

Abstract
Digital breast tomosynthesis (DBT) has been widely implemented in place of 2D mammography, although it is less effective in women with extremely dense breasts. Breast ultrasound detects additional early-stage, invasive breast cancers when combined with mammography; however, its relevant limitations, including the shortage of trained operators, operator dependence and small field of view, have limited its widespread implementation. Automated breast sonography (ABS) is a promising technique but the time to interpret and false positive rates need to be improved. Supplemental screening with contrast-enhanced magnetic resonance imaging (MRI) in high-risk women reduces late-stage disease; abbreviated MRI protocols may reduce cost and increase accessibility to women of average risk with dense breasts. Contrast-enhanced digital mammography (CEDM) and molecular breast imaging improve cancer detection but require further validation for screening and direct biopsy guidance should be implemented for any screening modality. This article reviews the status of screening women with dense breasts.
Keywords: Breast density, screening ultrasound, breast cancer, tomosynthesis, magnetic resonance imaging
Introduction
Mammography remains the primary screening method for breast cancer as it is proven to reduce breast cancer mortality by about 20% on long-term follow-up in randomized trials [1,2]. In observational studies, breast cancer mortality reduction is 25–31% for women invited for screening, versus 38–48% for women actually screened [3,4]. Mammography only reduced mortality in trials where detection of node-negative invasive cancers improved as a result of screening [5].
Not all women benefit equally from mammography. Women at high risk for breast cancer because of pathogenic mutations have a high rate of “interval cancers” detected because of lumps or other symptoms after a normal mammogram and before the next recommended screen [6–8]. Interval cancers typically have worse prognosis than screen-detected cancers. Interval cancer rates increase with increasing breast density [9] and are elevated in women with a personal history of breast cancer [10].
In women where mammography performs less well, there is interest in supplemental screening with MRI or ultrasound or other methods. Randomized trials of supplemental screening to examine mortality reduction would be prohibitively expensive and require long-term (> 10 year) follow-up, by which time the technologies will have changed so that results would be outdated. We should, instead, examine impact on intermediate endpoints, such as node-negative invasive cancer detection and interval cancer rates which are expected to translate to reduced mortality from breast cancer [11]. In a successful screening program, interval cancers should represent fewer than 10% of all cancers. The purpose of this review is to examine such intermediate endpoints for women with dense breasts undergoing supplemental screening.
Breast density, risk, and masking effect
