

Abstract
Purpose
Growing evidence supports the role of student assistantships in enhancing graduates’ preparedness for practice. However, there is limited evidence concerning the impact of aligning assistantships with graduates’ first doctor post. The aims of our study were to determine newly-qualified doctors’ views on the value their assistantship experience, effects on anxiety levels, confidence and preparedness for increased responsibilities, exploring change over time and whether effects differ according to assistantship alignment.
Design
We conducted a longitudinal cross-sectional online questionnaire study examining experiences of aligned and non-aligned assistantships across the transition from medical student to newly-qualified doctor. The questionnaire was distributed to final year medical students within Wales, UK (n=351) and those commencing their first post in Wales, UK (n=150) in June 2015 at Time 1 (T1), and repeated in September 2015 (1 month following transition, T2) and January 2016 (T3).
Results
Response rates at T1 were 50% (n=251, aligned=139, non-aligned=112), T2 36% (n=179, aligned=83, non-aligned=96) and T3 28% (n=141, aligned=69, non-aligned=72): 15% (n=73, aligned=36, non-aligned=37) completed all questionnaires. Paired longitudinal analysis was undertaken where possible. Significant differences were observed between participants on aligned and non-aligned assistantships in terms of the value they place on their assistantship experiences, their anxiety, confidence levels and preparedness for responsibility.
Conclusion
Although not sustained, aligned assistantships seem to provide graduates with additional benefits during the August transition. Further work is required to establish what it is about the aligned assistantship programme that works and why.
Keywords: workplace learning; transitions; students, medical; questionnaire; United Kingdom
Strengths and limitations of this study.
This is the largest study to date to examine the impact of assistantship alignment on aspects of preparedness for practice.
The longitudinal nature of the study enables us to examine the impact of the assistantship programme over time, rather than as a snapshot in time.
Although respondents came from a range of UK medical schools, those experiencing an aligned assistantship were all trained and subsequently worked in a single UK country.
This study comprises self-reported measures.
Introduction
Evidence suggests that medical students’ transition into the clinical workplace can have a negative impact on them in terms of their general anxiety and risk of burnout,1–3 alongside impacting patient care and safety.1 4–10 Thus preparedness for practice is an important focus for medical schools and regulators worldwide.11–15 The challenges of preparing for practice are clear. Tallentire et al identified how junior and senior doctors alike recognise the difficulties in translating knowledge into practice; with juniors expressing that they knew what to do, but not how to do it.16 Senior doctors attribute this cognitive gap to lack of rehearsal. Educational interventions can smooth this gap by increasing graduates’ preparedness for how. These include student assistantship, shadowing and induction periods.1 14 We focus here on student assistantships: ‘a period during which a student acts as assistant to a junior doctor, with defined duties under appropriate supervision’.14 Assistantship has been a compulsory part of the UK undergraduate curricular since 2011–2012. This period of acting up occurs during students’ final year, but how it is implemented differs across UK educational institutions.17 For example, different medical schools position it at different times across the curriculum with respect to final exams, at different locations and different durations.17–23 Often students staying locally are assigned to assistantships posts in the specific hospitals where they will subsequently work.20 However, few schools offer aligned assistantship placements within the specific team into which they will transition.18 19
At the beginning of their assistantship period students tend to report feeling generally competent with their own clinical skills,20 23 reflecting the plethora of previous literature in the general area of preparedness.1 Unsurprisingly, before–after studies tend to see general improvements in graduates’ self-reported confidence (or reduced anxiety) around their skills immediately following their assistantship period.18 20 21 23 By far the most common, robust finding across all studies is the facilitation of teamwork1 17–23: students are seen as team members, thus facilitating their understanding, confidence and a sense of belonging. Students experiencing assistantships unaligned with their first post (eg, not on the same ward or same speciality) feel disadvantaged compared with those whose assistantship is fully aligned.18 19
The opportunity within assistantship placements for students to engage in meaningful learning (taking up opportunities for active patient care involvement, increasing responsibility) is also highlighted across the studies.19 21 However, opportunities are not always present or taken up: for example, more missed opportunities can occur in surgical than during medical placements.21 Burford et al 21 believe that this is more to do with structural or cultural barriers to having ‘hands-on’ experiences, such as having fewer senior doctors around to support the juniors, than it is to students’ motivation. Despite this, familiarisation with the workplace environment (ie, wardcraft) is frequently reported.18 19 23
Research examining both supervisors’ and newly qualified doctors’ reports suggests that supervisors have a more optimistic view than students around graduates’ engagement in learning,21 and there is variation in supervisor experience (eg, some supervisors are reluctant to allow students to undertake routine trainee–doctor procedures).19 22 In Jones’ study examining the differences between an aligned and non-aligned model, consultants openly admitted to emotionally disinvesting in those not staying in their particular placement (non-aligned model) for their first trainee post as they ‘will not reap the benefits’.19
