

Abstract
Background
Patient centred communication (PCC) has been described as a method for doctor-patient communication. The principles of shared decision making (SDM) have been proposed more recently.
Aims
This study aimed to examine PCC and SDM empirically with respect to their mutual association, the variation in practitioners' working styles, and the associations with patient characteristics.
Methods
Sixty general practitioners recruited 596 adult patients who gave written consent to have their consultations videotaped. The tapes were assessed by two researchers, using a standardised instrument for global communication. For the purpose of this exploratory study, scales for PCC and SDM were based on subsamples of items in the MAAS.
Results
The scales for PCC and SDM were weakly associated (Pearson correlation: 0.25). Physicians varied more on SDM than on PCC. The intracluster correlation of the PCC and SDM scales were, respectively, 0.34 and 0.19. However, hypotheses regarding associations with patient characteristics were not confirmed. Neither PCC nor SDM scores were related to patient gender, education, age, functional health status or existence of chronic conditions.
Conclusion
The study provides evidence that PCC and SDM can be differentiated and comprise approaches to communication between clinicians and patients which may be more clearly distinguished by further focused research and training developments.
Background
The patient-centred communication method suggests that a care provider should 'understand the meaning of illness for the patient as well as interpret it in terms of the medical frame of reference' [1]. Although an extensive body of literature on the method has emerged, recent evaluations have led to concerns about possible multi-dimensionality and consensus as to its meaning has been difficult to achieve [2]. An alternative focus for an analysis of the doctor-patient interaction concerns the locus of decisional responsibility. Shared decision making has been introduced as a proposed middle ground between paternalistic decision-making and what has been termed 'informed' or 'consumer' choice where decisional responsibility is placed with patients [3]. This study examines the concepts of shared decision making (SDM) and the patient centred communication method (PCC).
Stewart et al. described PCC as a clinical method with six key components: exploring both the disease and the illness experience, understanding the whole person, finding common ground, incorporating prevention and health promotion, enhancing the doctor-patient relationship, and being realistic [1]. The principles of shared decision making can be located within the 'identification of common ground regarding management' component of PCC. It implies participation of both the patient and the clinician in the decision-making process, and it includes different aspects such as listing and provision of information on treatment options, checking of patients' understanding and preferences for involvement in decision making [4]. To date it has at times seemed that PCC and SDM may be viewed synonymously, perhaps under the umbrella term of 'partnership' between doctors and patients [5]. However, we explored whether PCC and SDM are different concepts.
We formulated four hypotheses for this study. Firstly, we hypothesised that a high level of PCC does not always imply a high level of SDM, and vice versa, meaning that the correlation between the two concepts is moderate at best (hypothesis 1). Secondly, we expected that doctors are more consistent in their use of the PCC method than in their use of the SDM method (hypothesis 2). The background of this hypothesis is that PCC reflects the competencies that professionals acquire during their training, which are more constant than the competencies of SDM. The PCC competencies apply to all consultations, while the SDM competences are more finite, flexible and may not be used by the profesional according to context, perceived suitability and appropriateness [4].
Furthermore, we hypothesised that PCC and SDM have different associations with patient gender and education. Empirical confirmation of such differences would lend further support to our hypothesis that the two methods are conceptually different. We expected that the likelihood of PCC is higher in female patients, but unrelated to educational level (hypothesis 3). It has been suggested that women tend to be more expressive, use more cooperative language and have stronger interpersonal associations, while men tend to be more reserved and less empathic than women [6]. Finally, the likelihood of observing SDM was expected to be higher in more highly educated patients, but unrelated to gender of the patient (hypothesis 4). SDM requires cognitive skills which may be more prevalent in people with higher educational attainments, or more likely to be expressed [7-9].
This exploratory study aimed to examine to what extent the concepts of shared decision making (SDM) and patient-centred communication method (PCC) are different or overlap. We used data already available from an observational study in general practice to test the four hypotheses.
Methods
Sample
Sixty GPs from 43 practices were recruited out of a systematic sample of 700 GPs in the Netherlands, which was stratified for urbanisation level to reflect the national situation. GPs were recruited for a larger research project, which focused on patients' views of the quality of care. We did not record reasons for refusals, but the participation grade of about 10% of the invited GPs is typical for this type of study. GPs were instructed to include 10 consecutive adult patients who visited the practice, and who gave written informed consent for this study. We did not record the number of refusals, but anecdotal information suggestions this was 10–20% of the patients who were invited. The Ethical Committee of the University Medical Centre St Radboud gave approval for this study.
