

Summary
Background
Multilevel approaches involving environmental strategies are considered to be good practice to help reduce the prevalence of childhood overweight.
Objectives
The objective of this study was to evaluate the effects of VIASANO, a community‐based programme using the EPODE methodology, on the prevalence of overweight in two pilot towns in Belgium.
Methods
We analysed data from a national school health monitoring system to compare changes in the prevalence of overweight and obesity over a 3‐year period (2007–2010) in children aged 3–4 and 5–6 years in the pilot towns with those of children of the same ages from the whole French‐speaking community of Belgium. Heights and weights of all participants were measured by trained school nurses using a standardized method.
Results
The prevalence of overweight (−2.1%) and overweight + obesity (−2.4%) decreased in the pilot towns, but remained stable in the comparison population (+0.1% and +0.2%, respectively). After adjustment for lack of homogeneity between the study populations, there was a trend towards a decrease in overweight (P = 0.054) and overweight + obesity (P = 0.058) in the pilot towns compared with the general population.
Conclusions
These results suggest that a community‐based programme, such as VIASANO, may be a promising strategy for reducing the prevalence of childhood overweight even over a short period of time.
Keywords: Childhood overweight, community‐based intervention, EPODE, prevention, obesity
Abbreviations
- BMI
body mass index
- CI
confidence interval
- EPODE
Ensemble Prévenons l'Obésité Des Enfants
Introduction
During the past 20 years, the prevalence of obesity, and of childhood obesity in particular, has increased throughout Europe and indeed most of the world 1, 2, 3, making this condition one of the main public health challenges of the 21st century. Although this trend seems to be stabilizing in some countries 4, 5, prevalences overall remain unacceptably high.
Childhood obesity can cause social, psychological and health problems 6, and is linked to obesity in adulthood 7, with considerable long‐term health and economic burden 8. Because reversal of obesity is difficult, prevention is crucially important 9, 10. Nevertheless, data suggest that focusing on individual behavioural change by modifying cognitive determinants alone, without broader social, cultural, physical, economic and political perspectives, is not effective 11, 12. Although evidence from controlled studies is inconclusive 13, multilevel and community‐based approaches to childhood obesity prevention 11, 12, 14, 15 are considered to be good practice 16, 17.
The EPODE (‘Ensemble Prévenons l'Obésité Des Enfants’) methodology was developed in 2004 in France as a community‐based programme that included broad environmental strategies to stimulate long‐term, sustainable behavioural change and prevent childhood obesity 18, 19, 20. The effects of using this approach in France appear promising 21, 22 and this strategy has since been adopted by many other countries in Europe and further afield (http://www.epode‐international‐network.com). Adoption of the EPODE methodology in Belgium resulted in the creation of the VIASANO programme (http://www.viasano.be). Starting with two towns in 2006, VIASANO now involves 19 towns in the French‐speaking and Flemish communities of Belgium.
Given the paucity of reports on the effectiveness of community‐based programmes to prevent obesity, especially in young children 23, 24, it is important to evaluate the effects of VIASANO on the prevalence of overweight and obesity. Here we report some initial results, comparing cross‐sectional data on changes in body mass index (BMI) from children in two pilot VIASANO towns situated in the French‐speaking part of Belgium, with data from children in the whole of the French‐speaking community of Belgium. Using this large community database as the comparison population we aimed to avoid any potential bias introduced by selection of a small number of control towns.
Participants and methods
Towns
The two pilot VIASANO towns were Mouscron, an urban town of 54 651 inhabitants, and Marche‐en‐Famenne, a rural town of 17 175 inhabitants, both within the French‐speaking community of Belgium. These towns were selected for the present analysis because they had been in the programme for at least 3 years 1 and full data (heights and weights of 3–6‐year‐old children) were available. The pilot towns had similar socio‐economic demographics to each other and to the rest of the French‐speaking community (Supporting Information Table S1).