Other research has examined the impact that assistantship alignment, gender, professional identity and anxiety, has on burnout across medical graduates’ transition into practice.24 Using a longitudinal 1 year cohort study, Monrouxe et al administered questionnaires across four time points from assistantship to 10 months' postgraduation. They found that self-reported anxiety, professional identity and patient-related burnout remained the same over time, with personal and work-related burnout increasing. Using linear mixed-effect models, they identified males as having significantly lower personal burnout but higher patient-related burnout than females. Additionally, anxiety was significantly associated with higher burnout, but professional identity was significantly related to lower burnout, over time. Furthermore, significantly lower personal and work-related burnout over time was found for those experiencing an aligned assistantship.25
However, despite the research around assistantships, there is sparse evidence for the relative effects of assistantship periods and even less around different assistantship models.1 18–23 Much of the research investigating the effects of the assistantship period utilises a before–after questionnaire format,20 21 23 25 or initial questionnaire with follow-up interviews,18 with only one study matching participant data from Time 1 (T1) and Time 2 (T2)24. Further, questionnaire content is inconsistent across studies with each programme having a different duration and configuration, thus limiting comparability. Furthermore, there is a general tendency for relatively low respondent numbers.18 21–23 Taken together this makes it difficult to draw any strong conclusions regarding the effects of the assistantship period. No one study builds on another.
Aims
This study aims to address gaps in the literature by building on our previous work,19 24 examining the relative value and effects of assistantship alignment with first post and addresses the following research questions:
RQ1: Do newly qualified doctors value their assistantship experience?
RQ1a: Does this differ according to alignment of assistantship with first post?
RQ1b: Does this change over time?
RQ2: When transitioning jobs in the first postgraduate year, does aligning assistantships with first post effect newly qualified doctors in terms of their:
RQ2a: Anxiety levels?
RQ2b: Confidence levels?
RQ2c: Preparedness for the step-change in responsibilities?
RQ2d: Does this change over time?
Methods
A longitudinal cross-sectional online questionnaire design was used to assess newly qualified doctors’ self-reported effects of aligned and non-aligned assistantships across a single country in the UK.
Study setting
The study is set in Wales, UK. The Welsh Deanery (provider of the initial postgraduate training in Wales) works closely with the two medical schools within the country: a predominantly school-entry 5-year course (iro 280 graduates annually) and a graduate-entry medical school (iro 70 graduates annually). Close collaboration between both schools on the Senior Student Assistantship (SSA: the final placement in Wales), makes this a distinctive country context within which to examine the impact of the assistantship variables. The SSA commences following students’ first post allocations with those remaining in Wales matched to their first job. Students leaving Wales are allocated an SSA placement in a role similar to their first job where possible. In 2015, 52% of graduates from Welsh medical schools (n=182) undertook an aligned SSA. All placements are designed to allow students to learn generic skills associated with day-to-day, high-quality patient management, commensurate with the General Medical Council’s ‘Outcomes for Practice’ document.13 Students’ first post on graduation begins on the first Wednesday in August. They continue in this post for 4 months until the first week in December when they rotate to their second postgraduate post.
Patient and public involvement
No patients or public representatives were involved in either the development of the study or participating in the study.
Procedure
Ethical approval for the study was obtained prior to commencement. Final year students at the two schools in Wales (n=351) and students commencing their first post in Wales (n=150; from 27 UK medical schools) were invited to complete an online questionnaire at three time periods: T1 during the SSA in Wales (8 June to 6 July 2015), T2 1 month after transition into practice (1–30 September 2015) and T3 1 month after their second post (4 January to 4 February 2016). Thus, only those participants who attended medical school in Wales, and subsequently began work in Wales, were aligned. However, as we continued to contact original T1 participants when they left Wales, non-aligned participants comprised graduates from medical schools within and outwith Wales. All participants graduating from medical schools outside Wales were non-aligned.
At T1, a link was sent via email to students in Wales by medical school administrators, and to other UK graduates outwith Wales by Foundation School administrators. Participants were invited to provide an email address if they wished to be entered into a prize draw. With consent this was used to track responses longitudinally. Only SEW had access to these identifying data. At T2 and T3, participants were invited by SEW directly if they previously provided an email address. Additionally, the link was circulated by programme administrators and posted on targeted social media outlets (eg, year group Facebook pages). Postgraduate representatives also raised awareness of the questionnaire.