Wolfe first related nodular dense patterns of breast tissue on mammography to risk of developing breast cancer [12], finding a 37-fold higher risk with the most nodular/dense pattern compared to the least nodular pattern. An analysis of the Dutch mammography screening program [13], which uses the Wolfe classification, showed a 41% mortality reduction in women with non-dense breasts (relative risk of death, RR, 0.59 [95% CI 0.44, 0.79]) compared to a 13% reduction in women with dense breasts (RR 0.87 [95% CI 0.52, 1.45]). Insofar as the confidence interval widely overlaps one in women with dense breasts, there may be no net benefit of mammography screening in women with dense breasts.
Gram et al. [14] described five density patterns of Tabár that are used in the Swedish screening program. Only the two nodular and very dense patterns have been associated with increased risk of developing breast cancer of 2.4-fold, though the uniformly concave pattern I can also mask breast cancer [15,16]. At 25 years of follow-up, women with dense breasts had a 1.9-fold higher mortality rate from breast cancer compared to women with fatty breasts, which was primarily attributed to higher incidence of disease [15].
The Breast Imaging Reporting and Data System (BI-RADS) [17], categories of breast density (developed through the American College of Radiology) are usually included in mammographic reports: A) almost entirely fatty; B) scattered areas of fibroglandular density; C) heterogeneously dense, which may obscure detection of small masses, and D) extremely dense, which lowers the sensitivity of mammography (Figure 1). The latter two categories are considered “dense”. In the latest edition of BI-RADS, greater emphasis is placed on the masking effect: in breasts where even a region of the breast is dense, small non-calcified masses can be hidden, and such breasts should be classified as heterogeneously dense [17].
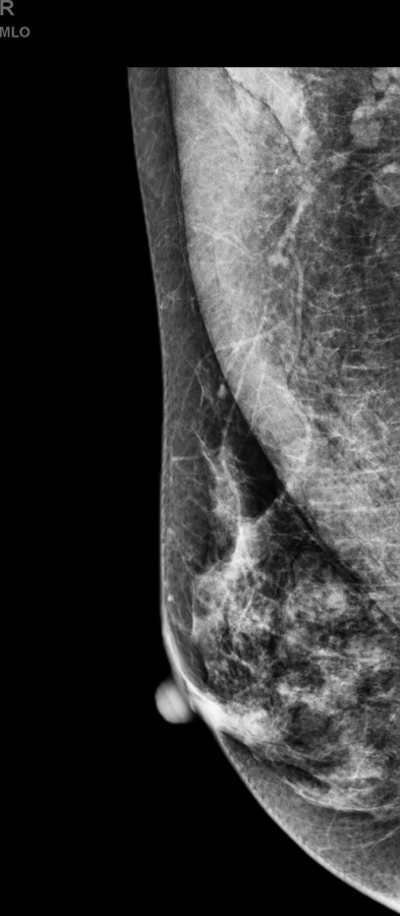
Fig. 1.
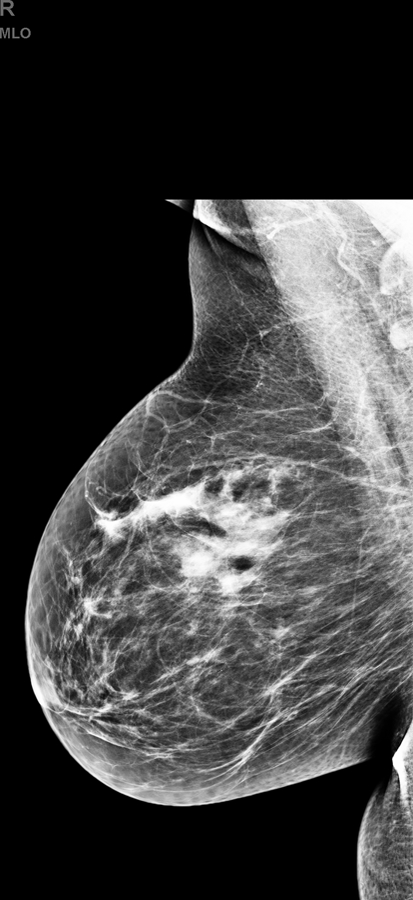
Examples of each category of breast composition with (a-b) fatty, (c-d) scattered fibroglandular, (e-f) heterogeneously dense, (g-h) extremely dense breasts; one case where the breast composition appears dense in just one quadrant (i-j) is also shown.
Approximately 43% of women aged 40–74 have dense breasts [18]. Around menopause, breast density tends to decrease in some women as the glandular tissue involutes (Figure 2). Automated software programs have been developed for quantitative, reliable, measurement of breast density [19–21]. Methods implemented for assessment of mammographic breast density include visual, semi- or fully automated approaches that include quantitative measurement of area-based or volumetric parameters. Visual, qualitative methods are based on human judgement and are therefore subjective; inter-observer variability can be significant among radiologists, whereas automated quantitative software provides results that are less subjective and more consistent [22].
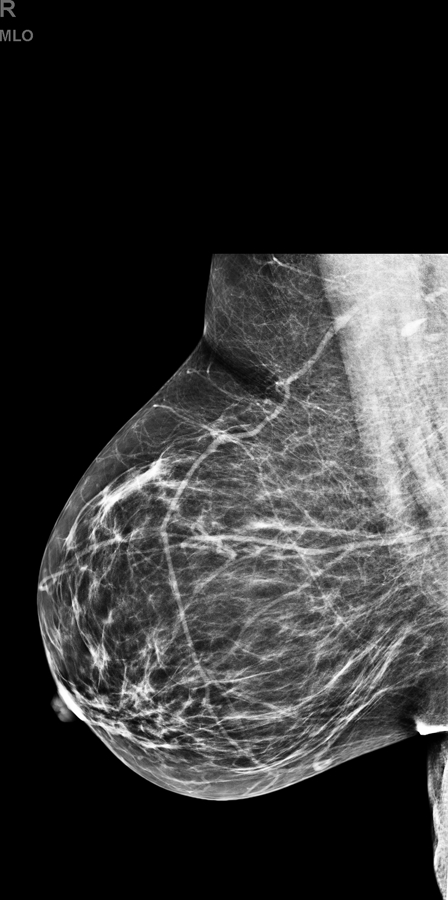
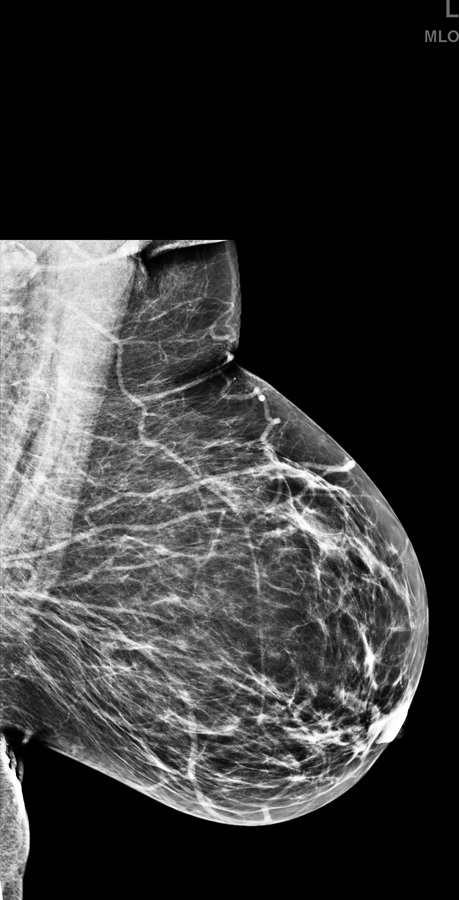
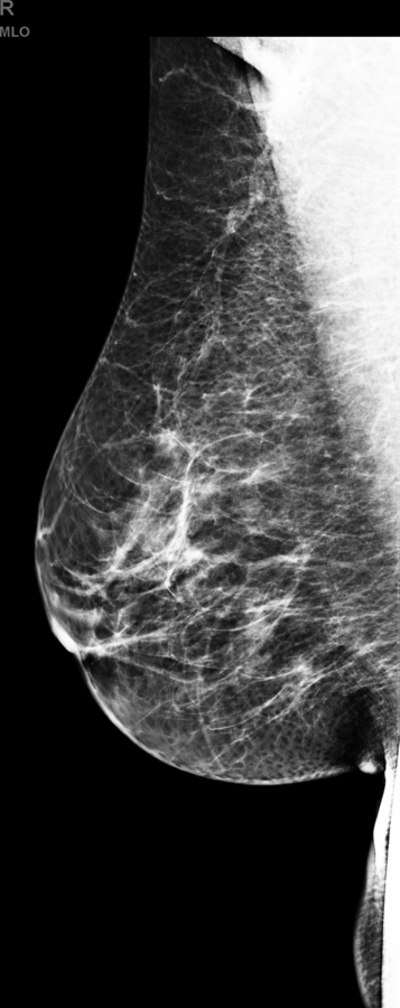
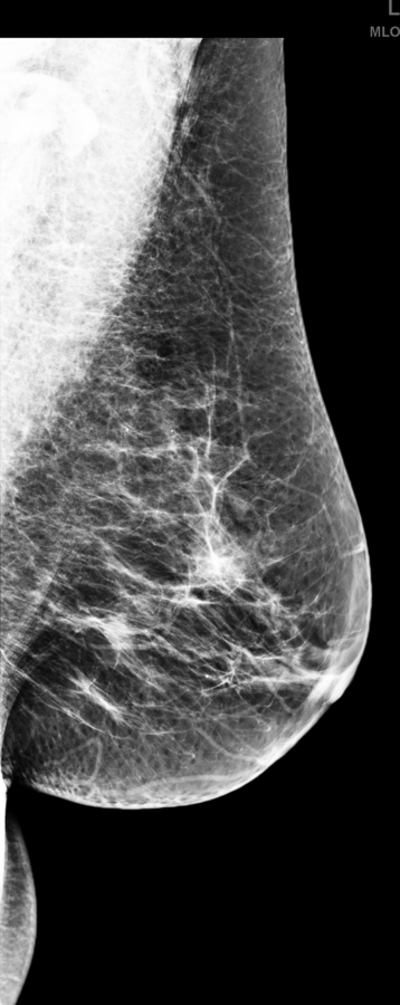
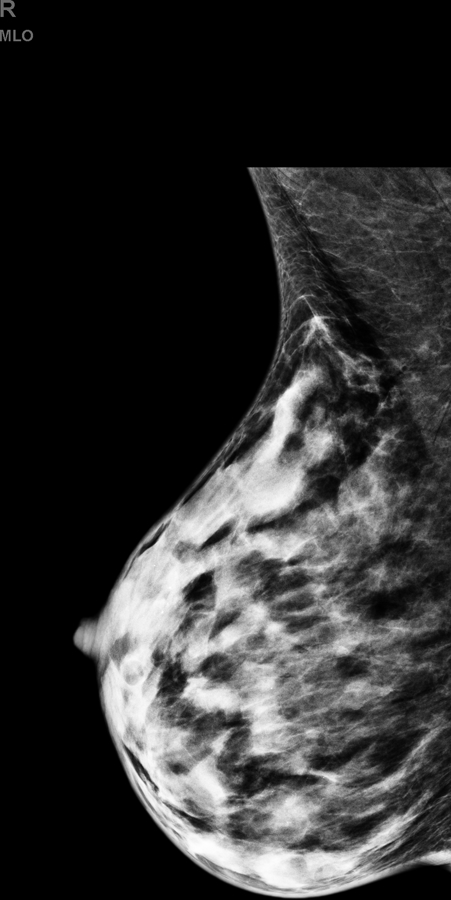
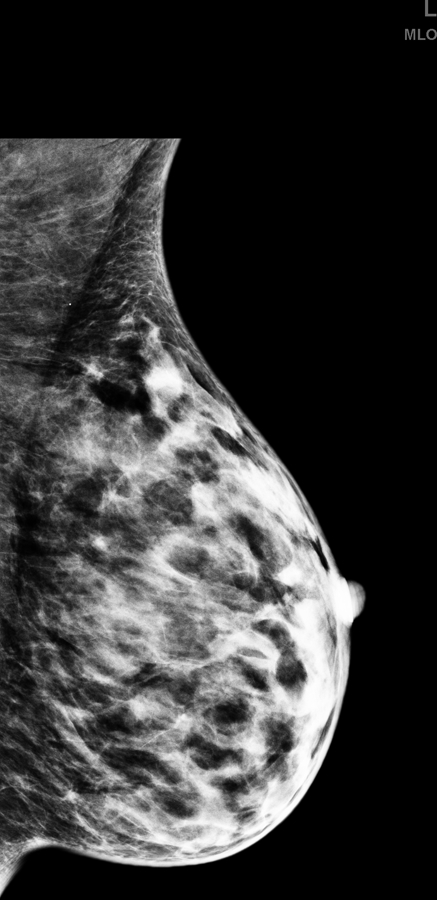
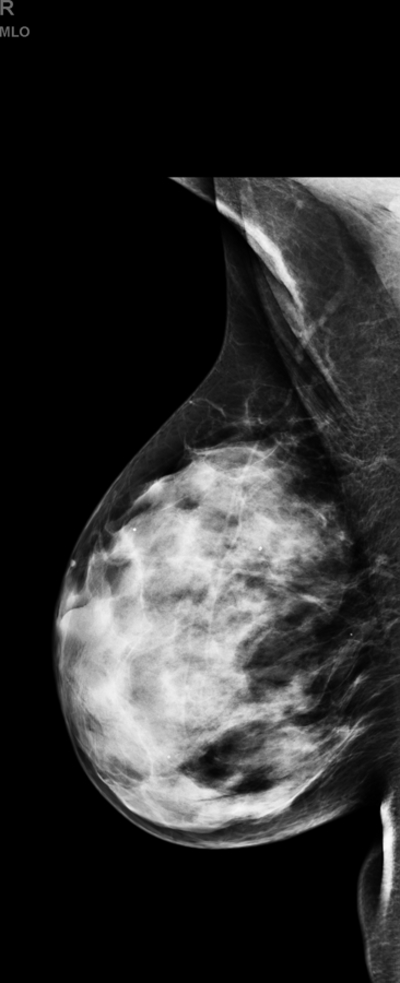
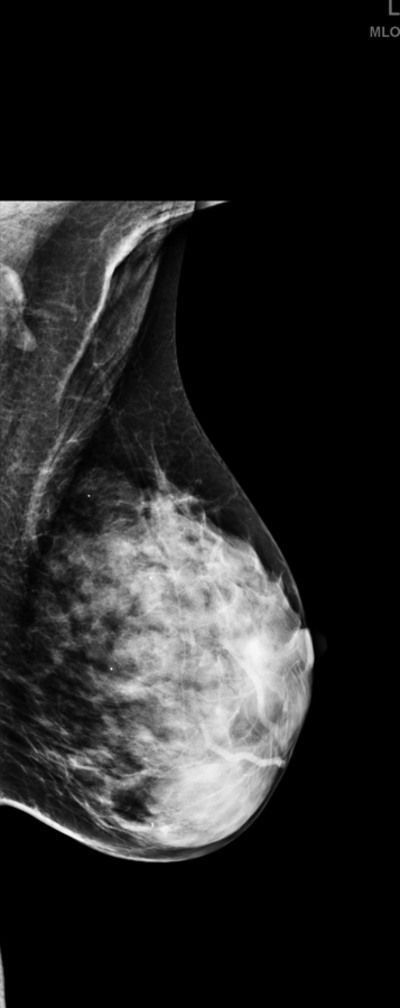
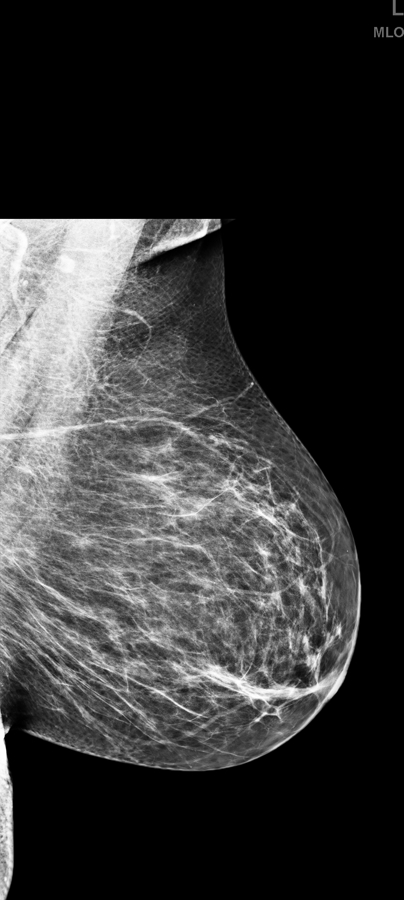
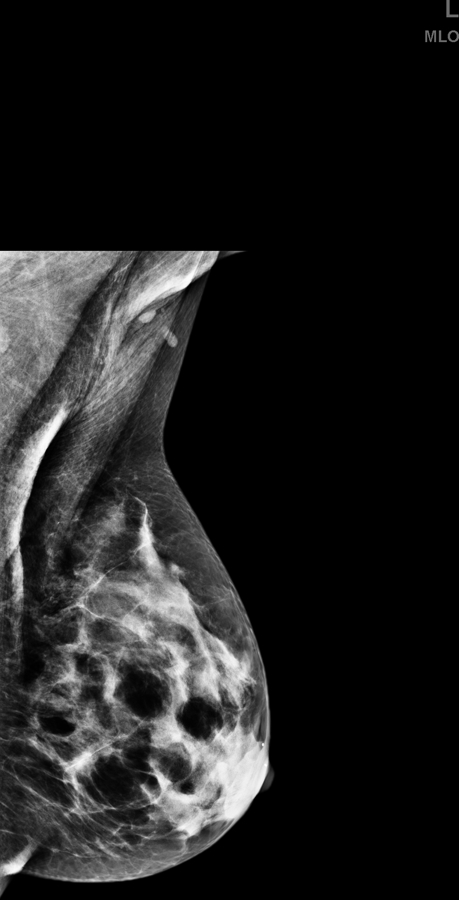
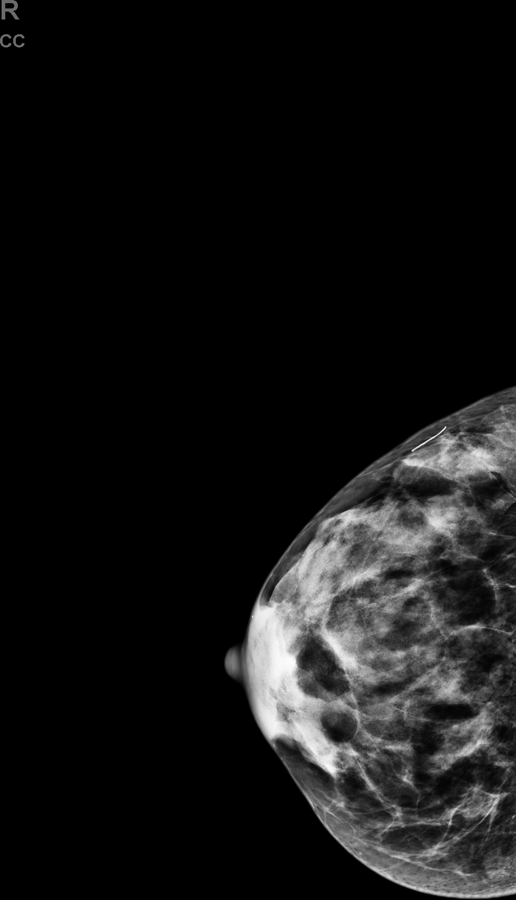
Fig. 2.
