

Abstract
Background:
Child maltreatment (CM) is robustly associated with youth risk for addictive behaviors , and recent findings suggest that this may be mediated through impulsive discounting of future rewards. However, research indicates that youth self-regulation (emotional and cognitive), particularly in peer contexts, is critical to consider in the study of decision making. The present study aimed to examine the indirect link between CM and alcohol and other drug (AOD) use problems, through delayed reward discounting (DRD), among a community sample of emerging adults. Further, the current investigation aimed to examine whether this indirect link was moderated by heart rate variability (HRV), a physiological proxy for regulation of stress reactivity.
Methods:
A sample of emerging adults (N = 225; Mage = 21.56; SDage = 2.24; 52.9% female) was assessed at two time-points, with one year between assessments. The sample was comprised of rural emerging adults from lower socioeconomic backgrounds. DRD was examined using a monetary choice task, and HRV reactivity was derived during a social stress task.
Results:
Increased CM experiences were significantly linked to riskier DRD. HRV reactivity amplified the indirect effect between CM and alcohol use problems via riskier DRD.
Conclusions:
The results demonstrate that the connection between CM and alcohol use problems via impulsive decision-making is modulated by acute stress response reactivity, as indexed by heart rate variability.
Keywords: Child Maltreatment, Decision Making, Delayed Reward Discounting, Alcohol Use & Misuse, Heart Rate Variability
Many young adults (i.e., individuals aged 18-25) engage in developmentally normative substance use behaviors in social contexts (Elkington, Bauermeister, & Zimmerman, 2011; Romer & Hennessy, 2007). Similarly, alcohol and other drug (AOD) use problems peak during emerging adulthood (Substance Abuse and Mental Health Services Administration, 2006), and emerging adults from low socioeconomic status (low-SES) rural areas are at an increased risk (Lambert, Gale, & Hartley, 2008). Moreover, emerging adults who report having had adverse childhood experiences, such as child maltreatment (CM), show suboptimal decision-making and are vulnerable for AOD use problems (Oshri et al., 2017; Rogers, Moeller, Swann, & Clark, 2010). Although aspects of the decision making process are modulated by executive function control (Bickel, Yi, Landes, Hill, & Baxter, 2011; McClure, Laibson, Loewenstein, & Cohen, 2004), growing evidence suggests that decision making is also influenced by the ability to regulate oneself during socially stressful situations (Casey & Caudle, 2013; Dom, De Wilde, Hulstijn, Van Den Brink, & Sabbe, 2006; William R Lovallo, Yechiam, Sorocco, Vincent, & Collins, 2006; Werner, Duschek, & Schandry, 2009). Psychobiological sensitivity to stress (i.e., stress reactivity) is a construct that refers to the individual’s ability to self-regulate in response to acute social stress. Vulnerabilities in self-regulation are exacerbated when emerging adults are exposed to situational social stress (Schriber & Guyer, 2016), such as social pressure to conform to risky behaviors, thereby resulting in suboptimal decision-making (e.g., the decision to binge on AOD). Thus, the present study aimed to examine the significance of self-regulation in the link between CM and AOD use problems via impulsive decision-making. We hypothesized that self-regulation, as indicated by a physiological response in the context of an experimentally induced acute social stressor , would modulate the indirect effect of CM on AOD use problems via impulsive decision-making.
Decision Making and AOD Use Problems
Impulsivity is increasingly recognized to be a multifaceted ‘family’ of conceptually related constructs and measures, one of which is impulsive decision-making (Lejuez et al., 2010; James MacKillop et al., 2016). Impulsive decision-making processes, such as delayed reward discounting (DRD), have been consistently shown to be associated with AOD use problems (Amlung, Vedelago, Acker, Balodis, & MacKillop, 2017; J. MacKillop et al., 2011). Similar to delay of gratification, DRD is a behavioral index of an individual’s tendency to devalue rewards that are postponed. A person’s inclination to prefer immediate rewards over larger but delayed rewards is thought to manifest behaviorally in favoring the short-term rewarding benefits of social drinking or substance use. Specifically, youth who score high on DRD may decide to use alcohol or other substances because of the salient and immediate feeling of reward via activation of dopaminergic pathways, which outweighs the decision to abstain and avoid the negative sequelae that may ensue from such behavior (Bickel et al., 2011; de Wit, 2009; Mitchell, Fields, D’esposito, & Boettiger, 2005).
DRD is often assessed with a task-based survey in which individuals choose their preference for monetary rewards that vary in size and in delay of receipt. Numerous cross-sectional and several longitudinal studies have shown that individuals with substance use disorders prefer to obtain short-term rewards, as compared to control group participants (Acheson, Vincent, Sorocco, & Lovallo, 2011; Bickel & Marsch, 2001; Petry, 2001). Longitudinal studies further suggest that impulsive discounting of rewards predicts the onset of addictive behavior (Audrain-McGovern et al., 2009; Fernie et al., 2013). Lastly, a meta-analysis of case-control studies showed a significant range of effect sizes in the link between DRD and substance use, with an aggregated effect size that was medium in magnitude (i.e., Cohen’s d ranging from .15 to .87 with a mean of .58; MacKillop et al., 2011).
Child Maltreatment and Impulsive Decision Making
Growing research and emerging theoretical models suggest that early life stress induces neurocognitive vulnerability that is linked to AOD use problems (W. R. Lovallo, 2013; Sinha, 2008). These perspectives on stress and development suggest that chronic adverse early experiences are processed cognitively, resulting in brain adaptations that shape coping behaviors (Ellis, Bianchi, Griskevicius, & Frankenhuis, 2017; W. R. Lovallo, 2013). For example, adverse childhood experiences may lead to alterations in stress neuro-circuitry, which is associated with increased impulsivity and increased salience of drug-related stimuli in challenging or stressful social situations (e.g., being evaluated by peers; Birn et al., 2017; Lovallo, 2013; Puetz and McCrory, 2015). Further, Thibodeau, Cicchetti, and Rogosch (2015) found that maltreatment was linked to impulsivity among youth, and that this path was moderated by a genetic polymorphism linked to reward pathways. Similarly, among a large cross-sectional sample of adults, child abuse and neglect was found to be related to more delayed reward discounting, which in turn was significantly associated with a higher frequency of substance use (Oshri et al., 2017). Thus, growing empirical evidence exists to support the hypothesis that impulsivity acts as a mechanism linking adverse rearing environments to downstream risk for substance use addiction.
Delayed Reward Discounting and Self-Regulation in Acute Social Stress Contexts
Emotional and cognitive regulation of acute stress are vital components in the process of decision making (Bechara, 2005). Because emerging adults’ choice to binge drink or abuse drugs often occurs in a peer context, self-regulation abilities are necessary to mitigate socially induced stress and therefore avoid risk behaviors (Mischel et al., 2010; Zelazo & Carlson, 2012; Zucker, Donovan, Masten, Mattson, & Moss, 2008). This research is particularly germane to maltreated individuals who are socioemotionally vulnerable due to their past adverse rearing experiences (Kim & Cicchetti, 2010). Maltreated youth are more likely to have impaired self-regulation abilities, and therefore are prone to making suboptimal decisions (Thibodeau et al., 2015), especially when under acute stress associated with peer contexts (Bolger & Patterson, 2001). This suboptimal decision making includes the preference for immediate smaller rewards rather than delayed but larger ones (Oshri et al., 2017). Thus, the process of making a choice, such as the decision to binge drink or not during socially stressful situations, may be significantly contingent on self-regulatory capacity.
Heart Rate Variability, Self-Regulation and Risk Behaviors
Quantifying individuals’ ability to self-regulate under conditions of social stress (e.g., performing in front of peers) is prone to measurement error, especially when measured through observations or self-report surveys (Beauchaine, 2015). Large body of research suggests that the use of psychophysiological proxies provides a particularly valid approach for the measurement of self-regulation (Laborde, Mosley, & Thayer, 2017; Obradović, Bush, Stamperdahl, Adler, & Boyce, 2010). In addition, the physiological measurement of youths’ regulation during social stress is enhanced by utilizing experimental tasks. For example, performance in front of an evaluative peer audience constitutes an acute situational stressor that is pertinent to young adults social contexts, and evokes a strong stress psychophysiological and attendant emotional response (Kemeny, 2009).
Heart rate variability (HRV) is a physiological parameter that has been shown to reflect self-regulatory capacities (i.e., emotional and executive control) via its activation by the autonomic nervous system (ANS; Appelhans and Luecken, 2006, Thayer and Siegle, 2002). The ANS is divided into two major branches: the sympathetic and parasympathetic nervous systems. The sympathetic nervous system (SNS) is responsible for energy mobilization in threatening situations: for example, the SNS increases cardiac activity when individuals are under perceived social stress. The parasympathetic nervous system (PNS) is involved in energy conservation and restorative functions: for example, the PNS counteracts the effect of the sympathetic system by decelerating heart rate. The ability of the PNS to rapidly modulate cardiac activity, including HRV, allows for flexibility in responding to environmental demands. Given that the vagus nerve is a key component of the PNS (Brodal, 2010), researchers often refer to parasympathetic activity as vagal tone. Accordingly, cardiac vagal tone indexes the contribution of the PNS to cardiac regulation, which is shown to be associated with self-regulation at the cognitive, emotional, social, and physiological levels (Laborde et al., 2017). Thus, psychophysiological theories regard HRV as a measure of the continuous interplay between the SNS and PNS that affects ones’ heart rate, which yields information about autonomic flexibility and the capacity for emotional and cognitive regulation of the stress response (Appelhans & Luecken, 2006). Per the psychophysiological literature, in the present study, vagal tone refers to the activity of the vagus nerve, which can be measured by obtaining high-frequency HRV (Laborde et al., 2017).
