

Abstract
Atrial fibrillation (AF) is the most common arrhythmia worldwide and is associated with significant morbidity and mortality. A number of risk factors have been associated with AF, though few studies have explored the association between gastrointestinal and liver diseases and AF. Additionally, AF and treatment for AF may predispose to gastrointestinal and liver diseases. We review the current literature on the bidirectional associations between gastrointestinal and liver diseases and AF. We highlight the gaps in knowledge and areas requiring future investigation.
Keywords: atrial arrhythmia, tachycardia, anticoagulation, cirrhosis, microbiome
Key points
(1) Atrial fibrillation (AF) has multiple well-established risk factors but few studies have examined the association between gastrointestinal and liver diseases.
(2) Gastrointestinal and liver diseases may increase the risk of prevalent and incident AF through various mechanisms. Autonomic modulation and inflammation may be particularly relevant.
(3) AF outcomes and various treatments for AF can affect the gastrointestinal tract and liver, causing significant morbidity and mortality.
(4) Future research is needed to address the knowledge gaps in our understanding of how the gastrointestinal tract and liver influence AF and vice versa.
AF is the most prevalent arrhythmia worldwide, with an estimated 33.5 million individuals with AF globally in 2010. 1 The true prevalence of AF is likely much higher as many individuals are asymptomatic or undiagnosed. Although there are many well-established risk factors for AF including older age, alcohol, smoking, obesity, diabetes mellitus, hypertension, heart failure, ischemic heart disease, and valvular heart disease, there are still many unanswered questions regarding AF risk. 2 Prevention and treatment of cardiovascular risk factors and structural heart disease, may help to reduce morbidity and mortality from AF.
Gastrointestinal and liver diseases are common among patients with AF. 3 Diseases of the liver and gastrointestinal tract may contribute to AF risk through various mechanisms, including autonomic modulation and inflammation (Figure 1). Conversely, AF and treatment of AF with ablation, antiarrhythmic drugs, and anticoagulants can influence the development of gastrointestinal and liver complications and diseases. In our review, we present and evaluate the evidence supporting the association of various gastrointestinal diseases and AF and discuss possible mechanisms underlying these associations. We also review how AF and its treatment may lead to the development of gastrointestinal disease.
Figure 1.

The bidirectional relationship between atrial fibrillation and gastrointestinal and liver diseases.
Gastrointestinal conditions may directly relate to atrial fibrillation through a variety of proposed mechanisms or through multiple shared risk factors. Additionally, complications of atrial fibrillation and the treatment of atrial fibrillation may cause gastrointestinal diseases.
AF, atrial fibrillation; GI, gastrointestinal.
Search strategy
We searched the PubMed database through October 2018 with the following terms individually or in combination: ‘atrial fibrillation,’ ‘atrial flutter,’ ‘arrhythmias, cardiac’, ‘digestive system diseases,’ ‘gastrointestinal diseases,’ ‘proton pump inhibitors,’ ‘amiodarone,’ ‘anticoagulants,’ ‘warfarin,’ ‘inflammation,’ ‘radiofrequency ablation,’ and ‘cryoablation.’ All articles were reviewed along with the references from the relevant articles to identify related articles for inclusion in the review.
Pathophysiology and mechanisms of AF
Two dominant hypotheses of AF pathogenesis are that ectopic triggers upon a susceptible atrial substrate or rapidly firing drivers initiate high-frequency, re-entrant atrial circuits. Myocyte sleeves within the pulmonary veins are the most common source for ectopic firing, which is mediated by abnormal calcium handling and the autonomic nervous system. Adrenergic stimulation promotes triggered activity by enhancing automaticity and calcium-dependent afterdepolarizations. 4 Cholinergic activation accelerates myocyte repolarization and regional heterogeneity of atrial refractoriness enhancing focal, early afterdepolarization and promoting the maintenance of AF re-entrant circuits. 4 The cardiac autonomic ganglionated plexi, located near the pulmonary veins and the ligament of Marshall, facilitate electrophysiological modulation of the atrium and arrhythmogenesis. Autonomic activity may play an important role in linking AF with gastrointestinal disease (Figure 2).
Figure 2.
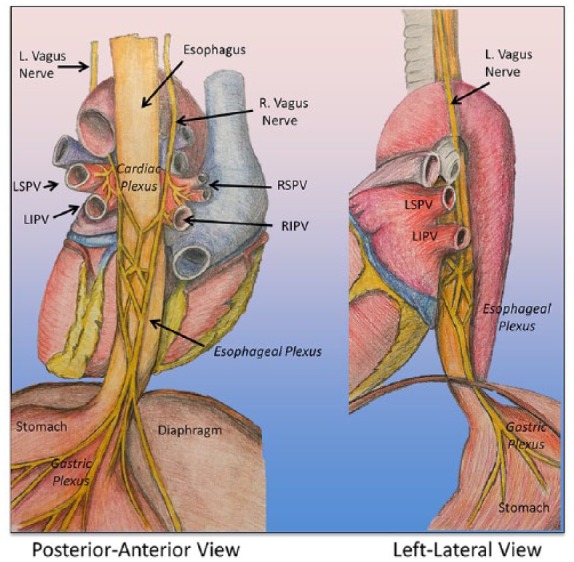
Anatomic relationship between the heart and the esophagus and stomach.
The juxtaposition of the esophagus to the left atrium and the parasympathetic innervation may be important factors that promote a bidirectional relationship of gastrointestinal diseases and AF.
L., left; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; R., right; RIPV, right inferior pulmonary vein; RSPV, right superior pulmonary vein.
The atrial substrate or underlying atrial cardiomyopathy are equally important to AF genesis. Alterations in cardiomyocytes, fibrotic changes, and interstitial infiltration of fat, inflammatory cells, or amyloid proteins, and other factors, have been well described to occur in patients with AF. 5 The histologic characteristics of the atrial substrate varies by AF risk factors and comorbidities. Atrial remodeling impairs cell coupling, slows conduction, and shortens atrial refractoriness promoting re-entry and the perpetuation of AF. Atrial inflammation may be of particular significance in the association of gastrointestinal and liver diseases and AF.
Gastrointestinal disease predisposing to AF
Inflammatory gastrointestinal conditions
Inflammation appears to play an important role in the pathogenesis of AF. Atrial biopsies in patients with drug-refractory AF show presence of inflammatory infiltrates, myocyte necrosis, and fibrosis, 6 and these changes may promote atrial structural remodeling and the development of the atrial substrate. Elevated C-reactive protein (CRP) has been associated with AF, and persistent AF is associated with higher mean CRP levels than observed with paroxysmal AF, 7 suggesting that an inflammatory state may promote the persistence of AF. Meta-analysis has shown a robust association of CRP and interleukin-6 and AF.8,9 In longitudinal studies, higher CRP confers a corresponding incremental AF risk.8,10–12 Finally, severe sepsis and the acute systemic inflammatory response has been associated with new-onset AF in the absence of cardiovascular comorbidities. 13
Inflammatory gastrointestinal diseases are characterized by systemic inflammation, and a few studies have explored a possible association with AF. Celiac disease is an autoimmune disorder characterized by inflammation and villous atrophy of the small intestine triggered by the ingestion of gluten in the diet of susceptible individuals. 14 Celiac disease is characterized by malabsorption, vitamin deficiencies, and increased systemic inflammation. 15 In two case-control studies, authors observed that individuals with untreated celiac disease had increased mean left atrial volume and P-wave dispersion, and prolonged atrial electromechanical delay, which may contribute to increased risk of AF.16,17 A large population-based study in Sweden suggested an association between celiac disease and prevalent and incident AF; 18 however, the association was inconsistent in other studies.19,20
Inflammatory bowel diseases (IBD), such as Crohn’s disease and ulcerative colitis, are autoimmune disorders marked by dysfunction of the intestinal immune response and inflammation in the gastrointestinal tract and multiple extra-intestinal sites. CRP correlates with IBD activity. 21 IBD, particularly IBD with active inflammation, may increase AF susceptibility by contributing to atrial structural remodeling. In one study, patients with IBD were observed to have altered atrial conduction, as measured by increased P-wave dispersion on electrocardiography, compared with referents. 22 Atrial electromechanical conduction as measured by transthoracic echocardiogram was prolonged in two small studies of IBD patients, compared with referents.23,24 A Danish nested case-control study with 24,499 IBD cases and 236,275 age- and sex-matched controls, observed a twofold increased risk of AF and a 1.5-fold increased risk of stroke during active IBD flares. 25 During periods of IBD remission, no association with AF or stroke was observed. 25
Gastroesophageal reflux disease
The prevalence of gastroesophageal reflux disease (GERD) has increased by approximately 50% since the1990s, owing largely to changes in diet and the growing obesity epidemic. 26 At the same time, the prevalence of AF has also been increasing. 1 The results from three large population-based studies on the association of GERD and AF are conflicting. A retrospective study from the database in the National Capitol Area military health system showed that GERD was associated with an 8% increased relative risk of AF adjusting for AF risk factors and cardiovascular disease. 27 In a Taiwan-based prospective study, participants with GERD had a higher incidence of AF compared with age-, sex-, and comorbidity-matched controls. 28 However, in a large US population-based study, esophagitis, but not GERD, was associated with AF, though the association with esophagitis and AF was no longer significant after accounting for confounding variables. 29 An important confounding factor to consider in studies of GERD and AF is healthcare utilization. Patients with GERD are more likely to be exposed to healthcare and, as a consequence, more likely to have AF detected, especially if they are asymptomatic.