Questionnaire development
The T1 questionnaire was developed following discussions with course developers, a group interview with final-year medical students in Wales undertaking assistantships (aligned/non-aligned), junior doctors and consultant supervisors.19 T1 questionnaire included eight items (box 1). T2 and T3 questionnaires included two identical questions (Q9 and Q10) as well as two questions included in the T1 questionnaire (Q1 and Q2). Additionally, T2 and T3 questionnaires included questions to suit the postgraduate context (Qs11–14). All three questionnaires included modified versions of the Hamilton anxiety rating scale (HAM-A),26 the Copenhagen burnout inventory27 and professional identity, cognitive flexibility and teamworking scales,28 reported elsewhere.25 The entire questionnaire comprised 16 screens including an introduction, three demographic/background screens, a ‘your story’ screen, a ‘prize draw’ screen and an ending summary screen. Participants could not move forward without completing each section (apart from the final ‘your story’ section) although they could navigate backwards through the questionnaire. Responses to all items in box 1 (the focus of this paper) comprised a 5-point Likert scale (strongly disagree=1, strongly agree=5). IBM SPSS Statistics V.20 was used to assist in the analysis. A combination of descriptive statistics, related-sample t-tests and repeated measures analysis of variance (ANOVA) was performed.
Box 1. Questionnaire Items T1–T3.
T1 Questionnaire (during assistantship)
Q1. My assistantship has been a waste of time.*
Q2. My anxieties about starting work in my first junior doctor post are greatly relieved.
Q3. This has been a valuable time for me to learn from mistakes now, before I have more responsibility.
Q4. The consultant in my team does not understand the purpose of the Assistantship programme.*
Q5. I have been given more responsibility than ever before.
Q6. I have received little in the way of ‘learning about the workplace’.*
Q7. I understand the job of a junior doctor better now.
Q8. I have had no valuable experience in managing critically ill patients (eg, attending cardiac arrest calls).*
T2 Questionnaire (first post)
Q1. My assistantship was a waste of time.*
Q2. My anxieties about starting work in my first junior doctor post were greatly relieved by my assistantship.
Q9. My assistantship enhanced my confidence about starting as a junior doctor.
Q10. My assistantship prepared me well for the responsibility of being a junior doctor.
Q11. Starting my junior doctor job has made me appreciate the value of my assistantship more.
Q12. On reflection, I think I could have made more of my assistantship experience.
Q13. My assistantship has prepared me well for the junior doctor post I will move to next.
T3 Questionnaire (second post)
Q1. My assistantship was a waste of time.*
Q2. My anxieties about starting work in my second junior doctor post were greatly relieved by my assistantship.
Q9. My assistantship enhanced my confidence about starting my second junior doctor post.
Q10. My assistantship prepared me well for the responsibility of my second junior doctor post.
*These questions were reversed scored, so a lower score indicates agreement with the negative statement.
Results
We begin by reporting participants and response rates for the questionnaire at each time point. We then report the item-by-item analyses for individual questions (over time where appropriate).
Respondents
At T1 we have 251 respondents (50% response rate; aligned=139, non-aligned=112; Table 1). Longitudinal data from three time points were available from 73 participants (aligned=36, non-aligned=37). Additionally, some participants completed the questionnaire at two time-points: 131 participants at T1 and T2 (aligned=65, non-aligned=66) and 103 participants (aligned 45, non-aligned=58) at T2 and T3, respectively.
Table 1.
Participants by alignment
| Questionnaire phase | Participants | Response rate (%) |
|||
| Aligned | Non-aligned | Total | |||
| All questionnaire data | T1 | 139 | 112 | 251 | 50 |
| T2 | 83 | 96 | 179 | 36 | |
| T3 | 69 | 72 | 141 | 28 | |
| Paired longitudinal data | T1 and T2 | 65 | 66 | 131 | 26 |
| T2 and T3 | 45 | 58 | 103 | 21 | |
| All time points | 36 | 37 | 73 | 15 | |
Individual item analysis: longitudinal data
We first report participants’ responses for specific items in the questionnaire, beginning with Qs 1, 2, 9 and 10 as these all have at least two time-points. Only participants who completed all three questionnaires were included in these analyses (n=36 aligned, n=37 non-aligned).
Q1. ‘My assistantship was a waste of time’ (all time points, reversed scored)
As scores were reversed for this statement, a lower score indicates agreement with the negative statement. There was a significant effect of time, F(2,142)=3.15, p=0.046. Pairwise comparison showed that the aligned and non-aligned groups agreed with this question significantly more at T2 than T1 (p<0.02; mean 4.9 at T1 vs 4.7 at T2; and 4.2 vs 3.9 for aligned and non-aligned participant groups, respectively) with no significant differences at T3 (mean 4.7 and 4.1 for aligned and non-aligned participant groups, respectively). Those experiencing a non-aligned assistantship agreed more with this statement at all three time points (p<0.0001: figure 1).
