

Abstract
Background: The annular ligament has a crucial role in the radial head stability and it is critical to the proper functioning of the proximal radio-capitellar joint. Its chronic injury may lead to radial head instability, elbow pain with decrease in motion and valgus deformity. Method: We present the case of a 53-year-old heavy laborer who reported a complex trauma of the right upper limb with a Floating Elbow Injury, associated to an open Monteggia fracture-dislocation. One month later, despite the definitive fixation with plates of both the forearm and the supracondylar fractures, X-rays showed the persistence of the radial head dislocation. A triceps autograft reconstruction for treating the chronic radial head dislocation, as described in literature, was not indicated in our patient, due to the recent surgery at the distal humerus site. Thus, it was decided to proceed to allograft reconstruction using a peroneal tendon from a cadaveric donor, fixed by modified Bell-Tawse Technique. Results: Two years after the surgery, x-rays showed the complete fractures’ healing; however a radial head notching was found. Conclusions: Allograft reconstruction of the annular ligament deserves to be considered as an adequate technique, whenever the surrounding soft tissues are critically compromised. In literature, the radial head notching complication is reported to be up to 36 %, and it may be related to the surgical technique, regardless of the graft used. (www.actabiomedica.it)
Keywords: annular ligament repair, allograft reconstruction, radial head dislocation
Introduction
The annular ligament plays a critical role in maintaining the position of the radial head, and the stability of the proximal radio-ulnar joint (PRUJ). PRUJ disruption distinguishes the Monteggia fractures from the other injuries associated with the radio-capitellar dislocation.
In cases of complex Monteggia fracture-dislocation, the anatomical restoration of the ulnar length and alignment is mandatory in order to obtain a congruent PRUJ (1, 2). Nevertheless, even if an appropriate surgical treatment is performed, Monteggia injuries may have a high rate of complications (3, 4), such as the chronic dislocation of the radial head. This is defined as a dislocation which is still present 4 weeks after the trauma. The causes may be located in residual ulnar deformity after internal fixation, in failure of the annular ligament healing, or in both. The resulting radial head instability may lead to elbow pain, decrease in motion, and valgus deformity (5, 6).
Case presentation
A right-hand-dominant 53-year-old heavy laborer reported a high-energy fall on his outstretched right arm. He was admitted to our Department having sustained an open fracture of his right forearm and an apparent elbow dislocation. No radial and ulnar pulses could be tracted at the wrist. X-rays revealed a supracondylar humeral fracture associated to an open Monteggia fracture-dislocation, classified as type IV according to Bado’s classification. According to Gustilo-Anderson classification of the open fractures, the soft tissue injury was classified as III C due to the involvement of the brachial artery.
An arterial thrombectomy using a Fogarty catheter was first performed, with the complete restoring of the distal pulses. However, an actual brachial artery damage was not found; a possible explanation could be an intensive artery spasm caused by the high energy of the trauma. It was decided then to proceed to the open reduction and plate fixation of the supracondylar humeral fracture, and to reduction and fixation of the forearm fractures using TEN nails. It was also performed a K-wire temporary stabilization of the humero-radial joint to avoid the radial head subluxation. Appropriate antibiotic coverage with Cefazoline and Gentamicin was immediately started.
Four weeks later, at the K-wire removal, X-rays revealed the radial head dislocation relapse (Fig. 1). The skin wound at the open fracture site was completely healed, and laboratory tests showed no signs of infection. Therefore, the patient underwent second surgery in order to obtain the anatomical reduction of the forearm fracture. TEN nails were removed and definitive fixation was performed using plates. No signs of PRUJ instability was apparently found during the intra-operative dynamic tests. Unexpectedly, the post-operative x-rays showed the persistence of the radial head dislocation.
Figure 1.