According to models proposed by Porges’ polyvagal theory (2011) and Thayer’s neurovisceral integration model (J. Thayer, 2009), self-regulation is indexed through coordination between the PNS and SNS. These systems orchestrate physiological homeostasis, wherein the organism can amass resources at rest yet still be capable to optimally respond to external social demands when needed. The neurovisceral model (J. Thayer, 2009) suggests that there are neuroanatomical connections between the ANS and brain regions associated with emotional processing (e.g., cortical and limbic areas), whereas the polyvagal theory (Porges, 2011) focuses on the neural connections between the vagus nerve and other cranial nerves that control peripheral structures involved in the behavioral expression of emotion when under social threat. Together, these two HRV theories converge to suggest that greater self-regulation abilities are indicated through the effective functioning of vagus nerve activation by the parasympathetic nervous system (Porges, 2011; J. F. Thayer & Brosschot, 2005). Similarly, the connection between HRV reactivity and stress reactivity has been linked to Gray’s approach-avoidance motivational theory (Beauchaine, 2001; Gray, 1987). Gray hypothesized that there are two systems that govern behavioral activity: the behavioral inhibition system (BIS) and the behavioral activation system (BAS; Gray, 1987). The behavioral inhibition system (BIS) underlies motivation to avoid aversive outcomes, such the long-term health effect of alcohol abuse. Alternatively, the behavioral activation system (BAS) underpins the motivation to approach rewarding outcomes, such as the motivation to drink alcohol with peers due to the rewarding social and psychopharmacological effects that are mediated by dopaminergic pathways. Thus, self-regulation capacities that are reflected by vagal tone (e.g., HRV reactivity) may be key in inhibiting AOD use during the individuals’ process of evaluating and considering using substances because of the associated dopaminergic rewards. Consequently, self-regulation capacities are likely to serve as an important component in achieving more optimal decision-making outcomes when under acute social stress.
The Present Study
The present study uses a measure of HRV reactivity to test the hypothesis that self-regulation of stress-reactivity moderates the link between child maltreatment and AOD use problems via impulsive decision-making (See Figure 1). AOD use symptoms are early indicators of the development of addictive behaviors, and bear negative social and health implications for emerging adults as they transition to adult roles. Given that cultural norms amongst young people are different for alcohol and drug use, and that there are differential psychopharmacological effects of these drugs, it is important to empirically delineate the distinct etiologies of each substance. Therefore, in the present study, we modeled alcohol and drug use problems separately, thereby adjusting for overlapping variance between the two. In addition, we intentionally used a purposive sampling strategy (Boehnke, Lietz, Schreier, & Wilhelm, 2011) to recruit rural low-SES emerging adults, who are at a significant risk for both adverse rearing environments and AOD use problems (Haberstick et al., 2014; Lee et al., 2015). Given that vagally-mediated HRV reflects the functional capacity of a set of brain structures that are matured by emerging adulthood, HRV is expected in the present study to serve as a stable psychobiological context (i.e., statistical moderator). Specifically, in young adulthood, vagal activity is hypothesized to act as a moderator between DRD and the attendant risk of developing AOD use problems. We hypothesized that child maltreatment severity would be associated with elevated impulsive decision making, indicated by DRD (Hypothesis 1); that higher DRD would be linked to increased AOD use problems (Hypothesis 2); and that lower levels of of self-regulation abilities, indicated by lower levels of HRV reactivity, would exacerbate these associations (Hypothesis 3).
Fig. 1.
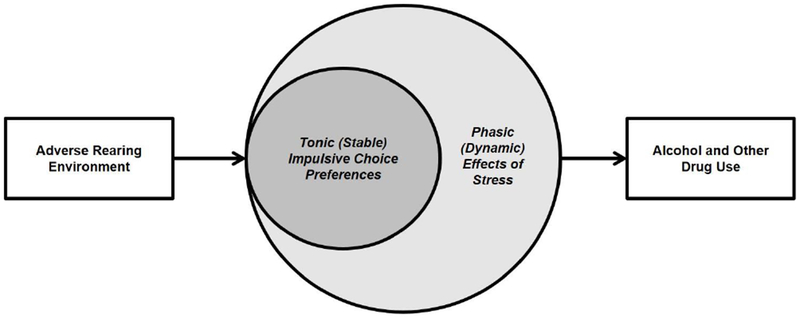
The Vagal Tone Pathway from Adverse Rearing Environment to Alcohol and Drug Use Problems via Decision Making Vulnerabilities
Type of stain: Black & White
MATERIALS AND METHODS
Participants
The data in the present study were collected in order to examine the mechanisms in the link between adverse childhood experiences and risk for addiction in rural areas. Thus, participants (N = 225) between the ages of 18 and 25 were recruited from a rural Southeastern community in the United States. Specifically, a rural sample of non-college-educated emerging adults were targeted in order to distinguish the sample from college-seeking young adults, who are often less ethnically diverse and from higher SES backgrounds. In addition, rural emerging adults are at an increased risk for socioeconomic adversity and substance use (Mack, Jones, & Ballesteros, 2017). Exclusion criteria included the presence of a cardiovascular condition or pregnancy, enrollment in high school or in college, and having a four-year college degree. Participants identified as male (n = 105, 46.7%), female (n = 119, 52.9%), or transgender (n = 1, 0.4%). The racial/ethnic makeup of the sample was diverse, with 59.6% identifying as White, 30.7% identifying as African American, 5.8% identifying as Hispanic/Latino/a, and 3.6% identifying as Other. The average age of participants was 21.56 (SD = 2.24). The majority of participants reported making less than $20,000 each year (n = 173, 76.9%).
Procedures
All study procedures were approved by the Institutional Review Board for ethical conduct in research. Participants were recruited by trained research assistants and community recruiters via in-person and local online advertisements. All study procedures took place in a private laboratory space on a university campus. Prior to arriving at the laboratory, participants were reminded not to use alcohol or other drugs within the past 24 hours before their participation in the study. Prior to any study activities, participants provided their informed consent. After informed consent was obtained, researchers connected participants to an electrocardiogram (ECG). Female participants were intentionally paired with female research assistants in order to enhance participants’ comfort with electrode placement. Researchers placed seven dermal electrodes on the left and right clavicle, the left and right rib, the upper and lower spine, and the sternum. Subsequently, participants were instructed to use headphones to listen to and watch a relaxing three-minute video of neutral nature landscapes in order to establish baseline HRV. The relaxation procedure, including video content and duration, was established based on recommendations for obtaining HRV (Malik et al., 1996) and a pilot phase in which ten participants gave feedback on the video segment. The large majority of participants (94.0%) rated the video as being “somewhat relaxing” to “very relaxing”.
Following the baseline assessment, researchers administered a five-minute mental arithmetic performance task to elicit an acute response to social stress. This social threat task has been shown to reliably elicit psychological (e.g., negative emotion) and physiological (ANS activation; e.g., vagal withdrawal) stress reactions (Gruenewald et al., 2004). During the task, participants were asked to quickly and accurately answer a series of increasingly difficult arithmetic problems, verbally, in front of an audience of research assistants. In order to account for differential math abilities, the difficulty of the task was adjusted (from easy to more difficult) based on participants’ response accuracy and speed. Research assistants were trained to remain neutral and to avoid giving feedback throughout the task. After the arithmetic stress task, participants were asked to view a three-minute relaxing video, and then answered a series of questionnaires. At the end of the procedure, participants reported how stressful the task felt for them (1= “not stressful at all”, 2 = “not very stressful”, 3 = “somewhat stressful”, 4 = “stressful”, and 5 = “very stressful”). The mean level was 3.57 and standard deviation was 1.08, with 84.3% participants rating the task as being somewhat to very stressful. Following the completion of study procedures, researchers debriefed all participants about the purpose of the mental math task, and offered a handout with local mental health resources.
At the first time point, participants gave their consent to participate in a brief follow-up survey. Approximately nine to twelve months after the baseline assessment, researchers contacted consenting participants via e-mail or text message. Subjects provided an additional informed consent via an online form, and then completed a brief online follow-up questionnaire. The attrition rate was moderate, with 65.3% of the subjects participating at Time 2.
Measures
Child maltreatment (T1).
The short form of the Childhood Trauma Questionnaire (CTQ-SF; Bernstein and Fink, 1998) was utilized to assess childhood experiences of maltreatment. Participants responded to 28 items about their experiences “while growing up”, on a Likert scale from one (never true) to five (very often true). This scale has been validated among normative community samples (Bernstein et al., 2003). The subscales that were utilized for the present study included physical abuse (α = .86), emotional abuse (α = .90), sexual abuse (α = .94), emotional neglect (α = .88), and physical neglect (α = .83).
Delayed reward discounting (T2).
The 27-item Monetary Choice Questionnaire (MCQ; Kirby and Petry, 2004) was utilized to measure delayed reward discounting. In the MCQ, participants indicated their hypothetical choice between a smaller immediate monetary reward, and a larger delayed monetary reward. The time delay varied for each item (e.g., 7, 19 or 136 days). For example, a participant may be asked “Would you rather have $14 today or $25 in 19 days”. Each item reflects choices between different preferences based on a hyperbolic discounting model (), in which the temporal discounting function is the free-ranging parameter k. Participants’ k values are inferred based on the pattern of choices. Three values of k were calculated for small, medium, and large reward magnitudes. Higher values of k represent greater reward discounting, and thus are indicative of participants’ preference for smaller, immediate rewards. Due to high positive skewness, k values were logarithmically transformed. For the present study, the log k values of small, medium, large magnitudes and composite log k were analyzed in the model separately.
Substance use (T1 & T2).
Participants self-reported on substance use behaviors at both the baseline and follow up time points.
Alcohol use problems.