Figure 1.
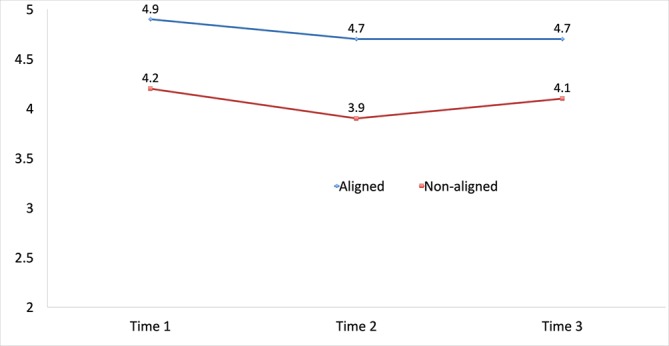
Main effect of value of assistantship experience (Q1).
Q2. ‘My anxieties about starting work in my [first/second] junior doctor post were greatly relieved by my assistantship’ (all time points)
The Huynh-Feldt correction was used as sphericity is not assumed. There was a significant effect of time, F(1.8,71)=7.18, p=0.002 and a significant interaction between time and assistantship alignment, F(1.8,71)=4.655, p=0.01: pairwise comparisons showed that participants experiencing an aligned assistantship reported agreeing with this question significantly more than those on a non-aligned assistantship at T1 (assistantship period) and T2 (first post: p<0.03), but by T3 (second job) this difference had disappeared (see figure 2).
Figure 2.
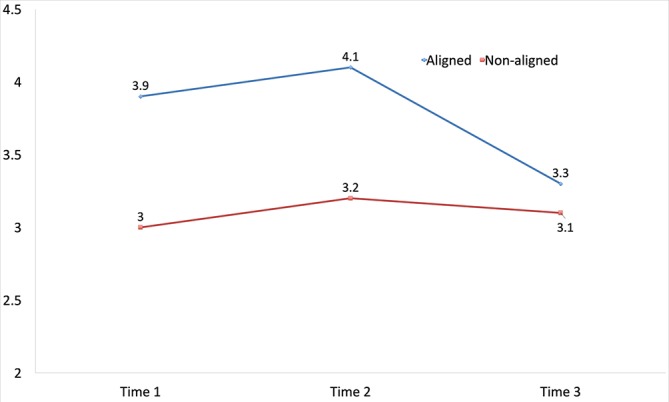
Interaction between assistantship experience and anxiety relief over time (Q2).
Q9. ‘My assistantship enhanced my confidence about starting my [second] junior doctor post’ (T2 and T3)
There was a significant effect of time, F(1,71)=27.0, p=0.0001 and interaction between time and assistantship alignment, F(1,71)=20.12, p=0.0001: at T2, pairwise comparison showed that participants experiencing an aligned assistantship were significantly more likely to agree that their assistantships had enhanced their confidence about starting in their first post than those experiencing a non-aligned assistantship (p<0.01; means 4.4 vs 3.5, respectively). However, at T3 the differences between aligned/non-aligned groups had disappeared (means 3.3 vs 3.4, respectively; figure 3).
Figure 3.
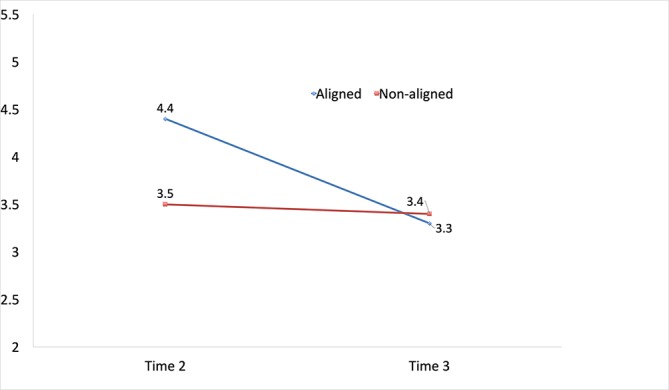
Interaction between assistantship experience and confidence over time (Q9).
Q10. ‘My assistantship prepared me well for the responsibility of my [second] junior doctor post’ (T2 and T3).
There was a significant main effect of time, F(1,71)=13.3, p=0.001: both groups reported feeling less prepared for the responsibility of their second than their first post. Pairwise comparisons were significant for aligned versus non-aligned assistantship groups: participants experiencing aligned assistantships reported feeling more prepared than those experiencing non-aligned assistantships (p<0.004; means: 4.0 vs 3.2, 3.2 vs 2.9 for aligned and non-aligned groups at T2 and T3, respectively: figure 4).
