

Abstract
Background
The majority of children who present with their first episode of nephrotic syndrome achieve remission with corticosteroid therapy. Children who fail to respond may be treated with immunosuppressive agents including calcineurin inhibitors (cyclosporin or tacrolimus) and with non‐immunosuppressive agents such as angiotensin‐converting enzyme inhibitors (ACEi). Optimal combinations of these agents with the least toxicity remain to be determined. This is an update of a review first published in 2004 and updated in 2006 and 2010.
Objectives
To evaluate the benefits and harms of different interventions used in children with idiopathic nephrotic syndrome, who do not achieve remission following four weeks or more of daily corticosteroid therapy.
Search methods
We searched Cochrane Kidney and Transplant's Specialised Register (up to 2 March 2016) through contact with the Information Specialist using search terms relevant to this review.
Selection criteria
RCTs and quasi‐RCTs were included if they compared different immunosuppressive agents or non‐immunosuppressive agents with placebo, prednisone or other agent given orally or parenterally in children aged three months to 18 years with SRNS.
Data collection and analysis
Two authors independently searched the literature, determined study eligibility, assessed risk of bias and extracted data. For dichotomous outcomes, results were expressed as risk ratios (RR) and 95% confidence intervals (CI). Data were pooled using the random effects model.
Main results
Nineteen RCTs (820 children enrolled; 773 evaluated) were included. Most studies were small. Eleven studies were at low risk of bias for allocation concealment and only four studies were at low risk of performance bias. Fifteen, eight and 10 studies were at low risk of detection bias, attrition bias and reporting bias respectively. Cyclosporin when compared with placebo or no treatment significantly increased the number of children who achieved complete remission. However this was based on only eight children who achieved remission with cyclosporin compared with no children who achieved remission with placebo/no treatment in three small studies (49 children: RR 7.66, 95% CI 1.06 to 55.34). Calcineurin inhibitors significantly increased the number with complete or partial remission compared with IV cyclophosphamide (2 studies, 156 children: RR 1.98, 95% CI 1.25 to 3.13; I2 = 20%). There was no significant differences in the number who achieved complete remission between tacrolimus versus cyclosporin (1 study, 41 children: RR 0.86, 95% CI 0.44 to 1.66), cyclosporin versus mycophenolate mofetil plus dexamethasone (1 study, 138 children: RR 2.14, 95% CI 0.87 to 5.24), oral cyclophosphamide with prednisone versus prednisone alone (2 studies, 91 children: RR 1.06, 95% CI 0.61 to 1.87), IV versus oral cyclophosphamide (1 study, 11 children: RR 3.13, 95% CI 0.81 to 12.06), IV cyclophosphamide versus oral cyclophosphamide plus IV dexamethasone (1 study, 49 children: RR 1.13, 95% CI 0.65 to 1.96), and azathioprine with prednisone versus prednisone alone (1 study, 31 children: RR 0.94, 95% CI 0.15 to 5.84). One study found no significant differences between three agents (cyclophosphamide, mycophenolate mofetil, leflunomide) used in combination with tacrolimus and prednisone. One study found no significant difference in the percentage reduction in proteinuria (31 children: ‐12; 95% CI ‐73 to 110) between rituximab with cyclosporin/prednisolone and cyclosporin/prednisolone alone. Two studies reported ACEi significantly reduced proteinuria.
Authors' conclusions
To date RCTs have demonstrated that calcineurin inhibitors increase the likelihood of complete or partial remission compared with placebo/no treatment or cyclophosphamide. For other regimens assessed, it remains uncertain whether the interventions alter outcomes because the certainty of the evidence is low. Further adequately powered, well designed RCTs are needed to evaluate other regimens for children with idiopathic SRNS. Since SRNS represents a spectrum of diseases, future studies should enrol children from better defined groups of patients with SRNS.
Keywords: Adolescent; Child; Child, Preschool; Humans; Infant; Angiotensin‐Converting Enzyme Inhibitors; Angiotensin‐Converting Enzyme Inhibitors/therapeutic use; Azathioprine; Azathioprine/therapeutic use; Cyclophosphamide; Cyclophosphamide/therapeutic use; Cyclosporine; Cyclosporine/therapeutic use; Dexamethasone; Dexamethasone/therapeutic use; Drug Resistance; Glucocorticoids; Glucocorticoids/therapeutic use; Immunosuppressive Agents; Immunosuppressive Agents/therapeutic use; Isoxazoles; Isoxazoles/therapeutic use; Leflunomide; Mycophenolic Acid; Mycophenolic Acid/analogs & derivatives; Mycophenolic Acid/therapeutic use; Nephrotic Syndrome; Nephrotic Syndrome/drug therapy; Prednisone; Prednisone/therapeutic use; Randomized Controlled Trials as Topic; Remission Induction
Interventions for idiopathic steroid‐resistant nephrotic syndrome in children
What is the issue?
Nephrotic syndrome is a condition where the kidneys leak protein from the blood into the urine. Corticosteroids are used in the first instance to achieve remission. Some children do not respond to this treatment (steroid‐resistant nephrotic syndrome) and other agents such as cyclophosphamide, calcineurin inhibitors (cyclosporin, tacrolimus) or angiotensin‐converting enzyme inhibitors may be used.
What did we do?
We searched Cochrane Kidney and Transplant's Specialised Register (up to 2 March 2016) through contact with the Information Specialist using search terms relevant to this review. Randomised controlled trials were included if they compared different immunosuppressive agents or non‐immunosuppressive agents with placebo, prednisone or other agent given orally or parenterally in children aged three months to 18 years with steroid‐resistant nephrotic syndrome.
What did we find?
This review found that when cyclosporin was compared to placebo or no treatment there was a significant increase in the number of children who achieved complete remission. Calcineurin inhibitors also significantly increased the number of children, who achieved complete or partial remission compared with IV cyclophosphamide. There was no improvement with other immunosuppressive agents. Angiotensin‐converting enzyme inhibitors significantly reduced the degree of proteinuria. However the number of studies was small with small numbers of children per study.
Summary of findings
Summary of findings for the main comparison.
Cyclosporin versus placebo/no treatment
| Interventions for idiopathic steroid‐resistant nephrotic syndrome in children | ||||||
| Patient or population: idiopathic steroid‐resistant nephrotic syndrome in children Setting: paediatric nephrology clinics Intervention: cyclosporin Comparison: placebo/no treatment | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with placebo/no treatment | Risk with Cyclosporin | |||||
| Complete remission: all renal pathologies | Study population | RR 7.66 (1.06 to 55.34) | 49 (3) | ⊕⊕⊝⊝ LOW 1 2 | ||
| 0 per 1000 | 0 per 1000 (0 to 0) | |||||
| Complete remission: FSGS | Study population | RR 5.83 (0.75 to 45.09) | 33 (2) | ⊕⊕⊝⊝ LOW 1 | ||
| 0 per 1000 | 0 per 1000 (0 to 0) | |||||
| Complete or partial remission: all renal pathologies | Study population | RR 5.48 (1.95 to 15.44) | 49 (3) | ⊕⊕⊝⊝ LOW 1 2 | ||
| 87 per 1000 | 477 per 1000 (170 to 1000) | |||||
| Complete or partial remission: FSGS | Study population | RR 5.00 (1.63 to 15.31) | 24 (1) | ⊕⊕⊝⊝ LOW 1 | ||
| 167 per 1000 | 833 per 1000 (272 to 1000) | |||||
| Moderate | ||||||
| 167 per 1000 | 834 per 1000 (272 to 1000) | |||||
| Adverse events: worsening of hypertension | Study population | not estimable | 24 (1) | ⊕⊕⊝⊝ LOW 1 | ||
| 167 per 1000 | Not estimable | |||||
| Moderate | ||||||
| 167 per 1000 | Not estimable | |||||
| Adverse events: infection | Study population | not estimable | 17 (1) | ⊕⊝⊝⊝ VERY LOW 1 3 | ||
| 429 per 1000 | Not estimable | |||||
| Moderate | ||||||
| 429 per 1000 | Not estimable | |||||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Few enrolled patients with few events
2 Risk of selection bias in 1 of 3 studies; 2 of 3 studies at risk of performance bias
3 Risk of performance bias
Summary of findings 2.
Calcineurin inhibitors versus IV cyclophosphamide
| Interventions for idiopathic nephrotic syndrome in children | ||||||
| Patient or population: idiopathic steroid‐resistant nephrotic syndrome in children Setting: paediatric nephrology clinics Intervention: calcineurin inhibitor (CNI) Comparison: IV cyclophosphamide (CPA) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with IV CPA | Risk with CNI | |||||
| Remission at 3 to 6 months: complete or partial remission | Study population | RR 1.98 (1.25 to 3.13) | 156 (2) | ⊕⊕⊝⊝ LOW 1 2 | ||
| 397 per 1000 | 787 per 1000 (497 to 1000) | |||||
| Moderate | ||||||
| 318 per 1000 | 629 per 1000 (397 to 994) | |||||
| Remission at 3 to 6 months: complete remission | Study population | RR 3.43 (1.84 to 6.41) | 156 (2) | ⊕⊕⊝⊝ LOW 1 2 | ||
| 128 per 1000 | 440 per 1000 (236 to 822) | |||||
| Moderate | ||||||
| 103 per 1000 | 354 per 1000 (190 to 662) | |||||
| Remission at 3 to 6 months: partial remission | Study population | RR 1.68 (0.43 to 6.56) | 156 (2) | ⊕⊝⊝⊝ VERY LOW 1 2 3 | ||
| 269 per 1000 | 452 per 1000 (116 to 1000) | |||||
| Moderate | ||||||
| 215 per 1000 | 361 per 1000 (92 to 1000) | |||||
| Adverse events: treatment failure (non response, serious infection, persistently elevated creatinine) at 6 months | Study population | RR 0.32 (0.18 to 0.58) | 124 (1) | ⊕⊕⊕⊝ MODERATE 4 | ||
| 541 per 1000 | 173 per 1000 (97 to 314) | |||||
| Moderate | ||||||
| 541 per 1000 | 173 per 1000 (97 to 314) | |||||
| Adverse events: medications ceased due to adverse events | Study population | RR 0.20 (0.04 to 0.86) | 131 (1) | ⊕⊕⊕⊝ MODERATE 4 | ||
| 154 per 1000 | 31 per 1000 (6 to 132) | |||||
| Moderate | ||||||
| 154 per 1000 | 31 per 1000 (6 to 132) | |||||
| Adverse events: serious infections | Study population | RR 0.49 (0.16 to 1.56) | 131 (1) | ⊕⊕⊕⊝ MODERATE 4 | ||
| 123 per 1000 | 60 per 1000 (20 to 192) | |||||
| Moderate | ||||||
| 123 per 1000 | 60 per 1000 (20 to 192) | |||||
| Adverse events: death | Study population | RR 0.33 (0.01 to 7.92) | 131 (1) | ⊕⊕⊝⊝ LOW 4 | ||
| 15 per 1000 | 5 per 1000 (0 to 122) | |||||
| Moderate | ||||||
| 15 per 1000 | 5 per 1000 (0 to 122) | |||||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Small patient numbers and events
2 High risk of attrition bias in one study
3 Heterogeneity between studies
4 Single study; small patient numbers and events
Summary of findings 3.
Cyclosporin versus mycophenolate mofetil with dexamethasone
| Interventions for idiopathic steroid‐resistant nephrotic syndrome in children | ||||||
| Patient or population: idiopathic steroid‐resistant nephrotic syndrome in children Setting: Paediatric and adult nephrology clinics Intervention: cyclosporin Comparison: mycophenolate mofetil with pulse dexamethasone | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with mycophenolate mofetil with pulse dexamethasone | Risk with Cyclosporin | |||||
| Remission at 52 weeks: complete remission (primary outcome 1,2) | Study population | RR 2.14 (0.87 to 5.24) | 138 (1) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 91 per 1000 | 195 per 1000 (79 to 476) | |||||
| Moderate | ||||||
| 91 per 1000 | 195 per 1000 (79 to 476) | |||||
| Remission at 52 weeks: complete or partial remission (primary outcome 1,2,3) | Study population | RR 1.38 (0.90 to 2.10) | 138 (1) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 333 per 1000 | 460 per 1000 (300 to 700) | |||||
| Moderate | ||||||
| 333 per 1000 | 460 per 1000 (300 to 700) | |||||
| CKD or death: death by 52 weeks | Study population | RR 0.18 (0.01 to 3.75) | 138 (1) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 30 per 1000 | 5 per 1000 (0 to 114) | |||||
| Moderate | ||||||
| 30 per 1000 | 5 per 1000 (0 to 114) | |||||
| CKD or death: 50% decline in GFR by 78 weeks | Study population | RR 2.29 (0.46 to 11.41) | 138 (1) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 30 per 1000 | 69 per 1000 (14 to 346) | |||||
| Moderate | ||||||
| 30 per 1000 | 69 per 1000 (14 to 346) | |||||
| Adverse effects (weeks 0 to 26): serious infection requiring hospitalisation | Study population | RR 0.65 (0.22 to 1.96) | 138 (1) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 106 per 1000 | 69 per 1000 (23 to 208) | |||||
| Moderate | ||||||
| 106 per 1000 | 69 per 1000 (23 to 208) | |||||
| Adverse effects (weeks 0 to 26): neuropsychiatric conditions | Study population | RR 1.26 (0.73 to 2.19) | 138 (1) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 242 per 1000 | 305 per 1000 (177 to 531) | |||||
| Moderate | ||||||
| 242 per 1000 | 305 per 1000 (177 to 531) | |||||
| Adverse effects (weeks 0 to 26): hypertension | Study population | RR 1.68 (0.66 to 4.29) | 138 (1) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 91 per 1000 | 153 per 1000 (60 to 390) | |||||
| Moderate | ||||||
| 91 per 1000 | 153 per 1000 (60 to 390) | |||||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Insufficient recruitment to exclude difference between treatments
Summary of findings 4.
Oral cyclophosphamide versus prednisone/placebo
| Interventions for idiopathic steroid‐resistant nephrotic syndrome in children | ||||||
| Patient or population: idiopathic steroid‐resistant nephrotic syndrome in children Setting: paediatric nephrology clinics Intervention: oral cyclophosphamide Comparison: prednisone/placebo | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with prednisone/placebo | Risk with Oral cyclophosphamide | |||||
| Complete remission: all renal pathologies | Study population | RR 1.06 (0.61 to 1.87) | 84 (2) | ⊕⊕⊝⊝ LOW 1 2 | ||
| 353 per 1000 | 374 per 1000 (215 to 660) | |||||
| Moderate | ||||||
| 374 per 1000 | 396 per 1000 (228 to 699) | |||||
| Complete remission: FSGS | Study population | RR 1.01 (0.43 to 2.37) | 63 (2) | ⊕⊕⊝⊝ LOW 1 2 | ||
| 250 per 1000 | 253 per 1000 (108 to 593) | |||||
| Moderate | ||||||
| 143 per 1000 | 144 per 1000 (61 to 339) | |||||
| Complete or partial remission | Study population | RR 0.88 (0.53 to 1.45) | 53 (1) | ⊕⊕⊝⊝ LOW 2 3 | ||
| 571 per 1000 | 503 per 1000 (303 to 829) | |||||
| Moderate | ||||||
| 571 per 1000 | 503 per 1000 (303 to 829) | |||||
| Treatment failure | Study population | RR 1.59 (0.87 to 2.88) | 60 (1) | ⊕⊕⊝⊝ LOW 2 3 | ||
| 360 per 1000 | 572 per 1000 (313 to 1000) | |||||
| Moderate | ||||||
| 360 per 1000 | 572 per 1000 (313 to 1000) | |||||
| Adverse events: all‐cause mortality | Study population | not estimable | 60 (1) | ⊕⊕⊝⊝ LOW 2 3 | Three events in cyclophosphamide group and two in prednisone group | |
| 80 per 1000 | 85 per 1000 | |||||
| Moderate | ||||||
| 80 per 1000 | 85 per 1000 | |||||
| Adverse events: hypertension with seizures | Study population | not estimable | 60 (1) | ⊕⊝⊝⊝ VERY LOW 2 3 | One event in each group | |
| 40 per 1000 | 28 per 1000 | |||||
| Moderate | ||||||
| 40 per 1000 | 28 per 1000 | |||||
| Adverse events: bone marrow suppression | Study population | not estimable | 60 (1) | ⊕⊝⊝⊝ VERY LOW 2 3 | No events in either group | |
| 0 per 1000 | 0 per 1000 (0 to 0) | |||||
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Unclear risk of selection bias; risk of attrition bias in 1 study and selection bias in 1 study; no blinding
2 Small patient numbers and few events
3 Unclear risk of selection bias; high risk of attrition bias
Background
Description of the condition
Nephrotic syndrome is a condition in which the glomeruli of the kidney leak protein from the blood into the urine. It results in hypoproteinaemia and generalised oedema. Children with untreated nephrotic syndrome are at increased risk of bacterial infection, characteristically resulting in peritonitis, cellulitis or septicaemia, of thromboembolic phenomena, protein calorie malnutrition. Prospective studies of children with newly diagnosed idiopathic nephrotic syndrome identified through Pediatric Surveillance Units in the Netherlands, Australia and New Zealand reported incidences of idiopathic nephrotic syndrome of 1.12 to 1.9 per 100,000 children aged below 16 years (El Bakkali 2011; Sureshkumar 2014; Wong 2007).
In clinical studies childhood nephrotic syndrome is classified into steroid‐sensitive nephrotic syndrome (SSNS), steroid‐resistant nephrotic syndrome (SRNS), congenital and infantile nephrotic syndrome (0 to 12 months) and nephrotic syndrome secondary to other diseases including Henoch Schönlein nephritis, systemic lupus erythematosus and hepatitis B nephropathy. Most children respond to corticosteroid therapy. In those children who fail to respond to corticosteroids, kidney biopsy is performed to determine pathology. The majority of children with SRNS have minimal change disease (MCD), mesangioproliferative glomerulonephritis (MesPGN) or focal segmental glomerulosclerosis (FSGS). FSGS is a leading cause of end‐stage kidney disease (ESKD) in children. FSGS is a heterogeneous disease with some children having FSGS secondary to immunological factors, some children having FSGS secondary to mutations in the genes coding for podocyte proteins including podocin and nephrin and a few older children having FSGS secondary to hyperfiltration (reduced kidney mass, obesity, diabetes mellitus) (Deegens 2011). A study of 1783 unrelated families found that single gene mutations responsible for SRNS were identified in 29.5% families overall with mutations in 25.3% children aged 1 to 6 years old, 17.8% in children aged 7 to 12 years and 10.8% in adolescents aged 13 to 18 years (Sadowski 2015). Few children with FSGS secondary to genetic mutations respond to immunosuppressive agents and in these children, nephrotic syndrome rarely recurs following kidney transplantation (Ding 2014). Children with SRNS may have corticosteroid resistant disease from initial presentation (Initial resistance) or may develop steroid resistance after one or more responses to corticosteroids (delayed steroid resistance). About one third of children suffer recurrence of nephrotic syndrome following kidney transplantation. Recent data suggest that recurrence of disease post transplant is much more common in children with SRNS and delayed steroid resistance (Ding 2014). These data are consistent with an immunological cause of SRNS in these children.
Description of the intervention
Oral corticosteroids are the first‐line treatment for a child presenting with idiopathic nephrotic syndrome. For children who present with their first episode of nephrotic syndrome, about 90% will achieve remission with corticosteroid therapy (Koskimies 1982). Of those who respond, about 95% will have responded after four weeks of daily corticosteroid therapy and 98% will have responded after eight weeks of corticosteroid therapy (ISKDC 1981a).