The Alcohol Use Disorders Identification Test (AUDIT; Babor et al., 2001) was used to measure alcohol use frequency and problems. The AUDIT was developed by the World Health Organization as a simple method of screening for excessive drinking, and its validity and reliability have been supported among community samples (Knight, Sherritt, Harris, Gates, & Chang, 2003; Selin, 2003). Ten items were administered to participants, who answered questions such as “How often do you have six or more drinks on one occasion?” Eight items were scored on a four-point Likert scale that ranged from zero (never) to four (daily or almost daily), and two items (e.g., “Have you or someone else been injured because of your drinking?”) were scored with a three-point Likert scale from zero (never) to three (yes and in the last year). A sum score of the ten items was calculated, with higher scores representing a greater severity of alcohol use problems. The scale exhibited good internal reliability (αΤ1 = .77, αΤ2 = .84). Then, the sum score was transformed to a binary variable to indicate if the participant met the clinical cutoff of AUDIT (cut-off larger than 5; “1” = above the cut-off and “0” = below the cut-off score; Berman et al., 2003).
Drug use problems.
The Drug Use Disorders Identification Test (DUDIT; Berman et al., 2003) was utilized to measure participants’ problematic drug use. DUDIT was developed as a parallel instrument to the AUDIT for identification of individuals with drug-related problems. A sum score was calculated, which was comprised of eleven items (e.g., “Do you use more than one type of drug on the same occasion?”). Nine items were scored on a Likert scale from zero (never) to four (daily or almost daily), and two items (e.g., “Has a relative, friend, doctor, or other health care worker been worried about your drug use or said to you that you should stop using drugs?”) utilized a three-point Likert scale ranging from zero (never) to three (yes and in the last year). Higher DUDIT scores represent greater drug use problems. The scale exhibited excellent internal reliability (αΤ1 = .90, αΤ2 = .90). Clinical cut-off scores on the DUDIT are 2 for female and 6 ( > 5) for male participants (Berman et al., 2003). In the present study, the sum score was transformed to a binary variable to indicate if the participants met the clinical cutoff on the DUDIT (“1” = at or above the cut-off and “0” = below the cut-off score).
High-frequency HRV reactivity.
HRV reactivity was utilized to assess emerging adults’ psychophysiological capacity to self-regulate during acute social stress via the parasympathetic nervous system (J. F. Thayer & Lane, 2000; J. F. Thayer & Siegle, 2002). Procedures were in accordance with current standards for measuring HRV in psychophysiological research (Berntson et al., 1997). HRV was measured using the BioNex system from MindWare Technologies (Gahanna, OH). Data were digitized with the MindWare HRV 3.1.0 Software module (MindWare Technologies, Ltd., Gahanna, OH) at a sampling rate of 1000 Hz. High-frequency components of HRV (0.12 to 0.42 Hz) were obtained via power spectrum analysis (Akselrod et al., 1981), in order to target parasympathetic neural activity. Past research has indicated that high frequency components of HRV are indicative of more effective self-regulation (Akselrod et al., 1981; Appelhans & Luecken, 2006). In order to estimate and correct for individual differences in respiration, spectral analysis of thoracic impedance was utilized (Ernst, Litvack, Lozano, Cacioppo, & Berntson, 1999). Derived from the ECG signal, inter-beat intervals (IBIs) were converted into 120s segments using an interpolation algorithm, and physically improbably IBIs were detected using a MAD/MED algorithm via MindWare software. Data were also manually inspected by trained researchers to detect abnormal R-R intervals such as inadvertent cardiac fluctuations and ectopic beats in HRV due to participants’ physical movement or breath. Abnormal R-R intervals were manually corrected by deleting extra beats and inserting mid-beats, as per the instructions of Mindware Technologies (Gahanna, OH).
A residualized change score was calculated for HRV reactivity using participants’ mean HRV during the baseline period and during the stress period (arithmetic task; see equation below). The use of a residualized change score allows for the adjustment of variance in baseline HRV (Berntson et al., 1997). A lower HRV residualized change score (ΔHRV) indicates a decrease from baseline to the stress task (i.e., more vagal withdrawal), and thus suggests a higher level of HRV reactivity and self-regulation.
Demographics.
Covariates included emerging adults’ gender, age, and family annual income. Gender was coded as “1” = male and “2” = female. Family annual income was reported as “1” for less than $20,000, “2” for $20,001-$50,000, “3” for $50,001-$70,000, “4” for $70,001-$100,000 and “5” for over $100,000, and then recoded to the median of each range.
Analytic Plan
A structural equation model (SEM) in Mplus Version 7.4 (Muthén & Muthén, 1998-2012) was used to test study hypotheses. The SEM was estimated using maximum likelihood estimation with robust standard errors. Missing data ranged from 0% to 34.7%. Missing data patterns were found to meet assumptions for missing completely at random (MCAR; Little’s MCAR test: χ2(27) = 28.05, p = .41), and therefore the full-information maximum likelihood (FIML) algorithm was used (Rubin & Little, 2002). FIML is a missing data method that has been shown to yield more efficient and less biased parameter estimates than traditional methods for handling missing data (Enders & Bandalos, 2001). Using standard model fit criteria (Hu & Bentler, 1999), a combination of fit indices were included to assess for adequate fit of the data to the structural model. These included the chi-square test of model fit, the comparative fit index (CFI), the root mean square error of approximation (RMSEA), the standardized root mean square residual (SRMR), and the weighted root mean square residual (WRMR). A confirmatory factor analysis (CFA) was used to assess the latent construct of child maltreatment (Brown, 2015), using five CTQ-SF subscales (i.e., physical abuse, sexual abuse, emotional abuse, physical neglect, and emotional neglect) as indicators. Next, SEM was used to model the associations between child maltreatment, DRD, substance use, and ΔHRV. Probit regression within the SEM framework was utilized to model AOD use problems as binary dependent variables. To test HRV reactivity as a moderator of the associations between DRD and substance use, maximum likelihood estimation of latent interaction effects was used (Klein & Moosbrugger, 2000). Subsequently, to examine the indirect effect conditional on level of HRV reactivity, a mediation procedure (i.e., RMediation) was used, which produces a confidence interval for the product of two normal random variables using three methods: distribution of the product of coefficients, Monte Carlo, and asymptotic normal theory with the multivariate-delta standard error (asymptotic-delta) method (MacKinnon, Fritz, Williams, & Lockwood, 2007; Tofighi & MacKinnon, 2011). The Johnson and Neyman technique (1936) was employed to interpret the moderating role of HRV reactivity.
RESULTS
Preliminary Analyses
Descriptive and correlational analyses were used to evaluate the level of exposure to adverse childhood experiences as well as elevated risk for AOD use problems in the current sample of rural youth (Table 1 and Figure 2). The current sample manifested significant child maltreatment experiences, with 31.6% reporting emotional abuse (clinical cutoff > 12), 28.6% reporting physical abuse (clinical cutoff > 9), 20.9% reporting sexual abuse (clinical cutoff > 7), 31.6% reporting emotional neglect (clinical cutoff > 14), and 23.1% reporting physical neglect (clinical cutoff > 9). Among the 225 participants, 42.7% at the first time-point, and 40.8% at second time-point met the AUDIT cut-off score indicating hazardous alcohol use. Additionally, in accordance with standard cut-off scores on the DUDIT (2 for female and 6 for male; Berman et al., 2003), 54.9% of participants at time-point 1 and 44.2% of participants at time-point 2 were suggested to have drug use problems. Overall, 66.2% of participants at time-point 1 and 58.2% of participants at time-point 2 reported having either alcohol or drug use problems, or both.
Table 1.
Descriptive Statistics and Correlations of Study Variables (N = 225)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Emotional Abuse | -- | |||||||||||||
| 2. Physical Abuse | .72** | -- | ||||||||||||
| 3. Sexual Abuse | .43** | .37** | -- | |||||||||||
| 4. Emotional Neglect | .67** | .58** | .31** | -- | ||||||||||
| 5. Physical Neglect | .64** | .63** | .35** | .66** | -- | |||||||||
| 6. DRD-Small | .16* | .18** | .08 | .12 | .04 | -- | ||||||||
| 7. Drug (T1) | .12 | .05 | −.03 | .04 | .08 | .00 | -- | |||||||
| 8. Drug (T2) | .08 | .06 | −.06 | −.05 | −.03 | .00 | .49** | -- | ||||||
| 9. Alcohol (T1) | −.05 | −.09 | −.06 | −.09 | −.06 | −.04 | .31** | .14 | -- | |||||
| 10. Alcohol (T2) | −.18* | −.23** | −.12 | −.18* | −.14 | −.09 | .16 | .34** | .58** | -- | ||||
| 11. ΔHRV | −.11 | −.04 | −.05 | −.10 | −.09 | .04 | .04 | .22** | .00 | .06 | -- | |||
| 12. Gender | .17** | .06 | .27** | .19** | .05 | −.05 | −.34** | −.29** | −.30** | −.13 | −.01 | -- | ||
| 13. Age | −.06 | .00 | .01 | −.02 | .00 | .06 | −.02 | .05 | −.01 | −.14 | −.11 | −.03 | -- | |
| 14. F-Income | −.24** | −.32** | −.23** | −.34** | −.30** | −.03 | .00 | .16 | .25** | .21* | .10 | −.15* | .00 | -- |
| Mean | 11.14 | 8.96 | 7.31 | 12.07 | 7.70 | −1.47 | 7.25 | 5.92 | 6.06 | 5.72 | .67 | 1.54 | 21.56 | 49.08 |
| SD | 5.81 | 4.76 | 4.93 | 5.11 | 3.68 | .67 | 8.94 | 8.31 | 5.32 | 5.94 | 1.34 | .51 | 2.24 | 31.32 |
Note. DRD = Delayed reward discounting; ΔHRV = HRV Residualized Change Score; Alcohol = Alcohol use problems continuous variable; Drug = Drug use problems continuous variable; F-Income = Family annual income. Gender was coded as 1 for male and 2 for female.
p < .05,
p < .05.
Fig. 2.