Figure 4.
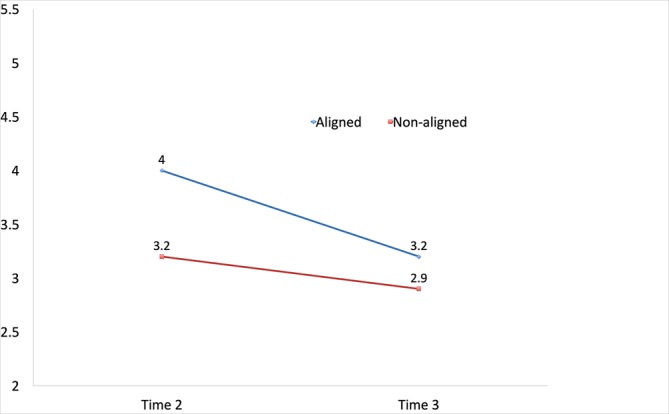
Main effect of preparedness for responsibility and assistantship experience (Q10).
Individual item analysis: single time-point items
We also asked questions specific to the time at which the questionnaire was delivered. Thus, at T1 these questions related to the specific assistantship placement participants (Qs 3–8, box 1), at T2 these are related to participants’ reflections on their assistantship and how well it prepared them for their junior doctor job (Qs 11–13, box 1). All participants were compared at each time point (n=139 and n=112 at T1, n=83 and n=96 at T2 for aligned and non-aligned, respectively: table 2). Of the nine questions analysed, all but one (Q12) were significantly different between aligned and non-aligned participant groups: neither group felt that they could have made more of their assistantship experience. Of the eight that were significantly different by alignment group, the aligned group rated items significantly higher than the non-aligned group for seven of these (note, some items were reversed scored as they were presented in a negative format). Thus, those on aligned assistantships felt: they were a valuable time for learning from mistakes (Q3); their consultant in their team understood the purpose of the assistantship programme (Q4); they were given greater responsibility (Q5); they learnt a lot about the workplace (Q6); understood the junior doctor role better (Q7); had valuable experiences in managing critically ill patients (Q8) and appreciated the value of the assistantship (Q11). However, when considering how well the assistantship post prepared them for their second junior doctor post (Q13), levels of agreement were higher among the non-aligned group.
Table 2.
Individual item analyses at times 1 and 2
| Statement | Alignment | n | Mean | Std. dev | Std. error Mean | t | df | Sig |
| Time 1 | ||||||||
| Q3. This has been a valuable time for me to learn from mistakes now, before I have more responsibility. | Aligned | 139 | 4.37 | 0.684 | 0.058 | 4.614 | 249 | 0.0001 |
| Non-aligned | 112 | 3.93 | 0.846 | 0.846 | ||||
| Q4. The consultant in my team does not understand the purpose of the assistantship programme.*† | Aligned | 139 | 4.01 | 0.925 | 0.078 | 2.570* | 233 | 0.011 |
| Non-aligned | 112 | 3.71 | 0.965 | 0.091 | ||||
| Q5. I have been given more responsibility than ever before. | Aligned | 139 | 3.93 | 1.047 | 0.089 | 3.343* | 214 | 0.001 |
| Non-aligned | 112 | 3.43 | 1.271 | 0.120 | ||||
| Q6. I have received little in the way of ‘learning about the workplace’.* | Aligned | 139 | 4.10 | 0.927 | 0.079 | 2.952 | 249 | 0.003 |
| Non-aligned | 112 | 3.76 | 0.893 | 0.084 | ||||
| Q7. I understand the job of a junior doctor better now. | Aligned | 139 | 4.14 | 0.782 | 0.066 | 3.975* | 211 | 0.0001 |
| Non-aligned | 112 | 3.69 | 0.968 | 0.091 | ||||
| Q8. I have had no valuable experience in managing critically ill patients (eg, attending cardiac arrest calls).*† | Aligned | 139 | 3.35 | 1.027 | 0.087 | 2.608* | 220 | 0.010 |
| Non-aligned | 112 | 2.97 | 1.197 | 0.113 | ||||
| TIME 2 | ||||||||
| Q11. Starting my junior doctor job has made me appreciate the value of my assistantship more. | Aligned | 83 | 4.28 | 0.668 | 0.733 | 7.644* | 162 | 0.0001 |
| Non-aligned | 96 | 3.27 | 1.071 | 0.109 | ||||
| Q12. On reflection, I think I could have made more of my assistantship experience. | Aligned | 83 | 2.80 | 1.124 | 0.123 | −0.559 | 177 | 0.577 |
| Non-aligned | 96 | 2.89 | 1.035 | 0.106 | ||||
| Q13. My assistantship has prepared me well for the junior doctor post I will move to next. | Aligned | 83 | 2.46 | 0.991 | 0.109 | −2.997 | 177 | 0.003 |
| Non-aligned | 96 | 2.93 | 1.088 | 0.111 | ||||
*Questions marked were reverse scored, so a lower score indicates agreement with the negative statement.
