

Abstract
Background
Although often considered to be lacking adequate evidence, nonsteroidal anti‐inflammatory drugs (NSAIDs) are widely used in the management of neuropathic pain. Previous surveys found 18% to 47% of affected people reported using NSAIDs specifically for their neuropathic pain, although possibly not in the United Kingdom (UK).
Objectives
To assess the analgesic efficacy of oral NSAIDs for chronic neuropathic pain in adults, when compared to placebo or another active intervention, and the adverse events associated with its use in clinical trials.
Search methods
We searched CENTRAL, MEDLINE, and EMBASE from inception to 29 May 2015, together with reference lists of retrieved papers and reviews, and an online trials registry.
Selection criteria
We included randomised, double‐blind studies of two weeks duration or longer, comparing any oral NSAID with placebo or another active treatment in chronic neuropathic pain.
Data collection and analysis
Two review authors independently searched for studies, extracted efficacy and adverse event data, and examined issues of study quality. We did not carry out any pooled analysis.
Main results
We included two studies involving 251 participants with chronic low back pain with a neuropathic component or postherpetic neuralgia; 209 of these participants were involved in a study of an experimental NSAID not used in clinical practice, and of the remaining 42, only 16 had neuropathic pain. This represented only third tier evidence, and was of very low quality. There was no indication of any significant pain reduction with NSAIDs. Adverse event rates were low, with insufficient events for any analysis.
Authors' conclusions
There is no evidence to support or refute the use of oral NSAIDs to treat neuropathic pain conditions.
Plain language summary
Oral nonsteroidal anti‐inflammatory drugs (NSAIDs) for neuropathic pain in adults
Neuropathic pain is pain which comes from damaged nerves, spinal cord, or brain. It is different from pain messages that are carried along healthy nerves from damaged tissue (for example, a fall or cut, or arthritic knee). Neuropathic pain is treated by different medicines to those used for pain from damaged tissue. Medicines that are sometimes used to treat depression or epilepsy can be very effective in some people with neuropathic pain.
Commonly used painkillers such as ibuprofen (a nonsteroidal anti‐inflammatory drug, or NSAID) are not usually considered to be effective in treating neuropathic pain, but in some parts of the world they are used commonly for neuropathic pain conditions.
In May 2015 we searched for clinical trials in which oral NSAIDs were used to treat neuropathic pain in adults. We found only two small studies that included 251 participants who had chronic low back pain with a neuropathic component, or had neuropathic pain after shingles. Of these 251 participants, 209 were in a study of an experimental drug that is not licensed and not available for use.
The trial results show that there was no difference between NSAIDs and placebo in terms of pain or adverse events (very low quality evidence). There is no good evidence to tell us whether or not oral NSAIDs are helpful to treat neuropathic pain conditions.
Background
The protocol for this review was based on a template for reviews of drugs used to relieve neuropathic pain. The aim was for all reviews to use the same methods, based on new criteria for what constitutes reliable evidence in chronic pain (Moore 2010a; Moore 2012a; Appendix 1).
Description of the condition
The 2011 International Association of the Study of Pain definition of neuropathic pain is "pain caused by a lesion or disease of the somatosensory system" (Jensen 2011), based on an earlier consensus meeting (Treede 2008). Neuropathic pain is a consequence of a pathological maladaptive response of the nervous system to 'damage' from a wide variety of potential causes. It is characterised by pain in the absence of a noxious stimulus and may be spontaneous (continuous or paroxysmal) in its temporal characteristics or be evoked by sensory stimuli (dynamic mechanical allodynia where pain is evoked by light touch of the skin). Neuropathic pain is associated with a variety of sensory loss (numbness) and sensory gain (allodynia) clinical phenomena, the exact pattern of which vary between patient and disease, perhaps reflecting different pain mechanisms operating in an individual patient and therefore potentially predictive of response to treatment (Demant 2014; Helfert 2015; von Hehn 2012). Pre‐clinical research hypothesises a bewildering array of possible pain mechanisms that may operate in people with neuropathic pain, which largely reflect pathophysiological responses in both the central and peripheral nervous systems, including neuronal interactions with immune cells (Baron 2012; Calvo 2012; von Hehn 2012). Overall, the treatment gains in neuropathic pain, to even the most effective of available drugs, are modest (Finnerup 2015; Moore 2013a), and a robust classification of neuropathic pain is not yet available (Finnerup 2013).
Neuropathic pain is usually divided according to the cause of nerve injury. There may be many causes, but some common causes of neuropathic pain include diabetes (painful diabetic neuropathy (PDN)), shingles (postherpetic neuralgia (PHN)), amputation (phantom limb pain), neuropathic pain after surgery or trauma, stroke or spinal cord injury, trigeminal neuralgia, and human immunodeficiency virus (HIV) infection.
Many people with neuropathic pain conditions are significantly disabled with moderate or severe pain for many years. Chronic pain conditions comprised five of the 11 top‐ranking conditions for years lived with disability in 2010 (Vos 2012), and are responsible for considerable loss of quality of life, employment, and increased healthcare costs (Moore 2014a).
In systematic reviews, the overall prevalence of neuropathic pain in the general population is reported to be between 7% and 10% (van Hecke 2014), and about 7% in a systematic review of studies published since 2000 (Moore 2014a). In individual countries, prevalence rates have been reported as 3.3% in Austria (Gustorff 2008), 6.9% in France (Bouhassira 2008), and up to 8% in the UK (Torrance 2006). Some forms of neuropathic pain, such as PDN and post‐surgical chronic pain (which is often neuropathic in origin), are increasing (Hall 2008). The prevalence of PHN is likely to fall if vaccination against the herpes virus becomes widespread.
Estimates of incidence vary between individual studies for particular origins of neuropathic pain, often because of small numbers of cases. In primary care in the UK between 2002 and 2005, the incidences (per 100,000 person‐years' observation) were 28 (95% confidence interval (CI) 27 to 30) for PHN, 27 (26 to 29) for trigeminal neuralgia, 0.8 (0.6 to 1.1) for phantom limb pain, and 21 (20 to 22) for PDN (Hall 2008). However, the incidence of trigeminal neuralgia has also been estimated at 4 in 100,000 per year (Katusic 1991; Rappaport 1994), and 12.6 per 100,000 person‐years for trigeminal neuralgia and 3.9 per 100,000 person‐years for PHN in a study of facial pain in the Netherlands (Koopman 2009). One systematic review of chronic pain demonstrated that some neuropathic pain conditions, such as PDN, can be more common than other neuropathic pain conditions, with prevalence rates up to 400 per 100,000 person‐years (McQuay 2007).
Neuropathic pain is known to be difficult to treat effectively, with only a minority of individuals experiencing a clinically relevant benefit from any one intervention. A multidisciplinary approach is now advocated, with pharmacological interventions being combined with physical or cognitive interventions, or both. Conventional analgesics are usually not effective, but without evidence to support or refute that view. Some people with neuropathic pain may derive some benefit from a topical lidocaine patch or low concentration topical capsaicin, though evidence about benefits is uncertain (Derry 2012; Derry 2014). High concentration topical capsaicin may benefit some people with PHN (Derry 2013). Treatment for neuropathic pain is more usually by so‐called unconventional analgesics (pain modulators) such as antidepressants like duloxetine and amitriptyline (Lunn 2014; Moore 2012b; Sultan 2008), or antiepileptics like gabapentin or pregabalin (Moore 2009; Moore 2014b; Wiffen 2013).
The proportion of people who achieve worthwhile pain relief (typically at least 50% pain intensity reduction; Moore 2013b) is small, generally only 10% to 25% more than with placebo, with numbers needed to treat for an additional beneficial outcome (NNT) usually between 4 and 10 (Kalso 2013; Moore 2013a). Neuropathic pain is not particularly different from other chronic pain conditions in that only a small proportion of trial participants have a good response to treatment (Moore 2013a).
The current National Institute for Health and Care Excellence (NICE) guidance suggests offering a choice of amitriptyline, duloxetine, gabapentin, or pregabalin as initial treatment for neuropathic pain (with the exception of trigeminal neuralgia), with switching if first, second, or third drugs tried are not effective or not tolerated (NICE 2013). This concurs with other recent guidance (Finnerup 2015).
Description of the intervention
Nonsteroidal anti‐inflammatory drugs (NSAIDs) are the most commonly used analgesics in general (Laine 2001). NSAIDs act by inhibiting the cyclooxygenases (COXs), which synthesise prostaglandins that are involved in inflammation and pain. The analgesic and anti‐inflammatory actions of NSAIDs are attributed to the inhibition of cyclooxygenase‐2 (COX‐2), while their adverse gastrointestinal effects are attributed to the inhibition of cyclooxygenase‐1 (COX‐1). Traditional NSAIDs such as ibuprofen are non‐selective. COX‐2‐selective NSAIDs were thus developed to reduce adverse gastrointestinal effects, but were later found to increase the risk of myocardial infarction and stroke. Therefore, rofecoxib and valdecoxib have been withdrawn from the market (EMEA 2005; FDA 2004). However, some traditional NSAIDs with relative selectivity for COX‐2 were also found to increase the risk of myocardial infarction (Grosser 2011).
