

Abstract
Background
About 5% to 10% of all deep vein thromboses occur in the upper extremities. Serious complications of upper extremity deep vein thrombosis, such as post‐thrombotic syndrome and pulmonary embolism, may in theory be avoided using thrombolysis. No systematic review has assessed the effects of thrombolysis for the treatment of individuals with acute upper extremity deep vein thrombosis.
Objectives
To assess the beneficial and harmful effects of thrombolysis for the treatment of individuals with acute upper extremity deep vein thrombosis.
Search methods
The Cochrane Vascular Information Specialist (CIS) searched the Specialised Register (29 March 2017), the Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 2), and three trial registries (World Health Organization International Clinical Trials Registry, ClinicalTrials.gov, and ISRCTN registry) for ongoing and unpublished studies. We additionally searched the registries of the European Medical Agency and the US Food and Drug Administration (December 2016).
Selection criteria
We planned to include randomised clinical trials irrespective of publication type, publication date and language that investigated the effects of thrombolytics added to anticoagulation, thrombolysis versus anticoagulation, or thrombolysis versus any other type of medical intervention for the treatment of acute upper extremity deep vein thrombosis.
Data collection and analysis
Two review authors independently screened all records to identify those that met inclusion criteria. We planned to use the standard methodological procedures expected by Cochrane. We planned to use trial domains to assess the risks of systematic error (bias) in the trials. We planned to conduct trial sequential analyses to control for the risk of random errors and to assess the robustness of our conclusions. We planned to consider a P value of 0.025 or less as statistically significant. We planned to assess the quality of the evidence using the GRADE approach. Our primary outcomes were severe bleeding, pulmonary embolism, and all‐cause mortality.
Main results
We found no trials eligible for inclusion. We also identified no ongoing trials.
Authors' conclusions
There is currently insufficient evidence from which to draw conclusion on the benefits or harms of thrombolysis for the treatment of individuals with acute upper extremity deep vein thrombosis as an add‐on therapy to anticoagulation, alone compared with anticoagulation, or alone compared with any other type of medical intervention. Large randomised clinical trials with a low risk of bias are warranted. They should focus on clinical outcomes and not solely on surrogate measures.
Plain language summary
Harms and benefits of dissolving blood clots in deep blood vessels in the arms
Background
A blood clot that forms in the deep blood vessels of the arms, blocking the passage of blood, is referred to as an acute upper extremity deep vein thrombosis. An acute upper extremity deep vein thrombosis currently affects 4 to 10 per 100,000 people in the general population. One of the most serious complications of an upper extremity deep vein thrombosis is a pulmonary embolism, which is a blockage of one of the major blood vessels in the lung. This can be a life‐threatening condition. Post‐thrombotic syndrome, in which the blood clot causes permanent swelling, skin colour changes, sores or ulcers, and decreased function of the affected limb, is another serious complication that can impact a person's quality of life.
Thrombolysis aims to break down the blood clot with the use of drugs infused directly into a blood vessel. A previous Cochrane Review looked at the beneficial and harmful effects of thrombolysis for the treatment of acute deep vein thrombosis of the lower extremities (e.g. the legs). While thrombolysis was found to lower the risk of post‐thrombotic syndrome, it had no effect on the risk of death, risk of a blood clot travelling to the lungs or brain, (where it can cause a stroke), or the risk of bleeding inside the skull. In this present review, we attempted to assess the benefits and harms of thrombolysis for the treatment of acute upper extremity deep vein thrombosis.
Study characteristics and key results
We found no randomised clinical trials (search current until March 2017) that met the inclusion criteria of our review. Hence, the benefits and harms of thrombolysis for acute upper extremity deep vein thrombosis remain unknown.
Conclusion
Large trials using proper methods and reporting on patient‐relevant outcomes are needed.
Background
Description of the condition
Upper extremity deep vein thrombosis (thrombosis in the subclavian, axiliary, or brachial vein, possibly extending to the brachiocephalic vein, superior vena cava, or internal jugular vein), accounts for approximately 5% to 10% of all deep vein thromboses (Kucher 2011; Engelberger 2012; Kearon 2016). The incidence of upper extremity deep vein thrombosis is 4 to 10 per 100,000 in the general population rising to 6 per 10,000 in individuals who are hospitalised (Koury 2011; Kucher 2011), and is increasing, possibly due to the more frequent use of central venous catheters (Kucher 2011; Engelberger 2012).
Upper extremity deep vein thrombosis can be divided into proximal upper extremity deep vein thrombosis, defined as thrombosis involving the axillary or more proximal deep arm veins, and distal upper extremity deep vein thrombosis, defined as thrombosis of the brachial or more distal deep arm veins. Proximal upper extremity deep vein thrombosis is the most frequent of the two types (Engelberger 2012; Kearon 2016).
Upper extremity deep vein thrombosis can be divided into two groups on the basis of aetiology.
1) Primary upper extremity deep vein thrombosis results from thoracic outlet syndrome, effort‐related thrombosis (also known as Paget–Schroetter syndrome), or thrombophilia, or is idiopathic. Primary upper extremity deep vein thrombosis accounts for 20% to 25% of all upper extremity deep vein thrombosis (Kucher 2011). Thoracic outlet syndrome and effort‐related thrombosis both cause upper extremity deep vein thrombosis by inducing microtrauma to the subclavian vessel. Thoracic outlet syndrome and effort‐related thrombosis often coexist. In thoracic outlet syndrome, the microtrauma is caused by compression of the subclavian vein due to abnormalities at various sites including the first rib, clavicle, subclavius muscle, costoclavicular ligament, or anterior scalene muscle (Joffe 2002; Kucher 2011). In effort‐related thrombosis the microtrauma is possibly induced by repetitive arm movements (Joffe 2002; Kucher 2011).
2) Secondary upper extremity deep vein thrombosis results from the presence of an indwelling central venous catheter, pacemaker, or defibrillator leads; surgery; trauma; pregnancy; use of oral contraceptives; or cancer. This secondary type accounts for 75% to 80% of all upper extremity deep vein thrombosis (Kucher 2011; Kearon 2016).
Clinical manifestations of upper extremity deep vein thrombosis include acute and chronic arm pain, swelling, discolourations, and dilated collateral veins over the arm, neck, or chest (Kearon 2016). When upper extremity deep vein thrombosis is suspected, the next step is either duplex ultrasonography or compression ultrasonography (Koury 2011; Kucher 2011; Bates 2012). Venography, computerised tomographic venography, and magnetic resonance venography may also be warranted in an attempt to better visualise the vein (Koury 2011; Kucher 2011; Bates 2012).
Between 10% and 50% of individuals who experience an upper extremity deep vein thrombosis will die within five years, mainly due to underlying malignant conditions as well as an increased risk of pulmonary embolism (Saseedharan 2012). Complications of upper extremity deep vein thrombosis include pulmonary embolism (5% to 6% of all cases), post‐thrombotic syndrome (15% to 20% of all cases), and recurrence (Elman 2006; Kucher 2011; Engelberger 2012; Kearon 2016). The dominant arm is more often affected, and complications occur more often when thrombosis involves the axiliary and more proximal veins rather than the brachial and more distal veins (Kearon 2016).
