

Supplemental Digital Content is available in the text
Keywords: heat stress, mine rescue, mining, occupational health and safety, physical exertion
Abstract
Objective:
To describe physiological responses of mine rescuers during a simulated mine emergency.
Methods:
Body-worn monitors (n = 74) and core temperature (Tc) capsules (n = 54) assessed heart rate (HR), respiration rate (RR), energy expenditure (EE), oxygen consumption ( ), Tc and skin temperature (Tskin), by team position and task. A multivariate analysis was performed with team positions, tasks, and measures as factors.
), Tc and skin temperature (Tskin), by team position and task. A multivariate analysis was performed with team positions, tasks, and measures as factors.
Results:
HRmean and HRpeak were 78.6% and 94.5%, respectively, of predicted maximum heart rate. Arduous labor tasks elicited higher HR, RR, and  than casualty care. Captains exhibited lower HRmean, HRpeak, RR, RRpeak,
than casualty care. Captains exhibited lower HRmean, HRpeak, RR, RRpeak,  , Tc, and Tskin compared with other positions. Tc mean exceeded 38.6 °C (n = 14 recorded Tc >39 °C).
, Tc, and Tskin compared with other positions. Tc mean exceeded 38.6 °C (n = 14 recorded Tc >39 °C).
Conclusions:
Captains’ physical loading and heat stress were lowest. Nonetheless, all tasks and positions induced high physical load and heat strain.
The mining industry has high occupational rates of serious injury and fatality: the Ontario Mining Industry reported 945 injuries in 2014 alone.1 Frequent accidents involving fires underground, falls of ground, mobile equipment collisions, exposure to harmful environments, and falls from heights, often require rescue.1 Ontario alone averages 44 mine-related rescues annually,2,3 although mine rescue related injuries are not recorded separately in the statistics (personal communication: Ontario Mine Rescue). Globally, mine rescue workers have died; and in 1998 the International Mine Rescue Body (IMRB) was specifically created in the aftermath of one such tragedy; which claimed the lives of six Polish mine rescuers during a mission, from heat-related illness.4 Canada has not had a similar tragedy to date, however, in 2015, Ontario conducted a comprehensive, underground mining health, safety and prevention review and identified: physiological factors associated with required fitness needs of volunteer, emergency responders; and acclimation to mine rescue conditions; as key health and safety issues, to have the greatest impact on improving health and safety outcomes.5
Currently, mine rescue work in Canada does not require a fitness standard. The Supreme Court of Canada (and described by Jamnik et al)6 states that a fitness standard for a workforce be: criterion-based and validly linked to the critical, life-threatening, physical demands of the job. Specifically, the standard be based on “safe” (properly executing the life-threatening, physically demanding emergency task) and “efficient” (completing tasks in a time frame suited to the emergency circumstance) requirements. The assignment of Safe and Efficient policies is the responsibility of the occupation-specific participant-matter experts. These standards must take into account the individualities of the participants (age, sex, experience).6 Therefore, to implement a fitness standard, describing the physical demands and the tasks performed during a mine rescue is a primary priority.6
Mine rescue work is performed by a team of volunteer mine employees who are trained in mine-related emergencies.3,7 During an emergency involving a casualty, rescuers are required to carry supplies; weighing approximately 142 kg.3,6 Furthermore, all tasks require personal protective equipment (PPE) (approximately 22 kg).3,7 Mine rescue teams consist of six members: Captain, Vice-Captain, No. 2, No. 3, No. 4 persons, and a Briefing Officer: who remains on surface for the duration of the emergency.3,7 The Captain is responsible for leading the team, communicating with the Briefing Officer, providing instructions to and ensuring the wellbeing of the team underground. The Captain does not perform other tasks unless under extreme circumstances.3 The Vice-Captain is responsible for providing some instruction, but will assist in all rescue-related tasks.3 Number 2, No. 3, and No. 4 persons have similar roles: work according to Captain's instructions and sharing tasks, (eg, eliminating hazards, treating a casualty, and firefighting).3 This division of labor creates inherent differences in physical loads between the Captain and other members of the team. Differences between team positions have never been examined in the literature to date.
Research studying mine rescue work has only examined specific rescue-related tasks; showing these tasks to be extremely physically demanding.3,8–11 Rescuers have never been studied during an actual mine rescue event. Stewart et al8 reported a mean increase to 91% of the age-predicted maxima heart rate (APMHR) of mine rescue volunteers across three validated tasks during a controlled, simulated mine rescue environment: fire suppression, incremental carries, and shoveling. The American Conference of Governmental Industrial Hygienists (ACGIH) sets a recovery HR threshold of 110 bpm after 1-minute of rest following activity, as a way to assess heart strain.12 This study determined rescuers could only achieve HR between 139 and 149 bpm after 90 seconds following fire suppression; and nearly 120 seconds after shoveling and incremental carries.8 Heart rate in this range is considered high and well above ACGIH threshold level values of 110 bpm.12 This is significant given that, in an actual emergency, there may not be time to adequately recover, and underlines the high risk for rescue participants during a mission.
These elevated physical loads can be exacerbated in underground mine conditions as they are characterized by temperatures exceeding 40 °C, and 60% humidity.12,13 The primary mechanism of heat loss (perspiration)14–16 is inhibited by high humidity and extensive protective equipment.10–11 These impaired cooling mechanisms, combined with high physical activity, will result in higher than normal core temperature (Tc), significantly increasing the risk of heat-related illnesses.10–11
Studies to date have been conducted in controlled, artificial settings, following precise work-rest schedules, in which individuals knew tasks beforehand and had ample time allocated for rest; often participants were not professional mine rescuers.8–11,13 In a real rescue, mine rescuers often work supra-maximally for short bouts, often exceeding workloads of 1000 W.8,9 Hardcastle et al9 stated that real-life emergencies would endure greater physiological responses (than the study scenario) due to inadequate rest and hydration for the duration of the rescue.
However, other than collecting physiology data during an actual mine rescue, the closest approximation would be a simulated mining emergency. The IMRB oversees a global competition biennially to present realistic mine rescue simulations to evaluate and share skills required to perform rescue operations in a mining environment. In 2016, Ontario hosted this competition in an underground mine, under stressful, highly realistic conditions, providing a unique opportunity to study mine rescue workers during a realistic mine rescue event.
Therefore the purpose of this study was threefold: (i) to describe the mean HR, peak HR (HRpeak), respiration rate (RR), peak RR, energy expenditure (EE), and mean oxygen consumption ( ) of the primary tasks performed in a mine rescue; (ii) to describe differences (if any) between the captain and other appointed positions on mine rescue teams; and (iii) to describe the Tc and skin temperature (Tskin) of mine rescuers during a simulated mine rescue emergency.
) of the primary tasks performed in a mine rescue; (ii) to describe differences (if any) between the captain and other appointed positions on mine rescue teams; and (iii) to describe the Tc and skin temperature (Tskin) of mine rescuers during a simulated mine rescue emergency.
METHODS
Participants
At the 10th biennial International Mine Rescue Competition (IMRC), 27 teams comprised of six members each, competed. Teams were comprised of a: Captain, Vice-Captain, No. 2 person, No. 3 person, No. 4 person, and a briefing officer. We only recruited participants going underground and therefore did not recruit the briefing officer, leaving us with a total of 135 eligible participants. Seventy-six mine rescue personnel agreed to participate in this study (56.3% response rate). Of the 76 participants, 57 provided additional consent to ingest a thermometric Tc pill (42.2% response rate). All participants provided written, informed consent prior to the start of data collection. This study was approved from the Institutional University Research Ethics Board (REB #6009820).
All participants were trained, mine rescue personnel who were currently participating in, and had regularly performed mine rescue training activities in the past. With the exception of one team (a team of experts put together from multiple countries), all team members had previously trained together as a team and had been selected by their home country as their “best” to represent them at the International Mine Rescue Competition (IMRC).