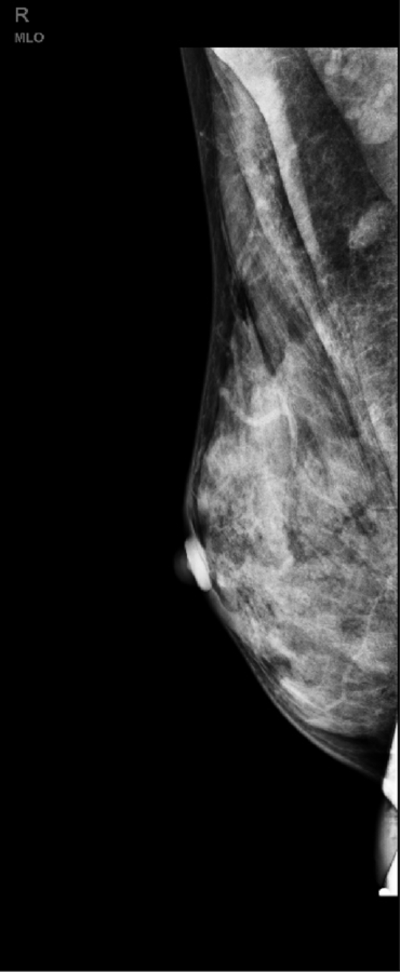
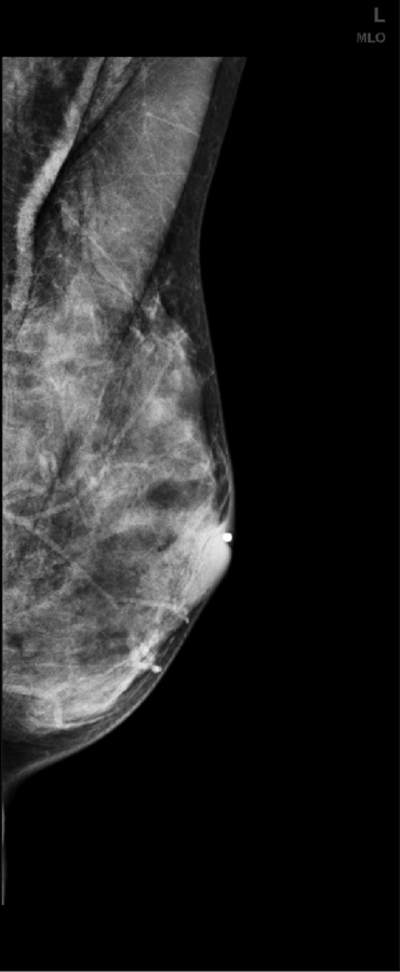
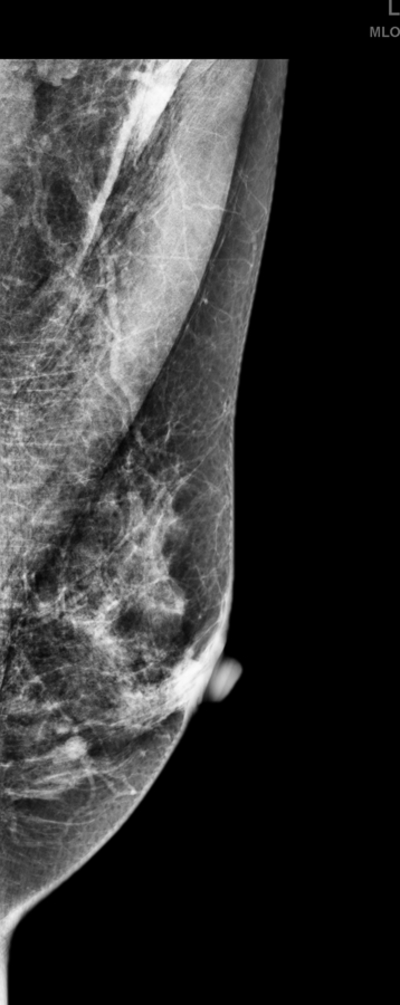
(a) Right and (b) left mediolateral oblique shows a normal screening mammography in a 47-old woman; menopause occurred at 48 years and four years later the, (c) right and (d) left mediolateral oblique screening mammography shows a decrease in breast density due to normal perimenopausal involutionary changes.
Mammographic density is one of the strongest risk factors for breast cancer: women with extremely dense breasts have four- to six-fold higher risk of developing breast cancer compared to those with fatty breasts [16]. It is estimated that density accounts for 39% of premenopausal and 26% of postmenopausal breast cancer [23]. Breast density is now incorporated in some risk models and should be considered in risk-based screening and targeted prevention [24,25].
Breast density decreases the sensitivity of mammography due to masking of non-calcified cancers, potentially delaying diagnosis with worse outcomes [26–28]. Studies have highlighted a decrease in the sensitivity of mammography from a level of 85.7%−88.8% in women with almost entirely fatty breasts to 62.2%−68.1% in women with extremely dense breasts [29,30]; mammographic sensitivity in dense breasts is under 50% when screening ultrasound has been performed and closer to 33% in studies where MRI has been included [31]. Cancers in women with dense breasts tend to be larger at detection [32]; this may be due to more rapidly growing tumors, delayed detection or both.
Full-field digital mammography has a slightly higher sensitivity compared to analog film-screen mammography in women with dense breasts [33]. Recently the European Society of Breast Imaging (EUSOBI) and 30 national breast radiology bodies recommended the adoption of digital mammography as a first priority to improve mammographic sensitivity in women with increased breast density [34].
Beyond 2D Mammography
Digital Breast Tomosynthesis (DBT)
Tomosynthesis, also known as 3D mammography, is a digital mammographic technique where low-dose images are acquired from multiple angles as the x-ray tube moves in an arc over the breast. Data from these projection images are typically reconstructed into 1-mm slices [35]. Automated breast density software has been developed for DBT with documented reliability of volumetric measurements [21,36].
Three prospective population-based trials, the STORM trial from Italy [37] and the Oslo tomosynthesis trials [38,39], showed that adding DBT to digital mammography resulted in an additional 2.7 and 2.3 cancers detected per 1000 screens, respectively. Friedewald et al [40], using historical multicenter data, showed that DBT improved cancer detection by 1.2 (95% CI, 0.8–1.6) per 1000 screens. DBT improved cancer detection and reduced recalls in the subgroups of women with scattered fibroglandular density and heterogeneously dense breasts; there was no significant drop in recalls from DBT in women with fatty breasts and no improvement in cancer detection in women with extremely dense breasts [41]. Meta-analysis showed absolute reduction in recall rate of 0.8 to 3.6% [42] from tomosynthesis and this benefit appears sustained [43] though further validation is needed.
Screening Ultrasound
Multiple studies have shown supplemental screening with ultrasound (US) after mammography in women with dense breasts increases breast cancer detection by 1.8 to 4.6 cancers per 1,000 women screened (Figure 3), depending on disease prevalence [44–49]. Across 23 series, encompassing 367,252 screens, 851 cancers have been reported seen only with screening US (2.3 per 1000) (Table 1) [26–28,44,46–48,50–60].
Fig. 3.


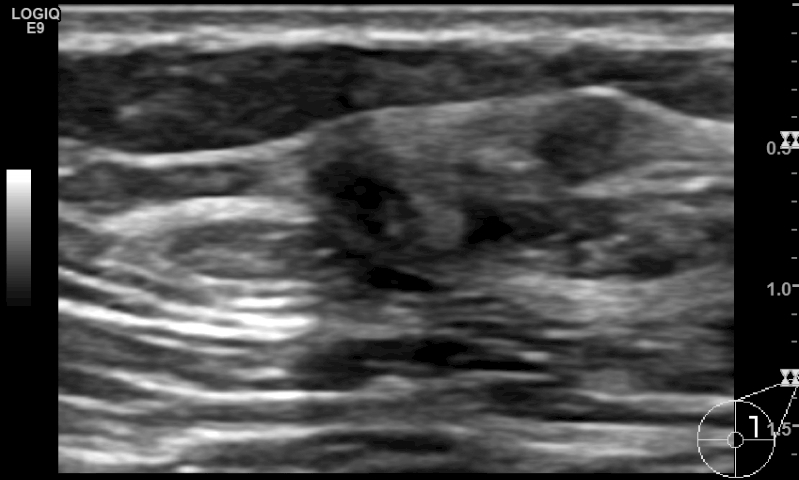
(a,b) Mediolateral oblique and (c,d) craniocaudal mammography in a 52-year-old woman shows dense breast composition type C. (e) Supplemental screening ultrasound shows an irregular hypoechoic 9 mm mass (yellow arrows) in the 2 o’ clock position of the left breast, adjacent to a cyst (green arrow). Biopsy of the irregular mass revealed an invasive, node-negative, intermediate grade, lobular carcinoma (ER positive, PR negative, HER2 negative, Ki-67<1%).
Table 1.
Results of studies examining screening ultrasound as an adjunct to mammography in women with dense breasts
| Author, Year | Number of women with Cancer a |
Number of Women Screened |
CDR per 1000 |
Net Added Recalls due to US (% of Screens) |
Biopsy Rate (%)b |
PPV3 of biopsies prompted only by US (%)c |
N Invasive, grade |
Mean size (mm, range) |
Node Negative (%) |
DCIS (% of cancers), grade |
BI-RADS 3 | Commentsd |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Single-center | ||||||||||||
| Gordon, 1995 | 30 | 12706 | 2.4 | NR | NR | 44/279 (16) | 44, no details about grade |
11 (4–25) | NR | 0 | NR | Diagnostic population |
| Buchberger, 2000 |
40e | 8970 | 4.5 | NR | NR | 40/405 (9.9) | 35, no details about grade |
9.1 (4–20) | 33/35 (94.3) | 5 (12.5), no details about grade |
NR | 8103 women in a screening population and 867 in a diagnostic population |
| Kaplan, 2001 | 5 | 1862 | 3.2 | 176 (9.5) | 97 (5.2) | 6/96 (6.3) | 5, no details about grade |
9 (6–14) | 5/5 (100) | 1 (16.7), no details about grade |
NR | Technologist performed |
| Kolb, 2002 | 34 | 5418 women, 13547 screens |
2.7 | 799 (5.9) | NR | 37/358 (10) | 36, no details about grade |
9.9 (range: NR) | 25/28 (89.3)f | 1 (2.7) , no details about grade |
NR | 1,354 exams in women with abnormal mammogram or CBE |
| Crystal, 2003 | 7 | 1517 | 4.6 | 90 (5.9) | 38 (2.5) | 7/38 (18) | 7; 1 low, 1 intermediate, 4 high-grade and 1 lobular |
9.6 (4–12) | 6/7 (85.7) | 0 | NR | |
| Leconte, 2003 | 16 | 4236 | 3.8 | NR | NR | NR | 14, no details about grade |
7 (4–17) | NR | 2 (12.5), no details about grade |
NR | Included 136 women with palpable mass |
| Brancato, 2007 | 2 | 5227 | 0.4 | NR | 65 (1.2) | 2/65 (3.1) | 2, no details about grade |
NR | 2/2 (100) | 0 | NR | Mammography-negative women |
| De Felice, 2007 | 12 | 1754 | 6.8 | NR | 46 (2.6) | NR | 10, no details about grade |
10 (5–15) | 10/10 (100) | 2 (16.7), no details about grade |
NR | |
| Youk, 2011 | 17 | 1418 | 12.0 | 200 | 80 (5.6) | 17/80 (21.3) | NRg | 13 (6–20) | NRg | NRg | NR | Mammography-negative women, retrospective database review, general screening and personal history of breast cancer subsets |
| Hooley, 2012 | 3 | 935 | 3.2 | 234 (25.0) | 53 (5.7) | 3/63 (4.8) | 2, no details about grade |
6.3 (5–9) | 2/2 (100) | 1 (33.3), no details about grade |
187 (20.0) | Technologist performed |
| Girardi, 2013 | 41 | 22,131 | 1.9 | NR | 422 (1.9) | 41/422 (9.7) | 37, no details about grade |
8 (5–12) | 36/37 (97.3) | 4 (9.8) , no details about grade |
NR | Mammography-negative women |
| Bae, 2014 | 329 | 106829 women, 116656 screens |
3.1 | NR | NR | NR | 282, no details about grade |
NRi | 253/282 (89.7) |
53 (15.8) no details about grade |
NR | Retrospective database review |
| Korpraphong, 2014 |
19 | 14483 screens |
1.4 | NR | NR | NR | NR | NR | NR | NR | NR | |
| Wilczek, 2016 | 4 | 1668 | 2.4 | 15 (0.9) | 12 (0.7) | NR | 4 (2 low-, 1 intermediate, 1 high-grade) |
21.8 (13–40) | 2/4 (50) | 0 | NR | ABUS, technologist performed |
| Destounis, 2017 |
18 | 4898 women, 5434 screens |
3.3 | NR | 100 (2.0) | 18/100 (18.0) | 18 (5 low-, 7 intermediate-, 4 high-grade and 2 not specified) |
1–5 mm: 1 case; 6– 10 mm: 7 cases; 11–15 mm: 4 cases; 16–20 mm: 1 case; >20 mm: 4 case; not specified: 1 case |
14/18 (78.0) | 0 | 101 (1.9)j | Retrospective review |
| Kim, 2017 | 8 | 778 | 10.3 | NR | NR | NR | 5 | 26.3 (1–70) | 4/5 (80) | 3 (37.5) | NR | |
| Multicenter | ||||||||||||
| Corsetti, 2008 | 37e | 9157 | 4 | NR | 449 (4.9) | 50/449 (11.1)k | 36, no details about grade |
NRl | 31/36 (86.1) | 1 (2.7), no details about grade |
NR | Self-referred women; 13/50 cancers excluded (palpable or symptoms) |
| Kelly, 2010 | 23e | 4419 women, 6425 screens |
3.6 | 557 (8.7) | 75 (1.2) | 23/75 (30.7) | 22 (7 low, 13 intermediate, 2 high) |
5 mm or less: 1 case; 6–10 mm: 13 cases; 11–20 mm: 6 cases; 21–50 mm: 1 case; >50 mm: 1 case |
NR | 1 (4.3), no details about grade |
NR | Automated arm, technologist acquired |
| Berg, 2012, prevalence |
14 | 2659 | 5.3 | 401 (15.1) | 207 (7.8) | 12/207 (5.8) | 30 (11 low, 7 intermediate, 6 high, 5 lobular and 1 mixed ductal- lobular) |
10 (median; range: 2–40) |
29/30 (96.7) | 2 (6.25) (1 intermediate- and 1 high- grade) |
NR | 1st screen; at least 1 other risk factor, 20% were high-risk women; ≥ BI-RADS 3 = positive. |
| Berg, 2012, incidence |
18 | 4841 screens |
3.7 | 356 (7.4) | 242 (5.0) | 18/242 (7.4) | Year 2, 3 screens; 612 women had MR screen after year 3 US screen |
|||||
| Weigert, 2017, prevalence |
11 | 2706 | 4.1 | 325 (12.0) | 151 (5.6) | 11/151 (7.3) | 9 (1 low, 6 intermediate, 2 high) |
25 (12–80) | 7/9 (77.8) | 2 (18.2), all intermediate grade |
NR | Technologist performed, BI-RADS 3 or higher considered recall as presented |
| Weigert, 2017, Incidencem |
30 | 10810 | 2.8 | 1073 (9.9) | 379 (3.5) | 30/379 (7.9) | 25 (3 low, 17 intermediate, 5 high grade) |
10.9 (4–30) | 20/25 (80.0) | 5 (16.7) (4 intermediate, 1 high grade) |
NR | Technologist performed, BI-RADS 3 or higher considered recall as presented |
| Brem, 2015 | 30 | 15318 | 2.0 | 2063 (13.5) | 551 (3.6) | 30/551 (5.4) | 28, no details about grade |
12.9 | 25/27 (92.6) | 2 (6.7), no details about grade |
19 (0.1) | ABUS, technologist performed |