Children who fail to respond to corticosteroids are treated with immunosuppressive agents such as calcineurin inhibitors (CNI) (cyclosporin, tacrolimus), cyclophosphamide, chlorambucil, mycophenolate mofetil, and the anti CD 20 monoclonal antibody, rituximab. Rates of complete and partial remission with CNI based on observational studies and individual groups in randomised controlled trials (RCTs) vary between 30% and 80% (Choudhry 2009; FSGS Study 2011; Niaudet 1994). Remission rates of up to 60% with combinations of intravenous (IV) methylprednisolone and cyclophosphamide are reported in observational studies (Tune 1996) and of around 50% in individual treatment groups in RCTs (Gulati 2012; ISKDC 1974; ISKDC 1996). Failure to achieve complete or partial remission is associated with progression to ESKD (Gipson 2006). Other non‐immunosuppressive agents including angiotensin‐converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARB), and fish oil have also been used in SRNS.
How the intervention might work
Corticosteroids, immunosuppressive agents and monoclonal antibodies may act by suppressing production of plasma factors by T and B cells since immunological mechanisms are believed to be responsible for some cases of SRNS. Some immunosuppressive medications including dexamethasone, the CNI, and rituximab may be effective in nonimmune causes of SRNS by directly targeting podocytes. ACEi and ARB reduce proteinuria and are aimed at reducing progressive glomerulosclerosis (Deegens 2011).
Why it is important to do this review
There is considerable diversity in the use of these agents with differences in treatment modes, combinations and dosage regimens. Optimal combinations with least toxicity remain to be determined. Despite the use of newer immunosuppressive agents, the response rate to therapy remains relatively low. The aims of the update of this systematic review initially published in 2002 were to identify new RCTs assessing the benefits and harms of interventions used to treat idiopathic SRNS in children and to incorporate them where appropriate in meta‐analyses.
Objectives
To evaluate the benefits and harms of different interventions used in children with idiopathic nephrotic syndrome, who do not achieve remission following four weeks or more of daily corticosteroid therapy.
Methods
Criteria for considering studies for this review
Types of studies
All RCTs and quasi‐RCTs, in which different agents were used in the treatment of children (aged three months to 18 years) with idiopathic SRNS, were included.
Types of participants
Inclusion criteria
Children aged three months to 18 years with SRNS (i.e. persistence of proteinuria > 3+ on dipstick, urinary protein‐creatinine ratio (UP/C) > 0.2 g/mmol (> 2mg/g) or > 40 mg/m2/h after four weeks or more of daily corticosteroid agent). Where a kidney biopsy was performed, only children with biopsy diagnoses of MCD, MesPGN, IgM nephropathy or FSGS were included. Children with initial steroid resistance and children with delayed steroid resistance were included.
Exclusion criteria
Children with SSNS, children with congenital nephrotic syndrome and children with other kidney or systemic forms of nephrotic syndrome defined on kidney biopsy, clinical features or serology (e.g. post‐infectious glomerulonephritis, Henoch‐Schönlein nephritis, systemic lupus erythematosus, membranous glomerulopathy or mesangiocapillary glomerulonephritis) were excluded. Children with FSGS secondary to hyperfiltration (obesity, diabetes mellitus, reduced kidney mass) were excluded.
Types of interventions
All interventions were potentially eligible. Interventions considered were as follows.
IV corticosteroid agent versus oral corticosteroid agent, placebo or no intervention
Different doses and/or durations of IV corticosteroid agent
Non‐corticosteroid immunosuppressive agent (with or without concomitant use of corticosteroid agent) versus corticosteroid agent alone
Two different non‐corticosteroid agents (with or without concomitant use of corticosteroid agent)
Different doses, durations and routes of administration of the same non‐corticosteroid agent (with or without concomitant use of corticosteroid agent)
Other non‐immunosuppressive agents such as ACEi or fish oil used with or without corticosteroid or non‐corticosteroid immunosuppressive agents.
Types of outcome measures
Primary outcomes
Number in complete remission during and following therapy (i.e. the child became oedema‐free and urine protein was < 1+ on dipstick, urinary UP/C < 0.02 g/mmol (< 2 mg/g) or < 4 mg/m2/h for three or more consecutive days)
Number in partial remission with reduction in proteinuria (i.e. proteinuria < 2+ , urinary UP/C < 0.2 g/mmol or < 40 mg/m2/h) and an increase in serum albumin levels
Number reaching ESKD.
Secondary outcomes
Changes in kidney function: serum creatinine (SCr); creatinine clearance (CrCl); estimated glomerular filtration rate (eGFR)
Adverse effects of therapy
Duration of remission or partial remission
Reduction in proteinuria.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Kidney and Transplant Specialised Register (up to 2 March 2016) through contact with the Information Specialist using search terms relevant to this review. The Specialised Register contains studies identified from several sources.
Monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL)
Weekly searches of MEDLINE OVID SP
Handsearching of kidney‐related journals and the proceedings of major kidney conferences
Searching of the current year of EMBASE OVID SP
Weekly current awareness alerts for selected kidney journals
Searches of the International Clinical Trials Register (ICTRP) Search Portal and ClinicalTrials.gov.
Studies contained in the Specialised Register are identified through search strategies for CENTRAL, MEDLINE, and EMBASE based on the scope of Cochrane Kidney and Transplant. Details of these strategies, as well as a list of handsearched journals, conference proceedings and current awareness alerts, are available in the Specialised Register section of information about the Cochrane Kidney and Transplant.
See Appendix 1 for search terms used in strategies for this review.
Searching other resources
No other resources were searched for this update because the scope of Cochrane Kidney and Transplant’s Specialised Register covers the most likely sources of studies.
Data collection and analysis
Selection of studies
The search strategy described was used to obtain titles and abstracts of studies that were relevant to the review. The titles and abstracts were screened independently by two authors, who discarded studies that were not applicable. However studies and reviews that might include relevant data or information on studies were retained initially. Two authors independently assessed retrieved abstracts and, if necessary the full text, of these studies to determine which studies satisfied the inclusion criteria. Disagreements were resolved in consultation with a third author.
Data extraction and management
Data extraction was carried out by the same authors independently using standard data extraction forms. Studies reported in non‐English language journals were translated before assessment. Where more than one publication of one study existed, reports were grouped together and the publication with the most complete data was used in the analyses. Disagreements were resolved in consultation with a third author.
Assessment of risk of bias in included studies
Studies to be included were assessed independently by two authors without blinding to authorship or journal. Discrepancies were resolved by discussion with a third author.
The following items were assessed using the risk of bias assessment tool (Higgins 2011) (seeAppendix 2).
Was there adequate sequence generation (selection bias)?
Was allocation adequately concealed (selection bias)?
-
Was knowledge of the allocated interventions adequately prevented during the study?
Participants and personnel (performance bias)
Outcome assessors (detection bias)
Were incomplete outcome data adequately addressed (attrition bias)?
Are reports of the study free of suggestion of selective outcome reporting (reporting bias)?
Was the study apparently free of other problems that could put it at a risk of bias?
Measures of treatment effect
For dichotomous outcomes (e.g. remission or no remission) results were expressed as risk ratios (RR) with 95% confidence intervals (CI). Where continuous scales of measurement were used to assess the effects of treatment (e.g. protein excretion), the mean difference (MD) was to be used, or the standardised MD (SMD) if different scales were to be used.
Adverse events were reported in the text if they could not be included in meta‐analyses.
Unit of analysis issues
Data from cross‐over studies were included in the meta‐analyses if separate data for the first part of the study were available. Otherwise results of cross‐over studies were reported in the text only.
Dealing with missing data
Any further information required from the original author was requested by written correspondence and any relevant information obtained in this manner was included in the review. We aimed to analyse available data in meta‐analyses using ITT data. However, where ITT data were not provided, or additional information could not be obtained from authors, available published data were used in the analyses.
Assessment of heterogeneity
Heterogeneity was analysed using a Chi2 test on N‐1 degrees of freedom, with an alpha of 0.05 used for statistical significance and by I2, which describes the percentage of total variation across studies that is due to heterogeneity rather than chance (Higgins 2003). I2 values of 25%, 50% and 75% correspond to low, medium and high levels of heterogeneity.
Assessment of reporting biases
The search strategy used aimed to reduce publication bias caused by lack of publication of studies with negative results. Where there were several publications on the same study, all reports were reviewed to ensure that all details of methods and results were included to reduce the risk of selective outcome reporting bias.
Data synthesis
Data was pooled using the random effects model but the fixed effects model was analysed to ensure robustness of the model chosen and susceptibility to outliers.
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was planned to explore possible sources of heterogeneity (e.g. participants, treatments and study quality). Heterogeneity among participants could be related to age and renal pathology. Heterogeneity in treatments could be related to prior agent(s) used and the agent, dose and duration of therapy. However there were insufficient studies of each intervention to allow subgroup analyses.
Sensitivity analysis
Sensitivity analysis was planned to determine the effect of removal of a single study on the results of a meta‐analysis when results of one study differed from other studies in the meta‐analysis. However there were insufficient studies of each intervention to allow sensitivity analysis.
'Summary of findings' tables
For this update we have presented the main results of the review in a 'Summary of findings' table/s. These tables present key information concerning the quality of the evidence, the magnitude of the effects of the interventions examined, and the sum of the available data for the main outcomes (Schunemann 2011a). The 'Summary of findings' table also include an overall grading of the evidence related to each of the main outcomes using the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) approach (GRADE 2008). The GRADE approach defines the quality of a body of evidence as the extent to which one can be confident that an estimate of effect or association is close to the true quantity of specific interest. The quality of a body of evidence involves consideration of within‐trial risk of bias (methodological quality), directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias (Schunemann 2011b). We have presented the following outcomes.
Complete remission
Partial remission
Complete or partial remission
Adverse events
Results
Description of studies
Results of the search
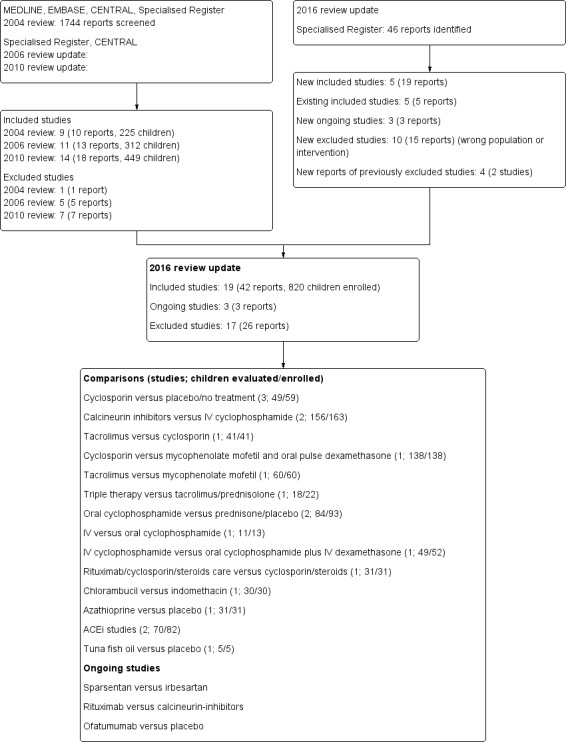
For the initial 2004 version of the review, of the 1744 titles and abstracts screened, 10 studies were identified; one study was excluded so nine studies (10 reports) were included in the review (Bagga 2004; Chongviriyaphan 1999; Elhence 1994; Garin 1988; ISKDC 1970; ISKDC 1974; ISKDC 1996; Lieberman 1996; Ponticelli 1993a). An update in 2006 identified four additional studies of which two were included (Kleinknecht 1980; Yi 2006) so the 2006 update included 11 studies (13 reports). A second update in 2010 identified three additional studies and the full publication of one study previously available as an abstract (Yi 2006). Therefore 14 studies (18 reports) were included in the 2010 update; 494 children entered the studies and 449 were evaluated.
A further search to March 2, 2016 identified 21 new studies, of which five were included (FSGS Study 2011; Gulati 2012; Magnasco 2012; Sinha 2015; Wu 2015). The 2016 update includes 19 studies (42 reports) comprising 820 children of whom 773 were evaluated (Figure 1). Although we were not able to obtain separate paediatric data from the authors, we chose to include FSGS Study 2011 because it was one of the largest studies looking at interventions for SRNS, 93 (67%) of participants were below 18 years of age and subgroup analyses by study authors showed no differences in outcomes between paediatric and adult participants. We also identified three ongoing studies. The first study is evaluating the safety and efficacy of sparsentan (a dual endothelin receptor) in a phase 2 study compared with irbesartan (an ARB) (NCT01613118). The second study is evaluating the 12 month relapse free survival in children with SRNS treated with rituximab or tacrolimus (NCT02382575). The third study is evaluating ofatumumab compared with placebo in children with steroid‐ and calcineurin‐inhibitor‐resistant nephrotic syndrome (NCT02394106).
Figure 1.
Flowchart of included and excluded studies
Included studies
Study characteristics are shown in Characteristics of included studies
Three studies compared cyclosporin with placebo or no treatment (49 children evaluated) (Garin 1988; Lieberman 1996; Ponticelli 1993a). Two studies (Garin 1988; Ponticelli 1993a) included children with MCD and FSGS while the third study (Lieberman 1996) included only children with FSGS. Lieberman 1996; Ponticelli 1993a included only children with initial steroid resistance.
Two studies compared oral CNI with IV cyclophosphamide. APN 2008 (32 children) compared oral cyclosporin with IV cyclophosphamide in children with initial steroid resistance. Gulati 2012 (131 children) compared oral tacrolimus with IV cyclophosphamide in children with initial and delayed steroid resistance. Both studies included children with MCD, FSGS and MesPGN.
Choudhry 2009 (41 children) compared oral cyclosporin with oral tacrolimus in children with initial or delayed steroid resistance. The study included children with MCD, FSGS and MesPGN.
FSGS Study 2011 (138 participants) compared cyclosporin with mycophenolate mofetil (MMF) and oral dexamethasone in children (93) and adults (45) with biopsy confirmed primary FSGS and initial steroid resistance. Separate paediatric data could not be obtained from the authors.
Wu 2015 (18/22 children evaluated) compared MMF, IV cyclophosphamide or leflunomide in three groups already receiving prednisone and tacrolimus. The study included children with MCD, FSGS, MesPGN and IgM nephropathy. The authors did not state whether the children had initial or delayed steroid resistance.
Sinha 2015 (60 children) compared tacrolimus with MMF to maintain remission in children with initial or delayed steroid resistance, who had achieved remission with tacrolimus. The study included children with MCD and FSGS.
Two studies (91/93 children evaluated) compared oral cyclophosphamide and prednisone with prednisone alone in children with initial steroid resistance (ISKDC 1974; ISKDC 1996). ISKDC 1974 included children with MCD, FSGS and MesPGN. ISKDC 1996 only included children with FSGS.
Two studies compared IV with oral cyclophosphamide in children with initial or delayed steroid resistance (Elhence 1994; Mantan 2008). In Mantan 2008 (49/51 children evaluated), IV dexamethasone was given to children in the oral cyclophosphamide group. Elhence 1994 (13 children) only included children with MCD while Mantan 2008 included children with MCD, FSGS and MesPGN.
Magnasco 2012 (31 children) compared rituximab and standard care (prednisolone and cyclosporin) with standard care alone in children with MCD, FSGS and unknown histology and with initial or delayed steroid resistance.
Kleinknecht 1980 (30 children) compared chlorambucil with indomethacin. This study did not report whether patients had initial or delayed steroid resistance. The study included children with MCD, FSGS and MesPGN.
ISKDC 1970 (31 children) compared azathioprine (AZA) and prednisone with placebo and prednisone in children with MCD, FSGS or MesPGN, who had initial steroid resistance.
Two studies evaluated ACEi. Bagga 2004 (25 children) compared different doses of the ACEi, enalapril in children with MCD, FSGS or MesPGN in a cross over study. Yi 2006 (45/55 children evaluated) compared the ACEi, fosinopril, and prednisone with prednisone alone. Both studies included children with initial and delayed steroid resistance.
Chongviriyaphan 1999 (5 children) compared fish oil with placebo in children with FSGS or MesPGN in a cross over study; the authors did not state whether the children had initial or delayed resistance.
No studies comparing high dose steroids alone with oral CNI or with other treatment regimens, placebo or no treatment were found.
Excluded studies
Seventeen studies (26 reports) were excluded.
Adeniyi 1979 was excluded because 31/36 included children had nephrotic syndrome considered secondary to Plasmodium malariae
Three studies were excluded because paediatric data could not be separated from adult data (Bhaumik 2002; Jung 1990; Shibasaki 2004)
Eight studies did not include children (Arora 2002; Koshikawa 1993; Kumar 2004a; Li 2006g; Ren 2011; Ren 2013; Saito 2014; Walker 1990a)
Two studies did not include children with nephrotic syndrome (Kano 2003) or included children with an ineligible renal pathology (Buyukcelik 2002)
Two studies evaluated interventions in children with SSNS (Hiraoka 2000; Iyengar 2006)
One study evaluated interventions in both children with steroid‐resistant and steroid‐dependent disease and the results could not be separated (Zhao 2013a).
Risk of bias in included studies
Figure 2.
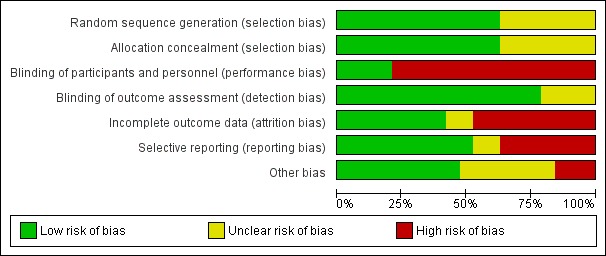
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
Figure 3.
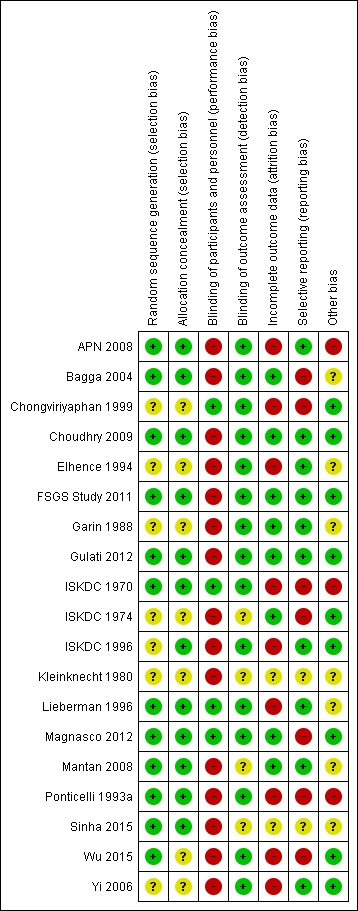
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Sequence generation was satisfactory in 12 studies (APN 2008; Bagga 2004; Choudhry 2009; FSGS Study 2011; Gulati 2012; ISKDC 1970; Lieberman 1996; Magnasco 2012; Mantan 2008; Ponticelli 1993a; Sinha 2015; Wu 2015) and unclear in the remaining seven studies.
Allocation concealment was adequate in 12 studies (APN 2008; Bagga 2004; Choudhry 2009; FSGS Study 2011; Gulati 2012; ISKDC 1970; ISKDC 1996; Lieberman 1996; Magnasco 2012; Mantan 2008; Ponticelli 1993a; Sinha 2015) and unclear in the remaining seven studies.