Measurements
A video-recording system, consisting of two cameras with built-in microphone, a monitor and a recorder, was installed by a researcher (EV) or an assistant. All consultations were recorded both in the consulting room and the examination room. The GP was responsible for switching from one camera to the other when necessary, and for recording patient and consultation data, such as the patients' age and gender, into a logbook directly after the consultation. The receptionist informed patients about the video recording and asked permission. Consent was registered by giving the patient a coloured card ((green=consent, red=no consent) to be handed to the GP at the start of the consultation. Video recordings were erased if patients revoked their permission.
The communication in each of the consultations was rated by one of two trained raters (MW and EV), using the MAAS (1995 version), a previously validated observation instrument comprising 12 items with a 7-point scale [10]. A previous validation study proved the reliability of this procedure [11]. These raters were unaware of this secondary analysis focusing on SDM and PCC at the time of the rating. The MAAS instrument provides a global assessment of communication, including aspects such as exploration of patients' needs, provision of information, and empathy. It is the instrument which is most able to assess the constructs of SDM and PCC without actually using the instruments developed specifically by key authors in those domains [12,13]. The first consultation within a series was not used in order to reduce the influence of a test effect; all subsequent consultations which met the inclusion criteria were used.
For the purpose of the secondary analysis in this study we constructed two subscales from the 1995 MAAS instrument. A PCC scale was the mean score of four items and a SDM scale was the mean score of three items from the MAAS instrument (box 1). Each of these items had three or four specific indicators that guided the scoring (see box 1). We accepted that these subscales represent an approximation of the issues that would be considered by a specifically designed tool. The advantage of using the existing MAAS data is that we avoided potential bias caused by intentions of the observers. Furthermore, by using subscales derived from one source instrument, the comparison is not influenced by methodological differences between the instruments, e.g. related to style of phrasing or the number and type of answering categories. Finally, we did not have the resources for scoring consultations with different instruments.
Patients' age and gender were recorded by the general practitioner on a written form. Patients' education (8 categories), perceived overall health status (5 categories), and number of chronic diseases (list of 25 conditions) was recorded by patients in a written questionnaire, which was handed out to all patients who had their consultation video-taped.
Analysis
First, descriptive tables were made to detail the patient sample. Then analyses of the PCC and SDM scales were made. Reliability analysis was performed to calculate Cronbach's alpha, which indicates the internal consistency of these scales. Pearson correlations were performed to examine the associations between PCC and PDM. Intracluster correlation coefficients were calculated for each scale to examine the clustering of scores within GPs and to examine the consistency of GPs' use of PCC and SDM. Finally, differences between subgroups were tested by means of analysis of variance. The statistical tests corrected for the sample size inflation due to the clustering of data with GPs [14]. Given the 60 GPs and 10 patients per GP (these numbers were based on a power calculation for the larger study), the actual standard deviations and intraclustercorrelations found, and alpha = 0.05 and power = 0.80, this study had the power the detect differences between equally-sized groups of 0.3 points on the SDM scale and 0.4 points on the PCC scale.
Results
Video-taped consultations of 596 patients from sixty GPs were available; due to technical problems recordings failed in 4 patients from one GP. From these patients, 427 responded to the written survey, that measured education, health status and chronic diseases (72% response rate). Table 1 describes the patient population. About two thirds (59%) of the patients were women and about a quarter (22%) was 65 years or older. About half the patients (47%) had low education attainments. About half (53%) reported a poor or moderate health status and about a half (48%) of the patients had one or more chronic diseases.
Table 1.
Patient sample (n = 596)
| Absolute number (percentage) | |
| Female patients | 354 (59%) |
| Patients aged 65 years or older | 121 (22%) |
| Educational level (n = 366) | |
| -Low | 172 (47%) |
| -Medium | 132 (36%) |
| -High | 62 (17%) |
| Perceived overall health status (n = 412) | |
| - Poor/fair | 300 (53%) |
| - Good/very good/excellent | 112(47%) |
| Patients with chronic diseases (n = 427) | 204 (48%) |
| Mean (standard deviation) | |
| Age in years (n = 517) | 49.2(17.1) |
| Mean Communication score (MAAS) | 2.3 (0.55) |
| Mean Patient-centred communication score (PCC) | 2.0 (0.68) |
| Mean Shared decision making score (SDM) | 2.3 (0.84) |
* Number of patients with valid data was 596, unless lower sample indicated.