The mechanism linking the association of GERD and AF is not well established but may involve vagally mediated, parasympathetic stimulation and inflammation as previously discussed in a comprehensive review. 30 In a small prospective case-control study, patients with AF and GERD who underwent catheter ablation were more likely to have triggered AF, independent pulmonary vein firing, and less left-atrial scar. 31 In addition, these patients were more likely to have a vagal response during AF ablation near parasympathetic ganglia as compared with those without GERD. 31 It is hypothesized that esophageal inflammation may activate afferent vagal neurons and contribute to AF through autonomic modulation of atrial refractoriness (Figure 2). Vagally induced atrial ischemia also has been suggested as a mechanism for AF in patients with GERD. 32
Gastrointestinal malignancy
Gastrointestinal malignancies, including colorectal and esophageal cancers, have been associated with an increased risk of AF in a few case-control studies.33–35 There are numerous mechanisms, which may explain the observed association of AF in patients with gastrointestinal cancers (Figure 3). 36 In one study, colorectal cancer patients had a twofold increased risk of AF compared with age-adjusted cohort participants without cancer; however, adjustment for other confounding variables was not performed. 35 A Danish population-based case-control study observed a higher prevalence of AF in patients with colorectal cancer [odds ratio (OR) of 11.8] but this increased prevalence was limited to the first 90 days after cancer diagnosis, suggesting that surgical treatment for the cancer may largely drive the association. 33
Figure 3.

Proposed mechanisms for the association between gastrointestinal cancer and atrial fibrillation.
AF, atrial fibrillation; GI, gastrointestinal.
Incident AF after surgical treatment of gastrointestinal cancer is high and is associated with poor surgical outcome, including pulmonary complications, sepsis, prolonged hospital stay, and mortality.37–39 Furthermore, in retrospective analyses, patients who develop AF after gastrointestinal cancer surgery are at increased risk for cardiovascular events within 1 year, 40 and death within 60 days. 41 After transthoracic esophagectomy, the rate of AF is reported to range from 10% to 46%37,38,42. Male sex, older age, history of cardiac and lung disease, and neoadjuvant chemotherapy are predictors of postesophagectomy AF.37,39,43,44 Prophylactic treatment with amiodarone has been shown to reduce AF in patients after transthoracic esophagectomy but not reduce hospital stay duration, morbidity or mortality. 45
Alcoholic liver disease
Multiple studies have demonstrated an association between high alcohol intake and AF.46–49 A meta-analysis showed that even moderate alcohol consumption is a risk factor for AF. 49 Individuals with alcohol-related liver disease who are heavy alcohol consumers are at risk for alcohol-related cardiomyopathy, which could predispose to heart failure and AF. In one study, patients with a history of recurrent alcohol-induced AF had an exaggerated sympathetic response to alcohol exposure compared with healthy controls. 50 In a community-based sample, the size of the left atrium increased by 0.16 mm per 10 g increase in daily alcohol consumption and adjustment for left atrial dimension attenuated the association between alcohol use and incident AF, indicating that left atrial enlargement may be an important mediator on the causal pathway between alcohol and AF. 51
Nonalcoholic fatty liver disease
Nonalcoholic fatty liver disease (NAFLD) is a common chronic liver disease that many consider the hepatic manifestation of metabolic syndrome. 52 NAFLD describes a heterogeneous condition over a spectrum of liver pathology, from simple steatosis to cirrhosis. Additional subphenotypes of NAFLD exist, including those at increased genetic risk for NAFLD and those with NAFLD but without obesity. Population studies evaluating the association between NAFLD and AF have been inconsistent.53–57 A meta-analysis of five cohort studies of over 200,000 participants concluded that patients with NAFLD had a twofold risk of AF compared with patients without NAFLD [pooled risk ratio 2.06, 95% confidence interval (CI) 1.1–3.85]. 58 However, there was significant heterogeneity in the studies and the wide confidence interval suggests uncertainty around the point estimate. 58 A subsequent study in the Framingham Heart Study cohort reported no significant association between NAFLD and prevalent or incident AF after 12 years of follow up. 59
Whereas NAFLD and AF share common risk factors, including obesity, hypertension, hypertriglyceridemia, insulin resistance and diabetes, in adjusted analyses, NAFLD has been associated with diastolic dysfunction, and left ventricular chamber remodeling, which may predispose to AF.60–62 There are several proposed mechanisms that may more directly link NAFLD and AF. First, NAFLD may trigger AF by increasing systemic inflammation, an effect that is associated with liver fat in analyses adjusting for obesity and metabolic syndrome.63,64 Second, NAFLD has been associated with autonomic dysfunction as assessed with electrochemical skin conductance test and heart rate variability test.65,66 Whereas the mechanism linking NAFLD with autonomic dysfunction is not well described, alterations in the autonomic nervous system may promote initiation and maintenance of AF. 67 In one study, patients with NAFLD had delayed atrial conduction with longer atrial electromechanical delay and higher P-wave dispersion compared with referents without NAFLD. 68 Third, NAFLD has been associated with an increased risk of diastolic dysfunction60–62 and ischemic heart disease, 69 adjusting for traditional risk factors and metabolic syndrome. Both diastolic dysfunction and ischemia predispose to AF. Finally, sleep apnea, which is characterized by intermittent hypoxia, is frequently observed in patients with NAFLD 70 and may increase atrial arrhythmogenicity. 71 Alternatively, the association between NAFLD and AF may be a result of shared risk factors. Specifically, many individuals with NAFLD have a higher ectopic fat burden, including more pericardial fat, which is associated with AF. 72 Pericardial fat was significantly associated with atrial conduction even after accounting for visceral and intrathoracic fat. 73 Additional studies are needed to determine if any associations between NAFLD and AF remain after accounting for pericardial fat.
Microbiome
The gastrointestinal tract comprises approximately 100 trillion bacterial cells and approximately 9 million bacterial genes, which far exceed the number of human cells or genes in the body.74,75 Recent evidence suggests the gut microbiome may have an important impact on cardiovascular disease, including atherosclerosis and hypertension.76–79 The microbiome may also influence fat partitioning in the liver, promoting NAFLD, 80 and indirectly contributing to cardiac dysfunction. Whether altered gut microbiota increase AF susceptibility by promoting atrial remodeling or alterations in the autonomic nervous system remains unknown (Figure 4).
Figure 4.

Proposed mechanisms for the interaction between the gut microbiome and atrial fibrillation.
Gut microbes convert dietary choline and L-carnitine, from red meat and eggs, to trimethylamine, which is oxidized to trimethylamine N-oxide in the liver. Trimethylamine N-oxide is associated with atherosclerosis, cardiovascular events, and an increased susceptibility to atrial fibrillation. Trimethylamine N-oxide may initiate atrial electrical remodeling, autonomic remodeling, and an upregulation of pro-inflammatory signaling pathways that may initiate atrial fibrillation. Lipopolysaccharides, which are derived from the outer membrane of Gram-negative bacteria, may enter the circulation through the gut mucosa and contribute to atrial fibrillation risk by increasing inflammatory cytokines and by altering the structural and electrical remodeling of the left atrium. The Mediterranean diet may favorably alter the gut microbiome and lower markers of oxidative stress and lipopolysaccharide levels, which may decrease atrial fibrillation risk.
LPS, lipopolysaccharides; TMA, trimethylamine; TMAO, trimethylamine N-oxide.
Gut-derived metabolites, including short-chain fatty acids, lipopolysaccharides, and trimethylamine N-oxide (TMAO) recently have been shown to play a role in the pathogenesis of cardiovascular remodeling. Gut microbes convert dietary choline and L-carnitine, from red meat and eggs, to trimethylamine, which is oxidized to TMAO in the liver. 79 TMAO is associated with atherosclerosis and cardiovascular events, possibly by increasing the production of pro-inflammatory cytokines.81,82 Experimental models have shown that TMAO may increase AF susceptibility. When TMAO is injected into the epicardial ganglionated plexi of dogs, atrial electrical remodeling, autonomic remodeling, and upregulation of pro-inflammatory signaling pathways were observed. 83 Whether circulating TMAO promotes AF via ganglionated plexi is not yet established.
Lipopolysaccharides, which are derived from the outer membrane of Gram-negative bacteria, may enter the circulation through the gut mucosa and contribute to atherosclerosis, possibly through worsening chronic inflammation. 84 A recent study reported higher circulating lipopolysaccharides levels in patients with AF compared with those in sinus rhythm. 85 AF patients with high lipopolysaccharides also had increased risk of major adverse cardiovascular events compared with those with low lipopolysaccharides levels. 85 More studies are needed to explore the relationships between lipopolysaccharides and AF.
Diet is a major influencer on the composition of an individual’s microbiome and dietary changes can rapidly shift the dominant microbial communities in the gut.86,87 A post hoc analysis of a randomized trial, PREDIMED (Prevencion con Dieta Mediterranea), reported that a Mediterranean diet conferred a lower risk for AF. 88 High adherence to the Mediterranean diet is associated with a favorable microbial profile, including lower Escherichia coli counts, higher proportions of bifidobacteria species 89 and low serum lipopolysaccharide. 85 AF patients who adhered to the Mediterranean diet had lower markers of oxidative stress and a lower risk of cardiovascular events compared with those not adhering to the diet. 90 It is unknown if lowering lipopolysaccharide levels, through altering the gut microbiota, decreases risk of AF or its complications.