Blinding
Four studies reported that care givers (families, research staff) were blinded to treatment groups (Chongviriyaphan 1999; ISKDC 1970; Lieberman 1996; Magnasco 2012). In the remaining fifteen studies care givers were not blinded to treatment groups.
Fifteen studies were considered at low risk of detection bias as the outcome was laboratory‐based and unlikely to be influenced by blinding. In two studies (ISKDC 1974; Mantan 2008), outcome of proteinuria was measured on dipstick or in a laboratory and it was unclear in how many children the outcome was laboratory‐based. In two studies (Kleinknecht 1980; Sinha 2015), no information was provided on how the outcome was assessed.
Incomplete outcome data
Attrition bias was considered to be present if more than 10% of participants were excluded from analysis. Eight studies were considered to have provided complete outcome data (Bagga 2004; Choudhry 2009; FSGS Study 2011; Garin 1988; Gulati 2012; ISKDC 1974; Magnasco 2012; Mantan 2008). Nine studies did not provide complete outcome data. In the remaining two studies, available only as abstracts (Kleinknecht 1980; Sinha 2015), it was unclear whether complete outcome data was provided.
Selective reporting
Reporting bias was considered to be present if studies did not report on the number of patients with remission (complete or partial) and on adverse effects and if results of the primary outcome were not reported in a way that allowed inclusion of the data in meta‐analyses. Ten studies were considered to be free of selective reporting (APN 2008; Choudhry 2009; Elhence 1994; FSGS Study 2011; Garin 1988; Gulati 2012; ISKDC 1996; Lieberman 1996; Mantan 2008; Yi 2006). Seven studies were considered to have reported outcomes selectively or no results could be included in meta‐analyses (Bagga 2004; Chongviriyaphan 1999; ISKDC 1970; ISKDC 1974; Magnasco 2012; Ponticelli 1993a; Wu 2015) as results for adverse events were either not reported or incompletely reported. In the remaining two studies (Kleinknecht 1980; Sinha 2015) available only as abstracts, it was unclear whether there was selective reporting of outcomes.
Other potential sources of bias
Nine studies reported funding by university or government agencies and were considered free of other potential sources of bias (Chongviriyaphan 1999; Choudhry 2009; FSGS Study 2011; Gulati 2012; ISKDC 1974; ISKDC 1996; Magnasco 2012; Yi 2006; Wu 2015). Three studies reported funding from pharmaceutical companies and were considered at risk of potential bias (APN 2008; ISKDC 1970; Ponticelli 1993a). Other potential sources of bias were unclear in the remaining seven studies as none reported on support.
The definition of steroid resistance varied between studies.
Eight studies defined steroid resistance as persistent proteinuria of > 4 mg/m2/h or UP/C > 1g/g after four weeks (FSGS Study 2011; Lieberman 1996; Wu 2015), five weeks (Kleinknecht 1980), six weeks (APN 2008) or eight weeks of prednisone (Bagga 2004; ISKDC 1970; ISKDC 1974).
Eight studies defined steroid resistance as persistent proteinuria > 40 mg/m2/h, > 2g/g or above 1 g/m2/d after four weeks (Choudhry 2009; Gulati 2012; Mantan 2008; Sinha 2015), five weeks (Ponticelli 1993a), eight weeks (Garin 1988; ISKDC 1996) or six months (Magnasco 2012) of prednisone.
One study defined steroid resistance as no response after eight weeks of prednisone (Yi 2006) but did not define the degree of proteinuria.
Two studies did not define steroid resistance (Chongviriyaphan 1999; Elhence 1994).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4
Cyclosporin versus placebo/no specific treatment
Remission
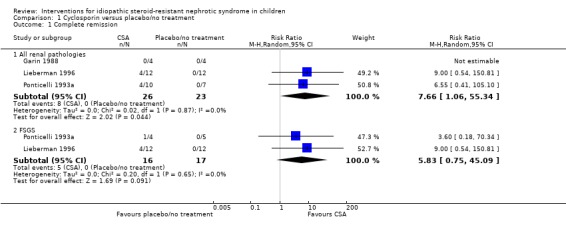
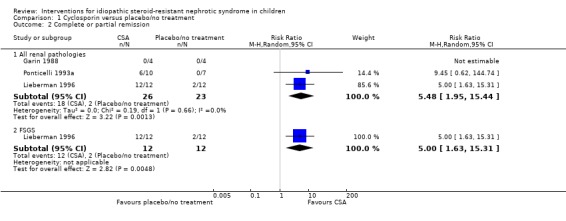
Cyclosporin significantly increased the number of children with SRNS who achieved complete remission compared with placebo or no treatment, irrespective of renal pathology (Analysis 1.1.1 (3 studies, 49 children): RR 7.66, 95% CI 1.06 to 55.34; I2 = 0%). The number who achieved complete or partial remission also was significantly increased with cyclosporin (Analysis 1.2.1 (3 studies, 49 children): RR 5.48, 95% CI 1.95 to 15.44; I2 = 0%).
Analysis 1.1.
Comparison 1 Cyclosporin versus placebo/no treatment, Outcome 1 Complete remission.
Analysis 1.2.
Comparison 1 Cyclosporin versus placebo/no treatment, Outcome 2 Complete or partial remission.
When treatment with cyclosporin was compared with placebo/no treatment in the subgroup of children with FSGS, the summary estimate (Analysis 1.1.2 (2 studies, 33 children): RR 5.83, 95% CI 0.75 to 45.09; I2 = 0%) was similar to that for the analysis for all renal pathologies (Analysis 1.1.1). Although the 95% CI crossed '1', a significant benefit of cyclosporin on complete remission in FSGS cannot be excluded because of the imprecision resulting from small patient numbers. In addition children treated with cyclosporin achieved complete or partial remission (Analysis 1.2.2 (1 study, 24 children): RR 5.00, 95% CI 1.63 to 15.31) significantly more frequently than children treated with placebo or no treatment. Relapse was reported in 2/6 children, who achieved partial or complete remission, by the end of 12 months of cyclosporin treatment (Ponticelli 1993a). Subgroup analysis, other than for renal pathology, was not possible because of small patient numbers.
Adverse events
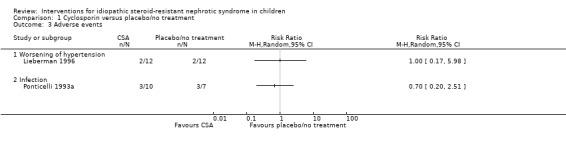
Lieberman 1996 reported no statistically significant difference in the number of children with worsening hypertension (Analysis 1.3.1 (1 study, 24 children): RR 1.00, 95% CI 0.17 to 5.98), and Ponticelli 1993a reported no statistically significant difference in the number of children with bacterial infections (Analysis 1.3.2 (1 study, 17 children): RR 0.70, 95% CI 0.20 to 2.51). However small numbers of events resulted in imprecision in the results so that it remains uncertain whether whether cyclosporin therapy is associated with any differences in adverse effects compared with placebo/no treatment. The Ponticelli 1993a study did not report adverse events (except bacterial infections) separately in children and adults. In the cross‐over study by Garin 1988, no child was reported to develop hypertension in either the cyclosporin or control group while one child developed kidney dysfunction while receiving cyclosporin and two developed kidney dysfunction while in the control group.
Analysis 1.3.
Comparison 1 Cyclosporin versus placebo/no treatment, Outcome 3 Adverse events.
Calcineurin inhibitors versus intravenous cyclophosphamide
Remission by three to six months
CNI significantly increased the number of children who achieved complete or partial remission (Analysis 2.1.1(2 studies, 156 children): RR 1.98, 95% CI 1.25 to 3.13; I2 = 20%) or complete remission (Analysis 2.1.2 (2 studies, 156 children): RR 3.43, 95% CI 1.84 to 6.41; I2 = 0%) compared with intravenous cyclophosphamide. While there was no statistically significant difference between treatment groups in the numbers achieving partial remission (Analysis 2.1.3 (2 studies, 156 children): RR 1.68, 95% CI 0.43 to 6.56; I2 = 71%), there was significant heterogeneity between the two studies leading to imprecision in the results so it is uncertain whether the intervention had any effect on the number of participants achieving partial remission.
Analysis 2.1.

Comparison 2 Calcineurin inhibitor versus IV cyclophosphamide, Outcome 1 Treatment response at 3 to 6 months.
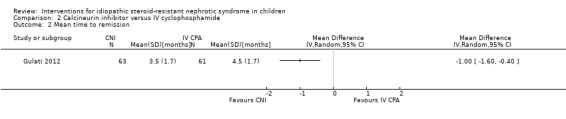
Gulati 2012 reported the mean time to remission was significantly shorter with tacrolimus compared with cyclophosphamide (Analysis 2.2 (1 study, 124 children): MD ‐1.00 months, 95% CI ‐1.60 to ‐0.40). The likelihood of complete or partial remission was significantly higher with tacrolimus within subgroups of initial steroid resistance (HR 2.78, 95% CI 1.54 to 5.03), delayed steroid resistance (HR 2.35; 95% CI 1.11 to 4.97), MCD (HR 2.37, 95% CI 1.32 to 4.23) and FSGS (HR 2.54, 95% CI 1.09 to 4.23). Within the tacrolimus treated subgroups, Gulati 2012 found no difference in efficacy based on pathology or whether children had initial or delayed steroid resistance.
Analysis 2.2.
Comparison 2 Calcineurin inhibitor versus IV cyclophosphamide, Outcome 2 Mean time to remission.
Outcomes at 12 months in children who achieved complete or partial remission
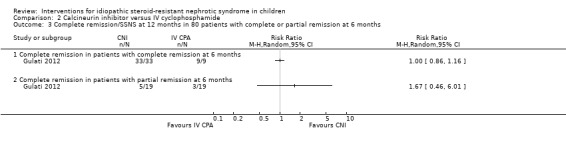
In Gulati 2012, 42 children achieved complete remission by six months and all maintained remission or developed SSNS with no significant difference between the treatment groups (Analysis 2.3.1 (1 study, 42 children): RR 1.00, 95% CI 0.86 to 1.16). Among 38 children who achieved partial remission by six months there was no statistically significant difference between the treatment groups in the numbers who subsequently achieved complete remission (Analysis 2.3.2 (1 study, 38 children): RR 1.67, 95% CI 0.46 to 6.01), non‐nephrotic proteinuria (Analysis 2.4.1 (1 study, 38 children): RR 1.00, 95% CI 0.58 to 1.72) or recurrence of steroid resistance (Analysis 2.4.2 (1 study, 38 children): RR 0.14, 95% CI 0.01 to 2.59). However because of small patient numbers and imprecision of results with wide CI, it remains uncertain whether tacrolimus or cyclophosphamide could have differential effects on these outcomes.
Analysis 2.3.
Comparison 2 Calcineurin inhibitor versus IV cyclophosphamide, Outcome 3 Complete remission/SSNS at 12 months in 80 patients with complete or partial remission at 6 months.
Analysis 2.4.
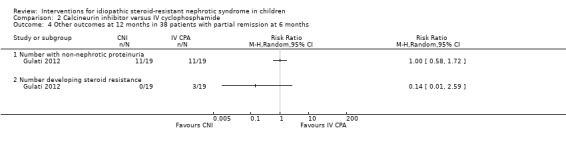
Comparison 2 Calcineurin inhibitor versus IV cyclophosphamide, Outcome 4 Other outcomes at 12 months in 38 patients with partial remission at 6 months.
Adverse effects
Gulati 2012 reported treatment failure (non‐response at 6 months, > 1 episode of serious infection requiring hospitalisation or declining GFR) (Analysis 2.5.1 (1 study, 124 children): RR 0.32, 95% CI 0.18 to 0.58), any serious adverse event (Analysis 2.5.2 (1 study, 131 children): RR 0.47, 95% CI 0.23 to 0.95) and the need to cease medications (Analysis 2.5.3 (1 study, 131 children): RR 0.20, 95% CI 0.04 to 0.86) were significantly more common in children treated with cyclophosphamide compared with tacrolimus. There were no significant differences between treatment groups in serious infections (Analysis 2.5.4 (1 study, 131 children): RR 0.49, 95% CI 0.16 to 1.56), persistent nephrotoxicity (Analysis 2.5.5 (131 children): RR 4.93, 95% CI 0.24 to 100.65) or deaths (Analysis 2.5.6 (1 study, 131 children): RR 0.33, 95% CI 0.01 to 7.92). Although there was no statistically significant difference between the groups for the outcomes of persistent nephrotoxicity and death, the CI were wide with the limits indicating imprecision of results so it remains uncertain whether there are differences in adverse effects between the interventions.
Analysis 2.5.
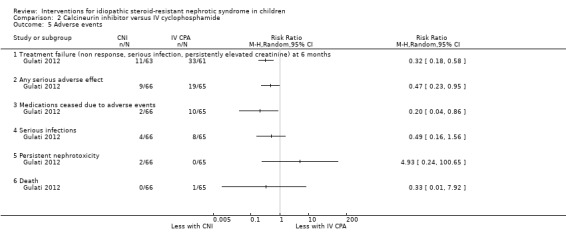
Comparison 2 Calcineurin inhibitor versus IV cyclophosphamide, Outcome 5 Adverse events.
Tacrolimus versus cyclosporin
Remission
At six months Choudhry 2009 found no significant differences between tacrolimus and cyclosporin treatment in the numbers of children who achieved complete remission (Analysis 3.1.1 (1 study, 41 children): RR 0.86, 95% CI 0.44 to 1.66), achieved partial remission (Analysis 3.1.2 (1 study, 41 children): RR 1.43, 95% CI 0.62 to 3.28), or achieved complete or partial remission (Analysis 3.1.3 (1 study, 41 children): RR 1.07, 95% CI 0.81 to 1.42) in children with initial or delayed steroid resistance. There were no significant differences in these outcomes at 12 months (Analysis 3.2). However
Analysis 3.1.
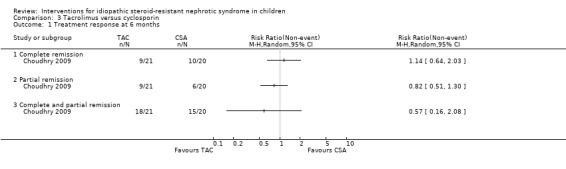
Comparison 3 Tacrolimus versus cyclosporin, Outcome 1 Treatment response at 6 months.
Analysis 3.2.
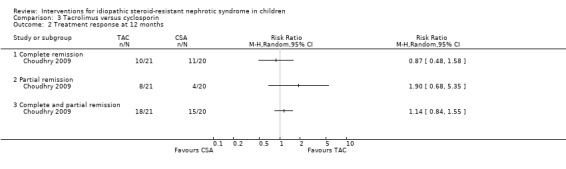
Comparison 3 Tacrolimus versus cyclosporin, Outcome 2 Treatment response at 12 months.
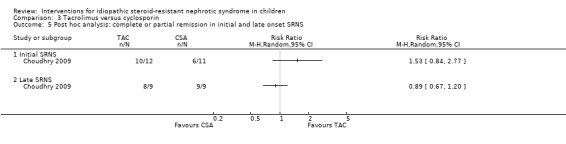
Significantly fewer children relapsed following treatment with tacrolimus compared with cyclosporin (Analysis 3.3 (1 study, 34 children): RR 0.22, 95% CI 0.06 to 0.90). In a post hoc analysis there were no significant differences between tacrolimus and cyclosporin therapy in the numbers of children with initial non‐response and late non‐response to steroids, who achieved complete remission (Analysis 3.4) or complete or partial remission (Analysis 3.5).
Analysis 3.3.
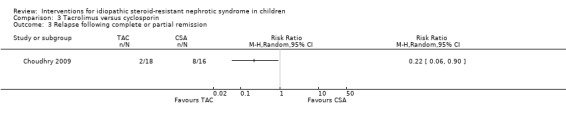
Comparison 3 Tacrolimus versus cyclosporin, Outcome 3 Relapse following complete or partial remission.
Analysis 3.4.

Comparison 3 Tacrolimus versus cyclosporin, Outcome 4 Post hoc analysis: complete remission in initial and late onset SRNS.
Analysis 3.5.
Comparison 3 Tacrolimus versus cyclosporin, Outcome 5 Post hoc analysis: complete or partial remission in initial and late onset SRNS.
Adverse events
Choudhry 2009 found no significant difference between medications in change in GFR (Analysis 3.6 (1 study, 41 children): MD ‐0.70 mL/min, 95% CI ‐16.71 to 15.31). Hypertrichosis (Analysis 3.7.6 (1 study, 41 children): RR 0.02, 95% CI 0.00 to 0.38) and gingival hypertrophy (Analysis 3.7.7 (1 study, 41 children): RR 0.08, 95% CI 0.01 to 0.56) were significantly less common with tacrolimus compared with cyclosporin. Diarrhoea was more common with tacrolimus (Analysis 3.7.9 (1 study, 41 children): RR 5.71, 95% CI 0.75 to 43.36) however this result was not statistically significant. Other reported adverse events including persistent and reversible nephrotoxicity and worsening of hypertension did not differ significantly between treatments (Analysis 3.7). However the wide CI indicate imprecision of results so it remains unclear whether there are differences in adverse effects between interventions. No children with new‐onset hypertension were reported.
Analysis 3.6.

Comparison 3 Tacrolimus versus cyclosporin, Outcome 6 Change in eGFR over 12 months.
Analysis 3.7.

Comparison 3 Tacrolimus versus cyclosporin, Outcome 7 Adverse events.
Cyclosporin versus mycophenolate mofetil plus pulse oral dexamethasone
Remission
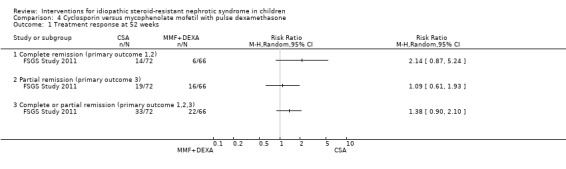
FSGS Study 2011 found no statistically significant differences between therapies in complete remission (Analysis 4.1.1 (1 study, 138 children): RR 2.14, 95% CI 0.87 to 5.24), partial remission (Analysis 4.1.2 (1 study, 138 children): RR 1.09, 95% CI 0.61 to 1.93), or complete or partial remission (Analysis 4.1.3 (1 study, 138 children): RR 1.38, 95% CI 0.90 to 2.10).
Analysis 4.1.
Comparison 4 Cyclosporin versus mycophenolate mofetil with pulse dexamethasone, Outcome 1 Treatment response at 52 weeks.
FSGS Study 2011 found no statistically significant differences between therapies for sustainable remission of proteinuria between 52 and 78 weeks in numbers with complete remission (Analysis 4.2.1 (1 study, 138 children): RR 1.38, 95% CI 0.41 to 4.66), partial remission (Analysis 4.2.2 (1 study, 138 children): RR 1.05, 95% CI 0.56 to 1.98), or no sustainable remission (Analysis 4.2.3 (1 study, 138 children): RR 0.95, 95% CI 0.77 to 1.18).
Analysis 4.2.

Comparison 4 Cyclosporin versus mycophenolate mofetil with pulse dexamethasone, Outcome 2 Sustainable remission between 52 and 78 weeks.