Experimental Design
The competition was organized by Ontario Mine Rescue personnel, who created a series of scenarios to reflect common, real-life emergencies. Judges (experts in Mine Rescue) score the performance of each team, according to the rules and regulations governing Mine Rescue Competitions, as described on the IMRB website. The competition took place in an operational, underground mine in Sudbury's 114 ore body and is the most realistic mine rescue scenario possible, barring an actual event. Actors played the part of victims, and smoke was actively produced for the fire simulation. The participants did not know what the competition consisted of, until the briefing occurred, just prior to mine entry; mimicking an actual emergency. The day before the competition, baseline data were collected for individual participants characteristics (height, weight, age, team role, and chest-circumference for the body-worn monitor). Prior to the mine-rescue event, participants were equipped with the body-worn monitoring devices and (for n = 57 participants) also directed to ingest a Tc pill 2 hours prior,14 both of which recorded and collected data continuously for the approximately 2-hour underground portion of the mine rescue simulation event. Up to four teams competed at a given time, as the starting of teams was staggered to process all teams over the 3 days (one team completing a task at any given time). Cameras were placed throughout the mine to video-record the primary key aspects of the competition for all teams. These tasks were time stamped, to allow for a coordinated examination of the physiological data with individual tasks.
During the underground competition, competitors were challenged by four key tasks. They descended underground via a jeep with a heavy basket containing various tools (weighing approximately 100 kg). Then leading into the four tasks are as follows:
-
(1)
The first task involved an unconscious casualty and a casualty in shock; rescuers treated the casualties and prepared them to be transported to surface.
-
(2)
The second task involved a simulated fire, in which rescuers constructed a barricade composed of various materials (eg, bricks, fire retardant wrapping, and beams).
-
(3)
The third task involved a conscious casualty impaled on a steel post (alive and requiring first aid and rescue). This required rescuers to utilize extrication tools and perform precise first aid treatment to the wound.
-
(4)
The fourth task, rescuers loaded the casualty into a basket with a trolley to perform removal of the impaled victim via an exit route with a steep incline. This basket, with tools and the casualty, weighed in excess of 180 kg. Tasks 1 and 3 were similar in nature (casualty care) as are tasks 2 and 4 (arduous labor).
See Appendix A (Supplemental Digital Content 1) for photographs illustrating and summarizing these four tasks.
Measures
Mining Environmental Conditions
Captains recorded ambient conditions with a portable weather meter (Kestrel 3500) Pocket Weather (Nielson-Kellerman, US) meter immediately upon arrival at each task site and these are the averages. See Table 1.
TABLE 1.
Ambient Conditions of the Mine in the IMRC
| Task | Dry-Bulb Temperature (°C) (Tdb) | Wet-Bulb Temperature (°C) (Twb) | Relative Humidity (RH) (°C) (%) |
| 1 | 25.7 | 22.0 | 72.4 |
| 2 | 34.7 | 24.7 | 43.8 |
| 3 | 18.0 | 17.0 | 90.6 |
| 4 | 18.0 | 17.0 | 90.6 |
IMRC, International Mine Rescue Competition.
Heart and Respiration Rates
A heart and respiration rate monitor (Equivital Life MonitorTM, Hidalgo, UK), with integrated technology, continuously measured and recorded HR, RR, Tskin, body position, and accelerometry. A Sensor Electronic Module (SEM) integrated within the belt, recorded Tskin via infrared thermometry, as well as saved all other recordings for later analyses. This device weighs 38 g, measures 78 mm × 53 mm × 10 mm, is water resistant, intrinsically safe, and is utilized via a fitted-chest strap, containing a two-lead electrocardiogram located underneath the pectorals (ECG) (256 Hz). The ECG collects cardiovascular data, including HR and rhythm (HRV); however, HRV data analysis is not included in this manuscript. All measures were continuously recorded from before entering the mine up until the belt was removed following the underground competition. This was further analyzed to determine peak and minimum HR and RR values. This device was fitted on participants approximately 10 minutes prior to competition briefing. Energy expenditure and estimated  were estimated from HR (First Beat Technologies Software, Jyväskylä, Finland). Energy expenditure described the physical load of each task performed by team positions and estimated
were estimated from HR (First Beat Technologies Software, Jyväskylä, Finland). Energy expenditure described the physical load of each task performed by team positions and estimated  provided insight on the cardiorespiratory fitness of the participants. RR was measured and recorded via thoracic expansion (around the lower part of the thorax) during breathing.
provided insight on the cardiorespiratory fitness of the participants. RR was measured and recorded via thoracic expansion (around the lower part of the thorax) during breathing.
Core Temperature
Tc was measured via an ingestible thermometric pill (VitalsenseTM, Respironics, Bend, Oregon), which measured Tc every 15 seconds and relayed recordings to the SEM for data storing. This medical-grade capsule has dimensions of 23 mm long × 8.6 mm diameter and weighs 1.6 g and is composed of biocompatible polycarbonate. Current literature involving ingestible Tc pills employs ingestion of 2 hours prior, as described by Hardcastle et al.9
Statistical Analysis
The participants’ characteristics (Table 2) and physiological measures displayed in the tables and figures depict the mean ± SE. Participants were organized by positions (Captain, Vice-Captain, No. 2 person, No. 3 person, and No. 4 person) and tasks (Casualty care: tasks 1 and 3; and Arduous Labor: tasks 2 and 4), unless otherwise specified. Age, weight, body mass index (BMI), and estimated  were not normally distributed, as determined by Shapiro-Wilks test (P < 0.05), thus the Mann–Whitney U test was used to compare the role of the Captain and all other positions (Vice-Captain, No. 2, No. 3, No. 4 persons). Height was normally distributed, as determined by the Shapiro-Wilks (P > 0.05) and thus an independent t test was utilized. There were no statistical differences found between Captain and other positions (Vice-Captain, No. 2, No. 3, and No. 4persons), for any baseline measure (age, height, weight, BMI, HRmax,
were not normally distributed, as determined by Shapiro-Wilks test (P < 0.05), thus the Mann–Whitney U test was used to compare the role of the Captain and all other positions (Vice-Captain, No. 2, No. 3, No. 4 persons). Height was normally distributed, as determined by the Shapiro-Wilks (P > 0.05) and thus an independent t test was utilized. There were no statistical differences found between Captain and other positions (Vice-Captain, No. 2, No. 3, and No. 4persons), for any baseline measure (age, height, weight, BMI, HRmax,  ), see Table 1.
), see Table 1.
TABLE 2.
Participant Characteristics (n = 76) Across All Tasks
| Total (n = 76) | Captain (n = 15) | Vice (n = 15) | No. 2 (n = 16) | No. 3 (n = 15) | No. 4 (n = 15) | |
| Age, y | 36.5 ± 0.70 | 37.5 ± 1.73 | 35.2 ± 1.55 | 35.4 ± 1.01 | 36.0 ± 1.16 | 38.5 ± 2.17 |
| Height, m | 1.8 ± 0.01 | 1.8 ± 0.02 | 1.8 ± 0.02 | 1.8 ± 0.02 | 1.7 ± 0.02 | 1.8 ± 0.02 |
| Weight, kg | 87.5 ± 1.65 | 90.4 ± 4.29 | 94.4 ± 3.87 | 82.8 ± 3.13 | 83.0 ± 3.74 | 87.0 ± 2.92 |
| BMI, kg m−2 | 27.8 ± 0.39 | 28.7 ± 1.20 | 29.2 ± 0.88 | 26.0 ± 0.6 | 26.8 ± 0.88 | 28.2 ± 0.53 |
| HRmax* predicted, bpm | 182 ± 1 | 182 ± 1 | 183 ± 1 | 183 ± 1 | 183 ± 1 | 181 ± 2 |
| Estimated ,† ml min−1 kg−1 (n = 70) | 45.4 ± 1 | 43.6 ± 1.66 | 44.1 ± 1.21 | 47.7 ± 0.47 | 46.4 ± 0.80 | 44.9 ± 0.83 |
*HRmax predicted was derived from the equation 208 – age × 0.7.34
†Highest value from all conditions during the IMRC; derived from Firstbeat Analysis Software via HRV data. BMI, body mass index; HR, heart rate; bpm: beats per minute; HRV, heart rate variability; IMRC, International Mine Rescue Competition; , the maximum volume of oxygen the person can utilize, measured in millilitres, per minute, per kilogram body weight.
Data from the Equivital Life Monitor for two participants were lost due to equipment malfunction, resulting in a final sample size of 74 participants. However, these two participants produced good quality data from the ingestible Tc pill, and therefore were included for the Tc data analysis. Data from three participants for the ingestible Tc pill were lost due to equipment malfunction, resulting in a final sample size of 54 participants for the ingestible thermometric Tc pill.
Linear mixed models were performed on all physiological variables across positions (Captain vs other positions and tasks Casualty Care vs Arduous Tasks) with Scheffe post hoc tests where needed. Significance was accepted at P < 0.05. All results were analyzed using STATA version 15 (Statacorp LLC, College Station, TX).
