiple regression/correlation analysis for the behavioral sciences. Routledge. [Google Scholar]
- Cohen S, & Janicki-Deverts D (2012). Who’s stressed? Distributions of psychological stress in the United States in probability samples from 1983, 2006, and 2009. Journal of Applied Social Psychology, 42(6), 1320–1334. [Google Scholar]
- Cohen S, Kamarck T, & Mermelstein R (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. [PubMed] [Google Scholar]
- Damjanovic AK, Yang Y, Glaser R, Kiecolt-Glaser JK, Nguyen H, Laskowski B, … Weng N (2007). Accelerated telomere erosion is associated with a declining immune function of caregivers of Alzheimer’s disease patients. Journal of Immunology, 179(6), 4249–4254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunlop WL, & Tracy JL (2013). Sobering stories: Narratives of self-redemption predict behavioral change and improved health among recovering alcoholics. Journal of Personality and Social Psychology, 104(3), 576. [DOI] [PubMed] [Google Scholar]
- Epel ES, Blackburn EH, Lin J, Dhabhar FS, Adler NE, Morrow JD, & Cawthon RM (2004). Accelerated telomere shortening in response to life stress. Proceedings of the National Academy of Sciences of the United States of America, 101(49), 17312–17315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frankl VE (1985). Man’s search for meaning. Simon and Schuster. [Google Scholar]
- Frazier P, Tennen H, Gavian M, Park C, Tomich P, & Tashiro T (2009). Does self-reported posttraumatic growth reflect genuine positive change? Psychological Science, 20(7), 912–919. [DOI] [PubMed] [Google Scholar]
- Galatzer-Levy IR, Huang SH, & Bonanno GA (2018). Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clinical Psychology Review, 63, 41–55. [DOI] [PubMed] [Google Scholar]
- Hammack PL (2008). Narrative and the cultural psychology of identity. Personality and Social Psychology Review, 12(3), 222–247. [DOI] [PubMed] [Google Scholar]
- Hayes SA, & Watson SL (2013). The impact of parenting stress: A meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(3), 629–642. [DOI] [PubMed] [Google Scholar]
- Huber PJ (1973). Robust regression: asymptotics, conjectures and Monte Carlo. The Annals of Statistics, 1(5), 799–821. [Google Scholar]
- King LA, Scollon CK, Ramsey C, & Williams T (2000). Stories of life transition: Subjective well-being and ego development in parents of children with down syndrome. Journal of Research in Personality, 34(4), 509–536. [Google Scholar]
- Kolling N, Wittmann MK, Behrens TE, Boorman ED, Mars RB, & Rushworth MF (2016). Value, search, persistence and model updating in anterior cingulate cortex. Nature Neuroscience, 19(10), 1280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin J, Epel E, & Blackburn E (2012). Telomeres and lifestyle factors: roles in cellular aging. Mutation Research/Fundamental and Molecular Mechanisms of Mutagenesis, 730(1), 85–89. [DOI] [PubMed] [Google Scholar]
- Lin J, Epel E, Cheon J, Kroenke C, Sinclair E, Bigos M, … Blackburn E (2010). Analyses and comparisons of telomerase activity and telomere length in human T and B cells: insights for epidemiology of telomere maintenance. Journal of Immunological Methods, 352(1–2), 71–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma H, Zhou Z, Wei S, Liu Z, Pooley KA, Dunning AM, … Wei Q (2011). Shortened telomere length is associated with increased risk of cancer: A meta-analysis. PloS One, 6(6), e20466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McAdams DP (2001). The psychology of life stories. Review of General Psychology, 5(2), 100. [Google Scholar]
- McAdams DP (2013). The psychological self as actor, agent, and author. Perspectives on Psychological Science, 8(3), 272–295. [DOI] [PubMed] [Google Scholar]
- McAdams DP, & McLean KC (2013). Narrative identity. Current Directions in Psychological Science, 22(3), 233–238. [Google Scholar]