Adverse events
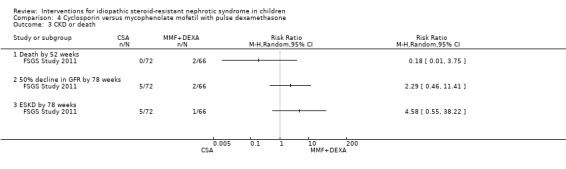
FSGS Study 2011 found no significant differences between therapies for death, 50% decline in GFR, or development of ESKD (Analysis 4.3). Adverse effects were reported for 0 to 26 weeks as all children were included up to that time. No significant differences between therapies were detected for serious infection requiring hospitalisation, total infections, total hospitalisations, gastrointestinal adverse effects, neuropsychiatric conditions, or hypertension (Analysis 4.4).
Analysis 4.3.
Comparison 4 Cyclosporin versus mycophenolate mofetil with pulse dexamethasone, Outcome 3 CKD or death.
Analysis 4.4.
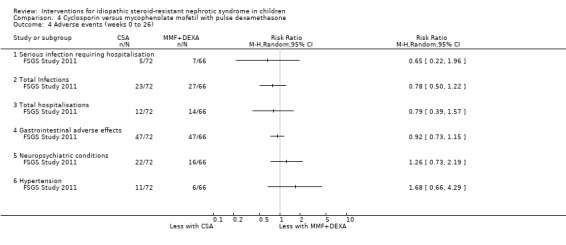
Comparison 4 Cyclosporin versus mycophenolate mofetil with pulse dexamethasone, Outcome 4 Adverse events (weeks 0 to 26).
While no significant differences were identified for the outcomes of remission and adverse events, the CI was wide, with the limits indicating the possibility of benefit or harm from cyclosporin compared with MMF with dexamethasone. The results are therefore imprecise, and results of future trials could change these estimates.
Triple therapy using different agents combined with tacrolimus and prednisone
Wu 2015 found no statistically significant differences in short term (complete remission) and long term responses (complete remission at 12 months) to cyclophosphamide, MMF or leflunomide combined with tacrolimus and prednisone between medications (Analysis 5.1; Analysis 5.2). However because of small numbers of patients and events, it remains uncertain whether any differences in efficacy exist between the interventions.
Analysis 5.1.
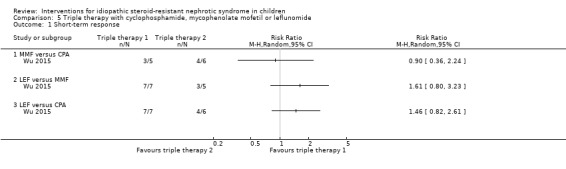
Comparison 5 Triple therapy with cyclophosphamide, mycophenolate mofetil or leflunomide, Outcome 1 Short‐term response.
Analysis 5.2.
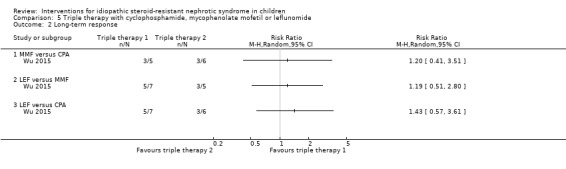
Comparison 5 Triple therapy with cyclophosphamide, mycophenolate mofetil or leflunomide, Outcome 2 Long‐term response.
Adverse effects were poorly reported but did not differ between groups.
Tacrolimus versus mycophenolate mofetil to maintain remission
Remission
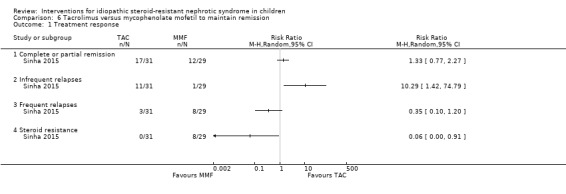
Sinha 2015 found no significant differences in the number with complete or partial remission (Analysis 6.1.1: (60 children): RR 1.33, 95% CI 0.77 to 2.27) or frequent relapses (Analysis 6.1.3 (60 children): RR 0.35, 95% CI 0.10 to 1.20). Infrequent relapses (Analysis 6.1.2 (60 children): RR 10.29, 95% CI 1.42 to 74.79) and steroid resistance (Analysis 6.1.4 (60 children): RR 0.06, 95% CI 0.00 to 0.91) were significantly fewer with tacrolimus. The authors concluded that 28/31 (90%) children treated with tacrolimus maintained remission satisfactorily (complete/partial remission or infrequent relapses) while 13/29 (48%) children treated with MMF maintained remission satisfactorily.
Analysis 6.1.
Comparison 6 Tacrolimus versus mycophenolate mofetil to maintain remission, Outcome 1 Treatment response.
The mean relapse rate/year did not differ significantly between therapies (Analysis 6.2 (60 children): MD ‐0.50 N/y, 95% CI ‐1.09 to 0.09).
Analysis 6.2.
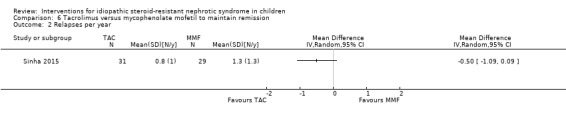
Comparison 6 Tacrolimus versus mycophenolate mofetil to maintain remission, Outcome 2 Relapses per year.
Adverse events
Sinha 2015 reported the mean prednisone dose was significantly lower in the tacrolimus group compared to MMF (Analysis 6.3 (60 children): MD ‐0.20 mg/d, 95% CI ‐0.36 to ‐0.04). There was no significant difference in change in GFR (Analysis 6.4 (60 children): MD 13.00 mL/min, 95% CI ‐3.71 to 29.71) between the tacrolimus and MMF treated children though the wide CI indicate that it remains uncertain whether change in GFR differs between treatment groups.
Analysis 6.3.
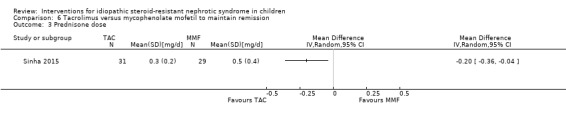
Comparison 6 Tacrolimus versus mycophenolate mofetil to maintain remission, Outcome 3 Prednisone dose.
Analysis 6.4.

Comparison 6 Tacrolimus versus mycophenolate mofetil to maintain remission, Outcome 4 Change in GFR.
Cyclophosphamide versus prednisone/placebo
Remission
There was no significant difference in the overall number of children (Analysis 7.1.1 (2 studies, 84 children): RR 1.06, 95% CI 0.61 to 1.87) or in those with FSGS (Analysis 7.1.2 (2 studies, 63 children): RR 1.01, 95% CI 0.43 to 2.37) who achieved complete remission after treatment with oral cyclophosphamide and prednisone compared with prednisone alone.
Analysis 7.1.
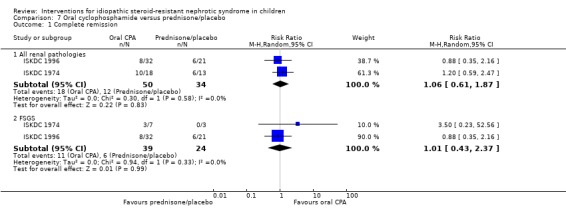
Comparison 7 Oral cyclophosphamide versus prednisone/placebo, Outcome 1 Complete remission.
ISKDC 1996 reported the number of children who achieved complete or partial remission did not differ significantly between treatment groups (Analysis 7.2 (1 study, 53 children): RR 0.88, 95% CI 0.53 to 1.45). Subgroup analysis, other than for renal pathology, was not possible because of small patient numbers.
Analysis 7.2.

Comparison 7 Oral cyclophosphamide versus prednisone/placebo, Outcome 2 Complete or partial remission.
ISKDC 1996 reported treatment failure (increase in SCr by ≥ 30%, SCr > 4 mg/dL, dialysis, or transplant) occurred in 36% (9/25) of the control group and 57% (20/35) of the treatment group (Analysis 7.3 (1 study, 60 children); RR 1.59, 95% CI 0.87 to 2.88).
Analysis 7.3.
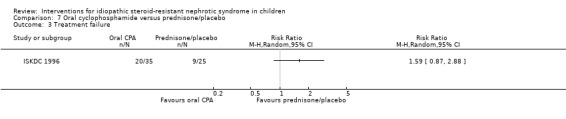
Comparison 7 Oral cyclophosphamide versus prednisone/placebo, Outcome 3 Treatment failure.
Adverse events
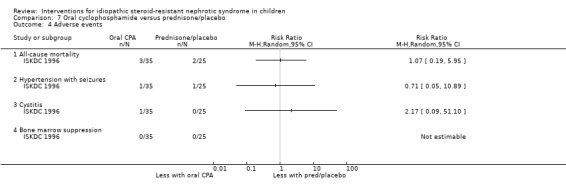
The number of children who had hypertension with seizures, cystitis or bone marrow suppression did not differ between the treatment groups (Analysis 7.4).Three children treated with cyclophosphamide and two with prednisone died (ISKDC 1996) (Analysis 7.4.1 (1 study, 60 children): RR 1.07, 95% CI 0.19 to 5.95). Deaths were related to sepsis, cardiorespiratory arrest and unknown factors. Adverse events in ISKDC 1974 were not reported separately for steroid‐sensitive and steroid‐resistant children.
Analysis 7.4.
Comparison 7 Oral cyclophosphamide versus prednisone/placebo, Outcome 4 Adverse events.
Intravenous versus oral cyclophosphamide
Remission
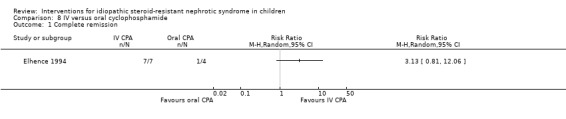
Elhence 1994 found no significant difference in the numbers of children achieving remission (Analysis 8.1.1 (1 study, 11 children): RR 3.13, 95% CI 0.81 to 12.06); small patient numbers resulted in wide CI so it remains uncertain whether any difference in efficacy exists. Two children treated with IV cyclophosphamide subsequently relapsed at 12 months.
Analysis 8.1.
Comparison 8 IV versus oral cyclophosphamide, Outcome 1 Complete remission.
Adverse events
Elhence 1994 reported vomiting was significantly more common in children treated with IV cyclophosphamide (Analysis 8.2.1 (1 study, 11 children): RR 5.63, 95% CI 0.38 to 83.67) but the numbers with bacterial infections (Analysis 8.2.2 (1 study, 11 children): RD ‐0.25, 95% CI ‐0.69 to 0.19) did not differ between treatment groups.
Analysis 8.2.

Comparison 8 IV versus oral cyclophosphamide, Outcome 2 Adverse events.
IV cyclophosphamide versus oral cyclophosphamide plus IV dexamethasone
Remission
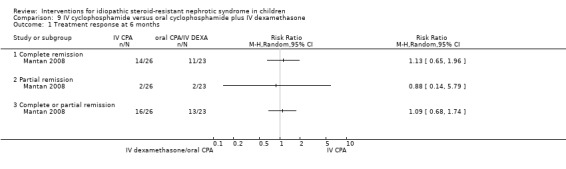
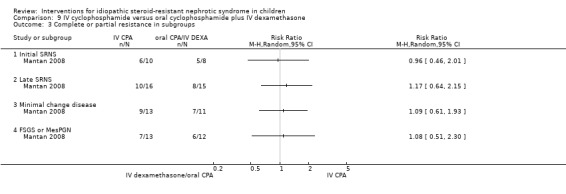
Mantan 2008 found no significant differences in the number of children with initial or delayed steroid resistance who achieved complete remission (Analysis 9.1.1 (1 study, 49 children): RR 1.13, 95% CI 0.65 to 1.96), partial remission (Analysis 9.1.2 (1 study, 49 children): RR 0.88, 95% CI 0.14 to 5.79), or complete or partial remission (Analysis 9.1.3 (1 study, 49 children): RR 1.09, 95% CI 0.68 to 1.74) after six months of treatment.
Analysis 9.1.
Comparison 9 IV cyclophosphamide versus oral cyclophosphamide plus IV dexamethasone, Outcome 1 Treatment response at 6 months.
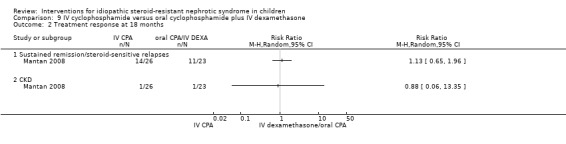
There were no significant differences in the number of children who had sustained remission or steroid‐sensitive relapses after 18 months of follow‐up (Analysis 9.2.1 (1 study, 49 children): RR 1.13, 95% CI 0.65 to 1.96). Chronic kidney disease developed in one patient in each treatment group during 18 months of follow‐up (Analysis 9.2.2 (1 study, 49 children): RR 0.88, 95% CI 0.06 to 13.35).
Analysis 9.2.
Comparison 9 IV cyclophosphamide versus oral cyclophosphamide plus IV dexamethasone, Outcome 2 Treatment response at 18 months.
There was no significant difference between treatments in the numbers who achieved complete or partial remission among children with initial SRNS (Analysis 9.3.1 (1 study, 18 children): RR 0.96, 95% CI 0.46 to 2.01) or late SRNS (Analysis 9.3.2 (1 study, 31 children): RR 1.17, 95% CI 0.64 to 2.15) though CI were wide due to small patient numbers indicating uncertainty as to whether differences exist between interventions. Similarly there was no significant differences between treatments in the numbers, who achieved complete or partial remission, among children with MCD (Analysis 9.3.3 (1 study, 24 children): RR 1.09, 95% CI 0.61 to 1.93) or among children with FSGS or MesPGN (Analysis 9.3.4 (1 study, 25 children): RR 1.08, 95% CI 0.51 to 2.30).
Analysis 9.3.
Comparison 9 IV cyclophosphamide versus oral cyclophosphamide plus IV dexamethasone, Outcome 3 Complete or partial resistance in subgroups.
Adverse events
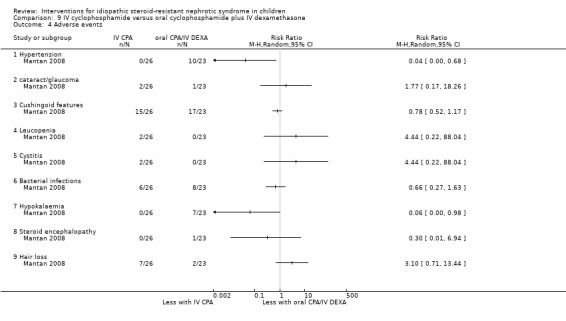
Mantan 2008 reported hypertension (Analysis 9.4.1 (1 study, 49 children): RR 0.04, 95% CI 0.00, 0.68) and hypokalaemia (Analysis 9.4.7 (1 study, 49 children): RR 0.06, 95% CI 0.00, 0.98) were significantly less common in children treated with IV cyclophosphamide. The other reported adverse events (cataracts/glaucoma, leucopenia, cushingoid features, cystitis, bacterial infections, steroid encephalopathy, hair loss) were not significantly different between treatment groups (Analysis 9.4).
Analysis 9.4.
Comparison 9 IV cyclophosphamide versus oral cyclophosphamide plus IV dexamethasone, Outcome 4 Adverse events.
Rituximab/cyclosporin/prednisolone versus cyclosporin/prednisolone
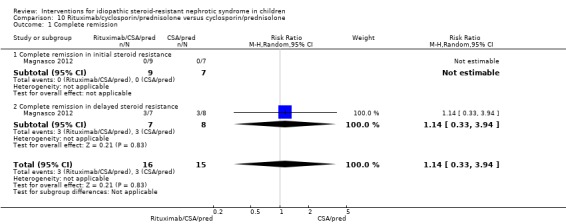
Magnasco 2012 reported no significant differences in the percentage reduction in proteinuria at three months (‐12; 95% CI ‐73 to 110) between treatment groups overall or among children with initial SRNS (‐3, 95% CI ‐6.7 to 179) or among children with delayed steroid resistance (‐48. 95% CI ‐79 to 93). There were no significant differences between treatment groups in the number of children, who achieved remission; remission was only seen in children with delayed steroid resistance (Analysis 10.1.2 (1 study, 15 children): RR 1.14, 95% CI 0.33 to 3.94), though event numbers were small indicating imprecision so it remains uncertain rituximab influences remission in children with delayed steroid resistance.
Analysis 10.1.
Comparison 10 Rituximab/cyclosporin/prednisolone versus cyclosporin/prednisolone, Outcome 1 Complete remission.
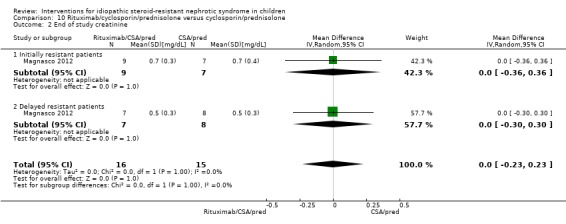
There were no significant differences between end of study creatinine (Analysis 10.2 (1 study, 31 participants): MD 0.00 mg/dL, 95% CI ‐0.23 to 0.23) and albumin levels (Analysis 10.3 (1 study, 31 participants): MD 0.25 g/L, 95% CI ‐0.22 to 0.72).
Analysis 10.2.
Comparison 10 Rituximab/cyclosporin/prednisolone versus cyclosporin/prednisolone, Outcome 2 End of study creatinine.
Analysis 10.3.

Comparison 10 Rituximab/cyclosporin/prednisolone versus cyclosporin/prednisolone, Outcome 3 End of study serum albumin.
Only adverse reactions related to rituximab were reported (abdominal pain; bronchospasm resulting in discontinuation of treatment; hypotension; skin rash; mild dyspnoea). There were no significant differences between the two treatment groups (Analysis 10.4).
Analysis 10.4.
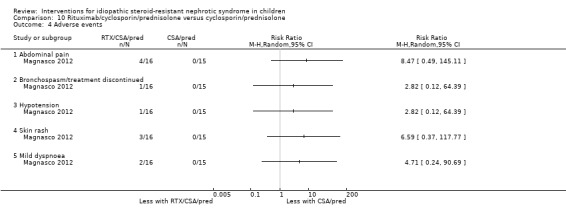
Comparison 10 Rituximab/cyclosporin/prednisolone versus cyclosporin/prednisolone, Outcome 4 Adverse events.
Chlorambucil versus indomethacin
Remission
Kleinknecht 1980 reported no significant difference between chlorambucil and indomethacin in the number who achieved complete remission (Analysis 11.1 (1 study; 30 children): RR 1.00, 95% CI 0.42 to 2.40) and in the number reaching ESKD (Analysis 11.2 (1 study, 30 children): RR 0.20, 95% CI 0.01 to 3.85).
Analysis 11.1.

Comparison 11 Chlorambucil versus indomethacin, Outcome 1 Complete remission.
Analysis 11.2.
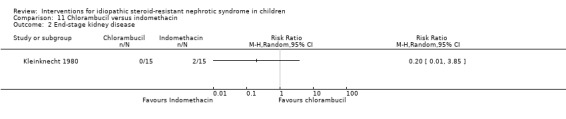
Comparison 11 Chlorambucil versus indomethacin, Outcome 2 End‐stage kidney disease.
Adverse events
Adverse events of chlorambucil or indomethacin were not reported.
Azathioprine versus placebo
Remission
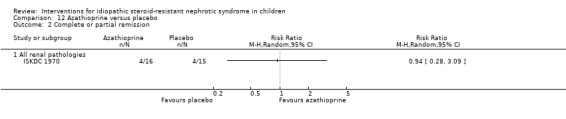
ISKDC 1970 reported no significant difference in the number of children who achieved complete remission (Analysis 12.1.1 (1 study, 31 children): RR 0.94, 95% CI 0.15 to 5.84) or complete or partial remission (Analysis 12.2.1 (1 study, 31 children): RR 0.94, 95% CI 0.28 to 3.09) after treatment with azathioprine and prednisone compared with placebo and prednisone.