How the intervention might work
One current hypothesis is that damage to the peripheral nerves is followed by an inflammatory reaction that relates to increased production of prostaglandins, amplifying sodium currents and calcium influx in peripheral nociceptive neurons, and enhancing neurotransmitter release in the central nervous system and depolarisation of second‐order nociceptive neurons (Vo 2009). Preclinical data suggest an immune pathogenesis of neuropathic pain, but clinical evidence of a central role of the immune system is less clear (Calvo 2012). NSAIDs inhibit the production of prostaglandins, and thus could lessen the peripheral and central sensory hypersensitivity that occurs with nerve injury‐associated inflammation. NSAIDs have been shown to reduce sensory hypersensitivity in animal models (Hasnie 2007; Kawakami 2002).
Why it is important to do this review
Although often considered to lack adequate evidence, NSAIDs are widely used in the management of neuropathic pain (Di Franco 2010; Vo 2009). Previous surveys found 18% to 47% of affected people reported using NSAIDs specifically for their neuropathic pain (Vo 2009), although possibly not in the UK (Hall 2013). It is therefore desirable to assess the best evidence on the efficacy and safety of NSAIDs in managing neuropathic pain. In chronic pain generally, and neuropathic pain in particular, few drugs produce the good level of pain relief that patients want in more than a minority of patients (Moore 2013a), which makes proper review of efficacy and harm important. This review will assist policy makers, physicians, and consumers to make decisions regarding the use of NSAIDs in managing neuropathic pain.
The standards used to assess evidence in chronic pain trials have changed substantially, with particular attention being paid to trial duration, withdrawals, and statistical imputation following withdrawal, all of which can substantially alter estimates of efficacy. The most important change is the move from using average pain scores, or average change in pain scores, to the number of patients who have a large decrease in pain (by at least 50%); this level of pain relief has been shown to correlate with improvements in comorbid symptoms, function, and quality of life.
Trials included and analysed needed to meet a minimum of reporting quality (blinding, randomisation), validity (duration, dose and timing, diagnosis, outcomes, etc) and size (ideally at least 500 participants in a comparison in which the NNT is 4 or above) (Moore 1998; Moore 2010a). This sets high standards and marks a departure from how systematic reviews have been conducted previously. These standards have been set out in the authors' reference guide for the Cochrane Pain, Palliative, and Supportive Care Review Group (Cochrane PaPaS Group 2012). This Cochrane systematic review used the standards to assess evidence and take both statistical and clinical significance into consideration, in order to provide an overview of the analgesic efficacy and safety of NSAIDs for neuropathic pain.
Objectives
To assess the analgesic efficacy of oral nonsteroidal anti‐inflammatory drugs (NSAIDs) for chronic neuropathic pain in adults, when compared to placebo or another active intervention, and the adverse events associated with its use in clinical trials.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) with double‐blind assessment of participant outcomes following two weeks of treatment or longer, although the emphasis of the review was on studies of eight weeks or longer. We required full journal publication, with the exception of online clinical trial results summaries of otherwise unpublished clinical trials, and abstracts with sufficient data for analysis. We did not include short abstracts (usually reports of meetings). We excluded studies that were non‐randomised, studies of experimental pain, case reports and clinical observations.
Types of participants
Studies included adult participants aged 18 years and above. Participants had one or more of a wide range of chronic neuropathic pain conditions including:
cancer‐related neuropathy;
central neuropathic pain;
complex regional pain syndrome (CRPS) Type II;
human immunodeficiency virus (HIV) neuropathy;
painful diabetic neuropathy (PDN);
phantom limb pain;
postherpetic neuralgia (PHN);
postoperative or traumatic neuropathic pain;
spinal cord injury;
trigeminal neuralgia.
Where studies included participants with more than one type of neuropathic pain, we planned to analyse results according to the primary condition.
Types of interventions
We included studies using NSAIDs at any dose, by oral route, administered for the relief of neuropathic pain and compared to placebo or any active comparator (for example, another NSAID).
Types of outcome measures
We anticipated that studies would use a variety of outcome measures, with the majority of studies using standard subjective scales (numerical rating scale (NRS) or visual analogue scale (VAS)) for pain intensity or pain relief, or both. We were particularly interested in the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) definitions for moderate and substantial benefit in chronic pain studies (Dworkin 2008). These are defined as at least 30% pain relief over baseline (moderate), at least 50% pain relief over baseline (substantial), much or very much improved on Patient Global Impression of Change (PGIC) (moderate), and very much improved on PGIC (substantial). These outcomes are different from those used in most earlier reviews (Seidel 2013), concentrating as they do on dichotomous outcomes where pain responses do not follow a normal (Gaussian) distribution. People with chronic pain desire high levels of pain relief, ideally more than 50%, and with pain not worse than mild (O'Brien 2010). Our preferred time point of outcome measures was at week 12, which is considered a standard measurement point and is typically required by regulatory bodies (Moore 2010a). However, we anticipated that there would be very limited data, and have included studies that reported outcomes at other time points, from two weeks onwards.
We planned to include a 'Summary of findings' table as set out in the author guide (Cochrane PaPaS Group 2012). We have not included a 'Summary of findings' table because there was no useful information to include.
Primary outcomes
Patient‐reported pain relief of 30% or greater
Patient‐reported pain relief of 50% or greater
PGIC much or very much improved
PGIC very much improved
Secondary outcomes
Any pain‐related outcome indicating some improvement
Withdrawals due to lack of efficacy
Participants experiencing any adverse event
Participants experiencing any serious adverse event. Serious adverse events typically include any untoward medical occurrence or effect that at any dose results in death, is life‐threatening, requires hospitalisation or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, is a congenital anomaly or birth defect, is an 'important medical event' that may jeopardise the patient, or may require an intervention to prevent one of the above characteristics/consequences.
Withdrawals due to adverse events
Specific adverse events, particularly somnolence and dizziness
Search methods for identification of studies
Electronic searches
We searched the following databases, without language restrictions.
Cochrane Central Register of Controlled Trials (CENTRAL, via the Cochrane Register of Studies Online database (CRSO)) to 29 May 2015.
MEDLINE (via Ovid) from 1946 to 29 May 2015.
EMBASE (via Ovid) from 1974 to 29 May 2015.
The search strategies for CENTRAL, MEDLINE, and EMBASE are listed in Appendix 2, Appendix 3, and Appendix 4, respectively.
Searching other resources
We reviewed the bibliographies of identified RCTs and review articles, contacted authors and known experts in the field, and searched ClinicalTrials.gov (ClinicalTrials.gov) and World Health Organization International Clinical Trials Registry Platform (ICTRP) (apps.who.int/trialsearch/) to identify additional published or unpublished data.
Data collection and analysis
We have included a Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flow chart (Liberati 2009).
Selection of studies
We determined eligibility by reading the abstract of each study identified by the search. We eliminated studies that clearly did not satisfy inclusion criteria, and we obtained full copies of the remaining studies. Two review authors read these studies independently and reached agreement by discussion. We did not anonymise the studies in any way before assessment.
Data extraction and management
Two review authors independently extracted data using a standard form and checked for agreement before entry into the Cochrane Collaboration's statistical software, Review Manager 2014, or any other analytical tool. We included information about the pain condition and number of participants treated, drug and dosing regimen, study design (placebo or active control), study duration and follow‐up, analgesic outcome measures and results, withdrawals and adverse events (participants experiencing any adverse event, or a serious adverse event).
Assessment of risk of bias in included studies
We used the Oxford Quality Score as the basis for inclusion, limiting inclusion to studies that were randomised and double‐blind as a minimum (Jadad 1996).
Two authors independently assessed the risk of bias in each study, using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), and adapted from those used by the Cochrane Pregnancy and Childbirth Group, with any disagreements resolved by discussion.
We assessed the following for each study.
Random sequence generation (checking for possible selection bias). We assessed the method used to generate the allocation sequence as: low risk of bias (any truly random process, eg random number table; computer random number generator); unclear risk of bias (method used to generate sequence not clearly stated). We excluded studies using a non‐random process (eg odd or even date of birth; hospital or clinic record number).
Allocation concealment (checking for possible selection bias). The method used to conceal allocation to interventions prior to assignment determines whether intervention allocation could have been foreseen in advance of, or during, recruitment, or changed after assignment. We assessed the methods as: low risk of bias (eg telephone or central randomisation; consecutively numbered sealed opaque envelopes); unclear risk of bias (method not clearly stated). We excluded studies that did not conceal allocation and were, therefore, at a high risk of bias (open list) (eg open list).
Blinding of outcome assessment (checking for possible detection bias). We assessed the methods used to blind study participants and outcome assessors from knowledge of which intervention a participant received. We assessed the methods as: low risk of bias (study stated that it was blinded and described the method used to achieve blinding, eg identical tablets; matched in appearance and smell); unclear risk of bias (study stated that it was blinded but did not provide an adequate description of how it was achieved). We excluded studies that were not double‐blind.
Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data). We assessed the methods used to deal with incomplete data as: low risk (less than 10% of participants did not complete the study and/or used 'baseline observation carried forward' analysis); unclear risk of bias (used 'last observation carried forward' analysis); high risk of bias (used 'completer' analysis).
Size of study (checking for possible biases confounded by small size). We assessed studies as being at low risk of bias (200 or more participants per treatment arm); unclear risk of bias (50 to 199 participants per treatment arm); high risk of bias (fewer than 50 participants per treatment arm).