Gastrointestinal tract infections
Gastrointestinal tract infections may contribute to the development of AF through the inflammatory cascade. Helicobacter pylori is a Gram-negative bacterium that is frequently detected in the gastric antrum and is the main pathogen contributing to gastric ulceration, gastritis, and gastric cancer. Several cross-sectional studies have observed higher rates of H. pylori infection among those with chronic AF.91,92 However, a meta-analysis of six studies observed no association between H. pylori infection and AF, though they did report significant publication bias. 93
Treatment of gastrointestinal and liver disease promoting AF
Proton-pump inhibitors (PPIs) have been associated both with the protection against and the induction of AF. PPIs have antioxidant properties through protection of glutathione stores and anti-inflammatory properties via inhibition of pro-inflammatory cytokines. 94 A few case series and small studies have reported that treatment with PPIs reduced AF symptoms95,96 but a larger population study has failed to demonstrate an effect of PPIs on AF. 28 The Taiwan National Health study showed that treatment with PPIs was associated with a higher risk of AF. 28 However, this finding may be due to a treatment bias. Others have postulated that hypomagnesemia, which has been correlated to higher rates of AF, may result from increased PPI exposure in the general population. 97
Gastrointestinal disease may alter efficacy of AF treatments
Malabsorption
Gastrointestinal malabsorption may result from underlying inflammatory and autoimmune conditions, such as IBD and celiac disease, intestinal infections, such as giardiasis, or from prior small or large intestine surgical resections. If large portions of the small intestine are resected, a patient may develop short bowel syndrome, which is characterized by reduced absorption of nutrients and fluid, diarrhea, vitamin deficiencies, and weight loss. The possibility of malabsorption of medications should be considered in patients with AF and gastrointestinal malabsorption. Oral antiarrhythmic medications, such as digoxin, and direct-acting oral anticoagulants (DOACs), such as dabigatran, are absorbed from the duodenum and proximal jejunum.98,99 Roux-en-Y gastric bypass surgery involves the creation of a small gastric pouch that connects directly to the distal jejunum, bypassing the distal stomach, duodenum, and proximal jejunum, altering the intestinal length and transient time. The changes noted in CYP3A4 expression following gastric bypass or surgical restriction may also impact bioavailability of various DOACs. 99 Dabigatran failure has been reported in patients with a history of Roux-en-Y gastric bypass or short-bowel syndrome. 99 The efficacy of DOACs in patients with a history of major gastrointestinal surgery, particularly to the stomach or small intestine, has been investigated in small, case-controlled and case series only. An investigation of 18 patients undergoing bariatric surgery compared with matched controls showed no difference in serum concentrations postoperatively for those receiving apixaban or dabigatran, but significantly lower levels for those receiving rivaroxaban. 100 However, a study of single-dose rivaroxaban showed no difference in pharmacokinetic parameters in 12 patients undergoing bariatric surgery. 101 Apixaban appears to be least affected by postoperative changes to the gastrointestinal tract due to high rate of absorption occurring in the small bowel and ascending colon and should be the preferred DOAC in patients undergoing bariatric surgery.99,100 In patients undergoing more extensive gastrointestinal-tract resections, DOACs should be avoided until well-conducted studies are available.
Summary of gastrointestinal and liver diseases and AF
There are multiple limitations to the current research investigating the association between various gastrointestinal conditions and their treatments with AF. First, the majority of studies are small and cross-sectional in design, which inhibits our ability to determine causality because of uncertain temporality, and the potential for residual confounding. Gastrointestinal diseases and AF share common risk factors (Figure 1) and most studies incompletely account for overlapping risk factors. Residual confounding and positive publication biases may contribute to many of the positive associations reported in the literature. There is a paucity of well-designed prospective studies evaluating gastrointestinal or liver diseases as risk factors for AF. Finally, it is unknown if treatment of gastrointestinal or liver disease reduces AF incidence or recurrence.
AF predisposing to gastrointestinal disease
Mesenteric ischemia
In patients with AF, ischemia is predominantly secondary to cardioembolic events rather than from in situ thromboembolism. 102 Major risk factors for cardioembolic events in patients with AF include history of prior stroke or transient ischemic attack, age greater than 75 years, hypertension, and structural heart disease. 103 In particular, women with AF are at increased risk for thromboembolic events, including mesenteric ischemia 104 (Table 1). Emboli to the visceral–mesenteric vasculature are the second most common site of peripheral thromboembolic disease after the vessels in the upper and lower extremities. 105 In a Taiwan-based study of patients with AF, the risk of developing mesenteric ischemia was higher with increasing CHA2DS2-VASc score 106 and those with a score ⩾ 2 had a threefold increase in risk compared with those having a score of 0. 107
Table 1.
Gastrointestinal complications of atrial fibrillation or treatment of atrial fibrillation.
| Condition | Incidence/prevalence | Severity | Presentation | Diagnosis | Treatment |
|---|---|---|---|---|---|
| Mesenteric ischemia | Incident rate 0.74 events/1000 person-years 104 | Ranges from mild/self-limited to catastrophic108–110 | Early: minimal and nonspecific abdominal pain
110
Late: severe abdominal pain, shock |
High clinical suspicion; contrast-enhanced CT showing bowel wall thickening, loss of bowel wall enhancement, pneumatosis, or portal venous gas108,109 | Angiography with catheter-directed therapy, mechanical thrombectomy, or laparotomy111–114 |
| Solid organ ischemia | Unknown, likely underdiagnosed | Usually not severe, as the involved organs have a well-developed collateral circulation and efficient compensatory mechanisms 115 | May involve the liver, spleen, or gallbladder; often occurs along with mesenteric ischemia1108 | Often asymptomatic and diagnosed incidentally on imaging115,116 | Supportive care |
| Esophageal ulceration | Prevalence postablation: 5–15%; 117 wide variation between studies and ablation technique | Ranges from mild to severe | Often asymptomatic or may have chest discomfort, nausea or fever post-AF ablation 118 | Direct visualization via EGD after ruling out AE fistula | Prevention: monitor the relationship of the esophagus to the ablation site using dynamic intra-ablation imaging119,140 and utilize esophageal temperature probes;
120
titrate energy delivered to high-risk locations during the procedure; use cryoablation
121
Treatment: proton-pump inhibitor therapy before and after ablation 122 |
| AE fistula | Incidence after catheter AF ablation: 0.01% and 0.2%123,124 Incidence after surgical AF ablation: 1.5% 125 | Frequently fatal; mortality rate 70–80%126,127 | Late complication of AF ablation usually presenting in the first 2–3 weeks postablation 128 Symptoms are often nonspecific, such as fever, generalized malaise, leukocytosis, recurrent neurologic events from septic or air embolization127,129 | High clinical suspicion; contrast-enhanced CT or MRI showing communication between the left atrium and esophagus 130 EGD is contraindicated, given risk of fatal air embolization 131 |
Emergent surgery with either direct or transthoracic extracardiac repair with or without cardiopulmonary bypass
126
Consider esophageal stenting in select cases132,133 Systemic antibiotic therapy |
| Esophageal–pericardial fistula | Rare | Severe | Severe chest or epigastric pain and fever | Evidence of pericardial effusion or pericarditis on electrocardiogram, CT scan or echocardiography | Conservative management with esophageal stenting, pericardial drainage, and systemic antibiotics 134 |
| Gastroparesis | Incidence after catheter AF ablation: 1.1–6.7%140,141 | Usually self-limited | Nausea, vomiting, epigastric fullness, discomfort, or bloating 137 | Monitor for symptoms during and postprocedure Gastric-emptying scan |
Conservative management; most recover spontaneously within 6 months 135 |
AE, atrio-esophageal; AF, atrial fibrillation; CT, computed tomography; EGD, esophagogastroduodenoscopy; MRI, magnetic resonance imaging.
AF treatments predisposing to gastrointestinal disease
Catheter ablation for AF and gastrointestinal complications
Several gastrointestinal complications may result from catheter-directed AF ablation, ranging from gastroparesis to severe esophageal injury or atrio-esophageal fistula (Table 1). Gastroparesis, defined by delayed gastric emptying in the absence of mechanical obstruction, may result from collateral injury to the vagus nerve, which innervates the pylorus and gastric antrum and is important for gastric emptying, 138 during pulmonary vein isolation procedures. There are several mechanisms which have been implicated as the cause for esophageal injury. First, the close proximity of the esophagus to the thermal energy source if ablation is performed along the posterior wall of the left atrium confers risk for thermal injury (Figure 2). 139 Whereas, there is considerable variation between individuals, the esophagus often traverses the left-side of the posterior wall of the left atrium 140 with a separation distance of less than 5 mm of tissue. 141 Individual variation in the size and thickness of the left atrium, and the presence of epicardial fat between the left atrium and esophagus also impact the degree of esophageal thermal injury.140,141 Procedure-related factors, including the use of general anesthesia, 142 the magnitude and duration of local tissue heating, 140 and the orientation, size or type of the ablation catheter used may also contribute to esophageal injury. The odds of esophageal injury is reported to increase by 1.4 for every 1°C increase in temperature. 143 The second possible mechanism for esophageal ulceration with AF ablation involves injury to the vagal anterior esophageal plexus, with subsequent impaired contraction of the lower esophageal sphincter predisposing to gastric reflux and esophagitis. Finally, thermal injury of the arterial supply to the esophagus may induce ischemia, impact healing, and promote ulcer formation.