Analysis 12.1.

Comparison 12 Azathioprine versus placebo, Outcome 1 Complete remission.
Analysis 12.2.
Comparison 12 Azathioprine versus placebo, Outcome 2 Complete or partial remission.
Adverse events
Adverse events of azathioprine were not reported.
High versus low dose enalapril
Bagga 2004 reported that low dose enalapril (0.2 mg/kg/d) reduced median urinary albumin/creatinine ratio from 3.9 (5th to 95th percentiles 1.9 to 11.6) to 2.3 (5th to 95th percentiles 0.8 to 5.2) but the difference was not significant. High dose enalapril (0.6 mg/kg/d) reduced median urinary albumin/creatinine ratio significantly from 5.2 (5th to 95th percentiles 2.1 to 10.5) to 2.5 (5th to 95th percentiles 0.8 to 3.3). In addition, the urinary albumin/creatinine reduction between the beginning and end of treatment was significantly lower with low dose enalapril (median 34.8, 95% CI ‐7.9 to 76.6) compared with high dose enalapril (median 62.9, 95% CI 40.6 to 71.6). These results were not able to be meta‐analysed.
SCr and potassium levels were unchanged by enalapril. Three children ceased enalapril because of a dry cough.
Fosinopril plus prednisone versus prednisone alone
Yi 2006 reported that fosinopril plus prednisone significantly reduced the 24 hour urinary protein excretion after four (Analysis 13.1.1 (1 study, 45 children): MD ‐1.27 g/d, 95% CI ‐1.62 to ‐0.92), eight (Analysis 13.1.2 (1 study, 45 children): MD ‐1.26 g/d, 95% CI ‐1.47 to ‐1.05) and 12 weeks of treatment (Analysis 13.1.3 (1 study, 45 children): MD ‐0.95 g/d, 95% CI ‐1.21 to ‐0.69) compared with prednisone alone. In addition, there were significant reductions in the tubular proteins, retinol binding protein (Analysis 13.2.1 (1 study, 45 children): MD ‐0.21 mg/L, 95% CI ‐0.33 to ‐0.09) and beta‐2 microglobulin (Analysis 13.2.2 (1 study, 45 children): MD ‐0.17 mg/L, 95% CI ‐0.27 to ‐0.07). Serum albumin at the end of the study did not differ significantly between the groups (Analysis 13.3 (1 study, 45 children): MD 1.20 g/L, 95% CI ‐6.58 to 8.98).
Analysis 13.1.

Comparison 13 Fosinopril plus prednisone versus prednisone alone, Outcome 1 Proteinuria.
Analysis 13.2.
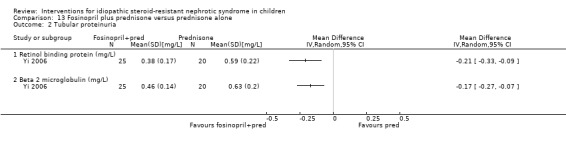
Comparison 13 Fosinopril plus prednisone versus prednisone alone, Outcome 2 Tubular proteinuria.
Analysis 13.3.
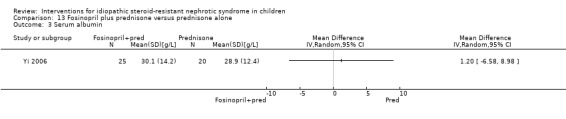
Comparison 13 Fosinopril plus prednisone versus prednisone alone, Outcome 3 Serum albumin.
No changes were reported in systolic blood pressure (Analysis 13.4 (1 study, 45 children): MD ‐0.87 mm Hg, 95% CI ‐3.33 to 1.59), CrCl (Analysis 13.5 (1 study, 45 children): MD ‐5.28 mL/min, 95% CI ‐9.66 to ‐0.90) or serum potassium (Analysis 13.6 (1 study, 45 children): MD 0.20 mmol/L, 95% CI ‐0.34 to 0.74).
Analysis 13.4.
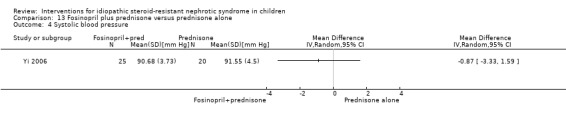
Comparison 13 Fosinopril plus prednisone versus prednisone alone, Outcome 4 Systolic blood pressure.
Analysis 13.5.

Comparison 13 Fosinopril plus prednisone versus prednisone alone, Outcome 5 Creatinine clearance.
Analysis 13.6.
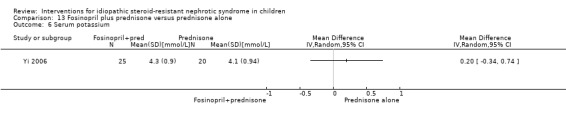
Comparison 13 Fosinopril plus prednisone versus prednisone alone, Outcome 6 Serum potassium.
Tuna fish oil versus placebo
In one small cross‐over study involving five children, there was no significant change in the degree of proteinuria or in CrCl after fish oil compared with placebo (Chongviriyaphan 1999). The results from each part of the cross‐over study were combined so that the RR and 95% CI could not be calculated.
Adverse events were not reported.
Discussion
Summary of main results
In this update we have now included 19 studies, enrolling 820 children of which 773 were evaluated.
Three studies examined the efficacy of CNI compared with placebo or supportive treatment. A meta‐analysis of three small studies (Garin 1988; Lieberman 1996; Ponticelli 1993a) showed that cyclosporin increased the number of children with SRNS, who achieved complete or partial remission. However this result was based on only 8/26 children, who achieved remission with cyclosporin compared with 0/23 children who achieved remission with placebo/no treatment. Nevertheless these data support previously published data from a large case series of 65 children with initial non‐response to steroids in which 46% of children with MCD (21/45) and 30% with FSGS (6/20) achieved complete remission with cyclosporin (Niaudet 1994). There were no data presented in these studies on the effect of cyclosporin on long term kidney function.
Two studies found no statistically significant differences in remission rates or prevention of kidney function deterioration with oral cyclophosphamide compared with prednisone alone (ISKDC 1974; ISKDC 1996). In addition children treated with oral CNI were significantly more likely to achieve complete or partial remission compared with IV cyclophosphamide (APN 2008; Gulati 2012). Choudhry 2009 found no significant differences in efficacy between tacrolimus and cyclosporin though the important cosmetic adverse effects of hirsutism and gum hypertrophy were limited to cyclosporin therapy. FSGS Study 2011 found no significant differences in efficacy between cyclosporin and mycophenolate mofetil with dexamethasone in children and young adults with primary FSGS. Among children, who achieved remission with tacrolimus, Sinha 2015 found that satisfactory remission (complete or partial remission and infrequent relapses) occurred more commonly with tacrolimus than mycophenolate mofetil.
These data suggest that CNI should be used in preference to cyclophosphamide in children with SRNS. Further studies are required to determine the relative efficacies of CNI and mycophenolate mofetil.
In the remaining studies of immunosuppressive agents, two studies (Elhence 1994; Mantan 2008) compared IV with oral cyclophosphamide and found no significant differences in efficacy between treatment groups. Single studies of azathioprine (ISKDC 1970) or tuna fish oil (Chongviriyaphan 1999) showed no evidence of benefit. Kleinknecht 1980 found no significant differences between chlorambucil and indomethacin in the number who achieved remission or developed ESKD. Wu 2015 found no significant differences in efficacy between mycophenolate mofetil, cyclophosphamide or leflunomide in children already treated with tacrolimus and prednisone. Magnasco 2012 found no significant benefit of rituximab over CNI with prednisone in children with SRNS, who were resistant to corticosteroids and CNI.
Two studies (Bagga 2004; Yi 2006) found that the ACEi, enalapril and fosinopril reduced proteinuria significantly in children with SRNS. However the studies were too short to provide data on whether ACE inhibition provides long term reduction in proteinuria and protects against deterioration in kidney function.
Overall completeness and applicability of evidence
Currently CNI, cyclophosphamide and mycophenolate mofetil are used to treat SRNS. There are limited data from RCTs to demonstrate the efficacy of CNI compared with placebo and from RCTs to show no significant benefit of cyclophosphamide. However two studies have demonstrated that CNI are more effective than cyclophosphamide with less toxicity. These data support the use of CNI in children with SRNS and suggest that cyclophosphamide should not be used. Although a single study (FSGS Study 2011) found no significant difference in efficacy between cyclosporin and mycophenolate mofetil with dexamethasone, it was underpowered so it could not completely exclude a significant difference between the interventions. Further studies are required to assess the efficacy of mycophenolate mofetil in SRNS though Sinha 2015 found that tacrolimus was more effective in maintaining satisfactory remission than mycophenolate mofetil. Magnasco 2012 found no benefit of rituximab in children with SRNS. However this was a small study with only three months of follow up in children with SRNS, who were also resistant to CNI. Therefore a role for rituximab in children with SRNS has not been excluded particularly in children who show some response to CNI.
We hypothesised that the different pathologies in SRNS would influence the response to immunosuppressive agents and that children with MCD would be more likely to respond to treatment than children with FSGS as suggested by some non‐randomised studies (Niaudet 1994; Ehrich 2007) though others have identified little difference (Chua 2009). While no differences in efficacy in children with MCD or FSGS could be demonstrated for comparisons between cyclosporin and cyclophosphamide or tacrolimus and mycophenolate mofetil, the studies were too small to exclude a difference in treatment responses between pathologies. Observational studies (Ehrich 2007) had suggested that the relative efficacies of treatment regimens differed between children with initial compared with delayed steroid resistance. Subgroup analyses in studies which enrolled children with initial and delayed steroid resistance found no differences in efficacy between such patient groups (Gulati 2012; Mantan 2008; Sinha 2015). However the subgroups involved small numbers of patients so a difference in efficacy of CNI between children with initial or delayed steroid resistance cannot be completely excluded.
Data from the PodoNet Registry cohort (Trautmann 2015) found that 22% of 1234 children with SRNS had received oral or pulse cyclophosphamide while 44% had received steroid pulses although no RCTs were identified, which examined the benefits or harms of high dose steroids with alkylating agents compared with placebo, prednisone or no specific therapy. Uncontrolled studies of regimens of alkylating agents and high dose steroids have reported complete remission in 32% to 65% of children (Hari 2001; Tune 1995; Tune 1996) though adverse events of these regimens are significant. No RCTs comparing a CNI and low or high dose prednisone with placebo, prednisone or no specific treatment were identified. A retrospective analysis of children with non‐genetic FSGS found that the cumulative proportion of children achieving complete remission after treatment with IV methylprednisolone, oral cyclosporin and oral prednisone was 84% and significantly higher than the 64% of children, who achieved complete remission with oral cyclosporin and oral prednisone alone (Ehrich 2007). In the PodoNet Registry cohort, a CNI with oral corticosteroids was the most commonly used intervention with 65% of children with SRNS receiving one or more periods of treatment with these medications (Trautmann 2015).
No study to date has taken into account the information that a proportion of patients with FSGS have mutations in genes coding for podocin, nephrin and other proteins and are unlikely to respond to therapy (Ehrich 2007). Two studies included information about genetic studies (APN 2008; Choudhry 2009) but the data were not used to exclude children from studies. Response to therapy with any medication varies between studies with the number of children achieving complete or partial remission varying between 0% to 100% (Lombel 2013). For example, FSGS Study 2011 found that in the USA 46% of patients responded to cyclosporin while studies from India (Choudhry 2009; Gulati 2012) found that over 80% responded to CNI. The differences in response to CNI between studies could be related to differences in the incidence of genetic mutations between different racial groups, to differences in the proportions of children with FSGS and MCD and to the inclusion of children with initial and delayed steroid resistance. FSGS Study 2011 only enrolled subjects with FSGS and initial steroid resistance whereas the Indian studies (Choudhry 2009; Gulati 2012) included children with FSGS and MCD and children with initial or delayed steroid resistance. If SRNS with delayed steroid resistance is more likely than initial steroid‐resistant disease to have an immunological cause as suggested by the higher incidence of recurrence post transplant in children with delayed steroid resistance (Ding 2014), then children with delayed steroid resistance may have increased response rates to immunosuppressive agents.
The incidence of reported adverse events during treatment was low but could be underestimated because of small patient numbers, short follow‐up periods and incomplete reporting. None of the three studies comparing cyclosporin with placebo/no treatment reported on nephrotoxicity though nephrotoxicity occurs in 9% of treated children (Niaudet 1992; Niaudet 1994; Ponticelli 1993b). The numbers with persistent or reversible nephrotoxicity did not differ between cyclosporin and tacrolimus. Similar number of children developed or suffered worsening of hypertension during treatments with cyclosporin or IV cyclophosphamide and with cyclosporin or tacrolimus. Episodes of Infection were more common with alkylating agents than with cyclosporin.
No subgroup analyses could be undertaken because of the paucity of data. Also funnel plots (Egger 1997) could not be used because of the limited number of studies for each intervention.
Quality of the evidence
Studies included in this systematic review were small, often of poor quality and addressed several different therapeutic regimens, which limited the opportunities for meta‐analysis. Study quality can affect study results (Schulz 1995) and combining poor quality studies in meta‐analyses can provide erroneous information on the benefits of therapy (Moher 1998). Eleven studies were at low risk for selection bias. Four studies were at low risk of performance bias although, since the majority of studies (15 studies) used a laboratory measurement of proteinuria for the primary outcome of remission, there was less risk of detection bias. Eight and 10 studies respectively were considered to be free of attrition or selective outcome bias. It is possible that attrition bias influenced the outcomes in the studies comparing cyclosporin with placebo/no treatment. In three studies 10/59 (17%) randomised patients, included in the meta‐analysis comparing cyclosporin with placebo/no treatment, were excluded from analyses after randomisation. Studies with attrition bias and thus no intention‐to‐treat analysis can exaggerate the efficacy of the experimental treatment (Hollis 1999).
In many analyses there were no statistically significant differences between the groups. However the CI were often very wide, with the limits indicating the possibility of substantial benefit or substantial harm from the intervention(s) compared with the comparator(s). The results in many studies for some outcomes were therefore imprecise indicating that if these interventions were analysed in new studies, the results could change the estimates of benefits and harms considerably. This is reflected in the Summary of Findings Tables. The overall quality of the evidence (GRADE) was considered low for the comparison of cyclosporin with placebo/no treatment (Table 1) because of small numbers of patients and events and because of increased risk of selection and performance bias. In the comparison of CNI with IV cyclophosphamide, the overall quality of the evidence for complete or partial remission was considered low or very low but considered to be moderate or low for adverse effects (Table 2). The quality of the evidence was downgraded because of small numbers of patients and events resulting in imprecision and the high risk of attrition bias in one study. In the comparison of cyclosporin with MMF and IV dexamethasone, the overall quality of the evidence was considered moderate (Table 3). It was downgraded because the number of recruited patients was insufficient to exclude a difference between medications. For the comparison of cyclophosphamide with prednisone/placebo, the quality of the evidence was considered low or very low because of imprecision and risk of bias (Table 4).
Potential biases in the review process
This review identified 19 studies of which two were available only as an abstract. Additional information was provided by the authors from two studies. The literature search is likely to identify all relevant published studies including studies only available as abstracts. Since 40% of study reports in the Cochrane Kidney and Transplant's Specialised Register have been identified by handsearching of conference proceedings, it remains possible that further studies of therapy for SRNS will be identified as conference proceedings from different congresses are searched.
Agreements and disagreements with other studies or reviews
The treatment of SRNS in children has been comprehensively reviewed recently by Chua 2009 and Colquitt 2007. Colquitt 2007 included nine RCTs (all included in this review), one controlled clinical trial (comparing six months with 18 months of IV methylprednisolone) and one prospective cohort study comparing IV methylprednisolone with IV dexamethasone. They concluded that while the available evidence suggested a beneficial effect of cyclosporin on remission rates and of cyclophosphamide on time to remission, the strength of the conclusions was limited by the poor quality of included studies. Chua 2009 assessed observational studies, which evaluated complete or partial remission in 494 children treated with cyclosporin or tacrolimus, 192 treated with oral alkylating agents, 71 treated with IV cyclophosphamide and 204 treated with IV pulse corticosteroid with cyclophosphamide or cyclosporin. Overall these observational studies indicated that one third to a half of patients with SRNS achieve complete remission with cyclosporin, cyclophosphamide and/or IV methylprednisolone. RCTs indicate that patients treated with cyclosporin are significantly more likely to achieve complete or partial remission when compared with placebo or no specific therapy or with IV cyclophosphamide. Based on these studies, the KDIGO guidelines (Lombel 2013) recommend that the initial treatment of children with SRNS should be with a CNI for a minimum of six months.
Authors' conclusions
The update of this systematic review continues to highlight how few studies have addressed the efficacy of interventions for SRNS in children. The studies were generally small and of variable quality. Many studies did not provide data on the duration of remission, on kidney dysfunction including the number progressing to ESKD or on mortality although these are important patient centred outcomes. However based on the included studies, CNI appear to be of benefit for children with SRNS while cyclophosphamide is less effective and more toxic suggesting that the initial treatment of SRNS should be with CNI. ACEi significantly reduce proteinuria in children with SRNS so they should be used in children with SRNS (Lombel 2013).
Further studies are required to assess therapies in SRNS. In particular further studies of mycophenolate mofetil or rituximab compared with CNI are warranted. These studies should be of sufficient duration to assess complete remission rates, relapse rates, kidney function and adverse events and to assess any differences in response between children with MCD or FSGS and children with initial steroid resistance and those with delayed steroid resistance. In addition studies should attempt to investigate the optimal dosing or blood concentrations of CNI or mycophenolate mofetil required to achieve remission in children with SRNS. Children with genetic mutations resulting in SRNS rarely respond to therapy. Children entering RCTs should be screened for mutations before study entry and those with mutations should be excluded from studies of immunosuppressive agents because of the risks of toxic therapies in such children.
The responses of children with SRNS to current immunosuppressive agents are variable but in many studies fewer than 50% respond to any therapies. Therefore different strategies are needed to treat SRNS. Medications that stabilise the podocyte skeleton (dexamethasone, CNI, rituximab) and antifibrotic drugs (pioglitazone) are being evaluated as treatments for SRNS (Deegens 2011).
Acknowledgements
We are grateful to Dr Doaa Habashy who contributed to the original iterations of this review (Habashy 2001; Habashy 2003; Habashy 2004; Habashy 2006), contributing to the design, quality assessment, data collection, entry, analysis and interpretation, and writing.
This work was presented at the Annual Scientific Meeting of the Australian and New Zealand Society of Nephrology, Sydney, Australia, 2‐4 September, 2002 and published in abstract form in Nephrology in 2002. The authors would like to thank Dr Arvind Bagga for providing additional study data. The authors wish to thank the Information Specialist of Cochrane Kidney and Transplant for her help with this study.