Measures of treatment effect
We planned to calculate the NNT as the reciprocal of the absolute risk reduction (ARR) (McQuay 1998). For unwanted effects, the NNT would became the number needed to treat to harm (NNH) and be calculated in the same manner. We planned to use dichotomous data to calculate risk ratio (RR) with 95% confidence intervals (CIs) using a fixed‐effect model unless we found significant statistical heterogeneity (Assessment of heterogeneity). We would not use continuous data in analyses. In the event, we did not carry out any analysis.
Unit of analysis issues
We accepted randomisation to individual participant only. The control treatment arm would be split between active treatment arms in a single study if the active treatment arms were not combined for analysis.
Dealing with missing data
We planned to use an intention‐to‐treat (ITT) analysis where the ITT population consisted of participants who were randomised, took at least one dose of the assigned study medication, and provided at least one post‐baseline assessment. Missing participants would be assigned zero improvement where possible. In the event, we did not carry out any analysis.
Assessment of heterogeneity
We planned to deal with clinical heterogeneity by combining studies that examined similar conditions. We planned to assess statistical heterogeneity visually (L'Abbé 1987), and using the I2 statistic. When the I2 value was greater than 50%, we intended to consider possible reasons for this. There were insufficient data to carry out any assessment of heterogeneity.
Assessment of reporting biases
The aim of this review was to use dichotomous data of known utility (Moore 2010d). The review did not depend on what authors of the original studies chose to report or not, although clearly difficulties arose if studies failed to report dichotomous results.
We planned to assess publication bias using a method designed to detect the amount of unpublished data with a null effect required to make any result clinically irrelevant (usually taken to mean an NNT of 10 or higher) (Moore 2008). In the event there were insufficient data to assess publication bias.
Data synthesis
We planned to analyse according to individual painful conditions, because placebo response rates with the same outcome can vary between conditions, as can the drug‐specific effects (Moore 2009a). We would use a fixed‐effect model for meta‐analysis, but planned to use a random‐effects model if there was significant clinical heterogeneity and it was considered appropriate to combine studies.
We examined data for each painful condition in three tiers, according to outcome and freedom from known sources of bias.
The first tier used data meeting current best standards, where studies reported the outcome of at least 50% pain intensity reduction over baseline (or its equivalent), without the use of last observation carried forward (LOCF) or other imputation method other than baseline observation carried forward (BOCF) for dropouts, reported an ITT analysis, lasted eight or more weeks, had a parallel‐group design, and had at least 200 participants (preferably at least 400) in the comparison (Moore 2010a; Moore 2012a). We planned to report these top‐tier results first.
The second tier used data from at least 200 participants, but where one or more of the above conditions was not met (for example, reporting at least 30% pain intensity reduction, using LOCF or a completer analysis, or lasting four to eight weeks).
The third tier of evidence used data from fewer than 200 participants, or where there were expected to be significant problems because, for example, of very short duration studies of less than four weeks, where there was major heterogeneity between studies, or where there were shortcomings in allocation concealment, attrition, or incomplete outcome data. For this third tier of evidence, no data synthesis is reasonable, and may be misleading, but an indication of beneficial effects might be possible.
In the event, no pooling of data was possible because there were not at least two studies involving at least 200 participants that reported dichotomous data in any one type of neuropathic pain.
Subgroup analysis and investigation of heterogeneity
We planned to conduct subgroup analyses to investigate heterogeneity according to:
different dosages of NSAIDs;
different time points of outcome measurement.
However, there were insufficient data.
Sensitivity analysis
We planned to conduct a sensitivity analysis by excluding studies with high risk of bias (having one or more domains on the 'Risk of bias' tool judged as 'high risk' as per the guidance provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), with all remaining trials judged at low risk of bias). However, there were insufficient data.
Results
Description of studies
Results of the search
Electronic searches identified 181 records in CENTRAL, 464 in MEDLINE, and 385 in EMBASE. After de‐duplication and screening we retained 10 possible studies for inclusion. Searches of on‐line clinical trial registries identified a further four. Figure 1 shows the flow diagram of study selection. Nine studies did not fulfil the entry criteria and three from ClinicalTrials.gov were either terminated or are still ongoing, but without any results. That left two studies for inclusion (251 participants).
1.
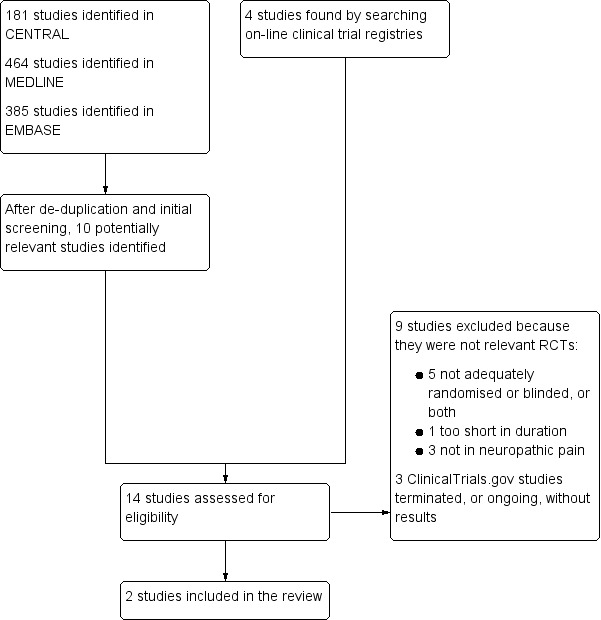
Flow diagram.
Included studies
The two included studies were in back pain, reporting data for participants with pain with a neuropathic component (Romano 2009), or in postherpetic neuralgia (Shackelford 2009). In both cases participants had initial pain of at least moderate severity. Both studies were short duration, of two or three weeks. One examined the effects of celecoxib alone and in combination with pregabalin (Romano 2009), and the other an experimental NSAID, GW406381, at two doses compared with placebo (Shackelford 2009). Together, these studies reported results on 251 participants with neuropathic pain. See Characteristics of included studies.
Excluded studies
We excluded nine studies (Cohen 1987; Dellemijn 1994; Jaffé 1974; Patarica‐Huber 2011; Pop‐Busui 2015; Solak 2007; Videman 1984; Weber 1993; Yu 2008). Reasons for exclusion were that studies were not randomised (Cohen 1987; Pop‐Busui 2015; Solak 2007), not double blind (Patarica‐Huber 2011; Yu 2008), were not conducted in conditions with a clear neuropathic component or where no indication of the presence of neuropathic pain was given (Jaffé 1974; Videman 1984; Weber 1993), or were below the threshold of two weeks of treatment (Dellemijn 1994). See Characteristics of excluded studies.
Risk of bias in included studies
The Oxford Quality scores for the included studies were 3 or 4 out of 5. Neither study described blinding in detail.
Figure 2 shows the 'Risk of bias' summary.
2.
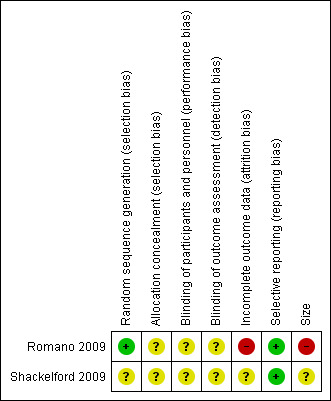
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
One study had low risk of bias for sequence generation (Romano 2009), but there were no details for allocation concealment. The other study did not report methods for either sequence generation or allocation concealment, and was judged to be at unclear risk of bias for this domain (Shackelford 2009.
Blinding
Both studies reported being double blind, but no methods were described.
Incomplete outcome data
One study reported only on completers, and we judged it to be at high risk of bias (Romano 2009). The other used LOCF imputation, and we judged the risk of bias as unclear in the circumstance of a short duration study (Shackelford 2009).
Selective reporting
We found no selective reporting bias.
Other potential sources of bias
Small size was a problem (high risk of bias) for Romano 2009, as it reported on only 16 participants who had a neuropathic component to their pain according to the study's strict diagnostic criteria. The other study had around 70 participants per group, and we judged that study to be at unclear risk of bias for this domain (Shackelford 2009).
Effects of interventions
Efficacy of NSAIDs
Given the small number of studies and the small size of the studies, there was no top tier evidence, and no second tier evidence. Only third tier evidence was available. We present efficacy results for the studies in Appendix 5.
Romano 2009 reported only on pre‐treatment and 4‐week post‐treatment with a celecoxib dose of 3 to 6 mg/kg/day (200 to 400 mg daily) in 16 participants with chronic low back pain and a Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) score of 12 and above. The mean pre‐treatment pain score was 47/100 mm, and the mean post‐treatment score was 46/100 mm. By contrast, the post‐treatment score was significantly reduced with both pregabalin and pregabalin plus celecoxib.
Shackelford 2009 reported on 25 mg and 50 mg of an experimental NSAID, GW406381, compared with placebo over three weeks of treatment in 209 participants with postherpetic neuralgia. For no outcome was there a statistically significant difference between GW406381 and placebo.
Adverse events and withdrawals
There were too few data to draw any conclusions about adverse events and withdrawals, details of which are in Appendix 6. There were numerically slightly more adverse events and withdrawals with GW406381 than with placebo in Shackelford 2009.
Serious adverse events were reported in 4/143 participants with GW406381 and none with placebo (Shackelford 2009). No deaths were reported in either study.
Discussion
Summary of main results
The main result was that there was no useful information to make judgements about the efficacy or safety of oral NSAIDs in treating neuropathic pain in general, or for any specific neuropathic pain condition. Only 225 participants in two included studies provided any information, and only 16 for an NSAID (celecoxib) likely to be used in clinical practice.