Description of the intervention
Thrombolytic drugs act by activating plasminogen which in turn forms the enzyme plasmin. Plasmin consequently degrades blood clots by breaking down the fibrin molecules which make up the clots (Ali 2014).
Different types of thrombolytic drugs exist, namely streptokinase, urokinase, and recombinant tissue plasminogen activator (rt‐PA). Streptokinase is a protein produced by different strains of streptococci (Ali 2014). Streptokinase binds to plasminogen and this complex converts plasminogen to plasmin (Ali 2014). Urokinase is an endogenous enzyme, synthesised by the kidney, that converts plasminogen to plasmin (Ali 2014). rt‐PA, in the presence of fibrin, converts plasminogen to plasmin. It preferentially targets fibrin‐bound plasminogen (Ali 2014).
Thrombolytic drugs may be administered in various doses and for varying durations. The route of administration may also differ (e.g. via a peripheral vein, resulting in systemic thrombolysis, loco‐regionally, or via a catheter directed at the occluding thrombus). The theoretical advantage of the loco‐regional and catheter‐directed methods is that they may reduce the amount of thrombolytic needed and may reduce the risk of bleeding compared to systemic thrombolysis (Patterson 2010).
Anticoagulation is currently the drug of choice when treating acute upper extremity deep vein thrombosis (Kearon 2016). The recommended acute anticoagulant is low‐molecular‐weight heparin or fondaparinux; unfractionated heparin is an alternative (Kearon 2016). Anticoagulants work by activating antithrombin, which in turn increases the rate of inactivation of coagulation factors, most importantly thrombin and factor Xa (Hull 2015). The degree of inactivation of thrombin and factor Xa depends on the anticoagulant (Hull 2015). The administration of unfractionated heparin results in effective inactivation of both thrombin and factor Xa, whereas low‐molecular‐weight heparin results in effective inactivation of factor Xa and to a lesser degree thrombin (Hull 2015). Fondaparinux almost exclusively inactivates factor Xa (Hull 2015).
How the intervention might work
Non‐randomised studies have shown that thrombolysis might be able to lyse the clot in the acute phase, preserving the venous valvular function (Patterson 2010; Petrakis 2000). Theoretically, this may reduce the risk of post‐thrombotic complications but could also increase the risk of bleeding.
Why it is important to do this review
No Cochrane Review has assessed the use of thrombolytics or anticoagulants for the treatment of acute upper extremity deep vein thrombosis.
One Cochrane Review from 2016 assessed the use of thrombolytic therapy plus anticoagulation versus anticoagulation alone for the treatment of acute deep venous thrombosis of the lower extremities (Watson 2016). This review showed thrombolytic therapy plus anticoagulation had no significant effect on mortality, risk of pulmonary embolism, stroke, or leg ulceration. However, thrombolytics were found to increase the proportion of participants with an improvement in venous patency, and with complete clot lysis, and to lower the risk of post‐thrombotic syndrome. This came at the cost of a higher risk of bleeding regardless of the route of administration (Watson 2016).
The American College of Chest Physicians (CHEST) guidelines from 2012 (Kearon 2016) reviewed the best management of individuals with acute upper extremity deep vein thrombosis and strongly recommended that they be given parenteral anticoagulation in the acute phase (Grade 1B). The guidelines also recommended giving anticoagulant therapy alone over thrombolysis (Grade 2C). The guidelines note that these recommendations are based on indirect evidence from studies performed in individuals with deep vein thrombosis of the legs, on observational studies, and on the understanding of the natural history of upper extremity deep vein thrombosis.
Objectives
To assess the beneficial and harmful effects of thrombolysis for the treatment of individuals with acute upper extremity deep vein thrombosis.
Methods
Criteria for considering studies for this review
Types of studies
Randomised clinical trials assessing the effects of thrombolytics for upper extremity deep vein thrombosis, irrespective of publication type, publication status, publication date, and language.
Types of participants
Participants of any age, diagnosed with acute upper vein deep vein thrombosis (as defined by the trialists).
Types of interventions
Any type of thrombolysis (streptokinase, urokinase, rt‐PA, etc.) investigated in trials comparing the effects of the following interventions.
Thrombolytics added to anticoagulation versus anticoagulation alone.
Thrombolytics versus anticoagulation.
Thrombolytics versus any other type of medical intervention.
We would have included trials investigating any type of medical therapy as a co‐intervention to thrombolysis providing the intervention was applied to all treatment arms.
Types of outcome measures
Primary outcomes
Proportion of participants with severe bleeding (defined by trialists)
Proportion of participants with pulmonary embolism (defined by trialists)
All‐cause mortality
Secondary outcomes
Post‐thrombotic syndrome (defined by trialists)
Quality of life (assessed using any valid scale); quality of life scales usually include both physical and mental health components, and we planned to assess both
Proportion of participants with a major adverse cardiovascular event (MACE) (defined by the trialist) (Kip 2008); we intended to assess each component of this composite outcome separately
Proportion of participants with a serious adverse event (defined as any untoward medical occurrence that resulted in death, was life threatening, was persistent, or led to significant disability or prolonged hospitalisation (ICH‐GCP 1997))
Any improvement in venous patency (assessed by objective measures such as venography, where pre‐ and postcomparative data on the degree of restoration of the lumen were available)
Complete clot lysis (defined as the achievement of full patency of the affected vein, or complete dissolution of the clot, by objective measures)
Recurrence of upper extremity deep vein thrombosis (as defined by the trialist) at 12 months
We planned to assess all continuous and dichotomous outcomes at two time points.
Up to one month.
At maximum follow‐up (more than one month) ‐ the time point of primary interest
We did not include cost as an outcome. We intended to narratively describe in the Discussion section whether any randomised clinical trials reported costs, but we did not consider that this would affect our main conclusions.
Search methods for identification of studies
Electronic searches
The Cochrane Vascular Information Specialist (CIS) searched the following databases for relevant trials.
Cochrane Vascular Specialised Register (29 March 2017)
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 2) via the Cochrane Central Register of Studies (CRS) (www.metaxis.com/CRSWeb/Index.asp) (29 March 2017)
See Appendix 1 for details of the search strategy used to search the CENTRAL.
The Cochrane Vascular Specialised Register is maintained by the CIS and is constructed from weekly electronic searches of MEDLINE, Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature), and AMED (Allied and Complementary Medicine), and through the handsearching of relevant journals. The full list of the databases, journals, and conference proceedings that we searched, as well as the search strategies we used are described in the Specialised Register section of the Cochrane Vascular module in the Cochrane Library (www.cochranelibrary.com).
The CIS searched the following trial databases (29 March 2017) for details of ongoing and unpublished studies.
World Health Organization International Clinical Trials Registry (apps.who.int/trialsearch/).
ClinicalTrials.gov (clinicaltrials.gov/).
ISRCTN register (www.isrctn.com/).
See Appendix 2 for details of trial registries searches.
Searching other resources
We searched the reference lists of review articles for any eligible trials. We also searched the trial registries of the European Medical Agency and the US Food and Drug Administration (December 2016). In addition, we looked through conference abstracts reported in the journal, CHEST, since 2003 and contacted Abbott laboratories, AB Kabi, Aventis Behringer, Bristol‐Myers Squibb, Chiesi, Genentech, Novo Nordisk, Microbix, Sanofi‐Aventis, and Sumitomo for details of any relevant ongoing studies.