RESULTS
Heart Data
Position
The HRmean for all participants during the four tasks was 143 ± 1 bpm, representing 78.6% of APMHR (Fig. 1A). Captains reported the lowest HRmean (135 ± 3 bpm) compared with Vice-Captain (149 ± 3 bpm, P = 0.020) and No. 2 persons (147 ± 3 bpm, P = 0.044). The HRpeak for all participants was 172 ± 1 bpm, which translates to an APMHR of approximately 94.5% (Fig. 1B). Captains (161 ± 3 bpm) reported the lowest HRpeak when compared with Vice-Captain (177 ± 3 bpm, P = 0.002); No. 2 persons (173 ± 3 bpm, P = 0.019); No. 3 persons (172 ± 2 bpm, P = 0.023); and No. 4 persons (176 ± 2 bpm, P = 0.002).
FIGURE 1.
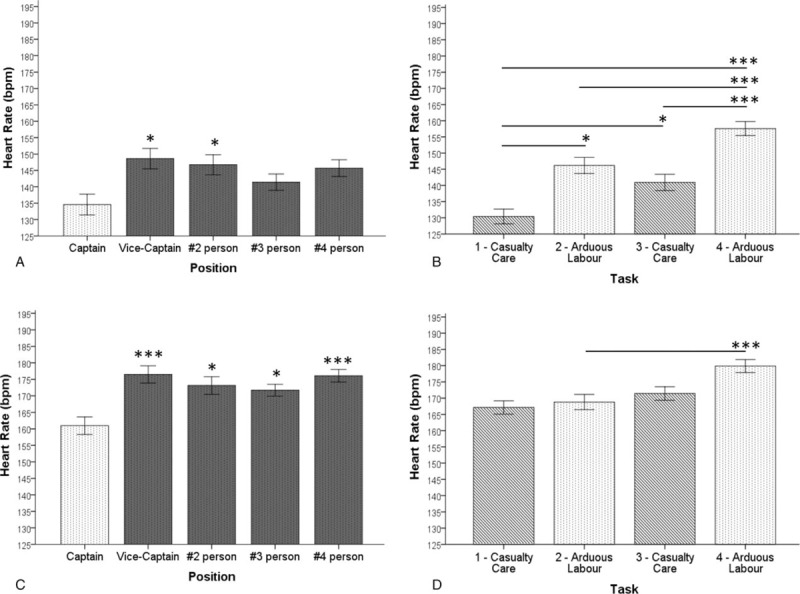
(A) Mean heart rate for all positions across all tasks; (B) mean heart rate for each task across all participants; (C) peak heart rates for each position across all tasks; (D) peak heart rates for each task across all participants; significance was accepted at P < 0.05 (∗P < 0.05, ∗∗P < 0.01, and ∗∗∗P < 0.005).
Task
Overall, HRmean values were high for all tasks ranging from 71.4% to 86.8% APMHR for all participants, which reflect vigorous intensity (Fig. 1C). Task 4 (158 ± 2 bpm) reported higher values than task 1 (130 ± 2 bpm, P = 0.000); task 2 (146 ± 3 bpm, P = 0.002); and task 3 (143 ± 3, P = 0.002). Also, task 3 reported higher values than task 1 (P = 0.011) and task 2 was also higher than task 1 (P = 0.011). Overall, HRpeak values were high for all tasks ranging from 91.8% to 98.9% of the calculated APMHR for all participants (Fig. 1D). Only task 4 (180 ± 2 bpm) reported higher HRpeak when compared with task 2 (169 ± 2 bpm, P = 0.000).
Respiration Rate
Position
RRmean for all participants was 34 ± 0 rpm (Fig. 2A). Captains (31 ± 1 rpm) reported lower RRmean when considering mean of all tasks when compared with the Vice-Captain (35 ± 1 rpm, P = 0.019), No. 2 person (35 ± 1 rpm, P = 0.024), and No. 3 person (35 ± 1 rpm, P = 0.012). RRpeak for all participants was 44 ± 0 rpm (Fig. 2B). Captains (41 ± 1 rpm) reported lower RRpeak when compared with No. 3 person (45 ± 1 rpm, P = 0.035) and No. 4 person (45 ± 1 rpm, P = 0.037).
FIGURE 2.
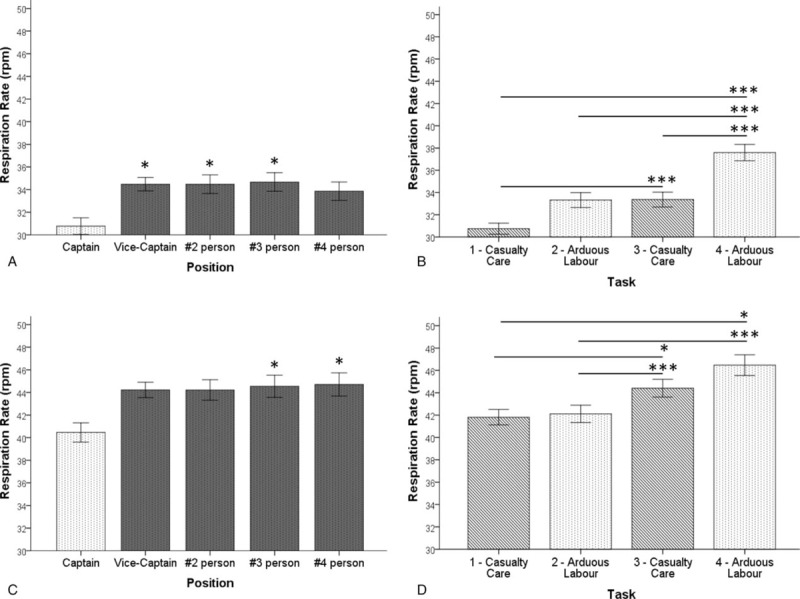
(A) Mean respiration rate for each position across all tasks; (B) mean respiration rate for each task across all participants; (C) peak respiration rate for each position across all tasks; (D) peak respiration rate for each task across all participants; significance was accepted at P < 0.05 (∗P < 0.05, ∗∗P < 0.01, and ∗∗∗P < 0.005).
Task
Overall, RRmean values were high for all tasks ranging from 31 ± 1 to 38 ± 1 rpm (Fig. 2C). Task 4 (38 ± 1 rpm) reported higher RRmean than all other tasks, Task 1 (31 ± 1 rpm, P = 0.000); Task 2 (33 ± 1 rpm, P = 0.000); and Task 3 (33 ± 1 rpm, P = 0.000). Also, Task 3 reported higher RRmean when compared with Task 1 (P = 0.000). Overall, RRpeak for all tasks was 44 ± 0 rpm (Fig. 2D). Task 4 (47 ± 1 rpm) reported higher RRpeak when compared with Task 1 (42 ± 1 rpm, P = 0.037) and task 2 (42 ± 1 rpm, P = 0.000). Task 3 (45 ± 1 rpm) also reported higher RRpeak from task 1 (P = 0.023) and task 2 (P = 0.000).
Total Energy Expenditure and Oxygen Consumption
Position
There were no significant differences reported for EE between positions. The lowest reported mean EE was Captains (11.0 ± 0.60 kcal min−1 or 769 ± 42 W) (1 Watt = 0.0143 kcal min−1). The reported mean EE for positions was Vice-Captains (13.2 ± 0.63 kcal min−1 or 923 ± 42 W); No. 2 persons (12.8 ± 0.76 kcal min−1 or 895 ± 56 W), No. 3 persons (11.6 ± 0.52 kcal min−1 or 811 ± 35 W); and No. 4 persons (12.3 ± 0.46 kcal min−1 or 860 ± 35 W). The  value for all positions was 27.2 ± 0.45 mL kg−1 min−1, which translates to approximately 60%
value for all positions was 27.2 ± 0.45 mL kg−1 min−1, which translates to approximately 60%  effort (Fig. 3A). Captains (24.1 ± 1.18 mL kg−1 min−1) reported lower
effort (Fig. 3A). Captains (24.1 ± 1.18 mL kg−1 min−1) reported lower  when compared with No. 2 person (29.5 ± 1.03 mL kg−1 min−1, P = 0.005), No. 3 person (27.6 ± 0.88 mL kg−1 min−1, P = 0.039), and No. 4 person (27.8 ± 0.87 mL kg−1 min−1, P = 0.037).
when compared with No. 2 person (29.5 ± 1.03 mL kg−1 min−1, P = 0.005), No. 3 person (27.6 ± 0.88 mL kg−1 min−1, P = 0.039), and No. 4 person (27.8 ± 0.87 mL kg−1 min−1, P = 0.037).