The VIASANO project
In line with the EPODE methodology 19, VIASANO operates from a dual perspective: (i) targeting the local population via social‐marketing techniques using local communication channels and (ii) targeting the environment or community in collaboration with local actors. Some examples of social‐marketing campaigns that have been targeted at the local populations are shown in the Supporting Information Table S2. The number of participants exposed to these actions varies according to the target group, from 20 to 30 for school classes or health professionals, up to 500 people for actions targeted at the general public. A rough estimate based on the nature and the number of these actions multiplied by the mean number of participants suggests that about 30 000 people were reached between 2007 and 2010.
Actions targeting the environment/community have ranged from renovation of a dilapidated residential area initiated by the local population in collaboration with the local authorities, collaboration with local police to make active commuting to schools safer, using local media to change social norms, or discussing the incorporation of health issues into school or company policies.
The number of events targeting children and families (n = 116) is approximately the same as the number of actions that have targeted the environment/community (n = 127). Between 2007 and 2010, the number of events taking place in Mouscron and Marche‐en‐Famenne increased every year (Supporting Information Figure S1).
Participants
For the present analysis, all children aged 3–4 (first‐year preschool) and 5–6 (third‐year preschool) years old who were living in Mouscron and Marche‐en‐Famenne in the years 2007 and 2010 were included. The comparison population consisted of children of the same ages and in the same school years from the whole French‐speaking community in Belgium (thus also including those from the two pilot towns) in 2007 (N = 76 864) and 2010 (N = 79 602).
Measurements
Data for the analysis were derived from the school health community surveillance registry (http://www.sante.cfwb.be), which records all children's weights and heights, independently measured at school by nurses working for the promotion of health in schools, a service of the French Community of Belgium. The nurses are trained to perform the measurements according to a specific measurement protocol 25. Weight is measured in light clothes (without shoes) to the nearest 0.1 kg using electrical digital scales (SECA, Hamburg, Germany). Standing height (without shoes) is measured to the nearest 0.5 cm by a ruler fixed to the wall. BMI is calculated as weight in kg divided by the square of the height in m (kg/m2). For the two pilot towns, the raw data (height, weight, BMI) were available, but for the whole French community, because of administrative restrictions, only data on percentages of overweight and obesity were available.
Statistical methods
The proportions of overweight and obese children were calculated for each study town, each period and each age group, using Flemish growth curves 26. 2 Similar percentages were obtained for the comparison population. Overweight and obesity were defined as values above the 85th and 97th percentiles, respectively.
For analysis of changes in the prevalence of overweight and obesity between 2007 and 2010, the two studied age groups were combined. Chi‐square tests were used to compare the proportions of overweight, obese, and overweight + obese children in 2007 and 2010, and to compare the distributions of BMI categories between the pilot towns and the comparison population. The differences in the proportions between the two study periods were calculated and their 95% confidence intervals (CI) computed. A z‐test 27 was used to compare the crude differences and the differences adjusted for sex and school grade in the pilot towns and in the comparison population. All analyses were performed using STATA v12.1 (StataCorp LP, College Station, TX, USA).
Results
A total of 1300 children were included from the two pilot towns for 2007 and 1484 children for 2010. Taking the two towns together, 9.5% of the children were overweight and 4.1% obese in 2007; in 2010, these proportions had decreased to 7.4% (−2.1%) and 3.8% (−0.3%), respectively (Table 1). The prevalence of overweight + obesity decreased from 13.6 to 11.2% (−2.4%, 95% CI −4.9 to 0.0%) (Table 2, Fig. 1). In the pilot towns, the proportion of children attending the 1st pre‐school year was higher in 2010 than in 2007 (732/1484 [49%] vs. 559/1300 [43%], Table 1); this finding may have influenced the results because the proportion of normal weight children was lower in the third preschool year. After adjustment for sex and school grade, the prevalence of overweight had decreased by 2% (P = 0.060), of obesity by 0.2% (P = 0.80) and of overweight + obesity by 2.2% (P = 0.082) (Table 2).