†Equal variances not assumed.
Discussion
Our study adds to the evidence from questionnaire studies concerning the effects of assistantships as transition interventions.20 23 25 We examined the relative value of aligning assistantship placements with students’ first post as newly qualified doctors across three time points: during the assistantship placement, 1 month into their first post and 1 month into their second post. Participants responded positively to statements concerning the impact of their aligned and non-aligned assistantship on their preparedness for practice across a range of domains. Participants who experienced an aligned assistantship at T1 were consistently more likely to attribute enhanced preparedness for their first junior doctor role (T2) to their assistantship experiences. Although participants who experienced an aligned assistantship felt this to be of greater value than those who did not at all time points, the effects of anxiety relief and enhanced confidence for the aligned group was diminished at T3. This finding accords with previous research suggesting that an extended shadowing placement – akin to the aligned assistantship model described here – has the potential to reduce anxiety associated with the August transition.29 The statistically significant differences observed between aligned and non-aligned groups'’ responses to anxiety-related questions within our data corroborate this idea, and also showed the limits of this benefit. It is important to note that what we are considering here is the issue of context-specific anxiety. This differs from generalised anxiety as measured by, for example, the Hamilton Anxiety Scale,26 which has been shown to be a predictor of burnout over this transition period.25 Interestingly, in these data at T3, participants who had experienced a non-aligned assistantship believed that their assistantship had prepared them well for their second post significantly more than those who had experienced an aligned assistantship. However, this item received the lowest means across all statements for both groups.
Taken together, these results suggest the importance of assistantships in general as a mechanism for supporting the transition of medical graduates into practice, but more importantly of the added value of aligned assistantships during this time. However, our results also demonstrate that this added value washes out over time: by the time participants reach their second transition a few months later, there appears to be little advantage to having undertaken an aligned assistantship. Indeed, our data suggest that at the point of rotating to their second post, non-aligned assistantships might convey some advantage; having started their first junior doctor post without any elongated shadowing period, they have undertaken this transition before. Ultimately, it appears that, rather than eliminating anxiety and lack of confidence around the transition into their junior doctor role, the aligned assistantships merely defers this until a later point. This does not necessarily mean that alignment is unhelpful; rather it means that this is not the end of the story and further interventions are required over time.
This study has a number of strengths and limitations. In terms of strengths, to our knowledge, this is the first study that has specifically examined the longitudinal impact of assistantships by analysing matched data, in addition to unpacking the differences between aligned and non-aligned models of assistantships. Thus, our data permit paired longitudinal analysis that has served to enhance our understanding of individuals’ perception of assistantship utility and emotional responses to changes in their role at different transition points during the first junior doctor year. Our data includes the views of graduates from 27 different UK medical schools.
While our study allowed for comparisons between students who undertook aligned and non-aligned assistantships, we recognise limitations. First, the aligned participant cohort is homogenous in its composition in that they all come from one of two medical schools within a single country. The study is also limited by attrition in response rates over time: reducing from n=252 (50% response rate) at Time 1 to n=141 (28% response rate) at Time 3, with n=73 responding across all three time-points. A number of factors may have contributed to this. At Times 2 and 3 our ability to contact graduates of Welsh medical schools undertaking their junior doctor training elsewhere in the UK was not possible unless participants had provided an email address in a previous questionnaire phase. This problem was compounded at Time 3; in January, a number of institutional email addresses provided by participants at Times 1 and 2 had expired if individuals left their institutions. The study is also subject to responder bias and it is possible that individuals with positive experiences of aligned assistantships and individuals with negative experiences of non-aligned assistantships represented the groups most likely to participate. Finally, we have used a questionnaire response format that is numerical. Given that we have been examining issues such as anxieties, anxiousness and preparedness for practice, Likert-scale responses can only provide us with a partial picture of the emotional journey our respondents went through.
Despite these limitations, our study suggests that consideration needs to be given to strategies that support junior doctors as they rotate to their second post. There may be value in considering the model of practice that was used within the Broad-Based Training programme which enabled trainees to spend 10% of their time in a forthcoming speciality.30 Further, although we have found that undertaking an aligned assistantship has positive outcomes, we have yet to fully understand what it feels like for an undergraduate medical student to transition into practice through these differentially aligned assistantship programmes. We also are unaware of the specific mechanisms through which the outcomes we report are achieved, and for whom they are most beneficial. Future research would benefit from undertaking a range of different studies – including more qualitative studies examining emotions and how these are managed as well as realist approaches. Such qualitative data could be analysed in a variety of ways, including specifically examining emotional talk and strategies around regulating emotions in situ.31 32 Realist research delves deeper into the whys and hows of interventions, unpacking these issues further to inform programme development.33 We urge future research around the assistantship programme to move into these realms. In addition, further research should seek to explore how graduates’ experience during their own assistantship influences their behaviour as assistantship supervisors towards the end of their first year as a newly qualified doctor.