Romano 2009 defined neuropathic pain on the basis of Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) score. There are difficulties with the case definition of neuropathic pain used in this study, and we are uncertain that the use of the LANSS scale alone is adequately able to distinguish a neuropathic component from the pain originating from other sources. We are uncertain concerning the hypothetical scenario of a patient with LANSS score greater than 12 but who could quite conceivably have a combination of non‐neuropathic and neuropathic pain (ie, a high LANSS score might identify a case of neuropathic pain, but it does not exclude co‐existent non‐neuropathic pain), especially if these are occurring in the same site. Interpretation of the results is difficult, not just because of the small numbers.
It is worth noting that GW406381, which showed no efficacy in postherpetic neuralgia (Shackelford 2009), did have efficacy in a third molar extraction acute pain model, in migraine, and in osteoarthritis of the knee (Boswell 2008; Varner 2009; Wentz 2008). Despite the drug not being available, therefore, the study provides the best evidence we have that NSAIDs may not be effective in neuropathic pain.
Most of the excluded studies or the ongoing studies would not have provided any additional useful evidence. Patarica‐Huber 2011, in a randomised but open study, found no additional benefit from adding diclofenac to gabapentin in 75 participants with neuropathic pain after anti‐neoplastic therapy for breast cancer.
Overall completeness and applicability of evidence
The evidence available was almost completely irrelevant to clinical practice. NSAIDs were used commonly for treating neuropathic pain in a recent review (Vo 2009), though not apparently in the UK (Hall 2013); the lack of any evidence to support this use is surprising. The striking discrepancy between the widespread use of NSAIDs by patients with neuropathic pain and an apparent consensus among pain specialists that these medications lack efficacy for neuropathic pain is not helped by this review. The absence of any reliable evidence of NSAID efficacy is a challenge to their continued widespread use.
Quality of the evidence
The quality of the evidence was poor. We identified two studies, only one of which used an intervention that is available, and only 16 participants in that study met our inclusion criteria. The study did not report any of our primary outcomes, which are of known clinical validity, but reported group mean results for an outcome that does not as a rule have a Gaussian distribution.
Potential biases in the review process
We know of no potential biases in the review process. We carried out a comprehensive search of the databases most likely to include relevant studies, and together with our own and our colleagues' knowledge of this treatment area, we consider it unlikely that there is a large body of unidentified or unpublished evidence showing a large effect from oral NSAIDs.
Agreements and disagreements with other studies or reviews
The results of this review, which show very little evidence concerning NSAIDs in neuropathic pain, reflect those of a similar previous review (Vo 2009). Neither the current NICE guidance, nor a large systematic review of pharmacotherapy for this population, mention using NSAIDs for neuropathic pain (Finnerup 2015; NICE 2013).
Authors' conclusions
Implications for practice.
For people with neuropathic pain
There is insufficient evidence to support or refute the suggestion that oral NSAIDs have any efficacy in any neuropathic pain condition.
For clinicians
There is insufficient evidence to support or refute the suggestion that oral NSAIDs have any efficacy in any neuropathic pain condition. The absence of any reliable evidence of oral NSAID efficacy is a challenge to their continued widespread use.
For policy makers
There is insufficient evidence to support or refute the suggestion that oral NSAIDs have any efficacy in any neuropathic pain condition, and in the absence of any supporting evidence they should probably not be recommended.
For funders
There is insufficient evidence to support or refute the suggestion that oral NSAIDs have any efficacy in any neuropathic pain condition.
Implications for research.
General
Large, robust randomised trials with patient‐centred outcomes would be required to produce evidence to support or refute efficacy of NSAIDs in neuropathic pain.
Design
There are no implications for design of studies.
Measurement (endpoints)
There are no implications for measurement.
Comparison between active treatments
NSAIDs cannot be compared with other treatments for neuropathic pain with established efficacy.
What's new
| Date | Event | Description |
|---|---|---|
| 28 May 2019 | Amended | Contact details updated. |
| 11 October 2017 | Review declared as stable | No new studies likely to change the conclusions are expected. |
History
Protocol first published: Issue 12, 2013 Review first published: Issue 10, 2015
| Date | Event | Description |
|---|---|---|
| 7 June 2017 | Review declared as stable | See Published notes. |
| 14 October 2015 | Amended | One author's affiliations updated. |
| 13 April 2015 | Amended | Change in authorship and title amended. See Acknowledgements and Published notes. |
| 5 February 2014 | Amended | Search strategy amended. |
Notes
The original title was registered (August 2012) as ‘Non steroidal anti‐inflammatory drugs for neuropathic pain and fibromyalgia’ and had 3 authors (RAM, C‐CC, C‐HC). At protocol publication (December 2013), the title had been changed to ‘Nonsteroidal anti‐inflammatory drugs for neuropathic pain’ (in line with PaPaS's decision to split reviews that included both neuropathic pain and fibromyalgia), and there were 4 authors (C‐CC, SHW, LTK, RAM). In April 2015, after discussion with the editors and authors, the authors were changed to RAM, C‐CC, PJW, SD, and ASCR and the title amended to ‘Oral nonsteroidal anti‐inflammatory drugs for neuropathic pain’.
2017
We performed a restricted search in June 2017 and did not find any studies likely to change the conclusions. One study which was ongoing when the last version of the review was published now has results posted (NCT01838044). This multi centre study randomised 180 participants with chronic low back pain with a neuropathic component to pregabalin plus celecoxib or pregabalin plus placebo for up to 10 weeks. The proportion with ≥ 50% reduction in weekly pain with pregabalin plus celecoxib at 10 weeks was 42%, and with pregabalin plus placebo was 38%. For a reduction of ≥ 30% the proportions were 64% and 59%. The modest numbers and unique add‐on design means that these results could not be pooled with those studies already in the review, and the absence of any large effect of celecoxib means that the conclusions would not change. We also identified a second potentially relevant study (Romanò 2009), but it was unclear whether this was either randomised or double blind. If appropriate, we will update the review if new evidence likely to change the conclusions is published, or if standards change substantially which necessitate major revisions.
Romanò CL, Romanò D, Bonora C, Mineo G. Pregabalin, celecoxib, and their combination for treatment of chronic low‐back pain. J Orthop Traumatol. 2009. Dec;10(4):185‐91. doi: 10.1007/s10195‐009‐0077‐z
Acknowledgements
We acknowledge the contribution of Dr Shu‐Hui Wang and Dr Liang Tseng Kuo to previous versions of the protocol.
The Oxford Pain Relief Trust, Oxford, UK and the Chang Gung Memorial Hospital, Chiayi, Taiwan provided institutional support for the review.
The National Institute for Health Research (NIHR) is the largest single funder of the Cochrane Pain, Palliative and Supportive Care Review Group. Disclaimer: the views and opinions expressed herein are those of the authors and do not necessarily reflect those of the NIHR, National Health Service (NHS) or the Department of Health.
Appendices
Appendix 1. Methodological considerations for chronic pain
There have been several recent changes in how the efficacy of conventional and unconventional treatments is assessed in chronic painful conditions. The outcomes are now better defined, particularly with new criteria of what constitutes moderate or substantial benefit (Dworkin 2008); older trials may only report participants with 'any improvement'. Newer trials tend to be larger, avoiding problems from the random play of chance. Newer trials also tend to be longer, up to 12 weeks, and longer trials provide a more rigorous and valid assessment of efficacy in chronic conditions. New standards have evolved for assessing efficacy in neuropathic pain, and we are now applying stricter criteria for the inclusion of trials and assessment of outcomes, and are more aware of problems that may affect our overall assessment.
The following are some of the recent insights that must be considered in this new review.
Pain results tend to have a U‐shaped distribution rather than a bell‐shaped distribution. This is true in acute pain (Moore 2011a; Moore 2011b), back pain (Moore 2010b), and arthritis (Moore 2010c), as well as in fibromyalgia (Straube 2010); in all cases average results usually describe the experience of almost no‐one in the trial. Data expressed as averages are potentially misleading, unless they can be proven to be suitable.
As a consequence, we have to depend on dichotomous results (the individual either has or does not have the outcome) usually from pain changes or patient global assessments. The Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) group has helped with their definitions of minimal, moderate, and substantial improvement (Dworkin 2008). In arthritis, trials shorter than 12 weeks, and especially those shorter than eight weeks, overestimate the effect of treatment (Moore 2009b); the effect is particularly strong for less effective analgesics, and this may also be relevant in neuropathic‐type pain.
The proportion of patients with at least moderate benefit can be small, even with an effective medicine, falling from 60% with an effective medicine in arthritis, to 30% in fibromyalgia (Moore 2009a; Moore 2010c; Straube 2008; Sultan 2008). A Cochrane review of pregabalin in neuropathic pain and fibromyalgia demonstrated different response rates for different types of chronic pain (higher in diabetic neuropathy and postherpetic neuralgia and lower in central pain and fibromyalgia) (Moore 2009a). This indicates that different neuropathic pain conditions should be treated separately from one another, and that pooling should not be done unless there are good grounds for doing so.
Finally, presently unpublished individual patient analyses indicate that patients who get good pain relief (moderate or better) have major benefits in many other outcomes, affecting quality of life in a significant way (Moore 2010d).