Table 1.
Proportions of overweight, obese and overweight + obese children for each population, period and school level
| Region | 2007 | 2010 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean age in months (SD) | Boys (%) | Overweight (%) | Obesity (%) | Overweight + Obesity (%) | Total N | Mean age in months (SD) | Boys (%) | Overweight (%) | Obesity (%) | Overweight + Obesity (%) | |
| Mouscron | ||||||||||||
| First‐year year pre‐school, age 3–4 | 414 | 46.8 (3.9) | 45.9 | 9.7 | 2.2 | 11.8 | 576 | 46.3 (3.5) | 49.7 | 7.3 | 3.1 | 10.4 |
| Third‐year pre‐school, age 5–6 | 558 | 68.3 (4.5) | 51.6 | 10.0 | 5.6 | 15.6 | 586 | 68.9 (4.5) | 47.6 | 8.4 | 4.3 | 12.6 |
| Marche‐en‐Famenne | ||||||||||||
| First‐year pre‐school, age 3–4 | 145 | 46.9 (3.6) | 49.7 | 6.9 | 3.4 | 10.3 | 156 | 46.8 (3.6) | 48.7 | 5.1 | 3.2 | 8.3 |
| Third‐year pre‐school, age 5–6 | 183 | 67.9 (4.8) | 50.8 | 9.3 | 4.4 | 13.7 | 166 | 65.9 (4.9) | 49.4 | 6.6 | 4.8 | 11.4 |
| Mouscron + Marche‐en‐Famenne | ||||||||||||
| First‐year pre‐school, age 3–4 | 559 | 46.8 (3.8) | 46.9 | 8.9 | 2.5 | 11.4 | 732 | 46.4 (3.5) | 49.5 | 6.8 | 3.1 | 10.0 |
| Third‐year pre‐school, age 5–6 | 741 | 68.2 (4.6) | 51.4 | 9.9 | 5.3 | 15.1 | 752 | 68.2 (4.7) | 48.0 | 8.0 | 4.4 | 12.3 |
| First and third‐years pre‐school | 1300 | 59.0 (11.4) | 49.5 | 9.5 | 4.1 | 13.6 | 1484 | 57.5 (11.7) | 48.7 | 7.4 | 3.8 | 11.2 |
| Comparison population (French Community) | ||||||||||||
| First‐ + third‐year pre‐school | 76864 | NA | 51.5 | 9.5 | 6.3 | 15.8 | 79602 | NA | 51.1 | 9.6 | 6.4 | 16.0 |
NA, not available; SD, standard deviation.
Table 2.
Comparison of changes in proportions of obesity and overweight between 2007 and 2010 in Marche‐en‐Famenne + Mouscron (pilot towns)
| Marche‐en‐Famenne + Mouscron (pilot towns) | Difference (95% CI) between 2007 and 2010 | Adjusted difference (95% CI) between 2007 and 2010* | P‐value |
|---|---|---|---|
| Overweight | −2.1 (−4.1 to 0.0)% | −2.0 (−4.0 to 0.0)% | 0.060 |
| Obesity | −0.3 (−1.7 to +1.1)% | −0.2 (−1.6 to +1.3)% | 0.80 |
| Overweight + obesity | −2.4 (−4.9 to 0.0)% | −2.2 (−4.6 to +0.3)% | 0.082 |
*Adjusted for sex and school grade. CI, confidence interval.
Figure 1.