| Ohuchi, 2016 | 67 | 36752 | 1.8 | 1932 (5.25) | NR | NR | 55, no details about grade |
14.2 | 47/55 (85.5) | 11 (16.7), no details about grade |
NR | Women aged 40–49 with any breast density |
| Buchberger, 2018 |
36 | 66680 | 0.5 | 397 (0.60) | 201 (0.30) |
36/201 (17.9) | 33, no details about grade |
14 (median; 3–32) | 25/33 (75.8) | 3 (8.3), no details about grade |
1255 (1.9) | Population-based observational study in Tyrol, Austria ages 40–69, all breast densities |
Number or women found to have cancer on screening ultrasound
Percent of women who underwent biopsy due to screening US
Percent of lesions biopsied due to screening US that were malignant
Studies utilized physician (radiologist) performed handheld screening ultrasound unless otherwise specified
These studies referred to numbers of cancers (and not to the number of women)
Kolb et al. provided this information for 28 of 36 invasive cancers
Youk et al, provided data about 8 of 10 cancers diagnosed in the general screening arm (7 of 8 were DCIS or stage 1; one of eight was node positive)
Bae et al did not report mean tumor size or range but 176/335 (53%) were minimal cancers and 52 (16%) were stage II
Destounis et al. provided this as a fraction of screens
13 of these women were found to have symptoms and were excluded from “US-screen-detected” cancers
Corsetti et al. did not provide the mean tumor size or range but 3/36 were stage T1a, 20/36 T1b, 10/36 T1c, 2/36 T2 and 1/36 stage T3
In year 4 of Weigert et al, of 3331 US, 53 recommended biopsies, 10 cancers, 358 BI-RADS 3. Higher PPV3 but v. high BI-RADS 3 rate.
ABUS: Automated Breast Ultrasound System; CDR: Cancer Detection Rate; NR: Not Reported; PPV: Positive Predictive Value; US: Ultrasonography
The proportion of invasive carcinomas detected on US that are node negative exceeded 80% in 15 of 19 studies and 90% in eight of 19 studies. Similar supplemental cancer detection was shown each year for three years in ACRIN 6666 [47]. Excellent outcomes from cancers detected at supplemental screening with US have been observed in a multicenter retrospective analysis with 7-year follow-up of 501 women reported by Kim et al [61] who found that women with US-detected cancer had 98% 5-year disease-free survival. The Japan Strategic Anti-cancer Randomized Trial (J-START) [58] showed significantly higher sensitivity in women assigned supplemental US (intervention) compared to the control group assigned only mammography. Screen-detected cancers were more frequently stage 0 and I with intervention (144 [71.3%] vs. 79 [52.0%], p=0.0194).
Interval cancer rates are reduced by addition of screening ultrasound to mammography, and in all studies were less than 10% of all cancers [58,62]. In the ACRIN 6666 study, the interval cancer rate was 9/111 (8%) across three years of study, suggesting that combined ultrasound and mammography was an effective strategy in women with a personal history of breast cancer or other intermediate risk factors and dense breasts [47].
Analysis of results from technologist-performed handheld screening US (HHUS) using standard documentation has shown a cancer detection rate of 2.5 per 1000 [63] that appears to be slightly lower than the 5.3 per 1000 rate observed across physician-performed screening US studies, though in part this reflects differences in disease prevalence [44,46,47]. HHUS is limited by a shortage of well-trained physicians and technologists, small field of view, and the requirement that a finding must be observed during scanning (operator dependence). Importantly, however, operator dependence for screening ultrasound is not worse than variation in mammographic interpretation [64]. Berg et al. found high reliability of 11 experienced breast imaging radiologists in detecting and characterizing lesions larger than 9 mm with US in patients [65] and for 64 specialist radiologists for lesions 5–9 mm in size in phantoms [66].
False positives increase when ultrasound is added to mammography. A 15.1% (95%CI: 13.5%−16.6%) absolute increase in callbacks was observed with the first, prevalent, screen in ACRIN 6666, which dropped to 7.4% (95%CI: 6.6%−8.2%) for incidence screens when prior US was available [47]. For technologist-performed US, Weigert et al. [59] observed a 12.0% absolute increase in recalls in the first round of screening which dropped to an average 9.9% in subsequent years.
In order to separate detection from image acquisition, and thereby potentially improve the availability of screening US, automated breast sonography (ABS) has been developed. Typically using a field of view of 15 cm and 3–5 acquisitions per breast, ABS can provide standardized exams and global visualization of the breast tissue. Such an exam produces several thousand images for review; the interpretation time in published series varies between 2.9 min and 9 min [54,57,67,68]. As with every imaging modality, there is a learning curve, depending on individual radiologic experience and protocols [54]. ABS can be used for the measurement of breast density [69,70], but incorporation of such techniques into clinical practice remains investigational.
ABS showed incremental cancer detection rate (ICDR) of 30 cancers among 15318 women screened (2.0 per 1000) in a prospective multicenter study [57]. Of the 30 cancers detected only with ABS, 28 (93.3%) were invasive with mean size 12.9 mm and 25/27 (92.6%) invasive cancers staged were node negative. The absolute increase in recall rate was 13.5% [57] (Table 1) and importantly, recalls from ABS are for immediate additional evaluation usually with HHUS. By comparison, a final assessment is typically rendered from HHUS (to include biopsy or short-interval follow-up), with only 50/16,676 (0.3%) of technologist-performed HHUS exams recalled for immediate additional evaluation (BI-RADS 0) across five series [63].
A study from Sweden, the European Asymptomatic Screening STUDY (EASY), showed an ICDR of 2.4 per 1000 women screened with ABS and almost stable recall rate of 2.3% [54]. In a reader study, ABS significantly increased detection of breast cancer with insignificant increase in false-positive rate [71]. A few studies comparing ABS and HHUS have shown similar lesion visualization and assessments [72,73]. Barriers to ABS implementation include the several thousand images to be reviewed with average 6-minute interpretation time [54] and learning curve in dismissing artifactual posterior shadowing at the interface of fat lobules [54,57,68].
Two studies have compared the performance of supplemental DBT and ultrasound in cancer detection in women with dense breasts and normal 2D mammography (Table 2). Interim analysis of first-year results among 3231 women in the ASTOUND trial [74] reported 24 additional cancers detected (23 invasive): DBT showed 13 (ICDR, 4.0 per 1,000 screens; 95% CI, 1.8 to 6.2) and physician-performed HHUS significantly more at 23 (ICDR, 7.1 per 1,000 screens; 95% CI, 4.2 to 10.0), while incremental false positive recall and added biopsy rates were similarly low [74]. Destounis et al. [75,76] retrospectively analyzed results from 7146 women with dense breasts screened with DBT followed by technologist-performed HHUS. That study reported on 39 cancers (30 invasive); four of them were recognized only by DBT vs. 17 (invasive) cancers solely by HHUS, with the few DBT-only detected cancers seen as calcifications [75]. Further study is ongoing.
Table 2.
Results of studies comparing performance of tomosynthesis (DBT) and ultrasound in women with mammography negative dense breasts.
| Author, Year |
Total Number of Cancers |
Number of Women Screened |
Number of cancers detected only by DBT |
Number of cancers detected only by US |
CDR of DBT |
CDR of US |
Recall rate of DBT |
Recall rate of US |
PPV3 of DBT |
PPV3 of US |
Comments |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tagliafico, 2016 |
24 | 3231 | 1 | 11 | 4.0 | 7.1 | 53 (1.7) | 65 (2.0) | 13/35 (37.1) |
23/47 (48.0) |
Mammography-negative women; interim analysis of 1st year results |
| Destounis, 2017 |
39 | 7146 | 4 | 17 | 3.0 | 4.9 | NR | NR | NR | NR | Retrospective review |
CDR: Cancer Detection Rate per 1,000 screens; DBT: Digital Breast Tomosynthesis; NR: Not Reported: US: Ultrasonography
Magnetic Resonance Imaging (MRI)
According to American College of Radiology guidelines, supplemental MRI is recommended annually beginning at age 25 to 30 years in women at high risk for breast cancer [77]. The National Comprehensive Cancer Network (NCCN) guidelines recommend MRI instead of mammography from ages 25–29 in high-risk women and thereafter as a supplement to mammography [78]. Importantly the Gail and BCSC models should not be used for estimating risk pertinent to deciding on MRI screening, though the Claus model can be used [77]. NCCN recommends MRI also be considered for supplemental screening in women with prior atypical biopsy or lobular carcinoma in situ due to lifetime risk of 20% or more [79], and the American College of Radiology recently recommended supplemental MRI screening for all women with a personal history of breast cancer diagnosed by age 50 and for those diagnosed later with dense breasts [80]. The relative amount of fibroglandular tissue should be included in the MRI report, together with background parenchymal enhancement (BPE); BPE may correlate even more strongly with risk of developing breast cancer [81]. Breast density can be quantified on MRI but this is not routine [82].