Appendix 2. Search strategy for CENTRAL via CRSO
MESH DESCRIPTOR Neuralgia EXPLODE ALL TREES (608)
(nerve adj1 pain*):TI,AB,KY (738)
neuralgia*:TI,AB,KY (1013)
(neuropathic adj1 pain):TI,AB,KY (972)
#1 OR #2 OR #3 OR #4 (2602)
MESH DESCRIPTOR Anti‐Inflammatory Agents, Non‐Steroidal EXPLODE ALL TREES (13455)
NSAID*:TI,AB,KY (2578)
("non‐steroidal anti‐inflammatory drug*"):TI,AB,KY (1200)
acemetacin:TI,AB,KY (88)
MESH DESCRIPTOR Apazone (29)
azapropazone:TI,AB,KY (48)
celecoxib:TI,AB,KY (838)
MESH DESCRIPTOR Indomethacin EXPLODE ALL TREES (1988)
indomet?acin:TI,AB,KY (2554)
MESH DESCRIPTOR ketoprofen EXPLODE ALL TREES (384)
ketoprofen:TI,AB,KY (809)
dexketoprofen:TI,AB,KY (96)
MESH DESCRIPTOR diclofenac EXPLODE ALL TREES (1342)
diclofenac:TI,AB,KY (3143)
MESH DESCRIPTOR etodolac EXPLODE ALL TREES (81)
etodolac:TI,AB,KY (181)
etoricoxib:TI,AB,KY (171)
fenbufen:TI,AB,KY (62)
MESH DESCRIPTOR fenoprofen EXPLODE ALL TREES (36)
fenoprofen:TI,AB,KY (85)
MESH DESCRIPTOR flurbiprofen EXPLODE ALL TREES (338)
flurbiprofen:TI,AB,KY (609)
MESH DESCRIPTOR ibuprofen EXPLODE ALL TREES (1130)
ibuprofen:TI,AB,KY (2391)
MESH DESCRIPTOR mefenamic acid EXPLODE ALL TREES (109)
(mefenamic acid):TI,AB,KY (227)
MESH DESCRIPTOR naproxen EXPLODE ALL TREES (804)
naproxen:TI,AB,KY (1529)
MESH DESCRIPTOR piroxicam EXPLODE ALL TREES (563)
piroxicam:TI,AB,KY (1009)
MESH DESCRIPTOR sulindac EXPLODE ALL TREES (137)
sulindac:TI,AB,KY (274)
tenoxicam:TI,AB,KY (335)
(tiaprofenic acid):TI,AB,KY (120)
meloxicam:TI,AB,KY (256)
nabumetone:TI,AB,KY (144)
#6 OR #7 OR #8 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 OR #40 OR #41 (20558)
#5 AND #42 (181)
Appendix 3. Search strategy for MEDLINE via Ovid
Neuralgia/ (8975)
(nerve adj1 pain*).tw. (266)
neuralgia*.tw. (8746)
(neuropathic adj1 pain).tw. (10746)
1 or 2 or 3 or 4 (22180)
exp Anti‐Inflammatory Agents, Non‐Steroidal/ (161371)
NSAIDs.tw. (17403)
"non‐steroidal anti‐inflammatory drug*".tw. (9525)
aceclofenac.tw. (244)
acemetacin.tw. (109)
Apazone/ (168)
azapropazone.tw. (212)
celecoxib.tw. (4109)
Ketoprofen/ (2298)
ketoprofen.tw (4285)
dexketoprofen.tw. (263)
Diclofenac/ (6228)
diclofenac.tw. (7675)
Etodolac/ (435)
etodolac.tw. (540)
etoricoxib.tw. (442)
fenbufen.tw. (249)
Fenoprofen/ (277)
fenoprofen.tw. (375)
Flurbiprofen/ (1665)
flurbiprofen.tw. (1941)
Ibuprofen/ (6936)
Ibuprofen.tw. (9092)
Indomethacin/ (26988)
Indomet?acin.tw. (32915)
Mefenamic Acid/ (952)
mefenamic acid.tw. (1007)
meloxicam.tw. (1300)
nabumetone.tw. (380)
Naproxen/ (3460)
naproxen.tw. (4572)
Piroxicam/ (2512)
piroxicam.tw. (2511)
Sulindac/ (1282)
sulindac.tw. (1639)
tenoxicam.tw. (503)
tiaprofenic acid.tw. (313)
or/6‐42 (180537)
randomized controlled trial.pt. (395260)
controlled clinical trial.pt. (89513)
randomized.ab. (349013)
placebo.ab. (152353)
drug therapy.fs. (1775945)
randomly.ab. (206141)
trial.ab. (301485)
groups.ab. (1312898)
or/44‐51 (3358432)
5 and 43 and 52 (464)
Appendix 4. Search strategy for EMBASE via Ovid
Neuralgia/ (7142)
(nerve adj1 pain*).tw. (444)
neuralgia*.tw. (12624)
(neuropathic adj1 pain).tw. (17866)
1 or 2 or 3 or 4 (33227)
exp Anti‐Inflammatory Agents, Non‐Steroidal/ (463132)
NSAIDs.tw. (29856)
"non‐steroidal anti‐inflammatory drug*".tw. (13859)
aceclofenac.tw. (730)
acemetacin.tw. (168)
Apazone/ (1161)
azapropazone.tw. (279)
celecoxib.tw. (2606)
Ketoprofen/ (10964)
ketoprofen.tw (4276)
dexketoprofen.tw. (263)
Diclofenac/ (31011)
diclofenac.tw. (8365)
Etodolac/ (2358)
etodolac.tw. (808)
etoricoxib.tw. (812)
fenbufen.tw. (347)
Fenoprofen/ (2554)
fenoprofen.tw. (505)
Flurbiprofen/ (6717)
flurbiprofen.tw. (2511)
Ibuprofen/ (38699)
Ibuprofen.tw. (13581)
Indomethacin/ (71855)
Indomet?acin.tw. (38395)
Mefenamic Acid/ (5064)
mefenamic acid.tw. (1328)
meloxicam.tw. (1956)
nabumetone.tw. (532)
Naproxen/ (22226)
naproxen.tw. (6799)
Piroxicam/ (10250)
piroxicam.tw. (3731)
Sulindac/ (6254)
sulindac.tw. (2063)
tenoxicam.tw. (780)
tiaprofenic acid.tw. (474)
or/6‐42 (474609)
random*.ti,ab. (982862)
factorial*.ti,ab. (25505)
(crossover* or cross over* or cross‐over*).ti,ab. (76128)
placebo*.ti,ab. (219329)
(doubl* adj blind*).ti,ab. (157024)
assign*.ti,ab. (263506)
allocat*.ti,ab. (93895)
RANDOMIZED CONTROLLED TRIAL.sh. (373370)
DOUBLE‐BLIND PROCEDURE.sh. (122820)
CROSSOVER PROCEDURE.sh. (42869)
or/44‐53 (1405901)
5 and 43 and 54 (385)
Appendix 5. Efficacy results
| Study | Outcomes | Efficacy |
| Romano 2009 | Self reported VAS before and after 4 weeks of treatment | For participants with LANSS > 12 (n = 16): Celecoxib only Pre 47 mm Post 46 mm Pregbalin only Pre 47 mm Post 36 mm Combination Pre 48 mm Post 23 mm Pregabalin and combination, but not celecoxib alone, showed significant pain intensity reduction |
| Shackelford 2009 | ≥30 pain reduction ≥50% pain reduction PGIC much or very much improved Also mean pain changes | ≥ 30% pain reduction Placebo ‐ 17/66 GW406381 25 ‐ 19/72 GW406381 50 ‐ 21/71 ≥ 30% pain reduction Placebo ‐ 4/66 GW406381 25 ‐ 10/72 GW406381 50 ‐ 12/71 PGIC responder Placebo ‐ 13/66 GW406381 25 ‐ 17/72 GW406381 50 ‐ 21/71 |
| PGIC: Patient Global Impression of Change; VAS: visual analogue scale | ||
Appendix 6. Adverse event results
| Study | Participants with at least one adverse event | Serious adverse events | Withdrawals |
| Romano 2009 | 16/36 | Not reported. Implication is that there were none No deaths reported | 4/42 discontinued due to adverse events |
| Shackelford 2009 | Placebo 27/66 GW406381 25 34/72 GW406381 50 41/71 | Placebo 0/66 GW406381 25 3/72 GW406381 50 1/71 None associated with study drug. No cardiovascular events, and no deaths. | All cause Placebo 5/66 GW406381 25 12/72 GW406381 50 11/71 Lack of efficacy Placebo 2/66 GW406381 25 4/72 GW406381 50 3/71 Adverse events Placebo 1/66 GW406381 25 7/72 GW406381 50 4/71 |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Romano 2009.
| Methods | Randomised, double‐blind, cross‐over (4 weeks each treatment, with 1 week washout) | |
| Participants | Chronic low back pain of at least 6 months' duration, due to disc prolapse, lumbar spondylosis, and/or spinal stenosis. Pain intensity > 40/100 mm N = 42, age 18 to 75 years Results reported according to LANSS score (non‐neuropathic <12; neuropathic ≥12) |
|
| Interventions | Celecoxib 3 to 6 mg/kg/day Pregabalin 1 mg/kg/day for 1 week than 2 to 4 mg/kg/day Treatment groups: celecoxib alone, pregabalin alone, celecoxib + pregabalin |
|
| Outcomes | Self‐reported VAS (0 to 100 mm) Withdrawals, adverse events |
|
| Notes | Oxford Quality Score: R = 2, DB = 1, W = 1. Total = 4/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly assigned to pre‐ordered sequence based on consecutive recruitment order |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Double‐blind, but method not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Data on 36 completers of 42 |
| Selective reporting (reporting bias) | Low risk | No problems detected |
| Size | High risk | 36 completers (16 with neuropathic pain according to LANSS criteria) |
Shackelford 2009.