The MAAS scale (12 items) had a Cronbach's alpha of 0.64 in this sample. The constructed PCC subscale had a Cronbach's alpha of 0.50 and the SDM scale had a Cronbach's alpha of 0.43. The mean scores for overall communication, patient centred communication (PCC) and shared decision making (SDM) were all around 2 on the scale that ranged from 0 to 6 (table 1).
Hypothesis 1
The Pearson correlation between PCC and SDM was 0.25 (p < 0.001, n = 596). This weak correlation lends support to hypothesis 1. The correlations between PCC and MAAS (total), and SDM and MAAS (total) were both 0.70 (both p < 0.001, n = 596). So it can be noted that PCC and SDM contribute equally to a summary assessment of communication in consultations, but they were only weakly associated with each other.
Hypothesis 2
The clustering of patient data within GPs was higher for PCC compared to SDM: the intracluster correlation was 0.34 for PCC and 0.19 for SDM. This implies that GPs were more consistent with respect to PCC, while they varied more across different patients with respect to SDM, supporting hypothesis 2. Figures 1 and 2 illustrate this graphically: the reliability intervals for aggregated mean scores per GP was larger for SDM than for PCC.
Figure 1.
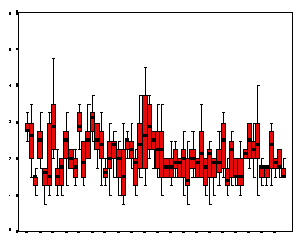
Boxplot of aggregated PCC scores per GP, with 95% confidence intervals.
Figure 2.
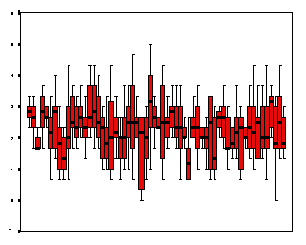
Boxplot of aggregated SDM scores per GP, with 95% confidence intervals.
Hypotheses 3 and 4
Table 2 shows the mean scores across subgroups of patients. No differences were significant: hypotheses 3 and 4 concerning associations with gender and education, respectively, were not confirmed. No significant differences were observed either across subgroups defined by age, functional health status or existence of chronic conditions.
Table 2.
Comparison of PCC and SDM between patient groups
| PCC | SDM | |
| Gender | ||
| - Man | 2.1 (0.63) | 2.4 (0.87) |
| - Women | 2.1 (0.71) | 2.3 (0.83) |
| (p > 0.60) | (p > 0.10) | |
| t = 0.447; n = 574 | t = 1.425; n = 573 | |
| Education | ||
| - Low | 2.2 (0.65) | 2.3 (0.78) |
| - Medium | 2.1 (0.66) | 2.4 (0.77) |
| - High | 2.0 (0.56) | 2.5(0.81) |
| (p > 0.40) | (p > 0.20) | |
| t = 0.741; n = 366 | t = 1.250; n = 366 | |
| Age | ||
| - 18–65 years | 2.1 (0.69) | 2.3 (0.83) |
| - 65+70 years | 2.0 (0.65) | 2.2 (0.93) |
| (p > 0.70) | (p > 0.40) | |
| t = 0.243; n = 516 | t = 0.706; n = 516 | |
| Functional health status | ||
| - Poor/average | 2.2 (0.62) | 2.3 (0.75) |
| - Good/very good/excellent | 2.2 (0.65) | 2.4 (0.84) |
| (p > 0.60) | (p > 0.30) | |
| t = 0.443; n = 412 | t = 0.889; n = 411 | |
| Chronic conditions | ||
| - No | 2.1 (0.65) | 2.3 (0.83) |
| - Yes | 2.1 (0.64) | 2.4 (0.80) |
| (p > 0.60) | (p > 0.05) | |
| F = 0.397; n = 426 | t = 1.653; n = 427 |
Legend: Mean scores and standard deviations between brackets. To correct for clustering of patients within GPs the original t-values have been divided by the square root of the 'design effect', which was 2.01 for PCC (ICC = 0.34) and 1.31 for SDM (ICC = 0.19). The design effect is 1+(n-1)*ICC, where n is the average cluster size (n = 10 in our study) and ICC the intracluster correlation.
Discussion
This explorative study provides some empirical evidence that patient centred communication and shared decision making are conceptually different. Hypotheses 1 and 2 were confirmed, indicating that the correlation between the two methods is weak (although existent) and physicians are more consistent in their use of PCC than in their use of SDM. Hypotheses 3 and 4, however, were not confirmed: no associations with patients' gender or education were found. These findings should be interpreted in the context of the limitations of this study.