Anticoagulation and liver injury
Patients with AF on treatment with warfarin or DOACs are at risk for liver injury, though the risk is relatively small. DOACs, with the exception of dabigatran, undergo hepatic metabolism through either glucuronidation or the cytochrome P450 system. An early direct thrombin inhibitor, ximelagatran, was withdrawn from the market after safety concerns regarding hepatotoxicity emerged. 144 A study from a large US-based healthcare database identified 960 hospitalizations for liver injury over 14 months of follow up (7.3 events per 1000 person-years) among patients with nonvalvular AF treated with DOACs. 145 The risk of liver injury was lowest for patients treated with dabigatran and highest for those treated with warfarin, whereas rivaroxaban and apixaban users had intermediate risk. 145 Risk factors for liver-injury hospitalization included underlying hepatobiliary disease, history of alcohol-use disorder, cancer, anemia, kidney disease, and heart failure. 145 In a large Canadian administrative database, DOACs were not associated with an increased risk of severe liver injury compared with warfarin. 146 Though liver injury is a relatively rare complication, clinicians and patients should consider risk factors for liver injury when choosing a specific oral anticoagulant.
Patients with chronic liver disease often have abnormalities in coagulation and a prolonged international normalization ratio; however, they are not protected against stroke and systemic thromboembolism associated with AF. 147 On average, patients with hepatic impairment who receive warfarin have a lower proportion of time spent within the therapeutic range and are at increased risk for bleeding events compared with those without liver disease. 148 A recent study based on the Taiwan National Health Insurance Database showed that those with cirrhosis treated with warfarin had a lower risk of ischemic stroke [hazard ratio (HR) 0.76, 95% CI 0.58–0.99] and no increased risk of intracranial bleeding compared with nonwarfarin users. 149 A limited number of studies have evaluated the safety of DOACs in patients with hepatic impairment. 150 In a retrospective cohort study of patients with chronic liver disease and AF, rates of all-cause bleeding were similar between the groups treated with DOACs and warfarin. 151 However, in a prospective, multicenter cohort study, warfarin, but not DOACs, was associated with an increased risk for major bleeding among those with liver fibrosis; though the sample size was small. 152 In patients with moderate hepatic impairment, as defined by the Child–Pugh category, DOACs should be used with caution and use should be limited to dabigatran and apixaban because these agents show similar bioavailability compared with controls, and no dose adjustments are needed. 153 DOACs should be avoided in patients with severe hepatic dysfunction, defined as Child–Pugh C cirrhosis, because of bleeding concerns. 154
Prior studies evaluating the management of esophageal varices in patients who are receiving anticoagulation for AF are limited. The American Society of Gastrointestinal Endoscopy considers esophageal band ligation as a high-bleeding-risk procedure. 155 The risks of stopping anticoagulation, with or without bridging therapy, in the setting of high-bleeding-risk procedures needs to be considered for the individual patient; there is no universal agreement across various practice guidelines.155,156 Additional studies are needed to determine the utility of alternative treatment approaches, such as the use of nonselective beta blockage, and the optimal use and timing of anticoagulation in patients with cirrhosis and varices.
Amiodarone and liver injury
Amiodarone is an antiarrhythmic drug used in the treatment of ventricular and atrial arrhythmias, including AF, which is associated with asymptomatic elevations in liver biochemical tests in up to 30% of patients after intravenous administration, or among those who use amiodarone long term. 157 Symptomatic hepatitis or liver failure and cirrhosis from amiodarone is fortunately very rare (0–3% of amiodarone users), but the risk is higher for prolonged users and with high doses. 163 In a meta-analysis of approximately 740 patients on low-dose amiodarone for at least 1 year, there were no statistically significant increases in gastrointestinal or liver-related adverse events compared with placebo. 159 Amiodarone-induced liver injury includes steatosis and steatohepatitis and can be difficult to distinguish from NAFLD. 160 Because amiodarone concentrates in the liver and has a relatively long half-life, amiodarone-induced liver injury can take time to resolve and may even become apparent after amiodarone has been discontinued. 160
Anticoagulation and gastrointestinal bleeding
Gastrointestinal bleeding is one of the most frequent complications of anticoagulation therapy for AF. Patients with AF on anticoagulation who experience major gastrointestinal bleeding may have an underlying gastrointestinal malignancy, which was observed in 8.1% of bleeding events in one large study. 161 Over multiple observational studies, the major bleeding rate for apixaban has ranged from 2.29% to 2.38% per 100 patient-years. 162 Whereas the rates of major bleeding are more variable in the published literature for dabigatran and rivaroxaban, overall, DOACs have similar or lower rates of major bleeding compared with warfarin.162,163 Of the DOACs, rivaroxaban has the highest major bleeding rate (up to 6% per 100 patient-years), 162 which has been confirmed in multiple studies. 145 In a systematic review of 28 studies, apixaban was the only DOAC to have lower rates of gastrointestinal hemorrhage compared with warfarin (HR 0.63, 95% CI 0.42–0.95). 164 However, in a larger meta-analysis of 43 studies, there was no difference in major gastrointestinal bleeding with apixaban compared with warfarin. 165 In this study, dabigatran had a slightly, but significantly, increased risk of major gastrointestinal bleeding compared with warfarin (OR 1.27, 95% CI 1.04–1.55) and rivaroxaban had the highest risk (OR 1.40, 95% CI 1.15–1.7). 165 Edoxaban was only evaluated in one of these trials, showing no difference in major gastrointestinal bleeding compared with warfarin (OR 0.93, 95% CI 0.78–1.11). 165 Though trials directly comparing the DOACs are not available, the existing ‘real world’ data and multiple meta-analyses on gastrointestinal bleeding suggest that apixaban may have fewer major bleeding complications compared with dabigatran and rivaroxaban, and may be the optimal treatment for patients with an underlying history of gastrointestinal hemorrhage, or those at increased risk of bleeding.145,164,165
Future directions
In summary, compared with our understanding of cardiometabolic risk factors for AF, substantial knowledge gaps exist in our understanding of the interrelations between gastrointestinal and liver diseases, and AF. Although the pathophysiology of AF has been extensively studied, the mechanisms that may predispose patients with gastrointestinal and liver diseases to AF are poorly understood. Adequately powered longitudinal studies evaluating the associations between gastrointestinal and liver diseases, and AF are needed. These studies should be adjusted for shared cardiac and gastrointestinal disease risk factors, which may confound the relations. Whereas gastrointestinal and liver diseases are not likely to be a major contributors to AF risk, understanding the mechanisms underlying any associations may further our understanding of AF and lead to novel preventative and treatment strategies.
Our current understanding of the microbiome and how gut organisms contribute to health and disease is in its infancy. Preclinical data show promising connections between the microbiome and AF. Large cohorts of participants well phenotyped for cardiometabolic diseases, including prevalent and incident AF, with a detailed assessment of the microbiome and large-scale serum metabolomic data, are lacking. Such cohorts may help us elucidate the metabolic by-products of microbiota so that we may understand how the microbiome impacts systemic inflammation and disease states.
Complications associated with both AF and its treatment contributing to gastrointestinal and liver diseases are rare, but often give rise to significant morbidity and mortality. AF-associated cardioembolic disease, which often leads to gastrointestinal complications, can be minimized with anticoagulation. However, AF is underdiagnosed 166 and patients are often undertreated. 167 Additional resources aimed at identifying patients with AF and ensuring AF patients have access to treatments, including DOACs, are needed in order to prevent gastrointestinal complications of AF.
Whereas the recognition and understanding of gastrointestinal complications of AF ablation is improving, additional studies are needed to study the safety, efficacy, and feasibility of various prevention strategies. This is of particularly importance as the number of AF ablation procedures continues to grow.
Conclusion
A bidirectional relationship between gastrointestinal and liver diseases, and AF, exists. An enhanced understanding of the pathophysiology and mechanisms by which gastrointestinal diseases may contribute to AF may lead to novel preventative and treatment strategies. Finally, the development of new and improved treatments for AF should focus on minimizing gastrointestinal and liver complications.
Acknowledgments
Emelia Benjamin and Robert Helm contributed equally to this work.
Footnotes
Funding: Dr Long is supported in part by the National Institute of Diabetes and Digestive and Kidney Diseases, K23 DK113252, and the Boston University School of Medicine Department of Medicine Career Investment Award.
Conflict of interest statement: The authors declare that there is no conflict of interest.
Contributor Information
Michelle T. Long, Section of Gastroenterology, Boston University School of Medicine, 85 East Concord Street 7th Floor, Boston MA 02118, USA.
Darae Ko, Evans Department of Medicine, Boston University School of Medicine, Boston, MA, USA.
Lindsay M. Arnold, Department of Pharmacy, Boston Medical Center, Boston, MA, USA
Ludovic Trinquart, Department of Biostatistics, Boston University School of Public Health, Boston, MA, USA.
Jason A. Sherer, Evans Department of Medicine, Boston University School of Medicine, Boston, MA, USA
Sunny-Skye Keppel, Evans Department of Medicine, Boston University School of Medicine, Boston, MA, USA.