Appendices
Appendix 1. Electronic search strategies
| Database | Search terms |
| CENTRAL |
|
| MEDLINE |
|
| EMBASE |
|
Appendix 2. Risk of bias assessment tool
| Potential source of bias | Assessment criteria |
| Was there adequate sequence generation? | Yes (low risk of bias): Random number table; computer random number generator; coin tossing; shuffling cards or envelopes; throwing dice; drawing of lots; minimization (minimization may be implemented without a random element, and this is considered to be equivalent to being random). |
| No (high risk of bias): Sequence generated by odd or even date of birth; date (or day) of admission; sequence generated by hospital or clinic record number; allocation by judgement of the clinician; by preference of the participant; based on the results of a laboratory test or a series of tests; by availability of the intervention. | |
| Unclear: Insufficient information about the sequence generation process to permit judgement. | |
| Was allocation adequately concealed? | Yes (low risk of bias): Randomisation method described that would not allow investigator/participant to know or influence intervention group before eligible participant entered in the study (e.g. central allocation, including telephone, web‐based, and pharmacy‐controlled, randomisation; sequentially numbered drug containers of identical appearance; sequentially numbered, opaque, sealed envelopes). |
| No (high risk of bias): Using an open random allocation schedule (e.g. a list of random numbers); assignment envelopes were used without appropriate safeguards (e.g. if envelopes were unsealed or non‐opaque or not sequentially numbered); alternation or rotation; date of birth; case record number; any other explicitly unconcealed procedure. | |
| Unclear: Randomisation stated but no information on method used is available. | |
| Was knowledge of the allocated interventions adequately prevented during the study? | Yes (low risk of bias): No blinding, but the review authors judge that the outcome and the outcome measurement are not likely to be influenced by lack of blinding; blinding of participants and key study personnel ensured, and unlikely that the blinding could have been broken; either participants or some key study personnel were not blinded, but outcome assessment was blinded and the non‐blinding of others unlikely to introduce bias. |
| No (high risk of bias): No blinding or incomplete blinding, and the outcome or outcome measurement is likely to be influenced by lack of blinding; blinding of key study participants and personnel attempted, but likely that the blinding could have been broken; either participants or some key study personnel were not blinded, and the non‐blinding of others likely to introduce bias. | |
| Unclear: Insufficient information to permit judgement of ‘Yes’ or ‘No' | |
| Were incomplete outcome data adequately addressed? | Yes (low risk of bias): No missing outcome data; reasons for missing outcome data unlikely to be related to true outcome (for survival data, censoring unlikely to be introducing bias); missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups; for dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically relevant impact on the intervention effect estimate; for continuous outcome data, plausible effect size (difference in means or standardized difference in means) among missing outcomes not enough to have a clinically relevant impact on observed effect size; missing data have been imputed using appropriate methods. |
| No (high risk of bias): Reason for missing outcome data likely to be related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups; for dichotomous outcome data, the proportion of missing outcomes compared with observed event risk enough to induce clinically relevant bias in intervention effect estimate; for continuous outcome data, plausible effect size (difference in means or standardized difference in means) among missing outcomes enough to induce clinically relevant bias in observed effect size; ‘as‐treated’ analysis done with substantial departure of the intervention received from that assigned at randomisation; potentially inappropriate application of simple imputation. | |
| Unclear: Insufficient information to permit judgement of ‘Yes’ or ‘No'. | |
| Are reports of the study free of suggestion of selective outcome reporting? | Yes (low risk of bias): The study protocol is available and all of the study’s pre‐specified (primary and secondary) outcomes that are of interest in the review have been reported in the pre‐specified way; the study protocol is not available but it is clear that the published reports include all expected outcomes, including those that were pre‐specified (convincing text of this nature may be uncommon). |
| No (high risk of bias): Not all of the study’s pre‐specified primary outcomes have been reported; one or more primary outcomes is reported using measurements, analysis methods or subsets of the data (e.g. subscales) that were not pre‐specified; one or more reported primary outcomes were not pre‐specified (unless clear justification for their reporting is provided, such as an unexpected adverse effect); one or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis; the study report fails to include results for a key outcome that would be expected to have been reported for such a study. | |
| Unclear: Insufficient information to permit judgement of ‘Yes’ or ‘No'. | |
| Was the study apparently free of other problems that could put it at a risk of bias? | Yes (low risk of bias): The study appears to be free of other sources of bias. |
| No (high risk of bias): Had a potential source of bias related to the specific study design used; stopped early due to some data‐dependent process (including a formal‐stopping rule); had extreme baseline imbalance; has been claimed to have been fraudulent; had some other problem. | |
| Unclear: Insufficient information to permit judgement of ‘Yes’ or ‘No'. |
Data and analyses
Comparison 1.
Cyclosporin versus placebo/no treatment
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete remission | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 All renal pathologies | 3 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 7.66 [1.06, 55.34] |
| 1.2 FSGS | 2 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 5.83 [0.75, 45.09] |
| 2 Complete or partial remission | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.1 All renal pathologies | 3 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 5.48 [1.95, 15.44] |
| 2.2 FSGS | 1 | 24 | Risk Ratio (M‐H, Random, 95% CI) | 5.0 [1.63, 15.31] |
| 3 Adverse events | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3.1 Worsening of hypertension | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Infection | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 2.
Calcineurin inhibitor versus IV cyclophosphamide
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment response at 3 to 6 months | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 Complete or partial remission | 2 | 156 | Risk Ratio (M‐H, Random, 95% CI) | 1.98 [1.25, 3.13] |
| 1.2 Complete remission | 2 | 156 | Risk Ratio (M‐H, Random, 95% CI) | 3.43 [1.84, 6.41] |
| 1.3 Partial remission | 2 | 156 | Risk Ratio (M‐H, Random, 95% CI) | 1.68 [0.43, 6.56] |
| 2 Mean time to remission | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3 Complete remission/SSNS at 12 months in 80 patients with complete or partial remission at 6 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3.1 Complete remission in patients with complete remission at 6 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Complete remission in patients with partial remission at 6 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Other outcomes at 12 months in 38 patients with partial remission at 6 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4.1 Number with non‐nephrotic proteinuria | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Number developing steroid resistance | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 5.1 Treatment failure (non response, serious infection, persistently elevated creatinine) at 6 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Any serious adverse effect | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 Medications ceased due to adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.4 Serious infections | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.5 Persistent nephrotoxicity | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.6 Death | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 3.
Tacrolimus versus cyclosporin
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment response at 6 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 Complete remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Complete and partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Treatment response at 12 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 Complete remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 Complete and partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Relapse following complete or partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4 Post hoc analysis: complete remission in initial and late onset SRNS | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4.1 Initial SRNS | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Late SRNS | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Post hoc analysis: complete or partial remission in initial and late onset SRNS | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 5.1 Initial SRNS | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Late SRNS | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Change in eGFR over 12 months | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 7.1 Persistent nephrotoxicity | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Reversible nephrotoxicity | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.3 Worsening of hypertension | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.4 Headache | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.5 Paraesthesia | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.6 Hypertrichosis | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.7 Gingival hyperplasia | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.8 Acne or skin infections | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.9 Diarrhoea | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.10 Sepsis/pneumonia | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 4.
Cyclosporin versus mycophenolate mofetil with pulse dexamethasone
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment response at 52 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 Complete remission (primary outcome 1,2) | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Partial remission (primary outcome 3) | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Complete or partial remission (primary outcome 1,2,3) | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Sustainable remission between 52 and 78 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 Complete remission (secondary outcome 1,2) | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Partial remission (secondary outcome 3) | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 No sustainable remission (secondary outcome 4,5) | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 CKD or death | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3.1 Death by 52 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 50% decline in GFR by 78 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 ESKD by 78 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Adverse events (weeks 0 to 26) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4.1 Serious infection requiring hospitalisation | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Total Infections | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 Total hospitalisations | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 Gastrointestinal adverse effects | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.5 Neuropsychiatric conditions | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.6 Hypertension | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 5.
Triple therapy with cyclophosphamide, mycophenolate mofetil or leflunomide
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Short‐term response | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 MMF versus CPA | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 LEF versus MMF | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 LEF versus CPA | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Long‐term response | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 MMF versus CPA | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 LEF versus MMF | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 LEF versus CPA | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 6.
Tacrolimus versus mycophenolate mofetil to maintain remission
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment response | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 Complete or partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Infrequent relapses | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Frequent relapses | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.4 Steroid resistance | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Relapses per year | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3 Prednisone dose | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 Change in GFR | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected |
Comparison 7.
Oral cyclophosphamide versus prednisone/placebo
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete remission | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 All renal pathologies | 2 | 84 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.61, 1.87] |
| 1.2 FSGS | 2 | 63 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.43, 2.37] |
| 2 Complete or partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 FSGS | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Treatment failure | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4.1 All‐cause mortality | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Hypertension with seizures | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 Cystitis | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 Bone marrow suppression | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 8.
IV versus oral cyclophosphamide
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 Vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Bacterial infection | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 9.
IV cyclophosphamide versus oral cyclophosphamide plus IV dexamethasone
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment response at 6 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 Complete remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Complete or partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Treatment response at 18 months | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 Sustained remission/steroid‐sensitive relapses | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 CKD | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Complete or partial resistance in subgroups | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3.1 Initial SRNS | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Late SRNS | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 Minimal change disease | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.4 FSGS or MesPGN | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4.1 Hypertension | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 cataract/glaucoma | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 Cushingoid features | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 Leucopenia | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.5 Cystitis | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.6 Bacterial infections | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.7 Hypokalaemia | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.8 Steroid encephalopathy | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.9 Hair loss | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 10.
Rituximab/cyclosporin/prednisolone versus cyclosporin/prednisolone
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete remission | 1 | 31 | Risk Ratio (M‐H, Random, 95% CI) | 1.14 [0.33, 3.94] |
| 1.1 Complete remission in initial steroid resistance | 1 | 16 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 1.2 Complete remission in delayed steroid resistance | 1 | 15 | Risk Ratio (M‐H, Random, 95% CI) | 1.14 [0.33, 3.94] |
| 2 End of study creatinine | 1 | 31 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.23, 0.23] |
| 2.1 Initially resistant patients | 1 | 16 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.36, 0.36] |
| 2.2 Delayed resistant patients | 1 | 15 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.30, 0.30] |
| 3 End of study serum albumin | 1 | 31 | Mean Difference (IV, Random, 95% CI) | 0.25 [‐0.22, 0.72] |
| 3.1 Initially resistant patients | 1 | 16 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.77, 0.77] |
| 3.2 Delayed resistant patients | 1 | 15 | Mean Difference (IV, Random, 95% CI) | 0.40 [‐0.20, 1.00] |
| 4 Adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4.1 Abdominal pain | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Bronchospasm/treatment discontinued | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 Hypotension | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 Skin rash | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.5 Mild dyspnoea | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 11.
Chlorambucil versus indomethacin
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 End‐stage kidney disease | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 12.
Azathioprine versus placebo
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Complete remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 All renal pathologies | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Complete or partial remission | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 All renal pathologies | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 13.
Fosinopril plus prednisone versus prednisone alone
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Proteinuria | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 After 4 weeks of treatment | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 After 8 weeks of treatment | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 After 12 weeks of treatment | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Tubular proteinuria | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Retinol binding protein (mg/L) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Beta 2 microglobulin (mg/L) | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Serum albumin | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 Systolic blood pressure | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5 Creatinine clearance | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6 Serum potassium | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected |
What's new
| Date | Event | Description |
|---|---|---|
| 6 October 2016 | New citation required and conclusions have changed | Five new studies included, new interventions included |
| 6 October 2016 | New search has been performed | New search, summary of findings tables incorporated |
History
Protocol first published: Issue 2, 2002 Review first published: Issue 2, 2004
| Date | Event | Description |
|---|---|---|
| 16 September 2014 | New search has been performed | Search strategies updated |
| 29 September 2010 | New citation required and conclusions have changed | Four new studies, new comparisons, risk of bias assessment replaces quality assessment and summary of findings tables included. |
| 9 October 2008 | Amended | Converted to new review format. |
Differences between protocol and review
Summary of findings tables have been incorporated into the 2016 update
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods |
|
|
| Participants |
|
|
| Interventions | CSA group
CPA group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated random lists, stratified by centre |
| Allocation concealment (selection bias) | Low risk | Central allocation by study coordinator |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants or investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Laboratory measure of primary outcome unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Complete follow‐up to 12 weeks, then non‐responders could be withdrawn to enter non‐responder protocol 5/15 CSA group withdrawn from 12 weeks onwards (4 treated with non‐responder protocol of high dose CSA) 14/17 CPA group withdrawn from 12 weeks onwards (7 treated with non‐responder protocol of pulse methylprednisolone) |
| Selective reporting (reporting bias) | Low risk | Complete or partial remission, adverse effects reported at 12 weeks |
| Other bias | High risk | Funded in part by a grant from Novartis Pharma |
| Methods |
|
|
| Participants |
|
|
| Interventions | High dose enalapril
Low dose enalapril
Co‐interventions
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated random numbers |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes opened by investigator, who did not manage the patients (information from author) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants or investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Laboratory assessment of outcome unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All patients randomised were included and completed the study (information from authors) |
| Selective reporting (reporting bias) | High risk | Outcomes reported (urinary albumin excretion, kidney function, adverse events) but no results could be included in meta‐analyses |
| Other bias | Unclear risk | Funding source not stated |
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment
Control
Co‐interventions: not reported |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Randomised double‐blind placebo controlled study |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Randomised double‐blind placebo controlled study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Cross‐over study of 6 patients; I patient (17%) did not complete the study with no reason provided |
| Selective reporting (reporting bias) | High risk | Outcomes (urine protein excretion, CrCl) reported; no report of adverse effects |
| Other bias | Low risk | Study supported by Ramathibodi Research Grant No.25/1996, Mahidol University, Bangkok |
| Methods |
|
|
| Participants |
|
|
| Interventions | TAC group
CSA group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated randomisation list were generated off site by colleague not involved in the study |
| Allocation concealment (selection bias) | Low risk | Sealed opaque serially numbered envelopes opened at randomisation |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants/investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Primary outcome was laboratory based and unlikely to be influenced by lack of blinding; blinding of outcome assessors, who assessed gum hypertrophy and hirsutism |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All patients followed up |
| Selective reporting (reporting bias) | Low risk | Outcomes (complete remission, partial remission, relapse, adverse events) reported |
| Other bias | Low risk | Study medications only provided by Pancea Biotec, India |