Supplementary Material
Acknowledgments
The authors wish to thank the wider research team for their involvement in the study design, helping to secure funding ethics approvals and data collection (Mr Michael Stechman, Dr Tom Yapp, Dr Anton Saayman, Dr Steve Riley, Dr Wyn Harris, Dr Lori Black). In addition, the authors thank Ms Nerys Jones and Ms Hannah Perks for their assistance in testing the questionnaire.
Footnotes
Contributors: LVM and AB contributed to the conception of the study; LVM, AB and SEW designed the work; SEW contributed to the acquisition of the data; SEW and LVM contributed to the analysis of the data and all authors contributed to the interpretation of data; SEW and LVM drafted the manuscript. All authors revised the manuscript critically for important intellectual content. All authors gave their final approval of the version to be published; all authors agree to be accountable for all aspects of the manuscript and will ensure that any questions relating to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Funding: The study was partly funded by a small research grant from the Association of the Study of Medical Education (ASME) and partly by the School of Medicine, Cardiff University who were informed of progress with the collection, analysis and interpretation of data but the researchers remained fully independent of the funders.
Competing interests: None declared.
Ethics approval: School of Medicine Research Ethics Committee at Cardiff University: SMREC Reference Number: 15/08.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: No additional unpublished data are available outside the research team.
Patient consent for publication: Not required.
References
- 1. Monrouxe LV, Bullock A, Gormley G, et al. New graduate doctors' preparedness for practice: a multistakeholder, multicentre narrative study. BMJ Open 2018;8:e023146 10.1136/bmjopen-2018-023146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Markwell AL, Wainer Z. The health and wellbeing of junior doctors: insights from a national survey. Med J Aust 2009;191:441–4. [DOI] [PubMed] [Google Scholar]
- 3. O’Donnell M, Noad R, Boohan M, et al. Foundation programme impact on junior doctor personality and anxiety in Northern Ireland. Ulster Med J 2012;81:19–25. [PMC free article] [PubMed] [Google Scholar]
- 4. Vaughan L, McAlister G, Bell D. ’August is always a nightmare': results of the royal college of physicians of edinburgh and society of acute medicine august transition survey. Clin Med 2011;11:322–6. 10.7861/clinmedicine.11-4-322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Young JQ, Ranji SR, Wachter RM, et al. "July effect": impact of the academic year-end changeover on patient outcomes: a systematic review. Ann Intern Med 2011;155:309–15. 10.7326/0003-4819-155-5-201109060-00354 [DOI] [PubMed] [Google Scholar]
- 6. Inaba K, Recinos G, Teixeira PG, et al. Complications and death at the start of the new academic year: is there a July phenomenon? J Trauma 2010;68:19–22. 10.1097/TA.0b013e3181b88dfe [DOI] [PubMed] [Google Scholar]
- 7. Phillips DP, Barker GE. A July spike in fatal medication errors: a possible effect of new medical residents. J Gen Intern Med 2010;25:774–9. 10.1007/s11606-010-1356-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Yaghoubian A, de Virgilio C, Chiu V, et al. "July effect" and appendicitis. J Surg Educ 2010;67:157–60. 10.1016/j.jsurg.2010.04.003 [DOI] [PubMed] [Google Scholar]
- 9. Massey N. Black Wednesday' expected to see rise in hospital patient deaths as junior doctors start work. The Mirror 2014. [Google Scholar]
- 10. Alexander C, Cameron A, Millar J, et al. Can new doctors be prepared for practice? A review. Clin Teach 2014;11:188–92. 10.1111/tct.12127 [DOI] [PubMed] [Google Scholar]
- 11. Langdale LA, Schaad D, Wipf J, et al. Preparing graduates for the first year of residency: are medical schools meeting the need? Acad Med 2003;78:39–44. [DOI] [PubMed] [Google Scholar]
- 12. Tokuda Y, Goto E, Otaki J, et al. Undergraduate educational environment, perceived preparedness for postgraduate clinical training, and pass rate on the national medical licensure examination in Japan. BMC Med Educ 2010;10:35 10.1186/1472-6920-10-35 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. General Medical Council. Tomorrow’s doctors: outcomes and standards for undergraduate medical education. London: General Medical Council, 2009. [Google Scholar]
- 14. GMC. Clinical placements for medical students: advice supplementary to tomorrow’s doctors (2009). London: General Medical Council, 2011. [Google Scholar]
- 15. GMC. Promoting excellence: standards for medical education and training. 2015. http://www.gmc-uk.org/Promoting_excellence_standards_for_medical_education_and_training_0715.pdf_61939165.pdf.