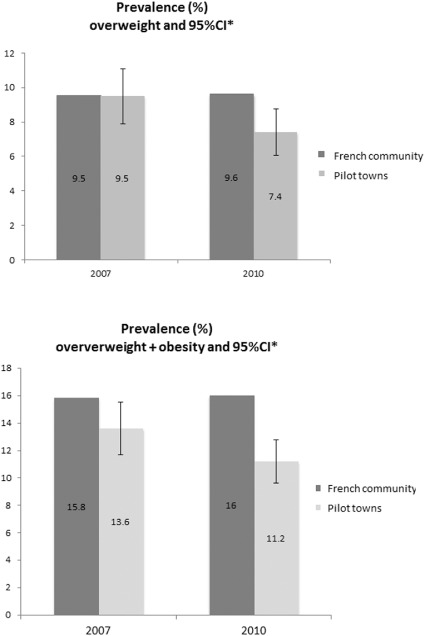
Evolution of the prevalence of overweight (upper panel) and overweight + obesity (lower panel) in the pilot towns and the comparison population (French Community). *95% confidence interval (CI) computed only for the pilot towns (Marche and Mouscron).
In the comparison population, there were 76 864 and 79 602 children for the school years 2007 and 2010, respectively. In 2007, 9.5% of these children were overweight and 6.3% obese; in 2010, these proportions were stable at 9.6% and 6.4%, respectively.
There was a trend to a reduction in the prevalence of overweight (−2% vs. +0.1%, P = 0.054) and overweight + obesity (−2.2% vs. +0.2%, P = 0.058) in the pilot towns compared with the control population (Table 3).
Table 3.
Comparison of changes in proportions of obesity and overweight between 2007 and 2010 in Marche‐en‐Famenne + Mouscron (pilot towns) with changes in the comparison population (French Community)
| Adjusted difference (95% CI) between 2007 and 2010 (pilot towns) | 2007 % in comparison population | 2010 % in comparison population | Difference between 2007 and 2010 in comparison population | P‐value | |
|---|---|---|---|---|---|
| Overweight | −2.0 (−4.0 to 0.0)% | 9.5 | 9.6 | +0.1% | 0.054 |
| Obesity | −0.2 (−1.6 to +1.3)% | 6.3 | 6.4 | +0.1% | 0.69 |
| Overweight + obesity | −2.2 (−4.6 to +0.3)% | 15.8 | 16.0 | +0.2% | 0.058 |
CI, confidence interval.
The chi‐squared test showed a difference in the categories of BMI in the pilot towns and the comparison population: in 2007, there were significantly fewer obese children in the pilot towns than in the comparison population (4.1% vs. 6.3%, P = 0.004); in 2010, the gap had increased with even fewer obese children in the pilot towns compared with the comparison population (3.8% vs. 6.4%; P < 0.0001).
Discussion
The aim of this study was to analyse trends in the prevalence of childhood overweight and obesity over a 3‐year period to gain early insight into the effectiveness of the VIASANO obesity prevention programme in two pilot towns. Given the methodological challenges of evaluating complex public health interventions and the difficulty of randomly assigning entire communities in community‐based programmes 15, 23, 28, we adopted a pragmatic approach to evaluate this intervention. Instead of comparing the prevalence of obesity with selected control towns, we chose to examine trends across the whole of the region, using data from a community surveillance programme for comparison (http://www.sante.cfwb.be). This approach, which can be viewed as a quasi experimental design 23, provides a more robust analysis and benefits from the fact that weights and heights were measured using the same standardized method by independent observers in the study and comparison populations. Our results show a trend to a reduction in the prevalence of overweight and in the prevalence of overweight + obesity in the participating communities, which was not present in the comparison population.
These results can be compared with those reported in the EPODE pilot towns, in which there was a significant decrease in the proportion of overweight and obese children (from 20.6% to 18.8%, P < 0.0001) during a 5‐year intervention period 29. This reduction (−1.8%), although smaller in absolute value than that reported in the present study (−2.4%), was significant in the EPODE study but not in VIASANO, possibly because of the longer intervention period, the larger sample sizes involved or differences in the ages of the children assessed.