| Methods | Randomised, double‐blind, parallel group with placebo control, 3 weeks | |
| Participants | Diagnosis of postherpetic neuralgia of at least 3 months’ duration (pain present ≥ 3 months from healing of herpes zoster skin rash) and pain intensity score averaging ≥ 4/10 over 7 day period at baseline Initial pain score 6.2/10 N = 209, age 18 to 90 years (mean 69 years), 50% female |
|
| Interventions | Placebo, n = 66 GW406381 25 mg, n = 72 GW406381 50 mg, n = 71 (GW406381 is an experimental drug that is not marketed) |
|
| Outcomes | Several pain outcomes, including percentage of subjects with a ≥ 30% or a ≥ 50% reduction in average daily pain NRS score during week 3 of treatment compared with baseline Withdrawals, adverse events |
|
| Notes | Oxford Quality Score: R = 1, DB = 1, W = 1. Total = 3/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Double blind, but method not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | LOCF imputation after withdrawal |
| Selective reporting (reporting bias) | Low risk | No problems detected |
| Size | Unclear risk | 66 to 72 participants in each treatment group |
DB: double‐blind; LANSS: Leeds Assessment of Neuropathic Symptoms and Signs; LOCF: last observation carried forward; NRS: numerical rating scale; R: randomised; VAS: visual analogue scale; W: withdrawals
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Cohen 1987 | Not obviously randomised, single blind, diabetic neuropathy (n = 18) |
| Dellemijn 1994 | 1 week in each part of cross‐over, malignant nerve pain (n = 16) |
| Jaffé 1974 | Not neuropathic pain, acute low back pain (n = 60) |
| Patarica‐Huber 2011 | Not blind, neuropathic pain after treatments for breast cancer (n = 75) |
| Pop‐Busui 2015 | Not randomised, not blind (n = 8) |
| Solak 2007 | Not randomised (order of presentation), post thoracotomy pain (n = 40) |
| Videman 1984 | Back pain, not neuropathic pain (n = 28, of whom 8 had sciatica) |
| Weber 1993 | Acute sciatica (n = 209) |
| Yu 2008 | Not double blind, post herpetic neuralgia (n = 72) |
Characteristics of ongoing studies [ordered by study ID]
NCT01088256.
| Trial name or title | Efficacy of etoricoxib on peripheral hyperalgesia |
| Methods | Randomised, double‐blind, parallel groups |
| Participants | Causalgia, polyneuropathy, postherpetic neuralgia, peripheral nerve injury, radiculopathy. Persistent pain ≥4/10 on numerical rating scale |
| Interventions | Etoricoxib 90 mg daily, placebo |
| Outcomes | Improved peripheral hyperalgesia at 12 months |
| Starting date | February 2011 |
| Contact information | Christoph Maier, Prof. Dr., Ruhr University of Bochum |
| Notes | Terminated 2012 |
NCT01264237.
| Trial name or title | Evaluation of the efficacy, tolerability and safety of etoricoxib (Arcoxia) in patients with neuropathic pain |
| Methods | Enriched enrolment randomised withdrawal design, double‐blind, placebo‐controlled |
| Participants | Postherpetic neuralgia, neuralgia |
| Interventions | Etoricoxib 90 mg daily, placebo |
| Outcomes | Time to efficacy failure (over 28 days) |
| Starting date | March 2011 |
| Contact information | Dr Stuart Ratcliffe, MBChB, MFPM, FRSM. Director of Pain Research, MAC UK Neuroscience Ltd |
| Notes | No update since 2011 |
NCT01838044.
| Trial name or title | Efficacy and safety study of celecoxib and pregabalin compared with celecoxib monotherapy, in patients with chronic low back pain having a neuropathic component |
| Methods | Randomised, double‐blind, parallel groups, placebo‐controlled |
| Participants | Chronic low back pain with high probability of a significant neuropathic component for 4 years or less |
| Interventions | Pregabalin and celecoxib, placebo and celecoxib |
| Outcomes | A range of pain outcomes, depression, sleep |
| Starting date | October 2013 |
| Contact information | Pfizer |
| Notes | Recruitment terminated on 3 April 2015 due to slow recruitment rate and lack of operational feasibility. Study was not terminated for reasons of safety or efficacy. |
Differences between protocol and review
The protocol incorrectly included complex regional pain syndrome Type 1 in the list of neuropathic pain conditions. This should be complex regional pain syndrome Type 2, and we have corrected the mistake in the full review.
Contributions of authors
CCC and RAM wrote the protocol. SD and RAM carried out searches with the assistance of the Editorial Base. RAM, SD, and PW identified studies for inclusion, and extracted data. RAM wrote the initial review draft. All authors were involved in writing the full review.
Sources of support
Internal sources
-
Chang Gung Memorial Hospital, Chiayi, Taiwan.
Provided funding (Chang Gung Research Project (CMRPG6E0041))
-
Oxford Pain Relief Trust, UK.
General institutional support
External sources
-
The National Institute for Health Research (NIHR), UK.
- NIHR Cochrane Programme Grant: 13/89/29 ‐ Addressing the unmet need of chronic pain: providing the evidence for treatments of pain
Declarations of interest
RAM has no conflicts relating to this review or any similar product.
C‐CC has no conflicts relating to this review or any similar product.
PW has no conflicts relating to this review or any similar product.
SD has no conflicts relating to this review or any similar product.
ASCR has no conflicts relating to this review or any similar product.
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Romano 2009 {published data only}
- Romanò CL, Romanò D, Bonora C, Mineo G. Pregabalin, celecoxib, and their combination for treatment of chronic low‐back pain. Journal of Orthopaedics and Traumatology 2009;10(4):185‐91. [DOI: 10.1007/s10195-009-0077-z] [DOI] [PMC free article] [PubMed] [Google Scholar]
Shackelford 2009 {published data only}
- Shackelford S, Rauck R, Quessy S, Blum D, Hodge R, Philipson R. A randomized, double‐blind, placebo‐controlled trial of a selective COX‐2 inhibitor, GW406381, in patients with postherpetic neuralgia. Journal of Pain 2009;10(6):654‐60. [DOI: 10.1016/j.jpain.2009.01.328] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Cohen 1987 {published data only}
- Cohen KL, Harris S. Efficacy and safety of nonsteroidal anti‐inflammatory drugs in the therapy of diabetic neuropathy. Archives of Internal Medicine 1987;147(8):1442‐4. [DOI: 10.1001/archinte.1987.00370080078016] [DOI] [PubMed] [Google Scholar]
Dellemijn 1994 {published data only}
- Dellemijn PL, Verbiest HB, Vliet JJ, Roos PJ, Vecht CJ. Medical therapy of malignant nerve pain. A randomised double‐blind explanatory trial with naproxen versus slow‐release morphine. European Journal of Cancer 1994;30A(9):1244‐50. [PUBMED: 7999406] [DOI] [PubMed] [Google Scholar]
Jaffé 1974 {published data only}
- Jaffé G. A double‐blind, between patient comparison of alclofenac (‘Prinalgin’)and indomethacin in the treatment of low back pain and sciatica. Current Medical Research and Opinion 1974;2(7):424‐9. [PUBMED: 4281380] [DOI] [PubMed] [Google Scholar]
Patarica‐Huber 2011 {published data only}
- Patarica‐Huber E, Boskov N, Pjevic M. Multimodal approach to therapy‐related neuropathic pain in breast cancer. Journal of B.U.ON. 2011;16(1):40‐5. [PUBMED: 21674848] [PubMed] [Google Scholar]
Pop‐Busui 2015 {published data only}
- Pop‐Busui R. Pilot study to determine effects of salsalate in type 1 diabetes and painful peripheral neuropathy (SALP). clinicaltrials.gov/ct2/show/NCT01480297 (accessed 5 June 2015) 2015.
Solak 2007 {published data only}
- Solak O, Metin M, Esme H, Solak O, Yaman M, Pekcolaklar A, et al. Effectiveness of gabapentin in the treatment of chronic post‐thoracotomy pain. European Journal of Cardio‐thoracic Surgery 2007;32(1):9‐12. [DOI: 10.1016/j.ejcts.2007.03.022] [DOI] [PubMed] [Google Scholar]
Videman 1984 {published data only}
- Videman T, Osterman K. Double‐blind parallel study of piroxicam versus indomethacin in the treatment of low back pain. Annals of Clinical Research 1984;16(3):156‐60. [PUBMED: 6236738] [PubMed] [Google Scholar]
Weber 1993 {published data only}
- Weber H, Holme I, Amlie E. The natural course of acute sciatica with nerve root symptoms in a double‐blind placebo‐controlled trial evaluating the effect of piroxicam. Spine 1993;18(11):1433‐8. [PUBMED: 8235813] [PubMed] [Google Scholar]
Yu 2008 {published data only}
- Yu C, Chen Y, Mu Y, Chen X, Ding X, Ya W. Effect of oxycodone and acetaminophen on postherpetic neuralgia. Chinese Journal of New Drugs 2008;17(23):2061‐2. [Google Scholar]
References to ongoing studies
NCT01088256 {published data only}
- Maier C. Efficacy of etoricoxib on peripheral hyperalgesia. www.clinicaltrials.gov/ct2/show/NCT01088256 (accessed 5 June 2015) 2012.