Data collection and analysis
We performed the review following Cochrane recommendations (Higgins 2011). We intended to perform the analyses using Review Manager 5.3 (RevMan 2014), STATA 14 (Stata 2014), and Trial Sequential Analysis (CTU 2011).
Selection of studies
Two review authors (JF and EEN) independently assessed each identified trial. If a trial was identified as relevant by one review author, but not by another, the reasoning behind each decision would be discussed. If no agreement could be reached, a third review author (JCJ) would resolve the issue.
Data extraction and management
We planned for two review authors (JF and EEN) to independently extract and validate data (including any use of venous stents or venoplasty) using data extraction forms designed for the purpose. We aimed to resolve any disagreement by discussion, consulting a third review author (JCJ) if necessary. If relevant data were not available, we intended to contact the trial authors.
Assessment of risk of bias in included studies
We intended to use the instructions given in the Cochrane Handbook for Systematic Reviews of Interventions in our evaluation of the methodology and risk of bias of the included trials (Higgins 2011). Two review authors (JF and EEN) would have independently assessed the included trials. We aimed to resolve any disagreement by discussion, consulting a third review author (JCJ) if necessary. We intended to evaluate the risk of bias in random sequence generation, allocation sequence concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other bias sources, in order to classify the randomised trials identified as being at low or high risk of bias. The latter trials overestimate benefits and underestimate harms (Schulz 1995; Moher 1998; Kjaergard 2001; Gluud 2006; Wood 2008; Lundh 2012; Savovic 2012).
We intended to classify each trial according to the following domains for each outcome result.
Random sequence generation
Low risk: if sequence generation is achieved using a computer random number generator or a random numbers table. Drawing lots, tossing a coin, shuffling cards and throwing dice are also considered adequate if performed by an independent adjudicator
Unclear risk: If there is insufficient information to permit a judgement of 'low risk' or 'high risk'
High risk: if the allocation sequence is not randomised or is only quasi‐randomised
Allocation sequence concealment
Low risk: if the allocation of participants is performed using a central independent unit; on‐site locked computer; or identical looking, numbered, sealed opaque envelopes, drug bottles or containers prepared by an independent investigator
Unclear risk: if there is insufficient information to permit a judgement of 'low risk' or 'high risk'
High risk: if the allocation sequence is known to the investigators who assigned participants
Blinding of participants and personnel
Low risk: if the participants and the personnel are blinded to treatment allocation and this is described
Unclear risk: if there is insufficient information to permit a judgement of 'low risk' or 'high risk'
High risk: if blinding of participants and personnel is not performed
Blinding of outcome assessment
Low risk: if the trial investigators performing the outcome assessments, analyses, and calculations are blinded to the intervention
Unclear risk: if there is insufficient information to permit a judgement of 'low risk' or 'high risk'
High risk: if blinding of outcome assessment is not performed
Incomplete outcome data
Low risk: (1) there are no dropouts or withdrawals for all outcomes, or (2) the numbers and reasons for the withdrawals and dropouts for all outcomes are clearly stated, could be described as being similar in both groups, and the trial handled missing data appropriately in intention‐to‐treat analysis using proper methodology (e.g. multiple imputations). Multiple imputation is a general approach to the problem of missing data. It aims to allow for the uncertainty about the missing data by creating several different plausible imputed datasets, and appropriately combining the results obtained from each of them. The first stage is to create multiple copies of the dataset, with the missing values replaced by imputed values. These are sampled from their predictive distribution based on the observed data; thus multiple imputation is based on a Bayesian approach. The imputation procedure must fully account for all uncertainty in predicting the missing values by injecting appropriate variability into the multiple imputed values. The second stage is to use standard statistical methods to fit the model of interest to each of the imputed datasets. The estimated associations from the imputed datasets will differ, and are only useful when averaged together to give overall estimated associations. Valid inferences are obtained because we are averaging over the distribution of the missing data given the observed data (Sterne 2009). As a general rule a trial is judged to be at a low risk of bias due to incomplete outcome data if the number of dropouts is less than 5%; however, this 5% cut‐off is not definitive
Unclear risk: if there is insufficient information to permit a judgement of 'low risk' or 'high risk'
High risk: the pattern of dropouts could be described as being different in the two intervention groups, or the trial uses improper methodology in dealing with the missing data (e.g. last observation carried forward)
Selective outcome reporting
Low risk: a protocol has been published before or at the time the trial was begun and the outcomes called for in the protocol are reported. If there is no protocol or the protocol is published after the trial has begun, reporting of the primary outcomes will grant the trial a grade of low risk of bias
Unclear risk: if there is no protocol and the primary outcomes are not reported
High risk: if the outcomes detailed in the protocol are not reported
Other bias risk
Low risk of bias: the trial appears to be free of other components (e.g. academic bias or for‐profit bias) that could put it at risk of bias
Unclear risk of bias: the trial may or may not be free of other components that could put it at risk of bias
High risk of bias: there are other factors in the trial that could put it at risk of bias (e.g. authors have conducted trials on the same topic, for‐profit bias, etc.).
Overall risk of bias
Low risk of bias: we intended to classify the outcome result as having an overall 'low risk of bias' only if we considered all of the bias risk domains described above to be at low risk of bias
High risk of bias: we intended to classify the outcome result as having an overall 'high risk of bias' if we considered any of the bias risk domains described above to be at unclear or high risk of bias
Measures of treatment effect
Dichotomous outcomes
We intended to calculate risk ratios (RRs) with 95% confidence interval (CI) for dichotomous outcomes.
Continous outcomes
We intended to include both end scores and change from baseline scores in our analyses. If both were reported, we would use end scores. We would calculate the mean differences (MDs) and standardised mean differences (SMDs) with 95% CI for continuous outcomes.
Unit of analysis issues
We intended individual participants to be the unit of analysis. We intended to include the results from the first phase of cross‐over trials (i.e. before participants cross over to another intervention). We did not intend to include cluster randomised trials.
Dealing with missing data
Dichotomous outcomes
We did not intend to impute missing values for any outcomes in our primary analysis. We intended to impute data in two of our planned sensitivity analyses for dichotomous outcomes (see 'Sensitivity analysis').
Continous outcomes
If both end scores and change from baseline scores were reported, then we intended to use end scores. If change values only were reported, we intended to analyse the results together with end scores (Higgins 2011a). If standard deviations were not reported, we intended to calculate them using data from the trial if possible. We did not intend to impute missing values for any outcomes in our primary analysis. We intended to impute data in our sensitivity analysis for continuous outcomes (see 'Sensitivity analysis').
Assessment of heterogeneity
We intended to investigate forest plots to visually assess any sign of heterogeneity between the included studies. Moreover, we intended to assess the presence of statistical heterogeneity using the Chi2 test (threshold P < 0.10) and by measuring the amount of heterogeneity using the I2 statistic (Higgins 2002; Higgins 2003).