The persistence of the radial head dislocation relapse at the 4-week x-rays follow-up
A triceps autograft reconstruction for treating the chronic head dislocation, as described in literature, was not indicated in our patient, due to the recent surgery at the distal humerus site. Thus, it was decided to proceed to allograft reconstruction using a peroneal tendon from a cadaveric donor, fixed by modified Bell-Tawse technique (Fig. 2).
Figure 2.
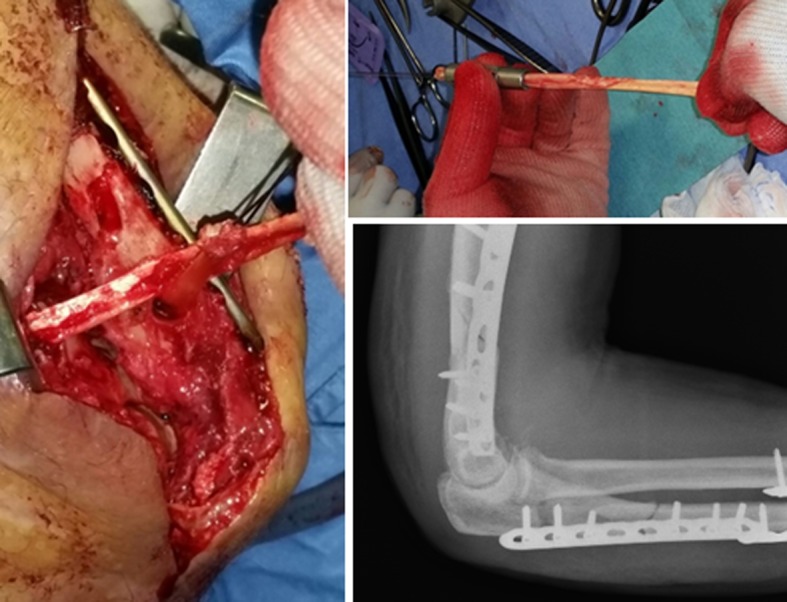
The allograft reconstruction with peroneal tendon from a cadaveric donor – intra-operative and post-operative
A Speed and Boyd’s approach was used to access the elbow. The exuberant tissue which had grown in the radial notch of the ulna was removed. The proximal ulna was decorticated at the level of the native annular ligament. A 12 cm x 4 mm strip of peroneal tendon from a cadaveric donor was prepared. A 4.5 mm bone tunnel was drilled through the ulna. The tendon was passed through the ulnar tunnel, then around the radial neck prior to its reduction. The graft was tensioned keeping the forearm in neutral position, and it was anchored on the medial side using a non absorbable suture. After surgery the elbow joint was immobilized in a fixed 90° elbow splint for three weeks.
At the splint removal, the patient was discharged to the Rehabilitation Unit to start a targeted rehabilitation program.
At the two-year follow-up the right elbow A-ROM was 5 degrees extension, 130 degrees flexion, 80 degrees supination, 5 degrees pronation. X-rays showed the complete fractures healing; however a radial head notching was found (Fig. 3).
Figure 3.

The clinical outcome and the radial head notching at the two-year follow-up
Discussion
The patient in herein study, who presented a rare combination of a Floating Elbow Injury associated to a type IV Monteggia fracture-dislocation, developed a chronic dislocation of the radial head.
The reasons which could have led to this complication were analyzed.
The aim of the second surgery was to obtain an anatomical reduction of the forearm fracture, which is mandatory to restore the congruity of the PRUJ. Nevertheless, it was not achieved. A possible reason is that it might had been underestimated the role played by the annular ligament integrity.
Many techniques of autograft reconstruction, for the treatment of the chronic dislocation of the radial head, have been described in literature.
In 1965, Bell Tawse et al. described a technique for the annular ligament reconstruction (ALR) using a strip from the central portion of the triceps brachii tendon. The tendon strip was left attached to the ulna, passed from posterior to anterior around the radial neck and fixed to the proximal ulna through a drill hole (7).