The most important limitation of the study is the rudimentary measurement of PCC and SDM. The indicators for these measurements were derived from the MAAS, an instrument that assesses the physicians' communication in consultations at a global level. The PCC and SDM scales were developed by us for this evaluation and not by the authors of MAAS. On the other hand, the MAAS is independent of the two research groups principally associated with the PCC and SDM constructs. The internal consistency of the two scales was considered acceptable for an exploratory study of this nature, given the number of items per scale and the Cronbach alpha of the total scale. However, the low reliability suggests that the dimensions can be further differentiated. More reliable scales would provide greater potential to identify significant associations with other factors. Better measures for both SDM were not available at the time this study was performed, but we encourage studies that use better measures which have become available recently [15,16].
Some elements may be common to both SDM and PCC. SDM implies the assessment of patients' understanding and concordance between doctor and patients concerning the decisions made, which reflects an approach that is consistent with the PCC method. However, it is possible to be even clearer about the exact nature of the intended interaction and to identify conceptual differences. SDM includes the provision of quantitative information and exploration of patients' preferences. This therefore suggests that it is located in a cognitive, rational paradigm. As such the SDM approach appears closer to evidence-based health care approach than may be the case with the patient-centred clinical method which placed patient views and agenda's at the core of the consultation. The patient-centred clinical method fits within a biopsychosocial approach to medical care delivery.
Whereas 'common ground' can be conceived as an agreement in broad terms, and as a platform for moving forward, SDM specifies a set of principles [17] and competences [4] that are needed to achieve the proposed goal of a negotiated decision. The difference with PCC therefore lies in the detailed process of elucidating the exact nature of the problem and outlining the range of options that need to be legitimately considered. It follows that each option, including the option of 'no action', has associated harms and benefits that require detailed explanation and an elaborate checking process that ensurses that the patient had understood both the factual data and that their views about the available choices will influence the decison that is finally made. In this way, SDM is more than an elaboration within the PCC model: it is also conceptually different [18].
A practical implication of this study is that medical educationalists should recognize that attention to patients' needs and emotions (patient centred communication) seems to be a fairly consistent working style of physicians. It is perhaps one of the competencies that doctors bring to their work from their qualification period [19]. Once established (a level of skill in PCC) it is hard to influence and it is therefore vital that medical curricula address this satisfactorily. In contrast, providing information and involving patients in decision making seems to be more variable. It may be influenced by the clinical problems presented and possibly also on patient characteristics (although this study did not show this) [20]. Aggregated scores per physician, based on videotaped consultations, are less consistent for SDM than for PCC. Skill acquisition in SDM hinges around the competences[4] of this approach. It is much more feasible for professionals to develop these skills in training [21]. Thus those involved in (post-graduate) training of doctors should also distinguish between PCC and SDM but may find it more fruitful to address the latter. Because of the greater variability in SDM in practice any performance assessment of GPs which examines their skills in SDM will require more cases for SDM than for PCC.
The theoretical implication of this study is that patient centred communication cannot be viewed as a unidimensional communication method. It therefore seems necessary to deconstruct the patient centred communication method into its different components in order to attain greater understanding of the interrelationships of consultation stages and tasks. Shared decision making cannot be considered as patient centred communication by another name. Maybe it is better to use patient-centred communication as a more embracing term which includes SDM and other aspects. Future studies are required with specifically designed instruments to explore which aspects can be distinguished conceptually and empirically [11,12]. Specifically, the ability of these instruments to distinguish the core elements of these constructs and to identify shared aspects should be evaluated.
Conclusion
The study provides evidence that PCC and SDM can be differentiated. Approaches to communication between clinicians and patients require further focused research and training developments.
Competing interests
None declared.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Contributor Information
Michel Wensing, Email: M.Wensing@hsv.kun.nl.
Glyn Elwyn, Email: ElwynG@cardiff.ac.uk.
Adrian Edwards, Email: EdwardsAG@cardiff.ac.uk.
Eric Vingerhoets, Email: Vingerhh@knmg.nl.
Richard Grol, Email: R.Grol@hsv.kun.nl.
References
- Stewart M, Brown J, Weston W, McWhinney L, McWilliam C, Freeman T. Patient-centred medicine: transforming the clinical method London, Sage, 1995.