NCT01264237 {published data only}
- Ratcliffe S. Evaluation of the efficacy, tolerability and safety of etoricoxib (Arcoxia) in patients with neuropathic pain. www.clinicaltrials.gov/ct2/show/NCT01264237 (accessed 5 June 2015) 2011.
NCT01838044 {published data only}
- Pfizer. Efficacy and safety study of celecoxib and pregabalin compared with celecoxib monotherapy, in patients with chronic low back pain having a neuropathic component. www.clinicaltrials.gov/ct2/show/NCT01838044 (accessed 5 June 2015) 2015.
Additional references
Baron 2012
- Baron R, Wasner G, Binder A. Chronic pain: genes, plasticity, and phenotypes. Lancet Neurology 2012;11(1):19‐21. [DOI: 10.1016/S1474-4422(11)70281-2] [DOI] [PubMed] [Google Scholar]
Boswell 2008
- Boswell DJ, Ostergaard K, Philipson RS, Hodge RA, Blum D, Brown JC, et al. Evaluation of GW406381 for treatment of osteoarthritis of the knee: two randomized, controlled studies. Medscape Journal of Medicine 2008;10(11):259. [PMC free article] [PubMed] [Google Scholar]
Bouhassira 2008
- Bouhassira D, Lantéri‐Minet M, Attal N, Laurent B, Touboul C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain 2008;136(3):380‐7. [DOI: 10.1016/j.pain.2007.08.013] [DOI] [PubMed] [Google Scholar]
Calvo 2012
- Calvo M, Dawes JM, Bennett DL. The role of the immune system in the generation of neuropathic pain. Lancet Neurology 2012;11(7):629‐42. [DOI: 10.1016/S1474-4422(12)70134-5] [DOI] [PubMed] [Google Scholar]
Cochrane PaPaS Group 2012
- Cochrane Pain, Palliative and Supportive Care Group. PaPaS author and referee guidance. http://papas.cochrane.org/papas‐documents (accessed 5 June 2015) 2012.
Demant 2014
- Demant DT, Lund K, Vollert J, Maier C, Segerdahl M, Finnerup NB, et al. The effect of oxcarbazepine in peripheral neuropathic pain depends on pain phenotype: a randomised, double‐blind, placebo‐controlled phenotype‐stratified study. Pain 2014;155(11):2263‐73. [DOI: 10.1016/j.pain.2014.08.014] [DOI] [PubMed] [Google Scholar]
Derry 2012
- Derry S, Moore RA. Topical capsaicin (low concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2012, Issue 9. [DOI: 10.1002/14651858.CD010111] [DOI] [PMC free article] [PubMed] [Google Scholar]
Derry 2013
- Derry S, Sven‐Rice A, Cole P, Tan T, Moore RA. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2013, Issue 2. [DOI: 10.1002/14651858.CD007393.pub3] [DOI] [PubMed] [Google Scholar]
Derry 2014
- Derry S, Wiffen PJ, Moore RA, Quinlan J. Topical lidocaine for neuropathic pain in adults. Cochrane Database of Systematic Reviews 2014, Issue 7. [DOI: 10.1002/14651858.CD010958.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Di Franco 2010
- Franco M, Iannuccelli C, Atzeni F, Cazzola M, Salaffi F, Valesini G, et al. Pharmacological treatment of fibromyalgia. Clinical and Experimental Rheumatology 2010;28(6 Suppl 63):S110‐6. [PUBMED: 21176430] [PubMed] [Google Scholar]
Dworkin 2008
- Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. Journal of Pain 2008;9(2):105‐21. [DOI: 10.1016/j.jpain.2007.09.005] [DOI] [PubMed] [Google Scholar]
EMEA 2005
- EMEA public statement on the suspension of the marketing authorisation for Bextra (valdecoxib) in the European Union. ema.europa.eu/docs/en_GB/document_library/Public_statement/2009/12/WC500018391.pdf (accessed 25 Spetember 2015).
FDA 2004
- FDA Public Health Advisory: Safety of Vioxx. fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm106274.htm (accessed 25 September 2015).
Finnerup 2013
- Finnerup NB, Scholz J, Attal N, Baron R, Haanpää M, Hansson P, et al. Neuropathic pain needs systematic classification. European Journal of Pain 2013;17(7):953‐6. [DOI: 10.1002/j.1532-2149.2012.00282.x] [DOI] [PubMed] [Google Scholar]
Finnerup 2015
- Finnerup NB, Attal N, Haroutounian S, McNicol E, Baron R, Dworkin RH, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta‐analysis. Lancet Neurology 2015;14(2):162‐73. [DOI: 10.1016/S1474-4422(14)70251-0] [DOI] [PMC free article] [PubMed] [Google Scholar]
Grosser 2011
- Grosser T, Smyth E. Chapter 34. Anti‐inflammatory, antipyretic, and analgesic agents; pharmacotherapy of gout. In: Brunton LL, Chabner BA, Knollmann BC editor(s). Goodman & Gilman's The Pharmacological Basis of Therapeutics. Available at accessmedicine.mhmedical.com/book.aspx?bookid=374 (accessed 5 Jun 2015). 12th Edition. New York: McGraw‐Hill, 2011. [ISBN: 978‐0‐07‐162442‐8] [Google Scholar]
Gustorff 2008
- Gustorff B, Dorner T, Likar R, Grisold W, Lawrence K, Schwarz F, et al. Prevalence of self‐reported neuropathic pain and impact on quality of life: a prospective representative survey. Acta Anaesthesiologica Scandinavica 2008;52(1):132‐6. [DOI: 10.1111/j.1399-6576.2007.01486.x] [DOI] [PubMed] [Google Scholar]
Hall 2008
- Hall GC, Carroll D, McQuay HJ. Primary care incidence and treatment of four neuropathic pain conditions: a descriptive study, 2002‐2005. BMC Family Practice 2008;9:26. [DOI: 10.1186/1471-2296-9-26] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hall 2013
- Hall GC, Morant SV, Carroll D, Gabriel ZL, McQuay HJ. An observational descriptive study of the epidemiology and treatment of neuropathic pain in a UK general population. BMC Family Practice 2013;14:28. [DOI: 10.1186/1471-2296-14-28] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hasnie 2007
- Hasnie FS, Breuer J, Parker S, Wallace V, Blackbeard J, Lever I, et al. Further characterization of a rat model of varicella zoster virus‐associated pain: Relationship between mechanical hypersensitivity and anxiety‐related behavior, and the influence of analgesic drugs. Neuroscience 2007;144(4):1495‐508. [DOI: 10.1016/j.neuroscience.2006.11.029] [DOI] [PMC free article] [PubMed] [Google Scholar]
Helfert 2015
- Helfert SM, Reimer M, Höper J, Baron R. Individualized pharmacological treatment of neuropathic pain. Clinical Pharmacology and Therapeutics 2015;97(2):135‐42. [DOI: 10.1002/cpt.19] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org (accessed 5 June 2015).