FIGURE 3.
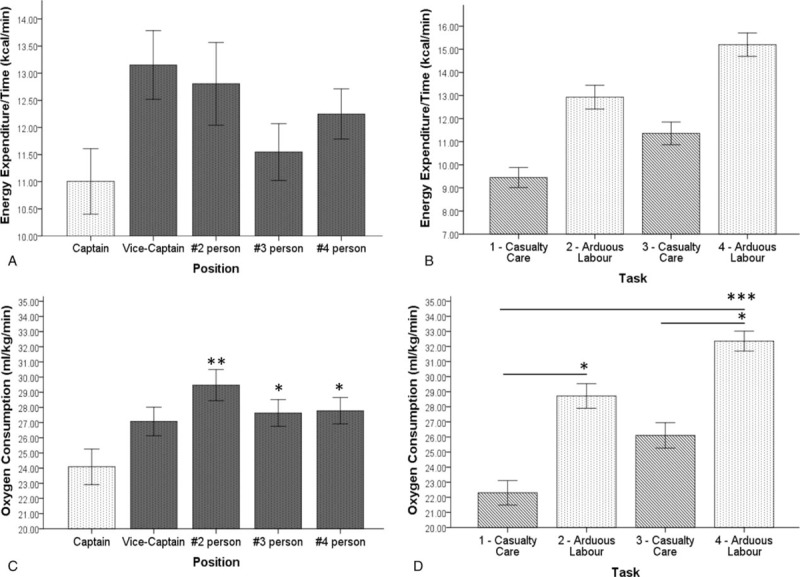
(A) Mean energy expenditure for each position across of all tasks; (B) mean energy expenditure for each task across all participants; (C) mean oxygen consumption for each position across all tasks; (D) mean oxygen consumption for each task across all participants; significance was accepted at P < 0.05 (∗P < 0.05, ∗∗P < 0.01, and ∗∗∗P < 0.005).
Task
There were no statistically significant differences reported for EE between tasks. The lowest reported mean EE was 9.5 ± 0.43 kcal min−1 or 661 ± 28 W for task 1. The highest reported mean EE was 15.2 ± 0.50 kcal min−1, or 1063 ± 35 W for task 4. The mean EE for task 2 was 12.9 ± 0.51 kcal min−1 or 902 ± 35 W, and for task 3 was 11.4 ± 0.50 kcal min−1 or 797 ± 35 W.  values were high for all tasks ranging from 22.3 ± 0.81 to 32.4 ± 0.66 mL kg−1 min−1, which translate to 49.1% to 71.4% of the estimated
values were high for all tasks ranging from 22.3 ± 0.81 to 32.4 ± 0.66 mL kg−1 min−1, which translate to 49.1% to 71.4% of the estimated  (Fig. 3D). Task 4 (32.4 ± 0.66 mL kg−1 min−1) was higher than task 1 (22.3 ± 0.81 mL kg−1 min−1, P = 0.001) and task 3 (26.1 ± 0.84 mL kg−1 min−1, P = 0.015). Also, task 2 (28.7 ± 0.81 mL kg−1 min−1) reported higher
(Fig. 3D). Task 4 (32.4 ± 0.66 mL kg−1 min−1) was higher than task 1 (22.3 ± 0.81 mL kg−1 min−1, P = 0.001) and task 3 (26.1 ± 0.84 mL kg−1 min−1, P = 0.015). Also, task 2 (28.7 ± 0.81 mL kg−1 min−1) reported higher  than task 1 (P = 0.024).
than task 1 (P = 0.024).
Temperature
Position
Tc mean for all participants was 38.3 ± 0.04 °C when considering mean of all tasks (Fig. 4A). The only difference for Tc mean reported was for Captains (38.0 ± 0.09 °C) when compared with No. 4 persons (38.5 ± 0.10 °C, P = 0.005). Tc peak for all participants when considering the mean of all tasks was 38.5 ± 0.04 °C (Fig. 4B). Captains (38.2 ± 0.08 °C) reported lower Tc peak when compared with Vice-Captains (38.6 ± 0.10 °C, P = 0.040) and No. 4 persons (38.7 ± 0.10 °C, P = 0.002). Tc peak for remaining positions was: No. 2 persons 38.5 ± 0.08 °C; and No. 3 persons 38.6 ± 0.08 °C. Tskin for all participants were 37.2 ± 0.06 °C when considering mean of all tasks (Fig. 4E). Captains (36.8 ± 0.13 °C) reported lower Tskin compared with Vice-Captains (37.2 ± 0.13 °C, P = 0.013), No. 2 persons (37.6 ± 0.10 °C, P = 0.001), and No. 3 persons (37.4 ± 0.10 °C, P = 0.002). Tskin peak for all participants were 37.7 ± 0.48 °C when considering all tasks (Fig. 4G). Captains (37.3 ± 0.12 °C) reported lower Tskin peak compared with Vice-Captain (37.8 ± 0.11 °C, P = 0.001), No. 2 person (38.0 ± 0.08 °C, P = 0.000), No. 3 person (37.9 ± 0.08 °C, P = 0.000), and No. 4 person (37.7 ± 0.12 °C, P = 0.005).
FIGURE 4.
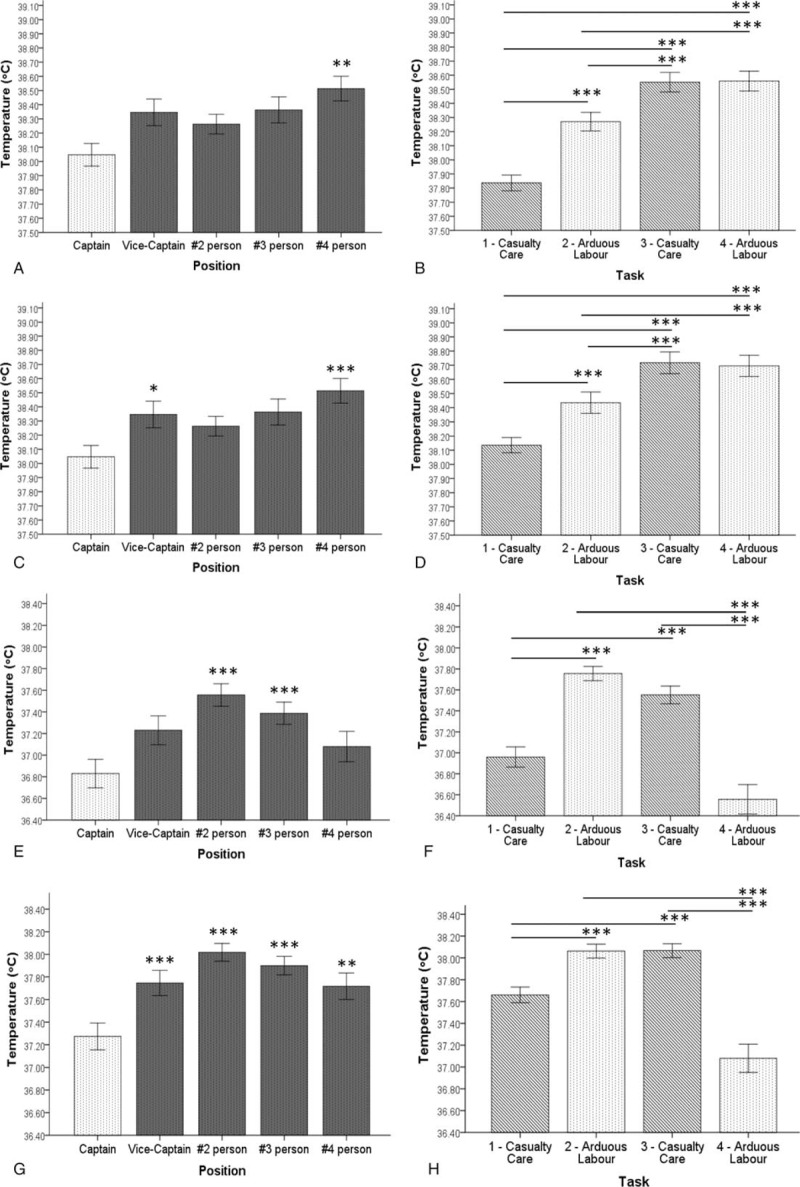
(A) Mean core temperature for each position across all tasks; (B) mean core temperature for each task across all participants; (C) peak core temperature for each position across all tasks; (D) peak core temperature for each task across all participants; (E) mean skin temperature for each position across all tasks; (F) mean skin temperature for each task across all participants; (G) peak skin temperature for each position across all tasks; (H) mean of all peak skin temperature for each task across all participants; significance was accepted at P < 0.05 (∗P < 0.05, ∗∗P < 0.01, and ∗∗∗P < 0.005).