For the reasons explained in the methods section, our analysis is based on Flemish growth curves, rather than international IOTF curves. The Flemish community of Belgium developed its own growth curves for children in order to have a better tool to define obesity and overweight in this part of the Belgian population. There are few socio‐cultural differences between the two main Belgian communities (Flemish and French‐speaking) and there are no equivalent curves specifically for the French‐speaking part of Belgium, so the French community decided to use the Flemish growth curves. However, the cut‐off points for the definitions of overweight and obesity are lower on the Flemish curves than on the IOTF curves; hence, estimations of the prevalence of overweight and obesity would be expected to be higher when using the Flemish curves than with the IOTF curves 30. Nevertheless, because the same definitions were used for the pilot towns and the comparison population, our comparisons remain valid.
The results of the present study provide evidence of early promise for this community‐based intervention, but should be interpreted with caution for several reasons. First, because of the non‐randomized nature of our study, our results may be subject to observational bias in the measurements of height and weight. However, measurement techniques were standardized in the pilot towns and the comparison population, performed by the same staff, using the same methods in both settings.
Second, at baseline in 2007, there were fewer obese children in the pilot towns than in the comparison population, which may explain some of the observed differences with a lower prevalence of overweight + obesity at the end of the 3‐year period in the pilot towns than in the overall population. However, it is notable that in the pilot towns, although the prevalence of obesity was initially lower than in the comparison population, it decreased further over this short period, increasing the gap between the pilot towns and the whole community.
Third, there were differences in the sex and school‐grade distributions between the pilot towns and the comparison population. In the pilot towns, there were more 1st pre‐school year children in 2010 than in 2007 (732 vs. 559), whereas the numbers were similar (752 vs. 741) for 3rd pre‐school year children. This could potentially have influenced the results because the proportion of healthy weight children was lower in the 3rd pre‐school year. To account for this possibility, we, therefore, adjusted for sex and school grade in our analysis.
Many factors need further evaluation, including longer‐term effects and whether similar trends can be confirmed in other participating towns. If so, it would be interesting to try and determine which elements of the programme contribute most strongly to the observed results, e.g., what changes in behaviour are associated with better results or with specific aspects of the programme, what variables can be linked to different outcomes in different towns, and whether this provides indications as to how to help individual towns achieve better results.
In conclusion, the results of this first evaluation are encouraging and provide further evidence that community‐based programmes, such as VIASANO, may play a role in the prevention of childhood overweight, although further analyses are needed to confirm these preliminary findings.
Conflicts of Interest Statement
The VIASANO project is partly sponsored by private partners: Carrefour Belgium, Ferrero, Orangina‐Schweppes, Unilever. The role of the private partners is regulated via an ethical charter (Supporting Information Appendix S1) in order to exclude any influence on the content of actions. These partners have no influence on the content of the VIASANO programme and played no role in the data analysis or in the writing of this paper. JB, NJ, MR, MD and CDL have received payment from Protein Health Communications, who coordinate VIASANO. The other authors declare that they have no conflicts of interest.
Supporting information
Figure S1. Number of actions per year.
Table S1. Basic socio‐economic data for the pilot towns and the comparison whole French‐speaking community.
Table S2. List of topics used in some of the early VIASANO campaigns and examples of actions that have targeted the local population.
Appendix S1. Partners Charter in the VIASANO Programme.
Acknowledgements
The weight and height data were provided by the General Health Direction (Fédération Wallonie‐Bruxelles). JV and J‐MB designed the study. JB collected the data and wrote the first draft of the paper. MD performed the statistical analyses. CB, NJ, MR, SJ, MD, CDL and JN reviewed and revised the paper. All authors read and approved the final version of the paper for publication.
Vinck, J. , Brohet, C. , Roillet, M. , Dramaix, M. , Borys, J.‐M. , Beysens, J. , Jacobs, N. , Jebb, S. , De Laet, C. , and Nève, J. (2016) Downward trends in the prevalence of childhood overweight in two pilot towns taking part in the VIASANO community‐based programme in Belgium: data from a national school health monitoring system. Pediatric Obesity, 11: 61–67. doi: 10.1111/ijpo.12022.