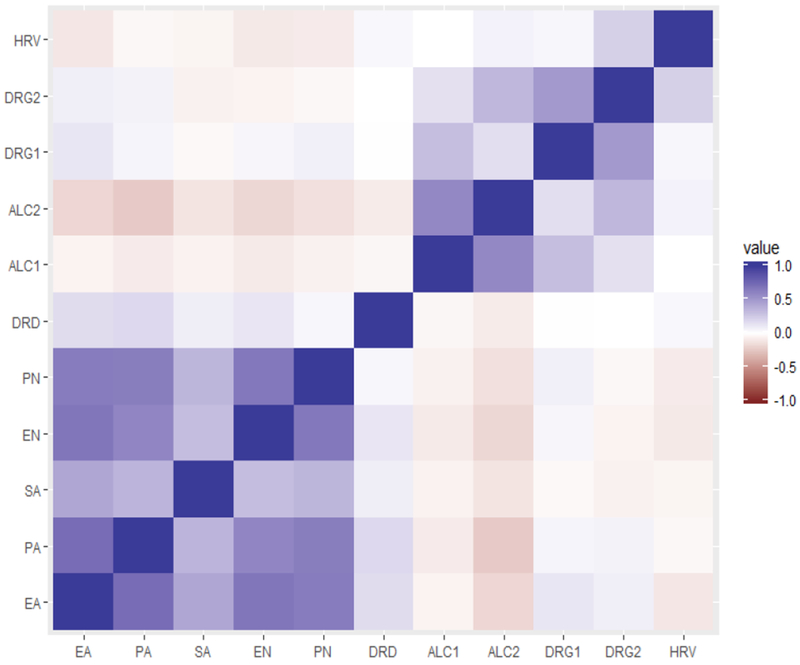
Correlation Heatmap of Study Variables.
Note: EA = Emotional abuse; PA = Physical abuse; SA = Sexual abuse; EN = Emotional neglect; PN = Physical neglect; ALC = Alcohol use problems (continuous); DRG = Drug use problems (continuous); HRV = HRV residualized change score. Blue squares indicate positive correlations, and red squares indicate negative correlations. The darker the color is, the stronger the correlational relationship is.
Type of stain: Color
In order to account for the common covariance between types of child maltreatment experiences, and to capture the variance of the most severe maltreatment, we employed a confirmatory factor analyses (CFA), a data reduction technique (Brown, 2015). The CFA confirmed the internal reliability of a single latent factor of child maltreatment, underlying the measurement of severity of child maltreatment experiences reflected by five indicators (i.e., physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect) (See Table 2). All factors loadings were moderate to high (λ > .45) and significant (p < .001; Brown, 2015) . The resulting model fit was excellent: χ2 (5) = 12.63 (p < .05). CFI = .99, SRMR = .02.
Table 2.
Measurement Model of Childhood Maltreatment Experiences (N = 225)
| Factors and Indicators | B (SE) | λ (SE) | R2 | 95%CI of λ |
|---|---|---|---|---|
| CM → Emotional Abuse | 1.00 (.00) | .86 (.03) | .26 | [.81, .91]*** |
| CM → Physical Abuse | .78 (.06) | .79 (.03) | .38 | [.72, .85]*** |
| CM → Sexual Abuse | .47 (.07) | .46 (.06) | .79 | [.35, .57]*** |
| CM → Emotional Neglect | .79 (.06) | .77 (.03) | .40 | [.71, .84]*** |
| CM → Physical Neglect | .63 (.05) | .77 (.03) | .41 | [.70, .84]*** |
Note. CM = Childhood maltreatment experiences; SE = Standard error; CI = Confidence interval. Model fit is good: χ2 (5) = 12.63 (p < .05). CFI = .99, SRMR = .02.
p < .001
Initial Model
A moderated mediation SEM model was used to concurrently test the moderation of the link between DRD and AOD use problems by HRV reactivity in the indirect effect from the child maltreatment factor to AOD use problems via DRD. Gender, age and family annual income were adjusted for in all the subsequent models. The reported model below refers to the small reward magnitude (other magnitudes are reported in the supplemental materials). The model was constructed following Preacher, Rucker, and Hayes (2007) Model 3, in which path b (the regressive path of AOD use problems on DRD) was moderated by HRV reactivity. The results of the SEM model are presented in Table 3 and Figure 3. The model exhibited an acceptable model fit: χ2 (63) = 85.94 (p < .05). CFI = .93, WRMR = .82, RMSEA = .04. Findings indicated positive significant associations between child maltreatment and DRD (β = .18, p < .05). No significant main effect was found for the association between DRD and alcohol use problems (β = .01, p = .92) nor between DRD and drug use problems (β = .12, p = .16) at the second time-point, after controlling for variance from substance use behaviors at the first time-point. In addition, ΔHRV was not significantly associated with alcohol use problems (β = −.05, p = .64) or drug use problems (β = .00, p = .97) at the second time-point. However, the interaction term of DRD and ΔHRV was associated with alcohol use problems (β = .17, p < .05) but not drug use (β = −.06, p = .41) at the second time-point, after controlling for the substance use behaviors at the first time-point1. To interpret the association between this interaction term and alcohol use problems, a parallel logistic regression model was conducted. Results indicated that with every one unit increase of the interaction term, one unit of DRD change resulted in an increase of participants’ alcohol use problems by 40% at the second time-point (logit = .34, OR = 1.40). These findings suggest that HRV reactivity moderated the associations between DRD (small magnitude) and alcohol use problems.
Table 3.
Moderated Mediation Model of the Associations between Child Maltreatment, Delayed Reward Discounting, Substance Use, and HRV Reactivity (N = 225)
| Paths | B (SE) | β | 95%CI of B |
|---|---|---|---|
| Direct effects | |||
| CM (T1) → DRD (T1) | .580 (.230) | .177 | [.129, 1.030]* |
| DRD (T1) → Alcohol (T2) | .011 (.117) | .009 | [−.219, .241] |
| ΔHRV (T1) → Alcohol (T2) | −.049 (.107) | −.042 | [−.259, .160] |
| CM (T1) → Alcohol (T2) | −.693 (.413) | −.178 | [−1.503, .117] |
| DRD (T1) → Drug (T2) | .158 (.111) | .124 | [−.059, .375] |
| ΔHRV (T2) → Drug (T2) | .005 (.116) | .004 | [−.223, .233] |
| CM (T1) → Drug (T2) | −.206 (.364) | −.050 | [−.920, .507] |
| Interaction Effects (small, medium, large magnitudes) | |||
| Small DRD | |||
| ΔHRV × DRD → Alcohol (T2) | .209 (.099) | .168 | [.014, .404]* |
| ΔHRV × DRD → Drug (T2) | −.082 (.101) | −.062 | [−.280, .115] |
| Medium DRD | |||
| ΔHRV × DRD → Alcohol (T2) | .07 (.11) | .05 | [−.14, .27] |
| ΔHRV × DRD → Drug (T2) | −.23 (.12) | −.15 | [−.47, .01] |
| Large DRD | |||
| ΔHRV × DRD → Alcohol (T2) | .06 (.11) | .04 | [−.16, .28] |
| ΔHRV × DRD → Drug (T2) | −.20 (.13) | −.14 | [−.46, .06] |
| Conditional Indirect Effect (small DRD) | |||
| CM → ΔHRV × DRD → Alcohol (T2) | .121 (.078) | .030 | [.001, .302]* |
| CM → ΔHRV × DRD → Drug (T2) | −.048 (.066) | −.011 | [−.196, .070 |
| Covariates | |||
| Alcohol (T1)→ Alcohol (T2) | 1.093 (.243) | .457 | [.616, 1.570]*** |
| Drug (T1) → Drug (T2) | 1.494 (.258) | .590 | [.987, 2.000]*** |
| Gender → DRD (T1) | −.150 (.144) | −.077 | [−.432, .132] |
| Gender → Alcohol (T2) | −.210 (.244) | −.090 | [−.687, .267] |
| Gender → Drug (T2) | −.166 (.252) | −.067 | [−.660, .327] |
| Age → DRD (T1) | .022 (.031) | .048 | [−.039, .082] |
| Age → Alcohol (T2) | −.094 (.056) | −.177 | [−.204, .017] |
| Age → Drug (T2) | −.013 (.057) | −.023 | [−.126, .099] |
| FIncome → DRD (T1) | .003 (.006) | .043 | [−.010, .016] |
| FIncome → Alcohol (T2) | −.008 (.011) | −.097 | [−.030, .014] |
| FIncome → Drug (T2) | .012 (.009) | .133 | [−.006, .029] |
Note. N = 225; DRD = Delayed reward discounting small logK value; T1 = Time 1; T2 = Time 2; SE = Standard error. CI = Confidence interval; CM = Childhood maltreatment experiences; ΔHRV = HRV Residualized Change Score; Alcohol = Alcohol use problems; Drug = Drug use problems; FIncome = Family annual income. Gender was coded as 1 for male and 2 for female. Model fit is acceptable: χ2 (63) = 85.94 (p < .05). CFI = .93, WRMR = .82, RMSEA = .04.
p < .05;
p < .01;
p < .001;
Fig. 3.
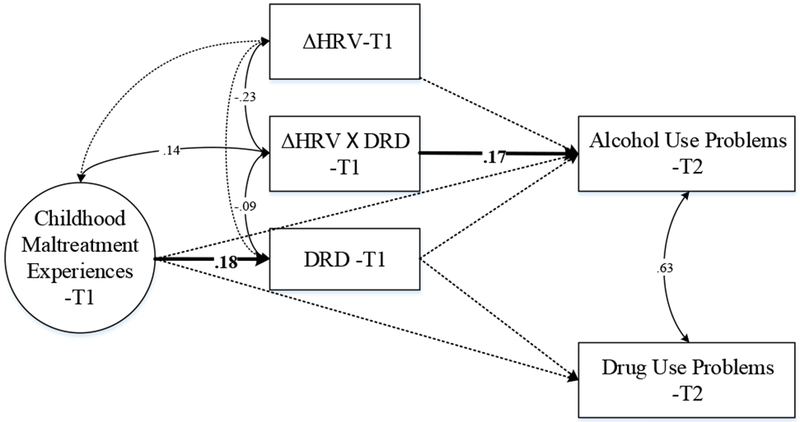
Moderated Mediation Model of the Associations Among Childhood Maltreatment, Delayed Reward Discounting, Substance Use, and HRV Reactivity during Young Adulthood.