The sensitivity of MRI in high-risk women varies across studies from 71 to 100% but importantly is not influenced by breast density. A meta-analysis of 11 studies showed a sensitivity of 77% for the performance of MRI alone and 94% when MRI was combined with mammography [83]. However, according to recent studies, simultaneous screening mammography has little added value in the detection of breast cancer in women who undergo screening with MRI [84–86], particularly in women with pathogenic BRCA1 mutations [87]. Prospective cohort studies have shown a cancer detection rate for MRI alone of 8.2 to 15.9 per 1000 [83,88–90].
In women with familial high-risk, the sensitivity of MRI is not affected by breast density; therefore, the National Institute for Health and Care Excellence [91] and the GC-HBOC [92] recommend annual MRI alone, for the evaluation of women with familial high risk between the ages of 30 to 39, without a personal history of the disease. Annual MRI surveillance increases the detection of small invasive cancers in pathogenic BRCA1/BRCA2 carriers. Although there are important differences in the natural history of breast cancers in BRCA1 compared with BRCA2 mutation carriers, an analysis by Heijnsdijk et al. [87] showed that implementation of MRI improved metastasis-free survival in both carrier subgroups after an average of three rounds of screening per woman; eight interval cancers occurred in 801 BRCA1 mutation carriers (representing 10.9% of all cancers in that subgroup, 3.6 per 1000 screens) compared to two among 474 BRCA2 mutation carriers (representing 3.9% of all cancers in that subgroup, 1.7 per 1000 screens). The faster growth rate of triple-negative and basal phenotype tumors common in women with pathogenic BRCA1 mutations should be kept in mind [93,94]. To address this, some high-risk screening programs recommend 6-month surveillance with clinical examination and/or breast ultrasound in addition to annual screening with MRI [95]. Modeling studies suggest alternating mammography and MRI yields slightly better outcomes than concurrent screening, with earlier detection of node-negative invasive cancers in high-risk women [96,97].
False positive rates represent a point of discussion regarding MRI screening; specificity of MRI varies across studies [90,98,99], with recall rates centered at approximately about 10% [100–102]. Positive predictive value of biopsies performed (PPV3) after MRI ranges between 22.0% and 63.2% (Table 3).
Table 3.
Performance of Abbreviated Screening Breast MRI
| Author, Year | N Cancersa |
N Women Screened |
CDR per 1000 screens |
Population | Biopsy Rateb (BR4 or 5, %) |
PPV3 of bx (%)c |
BR 3 | Overall Recall Rate (%) |
Magnet (T) | C+ sequences | T2/STIR | # Invasive Cancers |
Mean size (mm, range) |
Node Negative (%) |
# DCIS, grade |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kuhl, 2014 | 11 | 443 women 606 screens |
18.2 | 105 women only dense 220 PHBC 118 family hx |
45 (10.2) | 11/45 (24.4) | 53 (8.7) | 98/606 (16.2) | 1.5 | 1 axial T1 no FS |
ND | 7 | 8.4 (4–17) | 7/7 (100) | 4, all gr 2–3 |
| Jain, 2016 | 9 | 591 | 15.2 | High-risk | 39 (6.6) | 10/40 (25.0) | NS | 39/591 (6.6) | 1.5 or 3 | 1 axial T1FS | ND | 7 | NS | NS | 2d 1 gr2, 1 NS |
| Chen, 2017e | 13e | 356 | 36.5 | Dense; 6 PHBC; 29 family hx |
59 (16.6) | 13/59 (22.0)f | NSf | 59/356 (16.6) | 3 | 1 axial T1FS | NDf | 9 | All ≤ 1 cm | 9/9 (100) | 4, 1 gr2, 3 gr3 |
| Strahle, 2017 | 6g | 671 | 8.9 all 16.3 dense |
367 dense; 141 had family hx; no PHBC or known BRCA mutation |
16 (2.4) 16 (4.4) dense |
7/17 (41.2) | 0 | 16/671 (2.4) all 16/367(4.4) dense |
1.5 | 2 axial T1FS (@1.5 and 6 min) |
T2FS | 4 | 19 (7–40) | 4/4 (100) | 2g |
| Panigrahi, 2017h |
14 | 746 women 1052 screens |
13.3 | High risk | 47 (6.3) | 14/46 (30.4) | 35 (3.3) | 82/1052 (7.8) | 1.5 or 3 | 1 axial T1FS | ND | 12 | 10.7 (4–17) | NS | 2, gr 1 |
| Choi, 2018 | 12i | 725 women 799 screens |
15.0 | PHBC | 14 (1.9) | 12/19i (63.2) | 83 (10.4)i | 97/799 (12.1) | 1.5 or 3 | 1 sagittal T1FS | T2FS | 7i | 15 (5–20) | 6/7 (85.7) | 5i |
For all examinations, a scout localizer and pre-contrast T1W images were obtained; subtraction of the pre-contrast MRI from the first post-contrast MRI was performed and maximum intensity projection images were created from the subtraction images.
Abbreviations used: C+ = contrast-enhanced; ND=not done; PHBC = personal history of breast cancer; NS = not stated; BR = BI-RADS assessment; IDC = invasive ductal carcinoma; DCIS = ductal carcinoma in situ; gr = nuclear grade
Number of women found to have cancer
Biopsy rate, number of women biopsied as % of women screened
Number of biopsies malignant/total number of biopsies performed
An additional high nuclear grade DCIS was diagnosed in a patient who also had IDC on MRI
A separate publication by these authors in Academic Radiology 2017 details 16 cancers in 478 women and 41 biopsied lesions; these are likely overlapping series but extent of overlap, particularly among lesions biopsied, is unclear
An additional IDC was considered probably benign on the abbreviated protocol and suspicious when diffusion weighted imaging (DWI) was added to the abbreviated protocol; only 31 biopsies would have been performed after DWI, of which 14 were malignant
Seven malignancies were identified in six women: Two lesions of DCIS were identified in one patient (overall 3 DCIS lesions)
This series appears to entirely include what appears to be a subset published in 2016 by Harvey SC et al JACR
This institution lacked MRI-biopsy capability. 83 exams were assessed as BR3 on MRI, with 5 upgraded to BR4 at follow-up, 4 of which proved malignant, including 2 DCIS, 1 IDC, and 1 mucinous carcinoma: 4/83 (4.8%) BR3 exams proved malignant.
Importantly, MRI has been shown to downstage the disease [90]. Warner et al reported reduced advanced stage (stage II to IV) disease (1.9% vs. 6.6% among matched controls not able to have MRI) and increased node negative invasive cancers in the MRI group (85% vs. 54% in the control group) [103].
Excluding those who have bilateral mastectomy, women with personal history of breast cancer (PHBC) have a higher risk of the disease compared to pathogenic mutation-free women with family history [104], with lifetime risk of a second cancer exceeding 20% for those diagnosed by age 50 or those diagnosed later with dense breasts [80]. Mammographic sensitivity is reduced and interval cancer rate is at least doubled in women with PHBC [10]. When PHBC is present, MRI has considerably increased sensitivity compared to mammography; cancer detection rate for MRI is 10–29 cancers per 1000 screens in such women [80,104–108]. It has been shown that the addition of MRI in the surveillance of women with PHBC before the age of 50 improves the detection of aggressive cancers and reduces the interval cancer rate [109].
One prospective observational study was conducted by Kuhl et al. [99] to investigate the utility and accuracy of MRI as a supplemental screening tool in women at average risk for breast cancer. This study showed an overall supplemental cancer detection rate of 15.5 per 1000 screens (supplemental cancer detection rate 22.6 per 1000 cases at initial screening and 6.9 per 1000 cases at subsequent screening rounds) across all density categories; 85% of women with incident cancers had been screened with ultrasound also within the study. MRI-depicted cancers were small (median: 8 mm), node negative (93.4%), and 43% were high-grade; DCIS represented 33% of all cancers [99]. Those authors concluded that MRI screening improves early diagnosis of prognostically relevant breast cancer.
Berg et al. [110] reported 512/1215 (42.1%) women at elevated risk declined a no-cost MRI in the final year of ACRIN 6666. Recent reports of gadolinium accumulation in parts of the brain and elsewhere have raised concerns and prompted a black box warning [111], though there is no known adverse effect from this. To improve access, tolerance, and reduce cost, Kuhl and colleagues [112] introduced the ultrafast, 3-min, breast MRI for screening and demonstrated that abbreviated breast MRI maintained comparable sensitivity and specificity to the full diagnostic protocol. Table 3 summarizes results of abbreviated MRI to date [112–117]. Incremental cancer detection rate following abbreviated screening breast MRI ranges between 8.9 and 36.5 cancers per 1000 screens.
Future perspectives
There has been exploratory effort to evaluate contrast-enhanced spectral mammography (CESM) in the screening of women with dense breasts. In preliminary studies, CESM shows cancer detection comparable to MRI, with improved specificity [118], though few data from screening are yet published. Jochelson et al. [119] reported results from 307 women at increased risk who had screening CESM and MRI; 2 invasive cancers were seen on both modalities and one DCIS was seen only on MRI. PPV3 was 2/13 (15% for CESM) and 3/21 (14%) for MRI. There were more BI-RADS 3 assessments on MRI, with reduced specificity of MRI, but biopsy capability has only recently become available for CESM [119]. Unenhanced MRI technique with diffuse weighted imaging (DWI) is another promising modality for the detection of challenging, mammographically occult, breast cancers in women with dense breasts; the advantage of DWI is the ability to distinguish between normal microscopic tissue and malignancy without the use of intravenous gadolinium [120], though generalizability of DWI remains problematic [121].
Molecular breast imaging (MBI) is functional rather than anatomic imaging; standard views are obtained similar to mammography, i.e. craniocaudal and mediolateral oblique projections, for 10 minutes each, while mild compression is applied after intravenous injection of 99mTc-sestamibi [122]. Recent studies evaluating MBI as a supplemental screening technique for women with dense breasts have shown an ICDR ranging between 7.5 and 8.8 per 1000; the median size of cancer detected only by MBI is approximately 1.0 cm. The additional recall rate is 5.9% to 8.4%, while PPV3 varies between 19% and 33% [123–125].
Breast Density Inform and Current Practice
The potential impact of supplemental screening is gaining global attention from patients and policymakers. In the United States, 35 states have enacted legislation requiring some notification about breast density following a mammogram [11]; supplemental screening can be performed if ordered by a referring physician. In the UK and Australia, advocacy groups are making great efforts encouraging the density discussion; the website DenseBreast-info.org was developed for that purpose in the USA and will soon add content specific to healthcare providers in Europe. In France and Germany, for women with extremely dense breasts, a supplemental physician-performed ultrasound has been provided for many years and women are informed of this option in Greece. In Austria, since 2013, the Austrian Breast Cancer Early Detection Program provides supplemental ultrasound in women reported to have dense breasts on mammography. Currently, no clear guidelines have been established for widespread supplemental screening; a proposal for risk-adapted screening is illustrated in Fig 4.
Fig. 4.