Task
For Tc mean, task 4 (38.6 ± 0.07 °C) was higher than tasks 1 (37.8 ± 0.06 °C, P = 0.000) and task 2 (38.3 ± 0.07 °C, P = 0.000). Task 3 (38.6 ± 0.07 °C) was higher than tasks 1 (P = 0.000) and task 2 (P = 0.000). Additionally, task 2 was higher than task 1 (P = 0.000).
For Tc peak, task 4 (38.7 ± 0.07 °C) was higher than tasks 1 (38.1 ± 0.05 °C, P = 0.000) and task 2 (38.4 ± 0.08 °C, P = 0.000). Task 3 (38.7 ± 0.08 °C was higher than tasks 1 (P = 0.000) and task 2 (P = 0.000). Additionally, task 2 was also higher than task 1 (P = 0.000).
For Tskin, task 4 (36.6 ± 0.13 °C) was higher than tasks 3 (37.6 ± 0.08 °C, P = 0.000) and task 2 (37.8 ± 0.07 °C, P = 0.000). Task 3 was higher than task 1 (37.0 ± 0.10 °C, P = 0.000). Also, task 2 was higher than task 1 (P = 0.000).
Tskin peak, task 4 (37.1 ± 0.13 °C) was higher than task 2 (38.1 ± 0.06 °C, P = 0.000) and task 3 (38.1 ± 0.06 °C, P = 0.000). Task 3 was higher than task 1 (37.7 ± 0.07 °C, P = 0.000). Additionally, task 2 was higher than task 1 (P = 0.000).
DISCUSSION
To our knowledge, this is the first study to record physiological measures during an accurate enactment of a mine rescue simulation, in an operational, underground mine. It is also the first to assess the influence of team position and task on physiological loading of mine rescue participants during this simulated emergency. We employed objective methods to describe the following physiological measures: HR, RR, EE,  , Tskin, and Tc to gain insights on physiological responses and risk of heat-related events during a simulated mine rescue emergency. Captains displayed significantly lower physiological loads, except for EE, when compared with other positions. Both arduous labor and casualty care tasks required high physical demand, although arduous labor required higher demands with significantly higher HR, RR, and
, Tskin, and Tc to gain insights on physiological responses and risk of heat-related events during a simulated mine rescue emergency. Captains displayed significantly lower physiological loads, except for EE, when compared with other positions. Both arduous labor and casualty care tasks required high physical demand, although arduous labor required higher demands with significantly higher HR, RR, and  measures. Finally, all participants displayed elevated Tskin and Tc values. Our results highlight that all positions, including Captains, are performing very strenuous work during all mine rescue tasks performed in hot and humid conditions, putting them at risk for both heat stroke and a cardiovascular event.
measures. Finally, all participants displayed elevated Tskin and Tc values. Our results highlight that all positions, including Captains, are performing very strenuous work during all mine rescue tasks performed in hot and humid conditions, putting them at risk for both heat stroke and a cardiovascular event.
Task-Specific Demands
Simulated mine rescue-related tasks examined in similar studies (eg, shovel, casualty-carry, walk, etc) have documented the intense workload required to perform these tasks in comparison with the implementation of allotted rest intervals.8–10 Stewart et al8 reported mean %APMHR of 91% for the duration of a 9-minute, simulated work-circuit comprised of: incremental casualty carry, coal shoveling, and hose drag. Similar findings from Hardcastle et al9 highlighted mine rescuers performing mean workloads of 538 W for an average of 66 minutes that resulted in mean Tc of 38.14 °C in 10 individuals; this study was performed in an operational, shallow mine with much cooler conditions, without realistic mining conditions (Tdrybulb = 16.9 °C; Twetbulb = 14.9 °C); compared with the present study.
The simulated mine rescue competition in this study involved four primary tasks; which we sub-categorized into Casualty Care (Tasks 1 and 3) and Arduous Labor (Tasks 2 and 4). These tasks were developed by specialists in mine rescue (OMR), and reflect frequently occurring emergencies. Both laborious and casualty care tasks required a high physical demand, where arduous labor displayed higher HR, RR, and  measures. The inability to rest before the beginning of Tasks 2, 3, and 4, led to a sustained or greater HR and RR. In addition, although casualty care involves kneeling and seemingly a chance to recover, participants remained in hot ambient conditions while wearing approximately 40 lbs of gear. These were not favorable conditions for adequate recovery and thus impacted physiological responses. Both HRpeak and RRpeak increased during task 3, showing higher values than task 2 (arduous labor). During task 3, the casualty was impaled by a steel bar through their abdomen and anecdotally, was very realistic and distressing for the competitors. This likely contributed to the increase in HR and RR, via activation of the sympathetic system due to the visual stressors.17
measures. The inability to rest before the beginning of Tasks 2, 3, and 4, led to a sustained or greater HR and RR. In addition, although casualty care involves kneeling and seemingly a chance to recover, participants remained in hot ambient conditions while wearing approximately 40 lbs of gear. These were not favorable conditions for adequate recovery and thus impacted physiological responses. Both HRpeak and RRpeak increased during task 3, showing higher values than task 2 (arduous labor). During task 3, the casualty was impaled by a steel bar through their abdomen and anecdotally, was very realistic and distressing for the competitors. This likely contributed to the increase in HR and RR, via activation of the sympathetic system due to the visual stressors.17
Our results demonstrated that 31 (41.9%) participants exceeded 100% of the APMHR (182 bpm), during tasks 2 and 4. Tasks 1 and 3 also demonstrated moderate-vigorous intensity with 70% to 85% of APMHR. These values are much higher than previous findings8–10 Given that previous research examined mine tasks over a short duration, with scheduled rest breaks, this is not surprising.10,13 In our study, participants performed work for approximately 2 hours, where “rest” consisted of either walking or kneeling for brief periods (less than 5 minutes). This pattern is representative of mine rescue work, unlike that observed in previous literature.3 In comparison, Stewart et al,8 utilized a job-task circuit composed of 9 minutes of work followed by 24 minutes of rest, in which they still reported APMHR of nearly 100%.8 Future research should focus on methods to improve or maximize opportunities to rest (eg, hydration, rest protocol, or utilize back-up teams to reduce rescue mission time).
Participants’ mean and peak Tc were higher in task 3 compared with tasks 1 and 2, but not different from task 4. Whereas, mean and peak Tskin depicted a decrease from task 3 to task 4. This can be attributed to a decrease in ambient conditions (Table 2). Core temperature is less influenced by ambient conditions compared with Tskin, which is in direct contact with the environment.17 The resulting gradient between Tskin and Tc would improve the ability to dissipate heat and balance heat gained versus heat lost, ultimately stagnating the rise in Tc.17 Nonetheless, 30 of the 54 participants reported measures of mean Tc at 38.6 °C or above and the highest Tc recorded in the competition was 39.88 °C, which nearly meets the criteria (40 °C) for heat stroke as defined by the Taylor et al.18
A study by Varley,19 in mine rescuers during regular training, showed that, following an increase in Tc active cooling did not begin until approximately 25 minutes following training. This is significant because tracking Tc is not currently practiced during mine rescue. Current post-emergency policies include 6 hours of rest between shifts, and 24 hours of rest for those exposed to extreme heat.3 When emergencies exceed 24 hours, doctors must be made available 24 hours a day and each team member must be examined by the doctor at least once a day.3 During competitions paramedics are made available and remain at the end of the scenario to examine any individual experiencing any heat illness symptoms (eg, weakness, nausea, cramps, etc) (T. Hanley, Ontario Mine Rescue: personal communication, December 15, 2017). However, closer attention immediately following a rescue event should be given to all mine rescue personnel, including testing for ongoing heat strain. This monitoring should continue for at least an hour following team-exit from the mine after an emergency. Paramedics or doctors should be present at the exit, and examine all workers for visible symptoms of heat illness (eg, excessive sweating, lack of sweating, red skin, complacency, etc) and to make certain they are rehabilitating properly (eg, drinking plenty of water, resting, etc). Future research should focus on practices to actively cool rescuers throughout an emergency and immediately upon exit from the mine, which would be beneficial and potentially life saving.