Footnotes
Other French‐speaking towns started later, and administrative issues for obtaining BMI data for the children of the participating Flemish towns were not completely resolved at the time of writing.
Because specific growth curves for the French‐speaking population are not available, the French Community uses Flemish growth curves to calculate proportions of overweight and obese children. Because of administrative constraints, we had no access to raw data for this population, so we also used the Flemish growth curves to calculate proportions of overweight and obesity in the pilot towns in order to be able to compare the different sets of data.
References
- 1. World Health Organization . Childhood overweight and obesity on the rise. 2010. [WWW document]. URL http://www.who.int/dietphysicalactivity/childhood/en (accessed March 14, 2015).
- 2. Ng M, Fleming T, Robinson M, et al Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014; 384: 766–781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Institut Scientifique de Santé Publique . Enquête de santé par interview, Belgique 2008: Etat nutritionel. 2010. [WWW document]. URL https://his.wiv‐isp.be/fr/Documents%20partages/NS_FR_2008.pdf (accessed March 14, 2015).
- 4. Sundblom E, Petzold M, Rasmussen F, Callmer E, Lissner L. Childhood overweight and obesity prevalences levelling off in Stockholm but socioeconomic differences persist. Int J Obes (Lond) 2008; 32: 1525–1530. [DOI] [PubMed] [Google Scholar]
- 5. Peneau S, Salanave B, Maillard‐Teyssier L, et al Prevalence of overweight in 6‐ to 15‐year‐old children in central/western France from 1996 to 2006: trends toward stabilization. Int J Obes (Lond) 2009; 33: 401–407. [DOI] [PubMed] [Google Scholar]
- 6. Tsiros MD, Olds T, Buckley JD, et al Health‐related quality of life in obese children and adolescents. Int J Obes (Lond) 2009; 33: 387–400. [DOI] [PubMed] [Google Scholar]
- 7. Reilly JJ, Kelly J. Long‐term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes (Lond) 2011; 35: 891–898. [DOI] [PubMed] [Google Scholar]
- 8. Wang YC, McPherson K, Marsh T, Gortmaker SL, Brown M. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet 2011; 378: 815–825. [DOI] [PubMed] [Google Scholar]
- 9. Singh AS, Mulder C, Twisk JW, van Mechelen W, Chinapaw MJ. Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Rev 2008; 9: 474–488. [DOI] [PubMed] [Google Scholar]
- 10. Waters E, de Silva‐Sanigorski A, Hall BJ, et al Interventions for preventing obesity in children. Cochrane Database Syst Rev 2011; CD001871. [DOI] [PubMed] [Google Scholar]
- 11. Hollar D, Lombardo M, Lopez‐Mitnik G, et al Effective multi‐level, multi‐sector, school‐based obesity prevention programming improves weight, blood pressure, and academic performance, especially among low‐income, minority children. J Health Care Poor Underserved 2010; 21: 93–108. [DOI] [PubMed] [Google Scholar]
- 12. Gibbs L, Waters E, St Leger L, Green J, Gold L, Swinburn B. A settings‐based theoretical framework for obesity prevention community interventions and research. Aust N Z J Public Health 2011; 35: 104–106. [DOI] [PubMed] [Google Scholar]
- 13. Khambalia AZ, Dickinson S, Hardy LL, Gill T, Baur LA. A synthesis of existing systematic reviews and meta‐analyses of school‐based behavioural interventions for controlling and preventing obesity. Obes Rev 2012; 13: 214–233. [DOI] [PubMed] [Google Scholar]
- 14. King L, Gill T, Allender S, Swinburn B. Best practice principles for community‐based obesity prevention: development, content and application. Obes Rev 2011; 12: 329–338. [DOI] [PubMed] [Google Scholar]
- 15. Wolfenden L, Wyse R, Nichols M, Allender S, Millar L, McElduff P. A systematic review and meta‐analysis of whole of community interventions to prevent excessive population weight gain. Prev Med 2014; 62: 193–200. [DOI] [PubMed] [Google Scholar]
- 16. Bemelmans WJ, Wijnhoven TM, Verschuuren M, Breda J. Overview of 71 European community‐based initiatives against childhood obesity starting between 2005 and 2011: general characteristics and reported effects. BMC Public Health 2014; 14: 758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Lundy J, Bowdish L. Navigating Obesity: A Road Map Prevention. 2013. [WWW document]. URL http://www.uschamberfoundation.org/sites/default/files/publication/ccc/USCCF_ObesityReport_FINAL.pdf (accessed March 14, 2015).