- 16. Tallentire VR, Smith SE, Skinner J, et al. Understanding the behaviour of newly qualified doctors in acute care contexts. Med Educ 2011;45:995–1005. 10.1111/j.1365-2923.2011.04024.x [DOI] [PubMed] [Google Scholar]
- 17. Crossley JG, Vivekananda-Schmidt P. Student assistantships: bridging the gap between student and doctor. Adv Med Educ Pract 2015;6:447–57. 10.2147/AMEP.S62822 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Lightman E, Kingdon S, Nelson M. A prolonged assistantship for final-year students. Clin Teach 2015;12:115–20. 10.1111/tct.12272 [DOI] [PubMed] [Google Scholar]
- 19. Jones OM, Okeke C, Bullock A, et al. ’He’s going to be a doctor in August': a narrative interview study of medical students' and their educators' experiences of aligned and misaligned assistantships. BMJ Open 2016;6:e011817 10.1136/bmjopen-2016-011817 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Braniff C, Spence RA, Stevenson M, et al. Assistantship improves medical students' perception of their preparedness for starting work. Med Teach 2016;38:51–8. 10.3109/0142159X.2015.1045843 [DOI] [PubMed] [Google Scholar]
- 21. Burford B, Ellis E, Williamson A, et al. Learning opportunities in ’student assistantships'. Clin Teach 2015;12:121–7. 10.1111/tct.12269 [DOI] [PubMed] [Google Scholar]
- 22. Fullbrook A, Ross M, Mellanby E, et al. Initial experiences of a student assistantship. Clin Teach 2015;12:310–4. 10.1111/tct.12355 [DOI] [PubMed] [Google Scholar]
- 23. Hawkins A, Stanton A, Forbes K. An extended assistantship for final-year students. Clin Teach 2015;12:305–9. 10.1111/tct.12351 [DOI] [PubMed] [Google Scholar]
- 24. Monrouxe LV, Bullock A, Tseng HM, et al. Association of professional identity, gender, team understanding, anxiety and workplace learning alignment with burnout in junior doctors: a longitudinal cohort study. BMJ Open 2017;7:e017942 10.1136/bmjopen-2017-017942 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Monrouxe LV, Grundy L, Mann M, et al. How prepared are UK medical graduates for practice? A rapid review of the literature 2009-2014. BMJ Open 2017;7:e013656 10.1136/bmjopen-2016-013656 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol 1959;32:50–5. 10.1111/j.2044-8341.1959.tb00467.x [DOI] [PubMed] [Google Scholar]
- 27. Kristensen TS, Borritz M, Villadsen E, et al. The copenhagen burnout inventory: a new tool for the assessment of burnout. Work Stress 2005;19:192–207. 10.1080/02678370500297720 [DOI] [Google Scholar]
- 28. Adams K, Hean S, Sturgis P, et al. Investigating the factors influencing professional identity of first-year health and social care students. Learning in Health and Social Care 2006;5:55–68. 10.1111/j.1473-6861.2006.00119.x [DOI] [Google Scholar]
- 29. Van Hamel C, Jenner LE. Prepared for practice? a national survey of UK foundation doctors and their supervisors. Med Teach 2015;37:181–8. 10.3109/0142159X.2014.947929 [DOI] [PubMed] [Google Scholar]
- 30. Muddiman E, Bullock AD, MacDonald J, et al. ’It’s surprising how differently they treat you': a qualitative analysis of trainee reflections on a new programme for generalist doctors. BMJ Open 2016;6:e011239 10.1136/bmjopen-2016-011239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Lundin RM, Bashir K, Bullock A, et al. "I’d been like freaking out the whole night": exploring emotion regulation based on junior doctors' narratives. Adv Health Sci Educ Theory Pract 2018;23:7–28. 10.1007/s10459-017-9769-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Monrouxe LV, Rees CE. "It’s just a clash of cultures": emotional talk within medical students' narratives of professionalism dilemmas. Adv Health Sci Educ Theory Pract 2012;17:671–701. 10.1007/s10459-011-9342-z [DOI] [PubMed] [Google Scholar]
- 33. Kehoe A, McLachlan J, Metcalf J, et al. Supporting international medical graduates' transition to their host-country: realist synthesis. Med Educ 2016;50:1015–32. 10.1111/medu.13071 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.