- McAdams DP, Reynolds J, Lewis M, Patten AH, & Bowman PJ (2001). When bad things turn good and good things turn bad: Sequences of redemption and contamination in life narrative and their relation to psychosocial adaptation in midlife adults and in students. Personality and Social Psychology Bulletin, 27(4), 474–485. [Google Scholar]
- McLean KC, Pasupathi M, & Pals JL (2007). Selves creating stories creating selves: A process model of self-development. Personality and Social Psychology Review, 11(3), 262–278. [DOI] [PubMed] [Google Scholar]
- McLean KC, & Pratt MW (2006). Life’s little (and big) lessons: Identity statuses and meaning-making in the turning point narratives of emerging adults. Developmental Psychology, 42(4), 714–722. [DOI] [PubMed] [Google Scholar]
- McLean KC, & Syed M (2015). Personal, master, and alternative narratives: An integrative framework for understanding identity development in context. Human Development, 58(6), 318–349. [Google Scholar]
- Park CL (2010). Making sense of the meaning literature: an integrative review of meaning making and its effects on adjustment to stressful life events. Psychological Bulletin, 136(2), 257–301. [DOI] [PubMed] [Google Scholar]
- Pasupathi M (2001). The social construction of the personal past and its implications for adult development. Psychological Bulletin, 127(5), 651. [DOI] [PubMed] [Google Scholar]
- Pasupathi M, Wainryb C, Mansfield CD, & Bourne S (2017). The feeling of the story: Narrating to regulate anger and sadness. Cognition and Emotion, 31(3), 444–461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paz NSD, Siegel B, Coccia MA, & Epel ES (2018). Acceptance or despair? Maternal adjustment to having a child diagnosed with autism. Journal of Autism and Developmental Disorders, 48(6), 1971–1981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prather AA, Epel ES, Arenander J, Broestl L, Garay BI, Wang D, & Dubal DB (2015). Longevity factor klotho and chronic psychological stress. Translational Psychiatry, 5(6), e585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Puterman E, & Epel E (2012). An intricate dance: Life experience, multisystem resiliency, and rate of telomere decline throughout the lifespan. Social and Personality Psychology Compass, 6(11), 807–825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rose Addis D, & Tippett LJ (2008). The contributions of autobiographical memory to the content and continuity of identity a social-cognitive neuroscience approach. Self Continuity: Individual and Collective Perspectives. [Google Scholar]
- Rush AJ, Gullion CM, Basco MR, Jarrett RB, & Trivedi MH (1996). The Inventory of Depressive Symptomatology (IDS): Psychometric properties. Psychological Medicine, 26(3), 477–486. [DOI] [PubMed] [Google Scholar]
- Singer JA (2004). Narrative identity and meaning making across the adult lifespan: An introduction. Journal of Personality, 72(3), 437–460. [DOI] [PubMed] [Google Scholar]
- Sliwinski MJ (2008). Measurement-burst designs for social health research. Social and Personality Psychology Compass, 2(1), 245–261. [Google Scholar]
- Wentzensen IM, Mirabello L, Pfeiffer RM, & Savage SA (2011). The association of telomere length and cancer: A meta-analysis. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology, 20(6), 1238–1250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willeit P, Willeit J, Mayr A, Weger S, Oberhollenzer F, Brandstätter A, … Kiechl S (2010). Telomere length and risk of incident cancer and cancer mortality. JAMA, 304(1), 69–75. [DOI] [PubMed] [Google Scholar]
- Wrosch C, Amir E, & Miller GE (2011). Goal adjustment capacities, coping, and subjective wellbeing: The sample case of caregiving for a family member with mental illness. Journal of Personality and Social Psychology, 100(5), 934–946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu DSF, Cheng S-T, & Wang J (2018). Unravelling positive aspects of caregiving in dementia: An integrative review of research literature. International Journal of Nursing Studies, 79, 1–26. [DOI] [PubMed] [Google Scholar]