Emelia J. Benjamin, Evans Department of Medicine, Boston University School of Medicine, Boston, MA, USA Department of Epidemiology, Boston University School of Public Health, Boston, MA, USA The Framingham Heart Study, Framingham, MA, USA
Robert H. Helm, Evans Department of Medicine, Boston University School of Medicine, Boston, MA, USA
References
- 1. Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 study. Circulation 2014; 129: 837–847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Schnabel RB, Yin X, Gona P, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet 2015; 386; 154–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Laliberte F, Moore Y, Dea K, et al. Gastrointestinal comorbidities associated with atrial fibrillation. Springer Plus 2014; 3: 603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Chen PS, Chen LS, Fishbein MC, et al. Role of the autonomic nervous system in atrial fibrillation: pathophysiology and therapy. Circ Res 2014; 114: 1500–1515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Goette A, Kalman JM, Aguinaga L, et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: definition, characterization, and clinical implication. Heart Rhythm 2017; 14, e3–e40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Frustaci A, Chimenti C, Bellocci F, et al. Histological substrate of atrial biopsies in patients with lone atrial fibrillation. Circulation 1997; 96: 1180–1184. [DOI] [PubMed] [Google Scholar]
- 7. Chung MK, Martin DO, Sprecher D, et al. C-reactive protein elevation in patients with atrial arrhythmias: inflammatory mechanisms and persistence of atrial fibrillation. Circulation 2001; 104: 2886–2891. [DOI] [PubMed] [Google Scholar]
- 8. Alla VM, Thambidorai S, Anand K, et al. C-reactive protein and the risk of atrial fibrillation: a systematic review and meta-analysis. J Atr Fibrillation 2010; 2: 225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Wu N, Xu B, Xiang Y, et al. Association of inflammatory factors with occurrence and recurrence of atrial fibrillation: a meta-analysis. Int J Cardiol 2013; 169: 62–72. [DOI] [PubMed] [Google Scholar]
- 10. Aviles RJ, Martin DO, Apperson-Hansen C, et al. Inflammation as a risk factor for atrial fibrillation. Circulation 2003; 108: 3006–3010. [DOI] [PubMed] [Google Scholar]
- 11. Guo Y, Lip GY, Apostolakis S. Inflammation in atrial fibrillation. J Am Coll Cardiol 2012; 60: 2263–2270. [DOI] [PubMed] [Google Scholar]
- 12. Sinner MF, Stepas KA, Moser CB, et al. B-type natriuretic peptide and C-reactive protein in the prediction of atrial fibrillation risk: the CHARGE-AF Consortium of community-based cohort studies. Europace 2014; 16: 1426–1433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Walkey AJ, Greiner MA, Heckbert SR, et al. Atrial fibrillation among Medicare beneficiaries hospitalized with sepsis: incidence and risk factors. Am Heart J 2013; 165: 949–955.e943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Husby S, Murray JA. Diagnosing coeliac disease and the potential for serological markers. Nat Rev Gastroenterol Hepatol 2014; 11: 655–663. [DOI] [PubMed] [Google Scholar]
- 15. Korkmaz H, Sozen M, Kebapcilar L. Increased arterial stiffness and its relationship with inflammation, insulin, and insulin resistance in celiac disease. Eur J Gastroenterol Hepatol 2015; 27: 1193–1199. [DOI] [PubMed] [Google Scholar]
- 16. Bayar N, Çekin AH, Arslan Ş, et al. Assessment of left atrial function in patients with celiac disease. Echocardiography 2015; 32: 1802–1808. [DOI] [PubMed] [Google Scholar]
- 17. Efe TH, Ertem AG, Coskun Y, et al. Atrial electromechanical properties in coeliac disease. Heart Lung Circ 2016; 25: 160–165. [DOI] [PubMed] [Google Scholar]
- 18. Emilsson L, Smith JG, West J, et al. Increased risk of atrial fibrillation in patients with coeliac disease: a nationwide cohort study. Eur Heart J 2011; 32: 2430–2437. [DOI] [PubMed] [Google Scholar]
- 19. Lebwohl B, Emilsson L, Fröbert O, et al. Mucosal healing and the risk of ischemic heart disease or atrial fibrillation in patients with celiac disease; a population-based study. PLoS One 2015; 10: e0117529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. West J, Logan RF, Card TR, et al. Risk of vascular disease in adults with diagnosed coeliac disease: a population-based study. Aliment Pharmacol Ther 2004; 20: 73–79. [DOI] [PubMed] [Google Scholar]
- 21. Mosli MH, Zou G, Garg SK, et al. C-reactive protein, fecal calprotectin, and stool lactoferrin for detection of endoscopic activity in symptomatic inflammatory bowel disease patients: a systematic review and meta-analysis. Am J Gastroenterol 2015; 110: 802–819. Quiz 820. [DOI] [PubMed] [Google Scholar]
- 22. Dogan Y, Soylu A, Eren GA, et al. Evaluation of QT and P wave dispersion and mean platelet volume among inflammatory bowel disease patients. Int J Med Sci 2011; 8: 540–546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Efe TH, Cimen T, Ertem AG, et al. Atrial electromechanical properties in inflammatory bowel disease. Echocardiography 2016; 33: 1309–1316. [DOI] [PubMed] [Google Scholar]
- 24. Nar G, Ergul B, Aksan G, et al. Assessment of atrial electromechanical delay and left atrial mechanical functions in patients with ulcerative colitis. Echocardiography 2016; 33: 970–976. [DOI] [PubMed] [Google Scholar]
- 25. Kristensen SL, Lindhardsen J, Ahlehoff O, et al. Increased risk of atrial fibrillation and stroke during active stages of inflammatory bowel disease: a nationwide study. Europace 2014; 16: 477–484. [DOI] [PubMed] [Google Scholar]
- 26. El-Serag HB, Sweet S, Winchester CC, et al. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 2014; 63: 871–880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Kunz JS, Hemann B, Edwin Atwood J, et al. Is there a link between gastroesophageal reflux disease and atrial fibrillation? Clin Cardiol 2009; 32: 584–587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Huang CC, Chan WL, Luo JC, et al. Gastroesophageal reflux disease and atrial fibrillation: a nationwide population-based study. PLoS One 2012; 7: e47575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Bunch TJ, Packer DL, Jahangir A, et al. Long-term risk of atrial fibrillation with symptomatic gastroesophageal reflux disease and esophagitis. Am J Cardiol 2008; 102: 1207–1211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Roman C, Bruley des Varannes S, Muresan L, et al. Atrial fibrillation in patients with gastroesophageal reflux disease: a comprehensive review. World J Gastroenterol 2014; 20: 9592–9599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Reddy YM, Singh D, Nagarajan D, et al. Atrial fibrillation ablation in patients with gastroesophageal reflux disease or irritable bowel syndrome-the heart to gut connection! J Interv Card Electrophysiol 2013; 37: 259–265. [DOI] [PubMed] [Google Scholar]
- 32. Chauhan A, Mullins PA, Taylor G, et al. Cardioesophageal reflex: a mechanism for “linked angina” in patients with angiographically proven coronary artery disease. J Am Coll Cardiol 1996; 27: 1621–1628. [DOI] [PubMed] [Google Scholar]
- 33. Erichsen R, Christiansen CF, Mehnert F, et al. Colorectal cancer and risk of atrial fibrillation and flutter: a population-based case-control study. Intern Emerg Med 2012; 7: 431–438. [DOI] [PubMed] [Google Scholar]
- 34. Guzzetti S, Costantino G, Sada S, et al. Colorectal cancer and atrial fibrillation: a case-control study. Am J Med 2002; 112: 587–588. [DOI] [PubMed] [Google Scholar]
- 35. Guzzetti S, Costantino G, Vernocchi A, et al. First diagnosis of colorectal or breast cancer and prevalence of atrial fibrillation. Intern Emerg Med 2008; 3: 227–231. [DOI] [PubMed] [Google Scholar]
- 36. Farmakis D, Parissis J, Filippatos G. Insights into onco-cardiology: atrial fibrillation in cancer. J Am Coll Cardiol 2014; 63: 945–953. [DOI] [PubMed] [Google Scholar]
- 37. Lohani KR, Nandipati KC, Rollins SE, et al. Transthoracic approach is associated with increased incidence of atrial fibrillation after esophageal resection. Surg Endosc 2015; 29: 2039–2045. [DOI] [PubMed] [Google Scholar]
- 38. Murthy SC, Law S, Whooley BP, et al. Atrial fibrillation after esophagectomy is a marker for postoperative morbidity and mortality. J Thorac Cardiovasc Surg 2003; 126: 1162–1167. [DOI] [PubMed] [Google Scholar]
- 39. Rao VP, Addae-Boateng E, Barua A, et al. Age and neo-adjuvant chemotherapy increase the risk of atrial fibrillation following oesophagectomy. Eur J Cardiothorac Surg 2012; 42: 438–443. [DOI] [PubMed] [Google Scholar]
- 40. Nassoiy SP, Blackwell RH, Kothari AN, et al. New onset postoperative atrial fibrillation predicts long-term cardiovascular events after gastrectomy. Am J Surg 2016; 211: 559–564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Stawicki SP, Prosciak MP, Gerlach AT, et al. Atrial fibrillation after esophagectomy: an indicator of postoperative morbidity. Gen Thorac Cardiovasc Surg 2011; 59: 399–405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Ojima T, Iwahashi M, Nakamori M, et al. Atrial fibrillation after esophageal cancer surgery: an analysis of 207 consecutive patients. Surg Today 2014; 44: 839–847. [DOI] [PubMed] [Google Scholar]