Team Position Demands
For HRmean, Captains were different from Vice-Captain and No. 2 person (P < 0.05), but not different from No. 3 person and No. 4 person. Other physiological measures that followed this pattern included RRmean, RRpeak, and oxygen consumption, in which the Captain differed from a few positions, but not all. We hypothesize this is because the Captains as a group were often not as physically fit as the other team members which would result in eliciting higher physiological measures when performing lower intensity work.20 On the other hand, for HRpeak, Captains displayed lower values than all other positions; this may be attributed to the difference in responsibilities of roles during a competition. However, in real-life emergencies, Captains will help for the best outcome and therefore could elicit higher physiological responses.
Although Captains displayed lower physiological measures, except for EE, compared with other positions, Captains’ HRmean for the duration of the competition was 74.2% of APMHR, which still reflects vigorous physical activity. Considering HR,  , and EE are linearly correlated and there is no difference in EE, we suggest this may be due to the calculation used by Firstbeat Software (Firstbeat Technologies, Jyväskylä, Finland) to calculate values, which was not provided. Captains are required to wear the same PPE (approximately 22 kg) and walk the same distance, so it is expected that the Captain should have sufficient cardiovascular and muscular endurance to keep up with other members. Concern regarding a fitness standard is that it may prevent these members from active duty: causing a significant loss in experience and expertise.3 Captains are not lifting or carrying heavy equipment and casualties, so in theory, should not be required to meet the same muscular strength standard as other members. However, in a circumstance when another member is injured, the Captain must fill their role, and would be required to perform heavy lifting. Therefore, a multi-faceted fitness standard that encompasses all aspects of fitness (eg, muscular strength and endurance, cardiovascular endurance) should be implemented and should be the same for all positions.
, and EE are linearly correlated and there is no difference in EE, we suggest this may be due to the calculation used by Firstbeat Software (Firstbeat Technologies, Jyväskylä, Finland) to calculate values, which was not provided. Captains are required to wear the same PPE (approximately 22 kg) and walk the same distance, so it is expected that the Captain should have sufficient cardiovascular and muscular endurance to keep up with other members. Concern regarding a fitness standard is that it may prevent these members from active duty: causing a significant loss in experience and expertise.3 Captains are not lifting or carrying heavy equipment and casualties, so in theory, should not be required to meet the same muscular strength standard as other members. However, in a circumstance when another member is injured, the Captain must fill their role, and would be required to perform heavy lifting. Therefore, a multi-faceted fitness standard that encompasses all aspects of fitness (eg, muscular strength and endurance, cardiovascular endurance) should be implemented and should be the same for all positions.
When referring to Tskin and Tc, Captains were different from most other positions. In agreement with Hardcastle et al,9 the metabolic work performed (mean of 856.6 W for all positions) during the rescue event was sufficient to produce mean Tc values of 38.31 °C for all positions, and 38.10 °C for Captains. This is important as Tc of 38.0 °C is associated with an impaired ability to make decisions, and impaired reaction time.15,21 Captains are responsible for making decisions on behalf of the team, as well as any casualties encountered in the mine, making heat strain a major concern.3 Based on the results from Racinais et al,21 the Captain was making impaired decisions in the IMRC (Tc > 38.0 °C). As for other positions, the highest reported Tc was 39.88 °C, which is nearly considered heat stroke, and if not treated immediately can be fatal.19 Furthermore, at a Tc of 38.6 °C and above, physical heat strain has begun and, if not mitigated, will progress to acute heat illness and eventually the life-threatening condition of heat stroke.15
Heat stroke is a recognized serious risk for mine rescue, and has previously caused the death of several mine rescuers.19 However, cardiovascular disease (CVD) is also an important cause of death among miners22–24 and should be given equal consideration when developing prevention strategies for mine rescue work. Over the last decade, our understanding of CVD among structural firefighters has significantly improved and provides insight into potential preventive strategies for mine rescue. Mine Rescue workers perform under similar circumstances as structural firefighters and the physiology of cardiovascular arousal and other changes that occur in association with acute firefighting activities have been well characterized.25–29 Also, like mining, despite the strenuous nature of emergency duty, firefighters’ prevalence of low fitness, obesity, and other CVD risk factors are high.30,31 Statistical analyses have shown that on-duty CVD events do not occur at random in the fire service. They are more frequent at certain times of day, certain periods of the year, and are overwhelmingly more frequent during strenuous duties compared with non-emergency situations.27 Moreover, as expected, on-duty CVD events occur almost exclusively among susceptible firefighters with underlying CVD.27 These findings suggest that preventive measures with proven benefits be applied aggressively to workers.
Based on the descriptive data from this study and the literature around firefighting, we would make three recommendations for Mine Rescue programs globally. These recommendations are outlined below.
Recommendations for Mine Rescue
Mandatory Fitness Standard
First, as recommended in the Mining Health, Safety and Prevention Review (2015),5 we concur that a fitness standard should be developed for mine rescue workers. However, given the specific fitness requirements outlined in Jamnik et al6 for Canada, we would recommend a novel approach. Specifically, we recommend the development of a mandatory fitness program whereby “monitoring participation” in the program be a key aspect of achieving the fitness standard. Personalized fitness goals be set at the outset of the program start, including targets for: aerobic fitness (VO2max), percentage body fat, core body strength, and grip strength, with periodic testing to measure progress toward and maintenance of goals. Given the high heart rates reported in this study, a primary concern for workers (in addition to the risk of heat stroke) is that they would suffer a cardiac event during or after the rescue. Therefore to mitigate both risks, regular training, including an aerobic component, would protect workers from these outcomes.28–31 We recommend that body composition, with the goal to reduce total percentage fat, be included for workers, as higher body fat is associated with enhanced body heat retention.32 Core and grip strength are recommended as components of the fitness program to help protect workers from common physical injuries including slip/trip and back injuries. Enhanced core and grip strength have been shown to be protective for these types of injuries.33,34 Lastly we recommend that workers include regular training (three to five times per week) targeting their respiratory muscles to offset the negative impacts35–37 of wearing the self-contained breathing apparatus.
Furthermore, mine rescue workers should continue to have entry-level medical evaluations, but also institute periodic medical and fitness evaluations, and require return-to-work evaluations after any significant illness. A combination of a fitness evaluations (eg,  testing, grip strength, etc) and job simulation tasks (ie, rescue simulations) for a hybrid physical standard would be the best approach.6 Fitness evaluation would provide insight regarding the worker's general fitness and can be used to evaluate achievement of personal goals; this in combination with the successful completion of simulated rescue missions would, in our opinion, better safeguard workers. It is possible to consider different fitness standards based on team role; Captains might benefit from a lower standard for muscular strength, as they are not, under normal circumstances, involved in lifting tasks; however, based on the results from this study, we think they should be held to the same aerobic standard.
testing, grip strength, etc) and job simulation tasks (ie, rescue simulations) for a hybrid physical standard would be the best approach.6 Fitness evaluation would provide insight regarding the worker's general fitness and can be used to evaluate achievement of personal goals; this in combination with the successful completion of simulated rescue missions would, in our opinion, better safeguard workers. It is possible to consider different fitness standards based on team role; Captains might benefit from a lower standard for muscular strength, as they are not, under normal circumstances, involved in lifting tasks; however, based on the results from this study, we think they should be held to the same aerobic standard.
Finally, on the basis of the overwhelming evidence supporting markedly higher relative risks of on-duty death and disability among structural firefighters with established coronary heart disease,38–40 mine rescue workers, with clinically significant coronary heart disease should be restricted from participating in the mine rescue program.