- 18. Borys JM, Le Bodo Y, Jebb SA, et al EPODE approach for childhood obesity prevention: methods, progress and international development. Obes Rev 2012; 13: 299–315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Borys JM, Le Bodo Y, De Henauw S, et al Preventing Childhhod Obesity. EPODE European Network Recommendations. Cachan: Lavoisier, 2011.
- 20. Pettigrew S, Borys JM, du Plessis HR, et al Process evaluation outcomes from a global child obesity prevention intervention. BMC Public Health 2014; 14: 757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Romon M, Lommez A, Tafflet M, et al Downward trends in the prevalence of childhood overweight in the setting of 12‐year school‐ and community‐based programmes. Public Health Nutr 2009; 12: 1735–1742. [DOI] [PubMed] [Google Scholar]
- 22. Romon M, Duhamel A, Salleron J, Lommez A, Meyer J, Borys J. Évolution de la prévalence du surpoids et de l'obésité chez les enfants de 4 à 11 ans entre 2005 et 2010 dans les villes « EPODE ». Nutrition Clinique Et Métabolisme 2010; 24(S1): 58. (abst). [Google Scholar]
- 23. Bleich SN, Segal J, Wu Y, Wilson R, Wang Y. Systematic review of community‐based childhood obesity prevention studies. Pediatrics 2013; 132: e201–e210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Foster GD, Sundal D, Lent MR, McDermott C, Jelalian E, Vojta D. 18‐month outcomes of a community‐based treatment for childhood obesity. Pediatr Obes 2014; 9: e63–e67. [DOI] [PubMed] [Google Scholar]
- 25. Berghmans L, Massot C. Carnet de bord de la santé des jeunes 2010. 2010. [WWW document]. URL http://www.hainaut.be/sante/osh/medias_user/CBSJ2010_full.pdf (accessed March 14, 2015).
- 26. Laboratorium voor Antropogenetica . Growth Charts Flanders 2004. 2004. [WWW document]. URL http://www.vub.ac.be/groeicurven/english.html (accessed March 14, 2015).
- 27. Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ 2003; 326: 219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Victora CG, Habicht JP, Bryce J. Evidence‐based public health: moving beyond randomized trials. Am J Public Health 2004; 94: 400–405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Borys JM. Encouraging results in French EPODE pilot towns. EEN Newsletter No 5. 2010. [WWW document]. URL http://www.epode‐european‐network.com/index.php?option=com_content&view=article&id=154&Itemid=74&lang=en (accessed March 14, 2015).
- 30. Roelants M, Hauspie R, Hoppenbrouwers K. References for growth and pubertal development from birth to 21 years in Flanders, Belgium. Ann Hum Biol 2009; 36: 680–694. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Number of actions per year.
Table S1. Basic socio‐economic data for the pilot towns and the comparison whole French‐speaking community.
Table S2. List of topics used in some of the early VIASANO campaigns and examples of actions that have targeted the local population.
Appendix S1. Partners Charter in the VIASANO Programme.