- Mead N, Bower P. Patient-centredness: a conceptual framework and review of the empirical literature. Soc Sci Med. 2000;51:1087–1110. doi: 10.1016/S0277-9536(00)00098-8. [DOI] [PubMed] [Google Scholar]
- Charles C, Whelan T, Gafni A. What do we mean by partnership in making decisions about treatment? BMJ. 1999;319:780–782. doi: 10.1136/bmj.319.7212.780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elwyn G, Edwards A, Kinnersley P, Grol R. Shared decision-making and the concept of equipoise: defining the competences of involving patients in healthcare choices. Br J Gen Pract. 2000;50:892–899. [PMC free article] [PubMed] [Google Scholar]
- Richards T. Partnership with patients. BMJ. 1998;316:85–86. doi: 10.1136/bmj.316.7125.85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meeuwesen L, Schaap C, Van der Staak C. Verbal analysis of doctor-patient communication. Soc Sci Med. 1991;32:1143–1150. doi: 10.1016/0277-9536(91)90091-P. [DOI] [PubMed] [Google Scholar]
- Kaplan SH, Gandek B, Greenfield S, Rogers W, Ware JE. Patient and visit characteristics related to phyisicans' participatory decision-making style. Med Care. 1995;33:1176–1187. doi: 10.1097/00005650-199512000-00002. [DOI] [PubMed] [Google Scholar]
- Guadagnoli E, Ward P. Patient participation in decision-making. Soc Sci Med. 1998;47:329–339. doi: 10.1016/S0277-9536(98)00059-8. [DOI] [PubMed] [Google Scholar]
- Benbassat J, Pilpel D, Tidhar M. Patients' preferences for participations in clinical decision-making: a review of published surveys. Behav Med. 1999;24:81–88. doi: 10.1080/08964289809596384. [DOI] [PubMed] [Google Scholar]
- Van Thiel J, Kraan HF, Van der Vleuten CPM. Reliability and feasibility of meausring medical interviewing skills: the revised Maastricht history-taking and advice checklist. Med Educ. 1991;25:224–229. doi: 10.1111/j.1365-2923.1991.tb00055.x. [DOI] [PubMed] [Google Scholar]
- Ram P, Grol R, Rethans JJ, Schouten B, Van der Vleuten C, Kester A. Assessment of general practitioners by video observation of communicative and medical performance in daily practice: issues of validity, reliability and feasibility. Med Educ. 1999;33:447–454. doi: 10.1046/j.1365-2923.1999.00348.x. [DOI] [PubMed] [Google Scholar]
- Braddock CH, Fihn SD, Levinson W, Jonsen AR, Pearlman RA. How doctors and patients discuss routine clinical decisions: informed decision making in the outpatient setting. J Gen Intern Med. 1997;12:339–345. doi: 10.1046/j.1525-1497.1997.00057.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elwyn G, Edwards A, Mowle S, Wensing M, Wilkinson C, Kinnersley P, Grol R. Measuring the involvement of patients in shared decision making: a systematic review of instruments. Patient Educ Counsel. 2001;1406:1–19. doi: 10.1016/s0738-3991(00)00149-x. [DOI] [PubMed] [Google Scholar]
- Donner A, Birkett N, Buck C. Randomization by cluster, sample size requirements and analysis. Am J Epidem. 1981;114:906–915. doi: 10.1093/oxfordjournals.aje.a113261. [DOI] [PubMed] [Google Scholar]
- Braddock CH, Fihn SD, Levinson W, Jonsen AR, Pearlman RA. How doctors and patients discuss routine clinical decisions: informed decision making in the outpatient setting. Journal of General Internal Medicine. 1997;12:339–345. doi: 10.1046/j.1525-1497.1997.00057.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elwyn G. Shared decision making. Patient involvement in clinical practice. PhD Thesis, University of Nijmegen, Netherlands, 2001.
- Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (Or it takes at least two to tango). Soc Sci Med. 1997;44:681–92. doi: 10.1016/S0277-9536(96)00221-3. [DOI] [PubMed] [Google Scholar]
- Edwards A, Elwyn G, eds Evidence based patient choice: inevitable or impossible? Oxford, Oxford University Press. 2001.
- Elwyn G, Charles C. Shared decision making: the principles and the competences. In: Edwards A and Elwyn G, editor. Evidence-based patient choice – inevitable or impossible? Oxford, Oxford University Press; 2001. pp. 118–143. [Google Scholar]
- Elwyn G, Edwards A, Gwyn R, Grol R. Towards a feasible model for shared decision making: a focus group study with general practice registars. BMJ. 1999;319:753–757. doi: 10.1136/bmj.319.7212.753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edwards A, Elwyn G. Developing professional ability to involve patients in their care: pull or push? Qual Health Care 2001. 2001;10:129–130. doi: 10.1136/qhc.0100129... [DOI] [PMC free article] [PubMed] [Google Scholar]