| Methods |
|
|
| Participants |
|
|
| Interventions | IV CPA group
Oral CPA group
Co‐interventions: not reported |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants/investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Primary outcome was laboratory based and unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Loss to follow‐up: 15%; 2 from control group lost to follow‐up and excluded from analysis |
| Selective reporting (reporting bias) | Low risk | Outcome (complete remission, non‐remission, adverse effects) reported |
| Other bias | Unclear risk | Funding source not reported |
| Methods |
|
|
| Participants |
|
|
| Interventions | DEXA/MMF group
CSA group
Co‐interventions
|
|
| Outcomes | Primary outcomes
Secondary outcomes
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedules using randomly permuted blocks of random sizes were prepared by the Data Coordinating centre stratified by eGFR, race |
| Allocation concealment (selection bias) | Low risk | Study investigators were blinded to randomised schedules |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open label study; lack of blinding could influence patient management differently between treatment groups |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Study investigators were blinded to results of interim analyses done for the Data and Safety Monitoring Board Laboratory values for primary outcomes and some secondary outcomes unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Minimal participants were lost to follow up/did not attend assessments (< 1%); all patients included in outcome measurement |
| Selective reporting (reporting bias) | Low risk | All expected outcomes (remission, relapse, adverse effects) were reported |
| Other bias | Low risk | NIH funded |
| Methods |
|
|
| Participants |
|
|
| Interventions | CSA group
No treatment group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants/investigators not blinded; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Primary outcome was laboratory outcome based and unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All patients followed up and accounted for |
| Selective reporting (reporting bias) | Low risk | Complete/partial remission/adverse effects reported |
| Other bias | Unclear risk | Funding source not reported |
| Methods |
|
|
| Participants |
|
|
| Interventions | TAC group
CPA group
Co‐interventions
|
|
| Outcomes | Primary outcomes
Secondary outcomes
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Permuted block randomisation with stratification, by initial or late resistance, was performed centrally by individuals not involved in trial implementation |
| Allocation concealment (selection bias) | Low risk | Allocation was concealed in opaque sealed envelopes The investigators were blinded to the randomisation schedules |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and personnel delivering therapy were not blinded (one arm received tablets, one arm received injections) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The outcome assessment is at low risk of bias as it was a laboratory measure and unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Seven patients were lost to follow‐up (TAC (3), CPA (4)); this makes up 5% (7/131) and this number is unlikely to alter results; all included in safety analysis |
| Selective reporting (reporting bias) | Low risk | All outcomes of interest (complete or partial remission, remission, adverse effects) have been reported |
| Other bias | Low risk | Study medications (tacrolimus and cyclophosphamide) were provided by Panacea Biotec Study was supported by funding from the Indian Council of Medical Research |
| Methods |
|
|
| Participants |
|
|
| Interventions | AZA group
Placebo group
Co‐interventions: not reported |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Centrally derived table of random numbers |
| Allocation concealment (selection bias) | Low risk | "Reports were sent to a co‐ordinator, who assigned treatment and distributed drugs identified by code numbers to pharmacists at each clinic" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding of participants/investigators |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinding of participants/investigators |
| Incomplete outcome data (attrition bias) All outcomes | High risk | All patients followed up; 18% (7/38) excluded from analysis |
| Selective reporting (reporting bias) | High risk | Definition of partial remission not stated; no report of adverse effects |
| Other bias | High risk | Help with planning of study provided by employees of Wellcome Foundation and Burroughs Welcome |
| Methods |
|
|
| Participants |
|
|
| Interventions | CPA‐prednisone group
Prednisone group
Co‐interventions: not reported |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants/investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessment by quantitative measurement of protein on overnight urine collection or semi‐quantitative based on urinalysis Unclear how many patients had laboratory assessment of outcome |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All patients followed up |
| Selective reporting (reporting bias) | High risk | Complete and partial remission reported but no definition for partial remission provided; adverse effects not reported specifically for steroid‐resistant patients |
| Other bias | Low risk | Support from NIH AM 14490‐93, National Kidney Foundation, Kidney Foundation of New York, John Rath Foundation |
| Methods |
|
|
| Participants |
|
|
| Interventions | CPA‐prednisone group
Prednisone group
Co‐interventions: not reported |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Low risk | Central randomisation |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants/investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Primary outcome was laboratory based and unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 32/35 in treatment group and 21/25 in control group analysed for complete/partial remission and unclear why other patients not included. 11% excluded |
| Selective reporting (reporting bias) | Low risk | Outcomes of complete and partial remission, adverse events, kidney function included |
| Other bias | Low risk | Supported by NIH Grant 1 RO1 AM18234 and multiple other not for profit agencies in USA, UK, Netherlands |
| Methods |
|
|
| Participants |
|
|
| Interventions | Chlorambucil group
Indomethacin group
Co‐interventions: not reported |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of investigators/participants; lack of blinding could influence management. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information about how primary outcome was measured |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Data only available from conference proceedings |
| Selective reporting (reporting bias) | Unclear risk | Complete remission (no definition provided), ESKD |
| Other bias | Unclear risk | Funding source not stated Data from conference proceedings |
| Methods |
|
|
| Participants |
|
|
| Interventions | CSA group
Placebo group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Central computer generated list |
| Allocation concealment (selection bias) | Low risk | Central co‐ordinator |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding of participants/investigators; placebo‐controlled study |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Laboratory measurement of primary outcome unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 4/16 excluded from cyclosporin group and 3/15 excluded from control group for noncompliance (2 each group, 1 unknown CSA group, 1 each group for rising Cr). In view of small numbers, results likely to influence results (23% excluded) |
| Selective reporting (reporting bias) | Low risk | Outcomes of complete or partial remission, adverse events, kidney function |
| Other bias | Unclear risk | Funding source not stated |
| Methods |
|
|
| Participants |
|
|
| Interventions | RTX group
Control group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes | Trial registration number EUDRA CT 2007‐007796‐16 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Permutated block randomisation with blocks of variable size |
| Allocation concealment (selection bias) | Low risk | Allocation was concealed by contacting the holder of the allocation schedule at central administration |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Clinical investigators, study nurses enrolling patients, and the statistician were not blinded to group assignment Study staff responsible for follow up were blinded so their management of patients would not be influenced by treatment allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Study staff responsible for facilitating follow‐up data measurements by contacting patient families by phone were kept blinded Also, as the outcome measured was a laboratory value, lack of blinding is unlikely to affect outcome |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No loss to follow up All patients analysed; 1 patient from each group did not complete treatment due to adverse side effects |
| Selective reporting (reporting bias) | High risk | Data on partial remission not included Primary outcome (end study proteinuria) not provided in a form that can be included in meta‐analysis Adverse effects related to RTX were only reported |
| Other bias | Low risk | Supported by Italian Ministry of Health, the Renal Child Foundation, two other non‐Pharma related foundations |
| Methods |
|
|
| Participants |
|
|
| Interventions | IV CPA group
Oral CPA + IV DEXA group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Stratified randomisation, in blocks of four, were done separately with computer‐generated numbers to allocate patients with initial and late steroid‐resistance randomly..." |
| Allocation concealment (selection bias) | Low risk | "Allocation was concealed in sealed opaque envelopes, which were opened by an associate not involved in the study" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants/investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Primary outcome was serum albumin + urinary protein; urine protein measured either by urinalysis or UP/C. Unclear how many patients had laboratory measure of proteinuria |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3/52 (6%) patients excluded after randomisation (IV CPA group (1); oral CPA + IV DEXA group (2)) for non‐compliance; unlikely to have influenced results |
| Selective reporting (reporting bias) | Low risk | Primary outcomes: number in complete or partial remission and adverse effects reported |
| Other bias | Unclear risk | Funding source not reported |
| Methods |
|
|
| Participants |
|
|
| Interventions | CSA group
No treatment group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Sealed opaque envelopes numbered in sequence according to a random number table; stratified for adults/children |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants/investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Laboratory measure of primary outcome unlikely to be influenced by lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 3/20 (15%) children (all from no treatment group) lost to follow‐up and not included in results |
| Selective reporting (reporting bias) | High risk | No separate data available for adverse events in children |
| Other bias | High risk | Funded in part by Sandoz P.F, Milano, Italy |
| Methods |
|
|
| Participants |
|
|
| Interventions | TAC group
MMF group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratified block randomisation; stratified for histology and type of response |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered, sealed, opaque envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding and lack of blinding could result in differences in management |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information provided on how outcome was measured |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Abstract only; complete follow‐up to 12 months |
| Selective reporting (reporting bias) | Unclear risk | Abstract only |
| Other bias | Unclear risk | No information provided |
| Methods |
|
|
| Participants |
|
|
| Interventions | MMF group
CPA group
LEF group
Co‐interventions
|
|
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Simple randomization using a randomised digital table" |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding and lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | No blinding but outcome was laboratory based and unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Four (18%) excluded from analysis for loss to follow up or other |
| Selective reporting (reporting bias) | High risk | Incomplete reporting of adverse events |
| Other bias | Low risk | Supported by National Natural Science Foundation of China and others |
| Methods |
|
|
| Participants |
|
|
| Interventions | Fosinopril‐prednisone group
Prednisone group
Co‐interventions: none |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Computer generated random numbers were used to randomly allocate patients ..." |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants/investigators; lack of blinding could influence management |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Laboratory measurement of primary outcome unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 12/57 (21%) (fosinopril group (5); prednisone group (7)) lost to follow‐up and excluded from analysis |
| Selective reporting (reporting bias) | Low risk | Primary outcomes of study were reduction in proteinuria, CrCl; adverse effects reported |
| Other bias | Low risk | Ministry of Health Science Foundation of China (98‐1‐117) |
ACEi ‐ angiotensin converting enzyme inhibitors; ANC ‐ absolute neutrophil count; APN ‐ Arbeitgemeinschaft fur Padiatrische Nephrologie; ARB ‐ angiotensin receptor blocker; AZA ‐ azathioprine; BP ‐ blood pressure; CNI ‐ calcineurin inhibitor; CPA ‐ cyclophosphamide; CSA ‐ cyclosporin; Cr ‐ creatinine; CrCl ‐ creatinine clearance; DBP ‐ diastolic blood pressure; DEXA ‐ dexamethasone; DM ‐ diabetes mellitus; eGFR ‐ estimated glomerular filtration rate; ESKD ‐ end‐stage kidney disease; FSGS ‐ focal segmental glomerulosclerosis; GFR ‐ glomerular filtration rate; GI ‐ gastrointestinal; GN ‐ glomerulonephritis; HCT ‐ haematocrit; HIV ‐ human immunodeficiency virus; HSP ‐ Henoch‐Schonlein purpura; INS ‐ idiopathic nephrotic syndrome; intermittent ‐ prednisone given on 3 consecutive days out of 7; ISKDC ‐ International Study of Kidney Disease in Children; LEF ‐ leflunomide; LFT ‐ liver function test; M/F ‐ male/female; MCD ‐ minimal change disease; MCGN ‐ mesangiocapillary glomerulonephritis; MesPGN ‐ mesangioproliferative glomerulonephritis; MMF ‐ mycophenolate mofetil; MNS ‐ membranous nephrotic syndrome; NSAIDs ‐ nonsteroidal anti‐inflammatory drugs; RCT ‐ randomised controlled trial; RTX ‐ rituximab; SBP ‐ systolic blood pressure; SCr ‐ serum creatinine; SD ‐ standard deviation; SLE ‐ systemic lupus erythematosus; SRNS ‐ steroid‐resistant nephrotic syndrome; TAC ‐ tacrolimus; UP/C ‐ urinary protein/urinary creatinine ratio; WCC ‐ white cell count
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Adeniyi 1979 | Children had nephrotic syndrome secondary to Plasmodium malariae (31/36) |
| Arora 2002 | Adult patients |
| Bhaumik 2002 | Mixed population of adults and children; unable to separate data |
| Buyukcelik 2002 | Study of gemfibrozil on lipid profiles in children with nephrotic syndrome; ineligible renal pathology as all except one had MPGN |
| Hiraoka 2000 | SSNS patients |
| Iyengar 2006 | SSNS patients |
| Jung 1990 | Mixed population; unable to separate data |
| Kano 2003 | Included patients did not have nephrotic syndrome but moderate proteinuria with normal serum albumin levels |
| Koshikawa 1993 | Adult patients |
| Kumar 2004a | Adults patients |
| Li 2006g | Adult patients |
| Ren 2011 | Adult patients |
| Ren 2013 | Adult patients |
| Saito 2014 | Adult patients |
| Shibasaki 2004 | Not clear if paediatric patients were included and these could not be separated from adult patients; includes patients with non MCD or FSGS pathology |
| Walker 1990a | Adult patients |
| Zhao 2013a | Includes both steroid‐resistant and steroid dependent patients and results cannot be separated |
MCD ‐ minimal change disease; FSGS ‐ focal segmental glomerulosclerosis; MPGN ‐ membranoproliferative glomerulonephritis; RCT ‐ randomised controlled trial; SSNS ‐ steroid‐sensitive nephrotic syndrome
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | Efficacy and safety of RE‐021, a dual endothelin receptor and angiotensin receptor blocker, in patients with focal segmental glomerulosclerosis (FSGS): a randomised, double‐blind, active‐control, dose‐escalation study |
| Methods | Double blind RCT |
| Participants | Children and adults aged 8 to 75 years with primary FSGS |
| Interventions | Sparsentan (a dual endothelin receptor) versus irbesartan (ARB) |
| Outcomes | Change in UP/C in FSGS patients receiving Sparsentan over a range of doses (200 mg, 400 mg, 800 mg daily) for 8 weeks to determine safety and efficacy compared to treatment with irbesartan (300 mg daily) as active control |
| Starting date | 2013 |
| Contact information | Dr Howard Trachtman |
| Notes | Estimated primary completion date is December 2015; only US sites are enrolling children |
| Trial name or title | Efficacy and safety of rituximab to that of calcineurin inhibitors in children with steroid resistant nephrotic syndrome |
| Methods | Open label RCT |
| Participants | Children aged 3 to 16 years with SRNS (MCD, MesPGN or FSGS) |
| Interventions | Rituximab infusions weekly for 2 to 4 doses over up to 4 weeks compared with oral tacrolimus given until the child has achieved 6 months of relapse free survival |
| Outcomes | 12‐month relapse‐free survival in the ITT population; adverse effects |
| Starting date | March 2015; estimated enrolment 120 children |
| Contact information | Dr. Biswanath Basu, Nilratan Sircar Medical College, India (basuv3000@gmail.com) |
| Notes | Estimated study completion date March 2017 Other study numbers: PednephroRCT/PM/NRSMCH‐33, CTRI/2015/01/005364 |
| Trial name or title | Ofatumumab in children with steroid‐ and calcineurin‐inhibitor‐resistant nephrotic syndrome: a double‐blind randomised, controlled, superiority trial |
| Methods | RCT |
| Participants | Children aged 2 to 18 years with SRNS (MCD, MesPGN or FSGS) and resistance to CNI and MMF |
| Interventions | Single dose of IV Ofatumumab in normal saline versus placebo (normal saline alone); other immunosuppressive therapies will be withdrawn; all children with receive an ACEi |
| Outcomes | Complete or partial disease remission; adverse events |
| Starting date | March 2015; estimated enrolment 50 children |
| Contact information | Dr Gian Marco Ghiggeri, Istituto Giannina Gaslini, Italy (gmarcoghiggeri@ospedale‐gaslini.ge.it) |
| Notes | Estimated study completion date March 2018 |
ACEi ‐ angiotensin converting enzyme inhibitors; ARB ‐ angiotensin receptor blocker; CNI ‐ calcineurin inhibitor; FSGS ‐ focal segmental glomerulosclerosis; MCD ‐ minimal change disease; MesPGN ‐ mesangioproliferative glomerulonephritis; MMF ‐ mycophenolate mofetil
Contributions of authors
Designing the review; EH, DH, JC
Undertaking review update: EH, DH, SW (2016), NW, JC
Coordinating the review; EH
Study selection, quality assessment, data collection; EH, DH, SW, NW
Entering data into RevMan; DH, EH, SW, NW
Analysis of data; DH, EH, SW, NW
Interpretation of data; DH, SW, EH, NW, JC
Writing the review; DH, EH, NW, JC
Providing general advice on the review; EH, NW, JC
Sources of support
Internal sources
No sources of support supplied
External sources
-
NHMRC, Australia.
Cochrane Kidney and Transplant is supported in part by NHMRC grants
Declarations of interest
Elisabeth Hodson: none known
Sophia Wong: none known
Narelle Willis: none known
Jonathan Craig: none known
Notes
2010: The risk of bias assessment tool has replaced the quality assessment checklist used in previous versions of this review.
2016: Summary of findings tables have been incorporated
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
- Plank C, Kalb V, Hinkes B, Hildebrandt F, Gefeller O, Rascher W, et al. Cyclosporin A is superior to cyclophosphamide in children with steroid‐resistant nephrotic syndrome‐a randomized controlled multicentre trial by the Arbeitgemeinschaft fur Padiatrische Nephrologie. Pediatric Nephrology 2008;23(9):1483‐93. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bagga A, Mudigoudar BD, Hari P, Vasudev V. Enalapril dosage in steroid‐resistant nephrotic syndrome. Pediatric Nephrology 2004;19(1):45‐50. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]; Bagga A, Mudigoudar BD, Vasudev V, Hari P. Low (LD) versus high dose (HD) enalapril therapy in steroid resistant nephrotic syndrome (SRNS). Seventh Asian Congress of Pediatric Nephrology; 2000 Nov 4‐6; Singapore. 2000. [CENTRAL: CN‐00583291] [Google Scholar]
- Chongviriyaphan N, Tapaneya‐Olarn C, Suthutvoravut U, Karnchanachumpol S, Chantraruksa V. Effects of tuna fish oil on hyperlipidemia and proteinuria in childhood nephrotic syndrome. Journal of the Medical Association of Thailand 1999;82 Suppl(1):122‐8. [MEDLINE: ] [PubMed] [Google Scholar]
- Choudhry A, Bagga A, Menon S, Hari P. Randomized controlled trial (RCT) on efficacy and safety of cyclosporin (CyA) vs tacrolimus (Tac) in steroid resistant nephrotic syndrome (SRNS) [CRG030600042] [abstract no: 182 (OP)]. Pediatric Nephrology 2007;22(9):1480. [CENTRAL: CN‐00653722] [Google Scholar]; Choudhry S, Bagga A, Hari P, Sharma S, Kalaivani M, Dinda A. Efficacy and safety of tacrolimus versus cyclosporine in children with steroid‐resistant nephrotic syndrome: a randomized controlled trial. American Journal of Kidney Diseases 2009;53(5):760‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Elhence R, Gulati S, Kher V, Gupta A, Sharma RK. Intravenous pulse cyclophosphamide ‐ a new regime for steroid‐resistant minimal change nephrotic syndrome. Pediatric Nephrology 1994;8(1):1‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]; Gupta A, Elhence R, Kher V, Gulati S, Sharma RK. IV cyclophosphamide ‐ a new regimen for steroid nonresponsive minimal change disease [abstract]. 12th International Congress of Nephrology; 1993 Jun 13‐18; Jerusalem, Israel. 1993:84. [Google Scholar]
