

Abstract
A 78-year-old Japanese male was referred to our hospital with a 3-month history of anorexia and right abdominal pain. A colonoscopy showed circumferential narrowing of the ascending colon with deep ulceration. Biopsy was performed, and examination of the specimen demonstrated squamous cell carcinoma. Abdominal computed tomography demonstrated thickening of the wall of the ascending colon, multiple lymph node metastases, multiple liver metastases, and peritoneal dissemination. After right hemicolectomy, histological examination demonstrated adenosquamous carcinoma. Biomarker analysis showed a microsatellite stable, wild-type KRAS gene in exon 2 and BRAF V600E mutation. Despite undergoing intensive chemotherapy, the patient died 5 months postoperatively.
Keywords: Colon cancer, Adenosquamous carcinoma, BRAF V600E
Introduction
Colorectal cancer is one of the most common malignant solid tumors in Western countries as well as in Japan. With the exception of the lower rectum, most primary malignant colorectal tumors are adenocarcinoma, and the frequency of adenosquamous carcinoma of the colon and rectum is only approximately 0.1% [1–3]. The first case of colorectal adenosquamous carcinoma was reported by Herxheimer in 1907 and was described as a tumor with both adenocarcinoma and squamous cell carcinoma components [4]. So far, the ratio of adenocarcinoma and squamous cell carcinoma in the definition of adenosquamous carcinoma has not been established. Adenosquamous carcinoma of the colon and rectum is commonly located in the right colon and has a poor prognosis [5].
The BRAF gene is one of the RAF genes that participate in the RAS-RAF signaling pathway which mediate cellular responses to growth signals [6] and frequently mutate in colorectal cancer as well as in melanoma [7]. BRAF V600E is an activating mutation that accounts for approximately 90% of all BRAF mutations observed in colorectal cancer [8, 9]. The prognosis of colorectal cancer with BRAF mutation is reportedly poor [10].
So far, no reports have demonstrated the results of biomarker analysis of adenosquamous carcinoma of the colon and rectum. Here we describe an ascending colon adenosquamous carcinoma with BRAF V600E mutation.
Case presentation
A 78-year-old Japanese male was referred to Tokyo Metropolitan Cancer and Infectious diseases Center Komagome Hospital with a 3-month history of anorexia and right abdominal pain. He had a past medical history of gastric cancer. Laboratory evaluation revealed anemia and hypoalbuminemia. The levels of carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and squamous cell carcinoma antigen (SCC) were 488.2 U/ml (normal range, 0–37 U/ml), 8.7 ng/ml (normal range, 0–5.0 ng/ml), and 9.5 ng/ml (normal range, 0.3–1.7), respectively. A colonoscopy showed circumferential narrowing of the ascending colon with deep ulceration (Fig. 1). Biopsy was performed, and examination of the specimen demonstrated squamous cell carcinoma. Abdominal computed tomography demonstrated thickening of the wall of the ascending colon, multiple lymph node metastases, multiple liver metastases, and peritoneal dissemination.
Fig. 1.
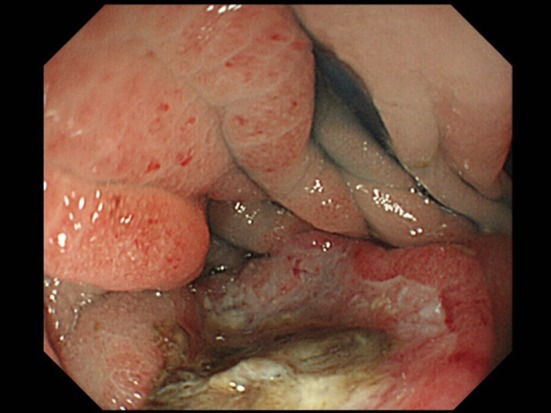
Colonoscopic findings: circumferential narrowing of the ascending colon with deep ulceration was observed
A right hemicolectomy was performed. Pathological examination of the colon specimen revealed an ulcerative lesion with a distinct border, measuring 8.0 × 6.5 cm (Fig. 2). The mass had invaded the retroperitoneal tissue, and lymphatic and venous invasion were observed. Five out of 46 lymph nodes contained metastatic tumor. Histological examination of the mass demonstrated mixed squamous cell carcinoma and adenocarcinoma, and the same finding was observed in the lymph nodes (Fig. 3a, b). There were regions of intermediate morphology at the interface of the part of the squamous cell carcinoma and the part of adenocarcinoma. Immunohistochemistry (IHC) staining provided confirmatory evidence mixed phenotypes in these regions, and was positive for CK5/6 and p63 in the part of the squamous cell carcinoma (Fig. 3c, d). The MIB-1 index was various values depending on the intra-tumor location, and it was approximately 80% at hot spot. The final pathological diagnosis was adenosquamous carcinoma, stage IVB (T4bN2aM1b) according to the 7th edition of the UICC TNM classification system.