- 43. Passman RS, Gingold DS, Amar D, et al. Prediction rule for atrial fibrillation after major noncardiac thoracic surgery. Ann Thorac Surg 2005; 79: 1698–1703. [DOI] [PubMed] [Google Scholar]
- 44. Ma JY, Wang Y, Zhao YF, et al. Atrial fibrillation after surgery for esophageal carcinoma: clinical and prognostic significance. World J Gastroenterol 2006; 12: 449–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Tisdale JE, Wroblewski HA, Wall DS, et al. A randomized, controlled study of amiodarone for prevention of atrial fibrillation after transthoracic esophagectomy. J Thorac Cardiovasc Surg 2010; 140: 45–51. [DOI] [PubMed] [Google Scholar]
- 46. Djousse L, Levy D, Benjamin EJ, et al. Long-term alcohol consumption and the risk of atrial fibrillation in the Framingham Study. Am J Cardiol 2004; 93: 710–713. [DOI] [PubMed] [Google Scholar]
- 47. Frost L, Vestergaard P. Alcohol and risk of atrial fibrillation or flutter: a cohort study. Arch Intern Med 2004; 164: 1993–1998. [DOI] [PubMed] [Google Scholar]
- 48. Kodama S, Saito K, Tanaka S, et al. Alcohol consumption and risk of atrial fibrillation: a meta-analysis. J Am Coll Cardiol 2011; 57: 427–436. [DOI] [PubMed] [Google Scholar]
- 49. Larsson SC, Drca N, Wolk A. Alcohol consumption and risk of atrial fibrillation: a prospective study and dose-response meta-analysis. J Am Coll Cardiol 2014; 64: 281–289. [DOI] [PubMed] [Google Scholar]
- 50. Maki T, Toivonen L, Koskinen P, et al. Effect of ethanol drinking, hangover, and exercise on adrenergic activity and heart rate variability in patients with a history of alcohol-induced atrial fibrillation. Am J Cardiol 1998; 82: 317–322. [DOI] [PubMed] [Google Scholar]
- 51. McManus DD, Yin X, Gladstone R, et al. Alcohol consumption, left atrial diameter, and atrial fibrillation. J Am Heart Assoc 2016; 5. pii: e004060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Younossi ZM, Stepanova M, Afendy M, et al. Changes in the prevalence of the most common causes of chronic liver diseases in the United States from 1988 to 2008. Clin Gastroenterol Hepatol 2011; 9: 524–530.e1; quiz e60. [DOI] [PubMed] [Google Scholar]
- 53. Karajamaki AJ, Pätsi OP, Savolainen M, et al. Non-alcoholic fatty liver disease as a predictor of atrial fibrillation in middle-aged population (OPERA Study). PLoS One 2015; 10: e0142937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Markus MRP, Meffert PJ, Baumeister SE, et al. Association between hepatic steatosis and serum liver enzyme levels with atrial fibrillation in the general population. Atherosclerosis 2016; 245: 123–131. [DOI] [PubMed] [Google Scholar]
- 55. Sinner MF, Wang N, Fox CS, et al. Relation of circulating liver transaminase concentrations to risk of new-onset atrial fibrillation. Am J Cardiol 2013; 111: 219–224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Targher G, Mantovani A, Pichiri I, et al. Non-alcoholic fatty liver disease is associated with an increased prevalence of atrial fibrillation in hospitalized patients with type 2 diabetes. Clin Sci (Lond) 2013; 125: 301–309. [DOI] [PubMed] [Google Scholar]
- 57. Targher G, Valbusa F, Bonapace S, et al. Non-alcoholic fatty liver disease is associated with an increased incidence of atrial fibrillation in patients with type 2 diabetes. PLoS One 2013; 8: e57183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Wijarnpreecha K, Boonpheng B, Thongprayoon C, et al. The association between non-alcoholic fatty liver disease and atrial fibrillation: a meta-analysis. Clin Res Hepatol Gastroenterol 2017; 41: 525–532. [DOI] [PubMed] [Google Scholar]
- 59. Long MT, Yin X, Larson MG, et al. Relations of liver fat with prevalent and incident atrial fibrillation in the Framingham Heart Study. J Am Heart Assoc 2017; 6. pii: e005227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Goland S, Shimoni S, Zornitzki T, et al. Cardiac abnormalities as a new manifestation of nonalcoholic fatty liver disease: echocardiographic and tissue Doppler imaging assessment. J Clin Gastroenterol 2006; 40: 949–955. [DOI] [PubMed] [Google Scholar]
- 61. Hallsworth K, Hollingsworth KG, Thoma C, et al. Cardiac structure and function are altered in adults with non-alcoholic fatty liver disease. J Hepatol 2013; 58: 757–762. [DOI] [PubMed] [Google Scholar]
- 62. Bonapace S, Perseghin G, Molon G, et al. Nonalcoholic fatty liver disease is associated with left ventricular diastolic dysfunction in patients with type 2 diabetes. Diabetes Care 2012; 35: 389–395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Ndumele CE, Nasir K, Conceiçao RD, et al. Hepatic steatosis, obesity, and the metabolic syndrome are independently and additively associated with increased systemic inflammation. Arterioscler Thromb Vasc Biol 2011; 31: 1927–1932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Hamirani YS, Katz R, Nasir K, et al. Association between inflammatory markers and liver fat: the multi-ethnic study of atherosclerosis. J Clin Exp Cardiolog 2014; 5. pii: 1000344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Liu YC, Hung CS, Wu YW, et al. Influence of non-alcoholic fatty liver disease on autonomic changes evaluated by the time domain, frequency domain, and symbolic dynamics of heart rate variability. PLoS One 2013; 8: e61803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Sun W, Zhang D, Sun J, et al. Association between non-alcoholic fatty liver disease and autonomic dysfunction in a Chinese population. QJM 2015; 108: 617–624. [DOI] [PubMed] [Google Scholar]
- 67. Olshansky B. Interrelationships between the autonomic nervous system and atrial fibrillation. Prog Cardiovasc Dis 2005; 48: 57–78. [DOI] [PubMed] [Google Scholar]
- 68. Ozveren O, Izgi C, Eroglu E, et al. Doppler tissue evaluation of atrial conduction properties in patients with non-alcoholic fatty-liver disease. Ultrason Imaging 2016; 38: 225–235. [DOI] [PubMed] [Google Scholar]
- 69. Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med 2010; 363: 1341–1350. [DOI] [PubMed] [Google Scholar]
- 70. Musso G, Olivetti C, Cassader M, et al. Obstructive sleep apnea-hypopnea syndrome and nonalcoholic fatty liver disease: emerging evidence and mechanisms. Semin Liver Dis 2012; 32: 49–64. [DOI] [PubMed] [Google Scholar]
- 71. Kanagala R, Murali NS, Friedman PA, et al. Obstructive sleep apnea and the recurrence of atrial fibrillation. Circulation 2003; 107: 2589–2594. [DOI] [PubMed] [Google Scholar]
- 72. Gaeta M, Bandera F, Tassinari F, et al. Is epicardial fat depot associated with atrial fibrillation? A systematic review and meta-analysis. Europace 2017; 19: 747–752. [DOI] [PubMed] [Google Scholar]
- 73. Friedman DJ, Wang N, Meigs JB, et al. Pericardial fat is associated with atrial conduction: the Framingham Heart Study. J Am Heart Assoc 2014; 3; e000477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Sender R, Fuchs S, Milo R. Revised estimates for the number of human and bacteria cells in the body. PLoS Biol 2016; 14: e1002533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Yang X, Xie L, Li Y, et al. More than 9,000,000 unique genes in human gut bacterial community: estimating gene numbers inside a human body. PloS One 2009; 4: e6074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Emoto T, Yamashita T, Sasaki N, et al. Analysis of gut microbiota in coronary artery disease patients: a possible link between gut microbiota and coronary artery disease. J Atheroscler Thromb 2016; 23: 908–921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Lim GB. Heart failure: gut flora–pathogenic role in chronic heart failure. Nat Rev Cardiol 2016; 13: 61. [DOI] [PubMed] [Google Scholar]
- 78. Marques FZ, Mackay CR, Kaye DM. Beyond gut feelings: how the gut microbiota regulates blood pressure. Nat Rev Cardiol. Epub ahead of print 24 August 2017. DOI: 10.1038/nrcardio.2017.120. [DOI] [PubMed] [Google Scholar]
- 79. Tang WH, Wang Z, Levison BS, et al. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med 2013; 368: 1575–1584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Leung C, Rivera L, Furness JB, et al. The role of the gut microbiota in NAFLD. Nat Rev Gastroenterol Hepatol 2016; 13: 412–425. [DOI] [PubMed] [Google Scholar]
- 81. Koeth RA, Wang Z, Levison BS, et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med 2013; 19: 576–585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Wang Z, et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011; 472: 57–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Yu L, Meng G, Huang B, et al. A potential relationship between gut microbes and atrial fibrillation: trimethylamine N-oxide, a gut microbe-derived metabolite, facilitates the progression of atrial fibrillation. Int J Cardiol 2018; 255: 92–98. [DOI] [PubMed] [Google Scholar]
- 84. Serrano M, Moreno-Navarrete JM, Puig J, et al. Serum lipopolysaccharide-binding protein as a marker of atherosclerosis. Atherosclerosis 2013; 230: 223–227. [DOI] [PubMed] [Google Scholar]