- D'Agati VD, Alster JM, Jennette JC, Thomas DB, Pullman J, Savino DA, et al. Association of histologic variants in FSGS clinical trial with presenting features and outcomes. Clinical Journal of The American Society of Nephrology: CJASN 2013;8(3):399‐406. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]; Ferris M, Norwood V, Radeva M, Gassman JJ, Al‐Uzri A, Askenazi D, et al. Patient recruitment into a multicenter randomized clinical trial for kidney disease: report of the focal segmental glomerulosclerosis clinical trial (FSGS CT). Clinical & Translational Science 2013;6(1):13‐20. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]; Gassman J, Fine R, Gibson D, Greene T, Hogg R, Kaskel F, et al. A preliminary report of the focal segmental glomerulosclerosis clinical trial (FSGS‐CT) [abstract no: F‐PO1984]. Journal of the American Society of Nephrology 2008;19(Abstracts Issue):559A. [CENTRAL: CN‐00790759]18235084 [Google Scholar]; Gassman JJ, Trachtman H, Gipson D, Friedman A, Greene T, Vento S, et al. Implementing a second randomized trial enrolling mid‐study treatment failures from the Focal Segmental Glomerular Sclerosis (FSGS) Clinical Trial [abstract no: 33]. Clinical Trials 2007;4(4):382. [CENTRAL: CN‐00767231] [Google Scholar]; Gipson D, Radeva M, Fine R, Friedman A, Gassman J, Greene T, et al. Focal Segmental Glomerulosclerosis Clinical Trial (FSGS‐CT) study cohort [abstract]. Journal of the American Society of Nephrology 2009;20(Abstracts issue):147A. [CENTRAL: CN‐00793840] [Google Scholar]; Gipson DS, Trachtman H, Kaskel FJ, Greene TH, Radeva MK, Gassman JJ, et al. Clinical trial of focal segmental glomerulosclerosis in children and young adults. Kidney International 2011;80(8):868‐78. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]; Gipson DS, Trachtman H, Kaskel FJ, Radeva MK, Gassman J, Greene TH, et al. Clinical trials treating focal segmental glomerulosclerosis should measure patient quality of life. Kidney International 2011;79(6):678‐85. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]; Greene T, Gassman J, Gipson D, Hogg R, Kaskel F, Moxey‐Mims M, et al. Multicenter randomized clinical trial of FSGS in children and young adults [abstract no: F‐PO1014]. Journal of the American Society of Nephrology 2005;16:558A. [CENTRAL: CN‐00794633] [Google Scholar]; Hogg RJ, Friedman A, Greene T, Radeva M, Budisavljevic MN, Gassman J, et al. Renal function and proteinuria after successful immunosuppressive therapies in patients with FSGS. Clinical Journal of the American Society of Nephrology: CJASN 2013;8(2):211‐8. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]; Kopp JB, Winkler CA, Zhao X, Radeva MK, Gassman JJ, D'Agati VD, et al. Clinical features and histology of apolipoprotein L1‐associated nephropathy in the FSGS Clinical Trial. Journal of the American Journal of Nephrology 2015;26(6):1443‐8. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]; Middleton JP, Yorgin P, Gipson D, Radeva M, Fine R, Friedman A, et al. Prevalence of blood pressure (BP) control in the Focal Segmental Glomerulosclerosis Clinical Trial (FSGS‐CT) study cohort [abstract]. Journal of the American Society of Nephrology 2009;20(Abstracts issue):148A. [CENTRAL: CN‐00795224] [Google Scholar]; Radeva M, McMahan J, Gassman J. Optimizing logistics under a three level administration system: coordination of the Focal Segmental Glomerular Sclerosis (FSGS) trial [abstract no: P63]. Clinical Trials 2007;4(4):417‐8. [CENTRAL: CN‐00794883] [Google Scholar]; Trachtman H, Fine R, Friedman A, Gassman J, Gipson D, Greene T, et al. Quality of life in children with focal segmental glomerulosclerosis (FSGS): baseline findings. Report of the FSGS‐Clinical Trial (CT) [abstract]. Journal of the American Society of Nephrology 2009;20(Abstracts issue):147A. [CENTRAL: CN‐00795355] [Google Scholar]
- Garin EH, Orak JK, Hiott KL, Sutherland SE. Cyclosporine therapy for steroid‐resistant nephrotic syndrome. A controlled study. American Journal of Diseases of Children 1988;142(9):985‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Gulati A, Bagga A, Nephrotic Syndrome Study Group. Multicenter randomized controlled trial comparing efficacy of tacrolimus to intravenous cyclophosphamide in children with steroid resistant nephrotic syndrome [abstract no: LB‐OR03]. Journal of the American Society of Nephrology 2011;22:1B. 21164031 [Google Scholar]; Gulati A, Sinha A, Gupta A, Kanitkar M, Sreenivas V, Sharma J, et al. Treatment with tacrolimus and prednisolone is preferable to intravenous cyclophosphamide as the initial therapy for children with steroid‐resistant nephrotic syndrome. Kidney International 2012;82(10):1130‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Abramowicz M, Barnett HL, Edelmann CM Jr, Greifer I, Kobayashi O, Arneil GC, et al. Controlled trial of azathioprine in children with nephrotic syndrome. A report for the international study of kidney disease in children. Lancet 1970;1(7654):959‐61. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]; Arneil GC. International trial of azathioprine in nephrotic syndrome in childhood [abstract]. Nephron 1971;8:95. [CENTRAL: CN‐00602053] [Google Scholar]
- Prospective, controlled trial of cyclophosphamide therapy in children with the nephrotic syndrome. Report of the International Study of Kidney Disease in Children. Lancet 1974;2(7878):423‐7. [MEDLINE: ] [PubMed] [Google Scholar]
- Tarshish P, Tobin JN, Bernstein J, Edelmann CM Jr. Cyclophosphamide does not benefit patients with focal segmental glomerulosclerosis. A report of the International Study of Kidney Disease in Children. Pediatric Nephrology 1996;10(5):590‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Kleinknecht C, Broyer M, Gubler MC, Palcoux JB. Irreversible renal failure after indomethacin in steroid‐resistant nephrosis. New England Journal of Medicine 1980;302(12):691. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]; Kleinknecht C, Broyer M, Palcoux JB, Gubler MC. Irreversible renal failure (RF) after indomethacin in steroid resistant nephrosis (SRN) [abstract]. Kidney International 1979;16(1):96. [CENTRAL: CN‐00446116] [DOI] [PubMed] [Google Scholar]
- Lieberman KV, Tejani A. A randomized double‐blind placebo‐controlled trial of cyclosporine in steroid‐resistant idiopathic focal segmental glomerulosclerosis in children. Journal of the American Society of Nephrology 1996;7(1):56‐63. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]; Tejani A, Lieberman K. A randomized placebo (PL) controlled double blind trial of cyclosporine (CSA) in steroid resistant (SR) idiopathic focal segmental glomerulosclerosis (FSGS) in children. A report of the New York, New Jersey Pediatric Nephrology Collaborative Study Group [abstract]. Journal of the American Society of Nephrology 1993;4(Program & Abstracts):289. [CENTRAL: CN‐00520391] [Google Scholar]
- Magnasco A, Ravani P, Edefonti A, Murer L, Ghio L, Belingheri M, et al. Rituximab in children with resistant idiopathic nephrotic syndrome. Journal of the American Society of Nephrology 2012;23(6):1117‐24. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mantan M, Bagga A, Hari P. Efficacy of IV pulse cyclophosphamide (CP) vs IV steroids and oral CP for steroid resistant nephrotic syndrome [abstract]. Pediatric Nephrology 2004;19(9):C75. [CENTRAL: CN‐00653731] [DOI] [PubMed] [Google Scholar]; Mantan M, Sriram CS, Hari P, Dinda A, Bagga A. Efficacy of intravenous pulse cyclophosphamide treatment versus combination of intravenous dexamethasone and oral cyclophosphamide treatment in steroid‐resistant nephrotic syndrome. Pediatric Nephrology 2008;23(9):1495‐502. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ponticelli C, Rizzoni G, Edefonti A, Altieri P, Rivolta E, Rinaldi S, et al. A randomized trial of cyclosporine in steroid‐resistant idiopathic nephrotic syndrome. Kidney International 1993;43(6):1377‐84. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bagga A, Gupta A, Dinda A, Hari P, Sinha A. Randomized controlled trial comparing efficacy of mycophenolate mofetil (MMF) & alternate day prednisone versus tacrolimus & prednisolone in maintaining remission in steroid resistant nephrotic syndrome (SRNS) [abstract no: P‐SUN200]. Pediatric Nephrology 2013;28(8):1600. [Google Scholar]; Sinha A, Bagga A. Randomized trial on efficacy of mycophenolate mofetil versus tacrolimus in maintaining remission in children with steroid resistant nephrotic syndrome [abstract no: HI‐OR05]. Journal of the American Society of Nephrology 2015;26(Abstracts):B2. [CTRI/2012/03/002479] [Google Scholar]
- Wu B, Mao J, Shen H, Fu H, Wang J, Liu A, et al. Triple immunosuppressive therapy in steroid‐resistant nephrotic syndrome children with tacrolimus resistance or tacrolimus sensitivity but frequently relapsing. Nephrology 2015;20(1):18‐24. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Li Z, Yi Z. Clinical study of fosinopril in children with steroid resistant nephrotic syndrome [abstract]. Pediatric Nephrology 2001;16(8):C114. [DOI] [PubMed] [Google Scholar]; Li ZH, Yi ZW. Clinical study of fosinopril in children with steroid resistant nephrotic syndrome [abstract no: 2344]. 23rd International Congress of Paediatrics; 2001 Sep 9‐14; Beijing (China). 2001. [CENTRAL: CN‐00445802] [Google Scholar]; Yi Z, Li Z, Wu XC, He QN, Dang XQ, He XJ. Effect of fosinopril in children with steroid‐resistant idiopathic nephrotic syndrome. Pediatric Nephrology 2006;21(7):967‐72. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
- Adeniyi A, Hendrickse RG, Soothill JF. A controlled trial of cyclophosphamide and azathioprine in Nigerian children with the nephrotic syndrome and poorly selective proteinuria. Archives of Disease in Childhood 1979;54(3):204‐7. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arora A, Ahlawat RS, Arora S, Arora N, Mandel AK. Randomised controlled study of enalapril in steroid resistant nephrotic syndrome. Indian Journal of Nephrology 2002;12(3):107‐12. [CENTRAL: CN‐00460300] [Google Scholar]
- Bhaumik SK, Barman SC. Comparison of pulse methyl prednisolone vs cyclosporin based therapy in steroid resistant focal segmental glomerulosclerosis [abstract]. Indian Journal of Nephrology 2002;12(4):190. [CENTRAL: CN‐00460392] [Google Scholar]
- Buyukcelik M, Anarat A, Bayazit AK, Noyan A, Ozel A, Anarat R, et al. The effects of gemfibrozil on hyperlipidemia in children with persistent nephrotic syndrome. Turkish Journal of Pediatrics 2002;44(1):40‐4. [MEDLINE: ] [PubMed] [Google Scholar]
- Hiraoka M, Sudo M, West Japanese Cooperative Study of Kidney Disease in Children. Low versus standard dosage of prednisolone for initial treatment of idiopathic nephrotic syndrome in children [abstract no: A0445]. Journal of the American Society of Nephrology 1996;7(9):1335. [Google Scholar]; Hiraoka M, Tsukahara H, Haruki S, Hayashi S, Takeda N, Miyagawa K, et al. Older boys benefit from higher initial prednisolone therapy for nephrotic syndrome. The West Japan Cooperative Study of Kidney Disease in Children. Kidney International 2000;58(3):1247‐52. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]; Hiraoka M, Tsukahara H, Haruki S, Hayashi S, Takeda N, Miyagawa K, et al. Older boys benefit from intensive initial prednisolone therapy for nephrotic syndrome [abstract]. Journal of the American Society of Nephrology 1999;10(Program & Abstracts):103A. [CENTRAL: CN‐00550605] [Google Scholar]
- Iyengar A, Damle H, Kulkarni C, Damle L, Phadke K. Steroid sparing effect of a herbal preparation in steroid‐dependent nephrotic syndrome. Pediatric Nephrology 2006;21(7):1031‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Jung A. Immunomodulatory treatment in children with steroid‐dependent/steroid‐resistant nephrotic syndrome [abstract]. European Journal of Clinical Investigation 1990;20 (2 Pt II):A 33. [CENTRAL: CN‐00253605] [Google Scholar]
- Kano K, Nishikura K, Yamada Y, Arisaka O. Effect of fluvastatin and dipyridamole on proteinuria and renal function in childhood IgA nephropathy with mild histological findings and moderate proteinuria. Clinical Nephrology 2003;60(2):85‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]; Kano K, Nishikura K, Yamada Y, Arisaka O. Effect of fluvastatin and dipyridamole on proteinuria and renal function in childhood IgA nephropathy with mild histological findings and moderate proteinuria [abstract no: T756‐757]. Nephrology Dialysis Transplantation 2003;18(Suppl 4):524‐5. [DOI] [PubMed] [Google Scholar]; Kano K, Nishikura K, Yamada Y, Arisaka O. Effect of fluvastatin on proteinuria [abstract no: M‐PO20068]. Nephrology 2005;10(Suppl 1):A33. [CENTRAL: CN‐00774540] [Google Scholar]; Kano K, Nishikura K, Yamada Y, Arisaka O. No effect of fluvastatin on the bone mineral density of children with minimal change glomerulonephritis and some focal mesangial cell proliferation, other than an ameliorating effect on their proteinuria. Clinical Nephrology 2005;63(2):74‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Koshikawa S. Clinical evaluation of an immunosuppressive drug, mizoribine (HE‐69) on steroid resistant nephrotic syndrome ‐ a multicenter double‐blind comparison study with placebo. Jin to Toseki [Kidney and Dialysis] 1993;34:631‐50. [CENTRAL: CN‐00602134] [Google Scholar]
- Kumar NS, Mishra RN, Singh AK, Prakash J. Effect of ace inhibitor and calcium channel blocker on proteinuria in subjects with steroid resistant idiopathic nephrotic syndrome [abstract]. Indian Journal of Nephrology 2001;11(3):110‐1. [CENTRAL: CN‐00461120] [Google Scholar]; Kumar NS, Singh AK, Mishra RN, Prakash J. Comparative study of angiotensin converting enzyme inhibitor and calcium channel blocker in the treatment of steroid‐resistant idiopathic nephrotic syndrome. Journal of the Association of Physicians of India 2004;52:454‐8. [MEDLINE: ] [PubMed] [Google Scholar]
- Li X, He Q, Lin W, Wang S, Chen J. Therapy of tacrolimus in steroid‐resistant minimal‐change nephrotic syndrome: a randomized controlled clinical trial [abstract no: F‐PO1105]. Journal of the American Society of Nephrology 2006;17(Abstracts):569A. [Google Scholar]
- Ren HQ, Zhong YF, Li Y, Cai Q, Han SJ, Hao XK, et al. Low‐dose tacrolimus combined with tripterygium in treatment of steroid‐resistant nephrotic syndrome: a prospective randomized controlled trial. Academic Journal of Second Military Medical University 2011;32(12):1340‐5. [EMBASE: 2011698533] [Google Scholar]
- Ren H, Shen P, Li X, Pan X, Zhang W, Chen N. Tacrolimus versus cyclophosphamide in steroid‐dependent or steroid‐resistant focal segmental glomerulosclerosis: a randomized controlled trial. American Journal of Nephrology 2013;37(1):84‐90. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Saito T, Iwano M, Matsumoto K, Mitarai T, Yokoyama H, Yorioka N, et al. Significance of combined cyclosporine‐prednisolone therapy and cyclosporine blood concentration monitoring for idiopathic membranous nephropathy with steroid‐resistant nephrotic syndrome: a randomized controlled multicenter trial. Clinical & Experimental Nephrology 2014;18(5):784‐94. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]; Saito T, Mitarai T, Yokoyama H, Yorioka N, Iwano M, Nishi S, et al. Effect of preprandial once‐a‐day administration of cyclosporine (CyA) for steroid resistant nephrotic syndrome (SRNS) [abstract no: SA‐PO997]. Journal of the American Society of Nephrology 2007;18(Abstracts):562A. [Google Scholar]; Saito T, Watanabe M, Ogahara S, Shuto H, Kataoka Y. Significance of blood concentration of cyclosporine at 2 hours after administration for the treatment of idiopathic membranous nephropathy with steroid resistant nephrotic syndrome [abstract no: SA285]. World Congress of Nephrology; 2009 May 22‐26; Milan, Italy. 2009. [Google Scholar]
- Shibasaki T, Koyama A, Hishida A, Muso E, Osawa G, Yamabe H, et al. A randomized open‐label comparative study of conventional therapy versus mizoribine onlay therapy in patients with steroid‐resistant nephrotic syndrome (postmarketing survey). Clinical & Experimental Nephrology 2004;8(2):117‐26. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Walker RG, Kincaid‐Smith P. Cyclosporin a (Cy‐A) treatment in focal and segmental hyalinosis and sclerosis (FSHS): a controlled trial [abstract no: 17]. Kidney International 1989;36(6):1162. [CENTRAL: CN‐00509552] [Google Scholar]; Walker RG, Kincaid‐Smith P. The effect of treatment of corticosteroid‐resistant idiopathic (primary) focal and segmental hyalinosis and sclerosis (focal glomerulosclerosis) with ciclosporin. Nephron 1990;54(2):117‐21. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Zhao K, Li Q, Ma Q, Zhang L, Duan Y. Treatment with tacrolimus and prednisone is preferable to intravenous cyclophosphamide for children with difficult‐to‐treat nephrotic syndrome [abstract no: P‐SUN205]. Pediatric Nephrology 2013;28(8):1601‐2. [EMBASE: 71127684] [Google Scholar]
References to ongoing studies
- Trachtman H. Efficacy and safety of RE‐021, a dual endothelin receptor and angiotensin receptor blocker, in patients with focal segmental glomerulosclerosis (FSGS): a randomized, double‐blind, active‐control, dose‐escalation study. www.clinicaltrials.gov/ct2/show/NCT01613118 (accessed 2 March 2016).
- Basu B. Efficacy and safety of rituximab to that of calcineurin inhibitors in children with steroid resistant nephrotic syndrome. www.clinicaltrials.gov/ct2/show/NCT023825752015; Vol. (accessed 2 March 2016).
- Ghiggeri GM. Ofatumumab in children with steroid‐ and calcineurin‐inhibitor‐resistant nephrotic syndrome: a double‐blind randomized, controlled, superiority trial. www.clinicaltrials.gov/ct2/show/NCT023941062015; Vol. (accessed 2 March 2016).
Additional references
- Chua A, Yorgin P. Steroid‐Resistant Nephrotic Syndrome. In: Molony DA, Craig JC editor(s). Evidence‐Based Nephrology. Wiley‐Blackwell, 2009. [Google Scholar]
- Colquitt JL, Kirby J, Green C, Cooper K, Trompeter RS. The clinical effectiveness and cost‐effectiveness of treatments for children with idiopathic steroid‐resistant nephrotic syndrome: a systematic review. Health Technology Assessment (Winchester, England) 2007;11(21):1‐93. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Deegens JK, Wetzels JF. Immunosuppressive treatment of focal and segmental glomerulosclerosis: lessons from a randomized controlled trial. Kidney International 2011;80(8):798‐801. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ding WY, Koziell A, McCarthy HJ, Bierzynska A, Bhagavatula MK, Dudley JA, et al. Initial steroid sensitivity in children with steroid‐resistant nephrotic syndrome predicts post‐transplant recurrence. Journal of the American Society of Nephrology 2014;25(6):1342–8. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Egger M, Davey‐Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple graphical test. BMJ 1997;315(7109):629‐34. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ehrich JH, Geerlings C, Zivicnjak M, Franke D, Geerlings H, Gellerman J. Steroid‐resistant idiopathic childhood nephrosis: overdiagnosed and undertreated. Nephrology Dialysis Transplantation 2007;22(8):2183‐93. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bakkali L, Rodrigues Pereira R, Kuik DJ, Ket JC, Wijk JA. Nephrotic syndrome in The Netherlands: a population‐based cohort study and a review of the literature. Pediatric Nephrology 2011;26(8):1241‐6. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gipson DS, Chin H, Presler TP, Jennette C, Ferris ME, Massengill S, et al. Differential risk of remission and ESRD in childhood FSGS. Pediatric Nephrology 2006;21(3):344‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck‐Ytter Y, Alonso‐Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336(7650):924‐6. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hari P, Bagga A, Jindal N, Srivastava RN. Treatment of focal glomerulosclerosis with pulse steroids and oral cyclophosphamide. Pediatric Nephrology 2001;16(11):901‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
- Hollis S, Cambell F. What is meant by intention to treat analysis? Survey of published randomised controlled trials. BMJ 1999;319(7211):670‐4. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anonymous. The primary nephrotic syndrome in children. Identification of patients with minimal change nephrotic syndrome from initial response to prednisone. A report of the International Study of Kidney Disease in Children. Journal of Pediatrics 1981;98(4):561‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Koskimies O, Vilska J, Rapola J, Hallman N. Long‐term outcome of primary nephrotic syndrome. Archives of Disease in Childhood 1982;57(7):544‐8. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lombel RM, Hodson EM, Gipson DS, Kidney Disease: Improving Global Outcomes. Treatment of steroid‐resistant nephrotic syndrome in children: new guidelines from KDIGO. Pediatric Nephrology 2013;28(3):409‐14. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta‐analyses?. Lancet 1998;352(9128):609‐13. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Niaudet P. Comparison of cyclosporin and chlorambucil in the treatment of steroid‐dependent idiopathic nephrotic syndrome: a multicentre randomized controlled trial. Pediatric Nephrology 1992;6(1):1‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Niaudet P. Treatment of childhood steroid‐resistant idiopathic nephrosis with a combination of cyclosporine and prednisone. French Society of Pediatric Nephrology. Journal of Pediatrics 1994;125(6 Pt 1):981‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ponticelli C, Edefonti A, Ghio L, Rizzoni G, Rinaldi S, Gusmano R, et al. Cyclosporin versus cyclophosphamide for patients with steroid‐dependent and frequently relapsing idiopathic nephrotic syndrome: a multicentre randomized controlled trial. Nephrology Dialysis Transplantation 1993;8(12):1326‐32. [MEDLINE: ] [PubMed] [Google Scholar]
- Sadowski CE, Lovric S, Ashraf S, Pabst WL, Gee HY, Kohl S, et al. A single‐gene cause in 29.5% of cases of steroid‐resistant nephrotic syndrome. Journal of the American Society of Nephrology 2015;26(6):1279‐89. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias: dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273(5):408‐12. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Schünemann HJ, Oxman AD, Higgins JP, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and 'Summary of findings' tables. In: Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
- Schünemann HJ, Oxman AD, Higgins JP, Deeks JJ, Glasziou P, Guyatt GH. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
- Sureshkumar P, Hodson EM, Willis NS, Barzi F, Craig JC. Predictors of remission and relapse in idiopathic nephrotic syndrome: a prospective cohort study. Pediatric Nephrology 2014;29(6):1039‐46. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Trautmann A, Bodria M, Ozaltin F, Gheisari A, Melk A, Azocar M, et al. Spectrum of steroid‐resistant and congenital nephrotic syndrome in children: the PodoNet registry cohort. Clinical Journal of The American Society of Nephrology: CJASN 2015;10(4):592‐600. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tune BM, Kirpekar R, Sibley RK, Reznik VM, Griswold WR, Mendoza SA. Intravenous methylprednisolone and oral alkylating agent therapy of prednisone‐resistant pediatric focal segmental glomerulosclerosis: a long‐term follow‐up. Clinical Nephrology 1995;43(2):84‐8. [MEDLINE: ] [PubMed] [Google Scholar]
- Tune BM, Lieberman E, Mendoza SA. Steroid‐resistant nephrotic focal segmental glomerulosclerosis: a treatable disease. Pediatric Nephrology 1996;10(6):772‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Wong W. Idiopathic nephrotic syndrome in New Zealand children, demographic, clinical features, initial management and outcome after twelve‐month follow‐up: results of a three‐year national surveillance study. Journal of Paediatrics & Child Health 2007;43(5):337‐41. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
- Habashy D, Hodson E, Craig J. Interventions for idiopathic steroid‐resistant nephrotic syndrome in children. Cochrane Database of Systematic Reviews 2001, Issue 2. [DOI: 10.1002/14651858.CD003594] [DOI] [PubMed] [Google Scholar]
- Habashy D, Hodson EM, Craig JC. Interventions for steroid‐resistant nephrotic syndrome: a systematic review. Pediatric Nephrology 2003;18(9):906‐12. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Habashy D, Hodson E, Craig J. Interventions for idiopathic steroid‐resistant nephrotic syndrome in children. Cochrane Database of Systematic Reviews 2004, Issue 3. [DOI: 10.1002/14651858.CD003594.pub2] [DOI] [PubMed] [Google Scholar]
- Habashy D, Hodson E, Craig J. Interventions for idiopathic steroid‐resistant nephrotic syndrome in children. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD003594.pub3] [DOI] [PubMed] [Google Scholar]
- Hodson EM, Willis NS, Craig JC. Interventions for idiopathic steroid‐resistant nephrotic syndrome in children. Cochrane Database of Systematic Reviews 2010, Issue 11. [DOI: 10.1002/14651858.CD003594.pub4] [DOI] [PubMed] [Google Scholar]