Fig. 2.

Gross finding: the resected specimen revealed an ulcerative mass with a distinct border, measuring 8.0 cm × 6.5 cm
Fig. 3.

Histologically, components of both adenocarcinoma and squamous cell carcinoma were found (a HE, b HE at high magnification). On IHC staining, CK5/6 and p63 were positive in the part of the squamous cell carcinoma (c CK5/6 and d p63)
Biomarker analysis showed a microsatellite stable, wild-type KRAS gene and BRAF V600E mutation (Fig. 4a). On IHC staining, BRAF V600E mutation expression was found in both segments of adenocarcinoma and squamous cell carcinoma (Fig. 4b).
Fig. 4.

On sequencing analysis, the BRAF V600E mutation (c.1799T > A) was found (a). On IHC staining, the tumor showed the expression of BRAF V600E in both the adenocarcinoma and squamous cell carcinoma components (b)
Despite undergoing postoperative chemotherapy with FOLFOX and bevacizumab, the patient died 5 months postoperatively.
Discussion
To the best of our knowledge, this is the first report on ascending colon adenosquamous carcinoma with a BRAF V600E mutation. Positive immunostaining for both CK5/6 and p63 has been reported to be highly predictive of a primary tumor of squamous epithelial origin [11]. In our case, both CK5/6 and p63 were positive in the part of the squamous cell carcinoma. Adenosquamous carcinoma can develop in various organs, including the colon, pancreas, and lung. The frequencies of adenosquamous carcinoma are 2.0–4.0% in lung cancer [12], 0.38–10% in pancreatic cancer [13], and 0.1% in colorectal cancer.
The histogenesis of adenosquamous carcinoma remains unclear; however, there are several hypotheses, including (1) direct transformation of ectopic squamous cells in the colonic mucosa into squamous cell carcinoma, (2) transformation of uncommitted basal cells into squamous cells, (3) squamous metaplasia of glandular cells, and (4) squamous metaplasia of adenocarcinoma cells. In general, the fourth hypothesis has been supported [14–17].
In a review of Japanese patients with adenosquamous colon cancer, Yokoi et al. reported that 48% were female, 56% had right-sided colon cancer, 94% were T3 or more, 62% had lymph node metastasis, and 33% were stage IV [18]. Adenosquamous carcinoma has been reported to be aggressive and has been found at advanced stages in previous studies. In a review of 145 patients with adenosquamous carcinoma, Cagir et al. described the overall rates of regional metastases and distant metastases as 46.0 and 42.4%, respectively [1]. Masoomi et al. reported that the rate of distant metastasis of adenosquamous carcinoma was 35.3% compared with 13.9% for adenocarcinoma [2]. The prognosis of adenosquamous colon cancer is relatively poor. Previous reports have demonstrated that the 5-year survival rate of adenosquamous carcinoma was worse than that of adenocarcinoma. The 5-year survival rates of adenosquamous carcinoma and adenocarcinoma are approximately 30 and 50%, respectively [1, 2, 19]. Frizelle et al. reported that the prognosis of adenosquamous carcinoma was worse than that of adenocarcinoma in stage III or IV colorectal cancer but similar to that of adenocarcinoma in stage I or II colorectal cancer [5].
In general, the primary treatment for colorectal adenosquamous carcinoma is surgical resection; however, so far, the standard chemotherapy for adenosquamous colon cancer has not been established because of its rarity. Chemotherapy with FOLFOX and bevacizumab was not at all effective in our case.