Assessment of reporting biases
We intended to use a funnel plot to assess reporting bias if 10 or more trials were included. We intended to assess the risk of publication and other reporting bias from any asymmetry in the funnel plot. For dichotomous outcomes we intended to test for asymmetry using the Harbord test (Harbord 2006). For continuous outcomes we intended to use the regression asymmetry test (Egger 1997).
Data synthesis
Meta‐analysis
We undertook this systematic review according to the recommendations stated in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) and according to Keus 2010 and Jakobsen 2014. We intended to use the statistical software Review Manager 5.3 (RevMan 2014) provided by Cochrane to meta‐analyse data.
Trial sequential analysis
Multiple meta‐analyses risk producing random errors due to both lack of data and repetitive testing of data (Pogue 1997; Brok 2008; Brok 2009; Thorlund 2009; Higgins 2011a; Wetterslev 2008). Trial sequential analysis (TSA) can be used to assess the risk of this occurring (www.ctu.dk/tsa/) (Thorlund 2011). The required information size can be estimated to minimise random errors (Wetterslev 2008; Wetterslev 2009), and is calculated using: the event proportion in the control group; a plausible relative risk reduction (e.g. based on prior reviews) or the relative risk reduction observed in the included trials with low risk of bias; and the assumed heterogeneity (Turner 2013) or diversity of the meta‐analysis (Wetterslev 2008; Wetterslev 2009). TSA allows an assessment of whether the significance threshold is breached each time a new trial is included in the meta‐analysis. This may be done despite not yet having reached the required information size, since the threshold boundaries adjust according to the amount of data included in the meta‐analysis (Wetterslev 2008).
We planned to estimate the diversity‐adjusted required information size (Wetterslev 2009) based on the proportion of participants with an outcome in the control group. As we planned to investigate three primary outcomes, we intended to use an alpha of 2.5% (Jakobsen 2014), a beta of 20%, and the diversity suggested by the trials in the meta‐analysis (Jakobsen 2014).
As anticipated intervention effects for the primary outcomes in the TSA we intended to use the following relative risk reductions or increases, because these seem to be the maximum realistic intervention effect estimates based on former studies, trials, and meta‐analyses.
Primary outcomes
Bleeding complications: relative risk reduction or increase of 100% (Watson 2016)
Pulmonary embolism: relative risk reduction or increase of 10% (Watson 2016)
All‐cause mortality: relative risk reduction or increase of 10% (Watson 2016)
We intended to estimate the diversity‐adjusted required information size (Wetterslev 2009) based on the proportion of participants with an outcome in the control group. As we planned to investigate seven secondary outcomes, we intended to use an alpha of 1.25% (Jakobsen 2014), a beta of 20%, and the diversity suggested by the trials in the meta‐analysis (Jakobsen 2014).
As anticipated intervention effects for the secondary outcomes in the TSA we intended to use the following relative risk reductions or increases, because they seem to be realistic intervention effect estimates based on former studies, trials and meta‐analyses as cited below.
Secondary outcomes
Post‐thrombotic syndrome: relative risk reduction or increase of 35% (Watson 2016)
Quality of life: observed standard deviation, a clinically relevant mean difference equal to standard deviation/2, an alpha of 1.43%, and a beta of 20%
MACE: clinically minimal relevant relative risk reduction or increase of 10%
Serious adverse events: clinically minimal relevant relative risk reduction or increase of 10%
Any improvement in venous patency: relative risk reduction or increase of 140% (Watson 2016)
Complete clot lysis: relative risk reduction or increase of 130% (Watson 2016)
Recurrent deep vein thrombosis: relative risk reduction or increase of 40% (Watson 2016)
As a supplementary TSA, we intended to use the limit of the CI closest to zero effect as the anticipated intervention effect for all TSAs (Jakobsen 2014).
Assessment of significance
We intended to assess our intervention effects using both random‐effects model meta‐analyses (DerSimonian 1986) and fixed‐effect model meta‐analyses (DeMets 1987). We intended to use the more conservative point estimate of the two (i.e. the estimate closest to zero effect) (Jakobsen 2014). If the two estimates had been equal, we would have used the estimate with the widest confidence interval. As we planned to investigate three primary outcomes, we therefore intended to consider a P value less than 2.5% as statistically significant (Jakobsen 2014). We intended to use an eight‐step procedure to assess whether the thresholds for significance were crossed or not (Jakobsen 2014).
We intended to present a table describing the types of serious adverse events in each trial.
Subgroup analysis and investigation of heterogeneity
We intended to perform the following subgroup analyses.
A: High risk of bias outcomes compared with low risk of bias outcomes
B: Route of administration:
Systemic thrombolysis.
Loco‐regional thrombolysis.
Catheter‐directed thrombolysis.
C: Type of thrombolytic drug:
Streptokinase.
Urokinase.
rt‐PA.
D: Types of participants (primary upper extremity deep vein thrombosis versus secondary upper extremity deep vein thrombosis).
E: Trials with different comparisons:
Thrombolytics added to anticoagulation versus anticoagulation.
Thrombolytics versus anticoagulation.
Thrombolytics versus any other type of medical intervention.
F: Participants who underwent thoracic outlet decompression compared with participants who did not. If there is great variability in when the thoracic outlet decompression was performed, we intended to perform a subgroup comparing the time of placement.
G: Participants who had a venous stent placed compared with participants who did not have a venous stent placed.
Sensitivity analysis
To assess the potential impact of bias, we intended to perform a sensitivity analysis excluding trials with overall 'high risk of bias'.
To assess the potential impact of the missing data, we intended to perform the two following analyses.
'Best‐worst‐case' scenario: we intended to assume that all participants lost to follow up in the experimental group: did not have severe bleeding, did not develop a pulmonary embolism, did not develop post‐thrombotic syndrome, did not have a major cardiovascular event, did not develop a serious adverse event, had an improvement in venous patency, had a complete clot lysis, did not have a recurrence, and survived. We intended also to assume a beneficial outcome with regard to quality of life (defined as the group mean plus both one and two standard deviations of the group mean). We intended to assume that all participants with missing outcomes in the control group: had severe bleeding, developed a pulmonary embolism, developed post‐thrombotic syndrome, had a major cardiovascular event, developed a serious adverse event, did not have an improvement in venous patency, did not have a complete clot lysis, had a recurrence, and died. We intended also to assume a 'harmful outcome' with regard to quality of life (defined as the group mean minus both one and two standard deviations of the group mean) (Jakobsen 2014).
'Worst‐best‐case' scenario: We intended to assume that all participants lost to follow‐up in the experimental group: had severe bleeding, developed a pulmonary embolism, developed post‐thrombotic syndrome, had a major cardiovascular event, developed a serious adverse event, did not have an improvement in venous patency, did not have a complete clot lysis, had a recurrence, and died. We intended also to assume a 'harmful outcome' with regard to quality of life (defined as the group mean minus both one and two standard deviations of the group mean). We intended to assume that all participants with missing outcomes in the control group: did not have severe bleeding, did not develop a pulmonary embolism, did not develop post‐thrombotic syndrome, did not have a major cardiovascular event, did not develop a serious adverse event, had an improvement in venous patency, had a complete clot lysis, did not have a recurrence, and survived. We intended also to assume a beneficial outcome with regard to quality of life (defined as the group mean plus both one and two standard deviations of the group mean) (Jakobsen 2014).