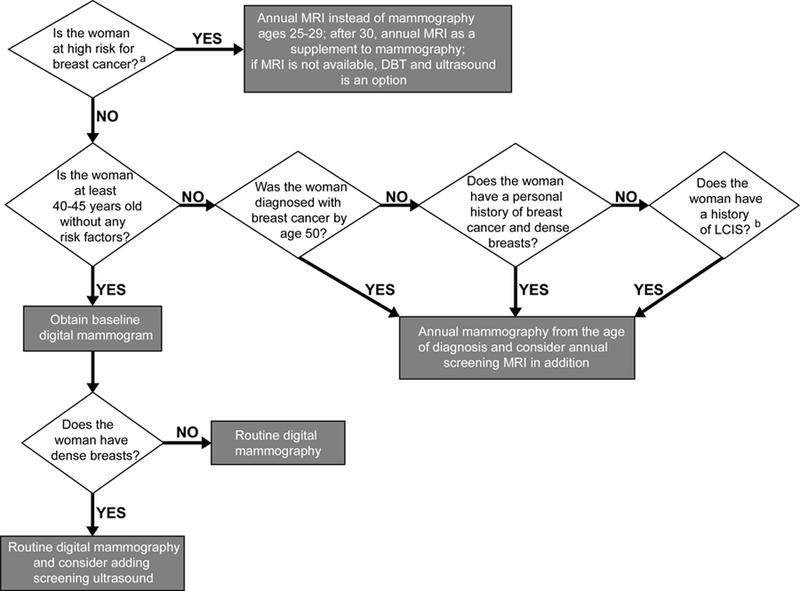
Flow chart illustrating a screening decision support tool according to risk stratification. a High risk is defined as: women with a known or suspected pathogenic mutation in BRCA, TP53, CHEK2, PTEN, ATM, CDH1, STK11, and PALB2; women having a lifetime risk greater than 20% according to acceptable models that determine risk of pathogenic mutations, with Tyrer-Cuzick model the most accurate at the population level (and which includes breast density as a risk factor); women treated with chest or mantle radiation therapy by age 30 and at least 8 years prior. b A personal history of lobular carcinoma in situ confers almost as high a risk as personal history of breast cancer and such women should consider supplemental screening with MRI, especially if the breasts are dense. Atypical lobular hyperplasia (ALH) and atypical ductal hyperplasia (ADH) confer 20–25% lifetime risk as well but there are no studies showing improved cancer detection in women with ALH or ADH who undergo MRI screening in addition to mammography.
Conclusions
The sensitivity of mammography is lower in women with dense breasts. Digital mammography has improved sensitivity compared to film-screen mammography and should be widely adopted in women with dense breasts. Breast density has been established as an independent risk factor for breast cancer and cancers tend to be more advanced at diagnosis compared to women with fatty breasts. US detects significantly more early-stage, invasive breast cancers than screening with mammography alone, leading to acceptably low interval cancer rates; however, a shortage of trained operators has precluded its widespread implementation. ABS is a promising technique but remains limited by the time to interpret and false positives. Tomosynthesis has been widely implemented in place of 2D mammography and has been shown to reduce significantly the recall rate and to increase the cancer detection rate, although it is less effective in women with extremely dense breasts and cancers may remain obscured in women with heterogeneously dense breasts. Supplemental screening with MRI in high-risk women has been shown to reduce late-stage disease and improve metastasis-free survival; the high cost has restricted MRI use to date. Widespread assessment of risk to include breast density and ascertain those women who should start early annual screening to include MRI is needed. Abbreviated MRI protocols may reduce cost and increase accessibility to women of average risk with dense breasts. Other methods such as CESM and MBI improve cancer detection but require further validation for screening.
Key points.
The sensitivity of mammography is reduced in women with dense breasts. Supplemental screening with US detects early-stage, invasive breast cancers.
Tomosynthesis reduces recall rate and increases cancer detection rate but is less effective in women with extremely dense breasts.
Screening MRI improves early diagnosis of breast cancer more than ultrasound and is currently recommended for women at high-risk. Risk assessment is needed, to include breast density, to ascertain who should start early annual MRI screening.
Acknowledgments
Funding: WAB receives support from National Institutes of Health grant 1R01A187593.
Abbreviations
- ABS
Three-Dimensional Automated Breast Sonography
- ACRIN
American College of Radiology Imaging Network
- ASTOUND trial
Adjunct Screening with Tomosynthesis or Ultrasound
- BI-RADS
Breast Imaging Reporting and Data System
- BCSC
Breast Cancer Surveillance Consortium
- CESM
Contrast-Enhanced Spectral Mammography
- DBT
Digital Breast Tomosynthesis
- DCIS
Ductal Carcinoma In Situ
- EASY
European Asymptomatic Screening Study
- ER
Estrogen Receptor
- EUSOBI
European Society Of Breast Imaging
- HHUS
Hand-Held Ultrasound
- GC-HBOC
German Consortium for Hereditary Breast and Ovarian Cancer
- ICDR
Incremental Cancer Detection Rate
- MBI
Molecular Breast Imaging
- MRI
Magnetic Resonance Imaging
- NCCN
National Comprehensive Cancer Network
- PHBC
Personal History of Breast Cancer
- PPV
Positive Predictive Value
- STORM trial
Screening with Tomosynthesis or Standard Mammography
- TDLUs
Terminal Ductal Lobular Units
- TOMMY trial
A comparison of TOMosynthesis with digital MammographY
- US
Ultrasound
Footnotes
Guarantor of the study: Wendie A. Berg, MD, PhD, Department of Radiology, University of Pittsburgh School of Medicine, Magee-Womens Hospital of UPMC, Pittsburgh, PA, USA
Conflict of interest: The authors declare no conflict of interest.
References
- [1].Oeffinger KC, Fontham ET, Etzioni R et al. (2015) Breast Cancer Screening for Women at Average Risk: 2015 Guideline Update From the American Cancer Society. JAMA 314:1599–1614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Tabar L, Vitak B, Chen TH et al. (2011) Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades. Radiology 260:658–663. [DOI] [PubMed] [Google Scholar]
- [3].Coldman A, Phillips N, Wilson C et al. (2014) Pan-Canadian study of mammography screening and mortality from breast cancer. J Natl Cancer Inst 106. [DOI] [PubMed] [Google Scholar]
- [4].Broeders M, Moss S, Nystrom L et al. (2012) The impact of mammographic screening on breast cancer mortality in Europe: a review of observational studies. J Med Screen 19 Suppl 1:14–25. [DOI] [PubMed] [Google Scholar]
- [5].Tabar L, Yen AM, Wu WY et al. (2015) Insights from the breast cancer screening trials: how screening affects the natural history of breast cancer and implications for evaluating service screening programs. Breast J 21:13–20. [DOI] [PubMed] [Google Scholar]
- [6].Brekelmans CT, Seynaeve C, Bartels CC et al. (2001) Effectiveness of breast cancer surveillance in BRCA1/2 gene mutation carriers and women with high familial risk. J Clin Oncol 19:924–930. [DOI] [PubMed] [Google Scholar]
- [7].Tilanus-Linthorst M, Verhoog L, Obdeijn IM et al. (2002) A BRCA1/2 mutation, high breast density and prominent pushing margins of a tumor independently contribute to a frequent false-negative mammography. Int J Cancer 102:91–95. [DOI] [PubMed] [Google Scholar]
- [8].Komenaka IK, Ditkoff BA, Joseph KA et al. (2004) The development of interval breast malignancies in patients with BRCA mutations. Cancer 100:2079–2083. [DOI] [PubMed] [Google Scholar]
- [9].Boyd NF, Guo H, Martin LJ et al. (2007) Mammographic density and the risk and detection of breast cancer. N Engl J Med 356:227–236. [DOI] [PubMed] [Google Scholar]
- [10].Houssami N, Abraham LA, Miglioretti DL et al. (2011) Accuracy and outcomes of screening mammography in women with a personal history of early-stage breast cancer. JAMA 305:790–799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Berg WA. (2016) Current Status of Supplemental Screening in Dense Breasts. J Clin Oncol pii: JCO658674. [DOI] [PMC free article] [PubMed]
- [12].Wolfe JN. (1976) Breast patterns as an index of risk for developing breast cancer. AJR Am J Roentgenol 126:1130–1137. [DOI] [PubMed] [Google Scholar]
- [13].van der Waal D, Ripping TM, Verbeek AL, Broeders MJ. (2017) Breast cancer screening effect across breast density strata: A case-control study. Int J Cancer 140:41–49. [DOI] [PubMed] [Google Scholar]
- [14].Gram IT, Funkhouser E, Tabar L. (1997) The Tabar classification of mammographic parenchymal patterns. Eur J Radiol 24:131–136. [DOI] [PubMed] [Google Scholar]
- [15].Chiu SY, Duffy S, Yen AM, Tabar L, Smith RA, Chen HH. (2010) Effect of baseline breast density on breast cancer incidence, stage, mortality, and screening parameters: 25-year follow-up of a Swedish mammographic screening. Cancer Epidemiol Biomarkers Prev 19:1219–1228. [DOI] [PubMed] [Google Scholar]
- [16].McCormack VA, dos Santos Silva I. (2006) Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev 15:1159–1169. [DOI] [PubMed] [Google Scholar]
- [17].Sickles EA, D’Orsi CJ, Bassett LW et al. ACR BI-RADS Mammography. In: D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA, eds. ACR BI-RADS Atlas, Breast Imaging Reporting and Data System. Reston, VA: American College of Radiology; 2013. [Google Scholar]
- [18].Sprague BL, Gangnon RE, Burt V et al. (2014) Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst 106:pii: dju255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Gubern-Merida A, Kallenberg M, Platel B, Mann RM, Marti R, Karssemeijer N. (2014) Volumetric breast density estimation from full-field digital mammograms: a validation study. PLoS One 9:e85952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Alonzo-Proulx O, Mawdsley GE, Patrie JT, Yaffe MJ, Harvey JA. (2015) Reliability of automated breast density measurements. Radiology 275:366–376. [DOI] [PubMed] [Google Scholar]
- [21].Ekpo EU, McEntee MF. (2014) Measurement of breast density with digital breast tomosynthesis--a systematic review. Br J Radiol 87:20140460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Destounis S, Arieno A, Morgan R, Roberts C, Chan A. (2017) Qualitative Versus Quantitative Mammographic Breast Density Assessment: Applications for the US and Abroad. Diagnostics (Basel) 7:pii: E30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Engmann NJ, Golmakani MK, Miglioretti DL, Sprague BL, Kerlikowske K, Breast Cancer Surveillance C. (2017) Population-Attributable Risk Proportion of Clinical Risk Factors for Breast Cancer. JAMA Oncol 3:1228–1236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Warwick J, Birke H, Stone J et al. (2014) Mammographic breast density refines Tyrer-Cuzick estimates of breast cancer risk in high-risk women: findings from the placebo arm of the International Breast Cancer Intervention Study I. Breast Cancer Res 16:451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Kerlikowske K, Ma L, Scott CG et al. (2017) Combining quantitative and qualitative breast density measures to assess breast cancer risk. Breast Cancer Res 19:97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Bae MS, Moon WK, Chang JM et al. (2014) Breast cancer detected with screening US: reasons for nondetection at mammography. Radiology 270:369–377. [DOI] [PubMed] [Google Scholar]
- [27].Hooley RJ, Greenberg KL, Stackhouse RM, Geisel JL, Butler RS, Philpotts LE. (2012) Screening US in patients with mammographically dense breasts: initial experience with Connecticut Public Act 09–41. Radiology 265:59–69. [DOI] [PubMed] [Google Scholar]
- [28].Kolb TM, Lichy J, Newhouse JH. (2002) Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology 225:165–175. [DOI] [PubMed] [Google Scholar]
- [29].Carney PA, Miglioretti DL, Yankaskas BC et al. (2003) Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Ann Intern Med 138:168–175. [DOI] [PubMed] [Google Scholar]
- [30].Kerlikowske K, Hubbard RA, Miglioretti DL et al. (2011) Comparative effectiveness of digital versus film-screen mammography in community practice in the United States: a cohort study. Ann Intern Med 155:493–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Berg WA. (2009) Tailored supplemental screening for breast cancer: what now and what next? AJR Am J Roentgenol 192:390–399. [DOI] [PubMed] [Google Scholar]