- 85. Pastori D, Carnevale R, Nocella C, et al. Gut-derived serum lipopolysaccharide is associated with enhanced risk of major adverse cardiovascular events in atrial fibrillation: effect of adherence to Mediterranean diet. J Am Heart Assoc 2017; 6. pii: 005784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. De Filippo C, Cavalieri D, Di Paola M, et al. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proc Natl Acad Sci U S A 2010; 107: 14691–14696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. David LA, Maurice CF, Carmody RN, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014; 505: 559–563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Martinez-Gonzalez MA, Toledo E, Arós F, et al. Extravirgin olive oil consumption reduces risk of atrial fibrillation: the PREDIMED (Prevencion con Dieta Mediterranea) trial. Circulation 2014; 130: 18–26. [DOI] [PubMed] [Google Scholar]
- 89. Mitsou EK, Kakali A, Antonopoulou S, et al. Adherence to the Mediterranean diet is associated with the gut microbiota pattern and gastrointestinal characteristics in an adult population. Br J Nutr 2017; 117: 1645–1655. [DOI] [PubMed] [Google Scholar]
- 90. Pastori D, Carnevale R, Bartimoccia S, et al. Does Mediterranean diet reduce cardiovascular events and oxidative stress in atrial fibrillation? Antioxid Redox Signal 2015; 23: 682–687. [DOI] [PubMed] [Google Scholar]
- 91. Wang DZ, Chen W, Yang S, et al. Helicobacter pylori infection in Chinese patients with atrial fibrillation. Clin Interv Aging 2015; 10: 813–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Montenero AS, Mollichelli N, Zumbo F, et al. Helicobacter pylori and atrial fibrillation: a possible pathogenic link. Heart 2005; 91: 960–961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Yan J, She Q, Zhang Y, et al. The association between arrhythmia and helicobacter pylori infection: a meta-analysis of case-control studies. Int J Environ Res Public Health 2016; 13. pii: E1139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Lin K, Chen X, Zhang L, et al. Proton pump inhibitors as also inhibitors of atrial fibrillation. Eur J Pharmacol 2013; 718: 435–440. [DOI] [PubMed] [Google Scholar]
- 95. Stollberger C, Finsterer J. Treatment of esophagitis/vagitis-induced paroxysmal atrial fibrillation by proton-pump inhibitors. J Gastroenterol 2003; 38: 1109. [DOI] [PubMed] [Google Scholar]
- 96. Weigl M, Gschwantler M, Gatterer E, et al. Reflux esophagitis in the pathogenesis of paroxysmal atrial fibrillation: results of a pilot study. South Med J 2003; 96: 1128–1132. [DOI] [PubMed] [Google Scholar]
- 97. Aparci M, Uz O, Atalay M, et al. May hypomagnesaemia; caused by proton pump inhibitor; increase atrial fibrillation risk? Int J Cardiol 2016; 207: 141. [DOI] [PubMed] [Google Scholar]
- 98. Denton-Beaumont RN, Banning AS, Gershlick AH. Malabsorption causing failure of pharmacological therapy in the treatment of atrial fibrillation. Int J Cardiol 2008; 128: e87–e88. [DOI] [PubMed] [Google Scholar]
- 99. Hakeam HA, Al-Sanea N. Effect of major gastrointestinal tract surgery on the absorption and efficacy of direct acting oral anticoagulants (DOACs). J Thromb Thrombolysis 2017; 43: 343–351. [DOI] [PubMed] [Google Scholar]
- 100. Rottenstreich A, Barkai A, Arad A, et al. The effect of bariatric surgery on direct-acting oral anticoagulant drug levels. Thromb Res 2018; 163: 190–195. [DOI] [PubMed] [Google Scholar]
- 101. Kroll D, Stirnimann G, Vogt A, et al. Pharmacokinetics and pharmacodynamics of single doses of rivaroxaban in obese patients prior to and after bariatric surgery. Br J Clin Pharmacol 2017; 83: 1466–1475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Halperin JL, Hart RG. Atrial fibrillation and stroke: new ideas, persisting dilemmas. Stroke 1988; 19: 937–941. [DOI] [PubMed] [Google Scholar]
- 103. Hughes M, Lip GY. Stroke and thromboembolism in atrial fibrillation: a systematic review of stroke risk factors, risk stratification schema and cost effectiveness data. Thromb Haemost 2008; 99: 295–304. [DOI] [PubMed] [Google Scholar]
- 104. Bekwelem W, Connolly SJ, Halperin JL, et al. Extracranial systemic embolic events in patients with nonvalvular atrial fibrillation: incidence, risk factors, and outcomes. Circulation 2015; 132: 796–803. [DOI] [PubMed] [Google Scholar]
- 105. Frost L, Engholm G, Johnsen S, et al. Incident thromboembolism in the aorta and the renal, mesenteric, pelvic, and extremity arteries after discharge from the hospital with a diagnosis of atrial fibrillation. Arch Intern Med 2001; 161: 272–276. [DOI] [PubMed] [Google Scholar]
- 106. Lip GY, Nieuwlaat R, Pisters R, et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro heart survey on atrial fibrillation. Chest 2010; 137: 263–272. [DOI] [PubMed] [Google Scholar]
- 107. Hu WS, Lin CL. CHA2DS2-VASc score in the prediction of ischemic bowel disease among patients with atrial fibrillation: insights from a nationwide cohort. Int J Cardiol 2017: 235: 56–60. [DOI] [PubMed] [Google Scholar]
- 108. Barajas RF, Jr., Yeh BM, Webb EM, et al. Spectrum of CT findings in patients with atrial fibrillation and nontraumatic acute abdomen. AJR Am J Roentgenol 2009; 193: 485–492. [DOI] [PubMed] [Google Scholar]
- 109. Hunt SJ, Coakley FV, Webb EM, et al. Computed tomography of the acute abdomen in patients with atrial fibrillation. J Comput Assist Tomogr 2009; 33: 280–285. [DOI] [PubMed] [Google Scholar]
- 110. Cormier RE, Chase BA, Peterson GS, et al. Abdominal pain, atherosclerosis, and atrial fibrillation. The case for mesenteric ischemia. Med Decis Making 1982; 2: 323–339. [DOI] [PubMed] [Google Scholar]
- 111. Berland T, Oldenburg WA. Acute mesenteric ischemia. Curr Gastroenterol Rep 2008; 10: 341–346. [DOI] [PubMed] [Google Scholar]
- 112. Cortese B, Limbruno U. Acute mesenteric ischemia: primary percutaneous therapy. Catheter Cardiovasc Interv 2010; 75: 283–285. [DOI] [PubMed] [Google Scholar]
- 113. Nishida A, Fukui K. Images in clinical medicine. Transcatheter treatment of thromboembolism in the superior mesenteric artery. N Engl J Med 2005; 353: e4. [DOI] [PubMed] [Google Scholar]
- 114. Popovic P, Kuhelj D, Bunc M. Superior mesenteric artery embolism treated with percutaneous mechanical thrombectomy. Cardiovasc Intervent Radiol 2011; 34(Suppl. 2): S67–S69. [DOI] [PubMed] [Google Scholar]
- 115. Wasilewska M, Gosk-Bierska I. Thromboembolism associated with atrial fibrillation as a cause of limb and organ ischemia. Adv Clin Exp Med 2013; 22: 865–873. [PubMed] [Google Scholar]
- 116. Hazanov N, Attali M, Somin M, et al. Splenic embolus: 13 cases from a single medical department. Isr Med Assoc J 2006; 8: 694–697. [PubMed] [Google Scholar]
- 117. Garg L, Garg J, Gupta N, et al. Gastrointestinal complications associated with catheter ablation for atrial fibrillation. Int J Cardiol 2016; 224: 424–430. [DOI] [PubMed] [Google Scholar]
- 118. Di Biase L, Dodig M, Saliba W, et al. Capsule endoscopy in examination of esophagus for lesions after radiofrequency catheter ablation: a potential tool to select patients with increased risk of complications. J Cardiovasc Electrophysiol 2010; 21: 839–844. [DOI] [PubMed] [Google Scholar]
- 119. Gavin AR, Singleton CB, McGavigan AD. Assessment of oesophageal position by direct visualization with luminal contrast compared with segmentation from pre-acquired computed tomography scan-implications for ablation strategy. Europace 2014; 16: 1304–1308. [DOI] [PubMed] [Google Scholar]
- 120. Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: executive summary. J Arrhythm 2017; 33: 369–409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121. Aksu T, Guler TE, Bozyel S, et al. An underestimated complication of atrial fibrillation ablation: gastroparesis. Pacing Clin Electrophysiol 2015; 38: 653–654. [DOI] [PubMed] [Google Scholar]
- 122. Zellerhoff S, Lenze F, Eckardt L. Prophylactic proton pump inhibition after atrial fibrillation ablation: is there any evidence? Europace 2011; 13: 1219–1221. [DOI] [PubMed] [Google Scholar]
- 123. Ghia KK, Chugh A, Good E, et al. A nationwide survey on the prevalence of atrioesophageal fistula after left atrial radiofrequency catheter ablation. J Interv Card Electrophysiol 2009; 24: 33–36. [DOI] [PubMed] [Google Scholar]
- 124. Pappone C, Oral H, Santinelli V, et al. Atrio-esophageal fistula as a complication of percutaneous transcatheter ablation of atrial fibrillation. Circulation 2004; 109: 2724–2726. [DOI] [PubMed] [Google Scholar]
- 125. Tan C, Coffey A. Atrioesophageal fistula after surgical unipolar radiofrequency atrial ablation for atrial fibrillation. Ann Thorac Surg 2013; 95: e61–e62. [DOI] [PubMed] [Google Scholar]
- 126. Al-Alao B, Pickens A, Lattouf O. Atrio-oesophageal fistula: dismal outcome of a rare complication with no common solution. Interact Cardiovasc Thorac Surg 2016; 23: 949–956. [DOI] [PubMed] [Google Scholar]