Body-Worn Physiological Monitoring
Our second recommendation is that Mine Rescue incorporates body-worn monitors, ideally capable of relaying physiological measures in real-time to the Briefing Officer during all rescue and simulation training events. The Briefing Officer should, in the future, use these indices to decide, in consultation with the Captain, whether to extract a team during a rescue for safety reasons. We do not think the current standard of regular health check-ins with the Captain, based on verbal confirmation from workers regarding their personal fitness to continue and visual cues is sufficient. We argue that given the high risk of a heat stress event and the poor conditions (eg, smoke, PPE obstruction) for visually identifying a problem, a better method needs to be put in place to proactively protect these workers. Although various personal monitoring devices exist, we would note that the Equivital from Hidalgo was well tolerated by all participants in this study, and it is the only wearable (to our knowledge) that is intrinsically safe for mine use while incorporating all the physiological measures we would recommend be monitored in real time (heart rate, respiratory rate, heart-rate variability, skin temperature, and body position). We recognize that this wearable does not measure true core temperature (only estimates it based on skin temperature); but we do not think the ingestible core temperature method is feasible, nor recommended, for regular use as a component of mine rescue work. Skin temperature in relation to heart rate is the best proxy measure for field use in first responders, including Mine Rescue workers, at this time.41–43
Heat Exposure Health Screening Standard
Lastly we recommend that upon exit from an emergency rescue and from simulated training exercises all mine rescue workers be automatically screened and treated for heat strain. It is clear based on the data from this study that many of the participants were suffering from some degree of heat strain when they exited the mine. Future studies should incorporate a survey question to capture this data and should continue to monitor the core temperature of participants after the simulation is over. We recommend that Mine Rescue organizations globally develop a standard screen practice, potentially including a rectal temperature measure upon exit from the emergency rescue or training simulation. These data should be maintained, collected, and studied to help develop better recovery practices for these workers; we would recommend that Ontario Mine Rescue, or similar bodies oversee this data. We would also recommend that workers be treated upon exit from the emergency as if they have heat exhaustion, as a component of the prevention process. As a measure to prevent the further progression to heat stroke, this would include immediate hydration and rapid efforts to cool the worker, ideally this would include water immersion of the torso.44,45 In addition, a recovery standard should be developed that includes mandatory 24 hour time-off from work after all rescues and training simulations. Currently, the Mine Rescue Handbook states: no one should be permitted to take a second shift until they have had at least 6 hours rest. Personnel exposed to extreme heat, and worked under the time limits of the OMR Heat Exposure Standard, must have 24 hours rest.3 This Recovery Standard should expand on the guidelines for the worker to follow, including: what symptoms to watch for, beverage and food consumption practices, physical activity engagement, and sleep. Future studies should verify the success of these programs in preventing heat stress and in enhancing worker recovery.
Other Considerations/Recommendations
Notably, we have not made any recommendations for practice regarding acclimatization, as a means to protect the workers from heat strain. The literature supports the use of acclimatization as one way to protect workers from a heat event.46 However despite the potential for workers to become acclimatized at work, due the rapid loss of this protection (within 3–5 days)46 in practice, it is difficult to maintain. Anecdotally, mine rescue workers told us that they were not acclimatized to the heat for the competition and unless both workers and workplaces wanted to create shift schedules to specifically address this effect or develop a program for daily exposure (eg, via simulated high temperature exposure) we do not see this as a practical approach for Canadian Mine Rescue workers at this time.
Other factors should be considered in future research to further protect these workers from injury and heat strain including: pre-fatigue, that is, worker activities just prior to emergency call; and an inability to sufficiently hydrate prior to and during an actual emergency.
Limitations
Although this competition provided a unique opportunity to study mine rescuers performing mine rescue tasks in an underground mine while participating in scenarios prepared by mine rescue experts and based on previous mining disasters, there are some limitations to this research. First, the scenarios created were part of a competition, not a true emergency, thus their true physiological data remain unknown. In addition because it was a competition participants had knowledge of “when” they were competing; and therefore had time to prepare physically. For example, they could ensure sufficient hydration and ample rest the night prior. Alternatively, this may also have had negative consequences on their performance, for example, this may have affected their ability to sleep due to nervousness. Second, a baseline collection of physiological responses was not possible due to scheduling of the event and the arrival times of teams. We could not influence or modify the schedule of the IMRC to fit our needs, as there were other aspects of the competition before and following the underground scenario. We were given a strict allocated time to get anthropometric measures the day prior to the event, and were unable to gather baseline physiological data. Third, we were unable to conduct a post competition survey to assess perceptions of heat illness and perceived exertion, again due to time constraints and language barriers. We never attempted to measure symptoms of heat illness after the competition; however, extrapolating from the results of Tc and HR, it is likely participants experienced them. Therefore, future research should utilize district and provincial competitions to allow ample time to collect baseline data (eg, HR, RR, Tc, etc) and post competition data (eg, heat illness symptoms and perceived exertion).
CONCLUSION
In conclusion mine rescue work is highly demanding with high risk of a heat stress or a cardiovascular event. Workers need to commit to a regular fitness program to offset these risks and government and industry needs to support this commitment. In addition, workers should be monitored throughout a rescue and training simulation for heat strain to safeguard their health. Lastly workers should be tested and treated for heat strain after every rescue and training simulation; this should include a planned recovery program for the worker. These changes will have practical implications on industry, but should also improve the overall health of the organization, which could have other benefits.
Supplementary Material
Acknowledgments
The authors would like to acknowledge the Ministry of Labour for equipment funding support, Workplace Safety North, and Ontario Mine Rescue for coordinating the research and organizing opportunities for participant recruitment as well as their help and expertise in interpreting the data in context of the mine rescue practice; in particular: Ted Hanley, Tim Ebbinghaus, and Shawn Rideout. They would acknowledge the Northern Ontario Centre for Advanced Technology (NORCAT) for their assistance with putting the technology in place in the mine and assisting with the data collection throughout the mine competition: in particular they would like to acknowledge Ed Wisniewski, Shawn Peplinski, Andrew Kostuik, and Eric Daoust. They would also thank Emily Jago, Brandon Vance, and Jordon Nixon for assisting with the collection of the data. Lastly, thank you to all the participants for giving their time to this study. Please note that this manuscript formed the basis for the Masters Dissertation for Mr. Justin Konrad.47
Footnotes
Clinical significance: Mine Rescue was identified as a priority issue by the Ministry of Labour's Mining Health, Safety and Prevention Review (2015). Recommendations include instituting a fitness standard and mitigating heat stress. This study is the first step in enacting these recommendations and was supported by the International Mine Rescue Body.
Funding sources: None.
The authors report no conflicts of interest.