- [32].Roubidoux MA, Bailey JE, Wray LA, Helvie MA. (2004) Invasive cancers detected after breast cancer screening yielded a negative result: relationship of mammographic density to tumor prognostic factors. Radiology 230:42–48. [DOI] [PubMed] [Google Scholar]
- [33].Pisano ED, Gatsonis C, Hendrick E et al. (2005) Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med 353:1773–1783. [DOI] [PubMed] [Google Scholar]
- [34].Sardanelli F, Aase HS, Alvarez M et al. (2017) Position paper on screening for breast cancer by the European Society of Breast Imaging (EUSOBI) and 30 national breast radiology bodies from Austria, Belgium, Bosnia and Herzegovina, Bulgaria, Croatia, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Italy, Israel, Lithuania, Moldova, The Netherlands, Norway, Poland, Portugal, Romania, Serbia, Slovakia, Spain, Sweden, Switzerland and Turkey. Eur Radiol 27:2737–2743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Niklason LT, Christian BT, Niklason LE et al. (1997) Digital tomosynthesis in breast imaging. Radiology 205:399–406. [DOI] [PubMed] [Google Scholar]
- [36].Machida Y, Saita A, Namba H, Fukuma E. (2016) Automated volumetric breast density estimation out of digital breast tomosynthesis data: feasibility study of a new software version. Springerplus 5:780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Ciatto S, Houssami N, Bernardi D et al. (2013) Integration of 3D digital mammography with tomosynthesis for population breast-cancer screening (STORM): a prospective comparison study. Lancet Oncol 14:583–589. [DOI] [PubMed] [Google Scholar]
- [38].Skaane P, Bandos AI, Gullien R et al. (2013) Prospective trial comparing full-field digital mammography (FFDM) versus combined FFDM and tomosynthesis in a population-based screening programme using independent double reading with arbitration. Eur Radiol 23:2061–2071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Skaane P, Bandos AI, Gullien R et al. (2013) Comparison of digital mammography alone and digital mammography plus tomosynthesis in a population-based screening program. Radiology 267:47–56. [DOI] [PubMed] [Google Scholar]
- [40].Friedewald SM, Rafferty EA, Rose SL et al. (2014) Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA 311:2499–2507. [DOI] [PubMed] [Google Scholar]
- [41].Rafferty EA, Durand MA, Conant EF et al. (2016) Breast Cancer Screening Using Tomosynthesis and Digital Mammography in Dense and Nondense Breasts. JAMA 315:1784–1786. [DOI] [PubMed] [Google Scholar]
- [42].Houssami N (2015) Digital breast tomosynthesis (3D-mammography) screening: data and implications for population screening. Expert Rev Med Devices 12:377–379. [DOI] [PubMed] [Google Scholar]
- [43].McDonald ES, Oustimov A, Weinstein SP, Synnestvedt MB, Schnall M, Conant EF. (2016) Effectiveness of Digital Breast Tomosynthesis Compared With Digital Mammography: Outcomes Analysis From 3 Years of Breast Cancer Screening. JAMA Oncol 2:737–743. [DOI] [PubMed] [Google Scholar]
- [44].Corsetti V, Houssami N, Ferrari A et al. (2008) Breast screening with ultrasound in women with mammography-negative dense breasts: evidence on incremental cancer detection and false positives, and associated cost. Eur J Cancer 44:539–544. [DOI] [PubMed] [Google Scholar]
- [45].Scheel JR, Lee JM, Sprague BL, Lee CI, Lehman CD. (2015) Screening ultrasound as an adjunct to mammography in women with mammographically dense breasts. Am J Obstet Gynecol 212:9–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Berg WA, Blume JD, Cormack JB et al. (2008) Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA 299:2151–2163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Berg WA, Zhang Z, Lehrer D et al. (2012) Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA 307:1394–1404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].Buchberger W, Niehoff A, Obrist P, DeKoekkoek-Doll P, Dunser M. (2000) Clinically and mammographically occult breast lesions: detection and classification with high-resolution sonography. Semin Ultrasound CT MR 21:325–336. [DOI] [PubMed] [Google Scholar]
- [49].Sprague BL, Stout NK, Schechter C et al. (2015) Benefits, harms, and cost-effectiveness of supplemental ultrasonography screening for women with dense breasts. Ann Intern Med 162:157–166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Gordon PB, Goldenberg SL. (1995) Malignant breast masses detected only by ultrasound. A retrospective review. Cancer 76:626–630. [DOI] [PubMed] [Google Scholar]
- [51].Kaplan SS. (2001) Clinical utility of bilateral whole-breast US in the evaluation of women with dense breast tissue. Radiology 221:641–649. [DOI] [PubMed] [Google Scholar]
- [52].Leconte I, Feger C, Galant C et al. (2003) Mammography and subsequent whole-breast sonography of nonpalpable breast cancers: the importance of radiologic breast density. AJR Am J Roentgenol 180:1675–1679. [DOI] [PubMed] [Google Scholar]
- [53].Crystal P, Strano SD, Shcharynski S, Koretz MJ. (2003) Using sonography to screen women with mammographically dense breasts. AJR Am J Roentgenol 181:177–182. [DOI] [PubMed] [Google Scholar]
- [54].Wilczek B, Wilczek HE, Rasouliyan L, Leifland K. (2016) Adding 3D automated breast ultrasound to mammography screening in women with heterogeneously and extremely dense breasts: Report from a hospital-based, high-volume, single-center breast cancer screening program. Eur J Radiol 85:1554–1563. [DOI] [PubMed] [Google Scholar]
- [55].Kim WH, Chang JM, Lee J et al. (2017) Diagnostic performance of tomosynthesis and breast ultrasonography in women with dense breasts: a prospective comparison study. Breast Cancer Res Treat 162:85–94. [DOI] [PubMed] [Google Scholar]
- [56].Kelly KM, Dean J, Comulada WS, Lee SJ. (2010) Breast cancer detection using automated whole breast ultrasound and mammography in radiographically dense breasts. Eur Radiol 20:734–742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [57].Brem RF, Tabar L, Duffy SW et al. (2015) Assessing improvement in detection of breast cancer with three-dimensional automated breast US in women with dense breast tissue: the SomoInsight Study. Radiology 274:663–673. [DOI] [PubMed] [Google Scholar]
- [58].Ohuchi N, Suzuki A, Sobue T et al. (2016) Sensitivity and specificity of mammography and adjunctive ultrasonography to screen for breast cancer in the Japan Strategic Anti-cancer Randomized Trial (J-START): a randomised controlled trial. Lancet 387:341–348. [DOI] [PubMed] [Google Scholar]
- [59].Weigert JM. (2017) The Connecticut Experiment; The Third Installment: 4 Years of Screening Women with Dense Breasts with Bilateral Ultrasound. Breast J 23:34–39. [DOI] [PubMed] [Google Scholar]
- [60].Bae MS, Han W, Koo HR et al. (2011) Characteristics of breast cancers detected by ultrasound screening in women with negative mammograms. Cancer Sci 102:1862–1867. [DOI] [PubMed] [Google Scholar]
- [61].Kim SY, Han BK, Kim EK et al. (2017) Breast Cancer Detected at Screening US: Survival Rates and Clinical-Pathologic and Imaging Factors Associated with Recurrence. Radiology 284:354–364. [DOI] [PubMed] [Google Scholar]
- [62].Corsetti V, Houssami N, Ghirardi M et al. (2011) Evidence of the effect of adjunct ultrasound screening in women with mammography-negative dense breasts: interval breast cancers at 1 year follow-up. Eur J Cancer 47:1021–1026. [DOI] [PubMed] [Google Scholar]
- [63].Berg WA, Mendelson EB. (2014) Technologist-performed handheld screening breast US imaging: how is it performed and what are the outcomes to date? Radiology 272:12–27. [DOI] [PubMed] [Google Scholar]
- [64].Bosch AM, Kessels AG, Beets GL et al. (2003) Interexamination variation of whole breast ultrasound. Br J Radiol 76:328–331. [DOI] [PubMed] [Google Scholar]
- [65].Berg WA, Blume JD, Cormack JB, Mendelson EB. (2006) Operator dependence of physician-performed whole-breast US: lesion detection and characterization. Radiology 241:355–365. [DOI] [PubMed] [Google Scholar]
- [66].Berg WA, Blume JD, Cormack JB, Mendelson EB, Madsen EL, Investigators A. (2006) Lesion detection and characterization in a breast US phantom: results of the ACRIN 6666 Investigators. Radiology 239:693–702. [DOI] [PubMed] [Google Scholar]
- [67].Vourtsis A, Kachulis A. (2018) The performance of 3D ABUS versus HHUS in the visualisation and BI-RADS characterisation of breast lesions in a large cohort of 1,886 women. Eur Radiol 28:592–601. [DOI] [PubMed] [Google Scholar]
- [68].Skaane P, Gullien R, Eben EB, Sandhaug M, Schulz-Wendtland R, Stoeblen F. (2015) Interpretation of automated breast ultrasound (ABUS) with and without knowledge of mammography: a reader performance study. Acta Radiol 56:404–412. [DOI] [PubMed] [Google Scholar]
- [69].Moon WK, Shen YW, Huang CS et al. (2011) Comparative study of density analysis using automated whole breast ultrasound and MRI. Med Phys 38:382–389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [70].Moon WK, Lo CM, Chang JM et al. (2013) Rapid breast density analysis of partial volumes of automated breast ultrasound images. Ultrason Imaging 35:333–343. [DOI] [PubMed] [Google Scholar]
- [71].Giger ML, Inciardi MF, Edwards A et al. (2016) Automated Breast Ultrasound in Breast Cancer Screening of Women With Dense Breasts: Reader Study of Mammography-Negative and Mammography-Positive Cancers. AJR Am J Roentgenol 206:1341–1350. [DOI] [PubMed] [Google Scholar]
- [72].Kim EJ, Kim SH, Kang BJ, Kim YJ. (2014) Interobserver agreement on the interpretation of automated whole breast ultrasonography. Ultrasonography 33:252–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [73].Wang HY, Jiang YX, Zhu QL et al. (2012) Differentiation of benign and malignant breast lesions: a comparison between automatically generated breast volume scans and handheld ultrasound examinations. Eur J Radiol 81:3190–3200. [DOI] [PubMed] [Google Scholar]
- [74].Tagliafico AS, Calabrese M, Mariscotti G et al. (2016) Adjunct Screening With Tomosynthesis or Ultrasound in Women With Mammography-Negative Dense Breasts: Interim Report of a Prospective Comparative Trial. J Clin Oncol JCO634147 [Epub ahead of print]. [DOI] [PubMed]
- [75].Destounis S, Arieno A, Morgan R. Comparison of Cancers Detected by Screening Ultrasound and Digital Breast Tomosynthesis. Abstract 3162. The American Roentgen Ray Society (ARRS) 2017 Annual Meeting (2017) New Orleans, LA. [Google Scholar]
- [76].Dense-Breast.Info. (2017) Comparison of Cancers Detected by Screening Breast Ultrasound and Digital Breast Tomosynthesis http://densebreast-info.org/img/hottopic_destounis_arrs_2017_comparisonbymodality.pdf (accessed on Jan 30, 2018). [DOI] [PubMed]
- [77].Saslow D, Boetes C, Burke W et al. (2007) American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 57:75–89. [DOI] [PubMed] [Google Scholar]