In 1969, Boyd et al. also described a technique using a strip from the triceps tendon which was passed around the radial neck from posterior to anterior without drilling any bone tunnel through the ulna (8).
In 1977, Lloyd et al. introduced a modified Bell-Tawse technique using the lateral bundle of the triceps tendon (9).
In 1999, Seel and Peterson described a two-hole technique using a tendon bundle from the triceps brachii (10).
Recently, other techniques using the brachioradialis tendon, the palmaris longus tendon, the extensor carpi radialis tendon and the superficial head of the brachialis muscle have been proposed (2, 6, 11-13).
Each technique previously listed, considers the use of autografts harvested from the structures surrounding the elbow. This was not indicated in our patient due to the recent surgery at the distal humerus site, and the soft tissue damage related to the open fracture of the forearm.
Therefore it was decided to proceed to allograft reconstruction using a peroneal tendon from a cadaveric donor, and a satisfying capacity of the elbow was restored.
The radial head notching which was found at the 2-year follow-up x-rays was a predictable complication, not so rare in literature, regardless of the graft used (14, 15). It may be related to the surgical technique, due to a residual ulnar bony deformity that stretches the neo-ligament, or due to a high tension made by the ligament suture, which constricts the radial neck during the forearm prono-supination (16, 17).
Some authors recommend to measure the maximum ulnar bow and add an osteotomy in cases of apparent ulnar bowing, to avoid the neo-ligament failure (18, 19).
Some authors also recommend the use of absorbable sutures. The suture would retain 100% strength for about two weeks, after which it would begin to dissolve avoiding an excessively high pressure exerted by the neo-ligament (17, 20).
In conclusion, we assume that allograft reconstruction deserves to be considered as an adequate technique for the treatment of the chronic annular ligament disruption, whenever the surrounding soft tissues are critically compromised.
References
- 1.Canton G, Hoxhaj B, Fattori R, Murena L. Annular ligament reconstruction in chronic Monteggia fracture-dislocation in tha adult population: indications and surgical technique. Musculoskelet Surg. 2018 Oct;102(1):93–102. doi: 10.1007/s12306-018-0564-6. [DOI] [PubMed] [Google Scholar]
- 2.Bae DS. Successful strategies for managing Monteggia injuries. J Pediatr Orthop. 2016 Jun;36(1):S67–S70. doi: 10.1097/BPO.0000000000000765. [DOI] [PubMed] [Google Scholar]
- 3.Korner J, Hoffmann A, Rudig L, Müller LP, Hessmann M, Lill H, Josten C, Rommens PM. Monteggia injuries in adults: Critical analysis of injury pattern, management, and results. Unfallchirurg. 2004;107(11):1026–1040. doi: 10.1007/s00113-004-0825-8. [DOI] [PubMed] [Google Scholar]
- 4.Egol KA, Tejwani NC, Bazzi J, Susarla A, Koval KJ. Does a Monteggia variant lesion result in a poor functional out come? A retrospective study. Clin Orthop Relat Res. 2005;438:233–238. doi: 10.1097/01.blo.0000168806.79845.8b. [DOI] [PubMed] [Google Scholar]
- 5.Bhaskar A. Missed Monteggia fracture in children: is annular ligament reconstruction always required? Indian J Orthop. 2009 Oct;43(4):389–395. doi: 10.4103/0019-5413.55978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Horii E, Nakamura R, Koh S, Inagaki H, Yajima H, Nakao E. Surgical treatment for chronic radial head dislocation. J Bone Joint Surg Am. 2002 Jul;84-A(7):1183–1188. doi: 10.2106/00004623-200207000-00014. [DOI] [PubMed] [Google Scholar]