Note. T1 = Time 1; T2 = Time 2; DRD = Delayed reward discounting (small rewards magnitude). ΔHRV = HRV residualized change score, with negative values indicating higher HRV reactivity. Gender, age, family annual income, and substance use at T1 were controlled in the analyses. The controlled paths are not displayed for clarity. Only standardized parameters of significant paths are presented in the figure.
Type of stain: Black & White
Mechanistic Analyses
Johnson and Neyman’s technique (1936) was used to probe and interpret the moderating roles of HRV reactivity on the associations between DRD and alcohol use problems (Figure 4). As Figure 4 suggests, for participants with lower levels of HRV reactivity (i.e., higher ΔHRV), DRD was associated with more alcohol use problems. Furthermore, DRD was associated with fewer alcohol use problems for participants with higher levels of HRV reactivity (i.e., lower ΔHRV).
Fig. 4.
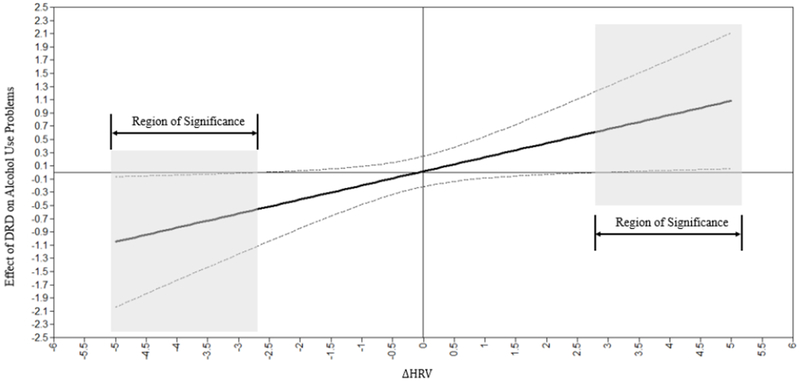
Interpretation of the Moderating Role of HRV Reactivity on the Associations between Delayed Reward Discounting and Alcohol Use Problems.
Note. Shadowed area indicates that among participants with lower HRV reactivity (i.e. high HRV residualized change score), DRD (small magnitude) is associated with higher levels of alcohol use problems significantly. However, with higher levels of HRV reactivity (i.e. low HRV residualized change score), DRD is associated with fewer alcohol use problems.
Type of stain: Black & White
A mediation procedure (MacKinnon et al., 2007; Tofighi & MacKinnon, 2011) was employed in order to test the conditional indirect effect (Preacher et al., 2007). Results showed that the indirect effect of child maltreatment on alcohol use problems through DRD, and conditional on ΔHRV, was significant (α*β = .03, p < .05). Specifically, the indirect effect between child maltreatment and alcohol use problems through DRD was positive among participants with low HRV reactivity but negative for participants with high levels of HRV reactivity.
DISCUSSION
Child maltreatment is significantly associated with neurocognitive vulnerabilities that are implicated in addictive behaviors among emerging adults (W. R. Lovallo, 2013; Oshri et al., 2017; Puetz & McCrory, 2015; Sinha, 2008). The present study extended this line of inquiry by utilizing longitudinal data drawn from a sample of low-SES rural emerging adults and incorporating an experimental task for self-regulation to test the impact of child maltreatment experiences on impulsive decision-making and attendant elevations in AOD use problems. Specifically, this study aimed to test the hypothesis that the effect of child maltreatment on decision-making and substance use risk is embedded within a context of psychobiological sensitivity to social stress (Karpyak et al., 2014). Findings showed that among emerging adults with poor self-regulation, as indicated by blunted reactivity in heart rate variability, more severe child maltreatment experiences were significantly linked to alcohol use problems via impulsive decision-making. Specifically, DRD was found to underlie the connection between adverse childhood experiences and risk for substance use problems, conditional upon level of HRV reactivity.
CM and DRD
In ort of our first hypothesis, child maltreatment severity was found to be significantly associated with a steeper discounting rate of delayed rewards. This finding corroborates neurobiological research that has shown adverse rearing environments to negatively impact neurobiological systems that subserve cognitive and emotional control functions. For example, William R Lovallo et al. (2013) and Lovic, Keen, Fletcher, and Fleming (2011) both reported that youth who experienced adverse childhood experiences were at risk for impulsive behaviors. Similarly, Oshri et al. (2017) found that adolescents who reported child abuse and neglect evinced higher levels of impulsive behaviors, and adults who reported child maltreatment evinced compromised DRD. In addition, recent research using fMRI technology demonstrates that early life stress can adversely affect executive control functions that are tied to DRD, such as working memory (Bickel et al., 2011), response inhibition (Harms et al., 2017) and reward salience in both animal (O’Connor, Moloney, Glennon, Vlachou, & Cryan, 2015) and human samples (Birn et al., 2017; Oswald et al., 2014).
Recent developmental evolutionary perspectives on child development offer insight to the question of why maltreated youth are at an increased risk for impulsive decision-making and risk behaviors such as drug use (Ellis et al., 2017). From this perspective, youth reared in harsh environments may have biologically adapted to their past unpredictable context. Relatedly, a key working hypothesis in developmental evolutionary perspectives is the specialization hypothesis (Ellis et al., 2017). According to this hypothesis, growing up under stressful conditions may lead to later disadvantageous decision-making under conditions of stress (i.e., early life stress sensitizes later responses to social stress). For example, youth who adapted to adverse rearing environments may value more immediate resources, as opposed to delayed and larger rewards, under conditions of current stress and uncertainty, but not in safe circumstances (Mittal, Griskevicius, Simpson, Sung, & Young, 2015). The functional valuation of more immediate rewards over larger but delayed rewards may be adaptive to youth in adverse contexts, because they perceive their environment to be dangerous and thus the future uncertain. This adaptation to an adverse childhood environment could become a liability as youth mature out of their home environment (Oshri, Duprey, Kogan, Carlson, & Liu, 2018). Such vulnerabilities are compounded during young adulthood, as youth are increasingly independent and their peer environment is growing particularly salient. Additionally, opportunities for substance use peak in young adulthood. Thus, taken together, the ability to make decisions about substance use in the context of social stress, given the increased salience of the peer network, can be particularly difficult for emerging adults who have been maltreated and who potentially have emotional and neurocognitive vulnerabilities (Erickson, Egeland, & Pianta, 1989).
DRD, AOD Use Problems, and Moderation by HRV Reactivity
In contrast to the second hypothesis, the direct association between DRD and substance use risk was not statistically significant. The lack of a significant direct effect of DRD on substance use may be an idiosyncratic reflection of the rural population used in the present study. In fact, a meta-analyses by MacKillop and colleagues (J. MacKillop et al., 2011) reported that the effect size between DRD and substance use significantly varied across populations, with clinical populations showing the strongest effect size. Alternatively, this non-significant effect may be better explained by theory and research on the role of self-regulation (emotional and cognitive) in decision making processes (Casey & Caudle, 2013).
The third hypothesis was partially supported, as the direct association between DRD and alcohol use risk was statistically significant only among youth with lower levels of self-regulation. Accordingly, the findings indicated that differential functioning in HRV reactivity, putatively reflecting self-regulation, served as a moderator in the indirect effect linking early adversity to substance use. This is consistent with studies that have found a moderating role of vagal tone in the link between early adversity and internalizing problems in youth (McLaughlin, Alves, & Sheridan, 2014), as well as harsh parenting and adjustment problems in youth (e.g., El‐Sheikh et al., 2001), independent of other aspects of impulsivity. The findings of the present study also support theories that underline the important role of emotional regulatory processes in youths’ decision making (Bickel et al., 2007; Rudolph et al., 2017), particularly in social contexts (Ahmed, Bittencourt-Hewitt, & Sebastian, 2015; King, McLaughlin, Silk, & Monahan, 2017), by showing that decision making is affected by stress reactivity under acute social stress. Research on the neural basis of impulsive actions suggests that the decision making process is based on separate systems: the cognitive control and the reward-based (also referred to as socio-emotional) systems (McClure et al., 2004). According to this line of research, when cognitive control can’t effectively modulate the socioemotional system, then decision making processes are more compromised. Because cognitive control functions are still developing through emerging adulthood, this theory is particularly relevant in this sample (Steinberg, 2010).
In addition, the findings on the role of HRV reactivity in the link between DRD and alcohol use problems corroborates Gray’s motivational model. Specifically, these results support the idea that the ANS modulates the reward salience of drugs and the individuals’ motivation to avoid or approach substance abuse behaviors (Beauchaine, 2001). Accordingly, self-regulation indexed by HRV reactivity was found to be instrumental in inhibiting alcohol abuse, possibly due to the increased ability of youth with higher HRV reactivity to process and evaluate using substances. Overall, the present findings add to research on risk factors for alcohol addiction by providing preliminary evidence for the role of the ANS system, and the parasympathetic nervous system in particular, in the influence of child maltreatment on reward valuation and attendant risk for addictive behaviors. Accordingly, this study joins a body of work in suggesting that self-regulatory processes are a critical component in youths’ decision-making and attendant risk for AOD use problems (Casey & Caudle, 2013).