We intended to present results from both scenarios in our review.
To assess the potential impact of missing SDs for continuous outcomes, we intended to perform the following sensitivity analysis.
Where SDs were missing and not possible to calculate, we intended to impute them from trials with similar populations and low risk of bias. If no such trials could be found, we intended to impute SDs from trials with a similar population.
We intended to impute SDs from all trials.
'Summary of findings'
We intended to use the GRADE system to assess the quality of the body of evidence associated with each of the major outcomes in our review by constructing 'Summary of findings' (SoF) tables using the GRADE software (www.guidelinedevelopment.org/; Guyatt 2008). The GRADE approach appraises the quality of a body of evidence based on the extent to which one can be confident that an estimate of effect or association reflects the item being assessed. The quality measure of a body of evidence considers within‐study risk of bias, the directness of the evidence, heterogeneity of the data, the precision of effect estimates (Jakobsen 2014), and risk of publication bias. We intended that our primary SoF tables and conclusions would be based on the results of trials with a low risk of bias, reporting on our primary outcomes of bleeding, pulmonary embolism, and all‐cause mortality (Schulz 1995; Moher 1998; Kjaergard 2001; Gluud 2006; Wood 2008; Lundh 2012; Savovic 2012).
Results
Description of studies
We assessed all studies according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) and the protocol for this review (Feinberg 2016).
Results of the search
Our search identified 61 references. On screening we found one duplicate, and excluded this and 59 other references. We obtained full text for one study and, on review, subsequently excluded this study also (Figure 1). We explain the reason for the exclusion of eight studies in the 'Characteristics of excluded studies' table.
1.
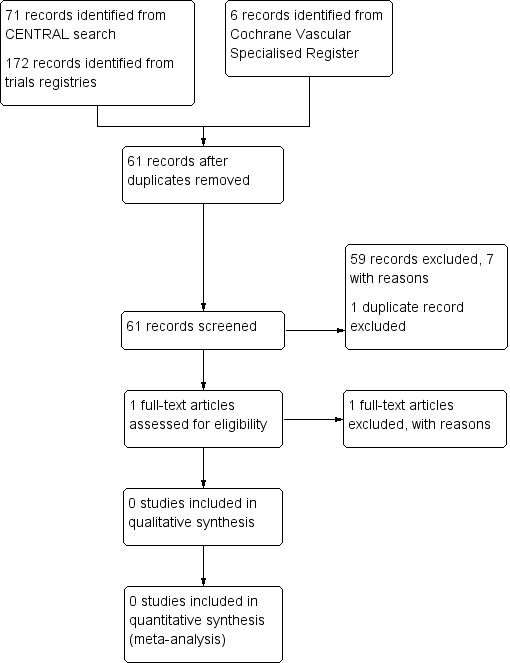
Study flow diagram.
Included studies
We identified no randomised clinical trials eligible for inclusion.
Excluded studies
We excluded all but eight of the studies identified through electronic searches for obvious reasons. Of the remaining eight, two studies were not randomised (AbuRahma 1996; Schrijver 2015), two studies randomised participants with acute lower extremity deep vein thrombosis (Sandset 2012; Haig 2015); three studies were of drugs other than thrombolytics (Monreal 1996; Arneklo‐Nobin 1998; Mismetti 2003) and one study compared two doses of thrombolytics (Krupski 1989). Please see Characteristics of excluded studies for further details.
Risk of bias in included studies
No study met the eligibility criteria.
Effects of interventions
No study met the eligibility criteria.
Discussion
Summary of main results
We identified no randomised clinical trials assessing thrombolysis for the treatment of acute upper extremity deep vein thrombosis as an add‐on therapy to anticoagulation, alone compared with anticoagulation, or alone compared with any other type of medical intervention.
Overall completeness and applicability of evidence
We identified no randomised clinical trials eligible for inclusion. As such, there is no evidence from randomised clinical trials conducted specifically in individuals with acute upper extremity deep vein thrombosis to support the use of thrombolysis. Randomised clinical trials have investigated the use of thrombolysis for the treatment of acute lower extremity deep vein thrombosis and a systematic review of the evidence for this intervention has been performed (Watson 2016). This systematic review also included trials in which a small number of participants had acute upper extremity deep vein thrombosis.
Quality of the evidence
We identified no randomised clinical trials eligible for inclusion and therefore were not able to assess the quality of the evidence.
Potential biases in the review process
None of the review authors have or had any conflicts of interests. The CIS conducted the comprehensive literature search. Two review authors independently screened the titles and abstracts of identified references. Any disagreement was settled through discussion. In addition, we looked through conference abstracts reported in the journal, CHEST, since 2003, and contacted Abbott laboratories, AB Kabi, Aventis Behringer, Bristol‐Myers Squibb, Chiesi, Genentech, Novo Nordisk, Microbix, Sanofi‐Aventis, and Sumitomo for any ongoing studies of relevance.
Agreements and disagreements with other studies or reviews
We have identified no former reviews assessing randomised clinical trials investigating the effects of thrombolysis in individuals with acute upper extremity deep vein thrombosis.
We identified three non‐randomised studies assessing thrombolysis for acute upper extremity deep vein thrombosis. Due to a lack of randomisation as well as other bias, the evidence from these three studies cannot guide clinical practice (Garattini 2016; Jakobsen 2013).
AbuRahma 1996 looked at 19 adults with axiliary‐subclavian vein thrombosis. Nine participants underwent conventional therapy with warfarin and heparin, and 11 underwent initial treatment with thrombolysis and subsequent treatment with warfarin and heparin. AbuRahma 1996 found thrombolysis to be superior to conventional therapy, but found that the difference in cost was USD 19,039 more for the treatment with thrombolysis.
Petrakis 2000 conducted a case‐report of 20 adults receiving either anticoagulation (n = 11) or thrombolysis (n = 9). They found increased clinical benefit of thrombolysis over anticoagulation and recommended thrombolysis for axiliary‐subclavian vein thrombosis when participants have a lifestyle depending on continuous usage of the involved extremity and also have at least a medium‐term life expectancy.
Sabeti 2002 conducted a retrospective cohort study of 95 consecutive adults with subclavian–axillary vein thrombosis treated with either systemic thrombolysis and subsequent anticoagulation (n = 33) or anticoagulation only (n = 62). They found that thrombolysis improved venous recanalisation rates versus anticoagulation, but on the basis of high rates of complications and a lack of clinical benefit, suggested that anticoagulation alone was the preferred option.
Authors' conclusions
Implications for practice.
As we identified no relevant randomised clinical trials, there is currently insufficient evidence to draw conclusion on the benefits or harms of thrombolysis for the treatment of individuals with acute upper extremity deep vein thrombosis as an add‐on therapy to anticoagulation, alone compared with anticoagulation, or alone compared with any other type of medical intervention. Clinicians may wish to consider the lack of randomised clinical trial evidence on the effects of thrombolysis for acute upper extremity deep vein thrombosis before using this intervention.
Implications for research.