- 7.Bell Tawse AJ. The treatment of malunited anterior Monteggia fractures in children. J Bone Joint Surg Br. 1965 Nov;47(4):718–723. [PubMed] [Google Scholar]
- 8.Boyd HB, Boals JC. The Monteggia lesion: a review of 159 cases. Clin Orthop Relat Res. 1969 Sep-Oct;66:94–100. [PubMed] [Google Scholar]
- 9.Lloyd-Roberts GC, Bucknill TM. Anterior dislocation of the radial head in children: aetiology, natural history and management. J Bone Joint Surg Br. 1977 Nov;59-B(4):402–407. doi: 10.1302/0301-620X.59B4.925049. [DOI] [PubMed] [Google Scholar]
- 10.Seel MJ, Peterson HA. Management of chronic post-traumatic radial head dislocation in children. J Pediatr Orthop. 1999 May-Jun;19(3):306–312. [PubMed] [Google Scholar]
- 11.Itadera E, Ueno K. Recurrent anterior instability of the radial head: case report. J Hand Surg Am. 2014 Feb;39(2):206–208. doi: 10.1016/j.jhsa.2013.11.006. [DOI] [PubMed] [Google Scholar]
- 12.Burnei G, Zaharia C. The treatment of congenital traumatic dislocation of the radial head; original technique. ARA Ann Congr Proc. 2014;37:388–394. [Google Scholar]
- 13.Nwoko OE, Patel PP, Richard MJ, Leversedge FJ. Annular ligament reconstruction using the distal tendon of the superficial head of the brachialis muscle: an anatomical feasibility study. J Hand Surg Am. 2013 Jul;38(7):1315–1319. doi: 10.1016/j.jhsa.2013.04.008. [DOI] [PubMed] [Google Scholar]
- 14.Nakamura K, Hirachi K, Uchiyama S, Takahara M, Minami A, Imaeda T, Kato H. Long-term clinical and radiographic outcomes after open reduction for missed Monteggia fracture-dislocations in children. J Bone Joint Surg Am. 2009 Jun;91(6):1394–1404. doi: 10.2106/JBJS.H.00644. [DOI] [PubMed] [Google Scholar]
- 15.Hugo DB. Radial neck osteolysis after annular ligament reconstruction: a case report. Clin Orthop Rel Res. 1997;342:94–98. [PubMed] [Google Scholar]
- 16.Galik K, Baratz ME, Butler AL, Dougherty J, Cohen MS, Miller MC. The effect of the annular ligament on kinematics of the radial head. J Hand Surg Am. 2007 Oct;32(8):1218–1224. doi: 10.1016/j.jhsa.2007.06.008. [DOI] [PubMed] [Google Scholar]
- 17.Tan L, Li YH, Sun DH, Zhu D, Ning SY. Modified technique for correction of isolated radial head dislocation without apparent ulnar bowing: a retrospective case study. Int J Clin Exp Med. 2015 Oct 15;8(10):18197–18202. [PMC free article] [PubMed] [Google Scholar]
- 18.Lincoln TL, Mubarak SJ. “Isolated” trau-matic radial-head dislocation. J Pediatr Orthop. 1994 Jul-Aug;14(4):454–457. doi: 10.1097/01241398-199407000-00006. [DOI] [PubMed] [Google Scholar]
- 19.Inoue G, Shionoya K. Corrective ulnar oste-otomy for malunited anterior Monteggia le-sions in children. 12 patients followed for 1-12 years. Acta Orthop Scand. 1998 Feb;69(1):73–76. doi: 10.3109/17453679809002361. [DOI] [PubMed] [Google Scholar]
- 20.Gomez-Alonso A, Garcia-Criado F, Parreno-Manchado F, Garcia-Sanchez J, Garcia-Sanchez E, Parreno-Manchado , Zambrano-Cuadrado Y. Study of the efficacy of Coated VICRYL Plus® Antibacterial suture (coated Polyglactin 910 suture with Triclosan) in two animal models of general surgery. J Infect. 2007;54:82–88. doi: 10.1016/j.jinf.2006.01.008. [DOI] [PubMed] [Google Scholar]