The present study found that physiological self-regulation of stress reactivity moderated the association between DRD of small reward magnitudes and alcohol use problems, but not the association between DRD of larger reward magnitudes and AOD use problems. Previous studies have found that the association between DRD and substance varies depending on reward magnitude, with the association between substance use and smaller reward magnitudes showing greater effect sizes (e.g., Amlung & MacKillop, 2011). In addition, it is possible that DRD of smaller reward magnitudes is more representative of the decisions that low-SES young adults make on a regular basis. Thus, self-regulation in the context of social stress may be more pertinent during such decisions. Furthermore, in the present study, child maltreatment was indirectly linked to riskier decision-making and alcohol use problems, but not drug use severity. Thus, there may be a different mechanism linking child maltreatment and drug use versus alcohol use. For example, one clear difference between alcohol and illicit drugs is legal status; thus, the relationship between childhood adversity and substance use may be selectively channeled within more socially acceptable and normative substance use. Given that this is a conjecture, the dissociation of relationships detected in this study warrants follow-up and more direct study.
Implications for Policy and Preventive Intervention
The present findings bear important implications for policy and intervention efforts to prevent AOD use problems among rural low-SES emerging adults who report child maltreatment experiences. Recent research suggests the need for family focused preventive intervention programs for adolescents that target self-regulation and the attendant psychobiological processes that bear implications for AOD use behaviors in young adulthood (Stormshak, DeGarmo, Chronister, & Caruthers, 2017). Furthermore, basic research that confronts the early life origins of disparities in physical and mental health can contribute to policy initiatives (Shonkoff, Boyce, & McEwen, 2009). For example, Larkin, Felitti, and Anda (2014) and Anda (2014) suggest that a biopsychosocial perspective be utilized to inform social policies that respond to adverse childhood experiences, in order to achieve population-wide improvements in overall health. The authors further discuss prevention and intervention response strategies that focus on multiple levels of at-risk individuals, including families, communities, and the larger society. This approach is supported by economic research on human capital development which has suggested that significant cost savings may result from effective implementation of these strategies (Mathur, 1999). Overall, significant mental health risk outcomes are reported to be attributed to childhood adversity (Afifi et al., 2008). Policy initiatives that address socioeconomic inequalities, and prevention efforts that aim to reduce exposure to adverse childhood events, could substantially decrease the prevalence of addiction psychopathology and associated mental health problems in the general population.
Developers of intervention programs may benefit from considering the risk for child maltreatment and its idiosyncratic effect on decision-making and AOD use risk. Recent research suggests that mindfulness interventions can impact HRV and emotion regulation (Hülsheger, Alberts, Feinholdt, & Lang, 2013), thereby possibly buffering the effect of child maltreatment on impulsive decision making and AOD use problems. Continuing on this line of argumentation, growing studies report that mindfulness-based stress reduction (MBSR) has a positive influence on emotional distress (e.g. Kilpatrick et al., 2011; Kumar et al., 2008) including brain areas linked with self-regulation (Hölzel et al., 2011). Further, despite the evidence of strong stability of DRD (Odum, 2011), increasing research suggests that brain plasticity exists, especially in the context of intensive neurocognitive training. For example, working memory training (Vinogradov, Fisher, & de Villers-Sidani, 2012) was shown to mitigate high DRD and, plausibly, the risk for addiction (Bickel et al., 2011). Thus, it is possible that preventive intervention programs can tailor content to effectively target self-regulation and working memory among at-risk emerging adults, potentially improving their decision making performance and reducing the risk for AOD use problems among these youth.
Limitations and Strengths
Our present findings should be interpreted within the study’s limitations. First, the targeted sample comprised rural low-SES emerging adults. In order to increase the generalizability of the present study, future research should test the current models in impoverished metropolitan samples. However, a strength of the present study is the use of an understudied sample of emerging adults that are at significant risk for AOD use problems. In addition, the present study used psychophysiological data as a proxy for self and emotional regulation, in relation to AOD risk among emerging adults. Recent research suggests that alcohol dependence might affect resting state HRV and therefore could have added spurious variance to the HRV results (Quintana, McGregor, Guastella, Malhi, & Kemp, 2013). To address this limitation, we obtained a more robust measure emotion regulation by measuring HRV reactivity during an experimental task (Cole, Martin, & Dennis, 2004). Lastly, in the present study self-regulation was measured under an experimental condition of acute social evaluative stress. This acute stress procedure aimed to measure self-regulation via HRV reactivity when under a social stress evinced from being evaluated during performance in front of a peer audience. However, other types of acute stressors could play a role in the mechanism that underlies youths’ motivation to binge drink, such as drinking alone to self-medicate. Overall, the present study carries important strengths that contribute to the confidence in the reported results. These include the use of a multi-method (quasi-experimental, task-based, and self-report) longitudinal follow-up design with an understudied sample of emerging adults that are at significant risk for adverse childhood experiences and AOD problems.
Supplementary Material
Acknowledgments
This work was supported by the Owens Institute for Behavioral Research (OIBR) at the University of Georgia, Athens, GA, and by the Sarah H. Moss Fellowship for faculty at the University of Georgia. Dr. Oshri is a mentored scientist at the Center for Translational and Prevention Science (P30 DA026285). Dr. MacKillop is the holder of the Peter Boris Chair in Addictions Research, which partially supported his role.
Footnotes
We tested DRD in the model using small, medium, and large magnitude rewards, as well as a composite DRD variable. Results of medium, large, and composite DRD showed a significant association with CM, a non-significant association with AOD use problems, and a directionally consistent moderating relationship. The interactional analyses for all reward magnitudes are reported in Table 3, and the entire models per each of the reward magnitudes are presented in the supplemental materials. The results are presented in Table 3.
CONFLICT OF INTEREST
AO, SL, ED do not have conflicts of interest in any form; JM is a principal in BEAM Diagnostics, Inc.
References
- Acheson Ashley, Vincent Andrea S, Sorocco Kristen H, & Lovallo William R. (2011). Greater discounting of delayed rewards in young adults with family histories of alcohol and drug use disorders: studies from the Oklahoma family health patterns project. Alcoholism: Clinical and Experimental Research, 35(9), 1607–1613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Afifi Tracie O, Enns Murray W, Cox Brian J, Asmundson Gordon JG, Stein Murray B, & Sareen Jitender. (2008). Population attributable fractions of psychiatric disorders and suicide ideation and attempts associated with adverse childhood experiences. American journal of public health, 98(5), 946–952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahmed Saz P, Bittencourt-Hewitt Amanda, & Sebastian Catherine L. (2015). Neurocognitive bases of emotion regulation development in adolescence. Developmental cognitive neuroscience, 15, 11–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akselrod Solange, Gordon David, Ubel F Andrew, Shannon Daniel C, Barger A Clifford, & Cohen Richard J. (1981). Power spectrum analysis of heart rate fluctuation: a quantitative probe of beat-to-beat cardiovascular control. Science, 220–222. [DOI] [PubMed] [Google Scholar]
- Amlung Michael, Vedelago Lana, Acker John, Balodis Iris, & MacKillop James. (2017). Steep delay discounting and addictive behavior: a meta‐analysis of continuous associations. Addiction, 112(1), 51–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anda Robert. (2014). Adverse childhood experiences: Connecting a developmental lens to the health of society.
- Appelhans Bradley M, & Luecken Linda J. (2006). Heart rate variability as an index of regulated emotional responding. Review of general psychology, 10(3), 229. [Google Scholar]
- Audrain-McGovern J, Rodriguez D, Epstein LH, Cuevas J, Rodgers K, & Wileyto EP (2009). Does delay discounting play an etiological role in smoking or is it a consequence of smoking? Drug Alcohol Depend, 103(3), 99–106. doi: 10.1016/j.drugalcdep.2008.12.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG (2001) AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Health Care. 2nd ed. World Health Organization, Geneva, Switzerland. [Google Scholar]
- Beauchaine Theodore. (2001). Vagal tone, development, and Gray’s motivational theory: Toward an integrated model of autonomic nervous system functioning in psychopathology. Development and psychopathology, 13(2), 183–214. [DOI] [PubMed] [Google Scholar]
- Beauchaine Theodore. (2015). Future Directions in Emotion Dysregulation and Youth Psychopathology. J Clin Child Adolesc Psychol, 44(5), 875–896. doi: 10.1080/15374416.2015.1038827 [DOI] [PubMed] [Google Scholar]
- Bechara A (2005). Decision making, impulse control and loss of willpower to resist drugs: a neurocognitive perspective. Nat Neurosci, 8(11), 1458–1463. doi: 10.1038/nn1584 [DOI] [PubMed] [Google Scholar]
- Berman A, Bergman H, Palmstierna T, & Schlyter F (2003). The Drug Use Disorders Identification Test (DUDIT) Manual. Stockholm, Sweden: Karolinska Institutet. [Google Scholar]
- Bernstein David P, & Fink Laura. (1998). Childhood trauma questionnaire: A retrospective self-report: Manual: Psychological Corporation. [Google Scholar]
- Bernstein David P, Stein Judith A, Newcomb Michael D, Walker Edward, Pogge David, Ahluvalia Taruna, … Desmond David. (2003). Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child abuse & neglect, 27(2), 169–190. [DOI] [PubMed] [Google Scholar]
- Berntson GG, Bigger JT Jr., Eckberg DL, Grossman P, Kaufmann PG, Malik M, … van der Molen MW (1997). Heart rate variability: origins, methods, and interpretive caveats. Psychophysiology, 34(6), 623–648. [DOI] [PubMed] [Google Scholar]
- Bickel Warren K, & Marsch Lisa A. (2001). Toward a behavioral economic understanding of drug dependence: delay discounting processes. Addiction, 96(1), 73–86. doi: 10.1046/j.1360-0443.2001.961736.x [DOI] [PubMed] [Google Scholar]
- Bickel Warren K, Miller Michelle L, Yi Richard, Kowal Benjamin P, Lindquist Diana M, & Pitcock Jeffery A. (2007). Behavioral and neuroeconomics of drug addiction: competing neural systems and temporal discounting processes. Drug and alcohol dependence, 90, S85–S91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel Warren K, Yi R, Landes RD, Hill PF, & Baxter C (2011). Remember the future: working memory training decreases delay discounting among stimulant addicts. Biol Psychiatry, 69(3), 260–265. doi: 10.1016/j.biopsych.2010.08.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birn Rasmus M, Roeber Barbara J, & Pollak Seth D. (2017). Early childhood stress exposure, reward pathways, and adult decision making. Proceedings of the National Academy of Sciences, 201708791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boehnke Klaus, Lietz Petra, Schreier Margrit, & Wilhelm Adalbert. (2011). Sampling: The selection of cases for culturally comparative psychological research.