The BRAF V600E mutation is found in 5–10% of colorectal cancer and is associated with right-sided tumor, elderly patients, female patients, and microsatellite instability (MSI). Patients with colorectal cancer with BRAF V600E have a poor clinical response to standard chemotherapy, resulting in a poor prognosis. Recent reports have demonstrated the response of colorectal cancer with BRAF V600E to concurrent treatment with a BRAF inhibitor and anti-EGFR antibody. Yaeger et al. reported that the BRAF inhibitor vemurafenib combined with the anti-EGFR antibody panitumumab might be effective in patients with BRAF-mutant metastatic colorectal cancer [20]; however, the response of adenosquamous colon cancer remains unknown.
Here, the tumor demonstrated microsatellite stability (MSS), whereas most colorectal cancers with BRAF V600E show MSI. In sporadic colorectal cancers, the BRAF mutation is observed in approximately 60% of high MSI tumors and only 5–10% of MSS tumors [7, 8, 21, 22]. BRAF-mutated colorectal cancer with MSS has a worse prognosis than MSI [10]. Consequently, the poor prognosis might be due to not only BRAF V600E but also due to MSS.
In our case, because BRAF V600E was detected not only in the adenocarcinoma component, but also in the squamous cell carcinoma component, there may be a link between the morphological and genetic features in adenosquamous carcinoma. As previously stated, among the several existing hypotheses regarding the histogenesis of colorectal adenosquamous carcinoma, the hypothesis of squamous metaplasia of adenocarcinoma cells has been supported.
We identified the BRAF V600E mutation in adenosquamous colon cancer. This report may help in determining the nature of adenosquamous carcinoma of the colon and rectum and may lead to the establishment of an effective treatment for this cancer. Therefore, further analyses are required to define the carcinogenesis of adenosquamous carcinoma of the colon and rectum.
Author contributions
All authors contributed to this work. Hiroyuki Ishida prepared the description of the clinical course and wrote the manuscript; Kazuro Chiba performed biopsy; Takeru Iijima performed genetic analysis; Shin-ichiro Horiguchi performed histological diagnosis; and Tatsuro Yamaguchi performed surgery, designed the study and wrote the manuscript.
Conflict of interest
No author has any conflict of interest.
Research involving human participants
This case report was conducted in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects.
Informed consent
Written informed consent obtained from the patient.
References
- 1.Cagir B, Nagy MW, Topham A, Rakinic J, Fry RD. Adenosquamous carcinoma of the colon, rectum, and anus: epidemiology, distribution, and survival characteristics. Dis Colon Rectum. 1999;42:258–263. doi: 10.1007/BF02237138. [DOI] [PubMed] [Google Scholar]
- 2.Masoomi H, Ziogas A, Lin BS, et al. Population-based evaluation of adenosquamous carcinoma of the colon and rectum. Dis Colon Rectum. 2012;55:509–514. doi: 10.1097/DCR.0b013e3182420953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Petrelli NJ, Valle AA, Weber TK, Rodriguez-Bigas M. Adenosquamous carcinoma of the colon and rectum. Dis Colon Rectum. 1996;39:1265–1268. doi: 10.1007/BF02055120. [DOI] [PubMed] [Google Scholar]
- 4.Herxheimer G. Ober heterologue cancroide. Beitr Pathol Anat. 1907;41:348–412. [Google Scholar]
- 5.Frizelle FA, Hobday KS, Batts KP, Nelson H. Adenosquamous and squamous carcinoma of the colon and upper rectum: a clinical and histopathologic study. Dis Colon Rectum. 2001;44:341–346. doi: 10.1007/BF02234730. [DOI] [PubMed] [Google Scholar]