There are currently no randomised clinical trials assessing the effects of thrombolysis for the treatment of individuals with acute upper extremity deep vein thrombosis. Trials may be conducted assessing the benefits and harms of thrombolytics given that thrombolysis might increase the chance of complete clot lysis and prevent post‐thrombotic syndrome in acute lower extremity deep vein thrombosis. However, this, in theory, could come at the expense of an increased risk of bleeding complications. Future trials may stratify participants according to the risk of bleeding in order to identify what patients may benefit from thrombolysis for acute upper extremity deep vein thrombosis. Future trials should preferably be large enough to assess clinical outcomes such as all‐cause mortality, serious adverse events, and quality of life and, as such, multicentre trials may be required. Such trials should also be conducted with low risk design, e.g. low risk of random errors, and low risk of systematic error (bias). Trials should also be designed and reported according to the SPIRIT and CONSORT guidelines (Schulz 2010; Chan 2013).
Notes
Parts of the methods section of the protocol of this review are based on a standard template established by Cochrane Vascular.
Acknowledgements
We would like to thank Cochrane Vascular for their help and guidelines.
Appendices
Appendix 1. CENTRAL search strategy
| #1 | MESH DESCRIPTOR Upper Extremity Deep Vein Thrombosis EXPLODE ALL TREES | 13 |
| #2 | MESH DESCRIPTOR Axillary Vein EXPLODE ALL TREES | 24 |
| #3 | MESH DESCRIPTOR Subclavian Vein EXPLODE ALL TREES | 95 |
| #4 | MESH DESCRIPTOR Thoracic Outlet Syndrome EXPLODE ALL TREES | 14 |
| #5 | UEDVT:TI,AB,KY | 3 |
| #6 | Paget*:TI,AB,KY | 189 |
| #7 | (upper near6 thromb*):TI,AB,KY | 68 |
| #8 | (arm near6 thromb*):TI,AB,KY | 308 |
| #9 | (central venous near6 thromb*):TI,AB,KY | 69 |
| #10 | (arm near3 clot*):TI,AB,KY | 17 |
| #11 | effort near3 thromb* | 2 |
| #12 | (subclavian near2 thromb*):TI,AB,KY | 32 |
| #13 | (thoracic and outlet):TI,AB,KY | 26 |
| #14 | (thoracic and outlet):TI,AB,KY | 26 |
| #15 | #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 | 780 |
| #16 | MESH DESCRIPTOR Thrombolytic Therapy EXPLODE ALL TREES | 1535 |
| #17 | MESH DESCRIPTOR Fibrinolytic Agents EXPLODE ALL TREES | 11015 |
| #18 | MESH DESCRIPTOR Fibrinolysis EXPLODE ALL TREES | 945 |
| #19 | MESH DESCRIPTOR Plasminogen Activators EXPLODE ALL TREES | 2240 |
| #20 | (plasminogen near2 activator* ):TI,AB,KY | 3667 |
| #21 | (tPA or t‐PA or rtPA or rt‐PA):TI,AB,KY | 2183 |
| #22 | (thromboly* or fibrinoly* or antithrombotic or antithrombic):TI,AB,KY | 8922 |
| #23 | (recanalis* or recanaliz*):TI,AB,KY | 1016 |
| #24 | (((clot* or thrombus) near3 (lyse or lysis or dissolve* or dissolution))):TI,AB,KY | 913 |
| #25 | urokinase:TI,AB,KY | 808 |
| #26 | alteplase :TI,AB,KY | 704 |
| #27 | reteplase:TI,AB,KY | 112 |
| #28 | tenecteplase:TI,AB,KY | 153 |
| #29 | saruplase:TI,AB,KY | 33 |
| #30 | anistreplase:TI,AB,KY | 156 |
| #31 | monteplase:TI,AB,KY | 14 |
| #32 | streptokinase:TI,AB,KY | 1294 |
| #33 | staphylokinase:TI,AB,KY | 17 |
| #34 | (avelizin or awelysin):TI,AB,KY | 0 |
| #35 | (celiase or distreptase or Kabikinase or kabivitrum):TI,AB,KY | 12 |
| #36 | (Streptase or streptodecase or apsac or Abbokinase or renokinase ):TI,AB,KY | 110 |
| #37 | (Actilyse or Activase or Eminase or Retavase or Rapilysin or desmopletase or u‐pa or alfimeprase ):TI,AB,KY | 89 |
| #38 | (streptodornase ):TI,AB,KY | 50 |
| #39 | (pro?urokinase or rpro?uk ):TI,AB,KY | 44 |
| #40 | (lumbrokinase or duteplase or lanoteplase or pamiteplase):TI,AB,KY | 45 |
| #41 | #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31 or #32 or #33 or #34 or #35 or #36 or #37 or #38 or #39 or #40 | 19114 |
| #42 | #15 and #41 | 71 |
Appendix 2. Clinical trials database searches
ClinicalTrials.gov
66 studies found for: arm and thrombolysis
67 studies found for: upper extremity and thrombolysis
0 studies for: paget schroetter
World Health Organization International Clinical Trials Registry
12 records for 8 trials found for: arm and thrombolysis
12 records for 8 trials found for: upper extremity and thrombolysis
0 studies for: paget schroetter
ISRCTN register
15 results arm and thrombolysis
No results found for "upper extremity and thrombolysis"
No results found for "paget schroetter"
Appendix 3. Glossary
Diversity‐adjusted required information size: this term relates to trial sequential analysis (see below). When performing a trial sequential analysis, you must calculate how much information is needed before you can make conclusions with confidence. The information size is diversity adjusted, meaning that, based on how much the trials differ between each other, we will require more or less information before we are confident in our results.
Patency (of a vessel): the degree of openness of a vessel (artery or vein). A vessel with a high patency is only blocked minimally and blood flows freely through the vessel.
Random‐effects model: a statistical model of how to meta‐analyse (pool or combine) study results. It can be seen as an alternative to the fixed‐effect model. It is a way of stating how will you weigh the results of small trials compared with the results from larger trials. There are different kinds of random‐effects models available for use.
Trial sequential analysis: an analysis that attempts to assess how robust the conclusions from your data are. Some people argue that it is a more sound statistical test than using the traditional P value that is often used in medical literature.
Characteristics of studies
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| AbuRahma 1996 | Not randomised |
| Arneklo‐Nobin 1998 | Experimental group was given reserpine (not a thrombolytic drug) |
| Haig 2015 | Treatment of deep vein thrombosis of the lower extremities |
| Krupski 1989 | Participants received two doses of thrombolysis. In addition, only one participant had deep vein thrombosis of the upper extremities |
| Mismetti 2003 | Compared heparin with warfarin |
| Monreal 1996 | Compared prophylactic heparin versus no heparin |
| Sandset 2012 | Treatment of deep vein thrombosis of the lower extremities |
| Schrijver 2015 | Not randomised |
Differences between protocol and review
None.
Contributions of authors
JF: Guarantor of the review, protocol drafting, acquiring trial reports, trial selection, data extraction, data analysis, data interpretation, review drafting and future review updates. EEN: Protocol drafting, acquiring trial reports, trial selection, data extraction, data analysis, data interpretation, review drafting and future review updates. JCJ: Protocol drafting, data interpretation, review drafting and future review updates.