- Bolger Kerry E, & Patterson Charlotte J. (2001). Developmental pathways from child maltreatment to peer rejection. Child development, 72(2), 549–568. [DOI] [PubMed] [Google Scholar]
- Brodal Per. (2010). The central nervous system: structure and function: Oxford University Press. [Google Scholar]
- Brown Timothy A. (2015). Confirmatory factor analysis for applied research: Guilford Publications. [Google Scholar]
- Casey BJ, & Caudle Kristina. (2013). The teenage brain: Self control. Current directions in psychological science, 22(2), 82–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole Pamela M, Martin Sarah E, & Dennis Tracy A. (2004). Emotion regulation as a scientific construct: Methodological challenges and directions for child development research. Child development, 75(2), 317–333. [DOI] [PubMed] [Google Scholar]
- de Wit H (2009). Impulsivity as a determinant and consequence of drug use: a review of underlying processes. Addict Biol, 14(1), 22–31. doi: 10.1111/j.1369-1600.2008.00129.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dom Geert, De Wilde Bieke, Hulstijn Wouter, Van Den Brink Wim, & Sabbe Bernard. (2006). Decision-making deficits in alcohol-dependent patients with and without comorbid personality disorder. Alcoholism: Clinical and Experimental Research, 30(10), 1670–1677. [DOI] [PubMed] [Google Scholar]
- El-Sheikh Mona, Harger JoAnn, & Whitson Stephanie M. (2001). Exposure to interparental conflict and children’s adjustment and physical health: The moderating role of vagal tone. Child development, 72(6), 1617–1636. [DOI] [PubMed] [Google Scholar]
- Elkington Katherine S, Bauermeister José A, & Zimmerman Marc A. (2011). Do parents and peers matter? A prospective socio-ecological examination of substance use and sexual risk among African American youth. Journal of adolescence, 34(5), 1035–1047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis Bruce J, Bianchi JeanMarie, Griskevicius Vladas, & Frankenhuis Willem E. (2017). Beyond Risk and Protective Factors: An Adaptation-Based Approach to Resilience. Perspectives on Psychological Science. [DOI] [PubMed] [Google Scholar]
- Enders Craig K, & Bandalos Deborah L. (2001). The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural equation modeling, 8(3), 430–457. [Google Scholar]
- Erickson Martha Farrell, Egeland Byron, & Pianta Robert. (1989). The effects of maltreatment on the development of young children.
- Ernst John M, Litvack Daniel A, Lozano David L, Cacioppo John T, & Berntson Gary G. (1999). Impedance pneumography: Noise as signal in impedance cardiography. Psychophysiology, 36(3), 333–338. [DOI] [PubMed] [Google Scholar]
- Fernie G, Peeters M, Gullo MJ, Christiansen P, Cole JC, Sumnall H, & Field M (2013). Multiple behavioural impulsivity tasks predict prospective alcohol involvement in adolescents. Addiction, 108(11), 1916–1923. doi: 10.1111/add.12283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray JA. (1987). Problems in the behavioural sciences, Vol. 5 The psychology of fear and stress: New York: Cambridge University Press. [Google Scholar]
- Haberstick Brett C, Young Susan E, Zeiger Joanna S, Lessem Jeffrey M, Hewitt John K, & Hopfer Christian J. (2014). Prevalence and correlates of alcohol and cannabis use disorders in the United States: results from the national longitudinal study of adolescent health. Drug and alcohol dependence, 136, 158–161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harms Madeline B, Birn Rasmus, Provencal Nadine, Wiechmann Tobias, Binder Elisabeth B, Giakas Sebastian W, … Pollak Seth D. (2017). Early life stress, FK506 binding protein 5 gene (FKBP5) methylation, and inhibition-related prefrontal function: A prospective longitudinal study. Development and psychopathology, 29(5), 1895–1903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hölzel Britta K, Carmody James, Vangel Mark, Congleton Christina, Yerramsetti Sita M, Gard Tim, & Lazar Sara W. (2011). Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Research: Neuroimaging, 191(1), 36–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu Li-tze, & Bentler Peter M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural equation modeling: a multidisciplinary journal, 6(1), 1–55. [Google Scholar]
- Hülsheger Ute R, Alberts Hugo JEM, Feinholdt Alina, & Lang Jonas WB. (2013). Benefits of mindfulness at work: The role of mindfulness in emotion regulation, emotional exhaustion, and job satisfaction. Journal of Applied Psychology, 98(2), 310. [DOI] [PubMed] [Google Scholar]
- Johnson Palmer Oliver, & Neyman Jerzy. (1936). Tests of certain linear hypotheses and their application to some educational problems. Statistical research memoirs. [Google Scholar]
- Karpyak Victor M, Romanowicz Magdalena, Schmidt John E, Lewis Kriste A, & Bostwick John M. (2014). Characteristics of Heart Rate Variability in Alcohol-Dependent Subjects and Nondependent Chronic Alcohol Users. Alcoholism: Clinical and Experimental Research, 38(1), 9–26. [DOI] [PubMed] [Google Scholar]
- Kemeny Margaret E. (2009). Psychobiological responses to social threat: evolution of a psychological model in psychoneuroimmunology: Elsevier. [DOI] [PubMed] [Google Scholar]
- Kilpatrick Lisa A, Suyenobu Brandall Y, Smith Suzanne R, Bueller Joshua A, Goodman Trudy, Creswell J David, … Naliboff Bruce D. (2011). Impact of mindfulness-based stress reduction training on intrinsic brain connectivity. Neuroimage, 56(1), 290–298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim Jungmeen, & Cicchetti Dante. (2010). Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathology. Journal of Child Psychology and Psychiatry, 51(6), 706–716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King Kevin M, McLaughlin Katie A, Silk Jennifer, & Monahan Kathryn C. (2017). Peer effects on self-regulation in adolescence depend on the nature and quality of the peer interaction. Development and psychopathology, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirby KN, & Petry NM (2004). Heroin and cocaine abusers have higher discount rates for delayed rewards than alcoholics or non-drug-using controls. Addiction, 99(4), 461–471. doi: 10.1111/j.1360-0443.2003.00669.x [DOI] [PubMed] [Google Scholar]
- Klein Andreas, & Moosbrugger Helfried. (2000). Maximum likelihood estimation of latent interaction effects with the LMS method. Psychometrika, 65(4), 457–474. [Google Scholar]
- Knight John R, Sherritt Lon, Harris Sion Kim, Gates Elizabeth C, & Chang Grace. (2003). Validity of brief alcohol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcoholism: Clinical and experimental research, 27(1), 67–73. [DOI] [PubMed] [Google Scholar]
- Kumar Sameet, Feldman Greg, & Hayes Adele. (2008). Changes in mindfulness and emotion regulation in an exposure-based cognitive therapy for depression. Cognitive Therapy and Research, 32(6), 734. [Google Scholar]
- Laborde Sylvain, Mosley Emma, & Thayer Julian F. (2017). Heart rate variability and cardiac vagal tone in psychophysiological research–recommendations for experiment planning, data analysis, and data reporting. Frontiers in psychology, 8, 213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lambert David, Gale John A, & Hartley David. (2008). Substance abuse by youth and young adults in rural America. The Journal of Rural Health, 24(3), 221–228. [DOI] [PubMed] [Google Scholar]
- Larkin Heather, Felitti Vincent J, & Anda Robert F. (2014). Social work and adverse childhood experiences research: Implications for practice and health policy. Social work in public health, 29(1), 1–16. [DOI] [PubMed] [Google Scholar]
- Lee Jungeun Olivia, Hill Karl G, Hartigan Lacey A, Boden Joseph M, Guttmannova Katarina, Kosterman Rick, … Catalano Richard F. (2015). Unemployment and substance use problems among young adults: Does childhood low socioeconomic status exacerbate the effect? Social Science & Medicine, 143, 36–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lejuez CW, Magidson Jessica F, Mitchell Suzanne H, Sinha Rajita, Stevens Michael C, & De Wit Harriet. (2010). Behavioral and biological indicators of impulsivity in the development of alcohol use, problems, and disorders. Alcoholism: Clinical and Experimental Research, 34(8), 1334–1345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovallo WR (2013). Early life adversity reduces stress reactivity and enhances impulsive behavior: implications for health behaviors. Int J Psychophysiol, 90(1), 8–16. doi: 10.1016/j.ijpsycho.2012.10.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovallo William R, Farag Noha H, Sorocco Kristen H, Acheson Ashley, Cohoon Andrew J, & Vincent Andrea S. (2013). Early life adversity contributes to impaired cognition and impulsive behavior: studies from the Oklahoma Family Health Patterns Project. Alcoholism: clinical and experimental research, 37(4), 616–623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovallo William R, Yechiam Eldad, Sorocco Kristen H, Vincent Andrea S, & Collins Frank L. (2006). Working memory and decision-making biases in young adults with a family history of alcoholism: Studies from the Oklahoma Family Health Patterns Project. Alcoholism: Clinical and Experimental Research, 30(5), 763–773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovic V, Keen D, Fletcher PJ, & Fleming AS (2011). Early-life maternal separation and social isolation produce an increase in impulsive action but not impulsive choice. Behav Neurosci, 125(4), 481–491. doi: 10.1037/a0024367 [DOI] [PubMed] [Google Scholar]
- Mack Karin A, Jones Christopher M, & Ballesteros Michael F. (2017). Illicit Drug Use, Illicit Drug Use Disorders, and Drug Overdose Deaths in Metropolitan and Nonmetropolitan Areas—United States. American journal of transplantation, 17(12), 3241–3252. [DOI] [PubMed] [Google Scholar]