- [78].National Comprehensive Cancer Network (NCCN) (2018) NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Genetic/Familial High-Risk Assessment: Breast and Ovarian NCCN, Fort Washington, PA. [DOI] [PubMed] [Google Scholar]
- [79].National Comprehensive Cancer Network (NCCN) (2018) NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Breast Cancer Screening and Diagnosis NCCN, Fort Washington, PA. [Google Scholar]
- [80].Monticciolo DL, Newell MS, Moy L, Niell B, Monsees B, Sickles EA. (2018) Breast Cancer Screening in Women at Higher-Than-Average Risk: Recommendations From the ACR. J Am Coll Radiol 15:408–414. [DOI] [PubMed] [Google Scholar]
- [81].King V, Brooks JD, Bernstein JL, Reiner AS, Pike MC, Morris EA. (2011) Background parenchymal enhancement at breast MR imaging and breast cancer risk. Radiology 260:50–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [82].Sak MA, Littrup PJ, Duric N, Mullooly M, Sherman ME, Gierach GL. (2015) Current and Future Methods for Measuring Breast Density: A Brief Comparative Review. Breast Cancer Manag 4:209–221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [83].Warner E, Messersmith H, Causer P, Eisen A, Shumak R, Plewes D. (2008) Systematic review: using magnetic resonance imaging to screen women at high risk for breast cancer. Ann Intern Med 148:671–679. [DOI] [PubMed] [Google Scholar]
- [84].Lo G, Scaranelo AM, Aboras H et al. (2017) Evaluation of the Utility of Screening Mammography for High-Risk Women Undergoing Screening Breast MR Imaging. Radiology 285:36–43. [DOI] [PubMed] [Google Scholar]
- [85].Riedl CC, Luft N, Bernhart C et al. (2015) Triple-modality screening trial for familial breast cancer underlines the importance of magnetic resonance imaging and questions the role of mammography and ultrasound regardless of patient mutation status, age, and breast density. J Clin Oncol 33:1128–1135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [86].van Zelst JCM, Mus RDM, Woldringh G et al. (2017) Surveillance of Women with the BRCA1 or BRCA2 Mutation by Using Biannual Automated Breast US, MR Imaging, and Mammography. Radiology 285:376–388. [DOI] [PubMed] [Google Scholar]
- [87].Heijnsdijk EA, Warner E, Gilbert FJ et al. (2012) Differences in natural history between breast cancers in BRCA1 and BRCA2 mutation carriers and effects of MRI screening-MRISC, MARIBS, and Canadian studies combined. Cancer Epidemiol Biomarkers Prev 21:1458–1468. [DOI] [PubMed] [Google Scholar]
- [88].Lehman CD, Blume JD, Weatherall P et al. (2005) Screening women at high risk for breast cancer with mammography and magnetic resonance imaging. Cancer 103:1898–1905. [DOI] [PubMed] [Google Scholar]
- [89].Leach MO, Boggis CR, Dixon AK et al. (2005) Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet 365:1769–1778. [DOI] [PubMed] [Google Scholar]
- [90].Kuhl CK, Schrading S, Leutner CC et al. (2005) Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol 23:8469–8476. [DOI] [PubMed] [Google Scholar]
- [91].National Institute for Health and Care Excellence. (2013) Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer. (Clinical guideline 164) https://www.nice.org.uk/guidance/CG164 (accessed on September 01, 2017). [PubMed]
- [92].Meindl A, Ditsch N, Kast K, Rhiem K, Schmutzler RK. (2011) Hereditary breast and ovarian cancer: new genes, new treatments, new concepts. Dtsch Arztebl Int 108:323–330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [93].Foulkes WD, Chappuis PO, Wong N et al. (2000) Primary node negative breast cancer in BRCA1 mutation carriers has a poor outcome. Ann Oncol 11:307–313. [DOI] [PubMed] [Google Scholar]
- [94].Tilanus-Linthorst MM, Kriege M, Boetes C et al. (2005) Hereditary breast cancer growth rates and its impact on screening policy. Eur J Cancer 41:1610–1617. [DOI] [PubMed] [Google Scholar]
- [95].Bick U (2015) Intensified surveillance for early detection of breast cancer in high-risk patients. Breast Care (Basel) 10:13–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [96].Le-Petross HT, Whitman GJ, Atchley DP et al. (2011) Effectiveness of alternating mammography and magnetic resonance imaging for screening women with deleterious BRCA mutations at high risk of breast cancer. Cancer 117:3900–3907. [DOI] [PubMed] [Google Scholar]
- [97].Cott Chubiz JE, Lee JM, Gilmore ME et al. (2013) Cost-effectiveness of alternating magnetic resonance imaging and digital mammography screening in BRCA1 and BRCA2 gene mutation carriers. Cancer 119:1266–1276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [98].Berg WA, Gutierrez L, NessAiver MS et al. (2004) Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology 233:830–849. [DOI] [PubMed] [Google Scholar]
- [99].Kuhl CK, Strobel K, Bieling H, Leutner C, Schild HH, Schrading S. (2017) Supplemental Breast MR Imaging Screening of Women with Average Risk of Breast Cancer. Radiology 283:361–370. [DOI] [PubMed] [Google Scholar]
- [100].O’Neill SM, Rubinstein WS, Sener SF et al. (2009) Psychological impact of recall in high-risk breast MRI screening. Breast Cancer Res Treat 115:365–371. [DOI] [PubMed] [Google Scholar]
- [101].Lehman CD. (2006) Role of MRI in screening women at high risk for breast cancer. J Magn Reson Imaging 24:964–970. [DOI] [PubMed] [Google Scholar]
- [102].Warren RM, Pointon L, Caines R et al. (2002) What is the recall rate of breast MRI when used for screening asymptomatic women at high risk? Magn Reson Imaging 20:557–565. [DOI] [PubMed] [Google Scholar]
- [103].Warner E, Hill K, Causer P et al. (2011) Prospective study of breast cancer incidence in women with a BRCA1 or BRCA2 mutation under surveillance with and without magnetic resonance imaging. J Clin Oncol 29:1664–1669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [104].Schacht DV, Yamaguchi K, Lai J, Kulkarni K, Sennett CA, Abe H. (2014) Importance of a personal history of breast cancer as a risk factor for the development of subsequent breast cancer: results from screening breast MRI. AJR Am J Roentgenol 202:289–292. [DOI] [PubMed] [Google Scholar]
- [105].Weinstock C, Campassi C, Goloubeva O et al. (2015) Breast magnetic resonance imaging (MRI) surveillance in breast cancer survivors. Springerplus 4:459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [106].Giess CS, Poole PS, Chikarmane SA, Sippo DA, Birdwell RL. (2015) Screening Breast MRI in Patients Previously Treated for Breast Cancer: Diagnostic Yield for Cancer and Abnormal Interpretation Rate. Acad Radiol 22:1331–1337. [DOI] [PubMed] [Google Scholar]
- [107].Gweon HM, Cho N, Han W et al. (2014) Breast MR imaging screening in women with a history of breast conservation therapy. Radiology 272:366–373. [DOI] [PubMed] [Google Scholar]
- [108].Lehman CD, Lee JM, DeMartini WB et al. (2016) Screening MRI in Women With a Personal History of Breast Cancer. J Natl Cancer Inst 108:pii: djv349. [DOI] [PubMed] [Google Scholar]
- [109].Cho N, Han W, Han BK et al. (2017) Breast Cancer Screening With Mammography Plus Ultrasonography or Magnetic Resonance Imaging in Women 50 Years or Younger at Diagnosis and Treated With Breast Conservation Therapy. JAMA Oncol 3:1495–1502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [110].Berg WA, Blume JD, Adams AM et al. (2010) Reasons women at elevated risk of breast cancer refuse breast MR imaging screening: ACRIN 6666. Radiology 254:79–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [111].U.S. Food and Drug Administration. (2017) FDA Drug Safety Communication: FDA warns that gadolinium-based contrast agents (GBCAs) are retained in the body; requires new class warnings https://www.fda.gov/Drugs/DrugSafety/ucm589213.htm (accessed on April 03, 2018).
- [112].Kuhl CK, Schrading S, Strobel K, Schild HH, Hilgers RD, Bieling HB. (2014) Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection-a novel approach to breast cancer screening with MRI. J Clin Oncol 32:2304–2310. [DOI] [PubMed] [Google Scholar]
- [113].Jain M, Jain A, Hyzy MD, Werth G. (2017) FAST MRI breast screening revisited. J Med Imaging Radiat Oncol 61:24–28. [DOI] [PubMed] [Google Scholar]
- [114].Strahle DA, Pathak DR, Sierra A, Saha S, Strahle C, Devisetty K. (2017) Systematic development of an abbreviated protocol for screening breast magnetic resonance imaging. Breast Cancer Res Treat 162:283–295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [115].Panigrahi B, Mullen L, Falomo E, Panigrahi B, Harvey S. (2017) An Abbreviated Protocol for High-risk Screening Breast Magnetic Resonance Imaging: Impact on Performance Metrics and BI-RADS Assessment. Acad Radiol 24:1132–1138. [DOI] [PubMed] [Google Scholar]
- [116].Choi BH, Choi N, Kim MY, Yang JH, Yoo YB, Jung HK. (2018) Usefulness of abbreviated breast MRI screening for women with a history of breast cancer surgery. Breast Cancer Res Treat 167:495–502. [DOI] [PubMed] [Google Scholar]
- [117].Chen SQ, Huang M, Shen YY, Liu CL, Xu CX. (2017) Abbreviated MRI Protocols for Detecting Breast Cancer in Women with Dense Breasts. Korean J Radiol 18:470–475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [118].Mori M, Akashi-Tanaka S, Suzuki S et al. (2017) Diagnostic accuracy of contrast-enhanced spectral mammography in comparison to conventional full-field digital mammography in a population of women with dense breasts. Breast Cancer 24:104–110. [DOI] [PubMed] [Google Scholar]
- [119].Jochelson MS, Pinker K, Dershaw DD et al. (2017) Comparison of screening CEDM and MRI for women at increased risk for breast cancer: A pilot study. Eur J Radiol 97:37–43. [DOI] [PubMed] [Google Scholar]
- [120].McDonald ES, Hammersley JA, Chou SH et al. (2016) Performance of DWI as a Rapid Unenhanced Technique for Detecting Mammographically Occult Breast Cancer in Elevated-Risk Women With Dense Breasts. AJR Am J Roentgenol 207:205–216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [121].Partridge S Breast DWI Potential and Pitfalls: Results of ACRIN 6702 and 6698 Multicenter Trials. The 6th International Congress on Magnetic Resonance Imaging 2018.
- [122].Hruska CB. (2017) Molecular Breast Imaging for Screening in Dense Breasts: State of the Art and Future Directions. AJR Am J Roentgenol 208:275–283. [DOI] [PubMed] [Google Scholar]
- [123].Rhodes DJ, Hruska CB, Phillips SW, Whaley DH, O’Connor MK. (2011) Dedicated dual-head gamma imaging for breast cancer screening in women with mammographically dense breasts. Radiology 258:106–118. [DOI] [PubMed] [Google Scholar]
- [124].Rhodes DJ, Hruska CB, Conners AL et al. (2015) Journal club: molecular breast imaging at reduced radiation dose for supplemental screening in mammographically dense breasts. AJR Am J Roentgenol 204:241–251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [125].Shermis RB, Wilson KD, Doyle MT et al. (2016) Supplemental Breast Cancer Screening With Molecular Breast Imaging for Women With Dense Breast Tissue. AJR Am J Roentgenol 207:450–457. [DOI] [PubMed] [Google Scholar]