Jadad 1996
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17(1):1‐12. [DOI: ] [DOI] [PubMed] [Google Scholar]
Jensen 2011
Katusic 1991
- Katusic S, Williams DB, Beard CM, Bergstralh EJ, Kurland LT. Epidemiology and clinical features of idiopathic trigeminal neuralgia and glossopharyngeal neuralgia: similarities and differences, Rochester, Minnesota,1945‐1984. Neuroepidemiology 1991;10(5‐6):276‐81. [PUBMED: 1798430] [DOI] [PubMed] [Google Scholar]
Kawakami 2002
- Kawakami M, Matsumoto T, Hashizume H, Kuribayashi K, Tamaki T. Epidural injection of cyclooxygenase‐2 inhibitor attenuates pain‐related behavior following application of nucleus pulposus to the nerve root in the rat. Journal of Orthopaedic Research 2002;20(2):376‐81. [DOI: 10.1016/S0736-0266(01)00114-0] [DOI] [PubMed] [Google Scholar]
Koopman 2009
- Koopman JS, Dieleman JP, Huygen FJ, Mos M, Martin CG, Sturkenboom MC. Incidence of facial pain in the general population. Pain 2009;147(1‐3):122‐7. [DOI: 10.1016/j.pain.2009.08.023] [DOI] [PubMed] [Google Scholar]
L'Abbé 1987
- L'Abbé KA, Detsky AS, O'Rourke K. Meta‐analysis in clinical research. Annals of Internal Medicine 1987;107:224‐33. [DOI] [PubMed] [Google Scholar]
Laine 2001
- Laine L. Approaches to nonsteroidal anti‐inflammatory drug use in the high‐risk patient. Gastroenterology 2001;120(3):594‐606. [DOI: 10.1053/gast.2001.21907] [DOI] [PubMed] [Google Scholar]
Liberati 2009
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta‐analyses of studies that evaluate health care interventions: explanation and elaboration. Annals of Internal Medicine 2009;151(4):W65‐94. [DOI: 10.7326/0003-4819-151-4-200908180-00136] [DOI] [PubMed] [Google Scholar]
Lunn 2014
- Lunn MP, Hughes RA, Wiffen PJ. Duloxetine for treating painful neuropathy, chronic pain or fibromyalgia. Cochrane Database of Systematic Reviews 2014, Issue 1. [DOI: 10.1002/14651858.CD007115.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
McQuay 1998
- McQuay H, Moore R. An Evidence‐based Resource for Pain Relief. 1st Edition. Oxford University Press, 1998. [ISBN: 978‐0192630483] [Google Scholar]
McQuay 2007
- McQuay HJ, Smith LA, Moore RA. Chronic Pain. In: Stevens A, Raftery J, Mant J, Simpson S editor(s). Health Care Needs Assessment. 3rd series. Oxford: Radcliffe Publishing, 2007. [ISBN: 978‐1‐84619‐063‐6] [Google Scholar]
Moore 1998
- Moore RA, Gavaghan D, Tramèr MR, Collins SL, McQuay HJ. Size is everything ‐ large amounts of information are needed to overcome random effects in estimating direction and magnitude of treatment effects. Pain 1998;78(3):209‐16. [DOI: 10.1016/S0304-3959(98)00140-7] [DOI] [PubMed] [Google Scholar]
Moore 2008
- Moore RA, Barden J, Derry S, McQuay HJ. Managing potential publication bias. In: McQuay HJ, Kalso E, Moore RA editor(s). Systematic Reviews in Pain Research: Methodology Refined. Seattle: IASP Press, 2008:15‐24. [ISBN: 978‐0‐931092‐69‐5] [Google Scholar]
Moore 2009a
- Moore RA, Straube S, Wiffen PJ, Derry S, McQuay HJ. Pregabalin for acute and chronic pain in adults. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD007076.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2009b
- Moore RA, Moore OA, Derry S, Peloso PM, Gammaitoni AR, Wang H. Responder analysis for pain relief and numbers needed to treat in a meta‐analysis of etoricoxib osteoarthritis trials: bridging a gap between clinical trials and clinical practice. Annals of the Rheumatic Diseases 2010;69(2):374‐9. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2010a
- Moore RA, Eccleston C, Derry S, Wiffen P, Bell RF, Straube S, et al. "Evidence" in chronic pain ‐ establishing best practice in the reporting of systematic reviews. Pain 2010;150(3):386‐9. [DOI: 10.1016/j.pain.2010.05.011] [DOI] [PubMed] [Google Scholar]
Moore 2010b
- Moore RA, Smugar SS, Wang H, Peloso PM, Gammaitoni A. Numbers‐needed‐to‐treat analyses‐‐do timing, dropouts, and outcome matter? Pooled analysis of two randomized, placebo‐controlled chronic low back pain trials. Pain 2010;151(3):592‐7. [DOI: 10.1016/j.pain.2010.07.013] [DOI] [PubMed] [Google Scholar]
Moore 2010c
- Moore RA, Moore OA, Derry S, Peloso PM, Gammaitoni AR, Wang H. Responder analysis for pain relief and numbers needed to treat in a meta‐analysis of etoricoxib osteoarthritis trials: bridging a gap between clinical trials and clinical practice. Annals of the Rheumatic Diseases 2010;69(2):374‐9. [DOI: 10.1136/ard.2009.107805] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2010d
- Moore RA, Straube S, Paine J, Phillips CJ, Derry S, McQuay HJ. Fibromyalgia: moderate and substantial pain intensity reduction predicts improvement in other outcomes and substantial quality of life gain. Pain 2010;149(2):360‐4. [DOI: 10.1016/j.pain.2010.02.039] [DOI] [PubMed] [Google Scholar]
Moore 2011a
- Moore RA, Straube S, Paine J, Derry S, McQuay HJ. Minimum efficacy criteria for comparisons between treatments using individual patient meta‐analysis of acute pain trials: examples of etoricoxib, paracetamol, ibuprofen, and ibuprofen/paracetamol combinations after third molar extraction. Pain 2011;152(5):982‐9. [DOI: 10.1016/j.pain.2010.11.030] [DOI] [PubMed] [Google Scholar]
Moore 2011b
- Moore RA, Mhuircheartaigh RJ, Derry S, McQuay HJ. Mean analgesic consumption is inappropriate for testing analgesic efficacy in post‐operative pain: analysis and alternative suggestion. European Journal of Anaesthesiology 2011;28(6):427‐32. [DOI: 10.1097/EJA.0b013e328343c569] [DOI] [PubMed] [Google Scholar]
Moore 2012a
- Moore RA, Straube S, Eccleston C, Derry S, Aldington D, Wiffen P, et al. Estimate at your peril: imputation methods for patient withdrawal can bias efficacy outcomes in chronic pain trials using responder analyses. Pain 2012;153(2):265‐8. [DOI: 10.1016/j.pain.2011.10.004] [DOI] [PubMed] [Google Scholar]
Moore 2012b
- Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database of Systematic Reviews 2012, Issue 12. [DOI: 10.1002/14651858.CD008242.pub2] [DOI] [PubMed] [Google Scholar]
Moore 2013a
- Moore A, Derry S, Eccleston C, Kalso E. Expect analgesic failure; pursue analgesic success. BMJ 2013;346:f2690. [DOI: 10.1136/bmj.f2690] [DOI] [PubMed] [Google Scholar]
Moore 2013b
NICE 2013
- National Institute for Health and Care Excellence (NICE). Neuropathic pain ‐ pharmacological management: the pharmacological management of neuropathic pain in adults in non‐specialist settings, 2013. www.nice.org.uk/guidance/cg173 (accessed 5 June 2015).
O'Brien 2010
- O'Brien EM, Staud RM, Hassinger AD, McCulloch RC, Craggs JG, Atchison JW, et al. Patient‐centered perspective on treatment outcomes in chronic pain. Pain Medicine 2010;11(1):6‐15. [DOI: 10.1111/j.1526-4637.2009.00685.x] [DOI] [PubMed] [Google Scholar]
Rappaport 1994
- Rappaport ZH, Devor M. Trigeminal neuralgia: the role of self‐sustaining discharge in the trigeminal ganglion. Pain 1994;56(2):127‐38. [DOI: 10.1016/0304-3959(94)90086-8] [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Seidel 2013
- Seidel S, Aigner M, Ossege M, Pernicka E, Wildner B, Sycha T. Antipsychotics for acute and chronic pain in adults. Cochrane Database of Systematic Reviews 2013, Issue 8. [DOI: 10.1002/14651858.CD004844.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Straube 2008
- Straube S, Derry S, McQuay HJ, Moore RA. Enriched enrollment: definition and effects of enrichment and dose in trials of pregabalin and gabapentin in neuropathic pain. A systematic review. British Journal of Clinical Pharmacology 2008;66(2):266‐75. [DOI: 10.1111/j.1365-2125.2008.03200.x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Straube 2010
- Straube S, Derry S, Moore RA, Paine J, McQuay HJ. Pregabalin in fibromyalgia ‐ responder analysis from individual patient data. BMC Musculoskeletal Disorders 2010;11:150. [DOI: 10.1186/1471-2474-11-150] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sultan 2008
- Sultan A, Gaskell H, Derry S, Moore RA. Duloxetine for painful diabetic neuropathy and fibromyalgia pain: systematic review of randomised trials. BMC Neurology 2008;8:29. [DOI: 10.1186/1471-2377-8-29] [DOI] [PMC free article] [PubMed] [Google Scholar]
Torrance 2006
- Torrance N, Smith BH, Bennett MI, Lee AJ. The epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey. Journal of Pain 2006;7(4):281‐9. [DOI: 10.1016/j.jpain.2005.11.008] [DOI] [PubMed] [Google Scholar]
Treede 2008
- Treede RD, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffin JW, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology 2008;70(18):1630‐5. [DOI: 10.1212/01.wnl.0000282763.29778.59] [DOI] [PubMed] [Google Scholar]
Varner 2009
- Varner J, Lomax M, Blum D, Quessy S. A randomized, controlled, dose‐ranging study investigating single doses of GW406381, naproxen sodium, or placebo in patients with acute pain after third molar tooth extraction. Clinical Journal of Pain 2009;25(7):577‐83. [DOI: 10.1097/AJP.0b013e3181a085fa] [DOI] [PubMed] [Google Scholar]
Vo 2009
- Vo T, Rice ASC, Dworkin RH. Non‐steroidal anti‐inflammatory drugs for neuropathic pain: How do we explain continued widespread use?. Pain 2009;143(3):169‐71. [DOI: 10.1016/j.pain.2009.03.013] [DOI] [PubMed] [Google Scholar]
von Hehn 2012
- Hehn CA, Baron R, Woolf CJ. Deconstructing the neuropathic pain phenotype to reveal neural mechanisms. Neuron 2012;73(4):638‐52. [DOI: 10.1016/j.neuron.2012.02.008] [DOI] [PMC free article] [PubMed] [Google Scholar]
Vos 2012
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990‐2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380(9859):2163‐96. [DOI: 10.1016/S0140-6736(12)61729-2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wentz 2008
- Wentz AL, Jimenez TB, Dixon RM, Aurora SK, Gold M, CXA20008 Study Investigators. A double‐blind, randomized, placebo‐controlled, single‐dose study of the cyclooxygenase‐2 inhibitor, GW406381, as a treatment for acute migraine. European Journal of Neurology 2008;15(4):420‐7. [DOI: 10.1111/j.1468-1331.2008.02093.x] [DOI] [PubMed] [Google Scholar]