- 127. Finsterer J, Stollberger C, Pulgram T. Neurological manifestations of atrio-esophageal fistulas from left atrial ablation. Eur J Neurol 2011; 18: 1212–1219. [DOI] [PubMed] [Google Scholar]
- 128. Moss CE, Fernandez-Caballero S, Walker D. Atrio-oesophageal fistula after transcatheter radiofrequency ablation. BMJ Case Rep 2015; 2015. pii: bcr2014204998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Chavez P, Messerli FH, Casso Dominguez A, et al. Atrioesophageal fistula following ablation procedures for atrial fibrillation: systematic review of case reports. Open heart 2015; 2: e000257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Dagres N, Kottkamp H, Piorkowski C, et al. Rapid detection and successful treatment of esophageal perforation after radiofrequency ablation of atrial fibrillation: lessons from five cases. J Cardiovasc Electrophysiol 2006; 17: 1213–1215. [DOI] [PubMed] [Google Scholar]
- 131. Khehra R, Agrawal S, Aoun E, et al. Unusual cause of upper gastrointestinal bleed, when OGD could be fatal. BMJ Case Rep 2015; 2015. pii: bcr2015210804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Shiraishi M, Morita H, Muramatsu K, et al. Successful non-operative management of left atrioesophageal fistula following catheter ablation. Surg Today 2014; 44: 1565–1568. [DOI] [PubMed] [Google Scholar]
- 133. Bailey CW, Tallaksen RJ. Pericardioesophageal fistula following left atrial ablation procedure. J Radiol Case Rep 2014; 8: 23–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Eitel C, Rolf S, Zachäus M, et al. Successful nonsurgical treatment of esophagopericardial fistulas after atrial fibrillation catheter ablation: a case series. Circ Arrhythm Electrophysiol 2013; 6: 675–681. [DOI] [PubMed] [Google Scholar]
- 135. Aksu T, Golcuk S, Guler TE, et al. Gastroparesis as a complication of atrial fibrillation ablation. Am J Cardiol 2015; 116: 92–97. [DOI] [PubMed] [Google Scholar]
- 136. Shah D, Dumonceau JM, Burri H, et al. Acute pyloric spasm and gastric hypomotility: an extracardiac adverse effect of percutaneous radiofrequency ablation for atrial fibrillation. J Am Coll Cardiol 2005; 46: 327–330. [DOI] [PubMed] [Google Scholar]
- 137. Jung HK, Choung RS, Locke GR, 3rd, et al. The incidence, prevalence, and outcomes of patients with gastroparesis in Olmsted County, Minnesota, from 1996 to 2006. Gastroenterology 2009; 136: 1225–1233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138. Pisani CF, Hachul D, Sosa E, et al. Gastric hypomotility following epicardial vagal denervation ablation to treat atrial fibrillation. J Cardiovasc Electrophysiol 2008; 19: 211–213. [DOI] [PubMed] [Google Scholar]
- 139. Lemery R. Left atrial anatomy, energy delivery and esophageal complications associated with ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2010; 21: 845–848. [DOI] [PubMed] [Google Scholar]
- 140. Bahnson TD. Strategies to minimize the risk of esophageal injury during catheter ablation for atrial fibrillation. Pacing Clin Electrophysiol 2009; 32: 248–260. [DOI] [PubMed] [Google Scholar]
- 141. Sanchez-Quintana D, Cabrera JA, Climent V, et al. Anatomic relations between the esophagus and left atrium and relevance for ablation of atrial fibrillation. Circulation 2005; 112: 1400–1405. [DOI] [PubMed] [Google Scholar]
- 142. Di Biase L, Saenz LC, Burkhardt DJ, et al. Esophageal capsule endoscopy after radiofrequency catheter ablation for atrial fibrillation: documented higher risk of luminal esophageal damage with general anesthesia as compared with conscious sedation. Circ Arrhythm Electrophysiol 2009; 2: 108–112. [DOI] [PubMed] [Google Scholar]
- 143. Halm U, Gaspar T, Zachäus M, et al. Thermal esophageal lesions after radiofrequency catheter ablation of left atrial arrhythmias. Am J Gastroenterol 2010; 105: 551–556. [DOI] [PubMed] [Google Scholar]
- 144. Agnelli G, Eriksson BI, Cohen AT, et al. Safety assessment of new antithrombotic agents: lessons from the EXTEND study on ximelagatran. Thromb Res 2009; 123: 488–497. [DOI] [PubMed] [Google Scholar]
- 145. Abraham NS, Noseworthy PA, Yao X, et al. Gastrointestinal safety of direct oral anticoagulants: a large population-based study. Gastroenterology 2017; 152: 1014–1022.e1. [DOI] [PubMed] [Google Scholar]
- 146. Douros A, Azoulay L, Yin H, et al. Non-vitamin K antagonist oral anticoagulants and risk of serious liver injury. J Am Coll Cardiol 2018; 71: 1105–1113. [DOI] [PubMed] [Google Scholar]
- 147. Tripodi A, Mannucci PM. The coagulopathy of chronic liver disease. N Engl J Med 2011; 365: 147–156. [DOI] [PubMed] [Google Scholar]
- 148. Efird LM, Mishkin DS, Berlowitz DR, et al. Stratifying the risks of oral anticoagulation in patients with liver disease. Circ Cardiovasc Qual Outcomes 2014; 7: 461–467. [DOI] [PubMed] [Google Scholar]
- 149. Kuo L, Chao TF, Liu CJ, et al. Liver cirrhosis in patients with atrial fibrillation: would oral anticoagulation have a net clinical benefit for stroke prevention? J Am Heart Assoc 2017; 6. pii: e005307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150. Morrill AM, Ge D, Willett KC. Dosing of target-specific oral anticoagulants in special populations. Ann Pharmacother 2015; 49: 1031–1045. [DOI] [PubMed] [Google Scholar]
- 151. Goriacko P, Veltri KT. Safety of direct oral anticoagulants versus warfarin in patients with chronic liver disease and atrial fibrillation. Eur J Haematol 2018; 100: 488–493. [DOI] [PubMed] [Google Scholar]
- 152. Pastori D, Lip GYH, Farcomeni A, et al. Incidence of bleeding in patients with atrial fibrillation and advanced liver fibrosis on treatment with vitamin K or non-vitamin K antagonist oral anticoagulants. Int J Cardiol 2018; 264: 58–63. [DOI] [PubMed] [Google Scholar]
- 153. Graff J, Harder S. Anticoagulant therapy with the oral direct factor Xa inhibitors rivaroxaban, apixaban and edoxaban and the thrombin inhibitor dabigatran etexilate in patients with hepatic impairment. Clin Pharmacokinet 2013; 52: 243–254. [DOI] [PubMed] [Google Scholar]
- 154. Steffel J, Verhamme P, Potpara TS, et al. The 2018 European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J 2018; 39: 1330–1393. [DOI] [PubMed] [Google Scholar]
- 155. Acosta RD, Abraham NS, Chandrasekhara V, et al.; ASGE Standards of Practice Committee. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc 2016; 83: 3–16. [DOI] [PubMed] [Google Scholar]
- 156. Chan FKL, Goh KL, Reddy N, et al. Management of patients on antithrombotic agents undergoing emergency and elective endoscopy: joint Asian Pacific Association of Gastroenterology (APAGE) and Asian Pacific Society for Digestive Endoscopy (APSDE) practice guidelines. Gut 2018; 67: 405–417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157. Vassallo P, Trohman RG. Prescribing amiodarone: an evidence-based review of clinical indications. JAMA 2007; 298: 1312–1322. [DOI] [PubMed] [Google Scholar]
- 158. Lewis JH, Ranard RC, Caruso A, et al. Amiodarone hepatotoxicity: prevalence and clinicopathologic correlations among 104 patients. Hepatology 1989; 9: 679–685. [DOI] [PubMed] [Google Scholar]
- 159. Vorperian VR, Havighurst TC, Miller S, et al. Adverse effects of low dose amiodarone: a meta-analysis. J Am Coll Cardiol 1997; 30: 791–798. [DOI] [PubMed] [Google Scholar]
- 160. Patel V, Sanyal AJ. Drug-induced steatohepatitis. Clin Liver Dis 2013; 17: 533–546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161. Flack KF, Desai J, Kolb JM, et al. Major gastrointestinal bleeding often is caused by occult malignancy in patients receiving warfarin or dabigatran to prevent stroke and systemic embolism from atrial fibrillation. Clin Gastroenterol Hepatol 2017; 15: 682–690. [DOI] [PubMed] [Google Scholar]
- 162. Potpara TS, Lip GY. Postapproval observational studies of non-vitamin K antagonist oral anticoagulants in atrial fibrillation. JAMA 2017; 317: 1115–1116. [DOI] [PubMed] [Google Scholar]
- 163. Cangemi DJ, Krill T, Weideman R, et al. A comparison of the rate of gastrointestinal bleeding in patients taking non-vitamin K antagonist oral anticoagulants or warfarin. Am J Gastroenterol 2017; 112: 734–739. [DOI] [PubMed] [Google Scholar]
- 164. Ntaios G, Papavasileiou V, Makaritsis K, et al. Real-world setting comparison of nonvitamin-K antagonist oral anticoagulants versus vitamin-K antagonists for stroke prevention in atrial fibrillation: a systematic review and meta-analysis. Stroke 2017; 48: 2494–2503. [DOI] [PubMed] [Google Scholar]
- 165. Miller CS, Dorreen A, Martel M, et al. Risk of gastrointestinal bleeding in patients taking non-vitamin K antagonist oral anticoagulants: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2017; 15: 1674–1683.e1673. [DOI] [PubMed] [Google Scholar]
- 166. Freedman B, Camm J, Calkins H, et al. Screening for atrial fibrillation: a report of the AF-SCREEN international collaboration. Circulation 2017; 135: 1851–1867. [DOI] [PubMed] [Google Scholar]
- 167. Marzec LN, Wang J, Shah ND, et al. Influence of direct oral anticoagulants on rates of oral anticoagulation for atrial fibrillation. J Am Coll Cardiol 2017; 69: 2475–2484. [DOI] [PubMed] [Google Scholar]