REFERENCES
- 1.Health and Safety Report: Mine Rescue Heat Stress Report. 2014; North Bay, ON, Canada: Workplace Safety North, 1-46. [Google Scholar]
- 2.Workplace Health and Safety Snapshot for Ontario Mining Sector in 2015. 2015; North Bay, Canada: Workplace Safety North, 2. [Google Scholar]
- 3.Handbook of Training in Mine Rescue and Recovery Operations. 2015; North Bay, ON Canada: Workplace Safety North, 1-252. [Google Scholar]
- 4.Gryska A. IMRB: Foundation for Global Mine Rescue Standards. Conference Proceedings: 2013 Mining Health and Safety Conference. Available at: https://www.workplacesafetynorth.ca/resources/imrb-foundation-global-mine-rescue-standards-0 Accessed August 17, 2018. [Google Scholar]
- 5.Mining Health, Safety and Prevention Review. Toronto, Canada: Ontario Ministry of Labour; 2015. [Google Scholar]
- 6.Jamnik V, Gumienak R, Gledhill N. Developing legally defensible physiological employment standards for prominent physically demanding public safety occupations: a Canadian perspective. Eur J Appl Physiol 2013; 113:2447–2457. [DOI] [PubMed] [Google Scholar]
- 7.Emergency Response and Mine Rescue. Toronto, Canada: Government of Ontario, Ministry of Labour; 2015. [Google Scholar]
- 8.Stewart IB, McDonald MD, Hunt AP, Parker TW. Physical capacity of rescue personnel in the mining industry. J Occup Med Toxicol 2008; 3:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hardcastle SG, Reardon FD, Kenny GP, Allen C. Assessing the Work Intensity of Mine Rescue Activities and its Relevance in Applying Heat Stress Management Protocols. 9th International Mine Ventilation Congress. New Delhi, India; 2009: 1–13. [Google Scholar]
- 10.Kampmann B, Bresser G. Heat stress and flame protective clothing in mine rescue brigadesmen: inter- and intraindividual variation of strain. Ann Occup Hyg 1999; 43:357–365. [PubMed] [Google Scholar]
- 11.Kenny G, Stapleton J, Lynn A, Binder K. Heat stress in Canadian deep mechanized mines: Laboratory simulation of typical mining tasks performed in varying environments. 13th International Conference on Environmental Ergonomics. Boston, USA; 2009:441–445. [Google Scholar]
- 12.ACGIH. TLVs and BEIs: Threshold limit values for chemical substances and physical agents, biological exposure indices; 2010. American Conference of Governmental Industrial Hygienists. Cincinnati, OH. [Google Scholar]
- 13.Kenny GP, Vierula M, Maté J, Beaulieu F, Hardcastle SG, Reardon F. A field evaluation of the physiological demands of miners in Canada's deep mechanized mines. J Occup Environ Hyg 2012; 9:491–501. [DOI] [PubMed] [Google Scholar]
- 14.Leong LC, Byrne C, Lee J. Human thermoregulation and measurement of body temperature in exercise and clinical settings. Ann Acad Med Singapore 2008; 37:347–353. [PubMed] [Google Scholar]
- 15.Sessler DI. Temperature monitoring and perioperative thermoregulation. Anesthesiology 2008; 109:318–338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tomaskova H, Jirak Z, Lvoncik S, Buzga M, Zavadilova V, Trlicova M. Health status and physical fitness of mines rescue brigadesmen. Int J Occup Med Environ Health 2015; 28:613–623. [DOI] [PubMed] [Google Scholar]
- 17.Kenney WL, Wilmore JH, Costill DL. Physiology of Sport and Exercise. Champaign, IL: Human Kinetics; 2015. [Google Scholar]
- 18.Taylor NAS, Tipton MJ, Kenny GP. Considerations for the measurement of core, skin and mean body temperatures. J Therm Biol 2014; 46:72–101. [DOI] [PubMed] [Google Scholar]
- 19.Varley F. A study of heat stress exposures and interventions for mine rescue workers. Soc Mining Metallur Explor Trans 2004; 316:135–142. [Google Scholar]
- 20.Aklan C, Robergs R, Kravitz L. Prediction of VO2 max from an individualized submaximal cycle Ergometer protocol. J Exerc Physiol Online 2008; 11:1–17. [Google Scholar]
- 21.Racinais S, Gaoua N, Grantham J. Hyperthermia impairs short-term memory and peripheral motor drive transmission. J Physiol 2008; 586:4751–4762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Weiner J, Barlow L, Sjogren B. Ischemic heart disease mortality among miners and other potentially silica-exposed workers. Am J Ind Med 2007; 50:403–408. [DOI] [PubMed] [Google Scholar]
- 23.Björ BM, Burström L, Eriksson K, Jonsson H, Nathanaelsson L, Nilsson TKF. Mortality from myocardial infarction in relation to exposure to vibration and dust among a cohort of iron-ore miners in Sweden. Occup Environ Med 2010; 67:154–158. [DOI] [PubMed] [Google Scholar]
- 24.Björ B, Burström L, Jonsson H, Nathanaelsson L, Damber L, Nilsson TKF. Fifty-year follow-up of mortality among a cohort of iron-ore miners in Sweden, with specific reference to myocardial infarction mortality. Occup Environ Med 2009; 66:264–268. [DOI] [PubMed] [Google Scholar]
- 25.Ramsden R, Smith J, Turcotte K, et al. Determinants of Injury and Death in Canadian Firefighters: A Case for a National Firefighter Wellness Surveillance System. 2018; Abbotsford, B.C.: BC Injury Research and Prevention Unit, 71. [Google Scholar]
- 26.Angerer P, Kadlez-Gebhardt S, Delius M, Raluca P, Nowak D. Comparison of cardiocirculatory and thermal strain of male firefighters during fire suppression to exercise stress test and aerobic exercise testing. Am J Cardiol 2008; 102:1551–1556. [DOI] [PubMed] [Google Scholar]
- 27.Elpidoforos S, Denise S, Antonios T, Dorothee B, Kales SN. Cardiovascular disease in US firefighters: a systematic review. Cardiol Rev 2018; 19:202–215. [DOI] [PubMed] [Google Scholar]
- 28.Horn GP, Kesler RM, Motl RW, Hsiao-Wecksler ET, Klaren RE, Ensari I. Physiological responses to simulated firefighter exercise protocols in varying environments. Ergonomics 2015; 58:1012–1021. [DOI] [PubMed] [Google Scholar]
- 29.Soteriades E, Smith D, Tsismenakis AJ, et al. Cardiovascular disease in US firefighters: a systematic review. Cardiol Rev 2011; 19:202–215. [DOI] [PubMed] [Google Scholar]
- 30.González-Alonso J, Teller C, Andersen SL, Jensen FB, Hyldig T, Nielsen B. Influence of body temperature on the development of fatigue during prolonged exercise in the heat. J Appl Physiol 1999; 86:1032–1039. [DOI] [PubMed] [Google Scholar]
- 31.Smith D. Firefighter fitness: improving performance and preventing injuries and fatalities. Curr Sports Med Rep 2011; 10:167–172. [DOI] [PubMed] [Google Scholar]
- 32.Selkirk GA, McLellan TM. Influence of aerobic fitness and body fatness on tolerance to uncompensable heat stress. J Appl Physiol 2001; 91:2055–2063. [DOI] [PubMed] [Google Scholar]
- 33.Sell K, Hofman J. The importance of grip strength for firefighters. NSCA'S TSAC Report. [Google Scholar]
- 34.Peate W, Bates G, Lunda K, Francis S, Bellamy K. Core strength: a new model for injury prediction and prevention. J Occup Med Toxicol 2007; 2:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Eves ND, Jones RL, Petersen SR. The influence of the self-contained breathing apparatus (SCBA) on ventilatory function and maximal exercise. Can J Appl Physiol 2005; 30:507–519. [DOI] [PubMed] [Google Scholar]
- 36.Dreger RW, Jones RL, Petersen SR. Effects of the self-contained breathing apparatus and fire protective clothing on maximal oxygen uptake. Ergonomics 2006; 49:911–920. [DOI] [PubMed] [Google Scholar]
- 37.Bruce-Low SS, Cotterrell D, Jones GE. Effect of wearing personal protective clothing and self-contained breathing apparatus on heart rate, temperature and oxygen consumption during stepping exercise and live fire training exercises. Ergonomics 2007; 50:80–98. [DOI] [PubMed] [Google Scholar]
- 38.Kales SN, Soteriades ES, Christoudias SG, Christiani DC. Firefighters and on-duty deaths from coronary heart disease: a case control study. Environ Health 2003; 2:1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kales SN, Soteriades ES, Christophi CA, Christiani DC. Emergency duties and deaths from heart disease among firefighters in the United States. N Engl J Med 2007; 356:1207–1215. [DOI] [PubMed] [Google Scholar]
- 40.Geibe JR, Holder J, Peeples L, Kinney AM, Burress JW, Kales SN. Predictors of on-duty coronary events in male firefighters in the United States. Am J Cardiol 2008; 101:585–589. [DOI] [PubMed] [Google Scholar]
- 41.Welles AP, Xu X, Santee WR, et al. Estimation of core body temperature from skin temperature, heat flux, and heart rate using a Kalman filter. Comput Biol Med 2018; 99:1–6. [DOI] [PubMed] [Google Scholar]
- 42.Cuddy JS, Buller M, Hailes WS, Ruby BC. Skin temperature and heart rate can be used to estimate physiological strain during exercise in the heat in a cohort of fit and unfit males. Military Med 2013; 178:e841–e847. [DOI] [PubMed] [Google Scholar]
- 43.Buller MJ, Tharion WJ, Cheuvront SN, et al. Estimation of human core temperature from sequential heart rate observations. Physiol Measure 2013; 34:781–798. [DOI] [PubMed] [Google Scholar]
- 44.Clapp A, Bishop P, Muir I, Walker J. Rapid cooling techniques in joggers experiencing heat strain. J Sci Med Sport 2001; 4:160–167. [DOI] [PubMed] [Google Scholar]
- 45.Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician 2005; 71:2133–2140. [PubMed] [Google Scholar]
- 46.Karlsen A, Nybo L, Norgaard SJ, Jensen MV, Bonne T, Racinais S. Time course of natural heat acclimatization in well-trained cyclists during a 2-week training camp in the heat. Scand J Med Sci Sports 2015; 25:240–249. [DOI] [PubMed] [Google Scholar]
- 47.Konrad J. (2018) Effect of a simulated mine rescue on physiological variables and heat strain of mine rescue workers (Master's Dissertation). Available at: https://zone.biblio.laurentian.ca/handle/10219/3131 Accessed December 5, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.