- MacKillop J, Amlung MT, Few LR, Ray LA, Sweet LH, & Munafo MR (2011). Delayed reward discounting and addictive behavior: a meta-analysis. Psychopharmacology (Berl), 216(3), 305–321. doi: 10.1007/s00213-011-2229-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKillop James, Weafer Jessica, Gray Joshua C, Oshri Assaf, Palmer Abraham, & de Wit Harriet. (2016). The latent structure of impulsivity: impulsive choice, impulsive action, and impulsive personality traits. Psychopharmacology, 233(18), 3361–3370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon David P, Fritz Matthew S, Williams Jason, & Lockwood Chondra M. (2007). Distribution of the product confidence limits for the indirect effect: Program PRODCLIN. Behavior research methods, 39(3), 384–389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mathur Vijay K. (1999). Human capital-based strategy for regional economic development. Economic Development Quarterly, 13(3), 203–216. [Google Scholar]
- McClure Samuel M, Laibson David I, Loewenstein George, & Cohen Jonathan D. (2004). Separate neural systems value immediate and delayed monetary rewards. Science, 306(5695), 503–507. [DOI] [PubMed] [Google Scholar]
- McLaughlin Katie A, Alves Sonia, & Sheridan Margaret A. (2014). Vagal regulation and internalizing psychopathology among adolescents exposed to childhood adversity. Developmental psychobiology, 56(5), 1036–1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mischel Walter, Ayduk Ozlem, Berman Marc G, Casey BJ, Gotlib Ian H, Jonides John, … Zayas Vivian. (2010). ‘Willpower’over the life span: decomposing self-regulation. Social cognitive and affective neuroscience, 6(2), 252–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell Jennifer M, Fields Howard L, D’esposito Mark, & Boettiger Charlotte A. (2005). Impulsive responding in alcoholics. Alcoholism: Clinical and Experimental Research, 29(12), 2158–2169. [DOI] [PubMed] [Google Scholar]
- Mittal Chiraag, Griskevicius Vladas, Simpson Jeffry A, Sung Sooyeon, & Young Ethan S. (2015). Cognitive adaptations to stressful environments: When childhood adversity enhances adult executive function. Journal of personality and social psychology, 109(4), 604–621. [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO. (1998-2012). BO Mplus user’s guide, 7. [Google Scholar]
- O’Connor Richard M, Moloney Rachel D, Glennon Jeffrey, Vlachou Styliani, & Cryan John F. (2015). Enhancing glutamatergic transmission during adolescence reverses early-life stress-induced deficits in the rewarding effects of cocaine in rats. Neuropharmacology, 99, 168–176. [DOI] [PubMed] [Google Scholar]
- Obradović Jelena, Bush Nicole R, Stamperdahl Juliet, Adler Nancy E, & Boyce W Thomas. (2010). Biological sensitivity to context: The interactive effects of stress reactivity and family adversity on socioemotional behavior and school readiness. Child development, 81(1), 270–289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odum Amy L. (2011). Delay discounting: trait variable? Behavioural processes, 87(1), 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oshri Assaf, Duprey Erinn B., Kogan Steven M., Carlson Matthew W., & Liu Sihong. (2018). Growth Patterns of Future Orientation among Maltreated Youth: A Prospective Examination of the Emergence of Resilience. Developmental Psychology. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oshri Assaf, Kogan SM, Kwon JA, Wickrama KAS, Vanderbroek L, Palmer AA, & MacKillop J (2017). Impulsivity as a mechanism linking child abuse and neglect with substance use in adolescence and adulthood. Dev Psychopathol, 1–19. doi: 10.1017/S0954579417000943 [DOI] [PubMed] [Google Scholar]
- Oswald Lynn M, Wand Gary S, Kuwabara Hiroto, Wong Dean F, Zhu Shijun, & Brasic James R. (2014). History of childhood adversity is positively associated with ventral striatal dopamine responses to amphetamine. Psychopharmacology, 231(12), 2417–2433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petry Nancy M. (2001). Substance abuse, pathological gambling, and impulsiveness. Drug and Alcohol Dependence, 63(1), 29–38. doi: 10.1016/s0376-8716(00)00188-5 [DOI] [PubMed] [Google Scholar]
- Porges Stephen W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation (Norton Series on Interpersonal Neurobiology): WW Norton & Company. [Google Scholar]
- Preacher Kristopher J, Rucker Derek D, & Hayes Andrew F. (2007). Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivariate behavioral research, 42(1), 185–227. [DOI] [PubMed] [Google Scholar]
- Puetz Vanessa B, & McCrory Eamon. (2015). Exploring the relationship between childhood maltreatment and addiction: a review of the neurocognitive evidence. Current addiction reports, 2(4), 318–325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quintana Daniel S, McGregor Iain S, Guastella Adam J, Malhi Gin S, & Kemp Andrew H. (2013). A meta-analysis on the impact of alcohol dependence on short-term resting-state heart rate variability: Implications for cardiovascular risk. Alcoholism: Clinical and Experimental Research, 37(s1). [DOI] [PubMed] [Google Scholar]
- Rogers Robert D, Moeller Frederick G, Swann Alan C, & Clark Luke. (2010). Recent research on impulsivity in individuals with drug use and mental health disorders: implications for alcoholism. Alcoholism: Clinical and Experimental Research, 34(8), 1319–1333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romer Daniel, & Hennessy Michael. (2007). A biosocial-affect model of adolescent sensation seeking: The role of affect evaluation and peer-group influence in adolescent drug use. Prevention Science, 8(2), 89. [DOI] [PubMed] [Google Scholar]
- Rubin Donald B, & Little Roderick JA. (2002). Statistical analysis with missing data. Hoboken, NJ: J Wiley & Sons. [Google Scholar]
- Rudolph Marc D, Miranda-Domínguez Oscar, Cohen Alexandra O, Breiner Kaitlyn, Steinberg Laurence, Bonnie Richard J, … Fettich Karla C. (2017). At risk of being risky: The relationship between “brain age” under emotional states and risk preference. Developmental cognitive neuroscience, 24, 93–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schriber Roberta A, & Guyer Amanda E. (2016). Adolescent neurobiological susceptibility to social context. Developmental cognitive neuroscience, 19, 1–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Selin Klara Hradilova. (2003). Test-retest reliability of the alcohol use disorder identification test in a general population sample. Alcoholism: Clinical and experimental research, 27(9), 1428–1435. [DOI] [PubMed] [Google Scholar]
- Shonkoff Jack P, Boyce W Thomas, & McEwen Bruce S. (2009). Neuroscience, molecular biology, and the childhood roots of health disparities: building a new framework for health promotion and disease prevention. Jama, 301(21), 2252–2259. [DOI] [PubMed] [Google Scholar]
- Sinha R (2008). Chronic stress, drug use, and vulnerability to addiction. Ann N Y Acad Sci, 1141, 105–130. doi: 10.1196/annals.1441.030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg Laurence. (2010). A dual systems model of adolescent risk-taking. Developmental Psychobiology: The Journal of the International Society for Developmental Psychobiology, 52(3), 216–224. [DOI] [PubMed] [Google Scholar]
- Stormshak Elizabeth, DeGarmo David, Chronister Krista, & Caruthers Allison. (2017). The Impact of Family-Centered Prevention on Self-Regulation and Subsequent Long-Term Risk in Emerging Adults. Prevention Science, 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration (2006) Results from the 2005 National Survey on Drug Use and Health: National Findings (Office of Applied Studies, NSDUH Series H-30, DHHS Publication No. SMA 06-4194), Rockville, MD. [Google Scholar]
- Thayer JF. (2009). Heart rate variability: a neurovisceral integration model.
- Thayer Julian F, & Brosschot Jos F. (2005). Psychosomatics and psychopathology: looking up and down from the brain. Psychoneuroendocrinology, 30(10), 1050–1058. [DOI] [PubMed] [Google Scholar]
- Thayer Julian F, & Lane Richard D. (2000). A model of neurovisceral integration in emotion regulation and dysregulation. Journal of affective disorders, 61(3), 201–216. [DOI] [PubMed] [Google Scholar]
- Thayer Julian F, & Siegle Greg J. (2002). Neurovisceral integration in cardiac and emotional regulation. IEEE Engineering in Medicine and Biology Magazine, 21(4), 24–29. [DOI] [PubMed] [Google Scholar]
- Thibodeau Eric L, Cicchetti Dante, & Rogosch Fred A. (2015). Child maltreatment, impulsivity, and antisocial behavior in African American children: Moderation effects from a cumulative dopaminergic gene index. Development and psychopathology, 27(4pt2), 1621–1636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tofighi Davood, & MacKinnon David P. (2011). RMediation: An R package for mediation analysis confidence intervals. Behavior research methods, 43(3), 692–700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vinogradov Sophia, Fisher Melissa, & de Villers-Sidani Etienne. (2012). Cognitive training for impaired neural systems in neuropsychiatric illness. Neuropsychopharmacology, 37(1), 43–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Werner Natalie S, Duschek Stefan, & Schandry Rainer. (2009). Relationships between affective states and decision-making. International Journal of Psychophysiology, 74(3), 259–265. [DOI] [PubMed] [Google Scholar]
- Zelazo Philip David, & Carlson Stephanie M. (2012). Hot and cool executive function in childhood and adolescence: Development and plasticity. Child Development Perspectives, 6(4), 354–360. [Google Scholar]
- Zucker Robert A, Donovan John E, Masten Ann S, Mattson Margaret E, & Moss Howard B. (2008). Early developmental processes and the continuity of risk for underage drinking and problem drinking. Pediatrics, 121(Supplement 4), S252–S272. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.