Sources of support
Internal sources
No sources of support supplied
External sources
-
Chief Scientist Office, Scottish Government Health Directorates, The Scottish Government, UK.
The Cochrane Vascular editorial base is supported by the Chief Scientist Office.
Declarations of interest
Joshua Feinberg (JF): None known Emil Eik Nielsen (EEN): None known Janus Christian Jakobsen (JCJ): None known
New
References
References to studies excluded from this review
AbuRahma 1996 {published data only}
- AbuRahma AF, Short YS, White JF 3rd, Boland JP. Treatment alternatives for axillary‐subclavian vein thrombosis: long‐term follow‐up. Cardiovascular Surgery (London, England) 1996;4(6):783‐7. [DOI] [PubMed] [Google Scholar]
Arneklo‐Nobin 1998 {published data only}
- Arneklo‐Nobin B, Norgren L, Johansen K. Beneficial effects of intra‐arterial reserpine after upper‐extremity embolectomy: a prospective randomised trial. European Journal of Vascular and Endovascular Surgery 1998;2(5):305‐8. [DOI] [PubMed] [Google Scholar]
Haig 2015 {published data only}
- Haig Y, Enden TR, Grøtta O, Sandset PM, Slagsvold CE, Sandbæk G, et al. Five‐year outcome after catheter‐directed thrombolysis for upper femoral and/or iliac vein thrombosis: results of a randomized controlled trial (the CaVenT study). Cardiovascular and Interventional Radiology 2015;38:s193. [Google Scholar]
Krupski 1989 {published data only}
- Krupski WC, Feldman RK, Rapp JH. Recombinant human tissue‐type plasminogen activator is an effective agent for thrombolysis of peripheral arteries and bypass grafts: preliminary report. Journal of Vascular Surgery 1989;10(5):491‐8. [DOI] [PubMed] [Google Scholar]
Mismetti 2003 {published data only}
- Mismetti P, Mille D, Laporte S, Charlet V, Buchmuller‐Cordier A, Jacquin JP, et al. Low‐molecular‐weight heparin (nadroparin) and very low doses of warfarin in the prevention of upper extremity thrombosis in cancer patients with indwelling long‐term central venous catheters: a pilot randomized trial. Haematologica 2003;88(1):67‐73. [PubMed] [Google Scholar]
Monreal 1996 {published data only}
- Monreal M, Alastrue A, Rull M, Mira X, Muxart J, Rosell R, et al. Upper extremity deep venous thrombosis in cancer patients with venous access devices ‐ prophylaxis with a low molecular weight heparin (Fragmin). Thrombosis and Haemostasis 1996;75(2):251‐3. [PubMed] [Google Scholar]
Sandset 2012 {published data only}
- Sandset PM. Thrombolysis reduced the postthrombotic syndrome in acute iliofemoral DVT. Annals of Internal Medicine 2012;156:31‐38. [DOI] [PubMed] [Google Scholar]
Schrijver 2015 {published data only}
- Schrijver AM, Borst GJ, Herwaarden JA, Vonken EJ, Moll FL, Vos JA, et al. Catheter‐directed thrombolysis for acute upper extremity ischemia. Journal of Cardiovascular Surgery 2015;56(3):433‐9. [PubMed] [Google Scholar]
Additional references
Ali 2014
- Ali R, Hossain MS, Islam A, Arman SI, Raju GS, Dasgupta P, et al. Aspect of thrombolytic therapy: a review. The Scientific World Journal 2014;2014:586510. [DOI: 10.1155/2014/586510] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bates 2012
- Bates SM, Jaeschke R, Stevens SM, Goodacre S, Wells PS, Stevenson MD, et al. Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest 2012;141(2 Suppl):e351S‐418S. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brok 2008
- Brok J, Thorlund K, Gluud C, Wetterslev J. Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta‐analyses. Journal of Clinical Epidemiology 2008;61(8):763‐9. [DOI] [PubMed] [Google Scholar]
Brok 2009
- Brok J, Thorlund K, Wetterslev J, Gluud C. Apparently conclusive meta‐analyses may be inconclusive. Trial sequential analysis adjustment of random error risk due to repetitive testing of accumulating data in apparently conclusive neonatal meta‐analyses. International Journal of Epidemiology 2009;38(1):287‐98. [DOI] [PubMed] [Google Scholar]
Chan 2013
- Chan A‐W, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža‐Jerić K, et al. SPIRIT 2013 Statement: defining standard protocol items for clinical trials. Annals of Internal Medicine 2013;158(3):200‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
CTU 2011
- Copenhagen Trial Unit. TSA ‐ Trial Sequential Analysis. www.ctu.dk/tsa/ 2011 (accessed 3 April 2014).
DeMets 1987
- DeMets DL. Methods for combining randomized clinical trials: strengths and limitations. Statistics in Medicine 1987;6(3):341‐50. [PUBMED: 3616287] [DOI] [PubMed] [Google Scholar]
DerSimonian 1986
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7(3):177‐88. [PUBMED: 3802833] [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315(7109):629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elman 2006
- Elman EE, Kahn SR. The post‐thrombotic syndrome after upper extremity deep venous thrombosis in adults: a systematic review. Thrombosis Research 2006;117:609‐14. [DOI] [PubMed] [Google Scholar]
Engelberger 2012
- Engelberger RP, Kucher N. Management of deep vein thrombosis of the upper extremity. Circulation 2012;126:768‐73. [DOI] [PubMed] [Google Scholar]
Garattini 2016
- Garattini S, Jakobsen JC, Wetterslev J, Bertele V, Banzi R, Rath A, et al. Evidence‐based clinical practice: overview of threats to the validity of evidence and how to minimise them. European Journal of Internal Medicine 2016;32:13‐21. [DOI: 10.1016/j.ejim.2016.03.020] [DOI] [PubMed] [Google Scholar]
Gluud 2006
- Gluud LL. Bias in clinical intervention research. American Journal of Epidemiology 2006;163(6):493‐501. [DOI] [PubMed] [Google Scholar]
Guyatt 2008
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck‐Ytter Y, Alonso‐Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336(7650):924‐6. [PUBMED: 18436948] [DOI] [PMC free article] [PubMed] [Google Scholar]
Harbord 2006
- Harbord RM, Egger M, Sterne JA. A modified test for small‐study effects in meta‐analyses of controlled trials with binary endpoints. Statistics in Medicine 2006;25(20):3443‐57. [PUBMED: 16345038] [DOI] [PubMed] [Google Scholar]
Higgins 2002
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21(11):1539‐58. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011a
- Higgins JP, Whitehead A, Simmonds M. Sequential methods for random‐effects meta‐analysis. Statistics in Medicine 2011;30(9):903‐21. [PUBMED: 21472757] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hull 2015
- Hull RD, Garcia DA. Therapeutic use of unfractionated heparin and low molecular weight heparin. UpToDate®. Available at: www.uptodate.com/contents/therapeutic‐use‐of‐unfractionated‐heparin‐and‐low‐molecular‐weight‐heparin September 2015 (accessed 30 October 2015).
ICH‐GCP 1997
- International ConHEWG International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. ICH Harmonised Tripartite Guideline. Guideline for good clinical practice CFR & ICH Guidelines. Vol. 1, Pennsylvania, USA: Barnett International/PAREXEL 1997.