- 6.Kolch W. Meaningful relationships: the regulation of the Ras/Raf/MEK/ERK pathway by protein interactions. Biochem J. 2000;351(2):289–305. doi: 10.1042/bj3510289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417:949–954. doi: 10.1038/nature00766. [DOI] [PubMed] [Google Scholar]
- 8.Rajagopalan H, Bardelli A, Lengauer C, et al. Tumorigenesis: RAF/RAS oncogenes and mismatch-repair status. Nature. 2002;418:934. doi: 10.1038/418934a. [DOI] [PubMed] [Google Scholar]
- 9.Beeram M, Patnaik A, Rowinsky EK. Raf: a strategic target for therapeutic development against cancer. J Clin Oncol. 2005;23:6771–6790. doi: 10.1200/JCO.2005.08.036. [DOI] [PubMed] [Google Scholar]
- 10.Lochhead P, Kuchiba A, Imamura Y, et al. Microsatellite instability and BRAF mutation testing in colorectal cancer prognostication. J Natl Cancer Inst. 2013;105:1151–1156. doi: 10.1093/jnci/djt173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kaufmann O, Fietze E, Mengs J, Dietel M. Value of p63 and cytokeratin 5/6 as immunohistochemical markers for the differential diagnosis of poorly differentiated and undifferentiated carcinomas. Am J Clin Pathol. 2001;116(6):823–830. doi: 10.1309/21TW-2NDG-JRK4-PFJX. [DOI] [PubMed] [Google Scholar]
- 12.Ruffini E, Rena O, Oliaro A, et al. Lung tumors with mixed histologic pattern. Clinico-pathologic characteristics and prognostic significance. Eur J Cardiothorac Surg. 2002;22:701–707. doi: 10.1016/S1010-7940(02)00481-5. [DOI] [PubMed] [Google Scholar]
- 13.Borazanci E, Millis SZ, RErkut Korn, et al. Adenosquamous carcinoma of the pancreas: Molecular characterization of 23 patients along with a literature review. World J Gastrointest Oncol. 2015;7:132–140. doi: 10.4251/wjgo.v7.i9.132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hickey WF, Corson JM. Squamous cell carcinoma arising in a duplication of the colon: case report and literature review of squamous cell carcinoma of the colon and of malignancy complicating colonic duplication. Cancer. 1981;47:602–609. doi: 10.1002/1097-0142(19810201)47:3<602::AID-CNCR2820470330>3.0.CO;2-8. [DOI] [PubMed] [Google Scholar]
- 15.Khan AQ, Griffin JW, Tedesco FJ. Squamous cell carcinoma of the ascending colon. Am J Gastroenterol. 1979;72:565–567. [PubMed] [Google Scholar]
- 16.Crissman JD. Adenosquamous and squamous cell carcinoma of the colon. Am J Surg Pathol. 1978;2:47–54. doi: 10.1097/00000478-197803000-00006. [DOI] [PubMed] [Google Scholar]
- 17.Schneider TA, Birkett DH, Vernava AM. Primary adenosquamous and squamous cell carcinoma of the colon and rectum. Int J Colorectal Dis. 1992;7:144–147. doi: 10.1007/BF00360355. [DOI] [PubMed] [Google Scholar]
- 18.Yokoi K, Tanaka N, Furukawa K, et al. A case of adenosquamous carcinoma of the ascending colon. J Nippon Med Sch. 2008;75:242–246. doi: 10.1272/jnms.75.242. [DOI] [PubMed] [Google Scholar]
- 19.Comer TP, Beahrs OH, Dockerty MB. Primary squamous cell carcinoma and adenoacanthoma of the colon. Cancer. 1971;28:1111–1117. doi: 10.1002/1097-0142(1971)28:5<1111::AID-CNCR2820280504>3.0.CO;2-V. [DOI] [PubMed] [Google Scholar]
- 20.Yaeger R, Cercek A, O’Reilly EM, et al. Pilot trial of combined BRAF and EGFR inhibition in BRAF-mutation metastatic colorectal cancer patients. J Clin Oncol. 2015;21:1313–1320. doi: 10.1158/1078-0432.CCR-14-2779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fransén K, Klintenäs M, Osterström A, et al. Mutation analysis of the BRAF, ARAF and RAF-1 genes in human colorectal adenocarcinomas. Carcinogenesis. 2004;25:527–533. doi: 10.1093/carcin/bgh049. [DOI] [PubMed] [Google Scholar]
- 22.Tie J, Gibbs P, Lipton L, et al. Optimizing targeted therapeutic development: analysis of a colorectal cancer patient population with the BRAF (V600E) mutation. Int J Cancer. 2011;128:2075–2084. doi: 10.1002/ijc.25555. [DOI] [PubMed] [Google Scholar]