Jakobsen 2013
- Jakobsen JC, Gluud C. The necessity of randomized clinical trials. British Journal of Medicine and Medical Research 2013;3(4):1453‐1468. [Google Scholar]
Jakobsen 2014
- Jakobsen JC, Wetterslev J, Winkel P, Lange T, Gluud C. Thresholds for statistical and clinical significance in systematic reviews with meta‐analytic methods. BMC Medical Research Methodology 2014;14:120. [PUBMED: 25416419] [DOI] [PMC free article] [PubMed] [Google Scholar]
Joffe 2002
- Joffe HV, Goldhaber SZ. Upper‐extremity deep vein thrombosis. Circulation 2002;106:1874‐80. [DOI] [PubMed] [Google Scholar]
Kearon 2016
- Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest 2016;149(2):315‐52. [PUBMED: 26867832] [DOI] [PubMed] [Google Scholar]
Keus 2010
- Keus F, Wetterslev J, Gluud C, Laarhoven CJ. Evidence at a glance: error matrix approach for overviewing available evidence. BMC Medical Research Methodology 2010; Vol. 10:90. [DOI] [PMC free article] [PubMed]
Kip 2008
- Kip KE, Hollabaugh K, Marroquin OC, Williams DO. The problem with composite end points in cardiovascular studies: the story of major adverse cardiac events and percutaneous coronary intervention. Journal of the American College of Cardiology 2008;51(7):701‐7. [PUBMED: 18279733] [DOI] [PubMed] [Google Scholar]
Kjaergard 2001
- Kjaergard LL, Villumsen J, Gluud C. Reported methodologic quality and discrepancies between large and small randomized trials in meta‐analyses. Annals of Internal Medicine 2001;135(11):982‐9. [DOI] [PubMed] [Google Scholar]
Koury 2011
- Koury JP, Burke CT. Endovascular management of acute upper extremity deep venous thrombosis and the use of superior vena cava filters. Seminars in Interventional Radiology 2011;28(1):3‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kucher 2011
- Kucher N. Clinical practice. Deep‐vein thrombosis of the upper extremities. The New England Journal of Medicine 2011;364(9):861‐9. [DOI] [PubMed] [Google Scholar]
Lundh 2012
- Lundh A, Sismondo S, Lexchin J, Busuioc OA, Bero L. Industry sponsorship and research outcome. Cochrane Database of Systematic Reviews 2012, Issue 12. [DOI: 10.1002/14651858.MR000033.pub2] [DOI] [PubMed] [Google Scholar]
Moher 1998
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta‐analyses?. Lancet 1998;352(9128):609‐13. [DOI] [PubMed] [Google Scholar]
Patterson 2010
- Patterson BO, Hinchliffe R, Loftus IM, Thompson MM, Holt PJ. Indications for catheter‐directed thrombolysis in the management of acute proximal deep venous thrombosis. Arteriosclerosis, Thrombosis, and Vascular Biology 2010;30:669‐74. [DOI] [PubMed] [Google Scholar]
Petrakis 2000
- Petrakis IE, Katsamouris A, Kafassis E, D'Anna M, Sciacca VV. Two different therapeutic modalities in the treatment of the upper extremity deep vein thrombosis: preliminary investigation with 20 case reports. International Journal of Angiology 2000;9(1):46‐50. [PUBMED: 10629326] [DOI] [PubMed] [Google Scholar]
Pogue 1997
- Pogue JM, Yusuf S. Cumulating evidence from randomized trials: utilizing sequential monitoring boundaries for cumulative meta‐analysis. Controlled Clinical Trials 1997;18(6):580‐93; discussion 661‐6. [PUBMED: 9408720] [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sabeti 2002
- Sabeti S, Schillinger M, Mlekusch W, Haumer M, Ahmadi R, Minar E. Treatment of subclavian‐axillary vein thrombosis: long‐term outcome of anticoagulation versus systemic thrombolysis. Thrombosis Research 2002;108(5‐6):279‐85. [PUBMED: 12676186] [DOI] [PubMed] [Google Scholar]
Saseedharan 2012
- Saseedharan S, Bhargava S. Upper extremity deep vein thrombosis. International Journal of Critical Illness and Injury Science 2012;2:21‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Savovic 2012
- Savovic J, Jones HE, Altman DG, Harris RJ, Juni P, Pildal J, et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Annals of Internal Medicine 2012;157(6):429‐38. [DOI] [PubMed] [Google Scholar]
Schulz 1995
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273(5):408‐12. [DOI] [PubMed] [Google Scholar]
Schulz 2010
- Schulz KF, Altman DG, Moher D, CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. Annals of Internal Medicine 2010;152(11):726‐32. [DOI] [PubMed] [Google Scholar]
Stata 2014 [Computer program]
- StataCorp. Stata: Release 14. Available at: www.stata.com. College Station (TX): StataCorp, 2014.
Sterne 2009
- Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ 2009;338:b2393. [PUBMED: 19564179] [DOI] [PMC free article] [PubMed] [Google Scholar]
Thorlund 2009
- Thorlund K, Devereaux PJ, Wetterslev J, Guyatt G, Ioannidis JP, Thabane L, et al. Can trial sequential monitoring boundaries reduce spurious inferences from meta‐analyses?. International Journal of Epidemiology 2009;38(1):276‐86. [DOI] [PubMed] [Google Scholar]
Thorlund 2011
- Thorlund K, Engstrøm J, Wetterslev J, Brok J, Imberger G, Gluud C. User manual for trial sequential analysis (TSA). www.ctu.dk/tsa/files/tsa_manual.pdf 2011 (assessed 15 May 2015).
Turner 2013
- Turner RM, Bird SM, Higgins JP. The impact of study size on meta‐analyses: examination of underpowered studies in Cochrane reviews. PloS One 2013;8(3):e59202. [PUBMED: 23544056] [DOI] [PMC free article] [PubMed] [Google Scholar]
Watson 2016
- Watson L, Broderick C, Armon MP. Thrombolysis for acute deep vein thrombosis. Cochrane Database of Systematic Reviews 2016, Issue 11. [DOI: 10.1002/14651858.CD002783.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wetterslev 2008
- Wetterslev J, Thorlund K, Brok J, Gluud C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta‐analysis. Journal of Clinical Epidemiology 2008;61(1):64‐75. [DOI] [PubMed] [Google Scholar]
Wetterslev 2009
- Wetterslev J, Thorlund K, Brok J, Gluud C. Estimating required information size by quantifying diversity in random‐effects model meta‐analyses. BMC Medical Research Methodology 2009;9:86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wood 2008
- Wood L, Egger M, Gluud LL, Schulz KF, Juni P, Altman DG, et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta‐epidemiological study. BMJ 2008;336(7644):601‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Feinberg 2016
- Feinberg J, Nielsen EE, Jakobsen JC. Thrombolysis for acute upper extremity deep vein thrombosis. Cochrane Database of Systematic Reviews 2016, Issue 4. [DOI: 10.1002/14651858.CD012175] [DOI] [PMC free article] [PubMed] [Google Scholar]